chapter 20 Working with Elders Who Have Dementia and Alzheimer’s Disease
1. Understand that elders with Alzheimer’s disease (AD) are persons first; they are not their disease. Therefore, person-centered care (personalized) focuses on overall well-being, reflecting the elders’ remaining strengths and abilities.
2. Describe person-centered care and personhood.
3. Gain awareness and sensitivity to the cognitive, physical, and psychosocial needs of elders with AD.
4. Describe occupation-focused care.
5. Relate suggestions to promote wellness through task simplification and modification.
6. Identify caregiving techniques, approaches, and interventions that can be used to help empower elders who have AD to participate in daily living tasks.
7. Suggest appropriate communication responses to elders with AD.
8. Problem solve antecedents and approaches to refocus unwanted behavioral responses.
Alzheimer’s disease, activity-focused care, personhood, person-centered care, “therapeutic fibs,” creative reality, rescuing, chaining, bridging
Travis is a certified occupational therapy assistant (COTA) who works in a skilled nursing facility. One of his responsibilities is consulting with staff at a special care unit for persons with AD. John, the charge nurse on the unit, contacts Travis. “We are having problems with Grace. She is wandering in and out of others’ rooms and taking their possessions, which is irritating the other residents. She is also having difficulty communicating her needs. Her performance with activities of daily living (ADL) functions seems variable. We are also having problems with increased agitation with Grace and all of our residents, especially at shift change. Do you have any ideas?”
Hilde is a COTA working on a subacute unit. Ruth, one of the elders, was admitted after a total hip replacement. After reviewing her chart, Hilde finds out that Ruth has a history of AD. Both Travis and Hilde can provide practical suggestions to better help these elders with AD function. This chapter provides background information about AD and occupational therapy (OT) interventions.
An estimated 5.3 million Americans have AD. AD is the sixth leading cause of all deaths in the United States, and the fifth leading cause of death in Americans age 65 and older.1 Between 2000 and 2006, heart disease deaths decreased nearly 12%, stroke deaths decreased 18%, and prostate cancer–related deaths decreased 14%, whereas deaths attributable to AD increased 47%.1 Every 70 seconds someone in the United States develops AD, and, by 2050, this time is expected to decrease to every 33 seconds.2 Over the coming decades, the “baby-boom” population is projected to add 10 million people to these numbers. In 2050, the incidence of AD in the United States is expected to approach nearly a million people per year, with a total estimated prevalence of 11 to 16 million people.3 The incidence of AD across the world is expected to double every 20 years so that today’s figure of 35.6 million people with the disease will rise to 65.7 million by 2030 and 115.4 million by 2050, if a cure is not found.4
Dementia does not follow a uniform or single predictable course. The dementia syndrome includes unpredictable fluctuations in basic memory, judgment, and performance.5 While depression, medications, and metabolic dysfunction may cause a reversible dementia, nonreversible dementia may be caused by small strokes (vascular dementia), dementia with Parkinson’s disease, dementia with Lewy bodies, frontal lobe dementias, and AD.6 Alzheimer’s is the most common form of dementia and accounts for 50% to 70% of cases.7 AD is a progressive, degenerative, and fatal disease of brain tissue that leads to memory loss and problems with thinking and carrying out daily life activities. Participation in routine occupations, using good judgment, being aware of surroundings, communicating effectively, and coping with life become more difficult as the disease progresses. Problems start gradually and become more severe over time, leading to a total disruption in performance patterns and the inability to participate in most areas of occupation.8 Although the rate of change varies, the usual stages are mild, moderate, severe, and terminal (Table 20-1).9
TABLE 20-1 Four Stages of Alzheimer’s Disease
| Early/mild impairment stage | Average 1 to 3 years, possibly longer Memory loss, especially with recent events Difficulty with complex cognitive tasks Difficulty with decision making and planning Decreased attention span and concentration Lack of spontaneity and lessening of initiative Impaired word-finding skills Preference for familiar settings |
| Mid-/moderate impairment stage | Average 5 to 7 years, possibly longer Chronic recent memory loss Difficulty with written and spoken language Tendency to ask questions constantly Tendency to experience visual-spatial perceptual problems Possible delusions, hallucinations, and agitation Increasing difficulty with familiar objects and tasks Assistance with ADL functions necessary Ability to respond to multisensory cueing Tendency to wander, pace, and rummage May get lost at times even inside the house |
| Late/severe impairment stage | Average 2 to 3 years Dependence on others for ADL functions Ability to respond to hand-over-hand activity Decreased interest in food Difficulty with chewing and swallowing Incontinence Decreased vocabulary Misidentification of familiar objects, persons Impaired ambulation/gait, increased falls Repetitious movement or sounds |
| Terminal stage | Average 3 months to 1 year Usually in bed or wheelchair Limited ability to track visually Mute or few incoherent words Little spontaneous movement Loss of appetite, severe weight loss Difficulty in swallowing Tendency to utter sounds rather than words Total dependence on others for care Possible development of contractions, skin breakdown Possible reaction to music and touch, fleeting attention span |
AD can last 3 to 20 years. Most people die after 8 years, often from pneumonia or other systemic problems. Causes of AD are not known, but current research suggests the involvement of two abnormal structures called plaques and tangles as prime suspects in damaging and killing nerve cells. Plaques are deposits of a protein fragment called beta-amyloid that build up between nerve cells. Tangles are twisted fibers of another protein called tau that form inside dying brain cells. Although most people develop some plaques and tangles as they age, those with Alzheimer’s tend to develop far more. The plaques and tangles tend to form in a predictable pattern, beginning in areas important in learning and memory and then spreading to other regions.8 With the help of standardized diagnostic criteria, physicians can now diagnose AD with an accuracy of 85% to 90% once symptoms occur.9,10 Intervention is based on the combination of medical and psychosocial support.8 Two types of medications are often used (cholinesterase and memantine) to support communication among nerve cells and delay problems with learning and memory.11 Recently, concerns have been raised about the growing number of herbal remedies, vitamins, and other dietary supplements being promoted as memory enhancers or interventions for AD. Claims of their effectiveness and safety are based mostly on anecdotal evidence or on very small clinical research studies.12 Because of unknown side effects or potentially dangerous interactions with prescribed medications, the COTA should encourage the elder and/or caregivers to consult a physician before beginning use of any alternative or complementary medicine approaches. Smith13 reported that of the 1.7 million residents of nursing homes in the United States, more than half have AD or some other form of dementia. COTAs work with elders who have AD and related dementia in hospitals, nursing homes, assisted living facilities, adult day programs, special care units, and homes. OT intervention for these elders usually focuses on participation in the various areas of occupation by concentrating on performance skills and patterns or modifying activity demands in considerations of various client factors and, the degree possible, within the elder’s context and environments.14
Person-Centered and Occupation-Focused Care for Elders with Alzheimer’s Disease
Like all human beings, elders who have AD or related dementia continue to seek meaningful participation in life. Although sometimes the behavior brought on by AD may make it appear as though they no longer are the same elders they once were, it is important to remember that they are not defined by the dementia.15,16 Personhood, as described by Kitwood,17 refers to one’s sense of self, the “I am” within each person. Kitwood described indicators of personhood and well-being for individuals with dementia, including the assertion of desire or will, the ability to experience and express a range of emotions, initiation of social contact, self-respect, humor, creativity, and self-expression. Person-specific or person-centered care daily supports elders with dementia and enhances and promotes their sense of personhood and meaning in life.18
The COTA developing a therapeutic program for elders with dementia individualizes care that supports wellness, strengths, and abilities. This personalized, or person-centered, care also supports the components of activity-focused care that recognizes that all of life is an activity of being and doing or, as OT philosophy articulates it, of seeking meaning through occupation.14 The tasks of life, therefore, are interconnected. The objectives of occupation-focused care include concentrating on abilities, not limitations; promoting the purposeful and meaningful use of time; supporting the sense of belonging; and enabling verbal and nonverbal communication skills. Occupation-focused care encourages positive behaviors and the development of interventions to refocus unwanted behaviors.18
Occupation-focused care redefines interventions, especially in long-term care settings and special care units. Success is achieved through augmenting the client’s strengths by reframing expectations and relating to all of daily life tasks as parts of meaningful occupation. It involves the willingness to enter the client’s world with sensitivity and flexibility and the provision of holistic support. In this process, the COTA must remain mindful that the goal is for the client to find meaning, not for the caregivers, staff, or OT personnel to understand such meaning.19
Communication: Understanding and Being Understood
Communicating with people who have AD is often challenging. As the disease progresses, verbal abilities decrease and communication continues through nonverbal gestures and sounds. Verbal and nonverbal communication reflects the same objectives: expressing thoughts and needs and supporting the elders’ self-image and a sense of worth. Other objectives for communication include improving socialization, maximizing quality of life, increasing involvement in a supportive community, understanding others, and promoting safety and comfort. COTAs must care enough to listen carefully. During the early stages of AD, changes that occur in language and communication include the onset of difficulty with using nouns. Substituted words are sometimes used for the noun.20 For example, Mary was asked to identify an object (a comb). Her response was, “Oh, honey, you know,” as she ran her hand through her hair. She was unable to use the noun comb but the gesture denoted she knew what the object was.
Reality orientation is usually embarrassing for elders with AD because of their inability to remember and retrieve words to answer questions. One type of response that maintains the dignity of elders with disorientation is to refrain from confronting them with corrections, especially if the confrontation would increase agitation. Caregivers should use creative reality with elders by focusing on the emotions being expressed and responding appropriately by validating feelings. Improvements in orientation and subjective sense of quality of life may result from verbal cues that encourage the person to use information processing rather than factual knowledge.21
A strategy called therapeutic fibs can be used as illustrated by the following story. Jim states, “My wife is taking me home in 5 minutes.” In reality, the intervention session has an additional 30 minutes remaining. Sue, the COTA, agrees with him, stating that he and his wife will soon be together and that he has a wonderful, caring wife. Sue realizes that a discussion of the amount of remaining time would increase Jim’s agitation. Sue, having validated Jim’s desire for his wife, can then redirect him to do a meaningful task. Elders asking for their mothers or wanting to go home may be seeking acceptance and the need to feel connected. They may also be expressing the need for safety, purposeful use of time, or the company of others. Telling them that their mother is dead or the facility is now their home can upset them. Instead, the COTA may say, “You are safe with me and I will be here today with you. If you are like your mother, she must have been wonderful. I miss my mother too; we used to have fun folding the laundry; perhaps you and I can work together.” The purpose of such communication is to acknowledge the meaning or emotion behind an elder’s statement.22
As the disease progresses, the ability to speak and understand decreases. Some elders become more intuitive, often with increased awareness of people’s attitudes and the environment.23 Therefore, caregivers should be aware of their nonverbal messages such as acting rushed, looking at the clock, sighing, or raising one’s voice. In time, elders with AD lose almost all language skills, but they may still occasionally utter a perfectly appropriate statement.24 For example, Juan talked a lot, but his words were just sounds that made no sense. When a caregiver impatiently spoke to him in an abrupt and firm tone, saying “Juan, time out; go to your room,” Juan responded, “In the military, I was in solitary confinement and I can do that standing on my head.” The family later confirmed that Juan had indeed been in the military and the story was true. The caregiver’s “drill sergeant” tone and body posture triggered Juan’s response.
People with AD need to experience acceptance and success, especially as their language skills diminish. COTAs can keep the dialogue going even when the words are few (Box 20-1).16
BOX 20-1 Suggestions for Improving Communication and Connectedness
 Attract the client’s attention by using touch and talking to him or her at eye level.
Attract the client’s attention by using touch and talking to him or her at eye level.
Use short, simple sentences to express one thought at a time. Be willing to repeat as needed, allowing time for the elder to respond. Do not appear rushed; offer the elder your full attention. Assess and limit distractions from the environment, such as the TV, vacuum cleaners, and loud nearby conversations.16
Be aware that asking questions often can be embarrassing for people with AD, who often have difficulty finding the right words for the answer. Instead, help them respond by giving as many multisensory verbal or nonverbal cues as possible. If asking a question, offer two choices. For example, ask Ella if she would like to shower before breakfast or after breakfast, showing her the towel and clean clothing that you are holding.
Do not try to apply logic or to give long explanations. Ignore the need to be right, to argue, or to confront. At times having information written down for elders helps them focus and understand, especially when they ask the same question repeatedly. For example, providing Richard with a business type letter with his name on it that states that his apartment has been paid in full and that he has a place to spend the night helps him retain the information. Be willing to supply this letter as often as he needs for reassurance of having a place to stay.
State requests with positive words (“Please sit here” rather than “Don’t sit there”).
Listen carefully to all of the words, gestures, and facial expressions that the person uses. Validate feelings behind the words. For example, if Henry’s words seem to make no sense but sound angry and upset, say, “You sound upset, Henry. I know when I feel that way I like a hug. Can I give you a hug?” However, be aware that some people are tactile defensive and become agitated when touched.
Realize that elders with AD often respond literally to words (because the fire alarm says “pull,” Hazel pulls it).
Be aware that elders with AD often revert to their primary language. COTAs may have to learn appropriate key words in that language to encourage therapy.
Behavior and Psychosocial Aspects
People with dementia are not “stupid”; they are forgetful and often maintain an inner wisdom. Like anyone else, they have needs and should be approached and cared for with respect. They also should have opportunities for proud and meaningful involvement. Knowledge of the elders’ life story often becomes the basis for COTAs to plan and carry out therapy. A “Life Story” book can be used for this purpose. This book can include pictures with captions, lists, favorite recipes, family traditions, schools attended, and military history. Using the book is an excellent tool for connecting with elders and as an intervention to refocus difficult behaviors and to reduce agitation.25
The behaviors of people with dementia are often attempts to communicate. For example, increased agitation may be the client’s way of communicating illness. Rapid pacing might be a sign of an inability to cope with others, escape from excessive noise, or environmental factors.26
Some of the typical behaviors displayed by people with AD include wandering, pacing, and rummaging or redistribution of personal belongings. Combativeness and aggression also can occur. Catastrophic reactions are explosive responses to distress.5 These reactions result from the inability to understand, interpret, and cope with real or imagined situations, people, the environment, or oneself. “Sun-downing” results from a combination of increased behavioral responses occurring in the mid-to-late afternoon. These responses often reflect physical problems such as dehydration and physical/emotional exhaustion. Screaming, yelling, and calling often reflect fear, a need for acceptance, and a lack of active participation and connectedness during the day. Other behavioral manifestations may include inappropriate sexual conduct, hitting or pushing staff or other elders, accusing or demanding speech, withdrawal from activities, and apathy. Elders with AD might also show perseveration in their actions by repetitious movement or sounds, such as wiping or patting the table surface, pulling on clothing, and shouting.27
Difficult behaviors are usually not done on purpose as a method of making care more difficult; rather, they are often part of the disease. At times, behaviors can be a problem to others but not to the elder.28 For example, Betty, who lives in a special care unit, goes into other people’s rooms. She looks through their closets and takes clothing and items from their drawers. This behavior suggests that Betty likes to feel in control and is “cleaning up the house.” Whose problem is it? Carmen, the owner of these possessions, is angry and feels that her privacy has been invaded. The facility staff meets the challenge of working with both people in a supportive way by identifying acceptable places for Betty to rummage, such as a bureau or desk in the social center and “busy boxes” or baskets filled with safe items. Examples of items to include in a “busy box” are balls of yarn, greeting cards, small scrapbooks, car brochures, maps, catalogs, fabric pieces, and carpet samples. Having Betty participate in the purposeful activity of carrying safe items can help address her need to feel connected.
A respectful response exists for every behavior. In some cases, attempting to reason with people with AD may not work, especially if they mistake others for people whom they do not like. Logic also may not work, especially with people who are having visual or auditory hallucinations.29 Usually, COTAs can identify the event that precipitated the unwanted behavior and make adjustments that might prevent it, stop it, or decrease the likelihood of recurrence. Three problem-solving tools can help refocus unwanted behavior: the behavioral profile, the behavioral analysis, and the behavioral observation form.
The behavioral profile is a tool used to examine the situation. COTAs can ask themselves the following thought-provoking questions: What exactly is happening? Why has the behavior happened, and what was the antecedent? Who is involved, and where is the behavior exhibited? When does the behavior usually occur? What now? (Box 20-2).
The behavioral analysis outlines the specific behavior by focusing on the client’s actions and defining the antecedent or possible causes. In addition, it outlines acceptable approaches and interventions with attention to the impact on the family, environment, and activity (Table 20-2).
TABLE 20-2 Problem: Pacing, or Wandering, or Both (Behavior Analysis Approach)
| Behaviors exhibited | Pacing with increases in speed, intensity, and length of time; unable to respond to normal fatigue Trying to exit area without supervision Displaying increased agitation, anxiety, frustration, pushing, or kicking Seemingly lost; packing and leaving Searching behavior for something unattainable (for example, mother) Inappropriately going into areas/rooms not their own |
| Possible cause or antecedent | May have feelings of fearfulness, insecurity May be reflecting on a past life role such as being in the workforce or being a parent May want to escape May be feeling out of control or sensing overmanipulation by others May be searching for something familiar or something lost May be acting consistent with former habits (always “on the go”) or doing a stress-reducing activity May reflect need for self-stimulation as a method to reestablish sense of well-being May be expressing a physical need such as hunger, constipation, or illness May result from anxiety, boredom, hyperenvironmental or hypoenvironmental stimulation |
| Interventions with the resident | Ask what the wandering is “telling” you: whether the client is hungry, needs to void, feels uncomfortable, is really lost. Identify positive aspects of the pacing/wandering. When attempting redirection, use a calm approach with eye contact. Use distraction techniques to break up the pacing pattern (offer to sit with the elder, have a glass of juice). Monitor elders for unwanted weight loss and excessive fatigue. Monitor elders for increased risks for falls and compromised safety. Have elders wear Medic-Alert ID bracelet of Alzheimer’s Association’s “Safe Return” program. Take photographs for the police, if elopement is a factor. Avoid stressful situations such as excessive environmental stimulation, too many people present, or overwhelming demands. Provide regular and consistent routines with familiar staff and caregivers. Develop a “head count” system for elders at high risk for elopement. |
| Family/caregiver focus | Discuss treatment approaches. Provide information on policies and procedures. Provide information such as the phone number of the local Alzheimer’s Association chapter and their “Safe Return” program. Instruct not to contradict the elder’s stories; instead, they should assure the elder that everything will be all right. This helps facilitate a sense of security and reduces feelings of fearfulness. Recommend to not overdramatize entrances, exits, and promises to return. Encourage walks with the elder and usage of walking areas, “discover” paths or fitness trails. Inform of possible risks for elopement even when the treatment area has a security system. Encourage use of local support groups for discussions with others. |
| Facility adaptations | Provide environmental changes and sensory stimulation to decrease stress and restlessness, and to increase physical well-being, gross motor skills, appetite, and healthy fatigue. Allow for environmental changes that promote purposeful ways to spend time. Remove environmental cues that suggest leaving the facility, such as coats and suitcases. Use familiar objects in rooms that facilitate a sense of comfort and security. Install Dutch doors, if permitted by regulations. Design walking areas, “discover” paths, or fitness trails within the care setting that offer safe, monitored spaces for pacing. Develop procedures to follow such as periodic unit safety checks and checks for missing persons. Provide routine orientation and escorts for new admissions. Alert visitors to facility procedures. For example, when leaving an area visitors should turn around and check that wandering elders have not followed them out of the door. Employ experienced, trained staff who know the elders. Introduce the elder to all staff, especially those near the doors (for example, switchboard operators and receptionists). Write problems/interventions on a Kardex after identifying any positive aspects from the physical activity of pacing and wandering. |
| Activity | Support physical exercise to promote overall wellness. Offer to walk with the elder as a meaningful activity. Suggest that the elder help out by taking letters to be mailed, visiting a friend, or picking up laundry. Establish a walking club, keep track of miles walked, and provide club t-shirts. Provide supervised outings with a focus on safety and the reduction of elopement risks. Offer expressive arts that include large muscle groups and movement or dancing activities. Present routine, familiar, normalized activities that promote sense of connectedness, respect, and meaningfulness. Set up a fitness trail that includes repetitive upper and lower extremity movements such as doing pulley activities, finger climbing ladders, and deep knee bends. Train volunteers and family members to involve the elders with the trail’s activities. |
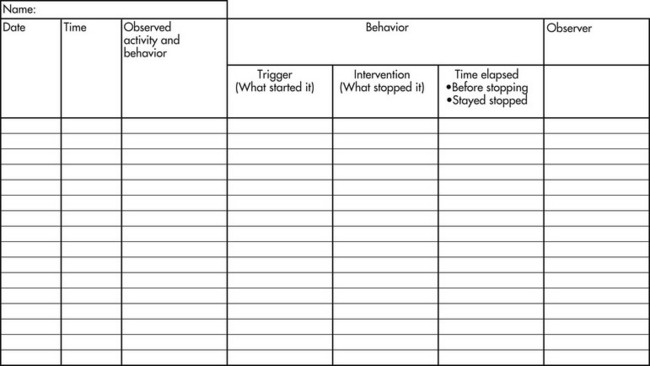
The behavior observation form is used to determine a behavioral pattern involving the time of day and possible antecedents. This form can help COTAs and other health care workers make appropriate changes for reducing or refocusing difficult behaviors (Figure 20-1).
The challenge of identifying the source of the difficult or unwanted behavior and a solution to the problem also requires critical reasoning. The following are some questions that COTAs can ask themselves to help with the critical reasoning process: What is this behavior “saying”? Whose problem is it? What are some environmental factors that might be contributing to the behavior?
The story of Alfonso, an elder in an AD special care unit, illustrates the importance of critical reasoning in addressing difficult or unwanted behaviors. Alfonso tries constantly to go out of the door because he thinks it is time to go to work. Possible reasons for his attempts to leave include the time of day, that he sees visitors leaving with their hats and coats, and lack of involvement in meaningful activities. The staff may not be trained to redirect him when his anxiety and agitation increases, the day room may be too noisy, or he may believe that the intercom voice is calling him to the phone. The COTA might consider the following options: asking him to help with a project (he might forget his need to leave), painting the exit door the same color as the walls on either side so it appears less obvious, involving Alfonso in a meaningful activity (drawing ideas from his life story), and spending some quality time with Alfonso.
Audrey is another person in the same unit. She often becomes combative when performing ADL functions, especially showering. In fact, she strikes the COTA during an assessment of showering. The COTA considers possible causes for this behavior: Did Audrey formerly take baths, and is she unhappy with the change in her routine? Is Audrey a very private person, and is she embarrassed that someone is helping her? Did she react to the COTA’s tone of voice? Is Audrey getting sick and unable to report it? Is she too tired when the shower is scheduled? Is she experiencing chronic pain such as arthritis, which may be upsetting her? Does she feel rushed? Has the showering task been simplified enough so that she can participate and feel in control? The COTA then considers the following behavioral interventions: asking Audrey to help wash down the shower, singing Audrey’s favorite hymn with her while she showers, postponing the shower for another time, and allowing Audrey to bathe with some of her clothes on or wrapping her in a bath blanket during the bathing process.
As illustrated by the preceding examples, handling the behavioral difficulties of elders who have AD can be a trial-and-error process until COTAs identify solutions that work. Each elder will respond differently. Different techniques, based on the person’s abilities, can succeed one time and fail the next. Even when COTAs cannot ascertain the exact reason for the behaviors, they can try the following intervention techniques. Distraction is a helpful technique, especially if the person is agitated. COTAs can be creative with ideas for distraction that involve the person in a meaningful activity, such as listening to music or offering a snack. Rescuing is another distraction technique: When one caregiver is in conflict with the client, a second caregiver responds by “rescuing” that person. This technique is illustrated by the following example. Sally, a nursing assistant, says to Theresa, the resident, “Don’t go out the door.” If Amy, the COTA, approaches Theresa in the same fashion, Theresa might feel outnumbered. Conversely, if Amy says, “Sally, Theresa and I want to be alone; please leave us,” Theresa might feel “rescued” and go with Amy.
Inappropriate timing, attempts to manipulate the elder to fit a schedule, and unrealistic performance expectations can cause negative behavior such as hitting. Consequently, caregivers must be aware of the elder’s mood before approaching with an ADL or social event.
Intervention
Observations, Screening, and Assessment
As with any OT client, the first step in the OT process is of assessment and development of the client’s occupational profile. The profile “provides an understanding of the client’s occupational history and experiences, patterns of daily living, interests, values, and needs. The client’s problems and concerns about performing occupations and daily life activities are identified, and the client’s priorities are determined.”14 Later, the registered occupational therapist (OTR)/COTA team should analyze the elder’s occupational performance to identity his or her assets, problems, or potential problems more specifically. During this phase of the evaluation, “actual performance is often observed in context to identify what supports performance and what hinders performance. Performance skills, performance patterns, context or contexts, activity demands, and client factors are all considered, but only selected aspects may be specifically assessed.”14 This helps the team identify targeted outcomes.
The OTR/COTA team may collaborate in the administration of the following evaluations among others. The Folstein Mini-Mental State is a short and simple quantitative measure of cognitive performance. This measure is a questionnaire in five areas of cognition, including orientation, registration (memory), attention, and calculation, as well as recall and language (following oral and written instructions).30 The Global Deterioration Scale measures clinical characteristics at seven levels based on the progressive stages of AD.31
The Allen Cognitive Performance Tests and the Routine Task Inventory examine cognitive function through the completion of tasks.32 The levels of function help predict behavior and effects on ADL functions. These levels range from the ability to use complex information and perform ADL functions accurately and safely to severe deficits in recognition and use of familiar objects. This assessment includes information on communication, response to tasks, and need for task simplification. It also addresses the role of the therapist during intervention. (See Chapter 7 for a more detailed explanation of these tests.)
The Cognitive Performance Test is a standardized functional assessment instrument designed for the evaluation of Allen cognitive levels.33 Six functional tasks—dressing, shopping, making toast, making phone calls, doing laundry, and traveling—comprise the test. This test also looks at the person’s abilities to process information in relation to functional performance.
The importance of the COTA being an integral part of the overall treatment team with other disciplines cannot be stressed enough.34,35 The continuous development of dementia-specific assessments provides the treatment team with sensitive, appropriate tools that not only bring together information about the elder’s challenges, but also encourage the recognition of the client’s personhood and how to build on current strengths and abilities.36,32 For example, the Person, Environment, Occupation measurement model helps determine how AD affects the function of both the person with disease and his or her family.37
Intervention Planning
OT for people with AD most often involves attention to participation in self-care and leisure occupations, consideration of communication and functional mobility, and careful regard for safety. Areas to address in intervention planning include decreased attention span, the inability to initiate tasks, difficulty with sequencing tasks, impaired judgment, and overall wellness. Intervention planning begins with establishing a cognitive and functional baseline and includes ability-based goals. These goals should identify functional capacity and needs to restore, maintain, or improve skills. The goals should focus on abilities and opportunities for participation in activities that support cognitive, physical, and psychosocial wellness. These goals should include interventions that enable person-centered caregiving and refocus difficult behaviors in a supportive and safe environment.
Intervention planning should include the use of assessment and observation to measure changes in functional status. The process of intervention planning includes providing and suggesting continuous modifications and adaptations of approaches, such as task simplification and cueing. The elder’s life story may be used as the basis for intervention that focuses on past (and present) wisdom and experiences. Intervention planning also involves assessing all aspects of intervention support and factors that lead to negative responses, including environmental components.38 For example, Andrew’s limited attention span prohibited him from eating more than a few mouthfuls of each meal. He was seated in a large dining room with five other people at his table. Music was played on the tape deck, and the staff often talked loudly with each other. When the COTA suggested relocating Andrew to a small dining area where the tables seated two and reducing the environmental stimulation, he was able to focus on his food and complete his meal.
Intervention Implementation
OT interventions consider the effects of dementia on the elder’s cognitive abilities and well-being. Success with interventions entails many crucial components, including the COTA’s flexibility and creativity. Success may need to be redefined, as exemplified by Beverly, a resident of a special care unit. Beverly liked to wear a yellow floral blouse and her favorite orange and black plaid skirt. She was proud of her ability to select and dress independently, although some disapproved of her choices.
Equally important for successful intervention is the COTA’s nonverbal approach. It should reflect acceptance and respect for the elder with AD. To ensure success, intervention should not place elders in situations in which their inabilities may lead to failure. For example, Clara had always been a talented knitter of lovely sweaters. Her ability to do intricate stitches became impaired as her dementia progressed. The COTA set up the stitches on large needles and helped her get started knitting squares using a basic stitch. Clara was able to knit the simple squares for a baby blanket and was delighted in the recognition of her success. This activity could be further adapted by involving Clara in winding yarn as her knitting abilities diminish.
Applying life history and experiences to functional abilities also is meaningful. For example, Sara, a 78-year-old mother of five, responds to normalization activities such as washing dishes, hanging laundry, and sweeping floors. These activities provide tactile stimulation, lower and upper body range of motion, strengthening, trunk stabilization, and fine hand motor skills.
COTAs can use their skills in analyzing activities to identify steps toward task simplification. Harry was able to dress himself independently when each item of clothing was placed on his bed in the appropriate sequence for dressing. Successful intervention also should focus on working with elders to promote active participation and collaboration. Charles had lost interest in feeding himself but accepted the COTA’s suggestion to have the caregiver place a hand over his hand. That way he could continue to feed himself with assistance rather than being fed by others.
When possible, intervention should be provided in appropriate and familiar settings.39 For example, Millie was unable to experience success with simple dressing tasks when she attempted them in the clinic. However, when the COTA arrived at Millie’s bedside early each morning, Millie was able to use visual cues found in her bedroom, including the bureau and closet, to trigger self-dressing skills.
Activities of Daily Living
COTAs can make a significant contribution to the well-being of elders with AD and enhance their quality of life by supporting ADL occupations. Understanding the activity’s demands, breaking down and simplifying tasks, and so on, enables these elders to become involved in performing these familiar skills. This understanding can be facilitated by using one-step commands and visual cueing, including objects or gestures. The use of the Allen’s stage levels can be a helpful measure of the elder’s level of functioning.40
Difficulties with ADL occupations associated with dementia include a decreased attention span, limited ability to follow directions, and increased length of time to complete tasks. Other difficulties include problems with sequencing, perception, and body awareness. Emotional responses of fear, paranoia, and reactions to excessive environmental stimulation that are real or imagined also can influence ADL functioning. Aggressive behavior of elders with cognitive impairments can significantly affect ADL outcomes.22
Modifications in the ways in which people with Alzheimer’s dementia carry out daily activities can help maintain their independence longer and even regain some lost function. Further maintaining engagement in meaningful activities for longer periods of time reduces dementia-related behaviors such as screaming, wandering, and physical aggression. The consistent use of directed verbal prompts and positive reinforcement maximizes ADL functional status, particularly with feeding.41 COTAs working on ADL functions will be most successful when they use creative problem solving. Therapy requires working with elders, not doing to or for them.16 COTAs should do everything possible to make ADL functions meaningful. The use of distraction techniques (for example, singing and holding items such as costume jewelry, scarves, and neckties) should be part of daily care. The COTA’s attitude, approach, and direct involvement are key components in supporting the elder’s quality of life.
COTAs should consider the timing when working on ADL functions. Often, these decisions are based on knowing the elder and responding to nonverbal language that suggests the best and worst times for these activities. Sometimes, COTAs must come back several times because many elders with AD are sensitive to being rushed. For example, Charles appeared agitated when the COTA wanted to work on dressing skills. After several attempts the COTA decided to return later. At that time, Charles was calmer and accepting of the activity.
Assisting with ADL functions can also provide opportunities for COTAs to monitor the elder’s physical well-being and safety. Elders with AD often do not report bruises, rashes, and blisters. Decreased cognitive ability and judgment, combined with an unawareness of perceptual difficulties, may lead to unsafe situations. Elders may eat dirt or plants, walk on wet floors, put their shoes on the wrong feet, forget necessary items such as glasses, misjudge a chair seat and fall, or scald themselves in the shower because they do not know how to turn on the cold water—all of these are examples of potential dangers.
When working with elders on ADL functions, COTAs should always focus on abilities by encouraging active involvement. The techniques of hand-over-hand guidance, chaining, and bridging can be used. Hand-over-hand guidance may help the elder complete the ADL task. With chaining, the caregiver begins a task by putting one hand over the elder’s hand and continuing until the elder can take over and complete the task. For example, Astrid had no idea what a toothbrush was or how to use it. However, when the COTA placed it in her hand and guided it to her mouth to start the brushing action, Astrid was able to complete the task independently. With these techniques the palmar surfaces of the hand or the surface receiving touch during a handshake can be a more “accepting” surface than the back of the hand. COTAs should establish contact with the elder’s palm before moving their hand around to the dorsal surface if needed for assisting the elder during activities.
With bridging, elders who are unable to perform any part of the daily living task can focus their attention by holding the same object the caregiver is using. This technique also can help to decrease anxiety. For example, Allan could not shave. The COTA demonstrated to the caregivers a bridging technique to try with Allan. She placed a turned-on electric razor in his hand so he could feel the vibration while she shaved him with another electric razor. By holding a razor, Allan was better able to focus attention on the task.16
The creativity and flexibility of COTAs can promote the remaining abilities of elders and their willingness to be actively involved in daily life tasks (Table 20-3). Knowledge of the client’s past routines is helpful during ADL functions.
TABLE 20-3 Suggestions for Provision of Activities of Daily Living Support for Elders with Alzheimer’s Disease
| Bathing | Know whether client prefers a bath or shower; use handheld shower head. If privacy is an issue, elder can bathe with some clothing on or with a bath blanket. If needed, elder may wash one part of the body per day until able to accept total bathing. Consider safety by using adaptations such as bath seats, grab bars, and floor mats. Create a warm and homelike bathing environment. Placing colorful beach towels on the walls can help reduce the room’s echo and loud water sounds. The towels also can be used to wrap elders if they become agitated during clothing removal. Consider alternatives such as having a family member present to assist with bathing to help reduce the elder’s anxiety. |
| Shaving | Use a mirror unless elders do not recognize themselves or feel that they are being “watched.” Use a bridging technique with elders incapable of actually shaving. Have them hold an electric razor that they can see, feel, and hear while shaving them with another electric shaver. |
| Oral care | Use a child-sized tooth brush. Pretend to be brushing your own teeth and encourage elders to mirror the activity. Use bridging technique of asking the elder to hold an extra set of dentures while removing the elder’s dentures. Set up a simulated dental chair and announce that the dentist has sent you to assist with dental care. Set up a monitor system so that presence of dentures are checked after each meal in case elders have wrapped them up in a napkin for disposal. |
| Dressing | Suggest clothing one size larger for dressing ease. Keep the clothes appropriate to the elder’s past lifestyle. Use verbal and visual cues to simplify each step, and always thank the elders for helping. If elders become anxious, ask them to show you how the clothing items are put on. If possible, use washable shoes with Velcro closures. Use 100% cotton clothing because it does not retain the odor of urine. Ask the elder to sit when dressing, especially if balance is a concern. |
| Toileting | Be aware of elder’s past toileting routines and habits. Use pictures of toilets with the word “toilet” on the bathroom doors. Determine whether the bathroom mirror prohibits elders from using the toilet because they do not recognize their image and think someone else is there. Be sure the toilet seat color contrasts with the floor. Change the seat or use a washable rug around the toilet base. Use key words to remind the elder about the task. Often, the words they used when toilet training their children work well. Offer the elder something (for example, a magazine) to hold or do while seated on the toilet. Never refer to pads for incontinence as “diapers” (use terms such as panties or shorts). Have different types of incontinence products available. Don’t assume that a full-sized item is needed immediately. For example, a pad placed within a panty can be used if urine is leaked. Use suspenders to keep full-sized incontinence products in place. |
| Eating* | Observe eating for safety problems such as overstuffing the mouth, not chewing before swallowing, and eating nonedibles (napkins, foam cups). If the elder is storing food in the mouth, check for a clear swallow. Obtain a swallowing evaluation if a problem is apparent. Offer the meal in a quiet area to decrease distractions and to improve attention span. If the food needs to be set up, always do that out of the elder’s sight. This prevents reinforcement of the elder’s inability to perform certain simple tasks. Provide color contrast between the food and the plate and the plate and the table. Avoid plastic utensils, which are easily bitten and broken. Obtain, if appropriate, a dietary order for variation in food textures. Simplify the meal by serving one item and one utensil at a time. If elders will not sit to eat, use finger foods or have a small bowl that can be easily carried. Incorporate food into a sandwich. Pureed food can be put into an ice cream cone to assist elders who want to continue self-feeding. If elders are not eating and no medical reasons prohibit it, use sugar or honey on the food to increase palatability. After a swallowing evaluation, if deemed appropriate, provide non-salty chicken or beef broth that can be poured over the food for a more “slurpy” consistency to facilitate an appropriate swallow. If the elder needs to be fed, bridge the task by having the elder hold a spoon or plastic cup. If the elder is disinterested in eating, alternate bites of hot and cold foods and sweet and nonsweet food. When the elder appears to stop eating or has lost all interest in food, ask the family to identify the elder’s “comfort foods” to facilitate reinterest in eating. Foods such as mashed potatoes and gravy, pizza, and macaroni give a sense of well-being. If weight loss is a problem, double the elder’s breakfast. Try to avoid commercial food supplements, if possible, by allowing time for the meal to be eaten and providing protein-enriched foods such as milkshakes. Sit with the elders. Have something to eat or drink to reduce elders’ anxiety that you don’t have anything to eat and therefore must have some of theirs. If elders refuse to eat because of not having money, provide a letter stating that their dues to your association (the name of your facility or place of practice) have been paid in full and meals are included in their membership. |
* See discussion of dysphagia in Chapter 18 for more specific information about safe eating.
Using Adapted Equipment
Elders with AD often refuse or misuse adapted equipment. Improper use may affect the elder’s safety, especially if the item does not look familiar. For example, a plate guard may appear so strange that the elder with AD might spend the mealtime trying to remove it from the plate. Sometimes, large, built-up handles on eating utensils may feel so different that clients do not use them. Reachers and other metal devices used for ADL functions can be used as weapons. Flatware with large handles and scoop dishes can be helpful because they closely resemble their ordinary counterparts. Adapting the environment by using color contrast between objects, pictures, words, labels, and arrows is often the best way to cue for successful involvement in ADL functions.
Using Activities to Promote Well-Being
Activities can be adapted for individuals and groups. The objectives of therapeutic activities are enhancing meaning, encouraging active participation, and ensuring success. All of life’s activities can be used as intervention modalities. Suggestions for cognitive activities are adapted trivia games, word puzzles, rhyming games, singing of familiar songs, and reminiscence. Others include spelling games, simple crafts, clothes-sorting, cards, and Life Story “book clubs.” Suggestions for physical activities include parachute exercises; dancing; and tossing, hitting, and kicking balls and balloons. An exercise program may include the use of handheld wands, light weights, scarves, and fabrics. Psychosocial activities include parties, service projects, grooming tasks, celebrations of special days, field trips, and pet care. Worship and related spiritual activities may offer elders with dementia a sense of the familiar, well-being, and security. Recommendations for normalizing activities are folding and hanging up laundry, dusting and sweeping, sorting silverware, and shining shoes.16
Environment-based interventions appear to have some positive effect on reducing agitation of people with dementia. Simulations of a natural environment (e.g., use of recorded sounds of babbling brooks, birds, and other small animals; large pictures of the outdoors) during bathing reduce agitation and can improve the relationship between caregivers and the individual.42 There is some evidence that ambient, nonvocal music has some calming effect on people with AD.43 The OTR/COTA team should consider this intervention as part of a multisensory stimulation program or as part of the background feature of a dining room, for example. However, music selection may need to be matched to the person’s taste. Because of the low cost, these types of intervention could be implemented in institutional, community, or home settings.
Communication with and Teaching Caregivers
OT intervention with elders who have AD focuses on maintaining functional abilities and preventing secondary complications. These objectives can be achieved by tailoring communication and education to caregivers. About 9.8 million family members, friends, and neighbors provide 8.4 billion hours of unpaid care for persons with AD each year. This care is estimated to make an annual contribution to the nation valued at 89 billion dollars.44 About 60% of unpaid caregivers are wives, daughters, daughters-in-law, granddaughters, and other female relatives, friends, and neighbors. At any one time, 32% of family and other unpaid caregivers of people with AD have been providing help for 5 years or longer, and 39% have been providing care for 1 to 4 years.45
Caregivers benefit from a variety of techniques, including written instruction and demonstration. The instructional method of requiring a “return demonstration” allows COTAs to observe first-hand that caregivers follow through with activities. Afterward, the COTA can make necessary suggestions or corrections. As the dementia progresses, caregivers provide more and more care, until they can no longer manage their caregiving responsibilities on their own. Caring for a person with AD is often very difficult, and caregivers have high rates of anxiety, stress, and burnout.46 Their life expectancy is reduced, and at least a third are depressed.47,48,49 Encouraging caregivers to strengthen their social support system for the long term should be a basic component of OT intervention.50 A basic occupational therapy plan for people with AD should include providing caregivers with information about progression of disease, referral to community resources, practical ideas for caregiving, and understanding of how the caregiving role is different from other family roles.51
The COTA/OTR team can formulate a maintenance program.52 Contributing to a maintenance program may require COTAs to sensitize caregivers to the nature and progression of AD. An understanding of task breakdown and simplification, activity modification, behavioral interventions, supportive communications, and the need for flexibility is essential in maintenance programs.
Terminal Stage Issues
Severe dementia, or terminal stage, is exhibited when the elder is oriented only to person and depends entirely on others for self-care. Defining the exact time of terminal, or end-stage, AD is difficult because of changes and variations in the disease process.53 For example, Vernon appeared to have entered the terminal stage because he had been refusing food for 2 weeks. When offered familiar “comfort” foods from his past and sweet foods, he suddenly started to eat again.
Many elders at the terminal stage of AD are kept in bed or positioned in wheelchairs or recliners. Unfortunately, those kept in bed often lie in the fetal position. These elders are dependent on others for basic life functions and display an almost total loss of communication skills or the ability to express pain.54 To help make them more comfortable, COTAs may provide positioning suggestions and passive range-of-motion exercises. A caring touch, hand-over-hand movement, and various sensory activities may produce a response. Some people become ill with symptoms leading to pneumonia or other systemic problems shortly before death. This is an important time for supporting family members and staff caregivers.50
Reimbursement for Services
A functional outcome must be meaningful, utilitarian, and sustainable over time. Currently, the maintenance of remaining abilities of elders with dementia, or any chronic illness, is not usually covered by third-party payers such as Medicare unless there is a need for “skilled” therapeutic coverage. Elders on Medicare Part A in Skilled Nursing Facilities under the Prospective Payment System (PPS) may qualify for therapy on the basis of their determined level of resources needed with the Resource Utilization Groups (see Chapter 6 for more details on the PPS system).55 For elders on Medicare Part B, the COTA/OTR team may address cognitive and physical impairment related to functional performance. Medicare will reimburse for cognitive disabilities that require “complex and sophisticated knowledge to identify current and potential capabilities.”55 All levels of assistance from total to standby address both physical and cognitive components. Table 20-4 outlines the cognitive components only. Behavioral issues with cognitive impairment can be focused on if they require skilled OT services.55
TABLE 20-4 Medicare Cognitive Levels of Assistance
| Assistance level | Cognitive assistance |
|---|---|
| Total assistance | Total assistance is the need for 100% assistance by one or more persons to perform all cognitive assistance to elicit a functional response to an external stimulation. A cognitively impaired patient requires total assistance when documentation shows external stimuli are required to elicit automatic actions such as swallowing or responding to auditory stimuli. Skills of an occupational therapist are needed to identify and apply strategies for eliciting appropriate, consistent automatic responses to external stimuli. |
| Maximal assistance | Maximum assistance is the need for 75% cognitive assistance to perform gross motor actions in response to direction. A cognitively impaired patient, at this level, may need proprioceptive stimulation and/or one-to-one demonstration by the occupational therapist because of the patient’s lack of cognitive awareness of other people or objects. |
| Minimum assistance | Moderate assistance is the need for 50% assistance by one person or constant cognitive assistance to sustain/complete simple, repetitive activities safely. The records submitted should state how a cognitively impaired patient requires intermittent one-to-one demonstration or intermittent cueing (physical or verbal) throughout the activity. Moderate assistance is needed when the occupational therapist/caregiver needs to be in the immediate environment to progress the patient through a sequence to complete an activity. This level of assistance is required to halt continued repetition of a task and to prevent unsafe, erratic, or unpredictable actions that interfere with appropriate sequencing. |
| Standby assistance | Standby assistance is the need for supervision by one person for the patient to perform new procedures adapted by the therapist for safe and effective performance. A patient requires such assistance when errors are demonstrated or the need for safety precautions is not always anticipated by the patient. |
| Independent status | Independent status means that no physical or cognitive assistance is required to perform functional activities. Patients at this level are able to implement the selected courses of action, demonstrate lack of errors, and anticipate safety hazards in familiar and new situations. |
The Physical Levels of Assistance are not included in this chart.
From Centers for Medicare and Medicaid Services (CMS). (2008). Medicare program integrity manual [WWW page]. Retrieved November 22, 2009, from www.cms.hhs.gov/manuals/downloads/pim83c06.pdf.
The COTA/OTR team may suggest a short-range program on the basis of continuous functional support, especially if a change in functional status has occurred. Often, elders with AD who receive Medicare reimbursement for care have an initial evaluation from OT. A maintenance program is then developed by the therapists and carried out by facility staff. Medicare will reimburse if skilled OT is needed to evaluate a “complex” patient to increase function or safety, and then to train staff to carry out the program.55 The OTR evaluates the elder and establishes the plan of care. The COTA may train caregivers to carry out the plan. OT practitioners may manage the elder for reevaluation when significant changes occur in functional status. As discussed in Chapter 6, memorandums from Medicare prevent automatic denials just because a person has the diagnosis of AD and mention benefits for therapeutic intervention with this diagnosis.55
Conclusion
COTAs can make a unique contribution to elders with AD. COTAs can treat these elders from the initial stages of forgetfulness and poor judgment by offering strategies for continuing independence. COTAs may also provide advice about late-stage care by focusing on positioning, feeding, and responses to sensory activities. Understanding the changes that occur as dementia progresses challenges elders, caregivers, and families to pursue creative and supportive solutions for daily care. The holistic programs and care provided by COTAs support the abilities and well-being of elders. When offered occupation-focused care, elders with dementia can have meaningful lives.
Case Study
Mildred is 78 years of age and has mid-stage AD. Mildred was formerly a teacher and experienced a happy family life with her husband of 58 years and their two sons. She has been widowed for the last 5 years. Mildred was originally brought to the special care unit where she currently resides when she was found wandering outside during the cold winter months.
At the special care unit the COTA helped assess Mildred’s functional status. The COTA identified the following abilities: Mildred follows one-step directions, responds to multisensory cueing, maintains strong socialization skills, and refers to her former profession by often mentioning her past role as a teacher. She also mentions her past interest in the activities of cooking and sewing.
Mildred functions at Allen’s Cognitive Level 3. The COTA observed that she was forgetful, with limited instructional carryover. Mildred experiences problems with sequencing ADL functions. She often becomes anxious, which leads to combativeness during ADL functions, especially bathing. Other assessment findings included the inability to toilet independently and use multiple utensils with meals. Communication challenges included receptive and expressive understanding of words, especially nouns.
The COTA instructed all staff members who work with Mildred to consider her strengths, as well as her attention span deficits and feelings of depression, as she attempts to cope with her disease.
Case Study Questions
1. Considering Mildred’s case, how can visual triggers and written phrases be used to help Mildred be as independent as possible?
2. What anxiety-reducing approaches can be explored? What specific interventions can be used during bathing?
3. How can the COTA develop a system for sequencing Mildred’s clothing?
4. What environmental issues might need to be addressed, especially in the bath/shower room?
5. What suggestions can be incorporated as mealtime interventions for promoting successful dining?
6. If Mildred can find the toilet, what strategies can enable her to remain continent?
7. How can the COTA use ADL functions as therapeutic modalities for reducing feelings of depression and helplessness?
8. How can the COTA make Mildred’s care “person-centered” and “activity-focused”?
1. In reference to the entire chapter, what are the basic symptoms of AD, and how do they affect elders with the disease and their caregivers?
2. Identify six ways to facilitate communication with elders who have dementia.
3. How can a functional assessment be used to develop intervention goals?
4. List three guidelines for the provision of ADL support to elders functioning at the mid-stage level of AD.
5. Outline six specific mealtime adaptations for elders with a short attention span.
6. List steps for getting dressed using task simplification.
7. What are possible antecedents and appropriate interventions for agitation?
8. Why do people with dementia wander, and how can the risk for elopement be decreased?
9. Give specific examples of ways that activity-focused care supports COTAs’ interventions.
10. Describe strategies to adapt the activity of folding laundry to address the elder’s cognitive, physical, psychosocial, and normalization needs.
1 Alzheimer’s Association. Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2009;5(3):234-270.
2 Jolley D. The epidemiology of dementia. Practice Nursing. 2009;20(Suppl. 6):S4-S6.
3 Shackle S. Alzheimer’s: The facts. New Statesman. 2009;138(4931):29-37.
4 Alzheimer’s Disease International. World Alzheimer’s report 2009: Executive summary. London, England: Author; 2009.
5 Neugroschl J., Sano M. An update on treatment and prevention strategies for Alzheimer’s disease. Current Neurology and Neuroscience Reports. 2009;9(5):368-376.
6 Leifer B. Alzheimer’s disease: Seeing the signs early. Journal of the American Academy of Nurse Practitioners. 2009;21(11):588-595.
7 Alzheimer’s Association. What is Alzheimer’s? Retrieved November 22, 2009, from http://www.alz.org/alzheimers_disease_what_is_alzheimers.asp, 2009.
8 Grossberg G., Kamat S. Alzheimer’s: The Latest Assessment and Treatment Strategies. Sudbury, MA: Jones & Bartlett; 2007.
9 Caroli A., Frisoni G. Quantitative evaluation of Alzheimer’s disease. Expert Review of Medical Devices. 2009;6(5):569-588.
10 Davatzikos C., Xu F., An Y., Fan Y., Resnick S. Longitudinal progression of Alzheimer’s-like patterns of atrophy in normal older adults: the SPARE-AD index. Brain: A Journal of Neurology. 2009;132(8):2026-2035.
11 Kurz A., Perneczky R. Neurobiology of cognitive disorders. Current Opinion in Psychiatry. 2009;22(6):546-551.
12 Chiappelli F., Navarro A., Moradi D., Manfrini E., Prolo P. Evidence-based research in complementary and alternative medicine III: Treatment of patients with Alzheimer’s disease. Evidence-Based Complementary and Alternative Medicine. 2006;3(4):411-424.
13 Smith D. Treatment of Alzheimer’s disease in the long-term-care setting. American Journal of Health-System Pharmacy. 2009;66(10):899-907.
14 American Occupational Therapy Association. Occupational therapy practice framework: Domain and process, 2nd ed. American Journal of Occupational Therapy. 2008;62:625-683.
15 Edvardsson D., Winblad B., Sandman P. Person-centered care of people with severe Alzheimer’s disease: Current status and ways forward. Lancet Neurology. 2008;7(4):362-367.
16 Hellen C.R. Alzheimer’s Disease: Activity-Focused Care. St. Louis, MO: Butterworth-Heinemann; 1998.
17 Kitwood T. Toward a theory of dementia care: Ethics and interaction. Journal of Clinical Ethics. 1998;9(1):23-34.
18 Fazio L. Developing Occupation-Centered Programs for the Community, 2nd ed. New York: Prentice Hall; 2007.
19 Murray L., Boyd S. Protecting personhood and achieving quality of life for older adults with dementia in the U.S. health care system. Journal of Aging and Health. 2008;21(2):350-373.
20 Schmidt K., Lingler J., Schulz R. Verbal communication among Alzheimer’s disease patients, their caregivers, and primary care physicians during primary care office visits. Patient Education and Counseling. 2009;77(2):197-201.
21 Spector A., Thorgrtimsen L., Woods B., Royan L., Davies S., Butterworth M., et al. Efficacy of an evidence-based cognitive stimulation therapy program for people with dementia. British Journal of Psychiatry. 2003;183:248-254.
22 Ballard C., Corbett A., Chitramohan R., Aarsland D. Management of agitation and aggression associated with Alzheimer’s disease: Controversies and possible solutions. Current Opinion in Psychiatry. 2009;22(6):532-540.
23 Hopper T. Indirect interventions to facilitate communication in Alzheimer’s disease. Seminars in Speech and Language. 2001;22(4):305-315.
24 Small J., Gutman G., Makela S., Hillhouse B. Effectiveness of communication strategies used by caregivers of persons with Alzheimer’s disease during activities of daily living. Journal of Speech, Language, and Hearing Research. 2003;46(2):353-367.
25 Bonder B., Dal Bello-Hass V. Functional Performance in Older Adults, 3rd ed. Philadelphia: FA Davis; 2009.
26 Farran C., Gilley D., McCann J., Bienias J., Lindeman D., Evans D. Efficacy of behavioral interventions for dementia caregivers. Western Journal of Nursing Research. 2007;29(8):944-960.
27 Gitlin L., Corcoran M. Occupational Therapy and Dementia Care: The Home Environmental Skills-Building Program for Individuals and Families. Bethesda, MD: AOTA Press; 2005.
28 Price, J., Hermans, D., Grimley-Evans, J., 2001. Subjective barriers to prevent wandering of cognitively impaired people. Cochrane Database of Systematic Reviews, Issue 1. Art. No.: CD001932.
29 Verkaik J., vanWeert J.C.M., Francke A. The effects of psychosocial methods on depressed, aggressive, and apathetic behaviors of people with dementia: A systematic review. International Journal of Geriatric Psychiatry. 2005;20:301-314.
30 Barker W., Luis C., Harwood D., Loewenstein D., Bravo M., Ownby R., et al. The effect of a memory screening program on the early diagnosis of Alzheimer’s disease. Alzheimer’s Disease and Associated Disorders. 2005;19(1):1-7.
31 de Jonghe J., Wetzels R., Mulders A., Zuidema S., Koopmans R. Validity of the severe impairment battery short version. Journal of Neurology, Neurosurgery, and Psychiatry. 2009;80(9):954-959.
32 Dementia Care Specialists. Facilitating functional and quality-of-life potential: Strength-based assessment and treatment for all stages of dementia. Topics in Geriatric Rehabilitation. 2006;22(3):213-227.
33 Burns T., Mortimer J. The cognitive performance test: A new approach to functional assessment in AD. Journal of Geriatric and Psychiatric Neurology. 1993;7(1):46.
34 Austrom M., Hartwell C., Moore P., Perkins A., Damush T., Unverzagt F., et al. An integrated model of comprehensive care for people with Alzheimer’s disease and their caregivers in a primary care setting. Dementia. 2006;5(3):339-352.
35 Evans L., Cotter V. Avoiding restraints in patients with dementia: Understanding, prevention, and management are the keys. American Journal of Nursing. 2008;108(3):40-49.
36 Brubacher D., Zehnder A.E., Monsch A.U., et al. Assessment of everyday behavior in Alzheimer’s disease patients: Its significance for diagnostics and prediction of disease progression. American Journal of Alzheimer’s Disease and Other Dementias. 2005;20:151-158.
37 Baum C., Perlmutter M., Edwards D. Measuring function in Alzheimer’s disease. Alzheimer’s Care Quarterly. 2000;1(3):44-61.
38 Clare, L., Woods, B., 2003. Cognitive rehabilitation and cognitive training for early-stage Alzheimer’s disease and vascular dementia. Cochrane Database of Systematic Reviews, Issue 4. Art.No.: CD003260. DOI: 10.1002/14651858.CD003260.
39 Dooley N., Hinojosa J. Improving quality of life for persons with Alzheimer’s disease and their family caregivers: Brief occupational therapy intervention. American Journal of Occupational Therapy. 2004;58:561-569.
40 Allen C.K. Occupational Therapy for Psychiatric Diseases: Measurement and Management of Cognitive Disabilities. Boston: Little Brown; 1985.
41 Watson R., Green S. Feeding and dementia: A systematic literature review. Journal of Advanced Nursing. 2006;54:86-93.
42 Whall A.L., Black M.E., Groh C.J., et al. The effect of natural environments upon agitation and aggression in late stage dementia patients. American Journal of Alzheimer’s Diseases. 1997;12:216-220.
43 Sherratt K., Thornton A., Hatton C. Music interventions for people with dementia: A review of the literature. Aging & Mental Health. 2004;8(1):3-12.
44 Alzheimer’s Association. 2008 Alzheimer’s disease facts and figures. Chicago: Alzheimer’s Association; 2008.
45 Alzheimer’s Association and National Alliance for Caregiving. Families care: Alzheimer’s caregiving in the United States, 2004. Retrieved November 22, 2009, from http://www.alz.org, 2004.
46 Yaffe K., Fox P., Newcomer R., Sands L., Lindquist K., Dane K., et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAMA. 2002;287:2090-2097.
47 Adams K. Specific effects of caring for a spouse with dementia: Differences in depressive symptoms between caregiver and non-caregiver spouses. International Psychogeriatrics. 2008;20:508-520.
48 Arlt S., Hornung J., Eichenlaub M., Jahn H., Bullinger M., Petersen C. The patient with dementia, the caregiver, and the doctor: Cognition, depression, and quality of life from three perspectives. International Journal of Geriatric Psychiatry. 2008;23:604-610.
49 Kim Y., Schulz R. Family caregivers’ strains: Comparative analysis of cancer caregiving with dementia, diabetes, and frail elderly caregiving. Journal of Aging and Health. 2008;20:483-503.
50 Mittelman M.S., Roth D.L., Clay O.J., Haley W.E. Preserving health of Alzheimer’s caregivers: Impact of a spouse caregiver intervention. American Journal of Geriatric Psychiatry. 2007;15:780-789.
51 Curry L.C., Walker C., Hogstel M.O. Educational needs of employed family caregivers of older adults: Evaluation of a workplace project. Geriatric Nursing. 2006;27(3):166-173.
52 American Occupational Therapy Association. Occupational therapy roles. American Journal of Occupational Therapy. 1993;47(12):1087.
53 Goldberg T., Botero A. Causes of death in elderly nursing home residents. Journal of the American Medical Directors Association. 2008;9(8):565-567.
54 Mitchell S., Teno J., Kiely D., et al. The clinical course of advanced dementia. New England Journal of Medicine. 2009;361(16):1529-1538.
55 Centers for Medicare and Medicaid Services. Skilled nursing facility prospective payment system refinements and consolidated billing guide. Retrieved November 22, 2009, from http://www.cms.hhs.gov/Manuals/, 2008.