chapter 22 Working with Elders Who Have Orthopedic Conditions
1. Identify the causes of fractures in the elder population.
2. Identify terminology related to fractures and their management.
3. Describe the precautions required after a hip pinning and implications of such a procedure relative to occupational performance.
4. Describe the precautions required after a total hip replacement and the implications of such a procedure relative to occupational performance.
5. Identify adaptive equipment and modified methods of performance that benefit elders with hip fractures.
6. Identify the signs and symptoms of osteoarthritis, rheumatoid arthritis, and gout.
7. Describe the effects of osteoarthritis, rheumatoid arthritis, and gout on occupational performance.
8. Explain the principles of joint protection, work simplification, and energy conservation.
orthopedic, fracture, osteoarthritis, compound fracture, transverse fracture, spiral fracture, comminuted fracture, closed reduction, open reduction, internal fixation, external fixation, delayed union, nonunion, malunion, HemoVac, total hip replacement, arthroplasty, antiembolus hosiery, rheumatoid arthritis, wrist subluxation, ulnar drift, swan-neck deformity, boutonnière deformity, Nalebuff type I deformity, joint protection, work simplification, energy conservation
The two weeks I spent in rehab were tough, but I had to learn how to walk all over again, just like a baby! Not only did the physical therapist teach me how to walk, the occupational therapist taught me how to dress, and how to do things around the house. They presented me with all sorts of new gadgets that would help me in my daily living.
Orthopedic problems are prevalent among elders. For example, an estimated 850,000 fractures occur annually in persons age 65 years or older.1 One of every two women and one in eight men older than age 50 years will experience an osteoporosis-related fracture.2 Orthopedic problems may result in elders being hospitalized for a surgical procedure, rehabilitation, and possibly being placed temporarily or permanently in a long-term care facility. Elders who sustain a hip fracture as a result of a fall have a 34% mortality rate within 1 year of the fracture.3 The most common complications of elders who undergo orthopedic surgery include stroke, cardiac failure, and severe infection. There is a reported 10.1% overall rate of mortality after orthopedic surgery for this population.4
The role of the certified occupational therapy assistant (COTA) and registered occupational therapist (OTR) team is to help maximize the occupational performance of elders who have orthopedic problems. Elders who would otherwise need to enter an extended care facility are often able to go home as a result of occupational therapy (OT) intervention. COTAs must be familiar with orthopedic conditions and their effects on occupational performance to ensure that appropriate evaluation and intervention are carried out. This chapter addresses orthopedic problems and conditions that contribute to these problems.
Fractures
Causes of Fractures
Causes of fractures include falls, trauma from automobile accidents, osteoarthritis, and metastatic carcinoma.5 Other factors such as a current or previous smoking habit,6 alcohol abuse,7 diabetes,8 and decreased level of physical activity also correlate with the incidence of fractures.9
The majority of fractures in elders result from falls.10 Factors associated with falling include poor vision, orthostatic hypotension, poor balance, diminished mobility, side effects of medication, muscle weakness, neurological diseases, reduced alertness, urge incontinence, a cluttered home environment, and dementia.11 (An in-depth examination of the causes of falls in elders is provided in Chapter 14.)
The number of elder drivers is increasing. For example, in 1995, about 9% of drivers in the United States were people age 70 years and older, and their number increased to 12% by 2010.12 It is estimated that by 2020, 20% of all people who drive will be older than age 65 years.13 Elders have greater rates of fatal crashes than younger drivers, and they do not deal well with complex traffic situations.14 Trauma resulting from auto accidents accounts for a portion of the fractures seen in the elder population.
Elders are more likely to sustain fractures after a fall because of osteoporosis, osteomalacia, and the diminished ability to repair microfractures.15 Stress fractures also can occur in elders who, for example, suddenly increase their levels of activity by jogging, walking farther than usual, or walking on a different terrain.16
Fractures may also be caused by cancer that has metastasized to bone. Although any cancer may metastasize to bone, metastases from carcinomas, particularly those that arise in the breast, lung, prostate, kidney, and thyroid, are most common. Metastatic lesions weaken the strength of bones and may lead to fractures.17
Types of Fractures
A fracture is a break in a bone. Although radiographs are used to diagnose the fracture, it does not reveal damage to soft tissues or cartilage. Fracture sites can disrupt the intraarticular, epiphyseal, metaphyseal, or diaphyseal portions of the bone. If a fracture occurs and dislocates a joint, it is a fracture-dislocation.18
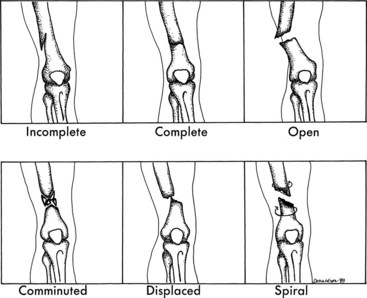
Various terms are used to categorize fractures. A fracture is considered to be compound or open if the bone protrudes through the soft tissue and skin. If the soft tissue and skin are undamaged, the fracture is considered to be closed or simple. Different physical forces can result in certain types of fractures. A transverse fracture occurs as a result of a direct force, whereas a spiral fracture results from a circular or twisting force. A fracture that results in more than two bone fragments is a comminuted fracture. Figure 22-1 shows these various types of fractures.
Medical Intervention for Fractures
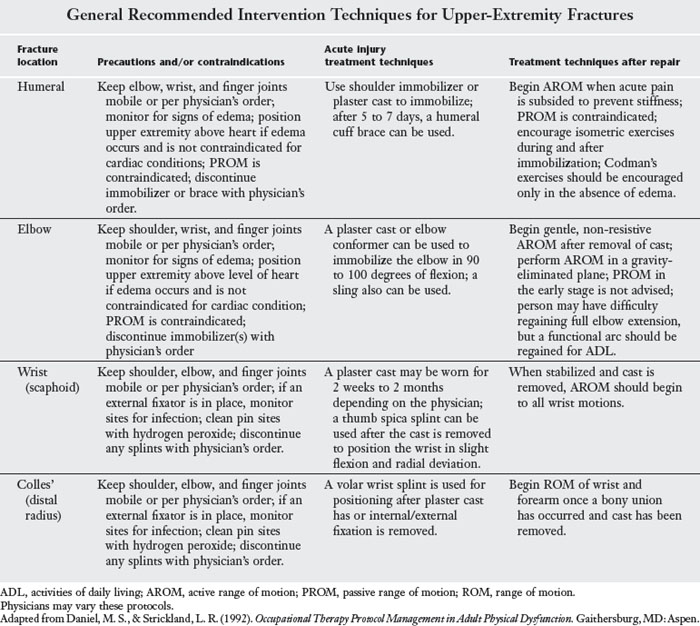
The goals of medical management of a fracture are to reduce pain and align the fracture for proper healing.18 The fracture can be aligned with or without surgery. The process of manually realigning (sometimes using traction devices) and then casting a fracture is termed closed reduction. The open reduction is a surgical procedure that is used to internally fixate the fracture site. Internal fixation is performed with the use of orthopedic nails, screws, pins, rods, or plates. When external fixation is used to align or reduce a fracture, the fixator device is attached with pins or wire, which is inserted through the soft tissues and into the bone (Figure 22-2). This device usually involves the use of screws and rods that are removed after the fracture has healed. The skin around placement sites of the rods or screws must be kept clean to prevent infection (Table 22-1).

FIGURE 22-2 External fixator in place to maintain reduction.
(From Hunter, J., Mackin, E., & Callahan, A. (Eds.). (1995). Rehabilitation of the Hand: Surgery and Therapy, 4th ed. St. Louis, MO: Mosby.)
TABLE 22-1 General Recommended Pin Site Care
| Frequency | 1-2 times each day |
| Massage | Massage site area gently to prevent abnormal adhesions/scars |
| Crusts | Remove from site |
| Cleaning solution | Peroxide or saline |
| Dressing | Dry dressing, especially if oozing |
Adapted from Sims, M., & Whiting, J. (2000). Pin-site care. Nursing Times, 96(48), 46.
COTAs also should be familiar with terminology relating to the healing of fractures. Three terms used to describe fractures that do not heal well are delayed union, nonunion, and malunion.18 Delayed union describes a fracture that heals at an abnormally slow rate. Nonunion describes a fracture that has not healed within 4 to 6 months. Malunion describes a fracture in which the bone heals in a normal length of time but with an unsatisfactory alignment.
Complications After Fractures
Several complications can occur after a fracture.18 Edema can lead to joint stiffness, and joint contractures often are caused by adhesions or prolonged immobilization. After a fracture, posttraumatic arthritis can occur in joints associated with or near the fracture site. Reflex sympathetic dystrophy is a syndrome that often occurs after minor injuries. The condition is believed to be related to the sympathetic nervous system and presents with severe pain, edema, stiffness, muscle atrophy, muscle spasms, contractions, and loss of bone mineralization. Myositis ossificans is the formation of heterotopic ossification near a traumatized area. The most common joints where heterotopic ossification forms are the arms, thighs, and hips.
Factors Influencing Rehabilitation
Several factors affect the outcome of rehabilitation efforts in elders who sustain fractures. Age is a predominant factor in rehabilitation.19 Elders may need more time than younger persons to achieve their greatest levels of independence. For example, in elders, a comminuted fracture of the proximal humerus should be immobilized for the shortest period possible to reduce the chances of development of adhesive capsulitis or frozen shoulder. With a younger person, the threat of such a complication may not always be a concern.
The general condition of elders also affects the course of rehabilitation. For example, elders who are in shock or are unconscious require different intervention than those who are alert and oriented. In addition, past and current medical conditions may affect the rehabilitation of elders who have fractures. Elders with congestive heart failure or chronic obstructive lung disease may be limited in their abilities to participate in endurance and strengthening activities. Furthermore, a large percentage of elders with fractures also have associated medical problems such as arthritis, hypertension, hearing impairments, heart disease, cataracts, orthopedic impairments, sinusitis, and diabetes.20
The presence of dementia often affects rehabilitation outcomes for elders with fractures. For example, teaching the integration of hip precautions or joint protection methods while engaging in self-care tasks to an elder with short-term memory deficits is difficult. (A detailed discussion of intervention considerations for elders who have dementia is presented in Chapter 20.)
Although hip fractures are the most common type of fracture sustained by elders, fractures of other bones also occur. COTAs should know the common fractures and general recommended intervention techniques (Table 22-2).
Hip fractures
Approximately 300,000 hip fractures occur annually in people older than age 65 years, and hip fractures are more common in women than in men.21 Fractures of the hip are classified by the type and direction of the fracture line.
Hip fractures usually require an open reduction internal fixation, or pinning procedure. The open reduction internal fixation of the involved hip usually must be protected from excessive force through weight-bearing restrictions (Table 22-3). The open reduction internal fixation site is sutured shut, and a HemoVac may be used for about 2 days.22 A HemoVac, which is connected to a suction machine, is a device that draws and collects drainage from the site. The HemoVac unit should not be disconnected for any activity and is usually removed by a registered nurse or a physician.
TABLE 22-3 Weight-Bearing Terminology
| Term | Definition |
|---|---|
| No weight bearing (NWB) | No body weight is borne on the involved side. |
| Toe-touch weight bearing (TTWB) | No weight is borne on the heel; weight is borne on the toes only. |
| Partial weight bearing (PWB) | A partial amount of the body weight can be borne on the involved side; usually a percentage of body weight (for example, 50% PWB) or pounds (PWB with 50 lb) is stated. |
| Weight bearingat tolerance (WBAT) | Weight bearing is allowed to the extent that it does not cause the elder too much pain; the elder tolerates the weight bearing. |
| Full weight bearing (FWB) | Full body weight is borne on the involved side. |
The amount of time required for a hip fracture to heal depends on the elder, the fracture site, the fracture type, and the severity of the injury. Most incisions for hip surgeries are 12 to 18 inches in length; however, some new surgical approaches that involve less cutting of muscle, tendons, and ligaments are being tested with the anticipation that the hospital length of stay will dramatically decrease.23
Many health care providers in hospitals follow a protocol or clinical pathway that outlines the timeframe for each professional’s rehabilitation tasks.24 Out-of-bed therapy activities for persons with hip pinnings are usually initiated 2 to 4 days after surgery.19 Most function returns within 6 weeks to 6 months after the fracture occurs; most persons experience little improvement in function from 6 months to 1 year after sustaining a fracture.25
Weight-bearing restrictions for hip pinnings
Depending on the type and severity of the fracture, the physician may restrict the amount of weight bearing allowed on the involved hip while the person is walking. Most weight-bearing restrictions are observed for 6 to 8 weeks, during which time the person may use crutches or a walker to ambulate.19 COTAs must be aware of any weight-bearing precautions before initiating therapy and should know the terminology related to weight-bearing restrictions (see Table 22-3).
Joint Replacements
Total Hip Replacements
Total hip replacements (THRs), or total hip arthroplasties (THAs), are often elective surgeries indicated for reducing pain and restoring motion for elders who have severe osteoarthritis, rheumatoid arthritis, or ankylosing spondylosis. Emergency THAs frequently follow traumatic injuries to the hip, such as after a motor vehicle accident or fall. A hip replacement, or arthroplasty, may be full or partial. During a full hip arthroplasty, the hip’s ball and socket are replaced with metal or metal and plastic prosthetic implants.26 During a partial joint replacement, which is commonly used for fractures of the femoral neck and head, the femoral neck and head are replaced with a prosthesis. Hip prostheses last approximately 10 to 15 years or longer in 90% of elders.27 When radiographs show evidence of loosening of the cement and the client is experiencing pain, a hip revision arthroplasty may be performed.28
The two basic surgical approaches for THRs are the anterolateral approach and the posterolateral approach.29 When an anterolateral approach of surgery is used, elders must avoid adduction, external rotation, and extension of the operated hip. If a posterolateral surgical approach is used, elders should avoid flexion beyond 60 to 90 degrees, adduction, and internal rotation of the operated hip.30 COTAs must be aware of which type of surgical approach was used to properly carry out OT intervention (Figure 22-3). COTAs also should note the position precautions for each surgical approach.

FIGURE 22-3 While the elder is supine, the elder’s legs should be abducted with a wedge to prevent hip rotation and adduction.
The movement precautions are usually observed for 6 to 12 weeks as indicated in a physician’s order (Table 22-4).30 Cemented THRs usually have no weight-bearing restrictions. When cement is not used, bony ingrowth is used to secure the prosthesis to the elder’s bone. Often 6 to 12 weeks of weight-bearing restrictions are required when this type of prosthesis is used.29
TABLE 22-4 Motion Precautions for Clients Who Have Had a Total Hip Replacement
| Approach | Position precautions |
|---|---|
| Anterolateral | |
| Posterolateral |
After THA surgery, physicians often instruct clients to wear antiembolus hosiery. These thigh-high hose are worn 24 hours a day and removed during bathing only. Clients are instructed to wear this hosiery because it assists with blood circulation, prevents edema, and reduces the risk for deep vein thromboses. If an elder has not been instructed to wear these hose and complains of pain or swelling in the affected leg, the physician should be consulted immediately because it could be a sign of the presence of a thrombus. COTAs should be skilled in donning and doffing antiembolus hosiery because they may need to assist elders before bathing. If the hose are to be worn for a length of time, caregiver training should occur because it is often difficult for elders to perform this task independently.
Researchers show that there are several milestones during rehabilitation, including adherence to hip precautions; ambulating 100 feet with a mobility aid; independence with home exercise program; and requiring supervision only with toileting, transfers, and activities of daily living (ADL).27
Three areas reported in research studies that are important concerns for clients with THA are sexual activity, driving, and work return.31 In a study of 86 clients with THA, 50% of preoperative clients reported experiencing difficulties with sexual activities because of hip problems, and 90% of these clients reported a desire for more information about sexual functioning after THA. The majority of clients (55%) resumed sexual activity within 2 months of the THA with physician approval and following positioning precautions. Most people report that the supine position during intercourse is the most comfortable.31 (A detailed discussion of addressing sexuality with elders is presented in Chapter 12.)
After surgery, driving reactions normalize between 3 and 8 weeks if elders resume good leg control. Return to work activities is dependent on the amount of stress and torque on joints. Typically, elders must take off from work for 3 to 6 weeks after surgery.
A number of studies exist on appropriate leisure activities after a THA.31 A survey of 28 orthopedic surgeons from Mayo Clinic recommended that activities such as cycling, golfing, and bowling are acceptable after a THA. Generally, many physicians counsel well elders to avoid participation in sports that impart high torque or stress on the hip joint, such as jogging. Often, active elders resume activities and athletics regardless of physician or therapist warnings.
Psychosocial issues after total hip replacement
A number of psychosocial issues may surface during an elder’s rehabilitation after a hip replacement. Dealing with a chronic condition such as arthritis can be stressful and frustrating; many elders are required to deal with pain, swelling, and mobility limitations on a daily basis. Providing information on support groups may be beneficial to the elder.
After a THR, some elders find it difficult to abide by the position precautions. They may view these precautions as impediments to resuming the lifestyles they had before the procedure, especially when they had no predisposing medical conditions that limited activities. COTAs should be empathetic to the elder’s concerns, but they must also help elders understand the rationale for adhering to hip precautions (Figure 22-4). The COTA also should address the consequences of not following these precautions. COTAs may need to reassure elders that healing takes time and that involvement in activities may continue but usually with some modifications.

FIGURE 22-4 The elder should extend operated leg and bear weight on arms when coming into a standing position.
Many elders feel guilty or become anxious when they require assistance from family or friends.32 Elders who are temporarily placed in an extended care facility while they heal may also find it difficult to accept assistance from nursing staff in the facility. Feelings of guilt are sometimes accompanied by financial worries about the cost of care. In addition, relocation to a new environment such as a hospital, extended care facility, or long-term care facility can be stressful.33 COTAs should encourage elders to talk about their feelings. When possible, discussing the situation with elders before they are moved to a new facility is beneficial. In addition, the elder should be thoroughly oriented to the new facility.
Occupational therapy interventions
The specific intervention strategies and techniques used with an elder who has had a THA vary depending on whether the anterolateral or posterolateral surgical approach was used (Table 22-5). Adaptive equipment is typically supplied to patients regardless of approach. The most used piece of adaptive equipment tends to be the raised toilet seat, which often is used for at least 6 months after THA. Other pieces of equipment that participants reported to be helpful were the reacher, long-handled shoehorn, and sock aid; however, they did experience some difficulties in using them.
TABLE 22-5 Occupational Therapy Interventions for Posterolateral and Anterolateral Approaches to Total Hip Replacement
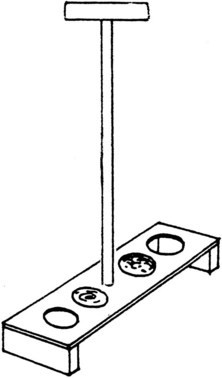
COTAs are involved in educating elders and their caregivers about proper and safe usage of adaptive equipment, observing hip precautions during functional activities, and making environmental adaptations. Laurel is a COTA who works in an acute care hospital and is involved in patient education. Before having a hip replacement, elders and their primary caregivers attend a class to prepare them to return home. Laurel reviews the precautions for both the posterolateral and anterolateral approaches. The elders bring clothing to practice using a dressing stick, reacher, sock aid, and long-handled shoehorn. Laurel has the elders practice transferring to and from a chair, couch, commode, and raised toilet seat. They also practice using reachers to retrieve items from the floor and cupboards. During one question-and-answer session, several elders expressed an interest in feeding their pets. Laurel asked a volunteer from her church to make pet feeders that could be easily lifted from the floor to the counter so that the elders could fill them with water and food without bending over (Figure 22-5). Laurel also reviews information in a notebook with elders and their caregivers that will be used as their home programs. After surgery, Laurel works with elders to review the dressing techniques and reinforces the information that they learned earlier in class. Laurel also makes recommendations for bathroom equipment that the elders may need to return home. Some elders have stated that it was helpful to be exposed to the information before surgery because it was harder for them to concentrate after surgery.
Knee Replacements
The knee joint has a large amount of synovium fluid, and thus one joint is often affected by rheumatoid and osteoarthritis.20 Chronic knee pain may cause difficulty in ascending and descending stairs, squatting, walking, and jogging, thus affecting one’s quality of life.
Nonsurgical intervention may include a variety of approaches, including medication, activity modification and exercise, braces, and weight reduction.20 Nonsteroidal antiinflammatory drugs (NSAIDs) are often prescribed to reduce swelling and pain. Intraarticular injections are sometimes used when oral NSAIDs are ineffective.
Activity modification is targeted to minimize symptoms by avoiding high-impact activities. Maintaining a healthy body weight is difficult for people with knee pain because it often decreases their activities without changing their intake of calories. If possible, elders with knee pain should try to maintain a regular exercise program to maximize aerobic conditioning.
Physical therapists may provide braces to help active elders regain a sense of knee stability during activities. Such knee braces are helpful in the short term, but people tend not to use them on a day-to-day basis.20 Surgical intervention includes a total knee joint arthroplasty or total knee replacement (TKR). Knee arthroplasties are best suited for sedentary persons older than age 65 years.30 Approximately 90% of TKRs are successful up to 10 years after surgery.
Rehabilitation after knee replacement
After a TKR, the knee is bandaged and changed 2 to 4 days after surgery. A HemoVac may be used and discontinued 2 to 3 days after surgery. To promote blood flow and decrease the chance of blood clot formation, the elder will likely wear thromboembolic disease (TED) hose. A knee immobilizer may be prescribed by some physicians. Others will prescribe the use of a continuous passive motion (CPM) machine,30 which is designed to slowly and smoothly range the knee into flexion and extension. Physical therapists monitor the CPM unit and prescribe exercises to the elder.
Occupational and physical therapy services will work with elders to meet the following goals: transfer independently to and from bed, walk with crutches or a walker on a level surface, independently ascend and descend three stairs, independently carry out one’s home exercise program, flex affected knee to 90 degrees, and extend knee to neutral. Other rehabilitation concerns of clients with TKRs include sexual activity, driving, and return to work. Many physicians do not discuss sexual activity related to the TKR. However, clients should be counseled to avoid sexual intercourse for 4 to 6 weeks after TKR. (See Chapter 12 for more specific information about resuming sexual activity after a TKR.) Resuming driving can occur as early as 3 weeks for some elders, whereas others are not ready to drive until 8 months after surgery. The ability to return to driving is dependent on exhibiting good leg control, limiting the use of narcotic pain relievers, and whether the overall recovery is unremarkable.34 Returning to work is more difficult to predict and is dependent on the type of work. Typically patients return to work 3 to 6 weeks after their surgery.34 Keep in mind these are generic timeframes; physicians may instruct their clients with different timeframes on the basis of the clients’ conditions.
Arthritis
Arthritis affects about 37 million of adults in the United States and is prevalent in nearly half of the elder population.2 The self-reported prevalence of arthritis is greater among women than men, and for women age 45 years and older, arthritis is the leading cause of activity limitation.35 Arthritis is also a leading predisposing condition for fractures.36 Arthritis causes bone demineralization. The pain from arthritis limits people’s activity, thus causing weight gain. These factors combined with environmental factors often result in falls or fractures.
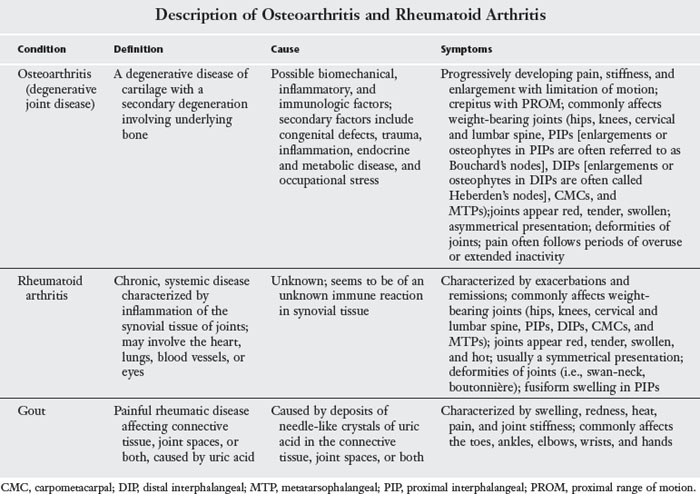
More than 100 types of arthritis have been identified; the three most common types in the elderly population are osteoarthritis (OA), rheumatoid arthritis (RA), and gout.35 Descriptions, causes, and symptoms of these three forms of arthritis are presented in Table 22-6.
Treatment for arthritis in elders can consist of any combination of therapy, medication, and surgery. Therapy may consist of the provision of physical therapy and OT. Medications commonly prescribed to elders who have arthritis are NSAIDs and cyclooxygenase-2 inhibitors (similar to NSAIDs but with fewer side effects). Performing surgery to replace joints is often a last resort.
COTAs must be aware of the physical restrictions and limitations that arthritis imposes on elders’ activities. Interventions by the COTA/OTR team should focus on helping elders manage their symptoms more effectively in addition to modifying occupational tasks.
Common Problems Associated with Arthritis
Osteoarthritis of the knee affects approximately 60% of people older than age 65 years.37 Limitations caused by knee OA include difficulty using stairs, squatting, and high-impact activities (i.e., running or jumping).30 These activities can be quite painful and can reduce the quality of life for an active elder.
Upper extremity deformities caused by OA can be problematic. Osteophytes form in the fingers and base of the thumb. Although osteophytes are not painful, they are seen at the distal interphalangeal (DIP) (Heberden’s nodes) and proximal interphalangeal (PIP) joints (Bouchard’s nodes). Such nodes result in difficulty and pain during pinching. In advanced stages, the thumb’s carpal metacarpal (CMC) joint can subluxate and result in joint instability.
The hands are the most severely affected joints in RA. Often, the PIP joints present with fusiform swelling or spindle-like shape. Boutonnière and swan-neck deformities are also finger deformities that may result from RA. Nalebuff deformities are common to the thumb when affected by RA. Ulnar drift is often present in the metacarpophalangeal (MCP) joints of the hand, and the wrist may sublux volarly.
Gout commonly affects the toes, ankles, elbows, wrists, and hands. Swelling can cause the skin to become taut around the joint and make the area appear red or purple and be tender. These presentations, in turn, reduce joint mobility (NIA, n.d.).
Occupational Therapy Intervention
The primary goal of OT intervention is to improve the quality of life of elders with arthritis. Specific goals may include maintaining joint mobility or joint stability, preventing joint deformity, maintaining strength, maintaining or improving functional ability, maintaining a healthy balance of rest and activity, modifying performance of activities, and improving psychosocial acceptance and coping mechanisms.
Maintenance of joint mobility and stability
COTAs may develop an exercise program for the elder to keep arthritic joints moving. Such an exercise program should seek to minimize stress to all involved joints. Elders with arthritis often find that taking a warm bath or shower after waking up in the morning relieves joint stiffness, thereby making it easier to exercise and engage in other activities. Elders with arthritis may also find it helpful to use a paraffin bath before engaging in wrist and hand exercises. COTAs should demonstrate service competency when using physical agent modalities.
Joints requiring stability may warrant orthotic intervention. A carefully designed splint may provide stability to a joint and improve function. For example, discomfort in the CMC joint may be reduced by fabricating a hand-based thumb spica splint to support the CMC joint in a functional position.38
Prevention of joint deformity
COTAs must be aware of the common types of joint deformities that may develop as a result of arthritis. Deformities include wrist subluxation, ulnar drift of the MCP joints, swan-neck deformity, boutonnière deformity, and Nalebuff type I deformity of the thumb.
Volar subluxation of the wrist frequently occurs in elders who have arthritis. A wrist cock-up splint may aid the elder in maintaining better wrist alignment, which will promote function and reduce pain.39 Ulnar drift, or ulnar deviation, of the MCP joints is another common deformity caused by arthritis. Ulnar drift is usually caused by the destruction and loosening of the radial collateral ligaments. Some experts suggest that the use of an ulnar drift splint may prevent further deformity.38
A swan-neck deformity of the finger results in PIP hyperextension with DIP flexion. A boutonnière deformity results in PIP flexion with DIP hyperextension. Both deformities can be splinted or surgically repaired with varying results. A Nalebuff type I deformity results in the metacarpal joint of the thumb flexed with hyperextension of the interphalangeal joint. A radial gutter thumb spica splint is often used for better positioning.40
To prevent further deformity, elders should be evaluated to determine whether they need splints that are appropriate for the deformity and activity level. In addition, elders should be taught joint protection techniques (Box 22-1).
BOX 22-1 Joint Protection Principles
 Respect pain. Monitor activities and stop to rest when discomfort or fatigue develops. For example, if kneeling or stooping to garden causes pain and stiffness, stop and rest. Next time, try sitting on a stool.
Respect pain. Monitor activities and stop to rest when discomfort or fatigue develops. For example, if kneeling or stooping to garden causes pain and stiffness, stop and rest. Next time, try sitting on a stool.
Reduce stresses on joints. Use the largest joint possible for activities. For example, when using hands to push up from a seated position, push up with the palms, not the back of the fingers.
Wear splints as prescribed to protect joints. For example, wear resting hand splints during exacerbation periods to reduce pain. Movements should be done in the opposite direction of deformity. For example, when wringing out a wash cloth, twist toward the radial side rather than the ulnar side.
Avoid sustaining a strong, tight grasp. For example, use foam or a cloth wrapped around handles to relax the grip needed to manipulate an object.
Avoid carrying and lifting heavy objects. For example, use a cart to move heavy objects. Distribute object weight evenly over many joints. For example, use both hands to handle a carton of milk.
Limit the amount of time spent climbing, walking, and standing. For example, take an elevator or escalators; drive or use a walking aid; sit whenever possible.
Avoid sustained flexion of the finger joints. For example, use a large sponge for cleaning; work with the fingers extended over the sponge rather than squeezing it.
Avoid using heavy objects. For example, cook with lightweight pots and pans rather than heavy cast-iron pots and pans.
Maintenance of strength
COTAs may be asked to develop graded strengthening programs for elders who have arthritis. These programs should include the principles of joint protection discussed previously. During periods of acute exacerbation of arthritis, elders should not engage in strengthening programs.
Improvement of functional ability
Functional ability can be improved through careful collaboration between the COTA, OTR, and the elder. This collaboration can help determine whether assistive equipment works well and is accomplishing the goal for which it was intended. For example, a rocker knife may allow the elder to continue to cut meat during meals. COTAs must observe how the elder handles the knife to ensure that the involved joints are protected as the knife is used and to ascertain that the knife actually cuts the meat.
Maintenance of life balance
Graded strengthening programs for elders who have arthritis are developed by OTRs and may be administered by COTAs. Assisting elders in achieving a balance between rest and activity is paramount. For example, elders are often tempted to schedule all activities during the morning hours with the hope of resting in the afternoon. However, a better balance is achieved when activities are scheduled throughout the day and an appropriate period of rest is incorporated after each activity. This type of schedule will help decrease the fatigue of elders and is less likely to lead to an exacerbation of their conditions. In addition, elders will likely accomplish more during the day.
Modification of activity
Work simplification and energy conservation techniques often benefit elders who have arthritis (Table 22-7). These elders must attempt to distribute their energy output evenly over the number of tasks to be accomplished. Incorporating energy conservation and work simplification techniques into the elders’ daily routines can assist them in maintaining a functional lifestyle.
TABLE 22-7 Principles of Work Simplification and Energy Conservation
| Pace | A moderate, slow pace is most productive; a slower pace is needed in a hot and humid atmosphere. |
| Rhythm | Working in a rhythmic manner saves energy and increases efficiency. |
| Eyes | Work in a well-lighted room, with local light for close work, and rest the eyes periodically. |
| Rest | Plan regular rest periods that are properly spaced during the day. |
| Body mechanics | Sit to work whenever possible; sit in a seat large enough to give full support; work with the elbows close to the body; if working at a table, the height of the table should be near the height of the elbows when they are bent at 90-degree angles. |
| Work areas | A place should be designated for all tools, utensils, and materials; materials should be located close to the area where they will be used. |
| Design of equipment | Handles of utensils and equipment should permit the maximum surface of the hand to come in contact with the handle; handles should be heat-resistant and built up as appropriate; handles that have impressions for the fingers should be used when possible; lightweight equipment should actually be light in weight. |
| Kitchen storage | Store supplies and utensils within easy reach; arrange the cupboards so that all articles are easy to see, easy to reach, and easy to grasp; store heavy equipment (e.g., stacks of plates and pans) on shelves that are easy to reach; use vertical dividers for dish storage, baking pans, trays, and lids; avoid clutter by eliminating or discarding unnecessary equipment. |
| Cooking | Use a cart for transporting food and dishes; slide heavy pots from the sink to the stove instead of lifting them; avoid holding containers or mixing bowls when preparing food; select equipment that can be used for more than one job. |
| Bed making | To avoid numerous trips around the bed, make one side completely and then the next side; if possible, keep the bed away from the wall; have the bed put on rollers if it must be moved. |
| Cleaning | When cleaning the bathtub, use long-handled brushes and sit on the edge of the bathtub; use a dust cloth on a long-handled stick for dusting baseboards and ceilings; have cleaning equipment available both upstairs and downstairs. |
Improvement of psychosocial well-being and coping mechanisms
The combination of acute and chronic pain, coupled with joint stiffness and immobility, can result in limitations of ADL such as dressing, and recreational and social outlets such as dancing. The population of elders who experience pain is challenged daily to use strategies that will enhance productive living. Elders who do not have coping and support systems will need assistance in developing such systems. COTAs may provide assistance by linking elders who have arthritis with community resources that can provide support and help elders develop coping mechanisms. Self-help courses sponsored by the Arthritis Foundation can provide social interaction. Alternative methods of pain control may include relaxation training, cognitive restructuring and modification, medication fading, and social assertiveness training. The process of helping elders cope with arthritis must involve a multidisciplinary approach for chronic pain management to be successful.
Case Study
Ford and Ida are meeting with a builder to design their retirement condominium. In planning the space, they have decided to consult with an agency that provides assistance for home design and modification for elders. They are awaiting a contact from the agency to schedule a meeting to begin plans for the new condominium.
One month previously, Ford fell during the nighttime in an attempt to go to the bathroom and sustained a hip fracture. Subsequently, he underwent an open reduction internal fixation and pinning of his right hip. Also, last year Ida had a TKA. Ida has considerable pain from RA. They hope to plan their ranch-style condominium to meet their current and future needs in relation to their health.
Case Study Review Questions
1. List the precautions that Ford might need to follow after his hip pinning procedure.
2. List the ADL functions that will be directly affected by Ford’s hip pinning procedure.
3. Describe the problems that Ida may be dealing with as a result of RA.
4. Name the wrist and hand deformities associated with RA that may be afflicting Ida.
5. Describe some possible causes for Ford’s fall that should be investigated.
6. Describe the ways in which Ford’s performance of ADL functions and his environment will need to be modified.
7. List appropriate recommendations for the living room, kitchen, bathroom, and bedroom for their new condominium.
1. Identify the most common causes of fractures in elders.
2. Why do elder women have a greater occurrence of orthopedic problems than elder men?
3. Why is it important for the COTA to have an understanding of the anterolateral and posterolateral approaches related to total hip replacements?
4. Identify two psychosocial issues that may have an effect on an elder after a total hip replacement.
5. Using joint protection techniques, explain how you would teach elders with arthritis in their hands to do the following:
6. Explain how you would teach an elder energy conservation techniques during the following activities:
1 Centers for Disease Control, 1996. Incidence and costs to Medicare of fracture among Medicare beneficiaries age 65 years—United States, July 1991-June 1992. Morbidity and Mortality Weekly Report, 45 (41), 877-883.
2 National Institute of Arthritis and Musculoskeletal and Skin Diseases. Living with arthritis [WWW page]. http://www.niams.nih.gov/Health_Info/Arthritis/default.asp, 2010.
3 Min L., Yoon W., Mariano J., Wenger N., Elliott M., Kamberg C., et al. The vulnerable elders: 13 Survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. Journal of the American Geriatrics Society. 2009;57(11):2070-2076.
4 White A., Hashimoto R., Norvell D., Vaccaro A. Morbidity and mortality related to odontoid fracture surgery in the elderly population. Spine. 2010;35:S146-S157.
5 Woolf A., Akesson K. Preventing fractures in elderly people. British Medical Journal. 2009;338(7685):89-96.
6 Söderqvist A., Ekström W., Ponzer S., Pettersson H., Cederholm T., Dalén N., et al. Prediction of mortality in elderly patients with hip fractures: A two-year prospective study of 1,944 patients. Gerontology. 2009;55(5):496-504.
7 Heuberger R. Alcohol and the older adult: A comprehensive review. Journal of Nutrition for the Elderly. 2009;28(3):203-235.
8 Wolinsky F., Bentler S., Li L., Obrizan M., Cook E., Wright K., et al. Recent hospitalization and the risk of hip fracture among older Americans. Journals of Gerontology. 2009;64A(2):249-255.
9 Moayyeri A., Bingham S., Luben R., Wareham N., Khaw K. Respiratory function as a marker of bone health and fracture risk in an older population. Journal of Bone and Mineral Research. 2009;24(5):956-963.
10 McKay C., Anderson K. How to manage falls in community dwelling older adults: A review of the evidence. Postgraduate Medical Journal. 2010;86(1015):299-306.
11 Chen J.S., Sambrook P.N., Simpson J.M., March L., Cumming R., Seibel M., et al. A selection strategy was developed for fracture reduction programs in frail older people. Journal of Clinical Epidemiology. 2010;63(6):679-685.
12 Insurance Institute for Highway Safety. How many older drivers are there? Retrieved July 8, 2010, from http://www.iihs.org, 2010.
13 National Institute on Aging. Age page: Older drivers [WWW page]. URL http://www.nia.nih.gov/HealthInformation/Publications/drivers.htm, 2010.
14 Classen S., Shechtman O., Awadzi K.D., Joo Y., Lanford D.N. Traffic violations versus driving errors of older adults: Informing clinical practice. American Journal of Occupational Therapy. 2010;64(2):233-241.
15 Kelsey J., Samelson E. Variation in risk factors for fractures at different sites. Current Osteoporosis Reports. 2009;4:127-133.
16 Guadalupe-Grau A., Fuentes T., Guerra B., Jose A. Exercise and bone mass in adults. Sports Medicine. 2009;39(6):439-468.
17 Lipton A. Bone continuum of cancer. American Journal of Clinical Oncology. 2010;33(Suppl. 3):S1-S7.
18 Egol K., Koval K., Zuckerman J. Handbook of Fractures, 4th ed. Hagerstown, MD: Lippincott Williams & Wilkins; 2010.
19 Sueki D., Brechter J. Orthopedic Rehabilitation Clinical Advisor. Maryland Heights, MO: Mosby; 2010.
20 Brotzman B., Wilk K. Handbook of Orthopedic Rehabilitation, 2nd ed. St. Louis, MO: Mosby; 2006.
21 Brauer C., Coca-Perraillon M., Cutler S., Rosen A. Incidence and mortality of hip fractures in the United States. Journal of the American Medical Association. 2009;302(14):1573-1579.
22 Kim Y. Comparison of primary total hip arthroplasties performed with a minimally invasive technique or a standard technique: A prospective and randomized study. Journal of Arthroplasty. 2006;21(8):1092-1098.
23 Heinrich S., Rapp K., Rissmann U., Becker C., König H. Cost of falls in old age: A systematic review. Osteoporosis International. 2010;21(6):891-902.
24 Parker, M., Handoll, H., 2006. Replacement arthroplasty versus internal fixation for extracapsular hip fractures in adults. Cochrane Database of Systemic Reviews 19 (2), CD000086.
25 Crotty, M., Unroe, K., Cameron, I., Miller, M., Ramirez, G., Couzner, L., 2010. Rehabilitation interventions for improving physical and psychosocial functioning after hip fracture in older people. Cochrane Database of Systematic Reviews, Issue 1, Art. No.: CD007624.
26 Hozak W., Parvisi J., Bender B. Surgical Treatment of Hip Arthritis: Reconstruction, Replacement, and Revision. Philadelphia: WB Saunders; 2009.
27 Khan, F., Ng, L., Gonzalez, S., Hale, T., Turner-Stokes, L., 2008. Multidisciplinary rehabilitation programmes following joint replacement at the hip and knee in chronic arthropathy. Cochrane Database of Systematic Reviews, Issue 2, Art. No.: CD004957.
28 Parker, M., Gurusamy, K., Azegami, S., 2010. Arthroplasties (with and without bone cement) for proximal femoral fractures in adults. Cochrane Database of Systematic Reviews, Issue 6, Art. No.: CD001706.
29 McGann W. Surgical approaches. In: Barrack R., Booth R., Lonner J., McCarthy J., Mont M., Rubash H., editors. Orthopedic Knowledge Update: Knee and Hip Reconstruction. Rosemont, IL: American College of Orthopedic Surgeons; 2006:311-322.
30 Bhave A. Rehabilitation after total hip and total knee replacement. In: Barrack R., Booth R., Lonner J., McCarthy J., Mont M., Rubash H., editors. Orthopedic Knowledge Update: Knee and Hip Reconstruction. Rosemont, IL: American College of Orthopedic Surgeons, 2006. (2006)
31 Brander V.A., Mullarkey C.F., Stulberg S.D. Rehabilitation after total joint replacement for osteoarthritis: An evidence-based approach. Physical Medicine and Rehabilitation. 2001;15(1):175-197.
32 Robnett R., Chop W. Gerontology for the Health Care Professional, 2nd ed. Sudbury, MA: Jones & Bartlett; 2010.
33 Alkema G., Wilber K., Enguidanos S. Community- and facility-based care. In: Blackburn J., Dulum C., editors. Handbook of Gerontology: Evidence-Based Approaches to Theory, Practice, and Policy. Hoboken, NJ: John Wiley & Sons, 2007.
34 Mullarkey C.F., Brander V. Rehabilitation after total knee replacement for osteoarthritis. Physical Medicine and Rehabilitation: State of the Art Reviews. 2002;16:431-443.
35 Walker J., Helewa A. Physical Rehabilitation in Arthritis. Philadelphia: WB Saunders; 2004.
36 Gillespie, L.D., Gillespie, W.J., Robertson, M.C., Lamb, S.E., Cumming, R.G., Rowe, B.H., 2009. Interventions for preventing falls in elderly people. Cochrane Database of Systematic Reviews, Issue 2. Art. No.: CD000340. DOI: 10.1002/14651858CD000340.pub2.
37 Mikuls T. Arthritis incidence: What goes down must go up? Arthritis and Rheumatism. 2010;62(6):1565-1567.
38 Riley M.A., Lohman H., Berger S.M., Cavanaugh M.T., Coppard B.M. Splinting on elders. In Coppard B.M., Lohman H., editors: Introduction to Splinting, 2nd ed, St. Louis, MO: Mosby, 2007.
39 Lohman H. Wrist immobilization splints. In Coppard B.M., Lohman H., editors: Introduction to Splinting, 2nd ed, St. Louis, MO: Mosby, 2007.
40 Lohman H. Thumb immobilization splints. In Coppard B.M., Lohman H., editors: Introduction to Splinting, 2nd ed, St. Louis, MO: Mosby, 2007.