Chapter 7 The principles of therapeutic exercise and physical activity
KEY POINTS
 Physical activity is essential for muscle, joint, general physical, psychological and social health, function and well-being
Physical activity is essential for muscle, joint, general physical, psychological and social health, function and well-beingINTRODUCTION
This chapter provides a brief overview of the importance of muscle, exercise and physical activity in the aetiology and management of common rheumatic conditions, such as osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, juvenile idiopathic arthritis, and others. It also gives practical advice on how to help people begin and continue regular exercise. Exercises for individuals with specific conditions can be found within the chapters following.
JOINTS = MOVEMENT
The reason for having a joint is to enable us to move and so function. Joints were made to move, if we do not move our joints stiffen, our muscles get weaker, we tire sooner and control of movement is poorer. All of these can contribute to pain, disability and increase the risk of developing acute and chronic ill-health (diabetes, heart disease, high blood pressure, depression, obesity). Physical activity is any movement produced by skeletal muscles that expends energy (Caspersen et al 1985). Exercise is a subcategory of physical activity defined as the planned, structured and repetitive movement, to maintain or improve physical fitness (e.g. cardiovascular fitness, muscle strength and endurance, flexibility and body composition) and psychological well being (ACSM 2006). Remaining physically activity is vital for everyone and benefits our muscles, joints, general physical (respiratory, cardiovascular health), psychological (self-confidence, self-esteem,) and social (independence, social interaction) well-being.
THE IMPORTANCE OF MUSCLE
Until relatively recently little consideration had been given to the importance of muscles in rheumatic conditions, most interest concentrated on what was happening inside the joint. However, synovial joints are comprised of intra-articular (bone cartilage, capsule, etc) and extra-articular structures (muscles, ligaments, nerves). If any articular structure is dysfunctional normal joint functioning will be compromised, leading to joint damage, pain and disability (Hurley 1999).
To appreciate the importance of muscle we need to appreciate its sensorimotor functions. Some muscle functions are obvious, others are less obvious but just as important. The most obvious function of muscle is to contract and effect controlled movement. Controlled antagonistic muscle activity enables functional stability so that we are mobile yet stable - we can stand upright, walk, stabilise our upper arms so our hands can perform dexterous movements. This control depends on accurate proprioceptive sensory information much of which arises from muscle receptors (muscle spindles and golgi tendon organs) that informs us about our body position, movement and loading. Without this sensory information we would not be able to produce controlled movement and over time uncontrolled, clumsy, jarring movement results in damage, so our muscles are vital for joint protection.
If, due to natural ageing processes, reduced activity, injury or rheumatic disease, muscles become deconditioned (weak, easily fatigued, proprioception impaired, movement poorly controlled) then neuromuscular protective mechanisms that protect our joints will be compromised. Over time this can result in damage to cartilage and subchrondral bone, pain and disability. Importantly, this means muscle sensorimotor dysfunction may be a cause of joint damage rather than simply a consequence of it (Hurley 1999). Therefore, maintaining well conditioned muscles may enable us to maintain healthy joints, or ameliorate some of the effects of joint damage.
BENEFITS OF EXERCISE
Muscle’s involvement in arthritis is good news, because of all the structures that comprise our joints, muscle is the tissue we can manipulate most easily through exercise and physical activity. When physical activity levels exceed the habitual load on our physiological or anatomical systems, our bodies adapt to accommodate the increased load-the ‘overload principle’. Exercise can increase strength, endurance and motor control, reducing pain and disability and minimising joint damage.
RANGE OF MOVEMENT
Movement is vital for joint health and function as it maintains the length of soft tissues (joint capsule, ligaments, tendons, muscles), washes synovial fluid across the avascular articular cartilage bringing nutrients and removing waste, stimulates repair and reduces joint effusion (Buckwalter 1995). Therefore joints must be moved through their full range of movement (ROM) frequently to avoid soft tissues shortening, cartilage atrophying and articulating bones fusing. Maintaining joint mobility is important for everybody, but even more so for people with rheumatic conditions who are at increased risk of loss of joint mobility and consequent stiffness, pain, muscle weakness and functional limitations (Zochling et al 2006).
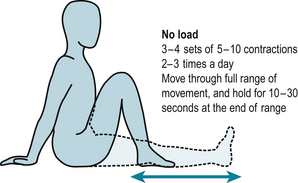
Movement can be maintained and regained by performing slow, controlled and sustained stretches at the end of ROM (Dagfinrud et al 2005). The amount of stretching done depends on how ‘irritable’ a joint is - how easily pain and effusion are provoked and if the stretching regimen has just begun. These should be performed in three to four sets of 5–10 stretches, two to three times a day (30–120 stretches in total) with each stretch held for 10–30 seconds without ‘bouncing’ (Fig. 7.1). This may cause mild discomfort, but should not cause pain.
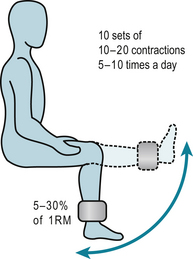
MUSCLE FUNCTION
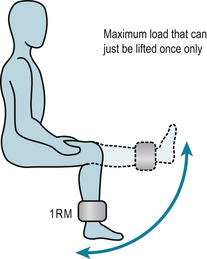
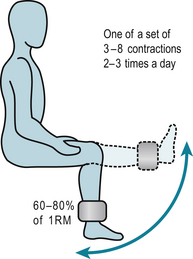
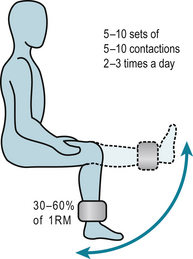
Inactivity leads to muscle weakness and increased fatigability. Fortunately, muscle has considerable ability to adapt to the loads and stresses placed on it. Specific rehabilitation regimens use the overload principle to improve muscle function. Using the load someone can lift only once through a certain range, called the 1 repetition maximum (1RM), as the reference load (Fig. 7.2) such regimens can:
FUNCTION
While we can address many specific aspects of muscle dysfunction with exercise regimens our ultimate aim is to help people maintain, regain and maximise functioning. Most people with rheumatic conditions want a level of muscle function that will enable them to perform their daily activities, as easily and comfortably as possible. Activities of daily living require a combination of strength, endurance and control, so exercise regimens that address muscle dysfunction must address these deficits. However, people also need to perform the activities that address their function deficits with functional activities such as sit-to-stand, steps-ups, stair climbing and balance (Fig. 7.6). These allow people to appreciate the relevance of exercise in the carry-over to easier performance of activities of daily living, maintenance of functional independence and their active involvement in their management.
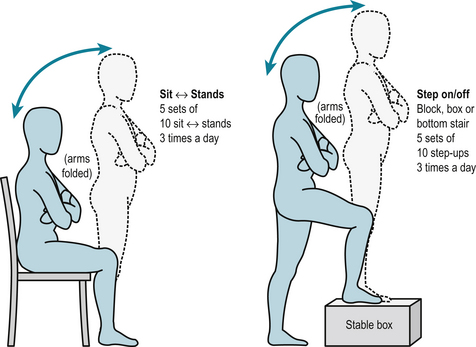
Progression of exercise is achieved by ‘overloading’ the tissues and pushing the limits of an individual’s current capabilities, for example increasing resistance, making the activity more challenging (lowering the height of a chair for sit-to-stand, increasing the height of the step for step-ups) or increasing the number of repetitions. Continuing to exercise at a given level will maintain strength, endurance, fitness and functioning at that level. However, once exercise is stopped, the stimulus for adaptation is removed and people regress. Consequently, doing less will result in regression and loss of muscle strength, endurance and control.
FORMAL REHABILITATION PROGRAMMES
Typically, exercise-based rehabilitation is carried out in hospital out-patient departments. These regimens take various forms, but predominantly involve land-based exercises supervised by healthcare professionals (usually physiotherapists, occupational therapists, exercise therapists) who devise an individualised exercise programme to address each patient’s needs and goals, using the overload principle to increase muscle strength, endurance, joint flexibility and function. This is performed individually or in groups and supplemented with a home exercise regimen. After they have completed the regimen (usually between one and six sessions) they are discharged with advice to continue exercising, follow-up is rare (Walsh & Hurley 2005).
Reviews of research regimens demonstrate that exercise is safe and effective for people with a wide range of rheumatic conditions (Brosseau et al 2004, de Jong & Vlieland 2005, Devos-Comby et al 2006, Fransen et al 2002, Hurley 2003, Klepper 2003, Minor 1999, Munneke et al 2005, Pelland et al 2004, Pendleton et al 2000, Roddy et al 2005, Stenström & Minor 2003, van Baar et al 1999, van Tulder et al 2002).
However, often these research regimens bear little resemblance to the clinical management as they tend to be prolonged, complex regimens that require supervised use of sophisticated equipment so people become reliant on therapists. Once supervised rehabilitation stops, people’s motivation to exercise wanes, exercise ceases and the benefits are lost. To sustain benefits, patients must continue to participate in regular exercise. Given the size of the population, the chronic, long-term nature of rheumatic conditions and limited resources, the clinical applicability of many exercise regimens is limited. Clinically practicable regimens have been developed that are more likely to be deliverable to large numbers of people (Bearne et al 2002, Ettinger et al 1997, Hay et al 2006, Hurley et al 2007, McCarthy et al 2004, Thomas et al 2002).
Hydrotherapy employs water-based exercises that utilises the warmth and buoyancy of water to relax muscles and reduce the weight-bearing load and stress on our legs and trunk, but also uses water to assist and resist movement to help us exercise more effectively (Cochrane et al 2005, Epps et al 2005, Foley et al 2003, Fransen et al 2007, Green et al 1993, Patrick et al 2001, Takken et al 2003, Verhagen et al 1997, 2004). Hydrotherapy is very popular with people but requires dedicated facilities and therapists which makes it very expensive. Given the limited healthcare budgets and the large number of people with rheumatic conditions only a small minority of people will ever receive a brief, one-off course of hydrotherapy. Increasingly local community pools are organising ‘aquatherapy’ classes that provide more people with the opportunity to participate in controlled water-based exercise classes, supervised by experienced therapists at moderate cost (Cochrane et al 2005). If aquatherapy classes are not available recreational swimming and exercising gently in a local pool is an excellent way to keep stiff painful joints moving.
Tai Chi and Yoga are other less traditional ways of exercising that are popular and widely available and early small trials have found them to be effective (Ernst 2006, Fransen et al 2007), but not everyone wants to participate in these types of activities. It makes no difference where people exercise whether they exercise alone at home, in a leisure centre or join an exercise class (Ashworth et al 2005), so personal preferences can be accommodated. Although people are often reluctant to exercise in groups the additional benefit of group exercise classes is the peer support and motivating reinforcement fellow participants provide, the facilities and social interaction all of which encourages commitment to long-term exercise.
SAFETY
The first rule of any healthcare intervention is ‘do no harm’. Physical activity and exercise is contraindicated in very few people-those with advanced, serious, unstable medical conditions, and those with very deformed and unstable joints. Theoretical fears that exercise and physical activity exacerbates inflammatory rheumatic conditions (Blake et al 1989, Merry et al 1991) have not been supported by evidence. In fact in people with mild to moderate rheumatic disease exercise improves aerobic fitness, muscle strength, pain and disability following exercise programs without exacerbating symptoms, radiological damage or disease activity (Bearne et al 2002, Brosseau et al 2005, Ekdahl & Broman 1992, Minor 1999, Munneke et al 2005, Nordemar et al 1981, Stenstrom et al 1991, 1993, van den Ende et al 1998, Zochling et al 2006). It is important that physical activity and exercise is sensibly planned and not overambitious, any new activity should be started slowly, increased gradually and performed moderately (see Patient Information Sheet 7.1). As a rough guide people are exercising moderately when they can do an activity and still hold a conversation but cannot sing (the informal ‘talk test’) and vigorously when they cannot talk while doing an activity (Meldrum 2003).
People may have concerns about the safety of exercise, which need to be discussed to allay fear and anxiety. Initially, supervised exercise may be required in order to reassure people that exercise is safe and encourage them to exercise. People with severe joint malalignment might be discouraged from undertaking strenuous strengthening exercises (Brouwer et al 2007) but should still be counselled to be physically active with precautions such as little and often, using a walking stick, etc. But it should be emphasised that for the vast majority of people sensibly planned physical activity and exercise is not harmful and the benefits of physical activity far outweigh the risks of inactivity.
INFORMAL EXERCISE AND PHYSICAL ACTIVITY
Fitting something else into a busy life is difficult. Moreover, notions of ‘going for the burn’ and ‘no pain no gain’ are incorrect, misguided, off-putting and potentially dangerous. If people perceive exercise as a damaging, burdensome chore, requiring ‘blood, sweat and tears’, expert instruction and supervision, and access to expensive, sophisticated, user-unfriendly equipment and facilities, they are unlikely to commence and continue exercising.
There’s no denying that acquiring health benefits from exercise does require effort, will-power and determination, but it does not require long bouts of exhausting, strenuous exercise, joining a gym or use of equipment. Since exercise is a subcategory of physical activity, our usual daily physical activities-walking, gardening, shopping, housework, occupational and leisure activities, a day out, etc – can all be regarded as ‘informal’ exercise that have health benefits (ACSM 2006, Fletcher et al 2001, NICE 2006, Pate et al 1995). The workload incurred during common daily physical activities can be expressed as metabolic equivalent (MET) of lying quietly doing nothing, e.g. lying = 1.0 (referent value), shopping = 4.2 (Fletcher et al 2001).
To attain health benefits, people need to accumulate 30 minutes of physical activity on most days of the week. This could, for example, be achieved by one 30-minute brisk walk, or accumulated during two 15-minute walks, or three 10-minute walks. Additional benefits are gained from doing activities for longer or at higher intensity, and as health benefits acquired from physical activity are ‘dose-related’, within reason, the more people do the better.
Walking is a very safe, simple and beneficial physical activity that doesn’t require specialist equipment or facilities. People can easily begin to exercise by increasing the amount they walk-walking rather than driving, getting off a bus earlier and walking the last bit. Almost anything that gets you up, active and out is good. More ‘formal’ exercise (e.g. cycling, swimming, yoga, Tai Chi or exercise classes) are excellent, but require extra effort, equipment, facilities and sometimes supervision which may be unavailable. People need to find something that they want to do that is comfortable, enjoyable, affordable and available, and find ways to integrate it into their lifestyle (NICE, 2006).
PSYCHOSOCIAL EFFECTS OF PHYSICAL ACTIVITY AND EXERCISE
Illness does not take place in a biological vacuum. People are not just affected by the biological or anatomical disruption caused by a pathology, they are also affected by their and other people’s psychological and emotional reaction to illness and many other social, and environmental factors (Hurley et al 2003, Main & Watson 2002, Turk 1996) (see Chs 5 & 11). People with rheumatic conditions are often elderly, have been inactive for some time, are unfit and have co-morbidities (e.g. respiratory, cardiovascular). While many people intuitively understand that movement is good for joints, they are concerned and confused by their experience that activity often causes joint pain and rest eases it. They interpret pain as signalling activity-induced joint damage, assume that rest prevents damage and promotes healing, and surmise that reducing physical activity will prolong the life of their joints and begin to avoid activities. These ‘fear-avoidance’ beliefs and behaviours lead to people becoming less active with all the attendant problems and consequences of inactivity (Dekker et al 1992).
The traditional ‘biomedical model’ of ill-health takes little account of health beliefs, but aims to ‘cure’ the underlying pathology using medical or surgical interventions, the patient is a passive recipient of these interventions. The ‘biopsychosocial model’ of ill-health (Main & Watson 2002, Turk 1996) is described in detail in Chapter 5. This model accepts there is often a biological cause of ill-health and symptoms. It takes a holistic approach to the assessment and treatment of rheumatic conditions and places much more importance on the influence of people’s health beliefs, understandings, experiences, emotions and social environment on their reaction to their health problems, their ability to cope with and adjust to living with the consequences of chronic ill-health. People’s attitudes and beliefs about their health, how they cope with ill-health and their confidence in their ability to do what they need to determines their reaction to ill-health and their ability to exercise. Attitudes and beliefs about the cause and prognosis of ill-health and effective treatment are major determinants of illness behaviour and willingness to exercise and undertake physical activity. People who ‘catastrophise’ and believe their ill-health to be inevitable, incurable and untreatable, will feel demoralised, anxious and helpless and their self-confidence is undermined (Main & Watson 2002, Turk 1996, Turner et al 2000). Coping strategies are efforts people make to minimize the effects of ill-health. People who employ passive coping strategies (e.g. resting, avoiding activities, relinquishing responsibility for pain control to others) have worse pain and function than people who use active coping strategies (e.g. remaining physically active, diverting attention) and avoid catastrophising (Keefe et al 1996). The coping strategies employed are based on people’s beliefs and past experiences. Self-efficacy is a person’s confidence in their ability to perform tasks like taking exercise (Bandura 1977). People with high self-efficacy are less anxious, less depressed and report less pain, are more physically active and more willing to attempt and persevere with exercise programmes than people with low self-efficacy (McAuley 1992, McAuley et al 1993).
Crucially, psychosocial traits are not set in stone, they can be altered for better or worse by positive and negative experiences (Main & Watson 2002, Turk 1996). This malleability presents opportunities to promote exercise and physical activity. Patient education and self-management interventions successfully challenge erroneous ill-health beliefs (Bodenheimer et al 2002, Coulter & Ellins 2007, Holman & Lorig 1997, Newman et al 2004, Superuio-Cabuslay et al 1996, Warsi et al 2003) about physical activity. For example informing people that rheumatic conditions are not untreatable, that pain-related activity does not signal joint damage, that movement is good for joints, inactivity is bad, how they could easily become more active, and reassure them about what they can (not) do. They also help people re-evaluate their problems, reduce anxiety, catastrophising and fear-avoidance behaviours and give people active strategies enabling them to help themselves.
INTEGRATED REHABILITATION PROGRAMMES
The most effective chronic ill-health management regimens integrate exercise with patient education on healthy life-styles, self management of disease and coping strategies (Griffiths et al 2007, Hurley et al 2007). Such programmes maximise the benefits from both physical and educational approaches, challenging erroneous health beliefs and inappropriate behaviour. The positive mastery experienced following successful completion of a simple, practical exercise regimen that people can perform themselves without exacerbating symptoms gives tangible, meaningful improvements (Hurley et al 2007). Such regimes enhance self-efficacy and provide active coping strategies (exercise/physical activity) that enable people to help themselves, reducing helplessness, disability and social isolation. The danger is that unsuccessful, negative experiences (for example involvement in complex exercise regimens, requiring expensive, specialized equipment, facilities and supervision) undermine self-efficacy, encourage passive coping strategies and dependency on others.
GETTING PEOPLE TO BEGIN AND CONTINUE EXERCISING
This section gives some practical advice about helping people begin and continue to exercise regularly. This may be best given during a supervised rehabilitation programme, reinforced with written information and regular follow-up.
GETTING GOING
People who are not normally active should be advised to begin with gentle non-weightbearing joint range of movement exercises (sitting on a bed, settee or the floor slowly bend and straighten their knees) (Fig. 7.1) or low impact activities such as a gentle walk (see Patient Information Sheet 7.2). They should assess how far they can walk before the onset of pain, set a target well within this distance, walk little and often within this distance, at a comfortable pace, resting frequently, using a walking stick if needed and training shoes or shoes with viscoelastic soles or insoles to reduce impact forces (Whittle 1999).
People often begin to experience pain after doing an activity for a short time, but continue to do the task until it is completed or pain becomes so bad they have to rest. This can reinforce negative feelings and worries about the association between physical activity and pain and joint damage. It can be helped by teaching people ‘rest-activity cycling’, where physical activity is interspersed with rest or less strenuous activities (pacing) (see Ch.10). People are encouraged to recognise how long it takes for them to begin to feel tired or experience mild discomfort, told to take a short rest at this point before returning to the task and take another break if pain starts to increase again or finish the task another time. Implementing simple relaxation techniques can also help reduce tension and anxiety (see Ch.11). Although rest-activity cycling may seem inconvenient and time consuming, people will find that by implementing it the time spent being active will gradually increase, activities will get easier and they will incur less pain.
To avoid ‘woolly’ plans being forgotten people should construct a very specific ‘action plan’ of achievable, personally meaningful goals. These might be simple ‘functional’ common activities of daily living such as walking to the shops, climbing a flight of stairs or doing the housework. The action plan should state exactly what activities they are going to do, when, where and how, and should be placed where it will be seen often (on a fridge door). Telling other people what they are trying to do can elicit peer support and turning intention into action (Mazzuca & Weinberger 1998).
People should always be nudging the boundaries of their capabilities, so that over days, weeks or months, if necessary, the frequency and intensity of exercises and activities is increased, for example by increasing the distance walked a little each time, walking more often and a little brisker. Monitoring progress highlights progress and goal-attainment, which is a powerful motivator for continued adherence. Once a goal has been achieved this achievement should be appreciated and rewarded. Then a slightly more challenging target can be set to push the boundaries of their capabilities a little further. If a goal proves too difficult a less ambitious target should be set to avoid disillusionment and undermining self-confidence and esteem. Once people have reached a level of physical activity that suits them, maintaining that level will maintain the gains they have achieved, dropping below this results in regression.
KEEPING GOING
Long term participation in regular exercise is disappointing; more than 50% of people stop exercising within 1 year (see Patient Information Sheet 7.3). This probably reflects the time and effort required for exercise which competes with work, family and leisure commitments, their attitudes and beliefs about exercise, family and social support and networks, and the many other priorities and problems in people’s lives. Long term adherence to exercise can be improved by enhancing self-efficacy which improves patient adherence with exercise programs (McAuley 1992, McAuley et al 1993, Rejeski et al 1998). Sustaining long–term adherence requires regular follow-up, and reinforcement of healthcare messages is usually required to re-motivate people. Unfortunately, given finite healthcare resources the large patient population and the chronic nature of benign rheumatic conditions, supervised exercise and regular follow-up is logistically difficult. Finding ways in which people maximise self-management and self-motivation are essential, for example people need to remind themselves of the health benefits of physical activity; exercise should be seen as a necessity not a chore; the dangers of inactivity should be understood; improvements that simple activities can bring should be experienced; and the support of family and friends should be encouraged.
Inevitably, people will experience times when they don’t, won’t or can’t exercise, because of pain, other commitments, inclement weather or they are too tired. Identifying potential barriers to exercise and planning ways of overcoming them can help. If a joint is painful they could rest until this subsides. If the weather’s bad, exercise indoors, take a walk where it’s sheltered or maybe rest for a day. It is important that a legitimate reason doesn’t become an excuse, so when the pain subsides, enthusiasm returns or the weather cheers up, unless people resume their previous level of activity, joint stiffness, pain, muscle weakness and disability will get worse.
CONCLUSION
In summary, muscle and movement are essential for joint health. Unfortunately, erroneous health beliefs (of the patient and health care practitioner) and poor patient management can be a barrier to exercise. As a consequence unchallenged inappropriate health beliefs lead to health behaviours that can exacerbate the problems associated with chronic rheumatic conditions. Exercise is very safe for most people, and common physical activities are an excellent way of people gaining health benefits associated with ‘formal’ exercise regimens. One of the best ways of increasing participation in regular physical activity is by participation in integrated exercise and self-management rehabilitation programmes. These enable people to appreciate, through experience, how a simple exercise programme is safe, reduces pain and improves function. In addition, these programmes use the more holistic biopsychosocial model of healthcare to challenge erroneous health beliefs, giving people active coping strategies and enhancing important psychosocial factors such as self-efficacy, self-esteem and social interaction. Ultimately, however, people need to appreciate that the benefits of simple physical activity far out-weigh the time and effort incurred.
References and further reading
ACSM. American College of Sports Medicine’s guidelines for exercise testing and prescription. Lippencott: Williams and Wilkins; 2006.
Ashworth, N.L., Chad, K.E., Harrison, E.L., et al., 2005. Home versus center based physical activity programs in older adults. Cochrane Database Syst. Rev. CD004017.
Bandura A. Self-efficacy: towards a unifying theory of behavior change. Psychol. Rev.. 1977;84:191-215.
Bearne L.M., Scott D.L., Hurley M.V. Exercise can reverse quadriceps sensorimotor dysfunction that is associated with rheumatoid arthritis without exacerbating disease activity. Rheumatology. 2002;41:157-166.
Blake D.R., Merry P., Unsworth J., et al. Hypoxic-reperfusion injury in the inflamed human joint. Lancet. 1989:289-293.
Bodenheimer T., Lorig K., Holman H., et al. Patient self-management of chronic disease in primary care. J. Am. Med. Assoc.. 2002;288:2469-2475.
Brosseau L., Pelland L., Wells G., et al. Efficacy of aerobic exercises for osteoarthritis (part II): a meta-analysis. Phys. Ther. Rev.. 2004;9:125-145.
Brosseau L., Wells G.A., Tugwell P., et al. Ottawa panel evidence-based clinical practice guidelines for therapeutic exercises and manual therapy in the management of osteoarthritis. Phys. Ther.. 2005;85:907-911.
Brouwer G.M., Van Tol A.W., Bergink A.P., et al. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis Rheum.. 2007;56:1204-1211.
Buckwalter J.A. Osteoarthritis and articular cartilage use, disuse, and abuse: experimental studies. J. Rheumatol.. 1995;43(Suppl.):13-15.
Caspersen C.J., Powell K.E., Christenson G.M. Physical activity, exercise and physical fitness: definitions and distributions for health -related research. Public Health Rep.. 1985;100:126-146.
Cochrane T., Davey R.C., Matthes Edwards S.M. Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis. Health Technol. Assess.. 2005;9:1-130.
Coulter A., Ellins J. Effectiveness of strategies for informing, educating, and involving patients. Br. Med. J.. 2007;335:24-27.
Dagfinrud H., Kvien T.K., Hagen K.B. The Cochrane review of physiotherapy interventions for ankylosing spondylitis. J. Rheumatol.. 2005;32:1899-1906.
de Jong Z., Vlieland T.P. Safety of exercise in patients with rheumatoid arthritis. Curr. Opin. Rheumatol.. 2005;17:177-182.
Dekker J., Bott B., van der Woude L.H.V., et al. Pain and disability in osteoarthritis: a review of biobehavioral mechanisms. J. Behav. Med.. 1992;15:189-214.
Devos-Comby L., Cronan T., Roesch S.C. Do exercise and self-management interventions benefit patients with osteoarthritis of the knee? A meta-analytic review. J. Rheumatol.. 2006;33:744-756.
Ekdahl C., Broman G. Muscle strength, endurance and aerobic capacity in rheumatoid arthritis: a comparative study with healthy subjects. Ann. Rheum. Dis.. 1992;51:35-40.
Epps, H., Ginnelly, L., Utley, M., et al., 2005. Is hydrotherapy costeffective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis. Health Technol. Assess. 9.
Ernst E. Complementary or alternative therapies for osteoarthritis. Nat. Clin. Pract. Rheumatol.. 2006;2:74-80.
Ettinger W.H., Burns R., Messier S.P., et al. A randomised control trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. J. Am. Med. Assoc.. 1997;277:25-31.
Fletcher G.F., Balady G.J., Amsterdam E.A., et al. Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation. 2001;104:1694-1740.
Foley A., Halbert J., Hewitt T., et al. Does hydrotherapy improve strength and physical function in patients with osteoarthritis – a randomised controlled trial comparing a gym based and a hydrotherapy based strengthening programme? Ann. Rheum. Dis.. 2003;62:1162-1167.
Fransen M., McConnell S., Bell M. Therapeutic exercise for people with OA of the hip and knee: a systematic review. J. Rheumatol.. 2002;29:1737-1745.
Fransen M., Nairn L., Winstanley J., et al. Physical activity for osteoarthritis management: a randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Care Res.. 2007;57:407-414.
Green J., McKenna F., Redfern E., et al. Home exercises are as effective as outpatient hydrotherapy for osteoarthritis of the hip. Rheumatology. 1993;32:812-815.
Griffiths C., Foster G., Ramsay J., et al. How effective are expert patient (lay led) education programmes for chronic disease? Br. Med. J.. 2007;334:1254-1256.
Hay E.M., Foster N.E., Thomas E., et al. Effectiveness of community physiotherapy and enhanced pharmacy review for knee pain in people aged over 55 presenting to primary care: pragmatic randomised trial. Br. Med. J.. 2006;333:995-998.
Holman H.R., Lorig K.R. Patient education: essential to good health care for patients with chronic arthritis. Arthritis Rheum.. 1997;40:1371-1373.
Hurley M.V. The role of muscle weakness in the pathogenesis of osteoarthritis. Rheum. Dis. Clin. North Am.. 1999;25:283-298.
Hurley M.V. Muscle dysfunction and effective rehabilitation of knee osteoarthritis: what we know and what we need to find out. Arthritis Rheum.. 2003;49:444-452.
Hurley M.V., Mitchell H.L., Walsh N. In osteoarthritis, the psychosocial benefits of exercise are as important as physiological improvements. Exerc. Sports Sci. Rev.. 2003;31:138-143.
Hurley M.V., Walsh N.E., Mitchell H.L., et al. Clinical effectiveness of “ESCAPE–knee pain” a rehabilitation programme for chronic knee pain: a cluster randomised trial. Arthritis Rheum.. 2007;57:1211-1219.
Keefe F.J., Kashikar-Zuck S., Opiteck J., et al. Pain in arthritis and musculoskeletal disorders: the role of coping skills training and exercise interventions. J. Ortho. Sports Phys. Ther.. 1996;24:279-290.
Klepper S.E. Exercise and fitness in children with arthritis: evidence of benefits for exercise and physical activity. Arthritis Care Res.. 2003;49:435-443.
Main C., Watson P. Psychological aspects of pain. Man. Ther.. 2002;4:203-215.
Mazzuca S., Weinberger M. Social support. In: Brandt K.D., Doherty M., Lohmander L., editors. Osteoarthritis. Oxford: Oxford University Press; 1998:331-338.
McAuley E. The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. J. Behav. Med.. 1992;15:65-88.
McAuley E., Lox C., Duncan T.E. Long-term maintenance of exercise, self-efficacy and physiological change in older adults. J. Gerontol. (Psycholo. Sci.). 1993;48:218-224.
McCarthy C.J., Mills P.M., Pullen R., et al. Supplementing a home exercise programme with a class-based exercise programme is more effective than home exercise alone in the treatment of knee osteoarthritis. Rheumatology. 2004;43:880-886.
Meldrum D.A.N. Lets get physical-exercise guidelines for cardiac patients. Perspect. Cardiol.. 2003:29-33.
Merry P., Williams R., Cox N., et al. Comparative intra-articular pressure dynamics in joints with acute traumatic and chronic inflammatory effusions: potential implications for hypoxic-reperfusion injury. Ann. Rheum. Dis.. 1991;50:917-920.
Minor M.A. Exercise in the treatment of osteoarthritis. Rheum. Dis. Clin. North Am.. 1999;25:397-415.
Munneke M., de Jone, Zwinderman A.H., et al. Effect of a high-intensity weight-bearing exercise program on radiologic damage progression of the large joints in subgroups of patients with rheumatoid arthritis. Arthritis Care Res.. 2005;53:410-417.
Newman P.S., Steed L., Mulligan K. Self-management interventions for chronic illness. The Lancet. 2004;364:1523.
NICE. Four commonly used methods to increase physical activity: brief interventions in primary care, exercise referral schemes, pedometers and community- based exercise programmes for walking and cycling. London: National Institute for Health and Clinical Excellence; 2006. http://www.nice.org.uk/ accessed January 2009
Nordemar R., Ekblom B., Zachrisson, et al. Physical training in rheumatoid arthritis: a controlled long- term study. Scand. J. Rheumatol.. 1981;10:17-30.
Pate R.R., Pratt M., Blair S.N., et al. Physical activity and public health. A recommendation from the centers for disease control and prevention and the American College of Sports Medicine. J. Am. Med. Assoc.. 1995;273:402-407.
Patrick D.L., Ramsey S.D., Spencer A.C., et al. Economic evaluation of aquatic exercise for persons with osteoarthritis. Med. Care. 2001;39:413-424.
Pelland L., Brosseau L., Wells G., et al. Efficacy of strengthening exercises for osteoarthritis (part I): a meta analysis. Phys. Ther. Rev.. 2004;9:77-108.
Pendleton A., Arden N., Dougados M., et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis.. 2000;59:936-944.
Rejeski W.J., Ettigner W.H., Martin K., et al. Treating disability in knee osteoarthritis with exercise: a central role for self-efficacy and pain. Arthritis Care Res.. 1998;11:94-101.
Roddy E., Zhang W., Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann. Rheum. Dis.. 2005;64:544-548.
Stenstrom C., Lindell B., Swanberg P., et al. Intensive dynamic training in water for rheumatoid arthritis functional class II: a long term study or effects. Scand. J. Rheumatol.. 1991;20:358-365.
Stenstrom C.H. Dynamic Therapeutic Exercise in Rheumatoid Arthritis. Stockholm: Karolinska Institute; 1993.
Stenström C.H., Minor M.A. Evidence for the benefit of aerobic and strengthening exercise in rheumatoid arthritis. Arthritis Care Res.. 2003;49:428-434.
Superuio-Cabuslay E., Ward M.M., Lorig K.R. Patient education interventions in osteoarthritis and rheumatoid arthritis: a meta-analytic comparison with nonsteroidal antiinflammatory drug treatment. Arthritis Care Res.. 1996;9:292-301.
Takken T., van der Net J., Kuis W., et al. Aquatic fitness training for children with juvenile idiopathic arthritis. Rheumatology. 2003;42:1408-1414.
Thomas K.S., Muir K.R., Docherty M., et al. Home based exercise programme for knee pain and knee osteoarthritis: randomised controlled trial. Br. Med. J.. 2002;325:752-756.
Turk D.C. Biopsychosocial perspectives on chronic pain. In: Gatchel R.J., Turk D.C., editors. Psychological Approaches to Pain Management: A Practitioner’s Handbook. New York: Guildford Press; 1996:3-32.
Turner J.A., Jensen M.P., Romano J.M. Do beliefs, coping and catastrophizing independently predict functioning in patients with chronic pain? Pain. 2000;85:115-125.
van Baar M.E., Assendelft W.J.J., Dekker J., et al. Effectiveness of exercise therapy in patients with osteoarthritis of the hip and knee. A systematic review of randomised clinical trials. Arthritis Rheum.. 1999;42:1361-1369.
van den Ende C.H.M., Vliet Vlieland T.P.M., Munneke M.W., et al. Dynamic exercise therapy in rheumatic arthritis: a systematic review. Br. J. Rheumatol.. 1998;37:677-687.
van Tulder M., Malmivaara A., Esmail R., et al. Exercise therapy for low back pain. A systematic review within the framework of the Cochrane Collaboration Back review Group. Spine. 2002;25:2784-2796.
Verhagen, A.P., Bierma-Zeinstra, S.M.A., Cardoso, J.R., et al., 2004. Balneotherapy for rheumatoid arthritis. Cochrane Database Syst. Rev.
Verhagen A.P., de Vet H.C.W., de Bie R.A., et al. Taking Baths: the efficacy of balneotherapy in patients with arthritis. A systematic review. J. Rheumatol.. 1997;24:1964-1971.
Walsh N.E., Hurley M.V. Management of knee osteoarthritis in physiotherapy outpatient departments in Great Britain and Northern Ireland. Rheumatology. 2005;44(Suppl. 1):383.
Warsi A., LaValley M.P., Wang P.S., et al. Arthritis self-management education programs: a meta-analysis of the effect on pain and disability. Arthritis Rheum.. 2003;48:2207-2213.
Whittle M. Generation and attenuation of transient impulsive forces beneath the foot: a review. Gait Posture. 1999;10:264-275.
Zochling J., van der Heijde D., Dougados M., et al. Current evidence for the management of ankylosing spondylitis: a systematic literature review for the ASAS/EULAR management recommendations in ankylosing spondylitis. Ann. Rheum. Dis.. 2006;65:423-432.
PATIENT INFORMATION SHEET 7.1
EXERCISING SAFELY
Controlled physical activity/exercise has many health benefits and few dangers, and very few people are too old or infirm to benefit, but remember the following: