Chapter 10 Joint protection and fatigue management
INTRODUCTION
Joint protection and fatigue management address the priority concerns of people with arthritis: pain, fatigue and hand and finger function (Heiburg & Kvien 2002, Hewlett et al 2005). Joint protection underlies all rehabilitation of people whose joints are at risk from arthritis (Cordery & Rocchi 1998), yet fatigue management is often inadequately addressed (Hewlett et al 2005). To be effective, both require people with arthritis changing habits and routines. Teaching facts can be done quickly but enabling long-term behavioural change requires greater input. This chapter discusses what joint protection and fatigue management strategies are, practical applications, evidence for effectiveness, how to help people change and outcome measures.
JOINT PROTECTION
Joint protection developed from understanding pathophysiology of joint diseases, joint biomechanics, forces applied during activity and how these contribute to the development of deformity (Brattstrom 1987, Chamberlain et al 1984, Cordery 1965, Cordery & Rocchi 1998, Melvin 1989). The aims of joint protection in inflammatory arthritis are to:
For people with osteoarthritis (OA) the aims are to:
Joint protection is an active coping strategy to improve daily tasks and role performance helping reduce frustration arising from difficulties with these, enhance perceptions of control and improve psychological status (Hammond et al 1999). Much of joint protection literature focuses on hand problems in rheumatoid arthritis (RA), so this is explored in detail in this chapter but strategies are similarly applicable in other conditions and for other joints.
PATHOPHYSIOLOGY OF HAND DEFORMITIES AND BIOMECHANICAL BASIS OF JOINT PROTECTION
Considering why deformities develop with RA helps in understanding how joint protection may contribute to preserving joint integrity. Deformities develop due to a combination of persistent synovitis disrupting joint structures and both normal and abnormal forces passing over joints (Adams et al 2005, Flatt 1995). In the longer-term, disruptions to bony architecture from erosions and osteophytes can further alter joint mechanics at any joint.
The wrist
The ulnar side is an early inflammation site. Triangular fibrocartilage disruption allows the proximal carpal row to rotate ulnarward. The distal row compensates by sliding radially, producing a radially deviating wrist. Laxity of the radio-ulnar ligament permits rotation of the radius and ulna, with the ulnar styloid becoming more prominent. Extensor carpi ulnaris can become displaced volarly, passing beneath the wrist joint axis, exerting a flexor pull. This, combined with wrist ligament laxity, and the natural volar incline of the distal radius, increases risk of wrist volar subluxation.
The metacarpophalangeal (MCP) joints
Persistent synovitis can weaken MCP collateral ligaments, volar plates and dorsal hoods leading to joint instability. The finger extensors can then slip volarly and ulnarly, increasingly acting as weak flexors. Normal MCP joint features contribute to ulnar deviation once joint structure is disrupted. These include: the flexor tendons approach the index and middle fingers from an ulnar direction exerting a significant ulnar torque; the metacarpal head anatomically predisposes to tendons slipping ulnarward; and the ulnar interossii exert a stronger pull than the radial (see Fig. 16.3 Ch 16).
The interphalangeal (IP) joints
Persistent synovitis can disrupt positioning of the extensor tendon central slip and lateral bands allowing Boutonniere deformity to develop. MCP joint inflammation can cause protective spasms in the interossii causing MCP flexion during finger extension (the intrinsic plus position), contributing to Boutonniere and swan-neck deformity development (see Fig. 16.4 Ch 16).
JOINT PROTECTION AND THE HANDS
Anatomical disruptions, combined with normal daily hand use patterns, can promote deformity. Power grip requires MCP ulnar deviation, especially in the 4th and 5th fingers. During lifting, external pressures in a volar or longitudinal direction increase strain on weakened wrist ligaments. Strong pinch grips increase intrinsic muscle pull promoting imbalance at the IP joints. Hand joint protection in RA thus focuses on changing movement patterns to limit: strong grips, twisting movements and sustained grips at the MCPs (reducing MCP ulnar forces); lifting heavy objects and sustained wrist radial positioning (reducing wrist volar and radial forces); and tight, prolonged key, tripod and pinch grips (reducing volar and ulnar forces on the MCP and IP joints).
In the early stages, many with RA are all too aware of hand function problems: dropping items, weaker grip, reduced dexterity and frustration from activities taking longer and being more painful. However, early signs of RA can be subtle (see Fig. 10.1). Whilst swelling may be noticeable, many do not notice a more prominent ulnar styloid, slight wrist radial deviation and 5th MCP ulnar deviation, early correctable finger deformities, nor gradual loss of movement. In early RA average losses are 20° wrist extension, 30° wrist flexion, 15° MCP flexion and only 40% of normal power and pinch grip strength (Hammond et al 2000). A third can develop hand deformities by two years (Eberhardt et al 1990). This suggests joint protection and hand exercises should be provided early and effectively to limit decline (Fig. 16.4 Ch 16).

Figure 10.1 The hand in early rheumatoid arthritis showing swelling of the metacarpophalangeal joints and proximal interphalangeal joints.
With permission from: Goldenburg DL 2003 Clinical features of rheumatoid arthritis. In: Hochberg MC et al (eds.) Rheumatology 3rd edn, Elsevier, London. Fig. 68.6 p 770.
JOINT PROTECTION PRINCIPLES
Principles taught are shown in Box 10.1 and in Chapter 16 (Box 16.4). Focus on priority messages in plain English. For example, for the hands:
BOX 10.1 Joint protection and energy conservation principles
Joint protection
Joint protection principles are reviewed in Palmer and Simons (1991).
JOINT PROTECTION STRATEGIES
Joint protection is the application of ergonomics to everyday activities, work and leisure. Many people find ways of reducing pain and fatigue in daily activities through trial and error, but this takes time. Joint protection and energy conservation education should apply a systematic approach to changing habits, finding new solutions and speeding up change. Strategies include:
Altering working methods
E.g. altering movement patterns during tasks; more efficient positioning, e.g. sitting on a perch stool to iron; and reducing forces from lifting, pushing/pulling, stretching/reaching, carrying (Figs 10.2-10.5).




Restructuring activities
E.g. reordering task sequences within these, eliminating unnecessary steps to increase efficiency.
Using assistive technology
Reducing effort required performing activities, e.g. jar openers, dycem matting, key turners, easy-grip scissors, walking aids (see Ch. 9, Fig. 9.3).
Altering the environment
E.g. bringing objects within the person’s reach envelope; reorganizing work areas to streamline activity processes; raising or lowering working heights.
Selecting appropriate product designs (universal designs)
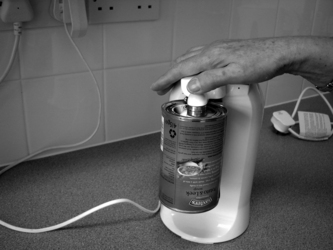
E.g. equipment with non-slip handles (e.g. irons, screwdrivers, Good Grip kitchen equipment); electric alternatives (e.g. can openers, see Fig. 10.6); lightweight models (e.g. hand held vacuum cleaners for stairs); labour saving equipment (e.g. tumble drier, plug pulls, see Fig. 10.7); lever taps. Further details on assistive technology and environmental adaptation can be found in Chapter 9.

FATIGUE MANAGEMENT
Fatigue increases pain, cognitive disturbance (e.g. reduced concentration) and psychological effects (e.g. increased stress, low mood). There are many possible causes (see Box 10.2) and multiple solutions are needed. Helping people identify potential causes helps them prioritise changes. Practical strategies include:
ENERGY CONSERVATION
This aims to reduce fatigue, pain and increase activity tolerance to achieve overall greater productivity and quality of life without exacerbating pain. Energy conservation principles are included in Box 10.1 and Chapter 16 (Box 16.4). Usually taught alongside joint protection, practical strategies include:
Pacing
This significantly improves duration of physical activity (Furst et al 1987) and includes:
Taking rest breaks
Many find resting against their personal standards, feeling this is ‘giving in’ and preferring to remain busy. Explain rest ‘recharges the batteries’ to keep going for longer. Recommend: regular short rest breaks, e.g. 3–5 minutes every 30–45 minutes sitting and relaxing joints; and/or ‘microbreaks’, i.e. 30 seconds every 5–10 minutes stretching and relaxing those joints and muscles being most used. Many express concerns that taking rests is seen as ‘slacking’ by managers at work, so microbreaks can be more achievable. Rest strategies are recommended to all workers by the Health and Safety Executive (2005) to reduce injury as they allow muscle recovery time. Developing habits is helped by e.g. setting a kitchen timer or mobile phone to ring/vibrate every 30 minutes; screen prompts every 5–10 minutes for microbreaks.
Balancing activities
Alternating heavy, medium and light activities during the day and week. Many do too much on ‘good days’ and suffer the consequences several days after (the boom and bust cycle). Breaking this habit requires attitudinal change. Many fear that, if they don’t get things done, they won’t meet work demands and family/home responsibilities. Activity diaries are useful in helping people identify and evaluate activity patterns (see Arthritis Research Campaign (2007) for an example).
Positioning
Planning
This includes using work simplification strategies. Can tasks be organised more efficiently? Can storage areas be more organised at home and work? Can certain tasks be avoided or eliminated, performed using different equipment, methods, or less often. Or as a final solution, can someone else help? Offering to reciprocate doing another activity or function for that person helps reduce the feelings of obligation or dependency.
Problem solving
Teach task analysis; select an activity identified as problematic by the person; review each task in turn to identify if a change is beneficial or necessary; identify a range of possible solutions or alternative methods for each task; try these; determine which works best; then practice.
SLEEP HYGIENE
A sleep diary can be helpful (see Useful Websites). Solutions depend on the problems and can include: using more supportive mattresses and pillows; establishing a regular bedtime and evening routine, e.g. relaxation, soothing music, warm bath or shower, gentle exercise; avoiding stimulants 2–3 hours before bedtime (tea, coffee, caffeinated soft drinks, alcohol, smoking); reducing stimuli in the bedroom, e.g. avoiding television and computer use, turning clock faces away, black-out curtains, muted colour schemes.
COGNITIVE INTERVENTIONS
Evaluate potential common psychosocial causes of fatigue: loss of valued activities, poor self-efficacy, anxiety and problematic social support (Katz &Yelin 1995, Lorish et al 1991, Riemsma et al 1998, Wolfe et al 1996). Cognitive approaches used by OTs include: stress management (including managing automatic negative thinking, relaxation); mindfulness therapy; goal-setting to increase valued activity engagement (e.g. paid/unpaid work, leisure, social activities); assertiveness and communication training; liaising with family and carers. Stress and pain management can help improve self-efficacy, coping and perceptions of control (Rhee et al 2002) and referral for individually tailored cognitive-behavioural therapy is beneficial for those with more severe problems (Evers et al 2002).
PHYSICAL INTERVENTIONS
Regular physical activity and exercise reduce aches, pain and fatigue and improve sleep quality. Evaluate current level of physical activity and discuss benefits of and overcoming barriers to exercise (see Ch. 7). Recommend simple walking programmes (see Useful Websites) and referral to physiotherapy as necessary.
MEDICAL INTERVENTIONS
Good pain control can significantly reduce fatigue (Pollard et al 2006). Encourage taking analgaesia and prescribed medication effectively (see Ch. 15). Whilst providing specific medication advice is outside the professional competency of most therapists, explain the benefits of medication, mode of action and that timing or dosage may be improved. Recommend discussing medication with the rheumatology nurse (via the Rheumatology department’s telephone advice line) or at their next Consultant, GP or rheumatology nurse appointment.
WHAT JOINT PROTECTION AND FATIGUE MANAGEMENT ARE NOT
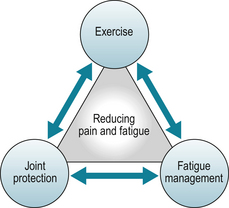
Joint protection is often misperceived as meaning stopping activities, keeping joints immobile and excess rest. It can be seen as ‘giving in’. Many find it confusing that the OT tells people to ‘protect joints’ (incorrectly perceived as limiting movement and activity) whilst the physiotherapist tells them to exercise as much as possible (incorrectly perceived as meaning all types of exercise causing pain and strain). These seem opposing messages. Rheumatology OTs and physiotherapists must give similar explanations to ensure patients are not confused. Emphasise ‘looking after joints’ means adapting activities and movements and reducing strain or force on joints. Exercise means being more physically active as well as stretching, strengthening and low-impact aerobic exercises. Exercise also applies joint protection principles, e.g. avoiding twisting (torque) forces or excess shock (e.g. high impact aerobics, wearing thin soled shoes whilst walking) and helps support joints so they are better able to tolerate forces that cannot be reduced. Fatigue management increases energy to be more physically active and do more enjoyable things in life. The combined benefits of all three help a more meaningful life to be lived (see Fig. 10.8).
HAND EXERCISES
Joint protection and fatigue management are normally provided alongside a) assessment for splints (see Ch. 12) and b) hand exercises, as joint protection principles (Box 10.1) include maintaining muscle strength and range of movement. Maintenance hand exercise programmes should be easily integrated into normal daily routine, and help maintain all hand grips, combining strengthening and stretching (Hammond 2004, Hoenig et al 1993, O’Brien et al 2006). Strengthening hand muscles aids joint stability by compensating for ligamentous laxity. Keep the number of exercises to a minimum to ensure they can be achieved but ensure plenty of repetition. Lengthy, complex, hand exercise regimens are unlikely to be followed long-term. A simple home programme is described in Box 10.3.
BOX 10.3 A home hand exercise programme
Find a comfortable position: support the arm to avoid shoulder aching. Do one hand at a time for best movement. Warm-up for each exercise:
 “Start with three slow repetitions: first about 70% as far as you can go, the second 90% and the third as far as you can comfortably go feeling a gentle pull, but not pain.” Three days the first week, gradually increasing repetitions and number of days over 4–8 weeks, to 10 repetitions most/every day.
“Start with three slow repetitions: first about 70% as far as you can go, the second 90% and the third as far as you can comfortably go feeling a gentle pull, but not pain.” Three days the first week, gradually increasing repetitions and number of days over 4–8 weeks, to 10 repetitions most/every day.HOW IS JOINT PROTECTION AND FATIGUE MANAGEMENT EDUCATION COMMONLY PROVIDED?
Education averages 1.5 hours over two appointments but is often less due to time constraints. Usual content is: education about the condition; how joints are affected by it; joint protection principles; demonstrations with short (e.g. 15–30 minutes) practice of common joint protection methods, e.g. making a cup of tea, rising from a chair; and discussing solutions to individuals’ problems, supported by a self-help booklet (Hammond 1997). In general, behavioural approaches are not used. This is still usual practice but is it effective?
EVIDENCE FOR JOINT PROTECTION AND ENERGY CONSERVATION EFFECTIVENESS
USUAL JOINT PROTECTION EDUCATION
Barry et al (1994) evaluated in a randomized controlled trial (RCT) 1 hour of individual education, similar to the ‘usual’ content above, and identified improvement in joint protection knowledge. Two trials have evaluated usual joint protection education for 2.5 hours (as part of an 8 hour standard arthritis education programme). These also improved knowledge but not behaviour (Hammond & Freeman 2001, Hammond & Lincoln 1999a). Interviews identified only 25% of participants considered they had made changes (Hammond & Lincoln 1999a).
However, analysis of hand use patterns before and after education showed many cited changes were performed beforehand. Education raised awareness of changes already subconsciously made. For others, barriers to change were:
Interventions need to address these barriers to be effective.
BEHAVIOURAL JOINT PROTECTION EDUCATION
In contrast, structured group programmes, of 8–16 hours duration, emphasising active learning, problem solving, behavioural approaches, frequent practice and home programmes have been proven effective.
An RCT with people with early RA (n = 127) compared an 8 hour cognitive-behavioural approach joint protection programme with a standard arthritis education programme (including 2.5 hours of usual joint protection, not using behavioural approaches). At 1 year the behavioural group, compared to the standard group, significantly improved the use of joint protection, improved functional ability and reduced hand pain, general pain and early morning stiffness (Hammond & Freeman 2001). Benefits continued at 4 years and the behavioral group had fewer hand deformities (Hammond & Freeman 2004). Timing of education needs careful consideration as there is evidence it can be provided both too early and too late (Hammond 2004). Other studies in patients with established RA have also shown benefits:
COMBINED JOINT PROTECTION, FATIGUE MANAGEMENT AND EXERCISE
RCTs in people with established RA have resulted in significant improvements in pain, functional and physical ability, self-efficacy and psychological status (Hammond et al 2008, Masiero et al 2007). An RCT in people with hand OA identified significant improvements at three months in grip strength and self-perceived hand function, in comparison to a control group receiving education about OA (Stamm et al 2002).
TEACHING JOINT PROTECTION AND FATIGUE MANAGEMENT
Facilitating behaviour change
Many attempts to change behaviour by making a change in knowledge (traditional handouts, demonstration, discussions) have been largely unsuccessful. Using cognitive, behavioural and learning theories to develop teaching programmes have been effective.
Groups provide a powerful modelling force for enabling joint protection behaviour change, enhancing self-efficacy (see Ch. 6) and increasing problem-solving activity with others facing similar difficulties. Group education can be more cost-effective. Treating six patients individually for 2 hours each (i.e. an ineffective level of education) takes 12 hours. Treating six patients in a group joint protection programme (e.g. Hammond & Freeman 2001, Hammond et al 2008) takes 12 hours and is proven effective. Therapists need to change services to deliver evidence-based practice.
Integrating behavioural approaches
The self-management cognitive-behaviour therapy approach is based on self-regulation and social cognitive theory (Kanfer & Gaelick 1989). This recommends four stages: creating a working relationship; creating and maintaining the motivation for change; developing and executing a behavioural change programme (including home programmes); and providing support to promote change and prevent relapse. (For further details see Hammond 2003).
Getting started - motivating for change and initial explanations
People must perceive joint protection and fatigue management are relevant now before they are likely to change, i.e. to be in contemplation (Prochaska & DiClemente 1992, Prochaska 2008, see Ch. 6). To help this attitudinal shift to contemplation, ask whether activities people have to do, need to do and enjoy doing are affected by arthritis and the causes (e.g. pain, fatigue, stiffness, frustration) and concerns for the future. This helps focus on the impact of arthritis and thus on contemplating the pros and cons of change (Prochaska 2008). Do they want to reduce these causes? Explain joint protection and fatigue management are proven effective and discuss the benefits (pros) that can be gained (i.e. reduced pain and fatigue, staying independent, better function, less frustration, actively helping manage symptoms, better physical and psychological wellbeing). Allow time for the person to discuss their cons (e.g. concerns about negative self-image, embarrassment, not wanting to use assistive devices, wanting to remain as they are, not wanting to take the time to change, concerns joint protection is slower and more difficult) (Niedermann et al, 2009a, in review). If they have no pain or difficulties currently, joint protection is not relevant and they are unlikely to shift from precontemplation. Explain the education available, provide written information and discharge. Education too early is unlikely to be sufficiently recalled when applicable later so ensure mechanisms are in place for people to self-refer (Hammond 2004).
If they do have pain or difficulties and seem to be moving through the decisional balance stage into contemplation or preparation, then:
At the next session, discuss their attitudes to joint protection and ask if they are ready to commit to education. Have the pros now outweighed the cons for them? (Niedermann et al 2009a, in review). Learning facts is easy, but changing habits is harder. To shift from preparation to action, recommend attending a group joint protection programme (e.g. the Looking After your Joints Programme) (Hammond & Freeman 2001) or if, individual sessions, at least three further sessions as fewer are ineffective (Hammond & Freeman 2001).
Promoting change – practise, goal setting and home programmes
During practical training, apply the educational and skills training approaches described in Chapter 6. Everyday movement patterns are automatic movements using open-loop motor control, i.e. pre-programmed, often from childhood. Change requires shifting to closed-loop motor control whilst learning new movement patterns. Start with part-blocked practice, i.e. single tasks repetitively performed. This can be an early home programme activity. Each week practice with progressively more complex activities, e.g. a hot drink, then snack meal then a full meal. If performance errors are noted delay feedback initially (e.g. 3 seconds) to enable the person to identify and problem solve their own errors. Teach mental rehearsal to improve skills and practice opportunities. Further details on motor learning can be found in Ezekiel et al 2000, Lehto et al 2000, Marley et al 2000 and Wishart et al 2000.
Goal setting helps people commit to weekly home practice. Each session ask them to state and, preferably, write down an action plan (see Box 10.4). Goals should be determined by the person: and specify what, how often and how much (see Ch. 6). Encourage identifying rewards contingent on achieving their plan. Pushing people to practise too much is unlikely to be successful. Use a 10 point scale (see Box 10.4): how confident are they to complete each task on a scale of 0-10? Then the whole plan? If the answer is less than 7, ask them to revise their goal/plan to be more achievable.

At the start of the each session, always review goal progress. The home programme is an important, integral part of treatment. Failure should not be criticised. Rather, identify barriers and jointly problem-solve overcoming these (see also Ch. 6., Box 6.3). Finally, schedule a follow-up appointment 6–8 weeks after education finishes to review progress and promote continuing independently setting goals for longer term change.
OUTCOME MEASURES
In addition to measures described in Chapter 4, specific measures include:
KNOWLEDGE
The Joint Protection Knowledge Assessment (Hammond & Lincoln 1999b): 20 multiple choice items assessing ability to identify best methods. Some arthritis knowledge questionnaires also include joint protection and fatigue management items (see Ch.6).
SELF-EFFICACY
The Joint Protection Self-Efficacy Scale (Niedermann et al 2009b, in review): 10 items assessing confidence in caring for hand and finger joints, and applying joint protection methods. The RA Self-Efficacy Scale (Hewlett et al 2001) includes questions about confidence in using joint protection and fatigue management strategies.
ADHERENCE
Direct observation
The Joint Protection Behaviour Assessment (Hammond & Lincoln 1999c): analyses hand movements whilst making a hot drink and snack meal. Performance is recorded then analyzed, using an assessment manual, coding for correct, partially correct or incorrect movements in 20 tasks (e.g. lift a kettle). A 10-item version is equally reliable (Klompenhouwer et al 2000) and skilled assessors can do this without recording.
IMPACT ON FUNCTIONAL AND HEALTH STATUS
Relevant scales can be found in Chapters 4, 6 and 16 (Box 16.3). More specific questionnaires are:
The Evaluation of Daily Activities Questionnaire (Nordenskiold et al 1996, 1998) evaluating functional ability with and without assistive devices/altered working methods. This is used to evaluate joint protection and in clinical practice in Scandinavia. A UK version is in development.
Fatigue: the Multidimensional Assessment of Fatigue: 16 questions concerning the quantity, degree, distress, impact, and timing of fatigue (Tack 1991). The Vitality subscale of the SF-36 comprises four items (full of life, energy, worn out, tired) with six responses from ‘all of the time’ to ‘none of the time’ (Ware & Sherbourne 1992).
CONCLUSION
Joint protection and fatigue management are effective if taught effectively. How education is provided makes a significant difference to whether patients with rheumatological musculoskeletal conditions benefit. Educational, cognitive and behavioural approaches are significantly more effective than traditional techniques and should be provided (NICE 2009). The whole team needs to support people in committing to make the time to learn how to successfully apply these effective self-management strategies.
Conduct a task analysis of two activities identifying the separate components and movements used for each task.Joint protection and fatigue
http:/www.arthritis.org/preventing-arthritis-pain.php/ (accessed March 2009).
Tips for Living Well section: joint protection and fatigue management ideas accessed March 2009
Arthritis information for patients: booklets on ‘Looking after your joints when you have arthritis,’ ‘Gardening with arthritis’, ‘Fatigue and arthritis’ accessed March 2009.
http:/campus.dyc.edu/arthritis/homepage.htm/ (accessed March 2009).
http:/osteoarthritis.about.com/od/joint/protection/Joint_Protection.htm/ (accessed March 2009).
http:/www.mayoclinic.com/health/joint-protection/AR00027/ (accessed March 2009).
Walking plan
http:/www.arthritistoday.org/fitness/walking/tips-andstrategies/walking-plan.php/ (accessed March 2009).
Sleep information and diary
http:/www.patient.co.uk/leaflets/sleep_diary.htm/ (accessed March 2009).
http:/www.iboro.ac.uk/departments/hu/groups/csru/pdf/Daily%20Sleep%Diary+Hygiene.pdf/ (accessed March 2009).
References and further reading
Adams J., Hammond A., Burridge J., et al. Static orthoses in the prevention of hand dysfunction in rheumatoid arthritis: a review of the literature. Musculoskeletal Care. 2005;3(2):85-101.
Arthritis Research Campaign. Looking After Your Joints when you have Arthritis. Chesterfield: Arthritis Research Campaign; 2007. www.arc.org.uk
Barry M.A., Purser J., Hazleman R., et al. Effect of energy conservation and joint protection education in rheumatoid arthritis. Br. J. Rheumatol.. 1994;33:1171-1174.
Brattstrom M. Joint Protection and Rehabilitation in Chronic Rheumatic Diseases, third ed. London: Wolfe Medical; 1987.
Chamberlain M.A., Ellis M., Hughes D. Joint protection. Clin. Rheum. Dis. 1984;10(3):727-743.
College of Occupational Therapists. Occupational Therapy Clinical Guidelines for Rheumatology: Joint Protection and Energy Conservation. London: College of Occupational Therapists; 2003.
Cordery J.C. Joint protection; a responsibility of the occupational therapist. Am. J. Occup. Ther.. 1965;19:285-294.
Cordery J., Rocchi M. Joint protection and fatigue management. Melvin J., Jensen G., editors. Rheumatologic Rehabilitation vol 1: Assessment and Management. . Bethesda, MD:American Occupational Therapy Association. 1998.
Eberhardt K.B., Rydgren L.C., Pettersson H., et al. Early rheumatoid arthritis-onset, course and outcome over two years. Rheumatol. Int.. 1990;10:135-142.
Evers A.W., Kraaimaat F.W., van Riel P.L., et al. Tailored cognitive-behavioral therapy in early rheumatoid arthritis for patients at risk: a randomized controlled trial. Pain. 2002;100(1–2):141-153.
Ezekiel H.J., Lehto N.K., Marley T.L., et al. Application of motor learning principles: the physiotherapy client as a problem-solver. III augmented feedback. Physiother. Can.. 2000;53(1):33-39.
Flatt A. The Care of the Arthritis Hand, fifth ed. St Louis: Quality Medical Publishing; 1995.
Furst G.P., Gerber L.H., Smith C.C., et al. A program for improving energy conservation behaviours in adults with rheumatoid arthritis. Am. J. Occup. Ther.. 1987;41(2):102-111.
Hammond A. Joint protection education: what are we doing? Br. J. Occup. Ther.. 1997;60(9):401-406.
Hammond A. Patient education in arthritis: helping people change. Musculoskeletal Care. 2003;1(2):84-97.
Hammond, A., 2004. What is the role of the occupational therapist? In: Sambrook, P., March, L. (Eds.), How to Manage Chronic Musculoskeletal Conditions. Best Pract. Res. Cl. Rheumatol. 18 (4), 491–505.
Hammond A., Bryan J., Hardy A. Effects of a modular behavioural arthritis education programme: a pragmatic parallel group randomized controlled trial. Rheumatology. 2008;47(11):1712-1718.
Hammond A., Freeman K. One year outcomes of a randomised controlled trial of an educational-behavioural joint protection programme for people with rheumatoid arthritis. Rheumatology. 2001;40:1044-1051.
Hammond A., Freeman K. The long term outcomes from a randomised controlled trial of an educational-behavioural joint protection programme for people with rheumatoid arthritis. Clin. Rehabil.. 2004;18:520-528.
Hammond A., Kidao R., Young A. Hand impairment and function in early rheumatoid arthritis. Arthritis Rheum.. 2000;43(Suppl. 9):S285.
Hammond A., Lincoln N. Effect of a joint protection programme for people with rheumatoid arthritis. Clin. Rehabil.. 1999;13:392-400.
Hammond A., Lincoln N. The joint protection knowledge assessment: reliability and validity. Br. J. Occup. Ther.. 1999;62(3):117-122.
Hammond A., Lincoln N. Development of the joint protection behaviour assessment. Arthritis Care Res.. 1999;12(3):200-207.
Hammond A., Lincoln N., Sutcliffe L. A crossover trial evaluating an educational-behavioural joint protection programme for people with rheumatoid arthritis. Patient Educ. Couns.. 1999;37:19-32.
Health and Safety Executive, 2005. Aching arms (or RSI) in small businesses: is ill health due to upper limb disorders a problem in your workplace? http://www.hse.gov.uk/pubns/indg171.pdf/ (accessed 10.3.09.).
Heiburg T., Kvien T. Preferences for improved health examined in 1,024 patients with rheumatoid arthritis: Pain has highest priority. Arthritis Rheum.. 2002;47(4):391-397.
Hewlett S., Cockshott Z., Kirwan J., et al. Development and validation of a self-efficacy scale for use in British patients with rheumatoid arthritis (RASE). Rheumatology. 2001;40:1221-1230.
Hewlett S., Cockshott Z., Byron M., et al. Patients’ perceptions of fatigue in rheumatoid arthritis: overwhelming, uncontrollable, ignored. Arthritis Care Res.. 2005;53(5):697-702.
Hoenig H., Groff G., Pratt K., et al. A randomized controlled trial of home exercise on the rheumatoid hand. J. Rheumatol.. 1993;20:785-789.
Kanfer FH., Gaelick L. Self management methods. In: Kanfer F.H., Goldstein A.P., editors. Helping People Change: A Textbook of Methods. third ed. New York: Pergamon Press; 1989:283-345.
Katz P.P., Yelin E.H. The development of depressive symptoms among women with rheumatoid arthritis. Arthritis Rheum.. 1995;38:49-56.
Klompenhouwer P., Lysack C., Dijkers M., et al. The joint protection behaviour assessment: a reliability study. Am. J. Occup. Ther.. 2000;54(5):516-524.
Lehto N.K., Marley T.L., Ezekiel H.J., et al. Application of motor learning principles: the physiotherapy client as a problem-solver. IV. Future directions. Physiother. Can.. 2000;53(2):109-114.
Lorish C.D., Abraham N., Austin J., et al. Disease and psychosocial factors related to physical functioning in rheumatoid arthritis. J. Rheumatol.. 1991;18:1150-1157.
Marley T.L., Ezekiel H.J., Lehto N.K., et al. Application of motor learning principles: the physiotherapy client as a problem-solver. II. Scheduling practice. Physiother. Can.. 2000;52(4):315-320.
Masiero S., Boniolo A., Wassermann L., et al. Effects of an educational-behavioural joint protection program on people with moderate to severe rheumatoid arthritis: a randomized controlled trial. Clin. Rheumatol.. 2007;26:2043-2050.
Melvin J.L. Rheumatic Disease in the Adult and Child: Occupational Therapy and Rehabilitation, third ed. Philadelphia: FA Davis; 1989.
NICE (National Institute of Clinical Excellence), 2009. Ch. 6.3. Occupational Therapy. In: Rheumatoid arthritis: national clinical guideline for management and treatment in adults. Royal College of Physicians, London,pp. 87–94.
Niedermann, K., 2009a. Perceived Pros and Cons of joint protection among people with rheumatoid arthritis and occupational therapists (in review).
Niedermann, K., Forster, A., Ciurea, A., et al., 2009b Development and psychometric properties of a joint protection self-efficacy scale (JP-SES) for people with rheumatoid arthritis (in review).
Nordenskiold U. Evaluation of assistive devices after a course of joint protection. Int. J. Technol. Assess. Health Care. 1994;10(2):293-304.
Nordenskiold U., Grimby G., Hedberg M., et al. The structure of an instrument for assessing the effect of assistive devices and altered working methods in women with rheumatoid arthritis. Arthritis Care Res.. 1996;9:21-30.
Nordenskiold U., Grimby G., Dahlin-Ivanoff S. Questionnaire to evaluate effects of assistive devices and altered working methods in women with rheumatoid arthritis. Clin. Rheumatol.. 1998;17:6-16.
O’Brien A.V., Jones P., Mullis R., et al. Conservative hand therapy treatments in rheumatoid arthritis. A randomised controlled trial. Rheumatology. 2006;45(5):577-583.
Palmer P., Simons J. Joint protection: a critical review. Br. J. Occup. Ther.. 1991;54:453-458.
Pollard L.C., Choy E.H., Gonzalez J., et al. Fatigue in rheumatoid arthritis reflects pain, not disease activity. Rheumatology. 2006;45(7):885-889.
Prochaska J.O., DiClemente C.C. Stages of change in the modification of problem behaviours. In: Hersen M., Eisler R.M., Miller P.M., editors. Progress in Behaviour Modification. Champaign, IL: Sycamore Press, 1992.
Prochaska J.O. Decision making in the transtheoretical model of behaviour change. Med. Decis. Making. 2008;28(6):845-849.
Rhee S.H., Parker J.C., Smarr K.L., et al. Stress management in rheumatoid arthritis: what is the underlying mechanism? Arthritis Care Res.. 2002;13(6):435-442.
Riemsma R.P., Rasker J.J., Taal E., et al. Fatigue in rheumatoid arthritis: the role of self-efficacy and problematic social support. Br. J. Rheumatol.. 1998;37:1042-1047.
Stamm T., Machold K.P., Smolen J.S. Joint protection and home hand exercises improve hand function in patients with hand osteoarthritis: a randomized controlled trial. Arthritis Care Res.. 2002;47:44-49.
Tack, B.B., 1991. Dimensions and Correlates of Fatigue in Older Adults with Rheumatoid Arthritis [dissertation]. University of California, San Francisco Assessment available at http://www.son.washington.edu/research/maf/ (accessed 12.2.09.).
Ware J.E.Jr, Sherbourne C.D. The MOS 36-Item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care. 1992;30:473-483.
Wishart L.R., Lee T.D., Ezekiel H.J., et al. Application of motor learning principles: the physiotherapy client as a problem-solver. 1. Concepts. Physiother. Can.. 2000;52(3):229-232.
Wolfe F., Hawley D.J., Wilson K. The prevalence and meaning of fatigue in rheumatic disease. J. Rheumatol.. 1996;23:1407-1417.