Chapter 14 Diet and complementary therapies
KEY POINTS
 A combination of weight loss/healthy eating and exercise is recommended in the management of osteoarthritis
A combination of weight loss/healthy eating and exercise is recommended in the management of osteoarthritisINTRODUCTION
Conventional medicine (pharmacological treatment) generally only offers symptom relief for chronic rheumatological conditions, and some patients are unwilling to take drugs for long periods, especially as they may have serious side-effects. Therefore, patients often seek out dietary or complementary approaches. These are discussed in turn in this chapter.
SECTION 1 DIET AND DIETARY THERAPIES
At some point, health professionals working in the area of musculoskeletal conditions will be asked by patients about the role that diet can play in managing their symptoms. Diet is one issue which is very important to many patients and may have a more important role than many health professionals acknowledge (Rayman & Pattison 2008). Dietitians are not yet widely viewed as core members of the rheumatology team and may not be easily accessed, thus it is important that some dietary issues can be safely addressed by other health professionals. This chapter will provide an overview of basic nutritional requirements for healthy eating in general and a more in depth examination of the available evidence for dietary advice in common musculoskeletal conditions. Dietary intervention usually involves adding a food, nutrient or substance to the diet for example a dietary supplement or removing food from the diet or making a total change to dietary intake. In general, diets are perceived to be harmless but, uninformed and unnecessary dietary restrictions will disturb normal diet and lifestyle patterns, increase the risk of nutritional deficiencies and even adversely affect medical treatment. Therefore, it is important to recognise when expert advice is necessary. To deal with this, two scenarios are discussed in the case studies at the end of this chapter.
HEALTHY EATING
A healthful diet is based on a varied intake of wholegrain cereals, low fat dairy products, fish and lean meats, olive oil based oils and margarines, fruit and vegetables, beans and pulses, is therefore low in fat, especially saturated fat, salt and sugar but adequate in energy, protein and fibre (Tables 14.1, 14.2).
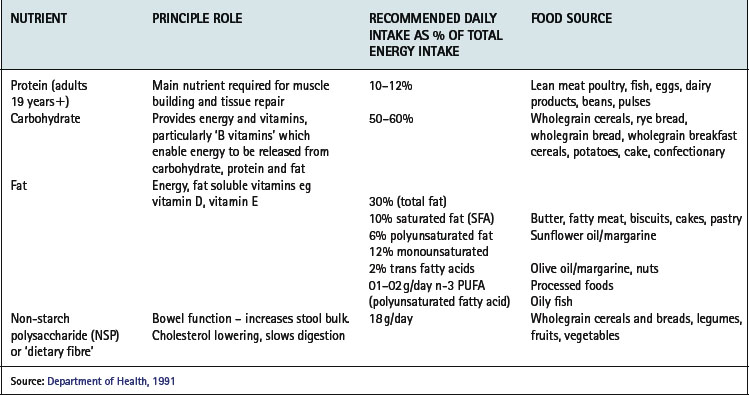
Table 14.2 Food groups and targets for intake
| FOOD GROUP | TARGETS FOR DIETARY INTAKES |
|---|---|
| Bread, potato, cereals, rice, flour, pasta | Average 6–11 portions/day (eg 1 portion = 1 slice bread) Use wholegrain and white |
| Sugars, sweets, biscuits, cakes | Eat ‘in moderation’ |
| Fats: butter, margarine, oil | Use olive oil & olive oil-based products Grill, poach, bake, steam instead of frying |
| Dairy products | ½-1 pint milk/day (any type) 4–5 yogurts a week 4–6 portions cheese a week (1 portion = 25 g) Use low fat products |
| Lean meat (beef, pork, lamb) | 2–3 portions a week |
| Poultry | > 2–3 portions a week |
| Fish (all types) | ≥ 2 portions a week |
| Eggs | 2–3 a week |
| Fruit & vegetables | 5 portions daily: 1 portion = 1 apple, 3 dried apricots,1 cereal bowl of mixed salad, 2 broccoli florets |
| Alcohol | Women ≤ 14 units/week Men ≤ 21 units/week (1 unit = ½ pint lager/beer (3–4% ABV); 125 ml glass wine (∼12% ABV); 1 pub measure of spirits) |
NUTRITION IN MUSCULOSKELETAL CONDITIONS
There is an enormous amount of dietary advice aimed at people with arthritis, particularly rheumatoid arthritis (RA). Unfortunately, the vast majority of claims made by self-styled diets for arthritis such as The Dong diet, Sister Hill’s diet, Norman F. Childer’s diet, and many more, are unsubstantiated, based on individual experience and cannot be generalised to everyone with the condition. Undertaking high-quality dietary intervention studies is complex and extremely difficult to do, thus ‘high-level’ evidence of efficacy of a dietary intervention is often lacking. Also, studies measure diverse outcomes making interpretation of the results more difficult. For example, global measures of well being and assessment of pain are more susceptible to placebo effect and convey a different message than measurements of objective, clinical outcomes. In addition, dietary advice recommended for other clinical conditions may be contradictory, thus adding confusion. The following section summarises dietary advice for which there is some evidence of efficacy in the rheumatic diseases.
FISH OILS AND OMEGA-3 FATTY ACIDS
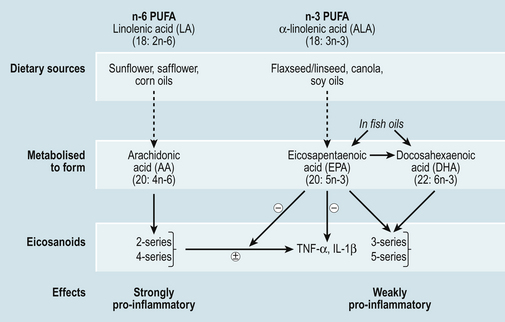
The majority of evidence for the beneficial effects of fish oils in the management of arthritis comes from studies in RA. Long chain omega-6 (n-6) and omega-3 (n-3) polyunsaturated fatty acids (PUFAs) are precursors of inflammatory mediators such as eicosanoids (Fig. 14.1) Metabolism of n-6 PUFA, yields arachidonic acid, a precursor of strongly inflammatory leukotrienes, prostaglandins and thromboxanes (two and four series) (Fig. 14.1), whereas n-3 PUFA are converted to eicosapentaenoic acid (EPA) and further to docosahexaenoic acid (DHA) which yield less inflammatory eicosanoids (three and five series). EPA and DHA are obtained from dietary sources found mainly in oily fish such as mackerel, sardines, halibut, herring, salmon, trout and fresh tuna (not tinned), whereas n-6 PUFAs are much more abundant in the diet for example in seeds, vegetable oils and margarines. The conversion pathways of n-3 and n-6 PUFA are shared, consequently they are in competition for the same enzyme necessary for adaptation (Fig. 14.1). So, in addition to advising patients to increase their intake of n-3 PUFA from fish or supplements, a reduction in the intake of n-6 PUFA may increase the effectiveness of n-3 PUFA supplements. This could be achieved by replacing sunflower oils/margarines with olive or rapeseed oils and olive oil based margarines.
There is good evidence for a therapeutic benefit of n-3 PUFA (EPA + DHA) in patients with RA if taken as fish oil supplements (Fortin et al 1995). A more recent systematic review of the same intervention studies, but specifically exploring pain control in people with RA, concluded that the amount of n-3 PUFA necessary to achieve a reduction in pain is 2.7–3 g/day (total EPA + DHA) for 3–4 months, that is, the maximum duration of these studies (Goldberg & Katz 2007).
The proportion of EPA and DHA in fish oil supplements varies greatly between products but it is possible to achieve an intake of 2 g n-3 PUFA from four or five fish oil capsules, containing 500 mg or more n-3 PUFA. The number of capsules required will also vary depending on oily fish consumption. Liquid fish oil preparations are more concentrated sources of n-3 PUFA and are often flavoured to improve tolerance.
Many ‘one-a-day’ type cod liver oil capsules contain high amounts of the fat soluble vitamins A and D. It is considered unsafe to take high doses of vitamin D long-term because of the risk of hypercalcaemia and hypercalciuria and also unsafe to take high doses of vitamin A because of toxicity or a possible increase in hip fracture. Pregnant women should avoid cod liver oil supplements because of the unknown tetratogenic effects of vitamin A at high doses (Rayman & Callaghan 2006a). Therefore, all patients should be advised to use fish body oil supplements.
N-3 PUFA rich fish oils have also been shown to be effective in secondary cardiovascular disease prevention (Mead et al 2006). Given that people with RA are at an increased risk of cardiovascular disease (Goodson & Solomon 2006), eating oily fish more than twice a week can be recommended. There has been concern over high levels of toxic substances such as dioxins, polychlorinated biphenyls (PCBs), and mercury levels in oily fish and fish oil supplements. The Food Standards Agency (FSA) recommends two portions of fish a week one of which should be oily for the general population. For people who want to eat more oily fish, the FSA has set a maximum of four portions of oily fish per week (Food Standards Agency 2002). Women of reproductive age and girls should limit their intake of oily fish to one portion a week and should avoid swordfish, marlin or shark because of high mercury levels. There is also a Europe wide dioxin limit which manufacturers of fish oil supplements adhere to so toxicity from these should not be a problem. People on anti-coagulation therapy should seek guidance from their medical practitioner before taking high doses of fish oil.
In summary, the evidence currently available suggests that there is a beneficial effect for people with RA from high dose long-chain n-3 PUFA, for 3 to 6 months duration. However, longer term safety of high dose fish oil supplementation has not been adequately monitored. The effect of n-3 PUFA from food sources on joint symptoms has not been investigated.
PLANT SOURCES OF N-3
EPA and DHA can be synthesised from α-linolenic acid (ALA) found most commonly in green leafy vegetables, flaxseeds, rapeseeds and canola oils, although the conversion of ALA to EPA and DHA is relatively inefficient. There is little evidence to support the efficacy of these oils in the management of rheumatic diseases (Rennie et al 2003). On the other hand, there is some supporting evidence for gamma-linolenic acid (GLA) supplementation. GLA is produced from n-6 linoleic acid and is found in plant oils such as evening primrose oil, blackcurrant seed and borage seed oils (Leventhal et al 1993, Little & Parsons 2001a, 2001b, Watson et al 1993). However, results are inconsistent and more research is required in this area before recommendations can be made.
NUTRITION IN OTHER CONDITIONS
There is some evidence ‘in vitro’ that long chain n-3 PUFAs, can affect the metabolism of osteoarthritic cartilage (Curtis et al 2002), but this is not sufficient to recommend high dose fish oil therapy in this group of patients. Patients with gout may be required to follow a diet low in dietary purines. Oily fish are rich in purines and may need to be avoided if gouty symptoms are exacerbated by the consumption of oily fish.
FRUIT, VEGETABLES AND ANTIOXIDANTS
Dietary antioxidants are of particular interest in the management of arthritis. These ‘phytochemicals’ are found extensively in fruits and vegetables particularly brightly coloured varieties such as oranges, apricots, mangos, carrots, peppers/capsicum, and tomatoes and in green leafy vegetables. The most common antioxidants are vitamins C, E and A, but there are many more, such as the carotenoids β-carotene and β-cryptoxanthin. Antioxidants play a crucial role in our internal defence system protecting against harmful metabolites and other substances. There is some evidence that higher dietary intakes of some antioxidants may lower the risk of developing inflammatory arthritis (Pattison et al 2004, 2005) and possibly dampen down the inflammatory response in established disease (Pattison et al 2007). However, this theory is based on epidemiological evidence of dietary intake in inflammatory arthritis. A recent systematic review did not support the use of individual antioxidant supplementation (vitamins A, C, E and selenium) in the treatment of any type of arthritis (Canter et al 2007).
In OA, a higher dietary intake and higher serum levels of vitamin D were associated with a lower risk of knee OA progression (McAlindon et al 1996) but more recent data from two large epidemiological studies of OA have not confirmed this association (Felson et al 2007). Results from a UK intervention study of vitamin D supplementation in established OA knee are awaited.
Anaemia is common in people with RA, usually as a manifestation of the anaemia of chronic disease associated with RA. Mild iron deficiency may actually be beneficial and suppress joint inflammation (Rayman & Callaghan 2006b). Therefore iron supplementation may be detrimental and is not recommended unless under medical supervision.
Overall, the practice of mega-dosing with nutritional supplements should be strongly discouraged. Not only is there no scientific evidence to support this treatment in rheumatic diseases, high doses of individual nutrients can be harmful. For example, long term, excessive vitamin C intake (> 1000 mg/day) can result in gastrointestinal disturbances. A high intake of selenium can lead to selenosis (loss of hair, skin and nails) and for many other nutrients the effect of high doses may yet be unknown.
VEGETARIAN AND VEGAN DIETS
The effects of vegetarian and vegan diets have been investigated in people with RA but not OA (Hafström et al 2001). The pooled results of the only four controlled studies found long-term clinical benefit for patients with RA after fasting followed by a vegetarian diet for three months or more (Müller et al 2001). If followed appropriately, vegetarian diets should not cause nutritional problems. However, vegan diets are much more nutritionally restrictive and may result in excessive weight loss. Patients should be encouraged to seek dietetic support. ‘Living food’ diets (uncooked, vegan diet) (Hänninen et al 2000) and gluten-free diets have also been evaluated in patients with RA but there is as yet little consistent evidence of their efficacy.
MEDITERRANEAN-TYPE DIET
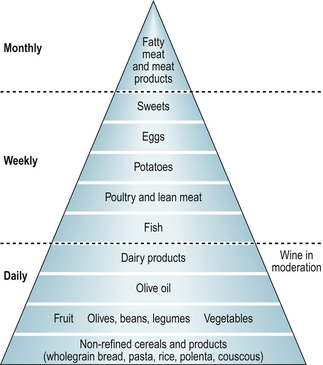
This way of eating is based on daily intakes of fresh fruits and vegetables, nuts, beans and pulses, olive oil, wholegrain cereals and regular oily fish and poultry consumption (Fig. 14.2). Thus, the diet contains n-3 PUFAs, olive oil, antioxidants, dairy products and unrefined carbohydrates. In a recent study, Swedish patients with RA who followed a modified Mediterranean diet for 3 months reported reduced inflammatory activity, increased physical functioning and improved vitality compared with those who followed the control diet (Sköldstam et al 2003). No such studies have been undertaken in people with OA.
BODY WEIGHT
‘Rheumatoid cachexia’ is a common occurrence, which in some can cause weight loss. Increased catabolism, muscle wasting and anorexia develop as a result of excess cytokine production (Morley et al 2006). Thus, nutritional support may not be effective unless given in combination with adequate pharmacological control of the inflammatory response. Elderly patients with hip fracture are often frail and of low body weight. Nutrition support is paramount in this group of patients to encourage healing and recovery. Efficacy has been demonstrated in randomized controlled trials (Avenell & Handoll 2003, Hedström et al 2006).
Epidemiological studies have shown that obesity precedes OA knee and people who are overweight in their 30s are at an increased risk of developing OA knee in their 70s (Felson 1988). There is limited but increasing evidence supporting the efficacy of weight loss as an intervention in overweight and obese patients with OA knee (Woolf 2007). The most successful intervention is a combination of exercise with a weight reduction plan (Messier et al 2004, NICE 2006).
Current dietary guidelines for the management of gout recommend weight loss in those who are overweight and a reduction or avoidance of alcohol (especially beer). Low animal purine diets are still prescribed for patients with gouty symptoms not adequately controlled by drugs (e.g. Allopurinol) (Zhang et al 2006). For further information on gout see Chapter 23.
FOOD AVOIDANCE
True food allergy is no more prevalent in people with RA than in the general population. Food intolerance is more common and dietary exclusion is a popular intervention with patients. A dietary exclusion programme is used to detect food intolerances in a minority of patients under strict dietetic supervision. Specific food stuffs identified by patients as causing flare-ups of symptoms are very individual and cannot be generalised to all people with RA. The risk of nutrient deficiencies must be emphasised if groups of foods are avoided and dietary assessment is recommended. The common belief that tomatoes and citrus fruits are ‘acidic’ and that consumption will exacerbate joint inflammation is not supported by human science. Stomach acids are far stronger than naturally occurring plant acids, plus the body is very efficient at maintaining an optimal pH. In fact these foods are rich in antioxidants such as vitamin C, lycopene and β-cryptoxanthin and should be included in a healthy diet.
A low starch diet has been investigated in the treatment of ankylosing spondylitis (Ebringer & Wilson 1996) but there is no evidence supporting use of this dietary regime in routine practice (Zochling et al 2006) (Table 14.3).
Table 14.3 Evidence for commonly used dietary supplements for management of arthritic symptoms
| SUPPLEMENT | OSTEOARTHRITIS | RHEUMATOID ARTHRITIS |
|---|---|---|
| Avocado/Soybean Unsaponifiables (ASU) | Good - hip and knee* | None |
| New Zealand green-lipped mussel (Perna canaliculus) | Inconclusive** | Inconclusive** |
| Shark cartilage | None – risk of toxic side effects | |
| Methylsulfonylmethane (MSM) | Limited – knee*** | None |
| Cider vinegar | None | None |
| Green Tea extract | None | None |
| Ginger | No effect*** | No effect |
| Curcumin | None | None |
| Rosehip extract | Limited for knee | None |
** Ernst E 2003
DIETARY SUPPLEMENTS
There is little convincing evidence that dietary supplements influence the course of RA (Table 14.3). However, dietetic consultation may be warranted if dietary intake is obviously insufficient to meet an individual’s nutritional requirements.
Glucosamine and chondroitin supplements have been extensively studied for the relief of symptoms in knee osteoarthritis. A review by Towheed et al (2005) concluded that glucosamine (sulphate or hydrochloride) was not superior to placebo for pain, stiffness and function as measured by the Western Ontario and McMaster University Osteoarthritis Index (WOMAC). There is some evidence that for patients with joint pain, who want to control symptoms with dietary supplements, taking 1500 mg with glucosamine sulphate may have beneficial symptomatic effects (Clegg et al 2006). However, there is no consensus regarding the use of glucosamine sulphate between international OA management guidelines. For example in the UK, NICE guidelines do not support the use of glucosamine sulphate in the management of OA (NICE 2008), whereas EULAR guidelines state that glucosamine sulphate and chondroitin sulphate have symptomatic effects in OA knee (Jordan et al 2003). Concerns have been raised about whether glucosamine causes abnormal glucose metabolism, asthma, hypersensitivity, or arteriosclerosis but there is little evidence to support these concerns.
DAIRY PRODUCTS, CALCIUM AND VITAMIN D
Of particular dietary importance to people with RA is calcium and vitamin D intake, necessary for maintaining strong and healthy bones and reducing the risk of osteoporosis (Department of Health 1998). Lower fat dairy products i.e. semi-skimmed or skimmed milk, reduced fat cheeses have the same calcium, if not more than the full fat products. Calcium enriched soya milks or other alternatives must be recommended to people who do not or cannot use dairy products as soya milk per se does not contain calcium. Vitamin D is generated by the action of UVB rays on the skin and is the most efficient source of vitamin D. There are some good dietary sources of vitamin D including fish oils, egg yolk, margarine and meat.
SECTION 2 COMPLEMENTARY THERAPIES
Patients and therapists often seek out complementary treatment to manage their rheumatic condition. Alternative therapies are used as a substitute for conventional approaches. Complementary therapies are used in addition to conventional treatment. These are described below. Many are used by appropriately trained therapists as adjuncts to conventional modalities (see Chs 8 & 11).
ACUPUNCTURE/ACUPRESSURE
Acupuncture involves the stimulation of points in the body with needles. Often, electrical stimulation is applied to the needles – electroacupuncture. In acupressure, the stimulation is by pressure from the fingers or sometimes special devices, such as the wrist-bands for treating nausea in pregnancy. Acupuncture was first discovered by the Chinese, and many modern practitioners still use ancient concepts, for example, that the needles influence the flow of energy in meridians. However, there is plenty of evidence that the needles stimulate several areas of the nervous system, releasing opioid peptides (popularly known as ‘endorphins’). Therefore, many western practitioners are discarding the traditional concepts and regard acupuncture as a particular form of nerve stimulation. However, it is important to distinguish acupuncture from transcutaneous electrical nerve stimulation (TENS): TENS usually only has a temporary effect, whereas acupuncture’s effect accumulates as the treatment is repeated. Usually a course of six or eight treatments is needed.
Although traditional Chinese theory seems to suggest that acupuncture can in some way treat the fundamental cause of the disease, in practice there is no evidence that acupuncture can modify the course of systemic diseases such as rheumatoid arthritis or ankylosing spondylitis. Its main contribution is in pain control. For example, reviews of nearly a dozen randomized controlled trials (RCTs) in osteoarthritis of the knee have shown acupuncture to be at least as effective as, and probably more effective than, non-steroidal anti-inflammatory drugs (NSAIDs) – for both controlling pain and improving function (White et al 2007). What was also impressive was that the effect of a course of treatment was still measurable after 6 months. These studies showed that true acupuncture alone was statistically significantly superior to placebo or ‘sham’ acupuncture alone.
For fibromyalgia, individual RCTs have reached different conclusions as to whether acupuncture, given as an adjunct to other treatments, reduces patients’ symptoms. A recent review found that the overall evidence was not high quality, but that all the studies that used electroacupuncture were positive (Mayhew & Ernst 2006).
OSTEOPATHY AND CHIROPRACTIC
These complementary therapies, though differing slightly in training and approach, both use the techniques of massage, mobilisation and manipulation. They are most often used for spinal problems (neck pain, back pain), which are beyond the scope of this chapter. These treatments seem to have a good reputation for safety, though manipulation of the spine has been known to cause injuries to the nervous system, and to interfere with its blood supply causing stroke. Treatment should be given only by registered practitioners.
Some techniques, particularly mobilization, are used for arthritis in peripheral joints, such as OA of the hip or knee. This approach is similar to conventional manual therapy which is discussed in the Physical Therapies chapter (Ch. 8). Overall, mobilisation in rheumatic diseases seems best used as part of a comprehensive treatment programme (Fiechtner & Brodeur 2002). One small study suggested that manipulative therapy could provide additional pain relief to other treatments for fibromyalgia (Gamber et al 2002).
HOMEOPATHY
In homeopathy, natural substances are given in highly diluted preparations – so dilute that often none of the original substance may be present. Although this appears to be contrary to the laws of physics, and homeopaths have not yet demonstrated how it could work, nevertheless many patients have reported significant benefits from homeopathy. It seems likely that the very detailed history that is needed in finding the exact remedy can itself act as a powerful therapy. Homeopathy would appear to be very safe.
One RCT found no effect of homeopathy compared with placebo in rheumatoid arthritis (Fisher & Scott 2001), but a systematic review of homeopathy for people with OA found four RCTs which provided some supportive evidence, and recommended more research (Long & Ernst 2001). In fibromyalgia, two small studies found homeopathy significantly better than placebo in lessening tender point pain (Fisher et al 1989) and improving the quality of life and global health (Bell et al 2004).
HERBAL MEDICINE
This section refers to medicines made from plants or plant extracts, and not to the food supplements or individual phytochemicals discussed in the previous section or listed in Table 14.3. Several herbs, such as Devil’s claw (Harpagophytum procumbens), willow bark extract, and nettle (Urtica dioica) are traditional folk treatments for painful conditions in many cultures. Recent research has increased the level of awareness of their side-effects as well as their interactions with many drugs.
Two reviews found no good evidence that any herb is beneficial for rheumatoid arthritis (Little & Parsons 2001a) or for osteoarthritis (Little & Parsons 2001b), other than those mentioned in the previous section. Many herbs are available for patients to purchase, but it seems sensible for health practitioners not to make recommendations unless they are qualified to do so. The situation also applies to Chinese herbs: prescribing them is a highly specialised skill that has to take into account individual dosage, particular combinations of herbs, significant variations in quality of the products, and toxicity.
BALNEOTHERAPY
This is treatment by bathing in warm water, usually with natural or added minerals or mud packs. Also known as ‘spa therapy’, it is often used on the European mainland and in Israel for inflammatory arthritis. Trials in patients with rheumatoid arthritis have generally shown that patients feel better after a course of balneotherapy, but the evidence is not good enough to draw conclusions (Verhagen et al 2003). In ankylosing spondylitis, one trial showed a short-lived effect compared with exercise alone (Altan et al 2006), but another study showed no effect of mud packs compared with fresh water (Codish et al 2005). There is some evidence that balneotherapy may be effective in fibromyalgia (Evcik et al 2002).
MAGNET THERAPY
There has been a considerable amount of laboratory research on the effects of magnetic fields in reducing the severity of pain, but rather few clinical trials. Magnets may be applied over the joint itself, or in wrist-bands in the hope of producing a systemic effect. Although there are some positive RCTs that seem to show magnets reduce pain from arthritis in the hip or knee (Harlow et al 2004, Wolsko et al 2004), because of problems with blinding the trials do not provide evidence strong enough to make recommendations.
TAI CHI
This eastern approach to physical exercise is suitable for older people, and includes a meditative element. It shows no overall effects in RA, but does improve the range of movement in ankle joints. It is also popular with patients, and it is one form of exercise that patients tend to continue to use (Han et al 2004). In elderly people with hip or knee OA, a recent study showed a trend to less benefit from tai chi than from hydrotherapy (Fransen et al 2007).
YOGA
A literature review found a small number of studies in patients with musculoskeletal conditions show some benefits, when compared with patients who did not practise yoga (Raub 2002).
SUMMARY
Diet is a popular intervention for people with musculoskeletal conditions. This might involve the exclusion of certain foodstuffs thought to aggravate symptoms, the addition of a supplement believed to ameliorate symptoms or a change of eating habits towards healthy eating for weight loss or weight maintenance and heart health. Although there is only limited scientific evidence to support either exclusion diets or dietary supplementation in the management of musculoskeletal conditions, dietary advice relevant to cardiovascular and bone health would benefit the majority and should be more widely available.
Alternative and complementary therapies are often used for chronic conditions. Acupuncture can produce pain relief in rheumatological conditions but there is no evidence that it can alter the course of the disease. Mobilisation of joints by osteopaths and chiropractors may be used as part of a multi-therapy approach. Homeopathy is safe and can be effective, though how much of the effect is due to the actual remedies is not known. Currently, there is insufficient evidence to recommend herbal remedies or other therapies.
CASE STUDY 14.1
Miss Hall has rheumatoid arthritis and is postmenopausal. In the past treatment has included intermittent oral steroids. Miss Hall’s physical activity levels are reduced due to her disease state. Miss Hall has been trying a ‘special diet’ for six months during which time she has avoided all dairy products and red meat. She is suffering from tiredness and fatigue, more so than usual and has lost weight, which she puts down to her RA. When challenged, Miss Hall admits she doesn’t really think that the ‘diet’ makes her feel any better and she admits that she finds it difficult and frustrating sticking to the diet. She feels hungry a lot of the time and her friends have commented on how thin she has become. Despite these effects, Miss Hall has continued with the diet hoping it will improve her arthritis.
Advice: Provide Miss Hall with an information leaflet on healthy eating. Discuss the nutritional requirements for a healthy diet and a healthy weight. Point out the risks of being underweight to bone health. Highlight the need for calcium and vitamin D for healthy bones and the benefits of fruit and vegetables for bone health and general health. As Miss Hall wishes to re-introduce the foods that she has excluded, suggest she keeps a record of everything she eats and drinks and note how she feels afterwards for example, if any symptoms of arthritis are provoked after eating dairy foods or meat. This action may help her assess for herself if the diet is appropriate and if not, how she can re-introduce the excluded foods.
CASE STUDY 14.2
Male, aged 65 years Height: 170 m Weight: 102 kg
Myocardial Infarction (MI) 3 years ago
Clinical diagnosis of knee osteoarthritis 6 months ago
DXA (bone density scan) osteopaenia at lumbar spine and femoral neck
Self-prescribed glucosamine sulphate
Work out his body mass index (BMI = weight in kg/height in metres2) and explain, sensitively, where this figure appears on a BMI chart – in the ‘obese’ category. Allow him to respond – how does this make him feel? Begin to explore his feelings and his attitude towards his weight. How does he feel his weight impacts on his life, for example, on his health, his hobbies, activities, marriage etc? Does he want to and feel able to address this? Is he at the stage where he is ready for change? In the first instance, suggest he keeps a food diary for a week or two to reveal his dietary intake. This may have some immediate impact on Mr Sowden himself. A completed food diary is a very useful tool for dietitians to use with patients at their initial appointments. Another suggestion might be that he could attend a slimming group – men do go and often do very well with peer support. Given his other dietary issues (raised cholesterol, osteopaenia and food avoidance), this is a more complex case and Mr Sowden should be referred to a registered dietitian in the hospital or community but your advice will have started Mr Sowden thinking about his eating habits and weight which will be very helpful when he attends his dietetic appointment.USEFUL WEBSITES AND PATIENT INFORMATION
Arthritis Research Campaign (arc) website (www.arc.org.uk) accessed January 2009 – Diet and Arthritis.
Arthritis Care (www.arthritiscare.org.uk) accessed January 2009 Healthy Eating and Arthritis.
CAMEOL (Complementary and Alternative Medicine Evidence On line) at (www.rccm.org.uk/cameol) accessed January 2009.
Complementary and Alternative Medicine Specialist Library (/www.library.nhs.uk/CAM/) accessed January 2009.
National Osteoporosis Society (www.nos.org.uk) accessed January 2009 – Healthy Eating for Strong Bones.
British Dietetic Association ‘Food facts’ (www.bda.uk.com) accessed January 2009 – Diet and rheumatoid arthritis, Diet and osteoarthritis, Osteoporosis plus various information sheets for weight management and healthy eating.
Food Standards Agency (FSA) (www.eatwell.gov.uk) accessed January 2009.
Arthritis: Improve your health, ease pain, and live life to the full Dorling Kindersley, London, 2006.
Arthritis: Your questions answered Dorling Kindersley, London, 2007.
Ernst, E., Pittler, M., Wider, B., 2006. The Desktop Guide to Complementary and Alternative Medicine. Mosby: Edinburgh .
References and further reading
Altan L., Bingol U., Aslan M., et al. The effect of balneotherapy on patients with ankylosing spondylitis. Scand. J. Rheumatol.. 2006;35(4):283-289.
Ameye L.G., Chee S.S. Osteoarthritis and nutrition. From nutraceuticals to functional foods: a systematic review of the scientific evidence. Arthritis Res. Ther.. 2006;8:R127.
Avenell A., Handoll H.H. A systematic review of protein and energy supplementation for hip fracture aftercare in older people. Eur. J. Clin. Nutr.. 2003;57(8):895-903.
Bell I.R., Lewis D.A., Brooks A.J., et al. Improved clinical status in fibromyalgia patients treated with individualized homeopathic remedies versus placebo. Rheumatology (Oxford). 2004;43(5):577-582.
Canter, P.H., Wider, B., Ernst, E., 2007. The antioxidant vitamins A, C, E and selenium in the treatment of arthritis: a systematic review of randomized controlled trials. Rheumatology Advance Access published May, 23.
Clegg D.O., Reda D.J., Harris C.L., et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N. Eng. J. Med.. 2006;354(8):795-808.
Cobb C.S., Ernst E. Systematic review of a marine nutriceutical supplement in clinical trials for arthritis: the effectiveness of the New Zealand green-lipped mussel Perna canaliculus. Clin. Rheumatol.. 2006;25(3):275-284.
Codish S., Dobrovinsky S., Abu S.M., et al. Spa therapy for ankylosing spondylitis at the Dead Sea. Isr. Med. Assoc. J.. 2005;7(7):443-446.
Curtis C.L., Rees S.G., Little C.B., et al. Pathologic indicators of degradation and inflammation in human osteoarthritis cartilage are abrogated by exposure to n-3 fatty acids. Arthritis Rheum.. 2002;46(6):1544-1553.
Department of Health. 1991. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom: Report of the Panel on Dietary References Values of the Committee on Medical Aspects of Food Policy. The Stationary Office, London.
Department of Health. 1998. Nutrition and Bone Health: with particular reference to calcium and vitamin D., Report of the Subgroup on Bone Health, Working Group on the Nutritional Status of the Population of the Committee on Medical Aspects of Food and Nutrition Policy. The Stationary Office, London.
Ebringer A., Wilson C. The use of a low starch diet in the treatment of patients suffering from ankylosing spondylitis. Clin. Rheumatol.. 1996;15(Suppl. 1):62-66.
Ernst E. Avocado-soybean unsaponifiables (ASU) for osteoarthritis - a systematic review. Clin. Rheumatol.. 2003;22(4-5):285-288.
Evcik D., Kizilay B., Gokcen E. The effects of balneotherapy on fibromyalgia patients. Rheumatol. Int.. 2002;22(2):56-59.
Felson D.T. Epidemiology of hip and knee osteoarthritis. Epidemiol. Rev.. 1988;10:1-28.
Felson D.T., Niu J., Clancy M., et al. Low levels of vitamin D and worsening of knee osteoarthritis: results of two longitudinal studies. Arthritis Rheum.. 2007;56:129-136.
Fiechtner J.J., Brodeur R.R. Manual and manipulation techniques for rheumatic disease. Med. Clin. N. Am.. 2002;86(1):91-103.
Fisher P., Scott D.L. A randomized controlled trial of homeopathy in rheumatoid arthritis. Rheumatology (Oxford). 2001;40(9):1052-1055.
Fisher P., Greenwood A., Huskisson E.C., et al. Effect of homeopathic treatment on fibrositis (primary fibromyalgia). Brit. Med. J.. 1989;299(6695):365-366.
Food Standards Agency. 2002. Survey of Dioxins and Dioxin-like PCBs in Fish Oil Supplements (Number 26/02) www.food.gov.uk/multimedia/pdfs/26diox.pdf.
Fortin P.R., Lew R.A., Liang M.H., et al. Validation of a meta-analysis: the effects of fish oil in rheumatoid arthritis. J. Clin. Epidemiol.. 1995;48:1379-1390.
Fransen M., Nairn L., Winstanley J., et al. Physical activity for osteoarthritis management: a randomized controlled clinical trial evaluating hydrotherapy or Tai Chi classes. Arthritis Rheum.. 2007;57(3):407-414.
Gamber R.G., Shores J.H., Russo D.P., et al. Osteopathic manipulative treatment in conjunction with medication relieves pain associated with fibromyalgia syndrome: results of a randomized clinical pilot project. J. Am. Osteopath. Assoc.. 2002;102(6):321-325.
Goldberg R.J., Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain. 2007;129:210-223.
Goodson N.J., Solomon D.H. The cardiovascular manifestations of rheumatic diseases. Curr. Opin. Rheumatol.. 2006;18:135-140.
Hafström I., Ringertz B., Spångberg A., et al. A vegan diet free of gluten improves the signs and symptoms of rheumatoid arthritis: the effects on arthritis correlate with a reduction in antibodies to food antigens. Rheumatology. 2001;40(10):1175-1179.
Han, A., Robinson, V., Judd, M., et al., 2004. Tai chi for treating rheumatoid arthritis, Cochrane. Database Syst. Rev. (3) CD004849.
Hänninen O., Kaartinen K., Rauma A.L., et al. Antioxidants in vegan diet and rheumatic disorders. Toxicology. 2000;155(1-3):45-53.
Harlow T., Greaves C., White A., et al. Randomised controlled trial of magnetic bracelets for relieving pain in osteoarthritis of the hip and knee. Brit. Med. J.. 2004;329(7480):1450-1454.
Hedström M., Ljungqvist O., Cederholm T. Metabolism and Catabolism in hip fracture patients. Nutritional and anabolic intervention-a review. Acta Orthop.. 2006;77(5):741-747.
Jordan K.M., Arden N.K., Doherty M., et al. EULAR Recommendations: an evidence based approach to the management of knee osteoarthritis: Report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann. Rheum. Dis.. 2003;62:1145-1155.
Leventhal L.J., Boyce E.G., Zurier R.B. Treatment of rheumatoid arthritis with gamma-linolenic acid. Ann. Int. Med.. 1993;119:867-873.
Little, C., Parsons, T., 2001a. Herbal therapy for treating rheumatoid arthritis. Cochrane Database Syst. Rev. CD002948.
Little, C.V., Parsons, T., 2001b. Herbal therapy for treating osteoarthritis. Cochrane Database Syst. Rev. CD002947.
Long L., Ernst E. Homeopathic remedies for the treatment of osteoarthritis: a systematic review. Brit. Homeopathic J.. 2001;90(1):37-43.
Mayhew E., Ernst E. Acupuncture for fibromyalgia–a systematic review of randomized clinical trials. Rheumatology (Oxford). 2006;46(5):801-804.
McAlindon T.E., Felson D.T., Zhang Y., et al. Relation of dietary intake and serum levels of vitamin D to progression of osteoarthritis of the knee among participants in the Framingham Study. Ann. Int. Med.. 1996;125:353-359.
Mead A., Atkinson G., Albin D., et al. Dietetic Guidelines on food and nutrition in the secondary prevention of cardiovascular disease – evidence from systematic reviews of randomized controlled trials. J. Hum. Nutr. Diet.. 2006;19(6):401-419. second update, January 2006
Messier S.P., Loeser R.F., Miller G.D., et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the Arthritis, diet and activity promotion trial. Arthritis Rheum.. 2004;50:1501-1510.
Morley J.E., Thomas D.R., Wilson M.G. Cachexia: pathophysiology and clinical relevance. Am. J. Clin. Nutr.. 2006;83:735-743.
Müller H., de Toledo F.W., Resch K.L. Fasting followed by vegetarian diet in patients with rheumatoid arthritis: a systematic review. Scand. J. Rheumatol.. 2001;30(1):1-10.
NICE. Clinical Guideline 43. Obesity: Guidance on the Prevention, Identification, Assessment and Management of Overweight and Obesity in Adults and Children. National Collaborating Centre for Chronic Conditions. London: Royal College of Physicians; 2006.
NICE. Clinical guideline 59. Osteoarthritis: the care and management of osteoarthritis. National Collaborating Centre for Chronic Conditions. London: Royal College of Physicians; 2008.
Pattison D.J., Lunt M., Welch A., et al. Diet and Disability in Early Inflammatory Polyarthritis. Rheumatology. 2007;46(Suppl. 1):i122.
Pattison D.J., Silman A.J., Goodson N.J., et al. Vitamin C and the risk of developing inflammatory polyarthritis: prospective nested case-control study. Ann. Rheum. Dis.. 2004;63:843-847.
Pattison D.J., Symmons D.P.M., Lunt M., et al. Dietary β–cryptoxanthin and inflammatory polyarthritis: results from a population-based prospective study. Am. J. Clin. Nutr.. 2005;82:451-455.
Raub J.A. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: a literature review. J. Altern. Complem. Med.. 2002;8(6):797-812.
Rayman M., Callaghan A. Polyunsaturated fatty acids in the treatment of arthritis. In: Nutrition and Arthritis. Oxford: Blackwell Publishing; 2006:146-183.
Rayman M., Callaghan A. Role of micronutrients in the amelioration of rheumatoid arthritis and osteoarthritis. In: Nutrition and Arthritis. Oxford: Blackwell Publishing; 2006:112-145.
Rayman M., Pattison D.J. Dietary manipulation in musculoskeletal conditions. Best Pract. Res. Clin. Rheumatol.. 2008;22:535-561.
Rennie K.L., Hughes J., Lang R., et al. Nutritional Management of rheumatoid arthritis: a review of the evidence. J. Hum. Nutr. Diet.. 2003;16:97-109.
Sköldstam L., Hagfors L., Johansson G. An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann. Rheum. Dis.. 2003;62:208-214.
Towheed, T.E., Maxwell, L., Anastassiades, T.P., et al., 2005. Glucosamine therapy for treating osteoarthritis (Review). Cochrane Database Syst. Rev. (2) CD002946pub2.
Verhagen, A.P., Bierma-Zeinstra, S.M., Cardoso, J.R., et al., 2003. Balneotherapy for rheumatoid arthritis. Cochrane Database Syst. Rev. CD000518.
Watson L., Byars M.L., McGill P., et al. Cytokine and prostaglandin production by monocytes of volunteers and rheumatoid arthritis patients treated with dietary supplements of blackcurrant seed oils. Brit. J. Rheumatol.. 1993;32:1055-1058.
White A., Foster N.E., Cummings M., et al. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford). 2007;46(3):384-390.
Wolsko P.M., Eisenberg D.M., Simon L.S., et al. Double-blind placebo-controlled trial of static magnets for the treatment of osteoarthritis of the knee: results of a pilot study. Altern. Ther. Health Med.. 2004;10(2):36-43.
Woolf A.D. What healthcare services do people with musculoskeletal conditions need? The role of rheumatology. Ann. Rheum. Dis.. 2007;66:293-301.
Zhang W., Doherty M., Bardin T., et al. EULAR evidence based recommendations for gout Part II: Management Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis.. 2006;65(10):1312-1324.
Zochling J., van der Heijde D., Dougados M., et al. Current evidence for the management of ankylosing spondylitis: a systematic literature review for the ASAS/EULAR management recommendations in ankylosing spondylitis. Ann. Rheum. Dis.. 2006;65:423-432.