Chapter 8 Physical therapies
Treatment options in rheumatology
KEY POINTS
 Physical therapies aim to control pain, minimise joint stiffness and limit joint damage with the least adverse treatment effects
Physical therapies aim to control pain, minimise joint stiffness and limit joint damage with the least adverse treatment effectsINTRODUCTION
Physical therapies are non-pharmalogical treatments which are widely used by therapists in the management of rheumatic diseases. This chapter briefly reviews the role of physical therapies (electrophysical agents (EPA), thermotherapy and cryotherapy, manual therapy and acupuncture) in common rheumatic conditions and discusses the current evidence and recommendations for clinical practice for these therapies.
THE AIMS OF PHYSICAL THERAPIES IN RHEUMATIC DISEASES
It is important our assessment and management of patients with rheumatic disease is holistic. This means therapists should consider the person with the rheumatic condition rather than the structure (e.g. synovial joint) or the pathological process (e.g. rheumatoid arthritis) prior to selecting any therapy. This holistic perspective has been conceptualised as the biopyschosocial model (see Chs 5 & 11) and suggests there is far more than just the pathology or structure which has an impact on the outcome of the disease. Therefore, a detailed subjective and objective patient assessment, which includes psychosocial factors (Kendall 1997) and health related quality of life, should be obtained (Ch. 4) and a collaborative process used to develop realistic, achievable, measurable patient orientated goals. As all patients with rheumatic disease are different, starting from a different baseline and with different needs, the physiological and psychological impact of each physical therapy should be considered on an individual basis.
When considered in a biopyschosocial context, physical therapies predominantly address the ‘bio’ aspect and aim to control pain, minimise joint stiffness, limit joint damage with the least adverse treatment effects. However, if applied judiciously physical therapies help maximise function and health-related quality of life.
ELECTROPHYSICAL AGENTS
Electrophysical agents (EPA) are used by healthcare practitioners to relieve pain, improve muscle function and reduce inflammation. An underlying premise of all EPAs is that applying an external energy source can beneficially alter physiological processes. In the management of rheumatic disease, electrical stimulation, low level laser therapy, ultrasound therapy and short wave diathermy are most frequently used.
SENSORY STIMULATION FOR PAIN RELIEF
Sensory stimulation means applying electrical stimulation with the intention of increasing the afferent nerve input. This effects a change at the spinal or supraspinal level of the neurological system (centrally), which can be used to alter pain perception. The rationale for this treatment is provided by the pain gate theory (Melzack & Wall 1965). This theory proposes that pain perception is regulated by a ‘gate’ at the level of the dorsal column of the spinal cord, which may be opened or closed by means of other inputs from peripheral nerves or the central nervous system (see Ch. 5). Essentially, electrical stimulation is aimed at modifying the peripheral input (stimulation of the A beta mechanoreceptor fibres at the skin) which inhibits nociceptor activity of C and A delta fibres (at the posterior horn) thus changing the level of excitability of the central components of the neurological system, e.g. central nociceptive transmission cells, wide dynamic range neurons (Robertson et al 2006).
Additionally, electrical stimulation is responsible for releasing chemical mediators (e.g. encephalins), which have a morphine type inhibitory effect on the C- fibre (nociceptor) system. Furthermore, activation of the A delta fibres may provoke impulses in the mid brain which inhibit the neurons at the original site via stimulation of the descending inhibitory pathways (Galea 2002). Thus, by changing the sensory input the perception of pain may be altered but not the underlying cause of the pain.
TRANSCUTANEOUS ELECTRICAL NERVE STIMULATION
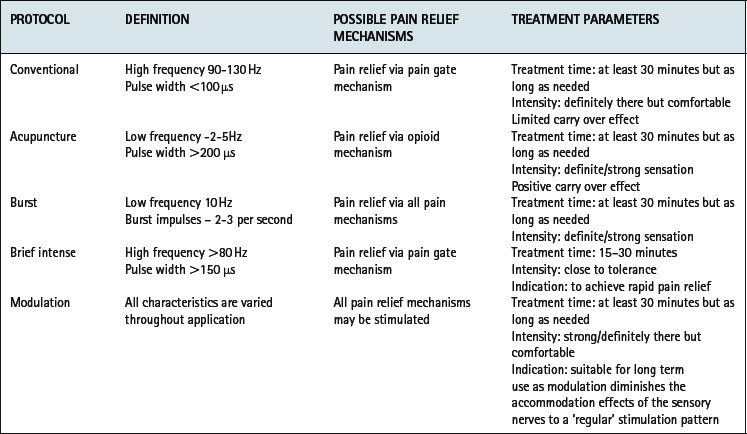
Transcutaneous electrical nerve stimulation (TENS) is an easily applied, non-invasive modality with relatively few contraindications (Fox & Sharp 2007, Robertson et al 2006) which can be readily adopted as a pain management strategy for patients with rheumatic conditions. Small battery operated TENS machines deliver an electrical impulse via surface skin electrodes (Fig. 8.1). Five parameters can be adjusted to achieve most effective pain relief – waveform, pulse duration and frequency, intensity and electrode position. Therapeutic methods of applying TENS are categorized into conventional, ‘acupuncture-like’, burst, brief intense and modulation (Watson 2007). Selection is based on the underlying condition, severity and duration of symptoms (Brosseau et al 2004) (Table 8.1). Recent meta-analyses of six randomised controlled trials (RCT) involving 268 patients with lower limb osteoarthritis (OA) suggest all modes of TENS improve pain, but not range of movement, function or strength regardless of the treatment protocol (Brosseau et al 2004). In patients with knee OA, longer courses of treatment (> 4 weeks) and greater intensity protocols (high burst or low frequency) may produce greatest pain relief (Osiri et al 2000). In people with inflammatory disease, acupuncture-like TENS reduces pain and increases muscle power, whilst conventional TENS improves self reported disease activity but not pain (Brosseau et al 2003a).

Clinical guidelines recommend acupuncture-like TENS for improving pain, oedema and power in patients with RA, (Brosseau et al 2004) as a relatively safe adjunct therapy for the relief of pain in patients with OA (Philadelphia Panel 2001) and for osteoporotic (OP) patients with intractable pain especially those with chronic low back pain and recent vertebral factures (Chartered Society of Physiotherapy 1999).
INTERFERENTIAL THERAPY
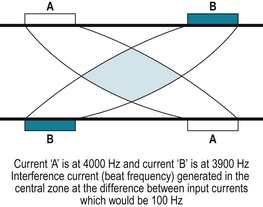
Interferential therapy (IFT) is an alternative method of sensory nerve stimulation, which applies two alternating currents of slightly different frequencies (kHz) at right angles to each other in a continuous stream. Theoretically, where the currents intersect an area of maximum stimulation is produced. However, as the spread of the current reduces the intensity in deep tissues the superimposed current may be less effective than immediately under electrodes and therefore may not achieve the desired therapeutic response (Robertson et al 2006). Clinically, medium frequency currents are applied which pass through the skin more comfortably than a typical low frequency current (due to skin resistance). At the intersection of the currents a beat frequency produces an effect similar to a low frequency current (Fig. 8.2). Using appropriate frequencies, sensory nerve stimulation can be achieved, activating the pain gate mechanism (between 80–130Hz) and opioid mechanisms (< 10Hz) associated with pain relief.
Evidence for the effectiveness of IFT in rheumatic disease is limited but it may reduce pain in patients with psoriatic arthritis (Walker et al 2006) and when combined with ultrasound may reduce pain and improve sleep in patients with fibromyalgia (Almeida et al 2003). However, due to the size of the apparatus, application of IFT is limited to use within the healthcare setting and therefore encourages reliance on healthcare practitioners rather than promoting self-management. Whilst there is some evidence to support the efficacy of sensory stimulation for pain relief no studies directly compare the clinical effectiveness of TENS and IFT. Without evidence of superior efficacy of one form of sensory stimulation, the small, battery operated TENS machine offers a relatively safe, inexpensive, easily self administered method of symptom control in patients with rheumatic diseases.
MOTOR STIMULATION OF INNERVATED MUSCLE
Motor stimulation is the production of a muscle contraction by electrical stimulation of the motor nerves. It is used for; increasing muscle strength and endurance, re-education of motor control, oedema reduction, increasing joint and soft tissue mobility and altering muscle structure and function (trophic changes). Therapeutically it can be used as a sole treatment, (Bircan et al 2002) superimposed over an active muscle contraction (Strojnik 1998) or as an adjunct to an exercise regimen (Fitzgerald et al 2003).
Gradual onset short duration pulses may be selected at frequencies between 30-100 Hz with on-off times and rate of ramping (progression) varying with clinical considerations. The number of repetitions is defined by the training response required and the amplitude is set at maximum individual tolerance. A two second pulse, followed by four second rest with a one second ramp, mimics physiological muscle contraction although the complexity of normal muscle group activity cannot be simulated (Robertson et al 2006).
In patients with rheumatoid arthritis (RA) with secondary disuse atrophy of the first dorsal interosseous of the hand, muscle stimulation improves hand function, strength and fatigue resistance of the first dorsal interosseus muscle (Oldham & Stanley 1989). Similarly, functional performance and quadriceps muscle torque improved by 10% in people with OA knee following muscle stimulation (Talbot et al 2003).
Whilst not included in any clinical guidelines for patients with rheumatic disease, motor stimulation should be considered as an adjunctive therapy for patients with gross muscle weakness secondary to rheumatic disease. However, the high amplitude needed to evoke a muscle contraction can be uncomfortable and may diminish patient compliance with the treatment.
LOW LEVEL LASER THERAPY
Low level laser therapy (LLLT) utilises a pencil-like beam of electromagnetic waves of a single frequency and defined wavelength to promote tissue healing and pain relief in a broad spectrum of soft tissue injuries and diseases. The effects of LLLT are not thermal but photochemical reactions in cells, termed photobioactivation. LLLT produces its physiological and therapeutic effects by applying enough energy to disturb local electron orbits, initiate chemical change, disrupt molecular bonds and produce free radicals at the cell membrane to control the inflammatory response, promote healing and pain relief (Box 8.1) (Robertson et al 2006, Watson 2000).
BOX 8.1 The potential photobioactivation effects of low level laser therapy
Activation & proliferation of fibroblasts
Alteration of cell membrane potentials
Stimulation of immune responses
Alteration of action potentials
Altered prostaglandin production
In patients with rheumatic disease the evidence for the use of LLLT is mixed. In patients with OA, LLLT is ineffective for pain relief (Brosseau et al 2005). However, LLLT is recommended in clinical practice guidelines for patients with RA as it improves pain and morning stiffness, but not function, range of movement, joint tenderness or swelling (Brosseau et al 2004).
ULTRASOUND THERAPY
In the management of rheumatic diseases, ultrasound therapy (US) is commonly used as an adjunctive therapy for its proposed effects on inflammation as well as for pain relief. It uses sound waves at very high frequencies (0.5-5 MHz) to produce mechanical vibration within the tissues. If applied in high doses absorption of US results in heating, which decreases pain and fluid viscosity, increases metabolic rate and blood flow (thermal effects) (Nussbaum 1997). At lower doses of US or following pulsed US non thermal, mechanical effects such as stable cavitation (formation of gas bubbles in tissues), standing waves (reflected waves superimposed on incident waves) and acoustic streaming (fluid movement which exerts pressure changes on a cell) occur (Maxwell 1992) which cause membrane distortion, increased permeability, increased nutrient transfer and facilitation of tissue repair (Mortimer & Dyson 1988). When applied to acutely inflamed tissues it encourages the inflammatory process to progress to the proliferation stage (Watson 2000).
Whilst there is evidence to support the physiological effects of US in laboratory or animal studies, (Mortimer & Dyson 1988) evidence for its clinical effectiveness in people with rheumatic conditions is limited (Brosseau et al 2004, Zhang et al 2007) and it is only recommended for those with arthritis of the hand (Casimiro et al 2002, Welch et al 2001). Moreover, a recent review concludes US may only be effective for people with carpal tunnel syndrome and those with calcific tendonitis of the shoulder (Roberston & Baker 2001) despite being a frequently used electrophysical modality in musculoskeletal conditions (Kitchen & Partridge 1996).
SHORT WAVE THERAPY
Short wave diathermy (SWD) produces its physiological and therapeutic effects by rapidly alternating electrical and magnetic currents at short wave frequencies (27.12 MHz). Continuous SWD is applied to tissues either inductively (metal cable, covered in insulating rubber, which is wrapped around the part to be treated) or capacitively (plate or malleable electrodes placed next to the area to be treated), usually for 20–30 minutes. It increases skin temperature by 3-7°C, muscle temperature by 2-6°C (Robertson et al 2006) and intra-articular heating has also been demonstrated (Oosterveld et al 1992).
Pulsed short wave diathermy (PSWD) or pulsed electromagnetic energy (PEME) is an intermittent oscillating high frequency (27.12MHz) output. The mean power depends on the peak (pulse) power, duration and frequency of the pulse. As a thermal effect is only produced with outputs above 7 Watts, the non thermal physiological effects of PSWD are postulated to occur due to agitation of ions, molecules, membranes and perhaps cells which accelerates membrane transport, phagocytic, and enzymatic activity (Kitchen & Partridge 1992, Low 1995, Robertson et al 2006).
Brief, high intensity bursts of electromagnetic energy:
Whilst based on reasonable biophysical evidence (Hill et al 2002), the evidence for the clinical effective of short wave therapy is mixed and some studies report no improvement of pain, stiffness or disability in patients with lower limb OA following PSWD (Callaghan et al 2000, Klaber Moffett et al 1996, Laufer et al 2005, Thamsborg et al 2005) whilst others conclude pulsed SWD may be beneficial (Van Nguyen & Marks 2002) after lengthy courses of treatment (Jan et al 2006). There is no evidence to suggest SWD may be beneficial for people with RA and it is not included in guidelines for the management of any rheumatic conditions.
ACUPUNCTURE
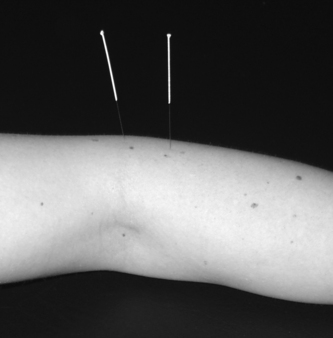
Acupuncture literally means ‘needle piercing’ – the practice of inserting very fine needles into the skin to stimulate specific anatomic points in the body (called acupoints or acupuncture points) for therapeutic purposes (Fig. 8.3). Heat, pressure, friction, suction, or impulses of electromagnetic energy may be used to stimulate the points.
Acupuncture is one of the more popular complementary interventions for arthritis (Ernst 1997) and it is gaining acceptance and utilization within western healthcare systems as a form of pain relief (Tindle et al 2005) where its effects are explained through the pain gate theory (Melzack & Wall 1965) and stimulation of the release of neurochemicals in the central nervous system (Cheung & Pomeranz 1979). In its traditional form (as a component of traditional Chinese medicine) acupuncture points are stimulated to balance the movement of energy (qi) in the body along energy channels (meridians) to restore health and the production of acupuncture analgaesia is explained via neural, humeral and biomagnetic mechanisms (Cao 2002).
Acupuncture is used by many physiotherapists, often within the NHS, and the Acupuncture Association of Chartered Physiotherapists is a recognised special interest group within the profession. Many doctors have also been trained in acupuncture, and there is a group of practitioners who have trained in acupuncture and who mainly work privately, sometimes also prescribing Chinese herbs (see Ch. 14).
Acupuncture needles can of course cause injuries, (for example, accidental penetration of the lung, which causes a pneumothorax or collapsed lung), but in the hands of a trained practitioner acupuncture is very safe (White et al 2001). The only contraindications are in patients who have an undiagnosed bleeding disorder, or a fear of needles. There is no evidence that acupuncture interacts with other treatments.
There is growing evidence that acupuncture is beneficial for pain management in peripheral joint osteoarthritis. A systematic review of 18 randomized controlled trials (RCTs) of acupuncture and electroacupuncture and a meta-analysis of data from three studies suggests acupuncture relieves pain in peripheral joint OA compared with sham acupuncture (Kwon et al 2006). This is supported by a recent systematic review and meta–analysis of eight RCTs which concurs that acupuncture is superior to sham acupuncture or usual care and suggests the effect size is comparable to that of nonsteroidal anitiinflammatory drugs (NSAIDs) whilst having fewer side effects (White et al 2007). However, the addition of acupuncture to a course of advice and exercise for osteoarthritis of the knee provided no further improvement in function and pain (Foster et al 2007) and whilst the National Institute of Health and Clinical Excellence recommended acupuncture for low back pain, their osteoarthritis guidelines do not (NICE 2008, 2009).
In patients with RA acupuncture does not alter pain, medication use or disease activity (Casimiro et al 2002). In patients with fibromyalgia, the evidence of effectiveness is mixed (Berman et al 1999, Mayhew & Ernst 2007, Sim & Adams 2002); some studies report short-lived, small beneficial effects (Deluze et al 1993, Guo & Jia 2005, Martin et al 2006) and others report no positive effects of acupuncture (Assefi et al 2005, Sprott 1998). Consequently, acupuncture is only recommended for short-term pain control in peripheral joint OA (Kwon et al 2006, White et al 2007) and in osteoporosis (Chartered Society of Physiotherapy 1999) but not in fibromyalgia (Mayhew & Ernst 2007) or RA (Casimiro et al 2005).
THERMOTHERAPY AND CRYOTHERAPY
Thermotherapy (the therapeutic application of a heating agent) and cryotherapy (the therapeutic application of a cooling agent) are widely used treatments to reduce pain, oedema and muscle spasm, improve tissue healing and facilitate range of motion and function. Clinically, superficial heating can be achieved by conductive methods, such as heat pads or paraffin wax baths, by radiation such as infra red light therapy and by convection, such as sauna or steam room (Hicks & Gerber 1992). Heating of the deeper tissues can be achieved by short wave diathermy (electromagnetic energy) and high doses of ultrasound therapy, which are discussed earlier in this chapter. Cryotherapy includes the use of ice packs and ice baths, commercially available gel packs or sprays and massage with ice over acupuncture points or painful areas.
Prior to application of either therapy, skin testing to establish normal cutaneous sensation is recommended as both heat and cold therapy have a measurable effect on surface and intra-articular temperature of joints, skin micro-circulation and core temperature (Oosterveld et al 1992) and patients with abnormal cutaneous sensation (e.g. diabetic neuropathy) are at risk of damage (Fox & Sharp 2007).
Thermotherapy and cryotherapy produce analgaesia via the pain gate theory (Melzack & Wall 1965) and reduce muscle spasm. However, thermotherapy increases tissue temperature, blood flow, metabolism and connective tissue extensibility, whilst cryoptherapy decreases tissue blood flow by initially causing vasoconstriction followed by vasodilatation (the ‘hunting reflex’), reducing tissue metabolism, oxygen utilization, inflammation and connective tissue extensibility (Box 8.2). Whilst there are differences in physiological responses, both therapies can be used in patients with rheumatic conditions and patient preference as well as physiological response should be considered when selecting which therapy to use.
BOX 8.2 The physiological changes in response to heat and cold therapy
| CRYOTHERAPY | THERMOTHERAPY | |
|---|---|---|
| Pain | ↓ | ↓ |
| Muscle spasm | ↓ | ↓ |
| Metabolism | ↓ | ↑ |
| Blood flow | ↓ | ↑ |
| Inflammation | ↓ | ↑ |
| Oedema | ↓ | ↑ |
| Connective tissue extensibility | ↓ | ↑ |
Despite being used for years as a safe and effective symptomatic treatment of rheumatic conditions, systematic reviews of thermotherapy and cryotherapy highlight a lack of good quality research (Brosseau et al 2003b). In patients with RA, hot or cold therapy has no effect on pain, swelling, ROM, strength or function (Dellhag et al 1992, Ivey et al 1994, Kirk & Kersley 1968, Rembe 1970); whereas ice massage improves pain, joint mobility and function in patients with knee OA (Yurtkuran & Kocagil 1999) and ice packs reduce swelling (Hecht et al 1983) and improve range of movement (Lin 2003) but may not relieve symptoms in painful peripheral joint conditions (Clarke et al 1999). Similarly, short-term application of hot packs are not useful in peripheral joint osteoarthritis (Hecht et al 1983) but may control pain and improve disability if applied for longer periods to patients with acute non specific low back pain (Nadler et al 2003a, 2003b).
Based on some evidence and anecdotal reports of effectiveness, thermotherapy and cryotherapy are useful palliative self management therapies for rheumatic patients and should be included in the management of patients with RA (Brosseauet al 2004), OA (Brosseau et al 2004, NICE 2008, Zhang et al 2007) and osteoporosis (Chartered Society of Physiotherapy 1999).
MANUAL THERAPY
Manual therapy is the skilled application of passive movement to a joint either within (‘mobilisation’) or beyond its active range of movement (‘manipulation’). This includes oscillatory techniques, high velocity low amplitude thrust techniques, sustained stretching and muscle energy techniques. Manual therapy can be applied to joints, muscles or nerves and the aims of treatment include pain reduction, increasing range and quality of joint movement, improving nerve mobility, increasing muscle length and restoring normal function. There are three paradigms for its therapeutic effects; physiological, biomechanical or physical, and psychological (Fig. 8.4).
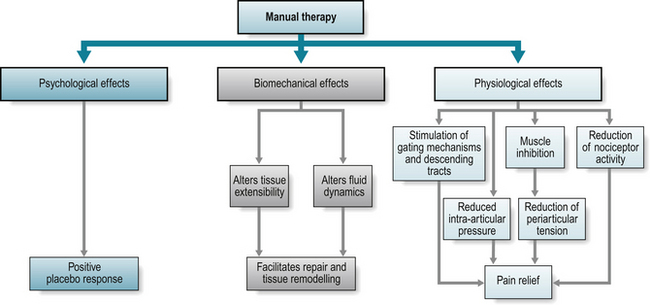
The physiological effects of manual therapy include the reduction of pain via the pain gate theory (Melzack & Wall 1965) and stimulation of the descending inhibitory tracts. Indirectly, manual therapy can reduce pain via inhibition of muscle spasm which reduces tension on the periarticular structures, lowering intraarticular pressure, or reduces nociceptor activity (Zuzman 1986).
The biomechanical effects of manual therapy include altering tissue extensibility and fluid dynamics thus facilitating repair and remodelling. Temporary increases in tissue extensibility following manual therapy occur through the mechanisms of creep (tissue lengthening following application of a constant force or load) and preconditioning (elongation following repeated loading) (Panjabi & White 2001). More permanent length changes need sufficient force, which are achieved in spinal manual therapy (Harms & Bader 1997), to produce microtrauma which elongates collagenous tissues (Threlkeld 1992). Repetitive movement of inflamed joints alters fluid dynamics, reducing intra articular pressure (Jayson & Dixon 1996, Levick 1979, Nade & Newbold 1983), increasing the rate of synovial blood flow and synovial fluid clearance (James et al 1994) thus improving range and movement quality.
The psychological effects of manual therapy or any therapy which has direct physical contact, such as massage, produces a response to the ‘laying on of hands’. This placebo response (a response produced by a mechanism with incidental ingredients or components which have no remedial effect for the disorder but result in a positive effect of treatment) is enhanced by ‘learned expectancy’ (previous experience of a stimuli establishes an habitual direction of response) and the therapeutic benefits of the patient – therapist interaction and relationship (Roche 2002).
Manual therapies are commonly used interventions regardless of reported non vascular and vascular side effects (Ernst 2007). Whilst mobilisations (movement to a joint within its physiological range of movement) are not associated with serious complications, manipulations (high velocity low amplitude trust techniques applied beyond active joint range of movement) can have severe adverse reactions. Spinal manipulation, particularly when performed on the cervical spine, is associated with mild to moderate adverse effects (30-61% of all patients) and can result in serious complications such as vertebrobasilar artery dissection followed by stroke (Ernst 2007, Taylor & Kerry 2005). Consequently, premanipulative testing protocols attempt to identify patients at risk of vertebrobasilar artery insufficiency (Magarey et al 2004) although the effectiveness of this screening has yet to be established. All guidelines contraindicate the use of manipulation in patients with RA due to the risk of joint instability particularly in the upper cervical spine (Neva et al 2006) and caution should be exercised when considering the use of manipulation in other inflammatory rheumatic conditions.
Whilst there is some evidence of the effectiveness of manual therapy in the treatment of acute and sub acute spinal pain (Bronfort et al 2004, Ferreira et al 2006, UK BEAM trial team 2004) in patients with peripheral joint disease manual therapy is often combined with other therapies which makes the relative contribution of each therapy difficult to determine (Deyle et al 2005). In patients with OA knee, a combination of manual therapy and exercise improves function and pain more than exercise (Deyle et al 2005). In patients with hip OA manual therapy improves pain, range of movement and function more than exercise alone (Hoeksma et al 2004). Those patients with the severest x-ray changes respond least to manual therapy although baseline levels of function, pain and range of movement do not predict treatment response (Hoeksma et al 2005). Consequently, evidence-based practice guidelines recommend the use of manual therapy combined with exercise for the reduction of pain in peripheral joint osteoarthritis (Brosseau et al 2005, NICE 2008).
MASSAGE
Massage has been used to reduce pain and oedema, increase circulation, improve muscle tone and enhance joint flexibility for years. Its effect may be explained by the pain gate theory (Melzack & Wall 1965) but it is also likely to have a placebo response similar to other manual therapies.
Evidence of its efficacy in rheumatic patients is limited; a course of massage improves function and pain in patients with OA knee (Perlman et al 2006) and pain and quality of life in patients with fibromyalgia (Brattberg 1999) although it is ineffective in patients with neck pain (Ezzo et al 2007). However, a systematic review of nine studies suggests massage is beneficial in patients with sub acute and chronic non-specific low back pain especially when combined with exercise and education but it was no better than manipulation and inferior to TENS for back pain relief (Furlan et al 2003). Whilst massage is not often recommended in clinical guidelines, as it has high patient satisfaction and low adverse effects it is a viable adjunct to therapy for patients with rheumatic disease.
CONCLUSION
Physical therapies are often used in the management of rheumatic conditions to relieve pain and improve function. Within the biopsychosocial model of health, physical therapies influence the ‘bio’ element of this framework but, if self administered, may enhance an individual’s ability to cope with their condition, thus improving their quality of life. Whilst there is some evidence for their efficacy (whether they work under ideal, controlled circumstances), evidence to support their clinical effectiveness (whether they work in usual clinical practice) remains weak.
There is some evidence that thermotherapy, TENS, and acupuncture can relieve pain in some rheumatic conditions but insufficient evidence for the efficacy of many electrotherapy interventions and manual therapy. However, insufficient evidence of effectiveness should not be interpreted as ‘ineffective’ – it also indicates an absence of evidence. Therefore clinical decisions should be made following a thorough assessment of an individual’s symptoms and treatment based on the available good quality evidence (basic principles and clinical effectiveness), practice guidelines, clinical experience and patient preference (Jones 1995) until a sufficient body of good quality studies are completed to unequivocally direct the use of physical therapies in the management of rheumatic disease.
Review the current guidelines for the management of rheumatoid arthritis (RA) on the NICE website (http://guidance.nice.org.uk) and consider which physical modalities may be included in an evidence based treatment programme for a patient with moderate, well controlled RA. Access the ‘electrotherapy on the web – an educational resource’ website (www.electrotherapy.org) and review the theories and evidence underpinning the use of transcutaneous electrical nerve stimulation (TENS). Consider how you would explain these concepts to a patient who is using TENS for pain relief, within the biopyschosocial framework.www.electrotherapy.org/ accessed January 2009.
www.macpweb.org accessed January 2009.
www.csp.org.uk accessed January 2009.
References and further reading
Almeida T.F., Roizenblatt S., Benedito- Silva A.A., et al. The effect of combined therapy (ultrasound and interferential current) on pain and sleep in fibromyalgia. Pain. 2003;104(3):665-672.
Assefi N., Sherman K., Jacobsen C., et al. A randomised clinical trial of acupuncture compared with sham acupuncture in fibromyalgia. Ann. Intern. Med.. 2005;143:10-21.
Berman B.M., Ezzo J., Hadhazy V., et al. Is acupuncture effective in the treatment of fibromyalgia? J. Fam. Pract.. 1999;48(3):213-218.
Bircan C., Senocak O., Peker O., et al. Efficacy of two forms of electrical stimulation in increasing quadriceps strength: a randomised controlled trial. Adv. Clin. Rehabil.. 2002;16(2):194-199.
Brattberg G. Connective tissue massage in the treatment of fibromyalgia. Eur. J. Pain.. 1999;3(3):235-244.
Bronfort G.H.M., Evans R.L., Bouter L.M. Efficacy of spinal manipulation and mobilization for low back pain and neck pain: a systematic review and best evidence synthesis. J. Spine.. 2004;4(3):335-356.
Brosseau, L., Judd, M.G., Marchand, S., et al., 2003a. Transcutaneous electrical nerve stimulation (TENS) for the treatment of rheumatoid arthritis in the hand. Cochrane. Database. Syst. Rev. 3 (CD004377).
Brosseau L., Wells G.A., Tugwell P., et al. Ottawa panel evidence based clinical practice guidelines for electrotherapy and themotherapy interventions in the management of rheumatoid arthritis. Phys. Ther.. 2004;8(11):1016-1143.
Brosseau L., Wells G.A., Tugwell P., et al. Ottawa panel evidence-based clinical practice guidelines for therapeutic exercises and manual therapy in the management of osteoarthritis. Phys. Ther.. 2005;85(9):907-971.
Brosseau L., Yonge K.A., Robinson V., et al. Thermotherapy for treatment of osteoarthritis. Cochrane. Database. Syst. Rev.. 2003;4:1-8.
Callaghan M.J., Whittaker P.A., Grimes S. An evaluation of pulsed shortwave on knee osteoarthritis using radioleucoscintigraphy: a pragmatic randomised, double bind controlled trial. Joint. Bone. Spine.. 2000;72:150-155.
Cao, X. 2002. Scientific bases of acupuncture analgesia. Acupuncture Electrotherapy Research, 27(1):1-14.
Casimiro L., Barnsley L., Brosseau L., et al. Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis. Cochrane. Database. Syst. Rev.. 2005;4:1-16. (CD003788)
Casimiro, L., Brosseau, L., Robinson, V., et al., 2002. Therapeutic ultrasound for the treatment of rheumatoid arthritis. Cochrane. Database. Syst. Rev. 3 (CD003787).
Chartered Society of Physiotherapy. Physiotherapy guidelines for the management of osteoporosis. London: Chartered Society of Physiotherapy; 1999.
Cheung R.S., Pomeranz B.P. Electroacupuncture analgesia could be mediated by at least two pain-relieving mechanisms; endorphin and non-endorphin systems. Life. Sci.. 1979;25(23):1957-1962.
Clarke G.R., Willis L.A., Stenner L., et al. Evaluation of Physiotherapy in the treatment of osteoarthritis of the knee. Rheumatol. Rehabil.. 1999;13:190-197.
Dellhag B., Wollersjö I., Bjelle A. Effect of active hand exercise and wax bath treatment in rheumatoid arthritis patients. Arthritis. Care. Res.. 1992;5(2):87-92.
Deluze C., Bosia L., Zirbs A., et al. Electroacupuncture in fibromyalgia: results of a randomised controlled trial. Br. Med. J.. 1993;306:393.
Deyle G.D., Allison S.C., Matekel R.L., et al. Physical therapy treatment effectiveness for osteoarthritis of the knee: a randomized comparison of supervised clinical exercise and manual therapy procedures versus a home exercise program. Phys. Ther.. 2005;85(12):1301-1317.
Ernst E. Acupuncture as a symptomatic treatment of osteoarthritis. A systematic review. Scand. J. Rheumatol.. 1997;26(6):444-447.
Ernst E. Adverse effects of spinal manipulation: a systematic review. J. R. Soc. Med.. 2007;100(7):330-338.
Ezzo J.H.B.G., Gross A.R., Myers C.D., et al. Cervical Overview Group. Massage for mechanical neck disorders: a systematic review. Spine. 2007;32(3):353-362.
Ferreira P.H., Ferreira M.L., Maher C.G., et al. A specific stabilisation exercise for spinal and pelvic pain: A systematic review. Aust. J. Physiother.. 2006;52:79-88.
Fitzgerald G.K., Piva S.R., Irrgang J.J. A modified neuromuscular electrical stimulation protocol for quadriceps strength training following anterior cruciate ligament reconstruction. J. Orthop. Sports. Phys. Ther.. 2003;33(9):492-501.
Foster, N.E., Thomas, E., Barlas, P., et al., 2007. Acupuncture as an adjunct to exercise based physiotherapy for osteoarthritis of the knee: randomised controlled trial. Br. Med. J. 335 (Sep).
Fox J., Sharp T. Practical Electrotherapy - a guide to safe application. London: Elsevier; 2007.
Furlan, A.D., Brosseau, L., Imamura, M., et al., 2003. Massage for low back pain (Cochrane review). Cochrane. Libr. (2).
Galea M. Neuroanatomy of the nocioceptive system. In: Baxter G.D., editor. Pain: a Textbook of Pain for Therapists. Edinburgh: Harcourt publishers; 2002:13-41.
Guo X., Jia J. Comparison of therapeutic effects on fibromyalgia syndrome between dermal-neurological electric stimulation and electric acupuncture. Chin. J. Clin. Rehabil.. 2005;9:171-173.
Harms M.C., Bader D.L. Variability of forces applied by experienced therapists during spinal mobilisation. Clin. Biomech.. 1997;12(6):393-399.
Hecht P.J., Backmann S., Booth R.E., et al. Effects of thermal therapy on rehabilitation after total knee arthroplasty: a prospective randomised study. Clin. Orthop. Relat. Res.. 1983;178:198-201.
Hicks J.E., Gerber L.H. Rehabilitation of patients with osteoarthritis. In: Moskiwitz R.W., Howell D.S., Goldberg V.M., et al, editors. Osteoarthritis: Diagnosis Medical and Surgical Management. WB Saunders Co; 1992:427-464.
Hill J., Lewis M., Mills P. Pulsed short wave diathermy effects on human fibroblast proliferation. Arch. Phys. Med. Rehabil.. 2002;83:832-836.
Hoeksma H.L., Dekker J., Ronday H.K., et al. Manual therapy in osteoarthritis of the hip: outcome of subgroup analysis. Rheumatology. 2005;44:461-464.
Hoeksma H.L., Dekker J., Ronday H.K., et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a randomised clinical trial. Arthritis. Rheum.. 2004;51(5):722-729.
Ivey M., Johnston R.V., Uchida T. Cryotherapy for postoperative pain relief following knee arthroplasty. J. Arthroplasty.. 1994;9(3):285-290.
James M.L., Cleland L.G., Gaffney R.D., et al. The effect of exercise on 99mTc-DTPA clearance from knees with effusions. J. Rheumatol.. 1994;21:501-504.
Jan M.H., Chai H.M., Wang C.L., et al. Effects of repetitive shortwave diathermy for reducing synovitis in patients with knee osteoarthritis: an ultrasonographic study. Phys. Ther.. 2006;86(2):236-244.
Jayson M.I., Dixon A.S.J. Intra articular pressure in rheumatoid arthritis of the knee: Pressure changes during joint use. Ann. Rheum. Dis.. 1996;29:401-408.
Jones M. Clinical reasoning and pain. Man. Ther.. 1995;1:17-24.
Kendall, N.S. (1997). Guide to assessing psycho-social yellow flags in acute low back pain: risk factors for long term disability and work loss Wellington, New Zealand: Accident and Compensation commission of New Zealand and the National Health Committee
Kirk J.A., Kersley G.D. Heat and cold in the physical treatment of rheumatoid arthritis of the knee: A controlled clinical trial. Ann. Phys. Med. Rehabil.. 1968;9(7):270-274.
Kitchen S., Partridge C. A survey to examine clinical use of ultrasound, shortwave diathermy and laser in England. Br. J. Ther. Rehabil.. 1996;3(12):644-650.
Kitchen S., Partridge C. Review of shortwave diathermy continuous and pulsed patterns. Physiotherapy. 1992;78:243-252.
Klaber Moffett J., Richardson P., Frost H., et al. Placebo controlled, double blind trial to evaluate the effectiveness of pulse short wave therapy for osteoarthritic hip and knee pain. Pain. 1996;167:121-127.
Kwon Y.D., Pittler P.H., Ernst E. Acupuncture for peripheral joint osteoarthritis. A systematic review and meta-analysis. Rheumatology. 2006;45(11):1331-1337.
Laufer Y., Zilberman R., Porat R. Effect of pulsed shortwave diathermy on pain and function of subjects with osteoarthritis of the knee: a placebo controlled, double blind clinical trial. Clin. Rehabil.. 2005;19:255-263.
Levick J.R. An investigation into the validity of subatmospheric pressure recordings from synovial fluid and their dependence on joint angle. J. Physiol.. 1979;289:55-67.
Lin Y.H. Effects of thermal therapy in improving the passive range of knee motion: comparison of cold and superficial heat applications. Clin. Rehabil.. 2003;17(6):618-623.
Low J. Dosage of some pulsed short wave diathermy trials. Physiotherapy. 1995;81:611-616.
Magarey M.E., Rebbeck T., Coughlan B., et al. Pre-manipulative testing of the cervical spine review, revision and new clinical guidelines. Man. Ther.. 2004;9(2):95-108.
Martin D., Sletten C., Williams B., et al. Improvement in fibromyalgia symptoms with acupuncture; results of a randomised controlled trial. Mayo. Clin. Proc.. 2006;81:749-757.
Maxwell L. Therapeutic ultrasound: its effects on the cellular and molecular mechanisms of inflammation and repair. Physiotherapy. 1992;78(6):421-426.
Mayhew E., Ernst E. Acupuncture for fibromyalgia-a systematic review of randomised clinical trials. Rheumatology. 2007;46:801-804.
Melzack R., Wall P.D. Pain mechanisms: a new theory. Science. 1965;150:971-979.
Mortimer A.J., Dyson M. The effect of therapeutic ultrasound on calcium uptake in fibroblasts. Ultrasound. Med. Biol.. 1988;14(6):499-506.
Nade S., Newbold P.J. Factors determining the level and changes in intra articular pressure in the knee joint of the dog. Am. J. Physiol.. 1983;338:21-36.
Nadler S.F., Steiner D.J., Erasala G.N., et al. Continuous low-level heat wrap therapy for treating acute non specific low back pain. Arch. Phys. Med. Rehabil.. 2003;84(3):329-334.
Nadler S.F., Steiner D.J., Petty S.R., et al. Overnight use of continuous low-level heat wrap therapy for relief of low back pain. Arch. Phys. Med. Rehabil.. 2003;84(3):335-342.
Neva M.H., Hakkinen A., Makinen H., et al. High prevalence of asymptomatic cervical spine subluxation in patients with rheumatoid arthritis waiting for orthopaedic surgery. Ann. Rheum. Dis.. 2006;65(7):884-888.
NICE, 2008. National Institute for Health and Clinical Excellence. Osteoarthritis: national clinical guideline for care and management in adults. London: NICE www.nice.org.uk/CG059www.nice.org.uk/CG059.
NICE, 2009. National Institute for Health and Clinical Excellence. The early management of persistent non specific low back pain. May 2009. London: NICE www.nice.org.uk/CG in press.
Nussbaum E.L. Ultrasound to heat or not to heat: that is the question. Phys. Ther. Rev.. 1997;2:59-72.
Oldham J.A., Stanley J.K. Rehabilitation of atrophied muscle in the rheumatoid arthritic hand: a comparison of two methods of electrical stimulation. J. Hand. Surg.. 1989;14(3):294-297.
Oosterveld F.G.J., Rasker J.J., Jacobs J.W.G., et al. The effect of local heat and cold therapy on the intra articular and skin surface temperature of the knee. Arthritis. Rheum.. 1992;35:146-151.
Osiri, M., Welch, V., Brosseau, L., et al., 2000. Transcutaneous electrical nerve stimulation for knee osteoarthritis. Cochrane. Database. Syst. Rev. 4 (CD002823).
Panjabi M.M., White A.A. Biomechanics in the musculoskeletal system. New York: Churchill Livingstone; 2001.
Perlman A.L., Sabrina A., Williams A.-L., et al. Massage therapy for osteoarthritis of the knee. A randomised controlled trial. Arch. Intern. Med.. 2006;166:2533-2538.
Philadelphia Panel. Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for knee pain. Phys. Ther.. 2001;81(10):1675-1700.
Rembe E.C. Use of cryotherapy on the postsurgical rheumatoid hand. Phys. Ther.. 1970;50(1):19-23.
Robertson V., Ward A., Low J., Reed A. Electrotherapy Explained. Principles and Practice, 7th edn. London: Elsevier; 2006.
Robertson V.J., Baker K.G. A review of therapeutic ultrasound: effectiveness studies. Phys. Ther.. 2001;81(7):1339-1350.
Roche P. Placebo and patient care. Gifford L., editor. Topical issues in Pain; Placebo and nocebo, pain management, muscles and pain, Vol. 4. Falmouth: CNS Press Limited. 2002:19-41.
Sim J., Adams N. Systematic review of randomized controlled trials of nonpharmacological interventions for fibromyalgia. Clin. J. Pain.. 2002;18(5):324-336.
Sprott H. Efficiency of acupuncture in patients with fibromyalgia. Clin. Bull. Myofacial Ther.. 1998;3:37-43.
Strojnik V. The effects of superimposed electrical stimulation of the quadriceps muscles on performance in different motor tasks. J. Sports. Med. Phys. Fitness.. 1998;38(3):194-200.
Talbot L.A., Gaines J.M., Ling S.M., et al. A home-based protocol of electrical muscle stimulation for quadriceps muscle strength in older adults with osteoarthritis of the knee. Br. J. Rheumatol.. 2003;30(7):1571-1578.
Taylor A.J., Kerry R. Neck pain and headache as a result of internal carotid artery dissection: implications for manual therapists. Man. Ther.. 2005;10(1):73-77.
Thamsborg G., Florescu A., Oturai P., et al. Treatment of knee osteoarthritis with pulsed electromagnetic fields: a randomized, double-blind, placebo-controlled study. Osteoarthritis. Cartilage.. 2005;13(7):575-581.
Threlkeld A.J. The effects of manual therapy on connective tissue. Phys. Ther.. 1992;72(12):893-902.
Tindle H.A., Davis R.B., Phillips R.S., et al. Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern. Ther. Health. Med.. 2005;11(1):42-49.
UK BEAM trial team. United Kingdom back pain exercise and manipulation (UK BEAM) randomised trial: effectiveness of physical treatments for back pain in primary care. Br. Med. J.. 2004;329(7479):1377. Dec 11
Van Nguyen J., Marks R. Pulsed magnetic fields for treating osteoarthritis. Physiotherapy. 2002;88:458-470.
Walker U.A., Uhl M., Weiner S.M., et al. Analgesic and disease modifying effects of interferential current in psoriatic arthritis. Rheumatol. Int.. 2006;10:904-907.
Watson, T. 2007. Electrotherapy on the web-an educational resource Accessed 2009 www.electrotherapy.org/
Watson T. The role of electrotherapy in contemporary physiotherapy practice. Man. Ther.. 2000;5(3):132-141.
Welch, V.B.L., Peterson, J., Shea, B., et al., 2001. Therapeutic ultrasound for osteoarthritis of the knee. Cochrane. Database. Syst. Rev. 3 (CD003132).
White A., Hayhoe S., Hart A., et al. Adverse events following acupuncture: prospective survey of 32 000 consultations with doctors and physiotherapists. Br. Med. J.. 2001;323(7311):485-486.
White A., Foster N.E., Cummings M., et al. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology. 2007;46(March):384-390.
Yurtkuran M., Kocagil T. Electroacupuncture and ice massage: comparison treatment for osteoarthritis of the knee. Am. J. Acupunct.. 1999;27:133-140.
Zhang W., Doherty M., Leeb B.F., et al. EULAR evidence based recommendations for the management of hand osteoarthritis: report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis.. 2007;66(3):377-388.
Zuzman M. Spinal manipulative therapy: review of some proposed mechanisms, and a new hypothesis. Aust. J. Physiother.. 1986;32(2):89-99.