21 Feline symmetrical alopecia
INTRODUCTION
Symmetrical alopecia is a common presentation in the cat. Historically, the alopecia was thought to be due to an endocrinopathy because of the lack of any apparent inflammation in many cases. It is now known that the majority of cases of symmetrical alopecia are due to pruritus. There are many causes for symmetrical alopecia, including parasitic and allergic disease, and a thorough and systematic investigation is indicated in recurrent disease to try to identify and correct the underlying cause.
CASE HISTORY
As in all dermatology cases, a thorough history (see Chapter 1) is essential in making an accurate diagnosis. Frequently, in cases of symmetrical alopecia, the client may be unaware that the cat is actually overgrooming.
The history in this case was as follows:
CLINICAL EXAMINATION
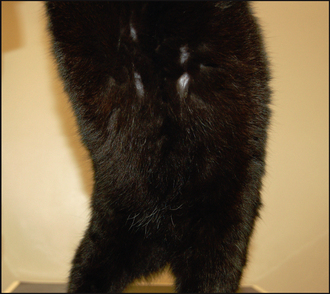
Feline symmetrical alopecia usually presents as non-inflammatory hair loss, although there may be evidence of focal excoriations. The most frequently affected areas include the neck, forelimbs, groin and flanks.
There are four main categories of disease that result in pruritus in cats: parasites; infections; hypersensitivity disorders; and a diverse fourth group which includes some infectious, autoimmune, metabolic and neoplastic diseases amongst others. When drawing up a list of differential diagnoses with a view to further investigation, it is important to initially rule out/treat parasitic infestations before considering the infectious and allergic causes of pruritus. Pruritus is often multifactorial and a methodical approach, following a series of sequential diagnostic rule-outs, will maximize the chances of making a diagnosis and instituting successful treatment and management.
In this case, there was a history of flea exposure, but thorough flea control had been instituted with no improvement, so flea allergy dermatitis, as a sole cause of the pruritus, was unlikely. Nevertheless, flea allergy dermatitis could still be involved and thorough flea control would need to be maintained. A limited antigen diet trial had been tried, but only for 4 weeks, and this is too short a period to be able to thoroughly exclude a cutaneous adverse food reaction. Ideally, a diet trial should be continued for a minimum of 6 weeks and on occasion for as long as 3 months. There was no history of an anxiety-inducing situation, but psychogenic alopecia should be considered where there is symmetrical alopecia.
CASE WORK-UP
The initial diagnostic tests taken at the first examination were to investigate the possible involvement of ectoparasitism and to rule out the involvement of dermatophytosis.
The following diagnostic tests were undertaken:
The first stage in the investigation of feline pruritus, whatever the presentation, is to rule out the involvement of ectoparasitism, particularly fleas. Visual examination for evidence of flea infestation, and microscopic examination of scale and skin scrapes for the detection of ectoparasites, are insensitive methods and thorough treatment of the patient, all in-contact animals and the household (and possibly car) environments is always indicated in these cases. If there has been no response to thorough ectoparasitic therapy, a diet trial and possibly intradermal and/or an ELISA environmental panel are indicated. Thus, the following further investigations were conducted:
Trial ectoparasitic treatment: Good flea control was already in place, but in order to be confident about ruling out the involvement of cheyletiellosis, all animals were treated with fortnightly applications of selamectin for a period of 4 weeks. There was no response to this and the cat continued to overgroom. Monthly applications of fipronil were continued after the trial selamectin therapy.
Diet trial: An extended, 10-week, restricted antigen diet trial was conducted, feeding a proprietary capelin and tapioca food. To give relief from pruritus, for the first 4 weeks of the trial the patient was treated with prednisolone (10 mg s.i.d. for 1 week then 5 mg s.i.d. for 1 week then 5 mg every other day). Re-examination after 4 weeks showed a marked improvement, with resolution of overgrooming and some hair regrowth over affected areas, but marked polyphagia had been evident and the cat had gained weight. After a further 6 weeks, there was recrudescence of overgrooming and alopecia.
Intradermal testing: An intradermal test was performed on completion of the diet trial, which gave positive reactions to the house dust mite Dermatophagoides farinae, the storage mites Acarus siro and Tyrophagus putrescentiae, as well as sheep epithelia, mixed feathers, couch grass, orchard grass, lambs quarter and alder.
Note that intradermal and serological allergy testing are less reliable and can be harder to interpret in the cat compared to the dog; nevertheless, some cats will produce strong positive reactions to one or both tests. The main reason to conduct these tests is for selection of allergens for immunotherapy.
DIAGNOSIS
The history, clinical signs, lack of response to thorough ectoparasitic therapy, and the extended diet trial and the positive intradermal test all supported and confirmed a diagnosis of atopic dermatitis. As with any investigation of pruritus, a positive intradermal test (or ELISA panel) alone would not support the diagnosis of atopic dermatitis, as healthy animals are frequently positive on these tests and a positive test does not rule out the involvement of the other differentials.
PROGNOSIS
Although atopic dermatitis is a lifelong, incurable condition, the prognosis for effective control of symptoms and a good quality of life is good in the majority of cases, although some cases can be challenging to manage.
AETIOPATHOGENESIS OF SYMMETRICAL ALOPECIA
The non-inflammatory nature of most cases of symmetrical alopecia in cats, and the response to ‘hormonal’ therapies such as megestrol acetate, initially led to the misconception that feline symmetrical alopecia was a hair growth cycle disorder, possibly an endocrinopathy. It is now known that, in the majority of cases, the alopecia is due to pruritus and the resulting self-trauma. There are, however, some rarer causes of symmetrical alopecia that are due to causes other than pruritus (see Chapter 28). Table 21.1 lists the common and some less common causes of symmetrical alopecia in cats.
Table 21.1 Causes of symmetrical alopecia in cats
Feline cutaneous reaction patterns
There are three other frequently encountered manifestations of feline pruritus: head and neck pruritus, miliary dermatitis, and lesions of the eosinophilic granuloma complex. These three presentations, along with symmetrical alopecia, have been termed the feline cutaneous reaction patterns. Cats may present with more than one reaction pattern at any one time. The recognition of one of the feline reaction patterns does not constitute a diagnosis, and although initial symptomatic therapy may be quite appropriate, further investigation is indicated for cats with recurrent disease, in order to try and establish the underlying cause of the pruritus and institute specific therapy for it. It is common for cats presenting with any of the feline cutaneous reaction patterns to have multiple diseases, including atopic dermatitis, flea allergy dermatitis and a cutaneous adverse food reaction.
Because of the diverse nature of the possible differential diagnoses, a systematic approach to the diagnosis is required. The work-up of such a case can be protracted and challenging, and it is important that the client understands from the outset the nature of such an investigation. The client must be committed and good communication is vital for a successful outcome. Cats can be very uncooperative with respect to diagnostic procedures and, at times, the necessity to treat symptoms to prevent further suffering can hinder diagnostic procedures.
EPIDEMIOLOGY
Symmetrical alopecia is a frequent clinical presentation and many of the underlying causes are encountered on a daily basis. The alopecia in this case was due to atopic dermatitis. The incidence of atopic dermatitis in cats is controversial. Most reports would suggest that this is a common disease and may perhaps be the most common feline allergic skin disease in geographical areas where the prevalence of fleas is low. An inherited predis-position has not been documented, although there are reports of familial involvement that do suggest a genetic component. No breed or sex predilections have been demonstrated, but young cats appear to be predisposed.
TREATMENT OPTIONS
Prior to starting treatment, the clinician should spend time discussing with the client the various options for treatment, their efficacy, cost and likely side-effects. The treatment choices available are essentially similar to those detailed in Chapter 6 for the treatment of canine atopic dermatitis, and include allergen avoidance and the use of antihistamines, essential fatty acid supplementation, glucocorticosteroids, ciclosporin and allergen-specific immunotherapy.
Antihistamines and essential fatty acid supplementation: Antihistamine therapy and/or essential fatty acid supplementation may be of benefit in the management of feline symmetrical alopecia due to atopic dermatitis. Antihistamine therapy in cats seems to be a more effective therapy for pruritus in comparison to dogs. Chlorphenamine (chlorpheniramine) is considered the antihistamine of choice when treating feline atopic dermatitis. The use of concurrent antihistamine and essential fatty acid supplementation gave an improved response in one study.
The following antihistamines may be of benefit:
Glucocorticoids: In general, the long-term use of glucocorticoids should be avoided, but because of their high good efficacy and low cost, glucocorticoids are commonly used for the management of feline allergic skin disease. Certainly, when there are financial constraints, they are probably the most appropriate treatment. Additionally, there is an argument for the use of glucocorticoids in cats with seasonal hypersensitivities where treatment is only required for a few months of the year.
Alternate-day therapy allows the hypothalamic–adrenal–pituitary axis time for recovery and makes the long-term use of glucocorticoids safer than daily treatment. Thus, the shorter-acting glucocorticoids, prednisolone or methylprednisolone, are the most ap-propriate drugs for the management of feline atopic dermatitis.
Although the use of short-acting glucocorticoids is preferred, it may be necessary to use longer-acting injectable products when it is not possible for owners to administer oral therapy to cats.
In general, cats are more resistant to, and develop fewer side-effects to, glucocorticoids in comparison to dogs. However, polyphagia, excessive weight gain, diabetes mellitus and, in rare cases, skin fragility syndrome are all potential side-effects. In addition, the onset of congestive heart failure has been documented in cats following glucocorticoid administration, in particular following treatment with methylprednisolone acetate.
Prednisolone dosage and administration:
Ciclosporin: Although an unlicensed product in the UK, clinical experience and a limited number of studies have shown ciclosporin to be a beneficial treatment for feline atopic dermatitis. It seems to be effective at an initial dosage of 5–7 mg/kg s.i.d. and in some cases it may be possible to reduce to alternate-day or twice-weekly therapy following a good response to daily dosage. Several weeks of therapy may be required before maximal response is seen. Side-effects may include gastrointestinal disturbance and gingival hyperplasia. Ciclosporin is a potent, immunosuppressive drug. There is at least one report of fatal toxoplasmosis in cats being treated with ciclosporin, and it is recommended to assess FIV, FeLV and toxoplasma serology prior to commencing therapy. It may be inadvisable to treat cats that are positive on toxoplasma serology.
Allergen-specific immunotherapy (ASIT): Immunotherapy is an option for treatment in cases where specific causative allergens have been identified. Many studies have demonstrated efficacy of immunotherapy for the treatment of feline atopic dermatitis. Reported response rates to immunotherapy vary between 50% and 75%. Certainly, in the authors’ experience this is a safe and in some cases highly beneficial therapy for the management of feline atopic dermatitis. One concern about the use of immunotherapy is the length of time it can take for any improvement to become apparent. The treatment should be continued for up to 1 year before being discontinued on the grounds of lack of efficacy.
Treatment in this case
When selecting treatment, consideration must be given to the severity of the case and the expectations and requirements of the owner. In this case, the patient was experiencing ongoing pruritus that required effective management.
Pruritus
As already stated, in some cases the owner may be unaware that the cat with symmetrical alopecia is pruritic. The following points may be helpful when documenting the pruritus:
Elizabethan collars
Some dermatologists recommend the use an Elizabethan collar following application of spot-on flea treatments to cats that are excessively overgrooming. There is a concern that the cat licks off and ingests the product, leading to apparent treatment failure. The collar is used for up to 48 hours following application.
Diet trials
Diet trials in cats are fraught with difficulty. Cats scavenge and will often obtain food from waste bins or be fed by well-meaning neighbours, and it is possible that many cases of food reactions in cats go undiagnosed for this reason. Consideration should be given to confining cats indoors for the duration of a diet trial, but the clinician should be aware that confinement might lead to overgrooming, as a result of boredom or stress. Cats can be fussy eaters and in the authors’ experience, they are more likely to eat a proprietary food than a home-cooked diet. Cyproheptadine, as well as having antihistaminic therapy, is also an appetite stimulant in cats and has been used to encourage cats to eat a restriction diet.
It is often necessary to control pruritus during a diet trial to prevent severe self-trauma. Glucocorticoid therapy should be used in these cases. A useful side-effect of this may be stimulation of the appetite, resulting in the cat eating the novel diet. Glucocorticoids should be withdrawn at least 2 weeks before completion of the restriction diet in order to be able to assess response. If the pruritus does not recur within a few days, continue the restricted diet for another month before provocative challenge with the original diet. Relapse of signs in association with challenge followed by improvement on re-institution of the restriction diet supports a diagnosis of a cutaneous adverse food reaction.
Client compliance
It is fair to say that in a number of cases of feline pruritus it is not possible to make a specific diagnosis. In the absence of a diagnosis, client compliance should be re-evaluated to ensure exclusion diets and trial therapies have been adhered to. If clinical symptoms persist, then other disease processes should be investigated and histopathology of biopsy samples, radiography, ultrasound, virus isolation and blood tests may be indicated.
Psychogenic alopecia
When all other differentials have been evaluated, psychogenic alopecia may be considered. It is important to stress that this is not a diagnosis that should be made on clinical signs alone and there should be a history of some stressful factors, such as:
The incidence of a psychogenic dermatosis as a sole cause of pruritus in the cat is considered by referral dermatologists to be extremely low, but in the authors’ opinion, psychogenic factors may exacerbate existing pruritic skin disease. Oriental breeds of cat may be at increased risk of developing psychogenic dermatosis, and cats that are inherently nervous, hyperaesthetic, fearful or shy are at increased risk.
FOLLOW-UP
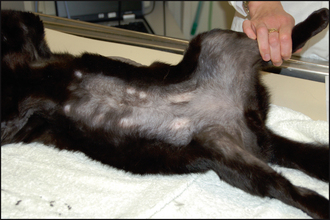
Within 8 weeks of starting treatment, there was complete regrowth of hair over the ventrum (Fig. 21.2). The frequency of administration of ciclosporin was reduced, initially to alternate-day therapy and then to twice weekly, over a 2-month period, without recurrence of self-trauma. At the time of writing, the cat is receiving monthly immunotherapy injections and twice-weekly ciclosporin at a dosage of 7 mg/kg. Over the next few months, attempts will be made to completely withdraw the ciclosporin therapy and to try and manage the pruritus on allergen-specific immunotherapy alone.