Chapter 13 Record and Report Writing
Introduction
Recording and report writing may not initially appear to be the most engaging aspect of clinical practice; however, it is a vital component within all settings. It is the professional duty of all occupational therapists to maintain accurate and up-to-date records, but little evidence or attention has been paid to this subject within the literature.
This chapter outlines the purpose and process of maintaining records and creating reports. Current themes in recording and format of care records are discussed. Aspects of recording and reporting the occupational therapy process are explored and examples provided. Finally, quality assurance and legal issues in recording and report writing are highlighted.
The focus of this chapter is on UK guidelines and standards, however, the principles are valid for good report writing internationally. Readers from other nations are recommended to follow this chapter up by consulting the specific guidance from their own professional body, national guidelines, standards and legislation.
What are records
The College of Occupational Therapists states that ‘care records include any material that holds information regarding an individual, collected as part of their care provision. Such material can be written, electronic, auditory or visual, and include computer or digital data, images, auditory or visual recordings, letters, notes, e-mails and duplicate copies’ (College of Occupational Therapists 2006a: 1).
In addition, there are some less obvious types of information that should be incorporated into care records. The occurrence, content and outcomes of any decisions made after discussions within supervision, or during official or unofficial discussions concerning the client, should be recorded in care records. If the practitioner is following specific national or local guidelines, procedures, care pathways or other standard process, this should also be demonstrated and recorded in the care record. It is also important to document fully all activity, including frequent and repetitious activities, otherwise they cannot be proven to have occurred. A client’s response to all outcomes should be recorded. Similarly, if a planned intervention does not occur, perhaps due to client non-attendance, this should be recorded with an explanation if possible. ‘This demonstrates that the therapist’s planning and care was disrupted for unavoidable reasons and that it was not withheld, or not provided, due to lack of organizational skills or lack of competence’ (College of Occupational Therapists 2006a: 5).
Purpose of records
The Department of Health states that, as high-quality information underpins the delivery of high-quality evidence-based health care, all information needs to be accurate, up to date and accessible in order:
Care records should provide an accurate record of a client’s condition over time, detailing the assessment, planning and delivery of the care provided and its evaluation. In turn this will:
Content and quality of records
The Professional Standards for Occupational Therapy Practice require that practitioners in all settings, keep records of ‘all occupational therapy activity and intervention made with, or on behalf of, the service user’ (College of Occupational Therapists 2003: 35).
Records must demonstrate everything that has been done for or with a client, including the clinical reasoning behind the care planning and provision. Occupational therapists need to demonstrate the outcomes of the care they have provided for the benefit of the client and others in the care team who have access to the records (College of Occupational Therapists 2006a).
To ensure good-quality care records, the Department of Health (2005) states that all organisations need to ensure that their staff are fully trained in record creation and maintenance, including having an understanding of what they are recording and why; how to validate information with the client or against other records to ensure that the correct data are recorded and how to correct errors. It is also important that staff understand what the records are used for and why accuracy is so important (Department of Health 2005).
The College of Occupational Therapists (2000) provides clear guidance for occupational therapists and occupational therapy services in relation to the content of care records. They state that all staff must:
(College of Occupational Therapists (2000) cited in the Professional Standards for Occupational Therapy Practice (2003: 35)).
The importance of accurate and full record keeping is further highlighted by the Health Professions Council Conduct and Competency Committee who regard record keeping as a competency and can take action ‘against practitioners where the care records demonstrate a lack of competence, either in the record keeping itself, or in their practice’. This includes an ‘unacceptable standard of record keeping, false or failed entries, or there being no evidence of activities such as assessment, treatment planning or the provision of information’ (College of Occupational Therapists 2006a: 4).
Legal and professional requirements
It is primarily the employer’s responsibility to ensure that care records created or used by their employees meet legal, national and local requirements, and that all staff have access to professional guidance and support appropriate to their roles, responsibilities and needs (College of Occupational Therapists 2006a).
The Health Professions Council Standards of Proficiency for Occupational Therapists (2003) states that registrant occupational therapists must be able to maintain records appropriately and:
It is important to remember that clinical notes have two purposes. Firstly to provide a clinical record of interventions with clients, and secondly (and only infrequently) they may be used as evidence in court proceedings. The College of Occupational Therapists (2003b) provides useful further guidance on the contents of good clinical notes from the perspective of their potential to be used as legal evidence.
In addition to guidelines from professional bodies, occupational therapists should follow local procedures and protocols when completing care records, meeting all the regulatory body requirements set for the workplace and for themselves as professionals (College of Occupational Therapists 2006a).
Signing and countersigning
It is a professional requirement for occupational therapists to ‘provide a clear signature, designation and date with all entries, additions or amendments’ (College of Occupational Therapists 2000cited in The College of Occupational Therapists 2003: 36). If using an electronic record-keeping system, it is important to ensure that electronic records clearly identify the member of staff making the record, in the absence of a signature to meet the same standards as written records.
Previously qualified staff were also required to countersign entries into records which were completed by students or support staff in order to ensure and demonstrate their accuracy (College of Occupational Therapists 2003). This however inferred that the practitioner had witnessed the treatment encounter and could ensure that the record accurately reflected the event that took place. By countersigning, this also identified the practitioner as the individual responsible for the events recorded. The College of Occupational Therapists recognised that it is not always possible to ensure that record entries are accurate, if the activities themselves have not been witnessed. It is therefore recommended that practitioners ‘meet local or regulatory body requirements for countersigning student or support staff entries in the records’ (Health Professions Council 2003b).
Use of acronyms and abbreviations
In their guidance on record keeping, the College of Occupational Therapists (2006a) highlight that abbreviations and acronyms are useful when trying to record in a concise way, especially if it can be assumed that the other members of the multi-disciplinary team will understand the terms used. However it should be remembered that a client has the right to access their records upon request and should be able to read and understand what is written in them. In addition, the use of certain terms and acronyms may change over time, and are likely to differ across different service providers. It is suggested that occupational therapy services should consider having an agreed number of acronyms or abbreviations in use and should ensure that these are defined fully within each set of care records (College of Occupational Therapists 2006a).
Timing and dating entries
It is necessary to record the date and time of the care provided to each client. This allows the therapist to document and demonstrate that the care was appropriate and proceeded as planned (or not). In addition, it allows the frequency of care to be monitored. It is important to remember that this may serve as a vital piece of evidence should care records be examined at a later date.
Timely record keeping
The longer the time lapse between an event occurring and it being recorded, the greater the chance of inaccuracies or omissions in the records. Records should be chronological and contemporaneous, made at the same time as the event being recorded, or immediately afterwards (College of Occupational Therapists 2003b).
Confidentiality and consent
In general client information must not be shared without consent from the individual themselves. However, there are exceptions to this rule. Disclosure is permitted if it is in the interest of the public to know the information and where a legal duty exists (College of Occupational Therapists 2006a). Practitioners should always manage client information in a way that respects their confidentiality, consent, right to access and best interests (College of Occupational Therapists 2006a). In 1997, a review of client-identifiable information within the National Health Service (NHS) in England, was chaired by Dame Fiona Caldicott. This review explored how patient information was being used and highlighted the potential of risk to confidentiality. A number of recommendations were made regarding information passing between organisations for reasons other than direct care, research or as a legal requirement. The aim was to ensure that client information is only ever shared for valid reasons and that the minimum necessary information was shared (Department of Health 2006). Following the review, the Caldicott committee developed six principles that should be followed when sharing client information.
Senior officers within health and social care services are now chosen to be Caldicott Guardians. They are responsible for ensuring that organisations achieve the highest standards possible for handling client-identifiable information (Department of Health 2006).
Documenting consent
Once consent, for assessment or intervention, is obtained from a client, it should be recorded and regularly confirmed. The nature of consent given (for example verbally, in writing, through a guardian or advocate, or by other means) should be recorded. All written consent forms should be kept in the client’s records. Consent should also be gained before a student observes or provides an intervention, and again the consent and nature of the consent should also be documented. A client’s refusal to consent to occupational therapy should also be documented, along with their reasons, if given (College of Occupational Therapists 2003). There are times when documenting consent may be difficult, for example when working with children or adults who may experience impaired capacity to make informed decisions. In such situations individuals should refer to national good practice guidelines or local standards.
Correcting errors
It is important that any errors noted are corrected immediately and initialled by the practitioner. Information should not be added or altered at a later date, and if any additions are essential, these should be noted as a separate or supplementary note or entry, dated and signed. Correction fluid should never be used to correct errors; instead they should be scored out with a single line so that the original text is still legible.
Format of care records
Care records may be kept in a variety of different ways, some of which are outlined below. Current developments in record keeping include the integration of care records across services, the move from paper-based records to electronic systems, and patient-held notes. Regardless of such innovations, the same standards of record keeping should be applied across all types of records.
One example of a specific record-keeping system used in some services is problem-orientated medical records. This system was first proposed in 1968 by Lawrence Weed in an attempt to improve the structure of the medical record by encouraging a more logical and clearer way of communicating information about an individual to another clinical professional (NHS Information Authority 1999). ‘SOAP’ notes, Subjective-Objective-Assessment-Plan, are the preferred format for note writing within this structure. This type of record keeping is frequently found in physical health settings, and is based upon a problem-solving approach which aims to gather information, appraise it, plan an action and evaluate an outcome. This system can be useful as it enables the reader to gain a quick understanding of a client’s functioning. However Blijlevens and Murphy (2003) critiqued SOAP notes and stated that they are too mechanistic and as they are based predominantly on a medical model do not necessarily fit with a holistic, client-centred philosophy of occupational therapy. In their review of the SOAP note-writing structure within their service, they found that the clients, ‘appeared to be regarded as made up of damaged body parts that needed to be restored to enable that person to perform fundamental activities in their home, and the notes did not reflect “who the client was in terms of their meaningful occupations and in what context these normally occurred”’ (Blijlevens and Murphy 2003: 4). As an alternative, they propose a structure based upon a more client-centred approach.
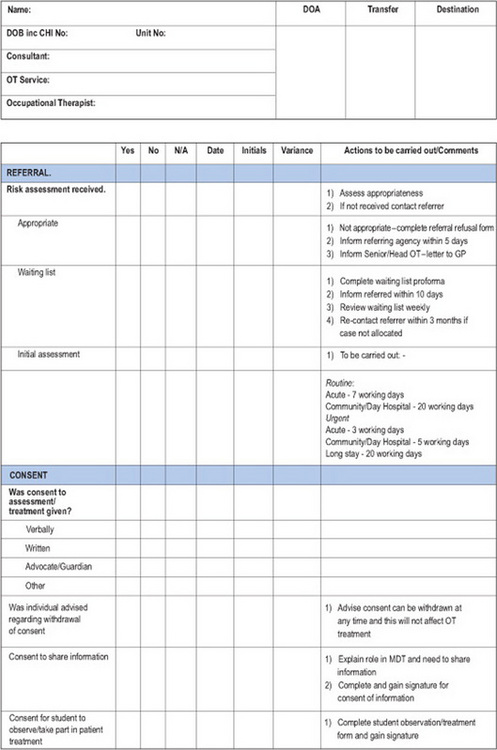
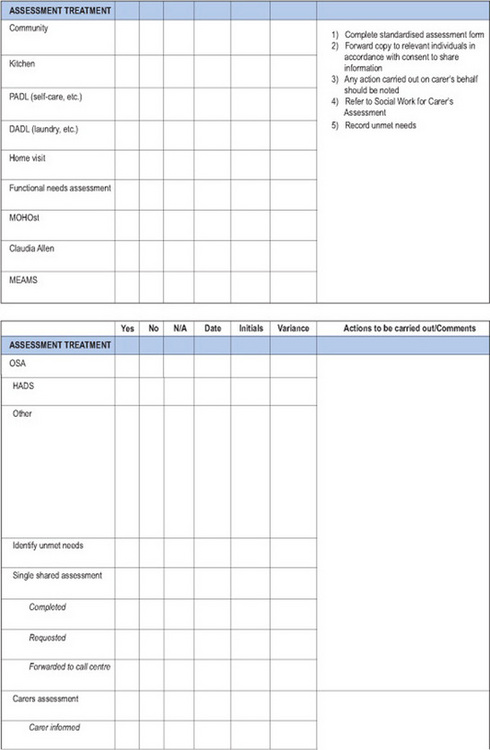
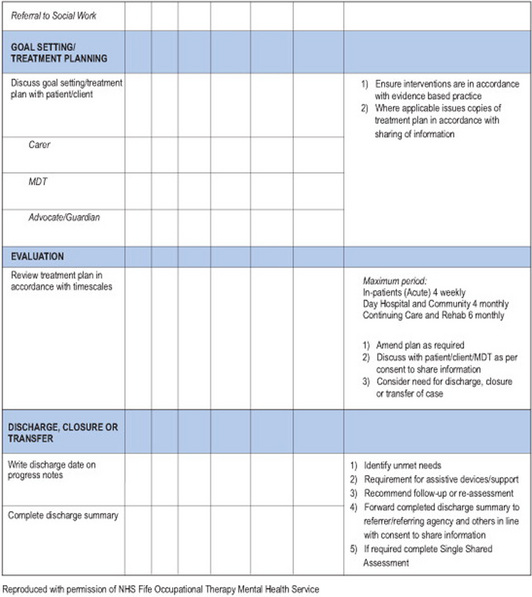
A large proportion of record-keeping systems are now multi-professional. There is now an increasing development of uni-professional and multi-professional integrated care pathways (ICPs) and the expansion of ICPs from health into social and community settings. ICPs are designed to provide an evidence-based plan of care for a client that incorporates appropriate national and local guidelines. They form a single, multi-professional record of care in an attempt to ensure best practice, co-ordination and consistency. They contribute to clinical governance procedures by providing an ‘expected pathway’ against which outcomes and interventions can be measured. This information and information on any variations from the expected pathway can provide opportunities to improve practice and improve the quality and outcomes of a client’s care (College of Occupational Therapists 2005). Duncan and Moody (2003) provide a useful overview of care pathways in general, and outline the development of an occupational therapy integrated care pathway in a mental health setting. An illustration of an occupational therapy integrated care pathway is given below (Figure 13.1).
Electronic care records
There is an international trend towards the introduction of electronic care records. Within the health service in the UK, development and use of electronic health records is a key part of the plan to develop an improved information system within the NHS. The proposed ‘NHS Care Records System’ will connect GPs with acute, community and mental health trusts in a single system, and will aim to replace existing paper-based systems by 2010. A national database will contain a summary of all records, making important service user information available at all times.
Garner and Rugg (2005) state that the use of electronic care records is likely to become ‘the major national programme strand to have an impact on occupational therapy’ in the near future, with an aim ‘to integrate records across multiple agencies including health and social care’ (p. 132).
In 1998, the College of Occupational Therapists and the Chartered Society of Physiotherapy commissioned ‘The Garner Project’ to explore the use of information and communication technologies within the allied health professions. The project specifically focused on the implementation of electronic care records within the two professions. The most recent phase of this ongoing project has assisted in identifying key themes for the occupational therapy profession to consider and respond to in light of the move towards electronic systems. These include organising client records, focusing on client’s views, involving staff, developing new ways of working, acknowledging problems of access and learning from others’ experience of using electronic records. Garner and Rugg (2005)suggest a number of actions that occupational therapy services can begin to take now, in order to prepare for the move towards electronic record-keeping systems in the future.
Patient-held records
In today’s health-care climate there is considerable emphasis upon providing cost-effective services. Patient-held records are thought to be a cost-efficient way of improving the care and outcome for those experiencing severe mental illness (Henderson and Laugharne 1999). Such records have become normal practice in some clinical settings, particularly obstetrics, paediatrics and chronic disease or disability management (Henderson and Laugharne 2005). Patient-held records may be particularly useful if an individual is receiving care from a variety of professionals. In addition, it is thought that they may allow the individual to be a more active participant in their care; for example being able to have the information that shows what has worked or been unhelpful in the past. This information may be useful in mental health settings when discussing issues such as relapse. It has been suggested that patient-held records also reduce any possible ‘coercive’ elements of treatment (Henderson and Laugharne 2005). However, possible difficulties exist. These include confidentiality issues, reliability of the client to carry the information and keep records safe and duplication of the information (Warner et al 2000). Practitioners are advised to follow local policy regarding whether or not duplicate records should be retained by the professional. If policies restrict the keeping of such records, it is the responsibility of that organisation or authority to accept any possible consequences (College of Occupational Therapists 2006a). According to Warner et al (2000), patient-held shared care records had no significant effect upon mental state or satisfaction of mental health service users. The uptake of the scheme was low by both staff and clients and it appeared that those experiencing a psychotic illness were less likely to use the records. In relation to the use of patient-held records in palliative care, a study by Cornbleet et al (2002) also found no significant evidence to support the introduction of such a scheme. There appeared to be no improvement in information giving or sharing, or to the degree to which the family were involved in decision making. However, most individuals who had a record found it to be of some benefit. Clearly this is an area that requires further investigation.
Recording and reporting the occupational therapy process
Referral
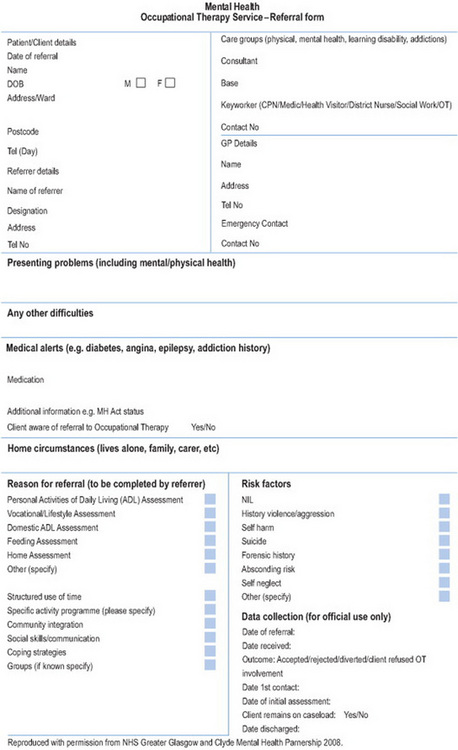
It is the practitioner’s responsibility to record or retain the referral details in the appropriate occupational therapy records (College of Occupational Therapists 2003). This should include the source and date of referral. There is also a requirement to inform the referring agency should the referral be declined. Justification should be provided. A documented system for prioritising referrals should be evident. At the same time, optimum use of resources should be sought. If the referral is considered inappropriate, it may be recommended that the client’s details are passed on to an alternative service. Should this occur, informed consent must be documented (College of Occupational Therapists 2003). Figure 13.2 illustrates an example of an occupational therapy referral form.
Assessment
All assessments including both standardised and non-standardised interview and observational assessments should be recorded. A description of the client factors, circumstantial aspects and features of the activity that allow or impinge upon performance should be acknowledged. The therapist’s confidence in the assessment results should also be included (American Occupational Therapy Association 2003). Should variables exist that would affect the results (for example a client’s tiredness), such factors should also be documented.
Within practice, many different types of assessments are used (see Chapter 6). If a standardised assessment is used the aims and procedures must be clearly stated. Any variation during the assessment that would affect the standardised process, must be recorded. The type of assessment used will depend upon the clinical area and needs of the client. Examples may include, but are not limited to, a comprehensive initial assessment, home visit assessments, workplace/vocational assessments, dressing assessments and kitchen assessments.
Stancliff (1998) suggests that private (or insurance-based) services provide further issues for consideration; demonstrating the value and effectiveness of an intervention through accurate documentation is particularly important for clients, services and contractors. McGuire (1997) proposes that occupational therapy reports must firstly focus upon function and highlight clearly the occupational performance area being addressed. Furthermore, practitioners should precisely record the relationship between any medical diagnosis/problem and function. However, it may be that a diagnosis is not always known. And by viewing the individual in a medical and compartmentalised way, practitioners may depersonalise the individual and exclude their knowledge, meanings and experiences (Blijlevens and Murphy 2003).
Recording progress
McGuire (1997) states that reports should clearly indicate progress made. Documentation should focus upon function. When using narratives in progress notes, practitioners should emphasise the functional focus by organising the content in relation to the overall performance area being addressed within the treatment plan (McGuire 1997). The practitioner should then clearly document the relationship between medical problem and occupational functioning. Progress in performance components (cognitive, sensorimotor, psychological) must be related directly to the client’s functional goals established within the performance areas (ADL, work/productivity, leisure) (McGuire 1997). As safety issues are particularly important these issues should be clearly documented (McGuire 1997). Furthermore, therapeutic expectations regarding improvement in the client’s safety or functional ability should also be documented. Reasons for slow or lack of progress must also be included. Finally, the skilled component of occupational therapy must be recorded, showing the clinical reasoning, and therapeutic strategies or principles used (McGuire 1997). Whilst these issues are important in all record keeping, they are particularly relevant when practitioners are concerned with demonstrating effectiveness to third-party payers.
Documenting clinical reasoning
Practitioners should document the clinical reasoning behind their care planning and service provision (College of Occupational Therapists 2006a); a task, it has been argued, that they are not always good at (Stancliff 1998).
Neidstadt (1996) suggests that mostly pragmatic and procedural reasoning styles are used within medical, physical health-orientated environments. However, narrative reasoning engages the individual in a life history story-telling process that ultimately places the practitioner in a better position to understand their client’s subjective experiences, values and goals for the future. By gathering and reporting this information, practitioners ultimately build a picture of the person through what they do. As a result, meaningful client-centred goals can be established (Neidstadt 1996).
Reflecting theory within documentation is a powerful method of communicating professional reasoning and rationale. Not only does it allow us to communicate to other professionals, or significant others, the aims, interventions and outcomes of therapy it also allows us to enhance professionalism and credibility amongst colleagues (Forsyth and Kielhofner 2002). However, it can be difficult to effectively communicate profession-specific models and perspectives within client reports. Forsyth and Kielhofner (2002) acknowledges that a disadvantage of professional terminology is that the language is not common to all professionals, clients or families/carers. However, they also suggest that practitioners do not use terminology due to lack of confidence rather than any contention from colleagues.
By documenting a clear relationship between the assessment outcomes, goals and proposed treatment plan, practitioners educate others regarding the varied scope of occupational therapy intervention (Kyle and Wright 1996). Efficient reporting should be organised and comprehensible. It should provide descriptive characteristics of the client and the context in which the assessment or intervention occurred. Documentation is particularly useful for sharing small, gradual and hard-to-detect changes. Evidence should be recorded either quantitatively or qualitatively (Tickle-Degnen 2000).
All assessment results should be recorded and comprise all decisions made including not to continue intervention either by the client or relevant other. It is important to remember that assessment results are shared jointly with the client and practitioner and that, within the bounds of legality, it is the client’s choice to share the information with relevant others or to withhold consent (Creek 2003).
Goal setting and treatment plans
Following an initial screening and subsequent assessment, collaborative goals are established (see Chapter 8 for further information) and should be recorded. Any needs or aims that cannot be addressed must also be recorded and reasons for this given (Creek 2003).
Despite this, a study carried out by Anderson et al (1991), expressed concern at the noticeable lack of goals within occupational therapy documentation. Without clear, measurable goals it is not possible to evaluate their achievement. Perhaps more worryingly, it is also suggested that there was little evidence to suggest that clients were involved in the treatment planning process (Anderson et al 1991); hopefully this situation has improved significantly in the intervening years. Occupational therapists are required to record each client’s assessed needs and subsequent goals and intervention plan (College of Occupational Therapists 2003). It is possible that existing resources may impact upon a practitioner’s ability to carry out the ideal, fully comprehensive treatment plan. In such cases, the practitioner should identify and record the objectives that must be achieved in order to provide a service that is considered to offer a minimum level of satisfaction and safety to clients and significant others (Creek 2003).
It is not only crucial that goals be clearly documented and client-centred but also measurable and, therefore, provide a means for evaluating therapy. Forsyth and Kielhofner (2002) state that measurable goals must contain the action to be carried out to demonstrate achievement of the goal. They should also specify the environment in which the goal relates to. Furthermore, the level of independence/degree of support needed should be recorded, and a clear timeframe should be specified.
Reassessment/alteration to treatment plans
In addition to documenting a clear treatment plan, all subsequent occupational therapy interventions and contacts must be documented. As assessment and evaluation of interventions are an ongoing process any changes to them should also be recorded.
Discharge planning
Clearly, discharging an individual from therapy will depend upon the clinical area and timescale. Creek (2003) states that practitioners usually write a short informative report when an individual is discharged. More detailed reports are produced when required. However, the depth of these reports will vary from location to location.
Any plans for a client’s discharge, case closure or transfer of care should be recorded within their treatment plans (College of Occupational Therapists 2003).
When considering discharge or transfer from the service, the practitioner should assess progress made towards agreed goals, and record the level of support or assistance needed in any areas of functioning. They should also make recommendations for future support or interventions if appropriate and propose any follow up or further assessment needed (College of Occupational Therapists 2003).
Ensuring standards of record keeping
Ensuring good standards of record keeping is an important aspect of service quality. Audits enable organisations to evaluate and monitor the services they provide, and allows the identification of potential areas of risk, inefficiency or ineffectiveness providing opportunities to take any necessary action to improve the quality of services provided The involvement of clients in the audit process is now actively encouraged, in order to gain their views as recipients of care. The College of Occupational Therapists (2004) has published a useful briefing paper to assist services in involving clients in such activities.
Gibson et al (2004) developed a retrospective audit tool of 61 standards from the College of Occupational Therapists core standard on record keeping. They used this tool to conduct an audit of 320 client records across many clinical specialisms within a service. The audit identified many areas of good practice, and areas which did not meet the standards were used to form the basis of a number of service action plans, highlighting how the audit process should be used as a learning opportunity. Participation in audit is now a clinical governance requirement, and many audit tools are now available to assist services in this process (College of Occupational Therapists, 2005b).
Legal issues in documenting and report writing
Practitioners should also consider their involvement in documentation that is not occupational therapy specific. These may include involvement in risk assessment and risk management, child protection reporting, and legal reports for court.
Risk assessment
In mental health settings, changes within legislation and highly publicised tragedies have led to increasing emphasis on accurate risk assessment and risk management (Newell 2001). Several clinical risk assessment tools have been developed and practitioners should select the most suitable tool for their clinical area and working environment, and for which they have received appropriate training.
Practitioners must assess the possibility of any health and safety risks and clearly document the outcomes of any risk assessment carried out. Contingency plans should be developed for risks that cannot be eradicated and any decisions made by the practitioner based upon their assessment should be documented (College of Occupational Therapists 2003). For example, practitioners should ensure that appropriate risk management policies and incident reporting procedures have been developed. However, Mandelstam (2005) describes a reduction of practitioner confidence in such decision making due to worries of legal action. This can lead to inaccurate perceptions of risk and overly defensive practices.
Child protection
Practitioners may have to be aware of possible involvement in scenarios whereby child protection issues are raised. The ‘Hidden Harm’ agenda (Scottish Executive 2006) reinforces the importance of effective communication and information sharing between agencies when working with individuals who may misuse drugs or alcohol. Confidentiality policies can present barriers to sharing relevant information. However, identifying a situation where a child may be at risk overrules any agency rules or obligations. All agencies should have clearly documented child protection procedures.
Court reports
Increasingly, practitioners are involved in claims and legal issues. In relation to clinical work, practitioners may become involved in court cases in the following ways:
As a witness of fact therapists may be asked to produce a statement or a report. Statements include personal details and professional background. It should also provide a coherent, chronological record of events. Technical jargon should be fully explained.
Records and notes may be required. The content of the report will differ depending upon the specific case. The referenced guidelines produced by the College of Occupational Therapists (2003) provide a useful example of how to structure a court report. According to Mandelstam (2005: 47), ‘the law aside, good professional practice anyway demands a reasonable standard of evidence, reasoning and documentation; if professionals record their decision making it is likely to be of a higher quality’.
Investigations carried out by the Health Professions Council into professional competence frequently centre around the inadequacy of record keeping. The importance of documenting the thoughts and evidence that have led a practitioner to make the decision cannot therefore be overemphasised. In general, the legal system is likely to focus more upon the decision-making process rather than the actual outcome or merits of decisions (Mandelstam 2005). It is of crucial importance that occupational therapists demonstrate their clinical reasoning process and document clearly, how the decision was reached.
Summary
This chapter has provided an overview of the key aspects of recording and report writing. Emerging issues (such as electronic records) have also been acknowledged. Although guidelines produced by professional bodies are available, variations in national and local procedures exist and should be referred to. This chapter provides essential information and guidance to effectively and accurately record clinical information and create reports. It should be treated as an initial introduction to the topic, equipping the reader to develop further skills and continue their reading, reflection and action regarding recording and report writing.
American Association of Occupational Therapy Association. Guidelines for documentation of occupational therapy. Cited. Sames KM, editor. 2005 Documenting occupational therapy practice. Prentice Hall: Pearson, 2003.
Anderson B, Llewellyn G, Bell J. Records: one measure of occupational therapy practice in the field of developmental disabilities. The Australian Journal of Occupational Therapy. 1991;38(2):77-81.
Blijlevens H, Murphy J. Washing away SOAP notes: refreshing clinical documentation. New Zealand Journal of Occupational Therapy. 2003;50(2):3-8.
College of Occupational Therapists. Occupational therapy record keeping (standards for practice). London: College of Occupational Therapists, 2000.
College of Occupational Therapists. Professional Standards for occupational therapy practice. London: College of Occupational Therapists, 2003.
College of Occupational Therapists. The occupational therapist and the court. In A step by step guide for occupational therapists and their staff. London: College of Occupational Therapists; 2003.
College of Occupational Therapists. COT/BAOT Briefing: 28 service user involvement. London: College of Occupational Therapists, 2004.
College of Occupational Therapists. COT/BAOT Briefing: 1 Integrated Care Pathways. London: College of Occupational Therapists, 2005.
College of Occupational Therapists. COT/BAOT Briefing: 40 Quality Briefing: Audit. London: College of Occupational Therapists, 2005.
College of Occupational Therapists. Record Keeping. In College of Occupational Therapists guidance 2. London: College of Occupational Therapists; 2006.
College of Occupational Therapists. Record keeping – issues of responsibility COT/BAOT briefing 43. London: College of Occupational Therapists, 2006.
Cornbleet MA, Campbell P, Murray S, et al. Patient-held records in cancer and palliative care: a randomized, prospective trial Palliative Medicine. 2002;16(3):205-212.
Creek J. Occupational therapy defined as a complex intervention. London: College of Occupational Therapists, 2003.
Department of Health. The Caldicott Guardian Manual. London: Department of Health, UK Council of Caldicott Guardians, 2006.
Department of Health. The Records Management: NHS Code of Practice. 2006. www.dh.gov.uk/en/Managingyourorganisation/Informationpolicy/Recordsmanagement/index.htm. Accessed on 07/04/2008
Duncan EAS, Moody KJ. Integrated care pathways in mental health settings: An occupational therapy perspective. British Journal of Occupational Therapy. 2003;66(10):473-478.
Forsyth K, Kielhofner G. Putting theory into practice. In Kielhofner G, editor: 2002 Model of Human Occupation Theory and Application, 3rd edn., Baltimore: Lippincott, Williams and Wilkins, 2002.
Garner R, Rugg S. Electronic care records: an update on the Garner project. The British Journal of Occupational Therapy. 2005;68(3):131-134.
Gibson F, Sykes M, Young S. Record keeping in occupational therapy: Are we meeting the standards set by the College of Occupational Therapists? The British Journal of Occupational Therapy. 2004;67(12):547-550.
Health Professions Council. Standards of Proficiency. London: Occupational Therapists Health Professions Council, 2003.
Health Professions Council. Standards of conduct, performance and ethics. In Your duties as a registrant. London: Health Professions Council; 2003.
Henderson C, Laugharne R. Patient held clinical information for people with psychotic illnesses. The Cochrane Database of Systematic Reviews. 1999;4:1-20.
Kyle T, Wright S. Reflecting the Model of Human Occupation in occupational therapy documentation. The Canadian Journal of Occupational Therapy. 1996;63(3):192-196.
Mandelstam M. Occupational therapy: law and good practice. London: College of Occupational Therapists, 2005.
McGuire MJ. Excellence and efficiency in documentation. Targeting your audience bridges the gap between services delivered and provider reimbursement. OT Practice. 1997:36-41.
Neidstadt M. Teaching strategies for the development of clinical reasoning American Journal of Occupational Therapy. 1996;50(8):676-684.
Newell S. Clinical risk assessment for an occupational therapy inpatient group programme. The British Journal of Occupational Therapy. 2001;64(4):200-202.
NHS Fife. Mental Health Occupational Therapy Service Integrated Care Pathway. NHS Fife. 2008.
NHS Greater Glasgow and Clyde Mental Health Partnership. Mental Health Occupational Therapy Referral Form. NHS Greater Glasgow and Clyde. 2008.
NHS Information Authority. Briefing Paper: Problem Orientated Medical Record (POMR) and SOAP. 1999.
Scottish Executive. Hidden harm. Next steps. Supporting children – working with parents. Edinburgh, UK: Scottish Executive, 2006.
Stancliff BL. Documentation insurance companies understand. OT Practice. 1998:55-56. July/August
Tickle-Degnen L. Monitoring and documenting evidence during assessment and intervention. The American Journal of Occupational Therapy. 2000;54(4):434-436.
Warner JP, King M, Blizard R, et al. Patient-held shared care records for individuals with mental illness: randomized controlled evaluation. The British Journal of Psychiatry. 2000;177:319-324.