Charting the menstrual cycle
Introduction
For most women, there are only about 30 days in a year when there is a reasonable chance of conceiving. For a successful pregnancy to eventuate, a whole chain of events need to come together precisely in the woman’s body, in her partner’s body and in their relationship on one of those days. Being able to accurately identify these relatively rare opportunities raises the odds of success considerably. Watching external clues of the body provides us with a method to do exactly that.
The BBT Chart
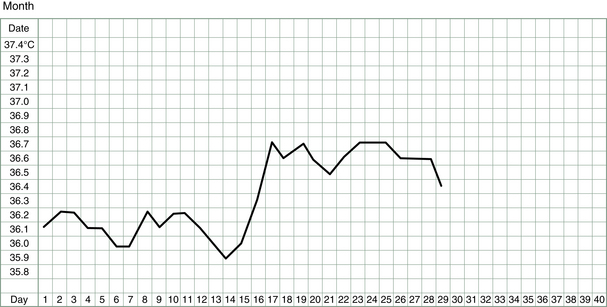
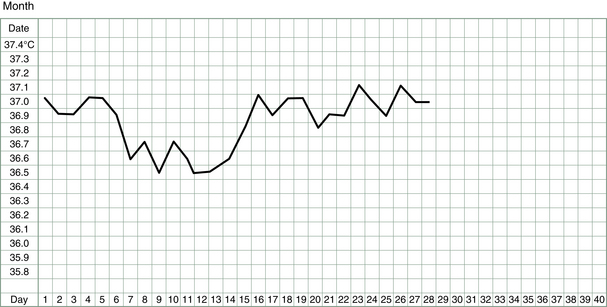
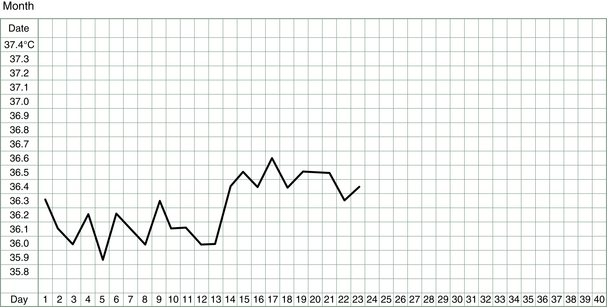
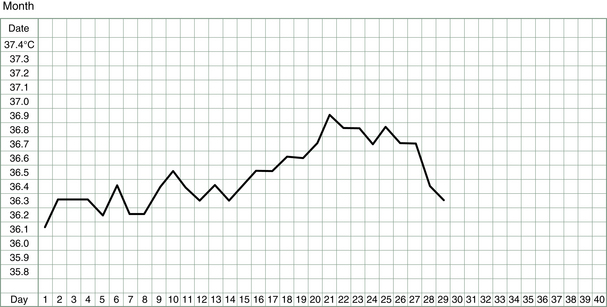
The basal body temperature (BBT) chart records the temperature of the body on waking. It is called basal because it is measured at a time when the body is deeply rested and the body’s metabolism and temperature is at its baseline. A woman’s basal body temperature rises after she has ovulated and begins to produce progesterone. In a typical menstrual cycle, a BBT chart looks something like that shown in Figure 3.1.
One of the very great strengths of Chinese medicine is discerning what is going on inside the body from watching or feeling what is going on on the outside of the body. Thus, the color and nature of the complexion tells us things about the functioning of the internal organs, as does the glint or lack thereof in the eyes, or the color and nature of the urine or the stools or the menstrual flow, or the strength of the artery at the wrist and inside the ankle, or the look of the tongue, and so on. The Chinese have observed so many minute details and over thousands of years correlated them with disease patterns or tendencies to manifest particular disease patterns but it was only in recent years that doctors in China incorporated into their battery of diagnostic skills two more external signs – namely, the change of basal body temperature observed during the menstrual cycle and the production of mucus by the cervix just before ovulation.
TCM gynecologists in China, having to rely on external observations more than pathology tests and investigative surgery, observed BBT patterns with a zeal and focus of attention that would not occur to a Western-trained gynecologist. Thus, the BBT chart has become a tool that reveals to TCM specialists so much more information than it does to a Western specialist. For most specialists in the West, reliance on laboratory results far supersedes reliance on information gathered by the patient and the doctor purely by careful observation. Thus, the BBT chart as a useful diagnostic tool is given little heed by most specialists in the West past indicating an ovulation or not.
Family planning and natural birth control advocates pay the BBT chart greater attention than do gynecologists but their aim is only to discover if, and more particularly when, an ovulation has occurred. The TCM specialist, as we shall discover, uses the BBT chart to discover much more than this.
Basal body temperature charts require no sophisticated equipment and are surprisingly sensitive to many factors related not only to the menstrual cycle but also to lifestyle and events.
Hot on the heels of the discovery of the changes of resting temperature during the menstrual cycle was the ‘discovery’ of the changes in vaginal secretions according to menstrual phase. Maybe this is one rare instance where Western physicians have noted and used for medical analysis a common external sign before doctors in China have. To be sure the Chinese have observed and said plenty over the last 2000 years about different sorts of vaginal discharges but to my knowledge they did not correlate changes in discharge with the menstrual cycle.
No matter who described the phenomenon first, TCM doctors have wasted little time in incorporating such useful observations into their diagnostic repertoire and have related quantity and quality of fertile mucus secretions to standard TCM diagnostic patterns.1
The How’s and Why’s of BBT Measurements and Other Observations
Recording the lowest body temperature each morning, and watching the secretions of the cervix and noting the changes in position in the cervix and then charting these observations will, over time, build an individual profile which is as informative as it is interesting. In addition, changes in breast symptoms, abdomen symptoms, bleeding patterns and general symptoms paint a picture that provides an accurate insight into the inner workings of those hormonal tides which ebb and flow each month.
History of the BBT Chart
The first people who started to examine menstrual charting were interested in improving the effectiveness of the rhythm method of contraception recommended by the Catholic religion. The rhythm method assumed that women ovulate on Day 14, or at least some time round the middle of the cycle. It had a woefully low success rate, simply because all women have different rhythms and any individual woman’s rhythms can change from one cycle to the next, depending on what is happening in her life. Similarly, couples trying to fall pregnant who believed that intercourse had to occur on Day 14 sometimes had a long wait, especially if the woman had a long cycle and ovulated, say, on Day 18 each month.
Researchers in this field then made the serendipitous discovery that the basal body temperature rose after ovulation, which added a welcome objective verification of ovulation. A method called natural family planning was developed based on this knowledge and women who measured their basal temperature were assured that they could feel quite confident that they were infertile after the basal temperature had risen. The rise in temperature reflects the action on the temperature-regulating centers of the brain by progesterone, a hormone which is produced after ovulation. The action of progesterone in lifting basal body temperature is clearly important enough to be conserved through many thousands of years of natural selection, since this hormone and its thermal activity appears in all our mammalian predecessors.
More advances came when researchers in Australia, the two Dr Billings, examined the relationship of hormonal production, cervical secretions and ovulation.2 They were able to establish that there was a reliably reproducible cyclic pattern in the cervical discharges (in response to estrogen and progesterone production) and that the most dramatic and easily observed changes occurred before and after ovulation. The work of two professors working at Melbourne and Monash Universities also confirmed that women’s own awareness of their cervical mucus could indicate ovulation more accurately than measurements of hormones by blood tests.3
Now the contraceptive method, approved by the Catholic Church, could be developed to a sophisticated enough degree that it actually worked. In fact the sympto-thermal method, as it rather clumsily came to be called, boasts a success rate as a contraceptive method of 98%. This compares very favorably with the rate for the condom of 97% and the oral contraceptive pill of 99.5%.4 Teaching programs sprung up all over the Western world and the method is variously called FAM (fertility awareness method), NFP (natural family planning) or the Billings method. The method not only gave women a wonderful insight into the workings of their own bodies but also liberated them from the need to use chemicals and devices if they did not want to fall pregnant.
Of course the very useful corollary of this method which was developed as a contraceptive aid was that it also could work the other way – it could help women conceive. Knowing when you’re fertile and need to avoid intercourse became knowing when you’re fertile and need to have intercourse. Not only do the chances of falling pregnant rise dramatically when intercourse is timed appropriately but the pregnancies which result from the precise timing of conception are generally more secure and the incidence of miscarriage is lower.5
The more that was learned about the qualities of the fertile mucus, the more was learned about how some aspects of fertility can be enhanced or hindered. For example, observation of the behavior of sperm in the fertile mucus can uncover some impediments to conception. Sometimes the mucus is too acid, or too alkaline, or may contain antibodies. There are various ways these can be overcome. It may be as simple as douching with dilute vinegar, for an alkaline vagina, or sodium bicarbonate for a too acid one. Antibodies in the fertile mucus is a little more difficult to treat and is discussed later.
Charting the Cycle from Day 1
Let us now revisit the cyclical changes of the cervix, ovaries and uterus. In this section, we wish to focus on the external cues produced by internal physiologic changes and what they tell us about fertility. These close observations are very useful in pinpointing subtle nuances which the TCM practitioner (or other infertility specialist) will use in their diagnosis.
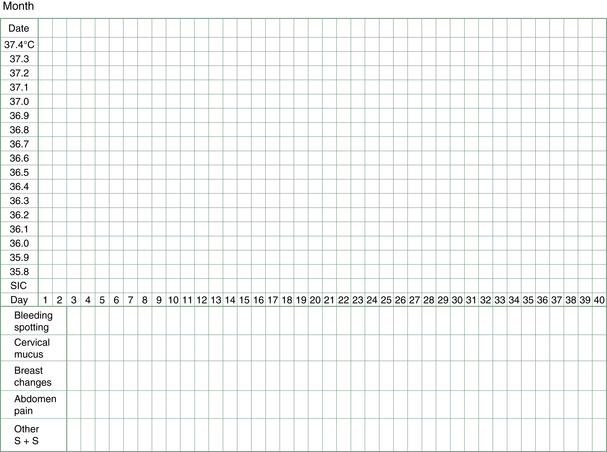
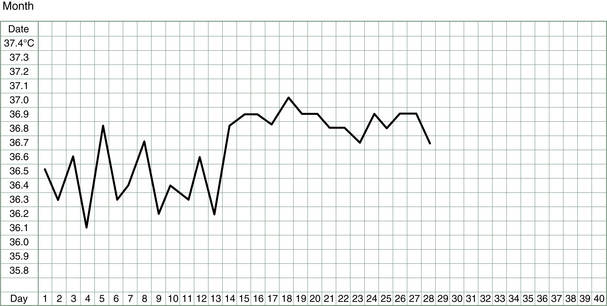
To start, all that is needed is a thermometer, a chart (see, e.g., Fig. 3.2) and a good night’s sleep (or at least 3–4 unbroken hours). For those women having regular menstrual cycles, charting starts at the beginning of a cycle, i.e., the first day of bleeding. For women not having periods or having them very sporadically, charting can start immediately but may be followed by a lengthy wait for a pattern to emerge.
Some women find charting their temperature makes them feel too obsessed by and focused on the whole business of getting pregnant; or, on the other hand, if they are not ovulating, too demoralized. To the former, it may be good advice to try charting for just three cycles so a pattern can be established. That pattern may be helpful in pinpointing a reason for a delay in falling pregnant, as we shall see below. Then taking the BBT each day can be dropped if it is truly causing distress. However, in most cases, I find that the woman becomes as curious as I am about her chart and starts to see it as a friendly tool rather than something reminding her of infertility. The journey together becomes an exciting one, as we start to see the effects of treatment on the shape of the chart and on her symptoms and signs.
For those women feeling demoralized by a chart showing no temperature changes, i.e., no ovulation, we will usually drop that method for a few months and concentrate on observing changes in fertile mucus secretions from the cervix. Hopefully, these will happen in response to treatment. As soon as an increase in discharge is noticed, then recording the basal temperature is again encouraged, so that the putative ovulation can be registered by a rise in basal body temperature.
Let us now go through the technique step by step.
The thermometer
In the case of recording and comparing changes in the resting or basal temperature of the body a reliable thermometer is needed – the change is a subtle fluctuation and not one which can be discerned subjectively, as can fever. A mercury or digital thermometer can be used. Digital thermometers are a little easier to read, especially in those groggy first few minutes of the day just after waking, but they are more expensive than the mercury type, and they can be slightly less accurate (although this is not usually a problem for our purposes). It is possible to buy a mercury thermometer designed to measure only the basal body temperature (called a basal body temperature thermometer). In this case the scale covers a narrower range than usual and the gradations are more spread out and easier to read than on a regular thermometer. However, most women use the regular thermometer normally kept in the bathroom cupboard for measuring fevers. Now, however, the thermometer will be kept on the bedside table.
On waking in the morning, after at the very least 3 h uninterrupted sleep, the thermometer is placed in the mouth and left for 3–5 min. BBT can also be measured by placing the thermometer in the vagina or rectum. Because these routes are slightly less convenient, they are less often used. However, if we are finding that the temperature readings are very erratic and it is hard to determine a pattern, then I sometimes recommend the vaginal route, which can give a more stable pattern.
The thermometer is removed, the temperature reading taken and its value noted on the chart under the correct day and date. For a mercury thermometer, it can be placed carefully on the bedside table and the reading taken some time later in the morning or even when going to bed the next evening. This is because most mercury thermometers will remain stable at the temperature they have reached until the mercury is given a firm shake down with a sharp flick of the wrist. After reading and recording the temperature, the mercury in the thermometer should be returned to its base level and the thermometer wiped clean ready for the next morning’s use.
It is important that the temperature is read at roughly the same time each morning, because later waking raises the basal body temperature. Thus, a very erratic-looking chart may reflect nothing more than a rather erratic sleep and waking pattern. Some studies have shown that the basal temperature rises 0.09°C for each hour of delayed rising in the morning.6 Thus, BBT charts can be adjusted for different waking times by moving the recorded temperature one square up or down for each hour of waking earlier or later than usual.
The urinary ovulation predictor kit
These kits can be used to test for the rise in luteinizing hormone (LH) prior to ovulation, i.e., at the later stages of the follicular phase. LH produced by the pituitary as the dominant follicle ripens usually does not last very long in circulation and so these kits test for a form of LH that has an extended life span due to transformation in the urine. It is recommended that the urine is tested during the day (not first thing in the morning) after avoiding liquids for about 2 h (so that the urine is not too dilute). A positive reading will show two colored lines with the test line being equal to or darker than the control line. This indicates the LH levels have risen and that an egg will probably be released within 12–48 h. Using the predictor kit in conjunction with the BBT is a useful strategy, especially if the fertile mucus signs are not pronounced. It gives a reliable guide to the most fertile days of the cycle and the best days to be having sex.
The chart
Many different variations of the BBT chart have been developed over the years, initially by those using BBT as a contraceptive tool. Basically, all charts record the basal body temperature and compare the values over the entire menstrual cycle. As other kinds of fertility signals were described (e.g., cervical fluid and position) by the Billings’, then provision was made for these to be recorded alongside the temperature readings. Room for other items of personal interest, such as dates of sexual intercourse, or late nights or the occurrence of relevant symptoms has also been added.
Each day the temperature is recorded on the chart, along with other observations related to fluctuations in the hormones (Fig. 3.2), e.g., changes in breast and nipple tenderness or swelling may be noticed or changes in abdomen bloating or discomfort, in sleep patterns, in moods, in food cravings and, most importantly, changes in vaginal lubrication and discharge (this latter can also include spotting of blood).
Fertile mucus
The changes in vaginal discharge which flag changes in fertility are determined both by subjective feelings of moisture at the vulva and by more objective observation of the discharge collected on underclothes, toilet tissue or fingers.
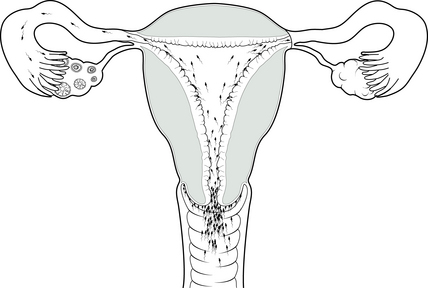
The estrogen peak, which stimulates the production of fertile mucus, usually starts on average 6 days before ovulation. Four different types of mucus are produced by specialized glands in the cervix in response to this estrogen (Fig. 3.3).7 The cervical discharge produced at infertile times (i.e., at all times except ovulation) is associated with a dry feeling at the vulva. It is called G-type mucus and is thick, pasty and impenetrable. It is produced in crypts of the cervix at the end of the cervical os nearest the vagina (Fig. 3.4). As estrogen levels begin to rise, the cervix produces, from crypts a little higher in the cervix, the more liquid L-type of mucus. This causes the vaginal sensation to be more sticky or wet. As ovulation approaches, crypts still higher in the cervical os produce mucus which is more stretchy and slippery. It is this S-type mucus that is sometimes referred to as the egg-white-like mucus. The sensation at the vulva now is distinctly wet and strings of S mucus, sometimes mixed with clumps of L mucus, may be noticed. The phenomenon which gives this mucus its elasticity is called spinnbarkeit, or ‘spinn’ for short.
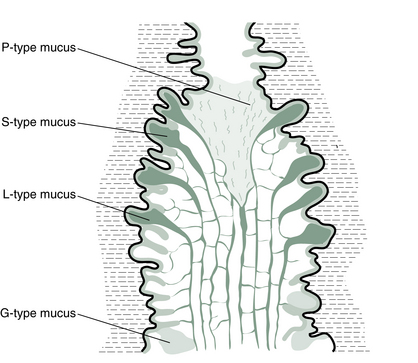
Finally, as ovulation is imminent, the mucus loses its stretch as the cervix produces its P mucus from the very top of the cervical canal. P mucus is so named for its rich potassium content. While this final secretion is less thick and stretchy, it is extremely lubricative and produces a slippery sensation in the vulva. The last day that P mucus is produced is the most fertile day of the whole cycle, i.e., the day before the egg is released or the day it is released.
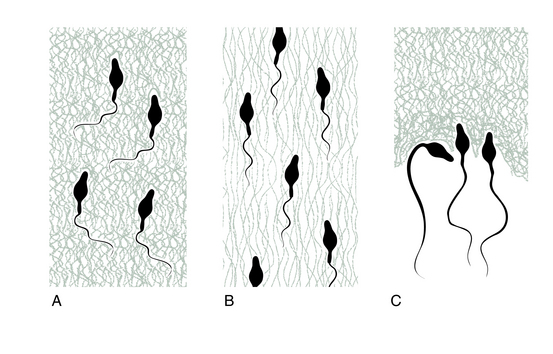
Fertile mucus forms graphic ferning patterns when it is dried on a smooth surface such as a glass microscope slide. The three different types of fertile mucus crystallize in three distinct patterns: the L mucus makes intricate and many branched ferns; the S mucus makes delicate pine needles lined up close and parallel; and the P mucus makes hexagons (Fig. 3.5).

The function of the branched L mucus is to catch and filter out some of the abnormal or poor-quality sperm before they reach even the uterus. The S mucus, on the other hand, provides a rapid sperm transit system, as it creates clear pathways for them to swim upwards to the uterus. Because it is composed of mucin strands lined up longitudinally it has the unusual quality of being particularly stretchy and adhesive to itself. For example if you tried to pour fertile mucus from one cup to another you would have to cut the flow with scissors if you wanted to stop it halfway.
The P mucus appears to have some quality which gives sperms a final boost or activation as they climb through the cervix to the uterus.
A summary of fertile mucus characteristics is given in Table 3.1.
Table 3.1
Summary of fertile mucus characteristics
| Characteristics | Function | |
| G type | Thick, pasty and impenetrable | Blocks entrance to uterus |
| L type | Sticky or wet. When dried, makes intricate branched ferns | Catches and filters out some of the abnormal or poor-quality sperm before they reach the uterus |
| S type | Stretchy and slippery like egg white. When dried, makes delicate pine needle shapes | Creates or facilitates pathways for sperm entry to the uterus |
| P type | Lubricating. When dried, makes hexagons | Activates sperm as they pass through the cervix to the uterus |
One easy way to evaluate quality and quantity of cervical secretions is to collect a little from the vaginal entrance (if it is plentiful enough) or gently from the cervical surface itself (if it is less plentiful) with clean fingers and see how much elasticity there is as the fingers are drawn apart (Fig. 3.6). Some women prefer to use toilet tissue to collect the fluid or rely on sensations of moisture alone. Some teachers of the Billings’ method stress learning to interpret the subjective sensations of dryness or lubrication at the vulva without further investigations using the fingers (presumably to avoid introducing infection to the vagina or for cultural reasons when this method is taught in developing countries).
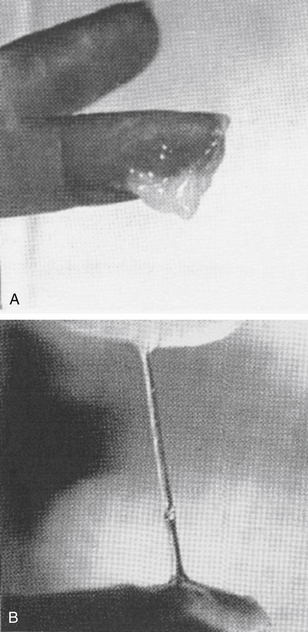
Figure 3.6 Examination of stretchy fertile mucus. (A) G-type mucus – no spinn. (B) S-type mucus – spinn.
The importance of recognizing the changes in the fertile mucus lies in the fact that it precedes ovulation and therefore alerts a woman to her most fertile days. The last day of any fertile mucus, whether seen as a secretion from the vagina or felt as a moist sensation, is often referred to as the ‘peak day’. This refers to the day of peak fertility, the day before or the day the egg is released. Nature’s design for conception is not random at all but has designed very exact timing. Producing the fertile mucus to facilitate the sperm’s journey up the cervix in the days before ovulation is aimed at getting these sperm inside the female reproductive tract well before the egg is released (Fig. 3.7). This is because this largest single cell in the body is one of the shortest lived, being fertilizable for only 6–12 h. Some of the millions of lively little sperm cells, on the other hand, have been known to survive for 5 days in the female reproductive tract, although they are most able to fertilize the egg in the first 48 h after delivery to the vagina. So, ideally, there will be a bunch of some hundreds of eager sperm that have survived the hazardous journey as far as the fallopian tubes, lying in wait for the egg as she is launched. Some studies have indicated that the day for sexual intercourse which then leads to the highest conception rate is, in fact, 2 days before ovulation.
The post-coital test
The post-coital test or PCT (also known as Sims–Huhner test) is an interesting test for examining the interaction of cervical mucus with the sperm. Sadly, this simple test is seldom performed in these days of the sophisticated ART clinic although a few facilities still offer it. The PCT looks at the sperm activity in the cervical mucus after sex. Because it must be carried out when there is fertile mucus present, i.e., close to the time of ovulation – the female partner is usually ‘tracked’ for several days with blood or urine tests to determine her hormonal status. She therefore has accurate warning of approaching ovulation. Fertile mucus leading up to ovulation can be removed on a swab and assessed for a number of criteria such as pH. On the day of ovulation or just before ovulation, the couple are requested to have sexual intercourse and then the woman attends the clinic some hours later for some of the fluid in the cervical canal to be removed and examined. A negative test shows no progressively motile sperm and a positive test shows more than five motile sperm per high power microscope field. Where the test is negative, the female partner sometimes receives the unfortunate label ‘hostile’ cervix or ‘hostile’ mucus. What this usually means is that there are antibodies in the mucus which disable or immobilize the sperm.
This test gives us a good idea about fertile mucus quality and sperm performance, and whether there are antibodies to the sperm. However, the useful information we receive from this cheap and non-invasive test does not necessarily influence what ART specialists can offer and so is often dispensed with by such specialists these days. For example, one prominent IVF specialist says,
Many couples will quite correctly opt for assisted conception whether the PCT is positive or negative. The complexities of timing the PCT, the indirectness of the limited information it provides and probability of recourse to treatment such as IVF irrespective of its result mean that many doctors dispense with it.8
In fact, timing the PCT is simple compared to the complexities of tracking with frequent blood tests and ultrasounds the artificially engineered menstrual cycles for IVF procedures. The information it gives us about the quality of the fertile mucus and the behavior of the sperm in it is as direct as any laboratory procedure so far designed in infertility investigations and while the information it provides is of course limited to events at the level of the cervix it is nevertheless useful when the couple are not ready to launch straight into the expensive and demanding technologic route. The relatively non-invasive PCT can provide information which is useful when pursuing other types of treatment. For example, a TCM practitioner can use to good advantage the results of a PCT – it tells us information about the Yin status of the female partner and how the Yin and the Yang of the two partners interact, nourish or facilitate each other. And, theoretically, the more we can refine our diagnosis and hone in exactly on the subtle nuances of this Yin–Yang dance, the more chance we have of exerting an effective influence on the couples’ fertility.
The oral contraceptive pill and fertile mucus
Some doctors have observed, and some pill manufacturers have published warnings about, a certain type of fertility impairment after stopping the combined oral contraceptive pill, even after the return of regular periods9: this condition occurs only in some women and seems to be independent of the number of years the pill has been taken. It appears that the mucus produced by the cervix in these women having difficulty getting pregnant after being on the pill is largely the G type, even though ovulation may be occurring. Thus, sperm cannot gain entry to the cervix.10 There is no medical treatment for this condition, which can last for up to 30 months in unfortunate women; however, applying the protocols outlined in Chapter 4 will address many different disorders of fertile mucus, including post-pill disturbances.
Other drugs and fertile mucus
• Antibiotics can provoke an overgrowth of vaginal candida or thrush in sensitive women. If this is severe, it will mask any evidence of fertile mucus. The thrush must be treated with antifungal agents (pharmaceutical or herbal) before the fertile mucus signs become clearly evident again.
• NSAIDs (non-steroidal anti-inflammatory drugs), used as analgesics, lower the prostaglandin levels and, as such, can influence the menstrual cycle and cause fertile mucus to become more scanty in some users.
• Antidepressants – including the selective serotonin reuptake inhibitors (SSRIs) – can also change the cervical mucus pattern, usually reducing the number of days of production of fertile mucus.
• Antihistamines can dry fertile mucus, since they dry most of the mucous membranes in the body.
• Clomifene, a fertility drug which stimulates pituitary activity, acts as an antiestrogen, inhibiting the function of the mucus-producing glands in the cervix.
Chinese medicine and fertile mucus
The TCM doctor is very interested in cervical mucus. The quantity and quality will tell us a lot about some important aspects of female fertility. Specifically, it reflects some aspects of the Yin energy. As we have seen before in Chapter 2, the Yin energy is an important prerequisite for not only ripening a mature, attractive and fertile egg but also for establishing a good ground for implantation – a thick and nourishing uterine lining. Fertile mucus is just one of a number of external cues we can use in assessing the Yin status.
If the fertile mucus is inadequate in quantity or quality, there are Chinese herbal treatments which can be used to address this. Earlier in this chapter, we described the different types of mucus produced by the different glands in the cervix. In Chapter 4, when we look more precisely at how Chinese herbs can influence the steps in the development of the egg and the preparation of the female body, you will see that the Blood and Yin tonics are important in the production of good-quality L mucus (and vaginal lubrication in general) but that small quantities of Yang tonics influence the production of the S mucus and finally, as Yang tonics are taken over a few more days, the P mucus.
Treatment which emphasizes quantity and quality of fertile mucus carries special importance if sperm numbers or motility are low. An environment which maximizes survival of sperm and encourages entry to the uterus may be all the advantage lightly handicapped sperm need.
Position of the cervix
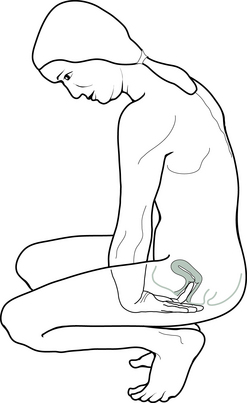
Some women find it useful to observe changes in the cervix itself as ovulation is approached. As the hormones signal the approach of ovulation, the shape, position and texture of the cervix changes. The ligaments that support the uterus respond to the peak of estrogen, which occurs just before ovulation by tightening: this has the effect of pulling the uterus further up in the body, and thus the cervix is positioned higher in the vagina. As the cervix moves higher in the vagina, it is a little more difficult to reach and some women find they need to squat to find its surface (Fig. 3.8). The texture of the surface of the cervix is softer at ovulation.
As the cervical glands release their fluid, the os of the cervix opens. This is clearly apparent to any woman who wishes to palpate the surface of her cervix. This can be checked conveniently at the same time as checking the fertile mucus, probably during the evening shower.
After ovulation, the position of the cervix is once again low in the vagina and quite easily palpated with a finger without resorting to contortionist antics.
Putting It All Together
The advantage of combining the BBT measurements with the observations of the cervix and its secretions is that they provide complementary information and can corroborate each other. Only the fertile mucus and LH predictor kits can indicate that ovulation is about to happen, but only the temperature shift observed in the BBT can show that ovulation has happened.
Once all these factors have been observed and charted throughout one menstrual cycle, what can we deduce? See, e.g., the chart shown in Figure 3.9. The numbers on this chart indicate:
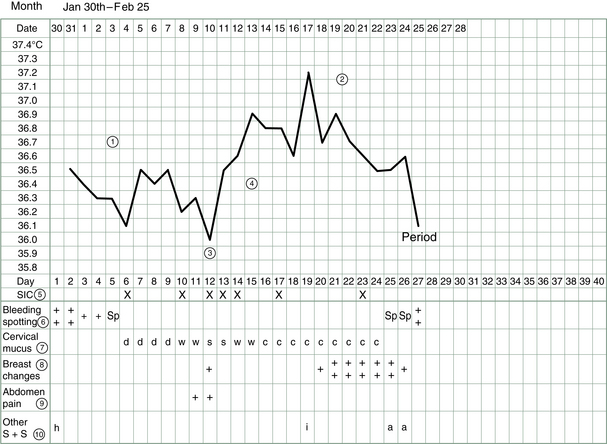
Figure 3.9 Example of BBT chart completed by patient. S + S = signs and symptoms; SIC = sexual intercourse.
1. Follicular phase – the first half of the cycle before ovulation should record relatively lower temperatures.
2. Luteal phase – after ovulation the temperatures should remain at a relatively higher level for 12–14 days.
3. Ovulation – the day before the temperatures become elevated is the most likely day of ovulation.
4. The thermal shift – the temperature rise should be 0.3°C or 0.4°C.
5. Sexual intercourse – frequency of sexual intercourse can be recorded in this column.
6. Bleeding – period flow and spotting can be recorded quantitatively with + signs.
7. Cervical mucus – changes such as the progression from dry to wet to slippery mucus are recorded. Different women may choose different symbols to record their observations (see below).
8. Breast changes – nipple tenderness and breast swelling or soreness can be recorded in this column.
9. Abdomen discomfort – ovulation or period pain can be recorded quantitatively with + signs in this column.
10. Other signs and symptoms – emotional changes, headaches, lower back pain or insomnia, etc., which may or may not be related to the menstrual cycle can be recorded in this column. A night of insomnia, drinking a lot of alcohol or fever can all push the BBT up. Individual symbols may be chosen. Any other events such as illness, travel or stress which might affect the cycle can also be recorded here.
In this particular chart (see Fig. 3.9):
1. The follicular phase average temperature was 36.3–36.4°C.
2. The luteal phase average temperature was 36.8°C; the elevated temperatures were maintained for 14 days, which indicates an adequate luteal phase and good progesterone levels.
3. Ovulation occurred on Day 12 or 13.
4. A thermal shift of 0.4°C between the average temperatures occurred.
5. Sexual intercourse occurred on Days 6, 10, 12, 13, 14, 17 and 23.
6. The period lasted 4 days with spotting on the day after the period and 2 days before the next period.
7. Cervical mucus was not evident after the period, i.e., the sensation was dry (d) until Day 10 and 11 when the vaginal sensation became wet (w) then slippery or stretchy (s) on Days 12 and 13. After ovulation the discharge was creamy or crumbly (c).
8. Breast swelling or soreness was experienced on the 6 days leading up to the period.
9. Some abdomen pain was experienced on the first day of the period and at ovulation.
10. A headache (h) occurred on the first day of the period and a night of insomnia (i) the night of Day 18, which pushed the temperature up on Day 19. Premenstrual anger was experienced (a).
BBT Charts and Pattern Diagnosis
The following methods of analyzing BBT charts were first described by doctors working in fertility clinics in China1 in the 1990s.
To begin with, we examine in some detail the sorts of patterns which might occur in the first 2 weeks of a menstrual cycle, i.e., before ovulation.
The follicular or low phase
Day 1 of the menstrual period is the first day of the follicular phase. From the day (or the day before) the menstrual period starts, the BBT should drop to its base level. This level can vary from woman to woman and to a lesser extent from cycle to cycle. Its average range is 36.2–36.5°C.
When the follicular phase is too low
The follicular phase of the cycle is naturally the lower phase of the biphasic graph; however, in some cases, the temperature readings are consistently extremely low (Fig. 3.10). If they are below the bottom level of the chart, i.e., below 36.0°C, this is an indication of a very low metabolic rate and low thyroid activity may be suspected. Accompanying symptoms which may be reported could be lethargy, weight gain and sensitivity to cold. Low thyroid activity is thought to affect fertility. In the most severe cases hypothyroidism can contribute to ovarian failure (this usually involves an autoimmune condition). Chinese medicine will describe this person as generally Yang deficient (or specifically Spleen and Kidney Yang deficient) and will apply treatment throughout the whole menstrual cycle to address this fundamental deficiency, i.e., to stimulate metabolism and warm the patient with the use of moxibustion and by using herbs that are heating in nature.
Later, when we examine the luteal phase, we will see a particular and specific type of Yang deficiency that affects the temperature of only the second phase of the cycle and possibly the progesterone levels produced after ovulation. This specific type of Kidney Yang deficiency may not involve general body symptoms and requires a special protocol of timed treatment which will be outlined in the next section.
When the follicular phase is too long
The length of the menstrual cycle is usually determined by the length of the follicular phase, i.e., the length of the follicular phase is variable, reflecting as it does the length of time it takes for the follicle in the ovary to grow to a certain size (around 2 cm) and then release a mature egg. In women with a 28-day cycle the follicular phase will typically be 14 days, but in women with a 35-day cycle this phase will last around 21 days and in women with a 24-day cycle it will be around 10 days. All are thought to be quite acceptable variations from the norm, although TCM treatment will attempt to steer the follicular phase towards 14 days.
Once ovulation has occurred, the luteal phase tends to be a standard 12–14 days, unless there is a defect in the function of the corpus luteum. This situation is described later in the subsection ‘Short luteal phase.’
According to TCM if ovulation is delayed (Fig. 3.11), then one of the prerequisite substances or conditions is absent or insufficient or the process of ovulation is obstructed (known as Qi stagnation) or the Shen or Heart is disordered (see Chs 2 and 4).
As described previously, the ‘nutrients’ required for an egg to develop to the point where it is ripe enough to be released and fertilized are the Kidney Jing, Kidney Yin and the Blood. If the Kidney Jing is insufficient, then ovulation will often be late or missed altogether in severe cases. Fertility can be severely compromised in these cases and even if conception is achieved the fetus may not be viable. The medicinals which strengthen Kidney Jing and Yin and nourish the Blood will be prescribed, often for a lengthy time.
During these cycles with extended follicular phases the woman may notice the fertile type of cervical mucus for longer than usual, or none at all.
When the follicular phase is too short
If the follicular phase is consistently short, say only 9 or 10 days (Fig. 3.12), then the TCM practitioner will use treatments to attempt to lengthen it. Often it will be necessary to clear Heat so that ovulations are not provoked prematurely.
The reason for this is that the egg and the follicle must not only grow to a certain size but must also reach a certain level of maturity, which takes time and energy and nourishment. The body loses blood and energy reserves during the period and these must be replaced in the days immediately following. At the same time, Yin and Blood reserves are required to nourish the rapidly developing follicle with its egg. If the egg is released only a few days after the end of the period, chances are it will not be as fully developed as possible. (Sometimes there is an egg already half-ripened from the previous cycle which is ready to leave the rank rather rapidly, but this tends to produce an unusually short cycle rather than a consistently short cycle.) Both herbs and acupuncture can be used to lengthen the follicular phase: to achieve this, treatment needs to begin before the end of the period, preferably around Day 3, so that the functions of the Chong and the Ren vessel can be reprogrammed.
When the follicular phase is too high
Some women have consistently high BBT readings, even in the pre-ovulatory phase (Fig. 3.13). This may reflect a high metabolic rate and possibly hyperactivity of the thyroid gland. The condition may be accompanied by a fast heart beat, feelings of agitation, insomnia or weight loss. In TCM, we generally attribute such a pattern to a phenomenon known as internal Heat. This condition predisposes to production of cervical mucus that is scanty or too acid or which contains antisperm antibodies. In addition, the endometrial lining may be too thin or dry. Therefore, measures must be taken to clear such Heat. This usually means using herbs which ‘clear Heat’ and reinforce Yin.
At the beginning of the follicular phase, i.e., the beginning of the new cycle, Day 1 of the period, if the temperature has not already dropped (ideally it should drop the day the period begins or the day before) or drops some time during the period or even after the period (i.e., Day 3–7) then some internal imbalance may be suspected (Fig. 3.14).
In TCM terms, this particular phenomenon is described as a failure of Yang transforming to Yin (see Ch. 2) but in clinical practice it can alert us to the possibility of an underlying condition such as endometriosis. The way TCM sees it, it reflects an incomplete discharge of all the endometrial blood, such as happens when endometrial implants outside the uterus bleed into the pelvic cavity or into a cyst. The TCM practitioner will attempt to correct this pattern by applying treatment from Day 1 of the period to facilitate complete discharge of blood and the switch from Yang to Yin. Underlying causes will then be addressed at other times of the cycle.
When the follicular phase is unstable
The values of BBT recorded in the follicular phase should be reasonably steady: not the same each day of course, but not varying (Fig. 3.15) by more than about 0.2 or 0.3°C (0.5°F). Fever, lack of sleep or alcohol consumption will cause unusually high readings.
If there are unexplained peaks and troughs in the chart from day-to-day, we describe these in Chinese medical terms as expressions of Liver- and Heart-Fire. What this means is that at some level the Shen is uneasy and treatment which clears Heat and reinforces Yin will be applied at this time to calm the mind. The patient will be encouraged to reduce stress and lead a more regulated life, incorporating relaxation techniques.
A summary of follicular phase patterns is given in Table 3.2.
Table 3.2
Summary of follicular phase patterns
| BBT Pattern | Diagnosis | Treatment |
| Low follicular phase | Generalized Yang deficiency | Warm Yang throughout cycle |
| Long follicular phase | Deficiency of Kidney Jing, Yin or Blood | Nourish Blood, reinforce Kidney Jing and Yin after the period |
| Short follicular phase | Heat, usually Yin-deficient Heat | Clear Heat and nourish Yin from early in cycle |
| High follicular phase | Heat, usually Yin-deficient Heat | Clear Heat and nourish Yin from early in cycle |
| High follicular phase initially | Obstruction of transformation of Yang to Yin | Promote Kidney Yang to Yin transformation, regulate period |
| Unstable follicular phase | Liver- or Heart-Fire | Clear Liver- or Heart-Fire, calm the mind |
Ovulation
As the follicle keeps growing (in response to stimulation by FSH from the pituitary), it will produce large quantities of estrogen. In some women, this has the effect of making the BBT drop a little (see Fig. 3.9, Day 12).
Some women notice this on their BBT charts and others do not. Because this peak of estrogen only lasts about 12 h its effect may not be detected on an early morning temperature reading if it happened for example between 10 a.m. and 10 p.m. In most women it has the effect of stimulating the cervical glands to produce fertile mucus. Women who are using a urine LH detection kit should notice that it becomes positive around this time.
It is the effect of the next hormone produced by the ovary, progesterone, which brings about a marked change in the BBT. In most women, as soon as progesterone is produced, the BBT rises quite markedly, i.e., 0.4–0.5°C (up to 1°F). We are not sure why basal temperature rises but, whatever the reason is, it is important, because progesterone and its action of warming the body (by acting on the temperature-regulating centers in the hypothalamus) is found throughout the evolution of mammals. Levels of progesterone remain high throughout pregnancy, so it is clearly considered an advantage to the embryo and the developing baby to be in a slightly warmer than usual environment.
The effect of progesterone can also be seen in measurable differences in metabolic rates during sleep – they are lowest at the end of the low phase (follicular phase) and highest at the end of the high phase (luteal phase).11,12
Thus, charting tells us at this point, when the waking temperature is registering higher on our chart, that ovulation has occurred.
Once 2 or 3 days of elevated temperatures have been recorded, then attempts at conceiving can be abandoned for another month. The egg survives for a very short time (about 12 h) after it is released and once the body has registered the circulating progesterone by raising its BBT significantly, then the egg has usually been and gone. You can see why charting temperature on its own is not a very useful tool for choosing when to try to conceive. However, several months of BBT graphs convey a good understanding of the hormonal comings and goings of the body and, when combined with observations of other signs, provides an extremely accurate record of the most fertile days.
As soon as progesterone starts to circulate, the cervical mucus dries up rapidly and the entrance to the cervix is blocked with an impenetrable (to sperm) ‘Keep Out’ sign. This secretion is thick and crumbly and white. The vaginal sensations will tend to be dry.
The drying up of the cervical fluid marks the end of the Yin phase and the rise in temperature indicates the successful switch from Yin to Yang.
The luteal or high phase
The temperature readings taken in this part of the cycle are a little more steady than in the follicular or low part of the cycle. This is because hormone production by the corpus luteum (tucked away inside the ovary) is less affected by external and emotional upheavals than are the hypothalamus and the pituitary (in the brain), which are more vulnerable to the influence of the external world and the emotions. Ideally, BBT values should waver no more than 0.1°C (0.2°F). In general, once the temperature has lifted by 0.3–0.5°C (1°F), it should maintain this level for at least 11 or 12 days, and preferably 13 or 14 days. If a menstrual cycle is shorter than 28 days, it usually means that ovulation has occurred early. However, it sometimes means that the luteal phase is inadequate. The temperature drop which occurs towards the end of a cycle signals the disappearance from the system of progesterone, i.e., the corpus luteum has disintegrated and is no longer producing this hormone. The longest the corpus luteum can be expected to survive in the absence of a pregnancy is 16 days, but 12–14 days is more typical. With the drop in the progesterone, the lining of the uterus loses its glue, so to speak, and will start to disintegrate and the period begins. If a conception has occurred and the embryo has successfully negotiated the trip down through the tubes and is also successful in embedding in the endometrium, the corpus luteum will be given a signal to continue producing progesterone until such time as the developing embryo can produce its own (about 8 weeks later).
The luteal phase is sometimes called the ‘inadequate luteal phase’ in gynecology texts if the corpus luteum does not keep the production of progesterone up for long enough to allow the newly arrived embryo to implant and develop in the endometrium.
When the second part of the cycle is not ideal, i.e., the temperature climbs too slowly or drops too soon or wavers up and down or doesn’t reach a higher enough temperature, it is said in Chinese medicine that the Yang of the Kidney is insufficient. One of the functions of Yang is to warm the body, and any deficiency in heat or metabolism will be ascribed by TCM to Yang deficiency.
Let us now look at the different sorts of patterns which may occur in the luteal phase and how TCM analyzes them.
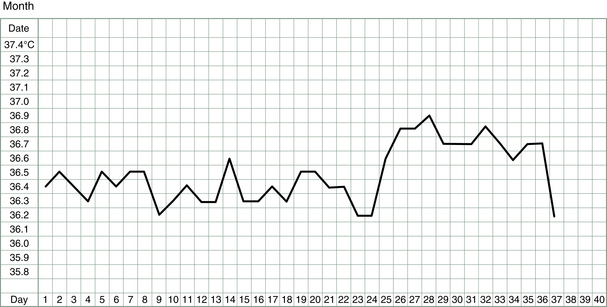
When the luteal phase is too short
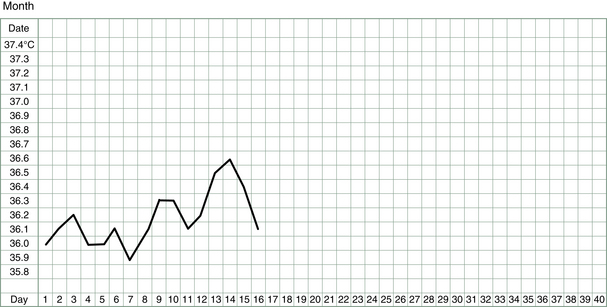
TCM evaluates any degree of Kidney Yang deficiency from the length of the luteal phase (i.e., how far short of 14 days is the period of time between ovulation and the first day of the period). In ideal situations it is a minimum of 12 days, preferably 14 days. If the rise in temperature only lasts for 3 days (Fig. 3.16), then one cannot even be sure that ovulation has occurred.
In such a case, the menstrual cycle may be barely 2½ weeks long. Blood tests may be necessary to determine if ovulation is occurring and, if it is not, the TCM practitioner will treat this case in the same way she would amenorrhoea (see Ch. 5). Kidney Jing, Yin or Yang tonic herbs will be prescribed to improve the quality of ovulation or the use of fertility drugs may be advised.
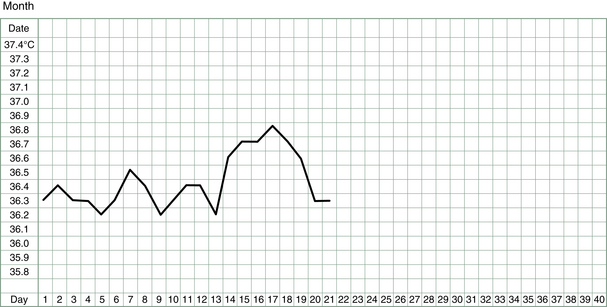
If the luteal phase is 5 or 6 days (cycle may be about 3 weeks long), then ovulation probably has occurred (Fig. 3.17) but large doses of Kidney tonic herbs will be used at different times of the cycle to improve the corpus luteum function and in some cases simultaneous use of drugs may be recommended.
A luteal phase that typically lasts 8–10 days (Fig. 3.18) reflects a milder Kidney weakness but one which nevertheless can compromise fertility because progesterone support will not be sufficient to ensure implantation.
Clomifene (Clomid), a well-known fertility drug, is often given for problems with ovulation, including inadequate luteal phases. In general the drug works very effectively in lengthening and raising the temperature in the luteal phase.
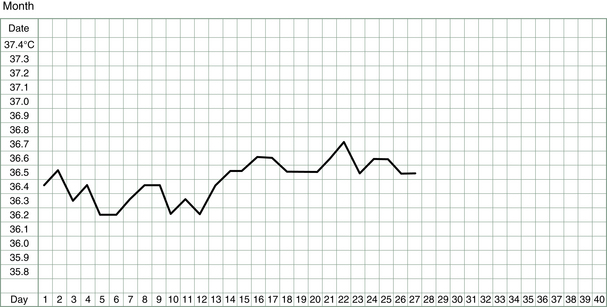
When the luteal phase is too low
After ovulation and the production of progesterone the temperature should ideally rise 0.4–0.5°C (1°F). The absolute values of temperature readings in the two phases is not as significant as the difference between them. A rise of 0.3°C is thought to be just adequate and a rise of 0.1 or 0.2°C is called a low luteal phase (Fig. 3.19) and represents a failure of Kidney Yang to properly fulfill its function. In this case, the Kidney Yang is weak right from the beginning of the luteal phase, whereas in the previous pattern it warmed the body to some degree but could not sustain it for long enough. In the case of a low luteal phase, we need to do more than strengthen the Kidney Yang function; we need to strongly build the very foundation of Kidney Yang – namely, Kidney Yin. It is only when Kidney Yin provides a strong base that Kidney Yang can grow out of it. And in some cases (depending on the clinical symptoms) it is the Qi or Blood which needs building before Kidney Yang can develop in the post-ovulatory phase.
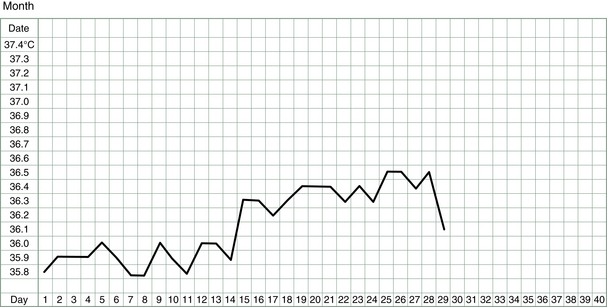
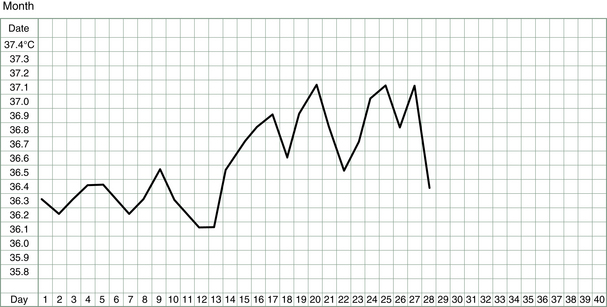
When the luteal phase is unstable
In the sawtooth pattern (Fig. 3.20) the BBT rises adequately at ovulation but it will drop and rise again over the course of the luteal phase. This pattern represents instability of the Heart and Liver Qi concurrent with Kidney Yang deficiency. The basis of such instability is nearly always emotional and often manifests in the follicular phase as well as the luteal phase especially where there is Kidney Yin deficiency. If luteal phase temperatures are higher then expected, or there are a number of high peaks, Liver Fire must be suspected.
Treatment of this pattern may require concomitant relaxation techniques and attention to stress reduction. The best way to stabilize the sawtooth luteal phase is to promote Kidney Yang by nourishing Blood. This involves the use of Blood tonics in combination with Kidney Yang tonics and has the result of calming the Liver and the Heart.
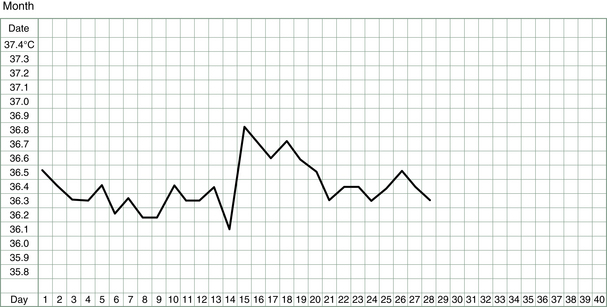
In the saddle pattern, the instability in this BBT is shown in a sudden and predictable plunge in the temperature about 1 week after ovulation (Fig. 3.21). There is a second smaller surge of estrogen during the luteal phase, which may in some women cause a drop in BBT for a day. The cervical glands may also respond to this estrogen, and more secretions may be noticed on this day.
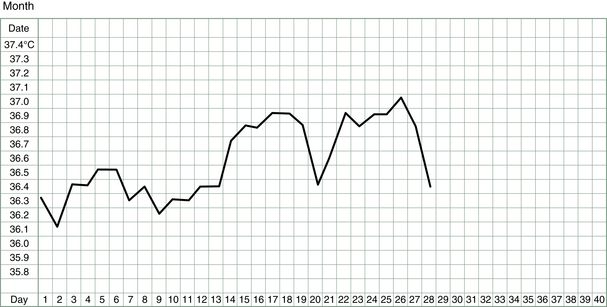
Surges of estrogen or drops in progesterone at this stage of the cycle indicate both lack of firm Kidney Yang and instability in the Heart and Liver. Generally, this is not a serious impediment to fertility because the Kidney Yang is not very deficient, as evidenced by the recovery of a good temperature level that is maintained until the end of the luteal phase (or into early pregnancy). However, because the disruption occurs at such a sensitive time in the cycle, just at the point where implantation is occurring, the TCM practitioner will attempt to change this pattern by boosting Kidney Yang and stabilizing the Heart and the Liver Qi.
When the luteal phase rises too slowly
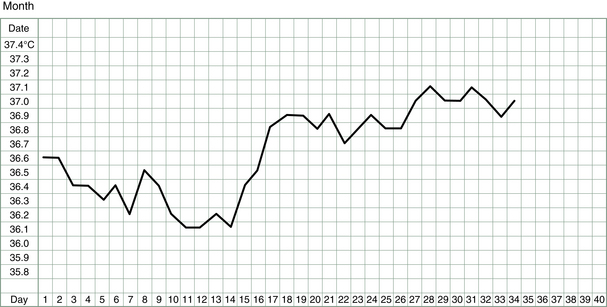
The luteal phase temperature reached in this pattern (Fig. 3.22) is eventually high enough for us to be convinced that progesterone and Kidney Yang levels are adequate; however, it takes several days (>3) for the temperature to rise after ovulation rather than the usual 1 or 2 days.
Some women observe the changes in the cervix and fertile mucus indicating ovulation well in advance (by some days) of the temperature rise. However, when the temperature rise does come it is quite clear that ovulation has indeed occurred. It is thought that these women may be slow to react to the circulating progesterone, their bodies taking a few days before the BBT is raised.
TCM classifies this pattern as a deficiency of Kidney Yang combined with Spleen Qi and Yang deficiency. In some cases there may be underlying Yin deficiency also or Liver Qi stagnation.
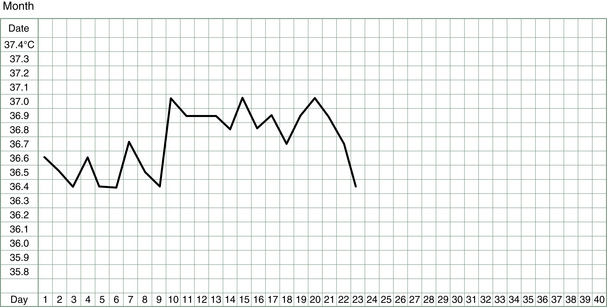
When the luteal phase declines too early
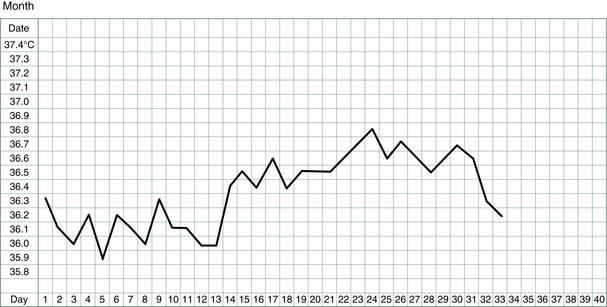
In this pattern (Fig. 3.23), the luteal phase lasts the usual 13 or 14 days until the start of the period but the temperature declines rapidly from its peak shortly after ovulation. It is normal to find that the temperature drops a day before the period starts, but it should not drop before that.
In TCM, this pattern indicates a form of Kidney Yang deficiency combined with Spleen Qi deficiency. Even though the period does not come early, the fact that the temperature has dropped indicates the decline of the Kidney Yang. The lack of Spleen Qi integrity is sometimes the cause of blood not being held securely in the endometrial blood vessels and so we may see some premenstrual spotting in this pattern. Of course an early decline of progesterone levels is another way of describing the phenomenon of premenstrual spotting.
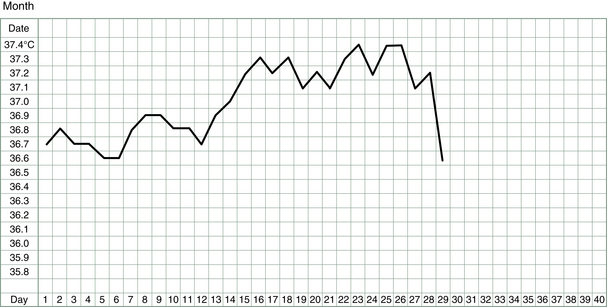
When the luteal phase is higher than usual or lasts longer than usual
This pattern represents no irregularities or malfunction; in fact, it indicates pregnancy (Fig. 3.24). There are a couple of other signs which may indicate pregnancy. As mentioned earlier, the egg is fertilized in the fallopian tube and then begins a slow journey down the tube as an embryo, which gradually divides into more and more cells. It reaches the uterus several days later and implants in the endometrium. When this happens there may be some slight spotting as the endometrium is disturbed. At this point too, the BBT may reach a higher value than recorded before, as more progesterone is produced in response to the implantation. Once 10 high temperatures have been recorded, a sensitive urine test will register the pregnancy hormone, human chorionic gonadotrophin (hCG), produced by the embryo.
Sometimes this pattern is confusing because a period still comes but the temperature does not drop. It is not so very unusual for periods to keep occurring at the expected monthly interval as many as 3 months into the pregnancy. Most often, the bleeding will be scantier than a normal period but occasionally this is not the case. Charting the basal temperature then is really the only way (other than to have frequent blood tests or ultrasounds) to confirm the ongoing existence of the pregnancy.
Some women may pick up a disturbing trend when they begin charting and that is that they are conceiving sometimes but suffering early stage miscarriages (Fig. 3.25).
In these cases, the temperature will stay elevated more than 16 or 17 days but fall not much later, so that it appears to just be a long cycle. If this pattern is repeated, then steps will be taken to prevent it in the future.
In some rare cases, the temperature will stay elevated because a corpus luteum cyst develops. This has the effect of maintaining the corpus luteum and its progesterone output past its usual lifetime; hence the period doesn’t come. A pregnancy test will be disappointingly negative but the corpus luteal cyst can be expected to resolve on its own. BBT patterns in the luteal phase are summarized in Table 3.3.
Table 3.3
BBT patterns in the luteal phase
| BBT pattern | Diagnosis | Treatment |
| Short luteal phase | Kidney Yang deficiency arising from Yin deficiency | Strongly supplement Kidney Yin in follicular phase to create Yang in luteal phase |
| Slightly short luteal phase | Kidney Yang deficiency | Boost Kidney Yang in luteal phase |
| Low luteal phase | Kidney Yang deficiency | Nourish Kidney Yin and Blood, boost Kidney Yang in luteal phase |
| Unstable luteal phase – sawtooth | Liver/Heart Qi unstable, Kidney Yang deficiency | Regulate Liver/Heart Qi, calm Liver Fire, boost Kidney Yang by nourishing Blood |
| Unstable luteal phase – saddle | Kidney Yang deficiency, Liver/Heart Qi unstable | Reinforce Kidney Yang, regulate Liver/Heart Qi |
| Slow-rise luteal phase | Kidney Yang deficiency, Spleen Qi deficiency | Reinforce Kidney Yin after period, invigorate Spleen Qi from early midcycle and boost Kidney Yang in the luteal phase |
| Early-decline luteal phase | Kidney Yang deficiency, Spleen Qi deficiency | Invigorate Spleen Qi and boost Kidney Yang in luteal phase |
| Long luteal phase | Pregnancy | Support Kidney Yang if necessary |
More on Discharges
Some vaginal discharges do not originate in the cervix and some that do originate in the cervix are not the fertile type. For some women there is a marked increase in the thick and rather dry or pasty discharge of the post-ovulatory phase in response to high progesterone levels (which can encourage growth of vaginal yeast organisms). It is not uncommon for women to notice an increase in thin or slippery discharge just before the period. This may just reflect the drop in progesterone as the corpus luteum stops functioning and does not indicate a fertile time. Or this thin discharge may be the beginning of fluid loss from the endometrial lining of the uterus.
Other women sometimes report seeing a moist or creamy discharge in the middle of the luteal phase. This may reflect a small surge of estrogen, which can occur at this stage, stimulating the cervical glands. This discharge does not indicate a second fertile period for that cycle.
Yet other women will notice some constant form of discharge all the way through the cycle right from the end of the period. This may be just a natural physiologic discharge which, if it is not associated with any infection or inflammation, is said to be quite normal for that woman. Although this is quite correct from a Western medical point of view, from the TCM point of view any excess discharge of fluid or mucus from the body is thought to reflect a disorder in the fluid metabolism. Often people with excess mucousy discharges (from various orifices) are said to be ‘Damp’ and it is the job of the TCM practitioner to help to correct this imbalance.
Clearly, determining fertile (and non-fertile) days in women with chronic discharge is not quite as simple as it is for women who have dry days before and after ovulation. A woman prone to Damp must closely observe any changes in the constant discharge, particularly toward wetter or more stretchy type of mucus, in order to ascertain the fertile period. Once again, the peak day of fertility will be the last day that this different sort of mucus is observed before the return of the usual discharge. If treatment clears the Damp successfully, observation of fertile mucus becomes easier.
Sometimes a vaginal discharge can mean an infection. It will usually have a different or offensive smell, may be colored (yellow or green) and may cause inflammation of the vagina or vulva. It is important that such infections are treated promptly (usually with antibiotics or antifungals, although herbs can also be very effective) and that intercourse is avoided until the infection or soreness is resolved. This is to prevent cross-infection and also to avoid discomfort or trauma to the inflamed tissue. Another sort of pathologic discharge may arise from inflammation of the cervix. This may be a watery sort of discharge and will not be offensive like an infection but may still be irritant. Although there is no drug treatment for such a discharge, TCM can treat it effectively with herbal decoctions and douches. For treatments of vaginal discharges, the reader is referred to TCM gynecology texts.13
References
1. Cheng, X.G. Use of the basal body temperature in pattern discrimination for patients with infertility and amenorrhoea. Shanghai J TCM. 1992;10:18–19.
2. Billings, E.L., Billings, J.J., Brown, J.B., et al. Symptoms and hormonal changes accompanying ovulation. Lancet. 1972;1:282–284.
3. Billings, E.L., Westmore, A. The Billings method. Melbourne: Anne O’Donavon; 1998. [203].
4. Hatcher, R.A., Trussell, J., Stewart, F., et al. Contraceptive technology, 16th edn. New York: Irvington; 1994.
5. Gray, R.H., Simpson, J.L., Kambic, R.T., et al. Timing of conception and the risk of spontaneous abortion among pregnancies occurring during the use of natural family planning. Am J Obstet Gynecol. 1995;172:1567–1572.
6. Royston, J.P., Abrams, R.M., Higgins, M.P., et al. The adjustment of basal body temperature measurements to allow for time of waking. Br J Obstet Gynaecol. 1980;87(12):1123–1127.
7. Odeblad, E., Hoglund, A. The dynamic mosaic model of the human ovulatory cervical mucus. Proc Nordic Fertil Soc. 1978. [January].
8. Jansen, R.P.S. Getting pregnant. Sydney: Allen and Unwin; 2003. [62].
9. Schering Pty Ltd. Notes distributed with Triquilar and other combined oral contraceptives. Tempe: Wood St; 2012.
10. Billings, E.L., Westmore, A. The Billings method. Melbourne: Anne O’Donavon; 1998. [174].
11. Meijer, G.A., Westerterp, K.R., Saris, W.H., et al. Sleeping metabolic rate in relation to body composition and the menstrual cycle. Am J Clin Nutr. 1992;55(3):637–640.
12. Bisdee, J.T., James, W.P., Shaw, M.A. Changes in energy expenditure during the menstrual cycle. Br J Nutr. 1989;61(2):187–199.
13. Macioca, G. Obstetrics and gynecology in Chinese medicine. London: Churchill Livingstone; 1998.