Male Infertility
Introduction
About one in five Australian couples have difficulty conceiving children. Male infertility is a contributing factor in half of these cases. Extrapolating these figures to the developed world translates into very large numbers of distressed couples seeking medical help for infertility. For example, there are more than 3 million men considered infertile in the USA; these are the ones trying to be fathers already but there are many more who don’t yet know their fertility status, because they haven’t yet tried to have children.
Where and How Sperm are Made
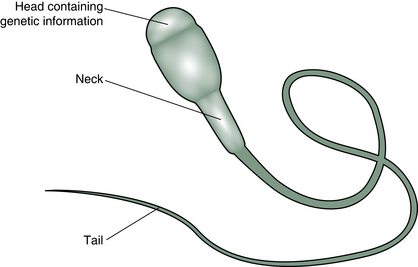
The sperm, known in biological circles as a ‘spermatozoon’, is a long thin cell with a head which contains the genetic material and a tail which propels the genetic material towards its destiny (Fig. 7.1).
The Sperm Factory
Sperm are made in the male gonads, which are known as the testes or testicles. These organs hang outside the body in the scrotum. The temperature in the scrotum is several degrees lower than that in the abdominal cavity just above it, and this low temperature seems to be important for the function of the sperm-making cells. Just 24 h of raised scrotal temperatures will cause malfunction of sperm production in animal studies.1
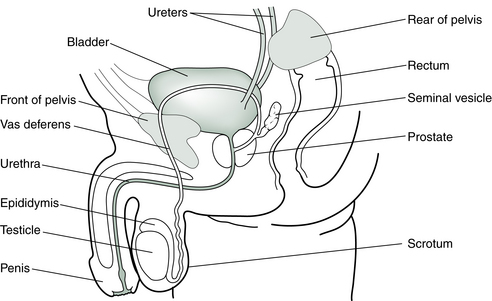
The sperm form over a period of about 48 days in the tubules in the testes, nurtured by the Sertoli cells, in sequential generations at different stages of development. They then spend 2 or more weeks in the epididymis (a fine, coiled tube 6 m long and about double the width of a scalp hair) to mature before moving into the vas deferens and the urethra on their way out of the body (Fig. 7.2). The ejaculate contains a mixture of sperm and fluid from the prostate gland and seminal vesicles.
Because of the long development and maturation time of sperm cells, events in a man’s life can have far-reaching (in time) effects on the quality of his sperm, e.g., an episode of high fever which wreaks some havoc on the delicate internal machinery of the testes can still influence adversely the quality of the sperm being ejaculated 9 or more weeks later.
To be considered fertile, the male of the human species needs to deposit a minimum of 40 million sperm in the female vagina during intercourse in the hope that just one will have a successful encounter with the egg. Once inside the acid environs of the vagina, few sperm can survive and within just a few minutes, the walls are littered with the corpses of millions. Over the next few hours all but a few are dead. The survivors are the sperm which were able to negotiate a passage through the cervix with the help of the protective cervical mucus and the dipping action of the cervix at orgasm, followed by the contractions of the uterus which propel the sperm into its higher reaches. Once inside the female reproductive tract, the sperm will be lured towards the egg in the tube by chemical signals.
Semen Analysis
Male fertility is investigated first by a sperm analysis performed in a pathology laboratory. A sperm test requires the collection, in a sterile plastic jar, of an ejaculation, which is then quickly examined in the laboratory. The sample is usually collected at least 24 h after the previous ejaculation. Doing a sperm test after 5 or more days of abstinence is not helpful because once the sperm have passed through the epididymis and are waiting in the testes for too long, their motility can diminish.
Normal Parameters
Current World Health Organization (WHO) standards2 for assessing male fertility are:
• Volume: more than 1.5 milliliter (mL)
• Count: more than 15 million sperm per mL
• Motility: more than 50% moving vigorously and purposefully
• Morphology: more than 4% normal forms (i.e., no deformities of the head, midpiece or tail).
‘Normal’ parameters, as they were defined less than two decades ago, described sperm counts of twice this amount and a much higher percentage of normal forms. The average sperm count has decreased by 1–2% per year from a substantially higher number decades ago.3 Standards for deposits in sperm banks have thus had to be lowered, or too many donors would nowadays be rejected.
Another way of assessing male infertility is to do retrospective studies of couples achieving or not achieving pregnancy. When a large population of men was studied, those who had succeeded in fathering a child in the previous 2 years had more than 48 million sperm/mL, with more than 63% moving, and more than 12% with normal morphology. Infertility was most likely if a man’s sperm count was less than 13.5 million sperm/mL, with less than 32% moving, and less than 9% having a normal shape. Men falling between these two groups had borderline fertility but could still establish a pregnancy.4
Sometimes a single ejaculate might give misleading results, especially if the sample was taken when the man was stressed. In such cases, the ejaculate will be a small volume and sperm from the vas deferens may not be ejected into the semen effectively. So, if a single test provides a low count it is always worth repeating the collection of the sample under different circumstances.
On average, we can expect to find about 500 million sperm in one ejaculate of a healthy fertile male. If all these sperm were capable of fertilizing an ovum, theoretically one ejaculate could impregnate all the fertile women of China. In reality, however, the chance of one particular sperm penetrating the egg is less than the chance of winning a million dollar lottery!
Some couples, however, have no trouble getting pregnant with sperm counts lower than normal. Some researchers in the field have gone so far as to say that sperm density tests are not always useful in distinguishing fertile from infertile men and are not useful in diagnosis or in monitoring the progress of treatment for male infertility.5 Ultimately, all that is really needed is one sperm!
Increasingly, andrology labs are finding that even normal looking sperm may have damage to their DNA. Oxidative stress – stress on the body that is caused by the cumulative damage of free radicals – is the main contributor to sperm DNA damage or fragmentation. A DNA fragmentation test will measure how much breakage there is in the DNA strands of the sperm chromosomes and give a DNA Fragmentation Index (DFI) score to indicate the likelihood of sperm contributing to infertility. The following scores indicate fertility potential for natural conception (or using IUI):
As many as one-third of men being investigated in the infertility clinic will show significant (>25%) damage to the sperm DNA. Causes include exposure to environmental and occupational pollutants, cigarette or drug use, infections, elevated testicular temperature (from using laptop computers, or frequent use of saunas and hot baths or from a varicocele), chronic diseases such as diabetes, cancer and cancer treatment, and poor diet.
These men are encouraged to avoid pesticides and other environmental toxins, heat sources and smoking, and to increase antioxidant intake. (See Ch. 12 for more discussion.) Frequent ejaculation (i.e. daily) is recommended to reduce the length of time sperm are exposed to reactive oxygen species in the testicular ducts.
More realistic assessment can be made of the working sperm’s performance if it is examined in a situation closer to real life, i.e., how the sperm behave in the medium of the mucus produced by the cervix at ovulation, not the confines of a plastic jar or a microscope slide. Now we are looking at the dance of female and male, Yin and Yang, together. A healthy display of flourishing Yin in the form of copious fertile mucus can nourish and enhance the Yang attributes of the sperm, i.e., they can swim and progress better. So, given the right environment, those healthy sperm from among a less impressive or sparse cohort may be selected and transported along by plentiful cervical mucus. However, this test (the post coital or Sims Huhner test) is seldom offered in ART clinics these days.
Declining Sperm Counts
There has been a lot of press about the precipitous decline in sperm counts over the last few generations. The average male sperm count dropped 45% from 113 million/mL in 1940, to 66 million/mL in 1990. Also the volume of semen dropped, effectively making the reduction in total numbers of sperm per ejaculation 50%. The number of men with low sperm counts (<20 million/mL) has tripled (from 6% to 18%), while the percentage with high sperm counts (>100 million/mL) has decreased. The more recently a man was born, the lower the average sperm count and the greater the number of abnormalities.6
Such a trend means that an average 30-year-old man today would have a sperm count about one-quarter the count of that of the average male born in 1925.
Such figures lead some specialists to speculate that if the decrease in sperm counts were to continue at this rate, in a few years we will witness widespread male infertility.3
The cause of this decrease appears to be the increased exposure to environmental pollutants, either during the time in the womb or later in life. PCBs (polychlorinated biphenyls), dioxin, phthalates, phenols and several pesticides such as DDT, have been shown to have a harmful effect on sperm as have the solvents used in manufacturing adhesives and printing inks and paints. Pregnancies of the partners of men exposed to damaging substances are also affected, experiencing a higher rate of stillbirth and premature delivery.7 Many of these substances and other chemicals used in farming or industry act like estrogens or anti-androgens.8–10 We will revisit this topic in more detail in Chapter 12.
The fact that sperm counts are lower in younger men than older men indicates that some of the damage may be occurring in the womb. It is thought that higher than normal estrogen levels in the womb might limit the number of sperm a man produces in adulthood by inhibiting the development of the Sertoli cells in the forming testicles. Since each of the Sertoli cells (which play an important role in the production of sperm) can only support a fixed number of sperm, the number a male acquires early in life will ultimately limit the quantity of sperm he can produce as an adult.
While the body is able to break down and excrete natural plant estrogens, many of the man-made compounds which act like estrogen resist normal breakdown and accumulate in the body, exposing humans and animals to low-level but long-term exposure. This pattern of chronic hormone exposure is unprecedented in our evolutionary experience and adapting to this new hazard is a matter of millennia not decades.11
Prescribed drugs may also be implicated in reduced sperm counts. In some cases, the effects of these drugs last for months after they have been discontinued. Testosterone replacement therapy, anabolic steroid use, cancer medications, certain antibiotics, some blood pressure medications, some ulcer or reflux medication, drugs for ulcerative colitis and some antidepressants have been observed to affect sperm production (Table 7.1).
Table 7.1
Some pharmaceutical drugs and their possible effects on sperm
| Class of drug | Effect on sperm |
| Drugs for high blood pressure: | |
| e.g., spironolactone | Lowers sperm count |
| e.g., calcium channel blockers | Interfere with binding of sperm to egg |
| Drugs for peptic ulcers or reflux: | |
| e.g., cimetidine | Lowers sperm count |
| Drugs for ulcerative colitis: | |
| e.g., salazopyrin (sulfasalazine) | Lowers sperm count |
| Testosterone and anabolic steroids | Lower sperm count |
| Some chemotherapy drugs | |
| e.g., methotrexate | Lowers sperm count |
| Drugs for epilepsy: | |
| e.g., phenytoin | Lowers sperm count |
| Drugs for urinary function: | |
| e.g., nitrofurantoin | Affects sperm motility |
| Drugs for gout; | |
| e.g., allopurinol, colchicine | Lowers sperm count |
| Antifungal medication: | |
| e.g., Grisovin and/or Griseostatin (griseofulvin) or ketoconazole | Lowers sperm count and increases abnormal forms |
| Drugs for depression | |
| e.g., SSRIs serotonin reuptake inhibitors | May lower sperm count and motility |
| Some antibiotics | |
| e.g., tetracycline, erythromycin, gentamicin and nitrofurantoin | Lower sperm count, affect morphology |
Age and Sperm
It has long been known that a woman’s reproductive capacity reduces as she ages. But until recently, it has been assumed that the age of the male partner was irrelevant to the question of fertility – there are plenty of stories of septuagenarians impregnating younger women. It has taken a long time for the researchers to take a hard look at the influence of age on male fertility. The first indications that age might be relevant emerged from studies of miscarriage rates in couples of different ages (see Ch. 8) and, more recently, research has examined the effect of male age on conception rates. This has shown that the older a man is, the longer it is likely to take his partner to conceive, irrespective of her age. The study concluded that in a couple who eventually have a baby, the probability that it will take more than 12 months to conceive nearly doubles, from around 8%, when the man is younger than 25 years, to around 15%, when he is older than 35 years. In other words, men as well as women have a biological clock that starts ticking (though perhaps not so urgently) as they get into their 30s (Fig. 7.3).12

Figure 7.3 The older a man is, the longer it is likely to take his partner to conceive, irrespective of her age.
IVF outcomes are significantly reduced in couples where the husband is more than 50 years of age.13 Particularly, it is the morphology and motility that declines with age.14
Constriction and Heat
Putting pressure on the testicles reduces sperm motility. Men whose sperm are not swimming so well are advised to stop putting pressure on them by avoiding tight underpants or cycling a lot.15
The effect of overheating the testicles with saunas or hot tubs or laptops has also been examined by various groups and it turns out that men with poor sperm quality are better off jumping in the ocean or a swimming pool rather than the hot tub or the sauna.16
More discussion of lifestyle and environmental effects on sperm count and quality can be found in Chapter 9.
Antisperm Antibodies, Vasectomies, Varicoceles, and Other Blockages
The organs which make sperm and the tubes that carry them are physically isolated from the body’s immune system. If this physical barrier is damaged, then the immune system is likely to tag the sperm cells as foreign and attack them with antibodies. A sperm thus coated with antibodies may die or stop swimming well or stick to its mates or just lose the ability to penetrate the egg.
If there is a blockage in the tubes carrying the sperm, whether this is from an infection or from a vasectomy, the sperm accumulate at the obstruction, causing irritation and inflammation, and an immune response is initiated. Even if this blockage is later removed by surgery, the immune reaction to the sperm persists, which sadly means that most reversed vasectomies are not successful in terms of future pregnancy. Sperm reappear in the semen in about 75% of men who undergo the procedure. Only 25–40%, however, then manage to father children naturally. In addition to the problem of antibodies, it is thought that the repaired epididymis does not adequately perform its function of maturing the sperm. Although of course, the sperm which do appear in the semen after a reversal are able to be used in an IVF cycle combined with intracytoplasmic sperm injection (ICSI).
Sperm which come into contact with the bloodstream of a female partner can also provoke an immune response. Since many sperm reach the abdominal cavity of a sexually active woman (by swimming out the top of the fallopian tubes), it is surprising that there are not more problems caused by women producing antisperm antibodies. But where there is an immune reaction, it is harder for sperm to traverse the fallopian tubes without being knocked out by swarming antibodies.
Another physical impediment impacting on male fertility is the not-uncommon varicocele, which is found in up to 40% of men presenting to an infertility clinic. This is a varicose vein in the scrotum which allows body temperature blood to spill backwards from the abdomen. The raised temperature in the sperm-making cells is one theory behind varicocele-related infertility but defective spermatogenesis in these cases has also been attributed to disturbed hormone status, spermatic venous hypertension, testicular congestion and hypoxia secondary to stasis, and excessive levels of oxidative species.
Surgery to correct varicoceles can often improve pregnancy outcomes, although it is not always a procedure undertaken routinely.17,18
Other obstructions in the tubes that carry the sperm can be present from before birth. Such congenital deformities can be the result of exposure to substances such as diethylstilbestrol (DES), which was taken by many pregnant women in the 1950s and 1960s to prevent miscarriage. Another congenital condition which reduces sperm count and quality is undescended testes. This is also dealt with effectively by surgery, especially if it is carried out during boyhood.
Trauma to the testicles or surgery itself can cause bruising and swelling, the effects of which may in some cases have long-term consequences on the delicate tubes. After surgery to the bladder or prostate gland, a condition sometimes develops called absent or retrograde ejaculation. This condition is also sometimes found associated with diabetes or after spinal injury. In such cases, the sperm and seminal fluid are not ejaculated at all or are ejaculated backwards into the bladder. In the latter case, sperm can be isolated from the urine and used with IVF techniques.
Diagnosis of Male Infertility in TCM
Sperm are delivered to the female genital tract in a fluid called semen. This fluid contains constituents important for sperm function and survival and for conditioning the lining of the uterus to accept an embryo containing the father’s proteins. Sperm constitutes only about 1% of the semen volume. The dynamic and fast-moving sperm represent the Yang within the moistening and nourishing Yin of the seminal fluid. When doctors of Chinese medicine are treating a sperm disorder, it is important that both the Yin and the Yang aspects are considered, i.e., both the sperm and the fluid containing them. You will see from the examples of treatments given below that both Yin and Yang are treated concurrently, with individual emphasis where necessary.
Male infertility, like female infertility, has everything to do with the Kidneys in TCM terms. As you will be aware, the Chinese medicine term ‘Kidney’ embraces more functions and areas in the body than does our concept of the kidney organs in Western medicine. Nevertheless, in Western medicine too, it is recognized that kidneys can be related to reproductive function, but this only becomes apparent when kidney function is seriously compromised. For men, renal disease has dire repercussions on fertility and sexuality.19
The basic requirement for full reproductive potential is strong Kidney Jing and a normal balance of Kidney Yin and Yang. Most cases of male infertility will be diagnosed as Kidney Yin or Yang deficiency. There appears to be a genetic base for male infertility in about 60% of cases.20 This alerts TCM doctors to the possibility that Kidney Jing weakness underlies a majority of male infertility cases and will often need to be addressed in treatment protocols alongside the usual treatments for Kidney Yin and Yang. However, where exposure to environmental pollutants in later life has caused a drop in sperm count and quality, we would not assume a Kidney Jing deficiency, although Kidney Yin and Yang function will still play a part in our treatments.
As with female infertility, the exceptions to Kidney deficiency infertility occur if there is mechanical blockage or there is a Damp-Heat condition (although these may overlay a Kidney deficiency). Thus, in the clinic we need to consider the diagnoses:
The latter two refer to particular clinical conditions and often represent complications of Kidney deficiency.
Kidney Yin Deficiency
Internal Heat is the main cause of poor sperm count in the Yin-deficient man. The slightly raised body temperature means that the sperm-producing cells do not function well and drying of fluids by the Heat means that the quantity and quality of the seminal fluid may be compromised. Internal Heat may cause inflammation of the prostate gland. As with female infertility, this is a common diagnosis of men attending infertility clinics in the West.
The diagnosis is made in the clinic by assessing all the usual sorts of symptoms and signs which indicate Yin deficiency:
In addition, there may be some Kidney symptoms such as urination frequency, dark scanty urine, poor urine flow, tinnitus, and heel pain. There may be rather a high libido but this is not necessarily accompanied by strong sexual prowess. There may also be premature ejaculation and inability to sustain erections for long.
In terms of the sperm test, it is not uncommon to see plentiful sperm but a high percentage have poor morphology and therefore less efficient motility and ability to penetrate the egg.
In the clinic, however, often the only sign to support the diagnosis of Yin-deficient infertility is a red tongue and may be the sort of hectic lifestyle which consumes Yin. The pulse may be rapid and thready, but often in fit men, it is not.
Kidney Yang Deficiency
Kidney Yang deficiency is the main and fundamental disorder of male reproduction. When Kidney Yang fails, not only are the sperm not manufactured properly but also the sexual apparatus does not function either. There will often be:
In addition, there may be other Kidney Yang-deficient signs, such as frequent copious pale urine, slight incontinence, lower back and knee pain and puffiness around the lower limbs. The salient feature of the sperm test is usually low numbers of sperm and poor motility.
Damp-Heat
Damp-Heat may accumulate in the lower Jiao generally or in the Liver/Gall Bladder channels specifically. The clinical signpost to a diagnosis of Damp-Heat infertility is an abnormal discharge from the penis or red itchy skin in the genital and groin area. There may be other signs of infection, such as painful urination or tenderness in the scrotum. Prostatitis may be the result of Damp-Heat in the lower Jiao.
As a cause of infertility, this is not so common in Western or developed countries because antibiotics are usually used promptly to address any genitourinary infections. But in China or other developing countries, low-grade untreated infections commonly contribute to the sort of inflammation which does not provide a conducive environment for sperm manufacture. In cases where there is infection in the urogenital tract, antibiotics may be appropriate and studies have shown that sperm counts can improve after such treatment.21
The nature of the antibiotic treatment is important, however, as some antibiotics may affect sperm function adversely.22
It is also the case that Damp-Heat may contribute to the development of immune infertility, even where there is no obvious infection. Men diagnosed with immune infertility (high antisperm antibody count), especially those who suffer from chronic prostatitis or local skin infections, will fall into a Damp-Heat infertility category in the TCM clinic.
If Kidney Yin or Yang deficiency is complicated with Damp-Heat then the Damp-Heat should be treated first.
Qi and Blood Stagnation
This category of male infertility includes all conditions which obstruct the passage of the sperm, abnormalities of blood circulation, and trauma (including surgery).
Some cases of Damp-Heat (such as gonorrhea) can lead to Blood and Qi stagnation infertility if inflammation in the epididymis causes the walls to stick together, creating an outright barrier to passage of the sperm.
Other obstructions in the tubes which carry the sperm were discussed above.
The varicocele, like other physical defects in the testes, may be treated surgically although this does not improve sperm production in all cases. Any abnormality in the way the blood flows is deemed to be a manifestation of ‘Blood stagnation’ and it is this underlying pathology that may need to be addressed before varicocele surgery can improve sperm counts.
As we saw above, anti-sperm antibodies often occur in men who have varicoceles and also are common in men who have had vasectomies reversed (or other sorts of testicular surgery or trauma), and men with this diagnosis and history will tend to fall into a Blood and Qi stagnation category. In some cases, there will be a history of inguinal hernia repair.23
Blood and Qi stagnation should be addressed before tonification of Kidney Yin and Yang if the stagnation is marked. In mild cases, Qi and Blood regulating herbs can be added to the base formula.
TCM Treatment of Infertility
Many reproductive specialists feel that treatment of male infertility is redundant in the brave new world of assisted reproduction wherein an embryologist can manipulate sperm with almost any sort of disability. However, while IVF with intracytoplasmic sperm injection (ICSI) offers many infertile men a chance to have a baby, it is not a panacea. Our aim should be to maximize the chance of each couple achieving a natural pregnancy while minimizing their health risks and financial costs and as such, increasing numbers of urologists who feel that the treatment of male infertility should not be ignored or sidelined.24
Additionally, the doctor of Chinese medicine is concerned with the quality of Kidney Jing the father will pass onto his offspring and will recommend that any men with a less than optimal semen analysis take the time to optimize Kidney Jing before conception attempts, whether using IVF/ICSI or not. If Jing is reflected in the integrity of the chromosomes, then one small study seems to verify that the use of Chinese herbs treating Kidney Jing and other relevant factors can reduce aneuploidy (incorrect chromosomal make-up) in sperm.25
Prescribing TCM treatment for male infertility is much simpler than prescribing treatment for female infertility. This is because once the diagnosis is made and the patient appears to tolerate the prescribed herbs, then the same formula (particularly those addressing Kidney Yin and Yang) tends to be continued for a long time, which, for a patient not receiving concurrent acupuncture treatment, reduces the number of clinic visits significantly. Remember that sperm take a long time to form (approx. 3 months) and so treatment should realistically continue for at least 6 months. Reports from China on the treatment of male infertility due to Kidney deficiency typically describe treatment protocols spanning 1 or more years.26 In China, the infertility clinics are generally dealing with a younger group of people than the infertility clinics in the West, so the long wait is more acceptable. Formulas for men to take over such a long time are often ground up and made into honey pills to make long-term consumption easier.
The other aspect of treatment of male infertility that makes it so simple compared with treatment of female infertility is that formulas can be constructed for long-term use, which address both Kidney Yin and Yang deficiency at the same time. Any formula which treats Kidney Yin or Yang over a long time must always take into consideration the other – as it is said in the classics, Yin and Yang depend on and generate each other. Thus, prescriptions like the guiding formulas shown below (which are used at a large teaching hospital in Guang Dong, China),26 can be applied to any case of low sperm count, or sperm with poor motility or poor morphology, so long as the diagnosis is Kidney deficiency.
The benefit that Chinese herbs bring to sperm quality has been the subject of a number of clinical trials in China, and include those treating autoimmune infertility.27–29
While the benefits are clearly demonstrated the mechanism remains to be elucidated. It is supposed that antioxidant activity in the herbs will contribute to improved DNA integrity and sperm manufacture but this remains to be proved. In one study, levels of the antioxidant superoxide dismutase did not change after administration of Chinese herbs, even though the sperm quality improved.30
In the case of autoimmune infertility, it appears that the herbs may influence the balance of T-lymphocyte subpopulations.31
Acupuncture treatment, like herbal treatment, is more simple for male infertility than for female infertility, in that the choice of points is not influenced by constantly changing hormone cycles. However, visits to the clinic need to be weekly or more and, if this is inconvenient, then Chinese herbs are often chosen as the preferred treatment for the long term.
Having said that, acupuncture has proven results in improving semen analyses in a number of clinical trials and hence, should be offered to any men with poor sperm quality, especially affecting morphology and motility. Many clinical trials carried out in different countries have shown that acupuncture can significantly improve sperm quality, especially motility and morphology.32–41
Most of these trials offered acupuncture over a 5–10 week period using points that addressed Kidney deficiency and mobilized Qi and Blood in local areas. The mechanism of action is not yet clear but we do know that substances in semen called met-enkephalins promote the motility of sperm42 and that acupuncture can enhance met-enkephalin levels.43 The level of met-enkephalin is abnormally low in the semen of men with poor motility of sperm but not in those with poor sperm counts. When met-enkephalin is added to the semen of healthy volunteers with normal sperm parameters in vitro, the sperm are able to maintain motility for longer than those without the added met-enkephalin. This may partially explain the observed improvement to motility after acupuncture. Thus, where motility is an issue, acupuncture may be of benefit, possibly even in the short term, e.g., applied at the time of the female partner’s ovulation.
Electroacupuncture was seen to improve testicular arterial blood flow, promising the possibility of increased delivery of nutrients, antioxidants and oxygen to the sperm-making cells.44 These researchers note that particular frequencies of electricity applied to certain acupuncture points provide a stimulus which could improve spermatogenesis by correcting metabolism in the microcirculatory bed and may address the damaged microcirculation associated with varicoceles, and with aging.
Acupuncture was also seen to improve abnormally low sperm counts and to lower elevated (>30.5°C) scrotal temperature in men with signs of genital tract inflammation.40
When planning treatment programs for patients with male factor infertility, it is useful to suggest attendance at the clinic for acupuncture at the time of their partner’s ovulation (in addition to whatever other regular treatments have been scheduled). A strongly invigorating treatment for the Kidneys can help sexual function at this time when the pressure to perform can be quite defeating. In cases of Kidney Yang deficiency, this treatment may also help to give slow sperm a bit of a hurry up! (See Tables 7.1 and 7.2 for point suggestions).
Table 7.2
Acupuncture pointsa used in the treatment of Kidney Yin deficiency male infertility
| Treatment goal | Acupuncture points |
| To treat Kidney Yin, Yang and Jingb | BL-23, KI-3, Ren-4 |
| To clear Yin-deficient Heat | KI-2 and KI-6 |
| For premature ejaculation | BL-52, DU-4, ST-27 |
| For excess libido | SP-6 |
| For spent Jing from excess sexual activity | ST-36, KI-12 |
| For excess nocturnal emissions with dreams | BL-15 and BL-43 |
| To open and regulate the Conception channel | LU-7 |
| To increase blood flow in the testiclesc | ST-29, SP-6 |
aReinforcing method is used except in the case of points used to clear Heat, where reducing or even method is used.
bCould also be useful at time of partner’s ovulation.
cUse electroacupuncture (10 Hz) joining SP-6 to ST-29 on the same side for 5–20 min.
Kidney Yin and Yang Deficiency
Herbal Formula: The formula of choice is:
Bu Shen Yi Jing Fang (Supplement the Kidneys Benefit the Jing formula)
| He Shou Wu | 15 g | Radix Polygoni Multiflori |
| Shu Di | 15 g | Radix Rehmanniae Glutinosae Conquitae |
| Gou Qi Zi | 15 g | Fructus Lycii Chinensis |
| Shan Yao | 15 g | Radix Dioscorea Oppositae |
| Shan Zhu Yu | 15 g | Fructus Corni Officinalis |
| Tu Si Zi | 15 g | Semen Cuscatae |
| Fu Pen Zi | 15 g | Fructus Rubi Chingii |
| Nu Zhen Zi | 15 g | Fructus Ligustri Lucidi |
| Bai Shao | 15 g | Radix Paeoniae Lactiflorae |
| Mu Dan Pi | 15 g | Cortex Moutan Radicis |
| Dang Shen | 15 g | Radix Codonopsis Pilulosae |
| Huang Qi | 15 g | Radix Astragali |
| Yin Yang Huo | 15 g | Herba Epimedii |
| Rou Cong Rong | 15 g | Herba Cistanches |
| Ba Ji Tian | 12 g | Radix Morindae Officinalis |
| Suo Yang | 12 g | Herba Cynomorii Songarici |
| Dan Shen | 12 g | Radix Salviae Miltiorrhizae |
| Lu Jiao Pian | 12 g | Cornu Cervi Parvum |
Using this guiding formula, herbs can be added or subtracted as required. However, because this formula broadly addresses all the factors at play in Kidney-related male infertility, it can often be prescribed as is, usually in an easy to take honey pill or powdered form. Kidney Yang function is addressed with the herbs Lu Jiao Pian, Ba Ji Tian, Rou Cong Rong, Yin Yang Huo, Tu Si Zi, Fu Pen Zi, and Suo Yang, while Kidney Yin is enriched with the herbs Nu Zhen Zi, Gou Qi Zi, Shan Zhu Yu, and Shu Di. Tonics He Shou Wu and Bai Shao nourish the Blood, He Shou Wu having a special effect on increasing semen quantity. Huang Qi, Dang Shen and Shan Yao invigorate the Qi. Mu Dan Pi regulates and cools the Blood, while Dan Shen regulates the Blood and calms the mind.
Although this excellent formula addresses both Kidney Yin and Yang if there is marked Yin deficiency Heat, then this must be addressed first or in addition. Kidney Yin will not be able to flourish in a dry or hot environment. A formula such as Zhi Bai Di Huang Wan (Eight Flavor Rehmannia pill) can be used initially or the above formula can be modified with these additions;
| Tian Dong | 15 g | Tuber Asparagi |
| Huang Bai | 12 g | Cortex Phellodendri |
| Zhi Mu | 15 g | Rhizoma Anemarrhenae |
| Han Lian Cao | 9 g | Herba Ecliptae Prostratae |
and the removal of Lu Jiao Pian, Yin Yang Huo and Suo Yang and reduction of doses of Ba Ji Tian and Rou Cong Rong.
If Yang deficiency is marked with signs of Cold, add:
| Rou Gui | 6 g | Cortex Cinnamomi Cassiae and/or |
| (Zhi) Fu Zi∗ | 6 g | Radix Aconiti Charmichaeli Praeparata |
If Yang deficiency is marked with poor erectile function, adding more Blood-regulating herbs to increase circulation to the genital organs improves function markedly.45
| Chuan Xiong | 9 g | Radix Ligustici Wallichii |
| Tao Ren | 12 g | Semen Persicae |
| San Qi | 6 g | Radix Pseudo-ginseng |
Acupuncture Points: Choose from the following points (and see Table 7.2):
| BL-23 | Shenshu |
| KI-3 | Taixi |
| Ren-4 | Guanyuan |
| KI-2 | Ranggu |
| KI-6 | Zhaohai |
| BL-52 | Zhishi |
| ST-27 | Daju |
| DU-4 | Mingmen |
| SP-6 | Sanyinjiao |
| ST-36 | Zusanli |
| KI-12 | Dahe |
| BL-15 | Xinshu |
| BL-43 | Gaohuangshu |
Choose from the following points (and see Table 7.3):
Table 7.3
Acupuncture pointsa used in the treatment of Kidney Yang deficiency male infertility
| Treatment goal | Acupuncture points |
| To treat Kidney Yin, Yang and Jingb | BL-23, KI-3, Ren-4 (use deep needling on Ren-4 with moxa), DU-4 |
| To treat Kidney Qi, Yang and Jing | Ren-6 |
| To treat Kidney Yang | GB-25 |
| To regulate genital function and sperm manufacture | BL-30 |
| To warm the lower Jiao | ST-29, Ren-8 (use moxa) |
| For leakage of sperm | KI-14 |
| For impotenceb | KI-2, KI-12, Ren-2, BL-52 |
| To increase blood flow in the testiclesc | ST-29, SP-6 |
aMoxa is applicable to all points, and reinforcing needling method.
bUseful at time of partner’s ovulation.
cUse electroacupuncture (10 Hz) joining SP-6 to ST-29 on the same side for 5–20 min.
Damp-Heat
In cases where Damp-Heat complicates Kidney deficiency, it is usually addressed first and the above formula for the Kidney deficiency is taken only when the Damp-Heat is resolved.
Herbal Formula: The representative formula to clear Damp-Heat in the lower Jiao is Bi Xie Fen Qing Yin (Dioscorea separating the Clear decoction) or, if the Damp-Heat is more specifically in the genitals, Long Dan Xie Gan Tang (Gentiana Draining the Liver decoction).
Bi Xie Fen Qing Yin (Dioscorea Separating the Clear decoction)
| Bi Xie | 12 g | Rhizoma Dioscorea |
| Yi Zhi Ren | 9 g | Fructus Alpiniae Oxyphyllae |
| Wu Yao | 9 g | Radix Linderae Strychnifoliae |
| Shi Chang Pu | 9 g | Rhizoma Acori Graminei |
Bi Xie drains Damp from the genitourinary system and Shi Chang Pu opens orifices to facilitate this draining. Yi Zhi Ren and Wu Yao warm the Bladder and Kidneys to facilitate efficient excretion of fluids.
Long Dan Xie Gan Tang (Gentiana Draining the Liver decoction)
| Long Dan Cao | 6 g | Radix Gentianae Scabrae |
| Huang Qin | 9 g | Radix Scutellariae Baicalensis |
| Zhi Zi | 9 g | Fructus Gardeniae Jasminoidis |
| Ze Xie | 9 g | Rhizoma Alismatis |
| Mu Tong | 9 g | Caulis Mutong |
| Che Qian Zi | 9 g | Semen Plantaginis |
| Sheng Di | 12 g | Radix Rehmanniae Glutinosae |
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Chai Hu | 9 g | Radix Bupleuri |
| Gan Cao | 3 g | Radix Glycyrrhizae Uralensis |
Long Dan Cao is the main herb in this formula, clearing lower Jiao Damp-Heat and Fire from the Liver channel. Huang Qin and Zhi Zi assist removal of Damp-Heat from the lower body. Chai Hu removes stagnation of Liver Qi and clears any resultant Heat. Mu Tong, Ze Xie and Che Qian Zi act as diuretics to enhance clearance of Damp. Sheng Di and Dang Gui are added to protect the Yin and the Blood and Gan Cao to protect the stomach from the bitter drying action of the above herbs.
Acupuncture Points: Choose from the following points (and see Table 7.4):
Table 7.4
Acupuncture pointsa used in the treatment of Damp-Heat male infertility
| Treatment goal | Acupuncture points |
| To strengthen Kidneys and clear Damp-Heat | Ren-4, KI-7, KI-10 |
| To treat discharge from the genitals | BL-27 and BL-28 |
| To clear Damp-Heat and treat impotence | BL-35 and Ren-1 |
| To clear Damp and gently boost Kidney Yang | DU-3 |
| To clear Damp-Heat from Liver channel and lower Jiao | LIV-8, LIV-5, GB-41, GB-27 |
| To support Damp-clearing action | SP-6 and SP-7 |
| To clear Heat, reduce general inflammation | LI-4, LI-11 |
| To increase blood flow in the testiclesb | ST-29, SP-6 |
aThese points can be used with even or reducing manipulation.
bUse electroacupuncture (10 Hz) joining SP-6 to ST-29 on the same side for 5–20 min.
| KI-7 | Fuliu |
| BL-27 | Xiaochangshu |
| BL-28 | Pangguangshu |
| BL-35 | Huiyang |
| DU-3 | Yaoyangguan |
| Ren-1 | Huiyin |
| Ren-4 | Guanyuan |
| LIV-8 | Ququan |
| LIV-5 | Ligou |
| SP-6 | Sanyinjiao |
| SP-7 | Lougu |
| KI-10 | Yingu |
| GB-27 | Wushu |
| GB-41 | Foot Linqi |
| LI-4 | Hegu |
| LI-11 | Quchi |
| ST-29 | Guilai |
Qi and Blood Stagnation
Herbal Formula: Where Qi and Blood stagnation contribute to a problem with healthy sperm production, then formulas such as Xue Fu Zhu Yu Tang or, in the case of simple Qi stagnation, Xiao Yao San (Free and Easy powder) can be used for a course of treatment before the main Kidney tonic formula is applied. For varicoceles or immune issues a formula such as Gui Zhi Fu Ling Wan can be adapted.
Xue Fu Zhu Yu Tang (Decoction for Removing Blood Stasis in the Chest)
| Dang Gui | 9 g | Radix Angelicae Sinensis |
| Sheng Di | 9 g | Radix Rehmanniae Glutinosae |
| Chi Shao | 6 g | Radix Paeoniae Rubra |
| Chuan Xiong | 6 g | Radix Ligustici Wallichi |
| Tao Ren | 12 g | Semen Persicae |
| Hong Hua | 9 g | Flos Carthami Tinctorii |
| Chai Hu | 3 g | Radix Bupleuri |
| Zhi Ke | 6 g | Fructus Citri seu Ponciri |
| Chuan Niu Xi | 9 g | Radix Cyathulae |
| Jie Geng | 6 g | Radix Platycodi Grandiflori |
| Gan Cao | 3 g | Radix Glycyrrhizae Uralensis |
Xiao Yao San (Free and Easy Powder)
| Chai Hu | 9 g | Radix Bupleuri |
| Bai Shao | 12 g | Radix Paeoniae Lactiflorae |
| Dang Gui | 9 g | Radix Angelicae Sinesis |
| Bai Zhu | 9 g | Rhizoma Atractylodis Macrocephalae |
| Fu Ling | 15 g | Sclerotium Poriae Cocos |
| Sheng Jiang | 3 g | Radix Rehmanniae Glutinosae |
| Bo He | 3 g | Herba Menthae |
| Gan Cao | 6 g | Radix Glycyrrhizae Uralensis |
Depending on the severity and nature of the stagnation (i.e. whether it is amenable to treatment with Chinese medicine), the following herbs may be added to Bu Shen Yi Jing Fang even after a course of Qi and Blood stagnation clearing herbs has been completed. For example:
| Xiang Fu | 9 g | Rhizoma Cyperi Rotundi |
| Wu Yao | 9 g | Radix Linderae Strychnifoliae |
| Tao Ren | 9 g | Semen Persicae |
| Hong Hua | 6 g | Flos Carthami Tinctorii |
Because the formula is taken for a long period of time, stronger Blood-moving herbs than these are not appropriate.
We can also add to this category more modern formulations which address immune issues.
Where there has been a diagnosis of varicocele or antisperm antibodies then using a formula which expands the actions of Gui Zhi Fu Ling Tang (shown in trials to improve sperm counts in men with varicoceles) can be used.46
Gui Zhi Fu Ling Tang (Ramulus Cinnamomi-Poria decoction) modified
| Gui Zhi | 6 g | Ramulus Cinnamomi Cassiae |
| Tao Ren | 6 g | Semen Persicae |
| Mu Dan Pi | 9 g | Cortex Moutan Radicis |
| Chi Shao | 9 g | Radix Paeoniae Rubra |
| Dan Shen | 18 g | Radix Salviae Miltiorrhizae |
| Wang Bu Liu Xing | 6 g | Semen Vaccariae |
| Che Qian Zi | 9 g | Semen Plantaginis |
| Fu Ling | 9 g | Sclerotium Poriae Cocos |
| Pu Gong Yin | 12 g | Herba Taraxaci Mongolici |
| Xiao Hui Xiang | 3 g | Fructus Foeniculi Vulgaris |
| Ju He | 3 g | Semen Citri Reticulatae |
| Chuan Lian Zi | 9 g | Fructus Meliae Toosendan |
| Xu Duan | 9 g | Radix Dipsaci |
| Huang Qi | 18 g | Radix Astragali |
To the basic therapeutic strategy of Gui Zhi Fu Ling Tang (clearing stasis and Damp), we include additional herbs to clear Qi and Blood stasis to improve circulation and to reduce inflammation. Herbs such as Wang Bu Liu Xing will help this formula target the testicles. And herbs such as Xiao Hui Xiang, Ju He, and Chuan Lian Zi are employed to specifically move the Qi in the testicles, ensuring no hindrance to the blood circulation. Dan Shen and Huang Qi are often employed in rather large doses when addressing autoimmune issues (examined further in Chapter 8).
Because inflammation is often associated with antisperm antibodies, herbs to clear Heat and Damp such as Pu Gong Yin are added.
Studies in China have found that herbal formulas which move the Blood and clear Damp-Heat while supporting Kidney Yin and Yang have a better effect on anti-sperm antibodies than does prednisone.29
Acupuncture Points: Choose from the following points (and see Table 7.5):
Table 7.5
Acupuncture pointsa used in the treatment of Qi and Blood stagnation male infertility
| Treatment goal | Acupuncture points |
| To increase circulation of Qi and Blood in the genitals | Ren-1 and Ren-2, ST-29, SP-6 |
| To encourage circulation of Blood | SP-10, PC-6 |
| To clear stagnation in lower Jiao | ST-30 and BL-31, BL-32, BL-33 |
| To move the Qi (or treat swelling or pain) in the genitals | LIV-1, LIV-4, K-11 |
| To increase blood flow in the arteries of the testiclesb | ST-29, SP-6 |
aPoints are needled with even or reducing technique.
bUse electroacupuncture (10 Hz) joining SP-6 to ST-29 on the same side for 5–20 min.
| Ren-1 | Huiyin |
| Ren-2 | Qugu |
| SP-6 | Sanyinjiao |
| SP-10 | Xuehai |
| ST-29 | Guilai |
| ST-30 | Qichong |
| BL-31 | Shangliao |
| BL-32 | Ciliao |
| BL-33 | Zhongliao |
| LIV-1 | Dadun |
| LIV-4 | Zhongfeng |
| K-11 | Henggu |
| PC-6 | Neiguan |
Also relevant are any of the points, such as those on the Liver and Kidney channels that are indicated for Shan Qi.47 Shan Qi includes disorders of the testicles which present with pain and swelling.
IVF Procedures
Aside from surgical intervention, infertility specialists in the West offer ART and IVF procedures for inadequate sperm. The onus of the ‘treatment’ falls largely on the female partner, though the handicap is not hers. Eggs collected from drug-stimulated ovaries can be fertilized in the laboratory with just a few sperm, not the millions per ejaculation required by nature. And in cases where those few sperm do not have enough motility to reach and fertilize the egg, technicians inject them into the egg using a technique called intracytoplasmic sperm injection (ICSI). In a given cycle, typically about two-thirds of the injected eggs are fertilized and about one-quarter to one-third of the women who receive these fertilized eggs will become pregnant – slightly fewer will deliver a full-term baby.
Where there are no sperm being produced at all in the ejaculate, specialists can extract sperm from the epididymis situated on top of the testis (in a procedure called microepididymal or percutaneous sperm aspiration, MESA or PESA) or in cases where there is maturation arrest, immature sperm can be extracted from testicular tissue (testicular sperm extraction or TESE). The individual sperm retrieved can then be injected into the egg using the ICSI technique. (We will discuss this further in Ch. 9.)
Diet and Lifestyle
Many aspects of diet and lifestyle are discussed in Chapter 12, but where sperm are concerned, the importance of avoiding damaging chemicals and fumes cannot be repeated too often. Sperm are extremely sensitive to the effects of chemicals in the environment and in food. In Chapter 12, we will explore environmental and dietary factors that might impact sperm quality alongside other aspects of lifestyle and behavior.
References
1. Jansen, R.P.S. Getting pregnant. Sydney: Allen and Unwin; 2003. [141].
2. Cooper, T. World Health Organization reference values for human semen characteristics. Hum Reprod Update. 2010;16(3):231–245.
3. Dindyal, S. The sperm count has been decreasing steadily for many years in Western industrialized countries: Is there an endocrine basis for this decrease? Internet J Urol. 2004;2(1):1–21.
4. Guzick, D.S., Overstreet, J.W., Factor-Litvak, P., et al. Sperm morphology, motility, and concentration in fertile and infertile men. N Engl J Med. 2001;345(19):1388–1393.
5. Badenoch, D.F., Evans, S.J., McCloskey, D.J. Sperm density measurement: should this be abandoned? Br J Urol. 1989;64(5):521–523.
6. Irvine, S., Cawood, E., Richardson, D., et al. Evidence of deteriorating semen quality in the United Kingdom: birth cohort study in 577 men in Scotland over 11 years. Br Med J. 1996;312(7029):467–471.
7. Savitz, D.A., Whelan, E.A., Kleckner, R.C. Effects of parents’ occupational exposures on risk of stillbirth, preterm delivery, and small-for-gestational-age infants. Am J Epidemiol. 1989;129(6):1201–1218.
8. Colborn, T., Myers, J.P., Dumanoski, D. Our stolen future. London: Little, Brown; 1996. [70].
9. Hauser, R., Meeker, J.D., Duty, S., et al. Altered semen quality in relation to urinary concentrations of phthalate monoester and oxidative metabolites. Epidemiology. 2006;17:682–691.
10. Wu, D.H., Leung, Y.K., Thomas, M.A., et al. Bisphenol A (BPA) confers direct genotoxicity to sperm with increased sperm DNA fragmentation. Fertil Steril. 2011;96(3):S5.
11. Colborn, T., Myers, J.P., Dumanoski, D. Our stolen future. London: Little, Brown; 1996. [81].
12. Ford, W.C.L., North, K., Taylor, H., et aland the ALSPAC study team. Increasing paternal age is associated with delayed conception in a large population of fertile couples: evidence for declining fecundity in older men. Hum Reprod. 2000;15(8):1703–1708.
13. Frattarelli, J.L., Miller, K.A., Miller, B.T., et al. Male age negatively impacts embryo development and reproductive outcome in donor oocyte assisted reproductive technology cycles. Fertil Steril. 2008;90(1):97–103.
14. Qian-Xi, Zhu, Meads, C., Lu, M.L., et al. Turning point of age for semen quality: a population-based study in Chinese men. Fertil Steril. 2011;96(3):572–576.
15. Povey, A.C., Clyma, J.A., McNamee, R. Modifiable and non-modifiable risk factors for poor semen quality: a case-referent study. Hum Reprod. 2012;27(9):2799–2806.
16. Saikhun, J., Kitiyanant, Y., Vanadurongwan, V., et al. The effect of saunas sperm movement characteristics of normal men measured by computer assisted sperm analysis. Int J Androl. 1998;21:358–363.
17. French, D., Desai, N.R., Agarwal, A., et al. Varicocele repair: does it still have a role in infertility treatment? Curr Opin Obstet Gynecol. 2008;20(3):269–274.
18. Daitch, J., Bedaiwy, M.A., Pasqualotto, E.B., et al. Varicocelectomy improves intrauterine insemination success rates in men with varicocele. J Urol. 2001;165(5):1510–1513.
19. Dinulovic, D., Radonjic, G. Diabetes mellitus/male infertility. Arch Androl. 1990;25:277–293.
20. Jansen, R.P.S. Getting pregnant. Sydney: Allen and Unwin; 2003. [140].
21. Cardoso, E.M., Santoianni, J.E., De Paulis, A.N., et al. Improvement of semen quality in infected asymptomatic infertile male after bacteriological cure. Medicina (Buenos Aires). 1998;58(2):160–164.
22. Hargreaves, C.A., Rogers, S., Hills, F., et al. Effects of co-trimoxazole, erythromycin, amoxicillin, tetracycline and chloroquine on sperm function in vitro. Hum Reprod. 1998;13(7):1878–1886.
23. Matsuda, T., Muguruma, K., Horii, Y., et al. Serum antisperm antibodies in men with vas deferens obstruction caused by childhood inguinal herniorrhaphy. Fertil Steril. 1993;59:1095–1097.
24. Alukal, J.P., Lipshultz, L.I. Why treat the male in the era of assisted reproduction? Semin Reprod Med. 2009;27(2):109–114.
25. Tempest, H.G., Homa, S.T., Zhai, X.P., et al. Significant reduction of sperm disomy in six men: effect of traditional Chinese medicine? Asian J Androl. 2005;7(4):419–425.
26. Hui, Luo Jian. Treatment of male infertility with Chinese herbs. Pacific Journal of Oriental Medicine. 1996;7:40–41.
27. De-Gui, Chang, Pei-hai, Zhang, Ahi-ping, Hu. Effect of Zengjing No.1 capsule on morphology and motility of sperm in patients with oligospermia. Chin J Integr Trad West Med. 2009;29(11):1029–1030.
28. Fu, B., Lun, X., Gong, Y. Effects of the combined therapy of acupuncture with herbal drugs on male immune infertility – a clinical report of 50 cases. J Trad Chin Med. 2005;25:186–189.
29. Lu, T.K., Ouyang, H.G., Jin, G.Y., et al. Clinical study on the treatment of male immune infertility by. Huzhangdanshenyin Zhonghua Nan Ke Xue. 2006;12(8):750–755.
30. Jin, B.F., Yang, X.Y., Bian, T.S., et al. Effects of Jujingwan on nitric oxide and superoxide dismutase in seminal plasma of asthenospermia patients. Zhonghua Nan Ke Xue. 2007;13(1):87–90.
31. Ma, H.G., Xu, J.X., Zhang, J.F., et al. The effect of Chinese medicine yiqihuoxuetang on T-lymphocyte subpopulation in peripheral blood of infertile men with antisperm antibodies. Zhonghua Nan Ke Xue. 2003;9:154–156.
32. Riegler, R., Fischl, F., Bunzel, B., et al. Correlation of psychological changes and spermiogram improvements following acupuncture (article in German). Urologe A. 1984;23(6):329–333.
33. Siterman, S., Eltes, F., Wolfson, V., et al. Effect of acupuncture on sperm parameters of males suffering from subfertility related to low sperm quality. Arch Androl. 1997;39(2):155–161.
34. Siterman, S., Eltes, F., Lederman, H., Bartoov, B. Does acupuncture treatment affect sperm density in males with very low sperm count? A pilot study. Andrologia. 2000;32(1):31–39.
35. Zhang, M., Huang, G., Lu, F., et al. Influence of acupuncture on idiopathic male infertility in assisted reproductive technology. J Huazhong Univ Sci Tech Med Sci. 2002;22(3):228–230.
36. Gurfinkel, E., Cedenho, A.P., Yamamura, Y., et al. Effects of acupuncture and moxa treatment in patients with semen abnormalities. Asian J Androl. 2003;5(4):345–348.
37. Pei, J., Strehler, E., Noss, U., et al. Quantitative evaluation of spermatozoa ultrastructure after acupuncture treatment for idiopathic male infertility. Fertil Steril. 2005;84(1):141–147.
38. Wang, Z.Q., Huang, Y.Q., Liang, B. Clinical observation on electroacupuncture and Chinese drug for treatment of oligospermia and asthenospermia of the male infertility patient. Zhongguo Zhen Jiu. 2008;28(11):805–807.
39. Siterman, S., Eltes, F., Schechter, L., et al. Success of acupuncture treatment in patients with initially low sperm output is associated with a decrease in scrotal skin temperature. Asian J Androl. 2009;11(2):200–208.
40. Dieterle, S., Li, C., Greb, R., et al. A prospective randomized placebo-controlled study of the effect of acupuncture in infertile patients with severe oligoasthenozoospermia. Fertil Steril. 2009;92(4):1340–1343.
41. Chen, A., Shen, A., Li, R., et al. Effect of acupuncture-moxibustion therapy on sperm quality in infertility patients with sperm abnormality. J Acup Tuina Sci. 2011;9(4):219–222.
42. Fujisawa, M., Kanzaki, M., Okada, H., et al. Metenkephalin in seminal plasma of infertile men. Int J Urol. 1996;3(4):297–300.
43. Bensoussan, A. The vital meridian. Melbourne: Churchill Livingstone; 1990. [112].
44. Cakmak, Y., Akpinar, I.N., Ekinci, G., et al. Point- and frequency-specific response of the testicular artery to abdominal electroacupuncture in humans. Fertil Steril. 2008;90:1732–1738.
45. Guo, J., Kong, L., Gao, X., et al. A parallel study of the effects in treatment of impotence by tonifying the Kidney with and without improving Blood circulation. J Trad Chin Med. 1999;19(2):123–125.
46. Ishikawa, H., Ohashi, M., Rayakawa, K., et al. Effects of Guizhi-Fuling-Wan on male infertility with varicocele. Am J Chin Med. 1996;24(3–4):327–331.
47. Deadman, P., Al-Khafaji, M., Baker, K. A manual of acupuncture. Hove: Journal of Chinese Medicine Publications; 1998. [655–656].