Assisted reproduction technology and in vitro fertilization
Introduction
The previous chapters of this text have examined in detail the TCM approach to infertility as it is practiced in clinics in China (and increasingly in clinics in the West). Let us now look at how assisted reproduction technology (ART), and specifically in vitro fertilization (IVF), approaches the treatment of infertility, and see where the two modalities can complement or influence each other. ART is a term used to include a variety of medical procedures used to bring eggs and sperm together without sexual intercourse. IVF is the most common and technologically sophisticated of these procedures. We shall summarize the different options offered in specialist reproductive medicine clinics below.
IVF, so controversial in the quite recent past, has rapidly gained public acceptance and its jargon has become everyday language. The IVF clinic is now frequently the first port of call for many couples who do not become pregnant as quickly as they would like. The strident voices of ethicists and feminists and moral arbiters have been all but silenced by the overwhelming momentum of this science, which has grown rapidly to meet the demands of modern population groups with dwindling fertility.
In humans, most babies are born as a result of in vivo fertilization but 1% (and rising) of all babies in the Western world are born through ART. In some countries, the rate is even higher and in Australia, where infertility patients receive significant government reimbursement, IVF is responsible for approximately 3% of all live births.1 Worldwide, IVF babies are numbered in their millions.
Social commentators have remarked that IVF could separate procreation and sex, in the way that the oral contraceptive pill separated sex and procreation in an earlier generation, a view shared by some IVF researchers who predict that in the future sex will be for fun, and IVF for procreation.2
In many countries, IVF is used more and more frequently by impatient couples who might not have significant fertility issues. One study done on nearly 1400 women between 28 and 36 with unexplained infertility, found that of those who pursued an ART solution, 53% had a baby, but so did 44% of the women who did not use ART.3
IVF Statistics
The reported success rates of assisted fertility treatment have edged upwards over the past 2 decades as new methods have been introduced and as techniques have improved. Ways of reporting success rates however, are far from standard.
Countries might report their IVF live birth rates as an overall figure, e.g., the national IVF live birth rate from all IVF cycles in Australia and NZ in 2009 was 17.2% per cycle.4
Or they may report birth rates according to the age range. For example, the national IVF live birth rate per cycle in the USA in 2009 was given as: 41.4% under age 35; 31.7% age 35–37; 22.3% ages 38–40; and 12.6% over age 41 (a significant percentage of these births were twins).5
Comparing individual IVF clinic’s success rates is not always easy because of such inconsistency in methods of reporting. Clinics understandably want their statistics to look good and have found different ways of doing this. Some clinics might include all their IVF patients in their data but will then choose just one particular period of time for analysis. One clinic, for example,6 gathered data on all the women who began IVF over a period of a few months in mid-2009, and reported that 3 years on, 65–70% of those under 38 years and 40–50% of those between 38 and 43 years, had a baby.
Other clinics might report figures for live births for only those women who have blastocysts (5-day old embryos) to transfer and give a cumulative number over a period of 2 years of attempts.7 The birth rate when presented like this was 60–80% for women under 38 years of age, and 50–60% for women 38–43 years.
I am often asked: What is the success rate in treating infertility with traditional Chinese medicine (TCM) and how does it compare to in vitro fertilization (IVF)? This is not an easy question to answer. TCM treatment for infertility is a cumulative process; it is not a discrete monthly program, the success of which can be measured per attempt or per cycle. However, now that some IVF clinics report success rates over a period of years rather than per cycle, we can think about making more meaningful comparisons. Controlled clinical trials are not common because of the difficulty in applying control conditions and statistical analysis to Chinese medicine treatment outcomes and there is a paucity of funding. One review, which presents a meta-analysis of the few trials and cohort studies that have been published, found that Chinese herbal medicine improves pregnancy rates twofold within a 4-month period compared with fertility drug treatment or IVF.8
Considering all the above, I find that more and more, the treatment options offered to couples coming to my clinic with infertility problems embrace both what Chinese medicine and ART can offer. These two medical models make interesting stable mates and so we shall spend some time examining the different paradigms at work.
The Art Clinic
First, we shall examine just what exactly happens in an ART clinic, starting from the most simple to the most complex procedures. Some clinics offer procedures such as ovulation induction, which do not involve manipulation of the eggs and sperm to achieve fertilization without sex, and these are discussed elsewhere (see Ch. 5).
Box 9.1 summarizes the different techniques offered in the reproductive medicine clinic.
Artificial insemination (AI)
Before a couple attempts IVF, some reproductive medicine clinics will suggest less intrusive techniques such as ovulation tracking or ovulation induction accompanied by artificial insemination at the appropriate time. If ovulation is absent or irregular, then there are a number of different drug regimens that can be attempted (discussed in Ch. 5). If the sperm picture is not good, but not hopeless, then washing and sorting the sperm and injecting the best of the bunch into the uterus close to the fallopian tubes at the time an egg is being released increases the chance of conception. Cycles of intrauterine insemination may or may not involve manipulation of the woman’s hormones with drugs similar to those used in an IVF cycle (but in smaller doses) depending on the clinic and the woman’s menstrual cycle history. Progress of follicle development is monitored with blood tests and ultrasounds to predict the day of ovulation. Pregnancy rates with these techniques are lower than with IVF and many patients will progress to IVF if they do not conceive after 3 or 4 rounds of AI.
In vitro fertilization (IVF)
IVF remains the most common protocol offered in an ART clinic.
The way most IVF programs proceed nowadays is explained below (summarized in Box 9.2).
Ovary stimulation
There are a few variations on the IVF theme. They are grouped into long or short cycles (summarized in Box 9.3). Except in the case of the ‘natural’ cycle, drugs are used to achieve what is a called a controlled hyper-stimulation of the ovaries.
Choice of cycle type and drugs depends on the age of the woman and what she has already tried with or without success, or on the individual preference of the IVF doctor, or sometimes on what drugs are currently available or the subject of recent studies.
The long downregulated cycle has been the most popular method for stimulating multiple egg growth in the majority of IVF clinics for the past few decades. In some clinics, this is still the case, however the short downregulated cycle is now becoming a more common and popular regimen since drugs are taken for fewer days.
Long downregulated (agonist) cycle (± ICSI)
To persuade the ovaries to produce multiple eggs, the menstrual cycle must be manipulated. In the menstrual cycle, prior to IVF being performed, the woman is given ‘downregulating’ drugs. These are gonadotrophin-releasing hormone (GnRH) agonists (called Lucrin/Lupron (Luprorelin) injection or Synarel (Nafarelin) nasal spray), which prevent the pituitary gland from producing hormones and thus interfering with the programed effects of the stimulatory drugs. (See Box 9.4 for other drug names.)
The agonist drugs cause a flare of FSH and LH as they stimulate, then inhibit the pituitary gland.
Once a period comes, and a blood test shows that the natural hormone levels are at baseline, drugs to stimulate the follicles in the ovaries can be given. These follicle-stimulating hormone (FSH) preparations (Gonal-F or Puregon or Follistim) are given by injection.
You may remember from Chapter 2 that in a normal menstrual cycle, anywhere between 1 and 30 follicles (depending on age), known as recruits, will begin to develop under the influence of FSH. However, only one (occasionally two) of these developing follicles will become dominant and release an egg in response to the FSH that a woman produces naturally.
In an IVF cycle, administration of daily injections of FSH will keep the level of this hormone constant and high, and thus encourage more of the recruits to grow and develop into large follicles containing mature eggs that can be collected surgically.
No amount of administered FSH will stimulate more follicles than are available to be recruited however. Progress is monitored by blood tests to check the levels of estrogen produced by the growing follicles and by ultrasound to measure the size of these follicles. The duration of FSH administration is also important. The normal length of the follicular phase generally needs to be made available to the growing follicles, although occasionally eggs will ripen more or less rapidly. Ideally, it is approximately 10–14 days after the stimulating drugs are started that the follicles will be large enough and the eggs mature enough to be harvested.
Short (antagonist) cycle (± ICSI)
The short cycle is so called because it involves less drug use over fewer days. Thus, the drugs used to prevent the release of eggs from ripened follicles are introduced midway into the stimulation phase, rather than some time before it. Following the same principles as described above for the long downregulated cycle, multiple eggs are stimulated to develop by daily injections of FSH and after approximately 6 days of stimulation, the antagonist drug will be added to ensure that none of these follicles release their eggs.
Like the agonists, the GnRH antagonists are also used to stop the hypothalamus stimulating the pituitary to produce FSH and LH but they do it without first causing the flare of LH, meaning they can be used for a much shorter period of time.
The shorter time of drug administration and the need for fewer injections has meant that this type of IVF cycle has increased in popularity in most clinics. Long-acting FSH preparations, called Elonva (corifollitropin alfa) are the next step in markedly reducing numbers of injections.
Short (agonist) cycle (± ICSI)
This variation of the long ‘downregulating’ protocol is sometimes called a flare cycle. It is less commonly used than the above described cycles.
In the flare cycle, the GnRH agonist is administered from the start of the period (and the FSH begins the next day), and is continued up until the eggs are mature, to suppress ovulation. This is enough time to get past the initial LH surge that agonist causes. The supposed benefit of such an approach is that the agonist will also cause a surge of FSH from the pituitary, which augments the administered dosage of FSH, thereby synergizing the growth of ovarian follicles. But the LH surge at the beginning is not thought to be so good for older women (who might already have elevated LH), possibly spoiling optimal development of ovarian follicles.
The short cycles (antagonist or agonist) offer the opportunity to test the natural levels of the FSH produced by the pituitary before proceeding. Some clinics like to assess ovarian responsiveness with a blood test taken on the 1st day of the cycle. A low FSH (<10 IU/L) indicates that the ovarian reserve is adequate and that the follicles will likely be responsive to the drugs.
A high FSH level indicates poor ovarian response, in which case the patient may be recommended to wait for another month.
‘Natural’ cycle with no suppression
Sometimes, there are clinical situations where it is advantageous to use no drugs. Of course because few eggs are collected the advantage usually conferred by IVF (that of more chance of creating a good embryo because of more eggs) is lost. This approach may be chosen when there has been repeated failure to respond to the usual drug regimens or the patient has some intolerance to the drugs, particularly the suppressing drugs. In a ‘natural’ cycle, young women are given no drugs, while older women may be given FSH injections but no suppressing drugs will be employed. Careful tracking is needed and when the lead follicle is nearing maturity, the trigger injection is given and egg collection is scheduled for 34 h later (rather than the usual 36 h for regular IVF, just to be sure to catch the egg before it ovulates). This approach, although rare, is sometimes considered with premature menopause patients who have naturally high levels of circulating FSH.
Egg collection, oocyte pick-up (OPU)
Once ultrasounds indicate that there is a cohort of follicles all approaching an ideal 20 mm in size, a trigger injection of human chorionic gonadotrophin, hCG, which in these circumstances acts like the luteinizing hormone (LH) that provokes ovulation, is given to mature the eggs and prepare the follicles to release them. (Occasionally if there has been a history of ovarian hyperstimulation syndrome (see below), then a dose of an agonist such as Synarel will be used to supply the LH surge. But before they escape (close to 36 h after the trigger), a needle guided by the surgeon’s hand will penetrate each follicle and gently extract it via the vagina. This is called oocyte pick-up or retrieval. In an ideal case, there will be plenty of eggs collected (5–10, sometimes more). The number varies and depends on some known factors such as age, and on some as yet unknown factors. The sperm (freshly donated in a private room often furnished with whisky and glossy 2D sex goddesses) are washed and sorted. Eggs meet sperm in a specially formulated medium in a Petri dish and (what’s left of) nature takes its course – or not.
Once an egg is successfully penetrated by a sperm, an extraordinary and complex series of events takes place. The chromosomes of the egg and the chromosomes of the sperm line up, and if the fit is good a new potential life begins.
However, sometimes this stage needs a little bit of help from the embryologist.
Intracytoplasmic sperm injection
Intracytoplasmic sperm injection (ICSI) may be performed as part of either the long or the short protocols. This technique involves the injection of a sperm directly into the cytoplasm of a harvested egg using a very fine needle. ICSI is usually performed where the sperm are unable to fertilize the egg under their own steam, e.g., if the sperm count is very low, or the sperm are not very motile, or are affected by antibodies. It is a technique that can sometimes be used to help men whose semen contains no sperm, because of a congenital or infective blockage or after vasectomy (the sperm may be collected from further up the reproductive tract). Before ICSI, at best 5% of infertile men could be treated; with it, the potential for infertile men to father children has increased many fold. With ICSI, any man who produces sperm, even if the sperm are never ejaculated, or if the sperm-making cells in the testes are defective, or even if the sperm die before they get anywhere, can potentially become a father. The method has been so successful that some IVF clinics do not even bother with normal fertilization, but simply inject sperm into the egg, hoping for higher fertilization rates.
Some additional fine tuning can be added to the ICSI procedure. This includes choosing a sperm from those that bind to a substance called hyaluron (referred to as PICSI), since only mature and structurally sound sperm will bind to this substance. Some clinics are using very high magnification of sperm (7000 instead of 400 times), particularly when there is a finding of high DNA fragmentation, to improve choice of the best sperm for ICSI. This is sometimes referred to as MICSI.
It is now accepted (by many IVF doctors) that with the advent of ICSI, male infertility should be no impediment at all to conception. Some andrologists (and Chinese medicine practitioners and naturopaths), however, feel that the health and vitality of the sperm is something that can and should be addressed rather than circumnavigated. While most of the focus has been on the age and quality of the egg, there is also evidence that the age and quality of the sperm influences not only fertility but also the integrity of the embryo (see Ch. 7).
Once fertilization occurs successfully and an embryo forms, it will be incubated in carefully controlled conditions and if after 3–5 days the embryo is still alive and dividing, it is ready to be transferred back to the womb where it belongs.
Preimplantation genetic diagnosis
In the case of known inherited genetic disorders in the couple or their family, one last procedure remains before the embryo is transferred.
Some cells are removed from the embryo and are analyzed for chromosomal disorders. This technique, called preimplantation genetic diagnosis (PGD) can diagnose hundreds of different genetic disorders. Only those embryos that pass the screening will be available for transfer or freezing. PGD, which can now analyze all the chromosomes of an embryonic cell, is sometimes advised for older women who are at higher risk of having chromosomal abnormalities in their embryos or women who have had previous chromosomal abnormality in a pregnancy or repeated implantation failure or repeated pregnancy losses.
Embryo transfer
A fine plastic catheter that has been loaded with the chosen embryo/s, is passed through the cervix into the uterus. The deposited embryo is held snuggly by the front and back walls of the uterus. It cannot fall out.
Embryos will sometimes be transferred at 3 days of age, particularly if there are not so many of them. But in the case where there are several embryos to choose from, allowing them to grow longer permits the embryologist to see which embryos are the fittest (Fig. 9.1).
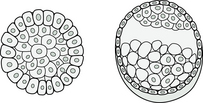
At the Morula stage, when the embryo is between 8–64 cells, it is not always easy to identify embryos with appropriate development potential. Approximately 40% of the embryos that look good on Day 3 will fail to progress to Day 5.
Embryos are able to develop to Day 3 using the maternal genomic drive. The embryo’s genome (which is made up of both maternal and paternal genetic material) is not activated until after 3 days and if there is a chromosome problem in the embryo, then its development may slow down or stop at this point. Also, if the embryo lacks the necessary ability to make energy, it will have difficulty continuing to divide and create new cells.
At 5 days, the embryo is called a blastocyst and has a greater chance of survival after transfer than do younger embryos. Usually, one blastocyst is transferred through the cervix to the uterus (called blastocyst transfer or BT); any more and the risk of multiple pregnancy is too great. Some IVF clinics will try to increase their pregnancy statistics by transferring larger numbers, but doing so can seriously compromise the health of resulting pregnancies and babies if there are multiple conceptions.
Frozen embryo or cryoblastocyst transfer
When a number of oocytes are collected and successfully fertilized as part of a stimulated IVF cycle, the number of embryos produced may be well in excess of what can be transferred at the time. Those embryos not transferred back to the uterus can be frozen for future use when they will be defrosted a few hours before a carefully timed transfer to an early luteal phase uterus. In a frozen embryo transfer cycle there may be some drug manipulation of the woman’s hormonal status, as in an IVF cycle, but less so. Estrogen may be prescribed to ensure the uterine lining thickens and, after the transfer, progesterone is given. But often there is a ‘natural’ cycle transfer, wherein no drugs are given but ovulation is tracked to correctly time the transfer. Some clinics find they get a higher pregnancy rate with fresh embryo transfers but studies have also found that pregnancies from frozen embryos have reduced miscarriage and complication rates,9 and that frozen embryo cycles are better for endometriosis patients.10
Implantation
The success of the next stage, implantation, depends on the environment inside the uterus, the uterine lining and most importantly, on the embryo itself. If the embryo is strong and has its genetic programing up and running well, it will very likely succeed in implanting and continue to develop. As you may remember from Chapter 8, a majority of embryos do not have what it takes to go the long haul from egg and sperm chromosome line up to a fully viable pregnancy, because there is plenty of opportunity for chromosomal blunders in this completely new genetic blueprint. Current ART knowledge does not allow for predicting the genetic viability of a particular embryo by its appearance or the vigorousness of its cell division, so after transfer it becomes a nerve-wracking case of wait-and-see with fingers crossed.
Despite the fact there may be several of them, the corpus lutei, which are needed to provide progesterone for the next stage do not function. The use of the downregulating drugs prevents the production of LH which is needed to stimulate the corpus luteum. That plus the fact that when the eggs are aspirated from the follicles at OPU some of the cells which are needed to form the corpus luteum are also removed which means that the corpus lutei, will need some additional help from an external source of progesterone. Thus progesterone injections, pessaries or gel may be given at this stage, or two or three injections of hCG (which has a structure very similar to LH) may be given to boost corpus luteum function.
Ovarian hyperstimulation syndrome
Ovarian hyperstimulation syndrome (OHSS) is an iatrogenic complication of IVF, the pathogenesis of which is poorly understood. It occurs in the days following the injection of hCG given to trigger final egg maturation and preparation for collection and is exacerbated by further hCG injections given in the luteal phase or by pregnancy. Mild hyperstimulation occurs in up to 25% of IVF patients and moderate to severe in up to 5%.
The main symptoms are ovarian enlargement, ascites (caused by leakage of fluid from follicles, increased capillary permeability or rupture of follicles), and hypovolemia (decreased blood volume that can increase risk of thrombosis). In severe cases, the blood flow to the kidneys is reduced and urine output falls dramatically or ceases altogether. In very severe cases, there is leakage of fluid into the chest cavity, giving rise to shortness of breath.
Enlargement of the ovaries can cause abdominal pain, nausea, and vomiting. Increased intra-abdominal pressure due to extra fluid accumulating in the abdominal space causes distenion, discomfort and pain. Blood from ruptured cysts, protein-rich fluid, and inflammatory mediators can all cause peritoneal irritation contributing to abdominal pain. If the pain is very acute it may indicate ovarian torsion, rupture of cysts, or hemorrhage.
There are some warning signs that might occur during the medication phase of the IVF cycle (especially in women of young age, those with low body weight, or with polycystic ovarian syndrome, or those who have had previous episodes of hyperstimulation).
• A large number, i.e., 15–30, of intermediate sized follicles (10–14 mm)
• High estrogen levels; some women experience OHSS at E2 levels of 2000–5000 pg/mL but levels can rise to 40 000 pg/mL in extreme cases
• Early symptoms (e.g., abdominal bloating and discomfort, mild nausea, weight gain, edema, lethargy and diarrhea prior to OPU).
If OHSS is pronounced, then the embryo transfer will be delayed for a future date and any embryos will be frozen awaiting that future opportunity.
Some clinics will use a different trigger if there is a clear risk of OHSS. Lucrin or Lupron can be used instead of hCG to provide a surge of LH which prepares the oocytes for collection in women on short antagonist IVF cycles. Since the surge is short lived, hyperstimulation is less likely. Extra luteal support in the form of estrogen and progesterone will be added in these cases.
References
1. Australian Bureau of Statistics. Catalogue no. 3301.0. Sydney: ABS; 2007.
2. Vajta, G., Rienzi, L., Cobo, A., et al. Embryo culture: can we perform better than nature? Reproductive BioMedicine Online. 2010;20(4):453–469.
3. Herbert, D.L., Lucke, J.C., Dobson, A.J. Birth outcomes after spontaneous or assisted conception among infertile Australian women aged 28 to 36 years: a prospective, population-based study. Fertil Steril. 2012;97(3):630–638.
4. Australian Institute of Health and Welfare, Assisted reproductive technology in Australia and New Zealand, 2009, http://www.aihw.gov.au/publication-detail/?id=10737420465&tab=2.
5. Society for Assisted Reproductive Technology. IVF success rate reports. http://www.sart.org/.
6. Genea, IVF success rates, 2012, http://www.genea.com.au/How-we-can-help/Our-Success/IVF-Success-Rates/Genea-IVF-Success-Rates.
7. IVF Australia, IVF Australia success rates, 2012, http://www.ivf.com.au/ivf-success-rates.aspx.
8. Ried, K., Stuart, K. Efficacy of traditional Chinese herbal medicine in the management of female infertility: A systematic review. Complement Ther Med. 2011;19(6):319–331.
9. Kalra, S., Ratcliffe, S.J., Milman, L., et al. Perinatal morbidity after in vitro fertilization is lower with frozen embryo transfer. Fertil Steril. 2011;95(2):548–553.
10. Mohamed, A.M., Chouliaras, S., Jones, C.J., et al. Live birth rate in fresh and frozen embryo transfer cycles in women with endometriosis. Eur J Obstet Gynecol Reprod Biol. 2011;156(2):177–180.