Reticular Formation, Electrical Activity of the Brain, and Alert Behaviour and Sleep
 Evoked cortical potentials
Evoked cortical potentials Non-REM
Non-REMReticular formation and reticular activating system
Reticular formation (RF) refers to the complex network of neurons and nerve fibres, which occupy midventral portion of brain stem around the central cavity. The brain stem RF can be considered to comprise medullary RF, pontine RF and midbrain RF. Structurally, brain stem reticular formation consists of:
Reticular activating system
Reticular activating system (RAS), also known as ascending reticular activating system (ARAS), is a complex polysynaptic pathway that projects diffusely from the brain stem reticular formation to the cerebral cortex.
Collaterals to RAS funnel from the following sources (Fig. 10.8-1):
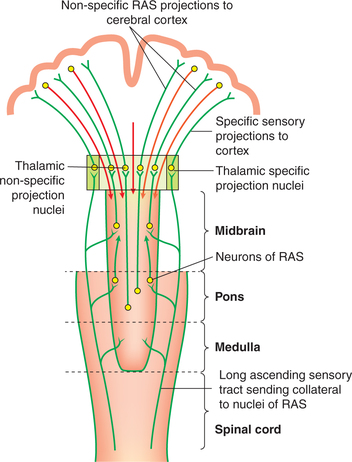
Fig. 10.8-1 Diagrammatic depiction of reticular activating system vis-a-vis specific sensory projections.
• Long ascending sensory pathways, such as spinothalamic tracts, are the important sources of collaterals to RAS. The fibres of the tracts conveying slow pain send the richest collateral connections to the RAS.
• In addition to long ascending sensory tracts, collateral to the RAS also funnel from the trigeminal, auditory, visual and olfactory pathway systems.
Efferent projections from RAS are:
• Majority of RAS fibres end in non-specific thalamic nuclei (intralaminar and midline nuclei), and from there projected diffusely and non-specifically to the whole neocortex (Fig. 10.8-1).
• Another part of RAS bypasses the thalamus to project diffusely to the cortex.
The RAS fibres occupy the core portion of the brain stem (Fig. 10.8-1), whereas the specific fibres occupy rather the lateral parts of brain stem.
Stimulation of RAS. The RAS is stimulated by impulses funneled into it through the collateral described above. Thus, the RAS is a non-specific system, which can be excited by any sensation.
Functions of reticular formation
1. Sleep-wakefulness. The RAS of reticular formation is the neural substrate of the consciousness.
• RAS sends a strong facilitatory drive to the central neurons, raising their background excitability and increasing their responsiveness to specific stimuli. Thus, when RAS is stimulated, there is wakefulness and alertness of the subject and the subject becomes fully conscious. This alertness is necessary even for proper sense perception. Conversely, when the RAS is inhibited, the subject is asleep.
• Lesions of RAS in experimental animals produce interminable sleep and coma. In human beings also, lesions in the RAS (e.g. tumours) cause prolonged sleep.
• Many agents producing sedation, hypnosis and anaesthesia (e.g. benzodiazepine and barbiturates) act by preventing synaptic transmission in RAS, and thus inhibiting the RAS.
2. Selective attention and sensory inattention. The reticular formation is also responsible for selective attention and sensory inattention through the corticofugal control of sensory input and due to habituation.
3. Conditioning and learning. Reticular formation is an integral part of the neural substrate for conditioning and learning (for details see page 559).
4. Control of muscle tone and regulation of postural reflex changes. Reticular formation modulates the tone of extensor (antigravity) muscles (for details see page 525).
5. Autonomic functions. The visceral regulating centres are an integral part of the reticular formation. The influence of higher neurons over the viscera and autonomic functions are mediated through the visceral centres in reticular formation.
6. Modulation of pain. By affecting the transmission of pain impulses through the substantia gelatinosa of the spinal cord, the serotonergic neurons modulate the perception of pain (for details see page 509).
7. Control of neuroendocrine system. The reticular formation projections play a role in the control of neuroendocrine systems in the hypothalamus.
Electrical activity of the brain
Evoked cortical potentials
Evoked potential refers to the surface electrical activity recorded from the surface of the scalp in response to a specific and adequate stimulus—auditory, visual or somatosensory. Stimulation by a specific adequate stimulus produces two types of electrical activity in the cerebral cortex known as primary evoked potential and diffuse secondary response.
Primary evoked potential. This is the initial, brief (lasting for few milliseconds) and localized response over the specific sensory cortex. The primary evoked potential is characterized by (Fig. 10.8-2):
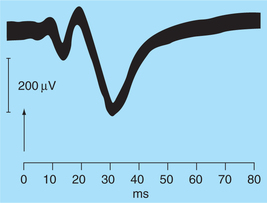
Fig. 10.8-2 Response evoked in contralateral sensory cortex by stimulation of sciatic nerve in a cat. The upward deflection is surface negative.
• Latency of about 5–12 ms (average 10 ms).
• First there appears a surface positive wave which is followed by a small negative wave.
• The primary evoked potential is highly specific in its location and can be observed only where the pathway from a particular sensory organ ends; that is, it is produced by the conduction of sensory signals through the specific sensory pathways.
Diffuse secondary response is characterized by:
• Latency of about 20–80 ms (average 50 ms), i.e. it appears about 50 ms of sensory stimulus.
• Positive–negative wave sequence of secondary diffuse response is frequently larger and more prolonged than the positive–negative wave sequence of primary evoked potential.
• The surface-positive diffuse secondary response unlike the primary is not highly localized. It can be recorded at the same time from most of the cerebral cortex. It is due to spread of impulses through the RAS to the cerebral cortex.
Electroencephalogram
The term electroencephalogram (EEG) (introduced by the German psychiatrist Hans Berger) refers to the record of spontaneous electrical activity of the brain taken from the surface of scalp (c.f. evoked potential which is the surface electrical activity recorded in response to a specific and adequate stimulus). The spontaneous electrical activity of the brain is largely due to graded or summated postsynaptic potentials in the many hundreds or thousands of brain neurons that underlie the recording electrode at the surface of scalp.
Normal electroencephalogram
The EEG consists of waves which are oscillations in the electrical potential of brain having following characteristics:
• The oscillations differ in the frequency and amplitude at different points on the scalp and during different stages of mental alertness.
• Different waves recorded in a normal person, depending on their frequency, are classified as alpha, beta, theta and delta (α, β, θ, δ) waves (Table 10.8-1, Fig. 10.8-3).
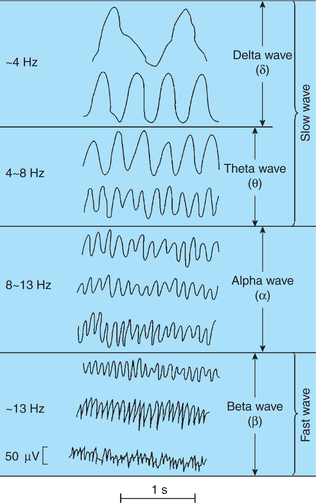
Waves of EEG (Fig. 10.8-3)
These are the most prominent component of EEG obtained from adult humans who are awake but quiet and at rest with the eyes closed. α-waves are said to result from spontaneous activity of non-specific thalamocortical system.
Characteristic features of α waves are:
• Frequency of α-waves varies from 8 to 13 Hz. The mean peak frequency in a large number of normal adults is 4.2 Hz.
• Amplitude of these waves slowly waxes and wanes, but the average amplitude is about 50 μV.
• Location. α-waves are most marked in the parietooccipital area of the scalp, though these are observed sometimes from other locations as well.
Alpha block or alpha attenuation refers to a phenomenon in which α-wave attenuates and are replaced by the fast, irregular waves of low amplitude. Alpha block occurs when:
• The persons open their eyes,
• When the individuals engage in conscious mental activity, such as doing mathematical calculations and
• When any form of stimulation is applied (Fig. 10.8-4).

The term aroused or alerting response is also used to denote α-block, since it is correlated with arousal or alerting response.
Delta (δ) waves do not occur in normal waking individuals. These are seen in following conditions:
Characteristic features (Fig. 10.8-4) are:
Abnormal eeg waveforms
1 Epilepsy
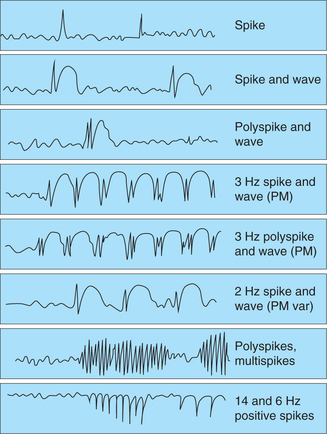
Electroencephalographic inspection is indispensable to the diagnosis of epilepsy. The waveforms of epilepsy (Fig. 10.8-5) include idiopathic abnormal waves, such as a spike, sharp wave and spike and slow wave complex.
2 Organic brain dysfunction
An abnormal wave appears when in brain functional trouble occurs due to cerebral tumour, brain blood vessel trouble (bleeding, clogging, artery/vein leakage, hardened brain artery, etc.) or brain injury caused by an external wound of the head.
3 Brain death
Criteria for labelling brain death is important because of the desire to obtain organs for transplant operations and the desire to remove heroic life-support system. Individual is declared dead when brain cells stop activity, the EEG waveform becomes flat in all channels and finally disappears.
Wakefulness and sleep
Wakefulness
The RAS of the reticular formation is the neural substrate of the consciousness and sleep–waking cycle. As described earlier, RAS is a complex polysynaptic pathway that projects diffusely from the brain stem reticular formation to the cerebral cortex both directly as well as via thalamus (for details see page 482).
Neural substrate for wakefulness
The neural substrate of wakefulness generating systems are:
1. Reticular activating system, as discussed above, is mainly responsible for the tonic maintenance of the cortical activation and behavioural arousal of the wakefulness.
2. Thalamus. The non-specific thalamic system is involved in the activation of entire cerebral cortex. These nuclei get tonic drive from the reticular formation, and in turn project diffusely to the cerebral cortex.
3. Hypothalamus and subthalamus. The posterior hypothalamus also acts as waking centre, as its stimulation causes wakefulness. Conversely, lesions of posterior hypothalamus result in coma.
Sleep
Sleep refers to a state of unconsciousness from which the individual can be aroused by sensory or other stimuli. When asleep, an individual is not aware of the environment and is unable to perform activities that require consciousness.
Sleep–wake cycle and factors affecting sleep
Sleep and wakefulness, like many of the body's regulatory mechanisms, have circadian rhythm of about 24 h. In a normal adult, the sleep–wake cycle consists of 7–8 h of sleep and 16–17 h of wakefulness. A newborn infant has many cycles of sleep and wakefulness in 24 h, but after the age of 2 years a single sleep–wake cycle is established.
The factors which favour the onset of natural sleep are:
• Comfortable surrounding temperature,
• Physical and mental relaxation,
• Consumption of a basic urge, such as hunger or sex and
• Low-frequency stimulation, such as by patting or knocking in a cradle or sitting in a moving vehicle.
The above-described factors have only a modest effect if any. The only behavioural factor that reliably and substantially increases sleep is prior sleeplessness. On the other hand, anxiety and emotional stimuli by release of epinephrine cause activation of RAS and make sleep more difficult.
Types and stages of sleep
Sleep is of two types: non-REM sleep and REM sleep, which alternate in a sleep cycle.
Non-REM sleep
Non-REM sleep, i.e. non-rapid eye movement sleep, is also known as slow wave sleep (SWS) because in this type of sleep brain waves are very slow.
In normal adults, sleep mostly begins with non-REM sleep. It is rest type of sleep which a person experiences during first hour of sleep after having been kept awake for many hours.
Stages and EEG patterns of non-REM sleep
State of quiet, awake rest with eyes closed. State of quiet, awake rest with eyes closed is the period in between the stage of wakefulness and stage of sleep characterized by α-waves, which are highly synchronized.
State of non-REM sleep. When an individual from the state of quiet rest with eyes closed enters the state of non-REM sleep, the consciousness is reduced. The non-REM sleep progresses in an orderly way from light to deep sleep in four stages.
Physiological changes during non-REM sleep
• Muscle tone decreases progressively.
• Heart rate and blood pressure are decreased.
• Respiration rate is also decreased.
• Eyes begin slow, rolling movement until they finally stop in stage 4 (deep sleep) with eyes turned upwards.
• Pituitary shows pulsatile release of growth hormone and gonadotropin.
REM sleep
REM sleep, i.e. ‘rapid eye movement’ sleep is also called ‘fast wave (desynchronized) sleep’ or ‘paradoxical sleep’ or ‘dream sleep’ or ‘deepest sleep’ (as explained below). In adults, the REM sleep follows non-REM sleep.
During REM sleep, EEG is characterized by a highfrequency and low-amplitude pattern (β-rhythm), i.e. some desynchronized pattern that is seen in the waking state. Because of EEG pattern of wakefulness, the REM is also called ‘paradoxical sleep’.
Dreaming occurs during REM sleep, so it is also called ‘dream sleep’.
Physiological changes during REM sleep
• Rapid eye movements are the hallmark of this state of sleep and that is why the name REM sleep. Rapid eye movements (saccadic eye movements) are bursts of small jerky movements that bring the eye from one fixation point to another to allow a sweeping of visual images of dreams.
• Heart rate and respiration rate become irregular.
• Penile erection in males and engorgement of clitoris in females may occur during REM sleep.
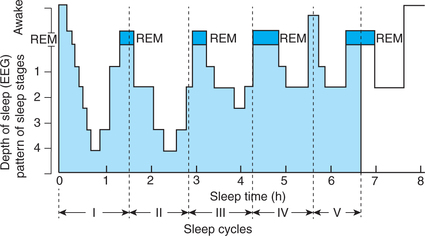
Sleep cycle
In a normal adult individual, the average sleep period of about 7–8 h is divided into about five cycles during which non-REM sleep and REM sleep alternate with each other. There is an orderly progression of sleep states and stages during a typical sleep cycle (Fig. 10.8-6).