The haematological examination
Haematological assessment does not depend only on the microscopic examination of the blood constituents. Physical signs, followed by examination of the blood film, can give vital clues about underlying disease. Haematological disease can affect the red blood cells (RBCs), the white cells (WBCs), the platelets and other haemostatic mechanisms, as well as the mononuclear-phagocyte (reticuloendothelial) system.
Examination anatomy
An important part of the examination involves assessment of all the palpable groups of lymph nodes. As each group is examined its usual drainage area must be kept in mind (see Figure 21.1). It follows that whenever an abnormality is discovered anywhere that might be due to infection or malignancy its draining lymph nodes must be examined. A decision about the size of the spleen is one of the most important aspects of the haematological examination. The normal spleen lies almost completely under the ribs and is not palpable. An enlarging spleen cannot displace the spine, kidney (it is retro-peritoneal) or the diaphragm and so displaces the stomach. Its anterior pole follows a course in line with the bony part of the tenth rib and as it descends below the rib cage moves across the abdomen towards the right iliac fossa.
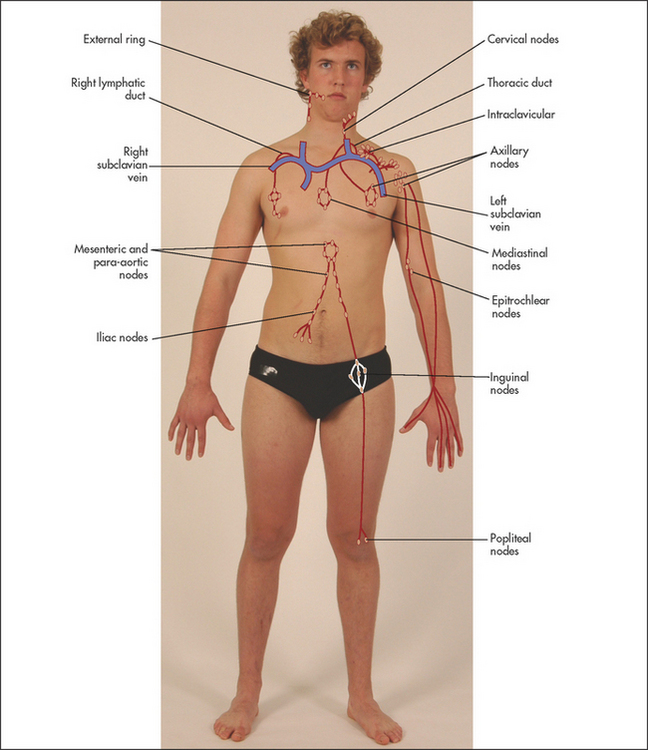
Figure 21.1 Usual drainage areas of lymph nodes (Adapted from Epstein O et al. Clinical examination, 4th edn. Edinburgh: Mosby, 2008.)
Ludwig Traube described a space defined superiorly by the sixth rib, laterally by the mid-axillary line and inferiorly by the left costal margin that is normally resonant to percussion. He noted that it became dull in the presence of a pleural effusion but did not realise that enlargement of the spleen also caused disappearance of this resonance (page 277).
General appearance
Position the patient as for the gastrointestinal examination—lying on the bed with one pillow. Look for signs of wasting and for pallor (which may be an indication of anaemia).1–3 Note the patient’s racial origin (e.g. thalassaemia). If there is any bruising, look at its distribution and extent. Jaundice may be present and can indicate haemolytic anaemia. Scratch marks (following pruritus, which sometimes occurs with lymphoma and myeloproliferative disease) should be noted.
Hands
The detailed examination begins in the usual way with assessment of the hands. Look at the nails for koilonychia—these are dry, brittle, ridged, spoon-shaped nails, which are rarely seen today. They can be due to severe iron deficiency anaemia, although the mechanism is unknown. Occasionally koilonychia may be due to fungal infection. They may also be seen in Raynaud’s phenomenon (see Figure 21.2). Digital infarction (see Figure 21.3) may be a sign of abnormal globulins (e.g. cryoglobulinaemia). Pallor of the nail beds may occur in anaemia but is an unreliable sign. Pallor of the palmar creases suggests that the haemoglobin level is less than 70 g/L, but this is also a rather unreliable sign.1


Note any changes of rheumatoid or gouty arthritis, or connective tissue disease (see Chapter 25). Rheumatoid arthritis, when associated with splenomegaly and neutropenia, is called Felty’s syndromea: the mechanism of the neutropenia is unknown, but it can result in severe infection. Felty’s syndrome may also be associated with thrombocytopenia (see Figure 21.4), haemolytic anaemia, skin pigmentation and leg ulceration. Gouty tophi and arthropathy may be present in the hands. Gout may be a manifestation of a myeloproliferative disease. Connective tissue diseases can cause anaemia because of the associated chronic inflammation.

Now take the patient’s pulse. A tachycardia may be present. Anaemic patients have an increased cardiac output and compensating tachycardia because of the reduced oxygen-carrying capacity of their blood.
Look for purpura (see Figure 21.4), which is really any sort of bruising, due to haemorrhage into the skin. The lesions can vary in size from pinheads called petechiae (from Latin petechia ‘a spot’; see List 21.1) to large bruises called ecchymoses (see Figure 21.5 and List 20.3 on page 269).

If the petechiae are raised (palpable purpura), this suggests an underlying systemic vasculitis, where the lesions are painful, or bacteraemia.
Epitrochlear nodes
The epitrochlear nodes must always be palpated. The best method is to flex the patient’s elbow to 90°, abduct the upper arm a little and place the palm of your right hand under the patient’s right elbow (see Figure 21.6). Your thumb can then be placed over the appropriate area, which is proximal and slightly anterior to the medial epicondyle. This is repeated with the left hand for the other side. An enlarged epitrochlear node is usually pathological. It occurs with local infection, non-Hodgkin’s lymphomad or, rarely, syphilis. Note the features and different causes as outlined in Lists 21.2 and 21.3. Certain symptoms and signs suggest that lymphadenopathy may be the result of a significant disease (see Good signs guide 21.1).

Axillary nodes
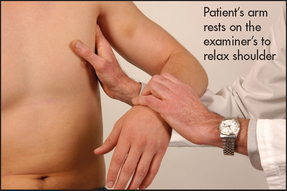
To palpate these, raise the patient’s arm and, using your left hand for the right side, push your fingers as high as possible into the axilla. Then bring the patient’s arm down to rest on your forearm. The opposite is done for the other side (see Figures 21.7 and 21.8).

Figure 21.7 Enlarged axillary nodes (Courtesy of Dr A Watson, Infectious Diseases Department, The Canberra Hospital)
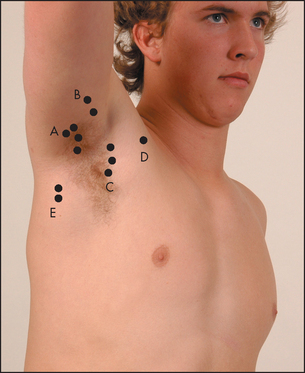
There are five main groups of axillary nodes: (1) central; (2) lateral (above and lateral); (3) pectoral (medial); (4) infraclavicular; and (5) subscapular (most inferior; see Figure 21.9). An effort should be made to feel for nodes in each of these areas of the axilla.
Face
The patient’s eyes should be examined for the presence of scleral jaundice, haemorrhage or injection (due to increased prominence of scleral blood vessels, as in polycythaemia; see Figure 21.10). Conjunctival pallor suggests anaemia and is more reliable than examination of the nail beds or palmar creases.3 In northern Europeans the combination of prematurely grey hair and blue eyes may indicate a predisposition to the autoimmune disease pernicious anaemia, where there is a vitamin B12 deficiency due to lack of intrinsic factor secretion by an atrophic gastric mucosa.
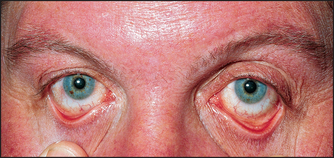
Figure 21.10 Polycythaemia rubra vera—prominent scleral blood vessels (From Marx J et al. Rosen’s emergency medicine. Mosby, 2009.)
The mouth should be examined for hypertrophy of the gums, which may occur with infiltration by leukaemic cells, especially in acute monocytic leukaemia, or with swelling in scurvy. Gum bleeding must also be looked for, and ulceration, infection and haemorrhage of the buccal and pharyngeal mucosa noted. Atrophic glossitis occurs with megaloblastic anaemia or iron deficiency anaemia. Multiple telangiectasias may appear around or in the mouth of patients with hereditary haemorrhagic telangiectasia. Look to see whether the tonsils are enlarged. Waldeyer’s ringe is a circle of lymphatic tissue in the posterior part of the oropharynx and nasopharynx, and includes the tonsils and adenoids. Sometimes non-Hodgkin’s lymphoma will involve Waldeyer’s tonsillar ring, but Hodgkin’s disease rarely does.
Cervical and supraclavicular nodes
Sit the patient up and examine the cervical nodes from behind. There are eight groups. Attempt to identify each of the groups of nodes with your fingers (see Figure 21.11). First palpate the submental node, which lies directly under the chin, and then the submandibular nodes, which are below the angle of the jaw. Next palpate the jugular chain, which lies anterior to the sternomastoid muscle, and then the posterior triangle nodes, which are posterior to the sternomastoid muscle. Palpate the occipital region for occipital nodes and then move to the postauricular node behind the ear and the preauricular node in front of the ear. Finally from the front, with the patient’s shoulders slightly shrugged, feel in the supraclavicular fossa and at the base of the sternomastoid muscle for the supraclavicular nodes. Causes of lymphadenopathy, localised and generalised, are given in List 21.4. Note that small cervical nodes are often palpable in healthy young people.4,5
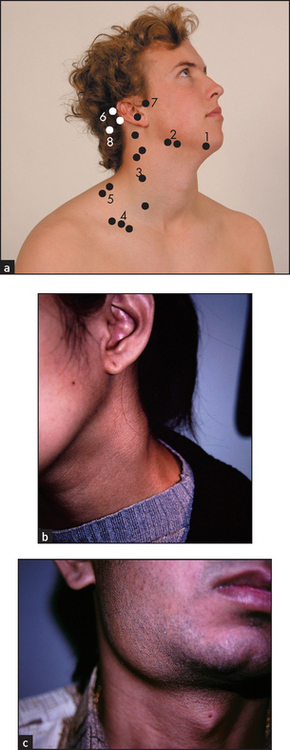
Figure 21.11 (a) Cervical and supraclavicular lymph nodes
1 = submental; 2 = submandibular; 3 = jugular chain (posterior cervical and anterior or deep cervical); 4 = supraclavicular; 5 = posterior triangle; 6 = postauricular; 7 = preauricular; 8 = occipital.
The detection of lymphadenopathy should lead to a search of the area drained by the enlarged nodes. This may reveal the likely cause (see List 21.4). Lymphangitis (see Figure 21.12), which is inflammation of the lymphatic vessels, may be visible in the drainage area of the abnormal nodes, especially if the enlargement is caused by infection.

Bone tenderness
While the patient is sitting up, tap over the spine with your fist for bony tenderness. This may be caused by an enlarging marrow due to infiltration by myeloma, lymphoma or carcinoma, or due to malignant disease of the bony skeleton. Also gently press the sternum and both clavicles with the heel of your hand and then test both shoulders by pushing them towards each other with your hands.
The abdominal examination
Lay the patient flat again. Examine the abdomen carefully, especially for splenomegaly6(see List 21.5 and Good signs guide 21.2), hepatomegaly, para-aortic nodes (rarely palpable), inguinal nodes and testicular masses. Remember that a central deep abdominal mass may occasionally be due to enlarged para-aortic nodes. Para-aortic adenopathy strongly suggests lymphoma or lymphatic leukaemia. The rectal examination may reveal evidence of bleeding or a carcinoma.
Two further methods of assessing for splenomegaly are described here:
1. Percussion of the Traube space: with the patient supine, abduct the patient’s left arm slightly, ask the patient to breathe normally and percuss across the space from its medial to lateral margins at a couple of levels. The note should remain resonant unless the spleen is enlarged.
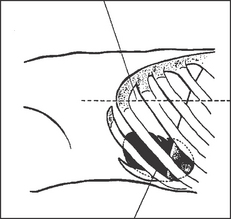
2. Percussion by the Castell method: with the patient still supine, percuss over the Castell spot (see Figure 21.13)—the lowest left intercostal space in the anterior axillary line—with the patient in full inspiration and expiration. The note will become dull during inspiration if the spleen is enlarged. The sensitivity and specificity of this test have been recorded as high as 82% and 83%, respectively.
Assessment of the patient with suspected malignancy is presented in List 21.6.7
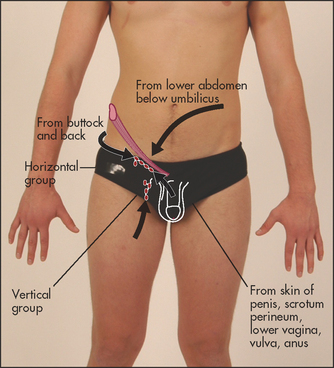
Inguinal nodes
There are two groups of inguinal nodes: one along the inguinal ligament and the other along the femoral vessels (see Figure 21.14). Small, firm mobile nodes are commonly found in otherwise normal subjects.
Legs
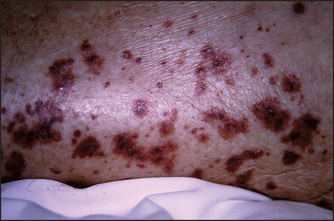
Inspect for any bruising, pigmentation or scratch marks. Palpable purpura over the buttocks and legs are present in Henoch-Schönlein purpuraf (see Figure 21.15). Drug reactions may cause purpura on the legs or elsewhere (see Figure 21.16). Leg ulcers may occur above the medial or lateral malleolus in association with haemolytic anaemia (including sickle cell anaemia and hereditary spherocytosis), probably as a result of tissue infarction due to abnormal blood viscosity. Leg ulcers can also occur with thalassaemia, macroglobulinaemia, thrombotic thrombocytopenic purpura and polycythaemia, as well as in Felty’s syndrome. Chronic use of hydroxyurea for myeloproliferative disorders can cause malar ulcers.

Figure 21.15 Henoch-Schönlein purpura (From McDonald FS, ed. Mayo Clinic images in internal medicine, with permission. © Mayo Clinic Scientific Press and CRC Press.)
Occasionally, popliteal nodes may be felt in the popliteal fossa.
The legs should also be examined for evidence of the neurological abnormalities caused by vitamin B12 deficiency: peripheral neuropathy and subacute combined degeneration of the spinal cord. Vitamin B12 is an essential cofactor in the conversion of homocysteine to methionine; in B12deficiency, the lack of methionine impairs methylation of myelin basic protein. Deficiency of vitamin B12 can also result in optic atrophy and mental changes. Lead poisoning causes anaemia and foot (or wrist) drop.
Signs of venous disease in the legs may indicate previous venous thromboses and damage to the venous valves between the superficial and deep veins. Look for signs of current venous thrombosis (page 91).
Fundi
Examine the fundi. An increase in blood viscosity, which occurs in diseases such as macroglobulinaemia, myeloproliferative disease or chronic granulocytic leukaemia, can cause engorged retinal vessels and later papilloedema. Haemorrhages may occur because of a haemostatic disorder. Retinal lesions (multiple yellow-white patches) may be present in toxoplasmosis (see Figure 41.5 on page 558) and cytomegalovirus infections (see Figure 41.6 on page 558).
References
1. Strobach, RS, Anderson, SK, Doll, DC, Ringenberg, QS. The value of the physical examination in the diagnosis of anaemia: correlation of the physical findings and the haemoglobin concentrations. Arch Intern Med. 1988; 148:831–832. [Palmar crease pallor can occur above a haemoglobin of 70 g/L.].
2. Nardone, DA, Roth, KM, Mazur, DJ, McAfee, JH. Usefulness of physical examination in detecting the presence or absence of anemia. Arch Intern Med. 1990; 150:201–204.
3. Sheth, TN, Choudray, NK, Bowes, M, Detsky, AS. The relation of conjunctival pallor to the presence of anemia. J Gen Intern Med. 1997; 12:102–106. [The presence of conjunctival pallor is a useful indicator of anaemia, but its absence is unhelpful. It is also a reliable sign.].
4. Linet, OI, Metzler, C. Practical ENT: incidence of palpable cervical nodes in adults. Postgrad Med. 1977; 62:210–211. [213. In young adults without chronic disease, palpable cervical lymph nodes are often detected but are not clinically important. Remember, posterior cervical nodes are almost never normal.].
5. Habermann, TM, Steensma, DP. Lymphadenopathy. Mayo Clin Proc. 2000 Jul; 75(7):723–732.
6. Grover, SA, Barkun, AN, Sackett, DL. Does this patient have splenomegaly. JAMA. 1993; 270:2218–2221. [A valuable guide to assessment of splenomegaly, although the recommendations are controversial. A combination of percussion and palpation may best identify splenomegaly, but in contrast to hepatomegaly, percussion may be modestly more sensitive, according to the few available studies. Our conclusion is that this needs to be better established; in practice splenomegaly is often missed by percussion alone.].
7. Cancer detection in adults by physical examination. US Public Health Service. Am Fam Phys. 1995; 51:871–874. [877–880, 883–885.].
aAugustus Roi Felty (1895–1963), physician, Hartford Hospital, Connecticut, described this in 1924.
bAlfred Hess (1875–1933), professor of paediatrics, New York, described this in 1914.
cThis test is only of historical interest these days, as a platelet count can be obtained almost as quickly in most hospitals and clinics. A blood pressure cuff, placed over the upper arm, is inflated to a point 10 mmHg above the diastolic blood pressure. Wait for 5 minutes, then deflate the cuff and wait for another 5 minutes before inspecting the arm. Look for petechiae, which are usually most prominent in the cubital fossa and near the wrist, where the skin is most lax. Fewer than 5 petechiae per cm2 is normal, while more than 20 is definitely abnormal, suggesting thrombocytopenia, abnormal platelet function or capillary fragility.
dThomas Hodgkin (1798–1866), famous student at Guy’s Hospital, London, described his disease in 1832. The first case he described was a patient of Richard Bright’s. Hodgkin was one of the first to use the stethoscope in England. On failing to be appointed a physician, he gave up medicine and became a missionary.
eHeinrich Wilhelm Gottfried von Waldeyer-Hartz (1836–1921), Berlin anatomist.
fHenoch-Schönlein purpura is also characterised by glomerulonephritis (manifested by haematuria and proteinuria), arthralgias and abdominal pain.