Chapter 19 A place for new research directions
The previous chapter explored the history of clinical reasoning research, identifying trends in research that investigated and represented the nature of clinical reasoning and core issues such as novice/expert differences and the use of decision theory in clinical decision making. A broad transition and paradigm shift was identified from a focus on quantitative research to an increasing emphasis on qualitative research.
In this chapter we extend this discussion into four areas: reflections on the changing research questions that have been and are being addressed in this field; areas of clinical reasoning that require further research; factors influencing research directions; and an interpretation of the current direction that cutting edge clinical reasoning research is taking.
SETTING THE CONTEXT
Clinical reasoning is the core of clinical practice; it enables practitioners to make informed and responsible clinical decisions and address problems faced by their patients or clients. Around 20 years ago Schön (1987) pointed out that when a practitioner deals with new professional problems the first issue is ‘problem setting’. This means choosing and naming the things that will be noticed and the things that will be ignored, which he described as ‘naming and framing’ (p. 4). The naming and framing process is essentially linguistic and discursive; it depends on factors such as ‘disciplinary backgrounds, organizational roles, past histories, interests and political/economic perspectives’ (p. 4). Schön indicated that this process of problem setting is also an ontological process. The professional is engaged in a localized and specialized form of world making and world interpretation. From this point of view, professional practice is much more than a straightforward epistemological or knowledge framing task, and practice involves much more than acquiring and mastering a body of propositional knowledge and learning how to apply it. From the interpretive viewpoint, mastering and applying a body of knowledge are still important, but being a professional such as a dentist or a physiotherapist is a much greater challenge. It is a way of being in the world.
This ontological idea of professionalism is echoed in the work of others, such as Thomas Kuhn (1996). Kuhn described how professionals (scientists, in his case) live in the world, and perceive it, in a way that is radically different from non-professionals, and that this comes about because they have internalized a particular way of perceiving the world. A layperson might see lines on paper whereas a cartographer instantly perceives a terrain (Kuhn 1996, p. 111). Kuhn also wrote that when scientists undergo a paradigm shift, that is, a radical change in the sets of ideas and assumptions they use to perceive and conceptualize the world, they talk of life after this experience as being like living in a new world.
Vygotsky (1978) noted that this internalization of particular ways of perceiving the world is true of all humans, starting at an early age. He used the example of a clock. When we see a clock, we learn to perceive it instantly as a clock, not something round and black-cased with hands, which is then consciously and deliberately interpreted as being a clock. If there is interpretation it is instantaneous and unconscious. Shotter (2000) realized that professional ways of seeing the world are extensions of this. Professional socialization shapes our attention and makes us see things in particular ways. For example, one medical student in a research project on learning clinical reasoning (Loftus 2006, p. 199) spoke of being able to instantly recognize ‘glaring cardiac signs’ in a patient. Shotter (2000), following Vygotsky, maintained that it is through our language that this process occurs. These ways of responding to situations become embodied within us, and are therefore ontological rather than purely epistemological (i.e. words and knowledge). Professional ways of seeing the world are included among what Vygotsky (1978) described as higher mental functions. Such functions are the more complex and intellectually demanding skills that humans can develop, such as clinical reasoning, and they are qualitatively different from the lower mental functions or component cognitive skills (e.g. analysis) which they may incorporate.
THE CHANGING SHAPE OF RESEARCH QUESTIONS IN CLINICAL REASONING RESEARCH
Historically, in the majority of clinical reasoning research, researchers have stood outside the phenomenon of clinical reasoning, looking in, and addressed three key questions:
Not surprisingly, given the historical context of the scientification of health care and the dominance of medicine, these questions fit the expectations of the empirico-analytical research paradigm and the biomedical model. In both cases hypothetico-deductive reasoning or hypothesis generation and testing is the dominant mode of reasoning and decision making. The empirico-analytical research paradigm adopts a positivist philosophical stance where objectivity is the key issue and sense data determine reality; its goal is to measure, test hypotheses, discover, predict, explain, control, generalize and identify cause–effect relationships. Within the biomedical model the body is seen as a machine that can be adjusted or treated in seeking to cure (a person’s condition) or restore the body to normal functioning. If this restitution narrative fails (which is common in chronic conditions) the patient may be labelled ‘failed’ or ‘failing’ or ‘noncompliant’ (Alder 2003). In the wellness model, in comparison, which fits with the interpretive and critical paradigms, the patient – the person – has greater initiative and support to write a different (e.g. ability) narrative.
When clinical reasoning research entered the interpretive paradigm the philosophical stance turned to idealism. In this philosophy the emphasis is on the actors’ ideas or embodied knowing as the determinant of social reality, and multiple constructed or storied realities of the social world are recognized and acknowledged. Within this paradigm researchers seek to understand, interpret, seek meaning, describe, illuminate and theorize about lived experiences and actions. The context of human actions (including decision making) is seen as a vital influence on these actions and experiences. Hence, the way clinical reasoning came to be viewed changed towards a greater valuing of the narrative, contextual, conditional and interpersonal dimensions of practice. And the focus shifted onto the larger interactive phenomenon of making clinical decisions in the context of people with healthcare needs, their interests and concerns, their families, and the healthcare team.
Research in the interpretive paradigm has been conducted by Benner (1984) in nursing (with an emphasis on seeking understanding of behaviours and context), by Crepeau (1991) and Fleming (1991) in occupational therapy (with an emphasis on structuring meaning and interpreting the problem from the patient’s perspective) and by Jensen et al (1992, 2007) in physiotherapy (with a focus on elucidating the complex and unknown processes that occur during therapeutic interventions). The clinical reasoning processes which such approaches describe focus on seeking a deep understanding of patients’ perspectives and the influence of contextual factors, in addition to the more traditional and clinical understanding of the patient’s condition. The relevance of this broader perspective is evident in the growing body of research demonstrating that the meaning patients give to their problems (including their understanding of and feelings about their problems) can significantly influence their levels of pain tolerance, disability and eventual outcome (Borkan et al 1991, Feuerstein & Beattie 1995, Malt & Olafson 1995). As the volume and depth of research into clinical reasoning expands, it is becoming more and more apparent that traditional clinical reasoning models do not encompass the varying dimensions or reflect the diverse discipline-specific practice paradigms that exist across the health professions.
New questions being addressed in interpretive research include:
Another emerging trend in seeking to enhance clinical reasoning is critical paradigm research. This paradigm is underpinned by the philosophical stance of historical realism in which it is recognized that social practices and culture shape practice over time. The goals of research in this paradigm are to improve, reform, empower, or change reality or a situation. Here we see the place of the individual as an agent of change, and action for self-enhancement as well as a change in the role of the health professional from provider to collaborator. Action research, collaborative inquiry and new paradigm research (Reason & Rowan 1981), with an emphasis on the researcher as the subject, means and object of his or her own research, are some of the strategies adopted here.
Limited research in this paradigm has been conducted specifically looking at clinical reasoning as a phenomenon. However, there is an emerging body of research, often blending interpretive and critical paradigm research (Charles et al 2005, McCormick 1998, Trede 2006), into the adoption of collaborative decision-making models and patient empowerment. In keeping with a growing interest in patient-centred care and in health practice models beyond the biomedical model, research questions in this category include:
AREAS OF CLINICAL REASONING NEEDING MORE RESEARCH
Returning to the notion of naming the things to be noticed about the problem to be solved and framing of the problem (e.g. within disciplinary backgrounds), we can identify a link between research paradigms and these actions (Table 19.1).
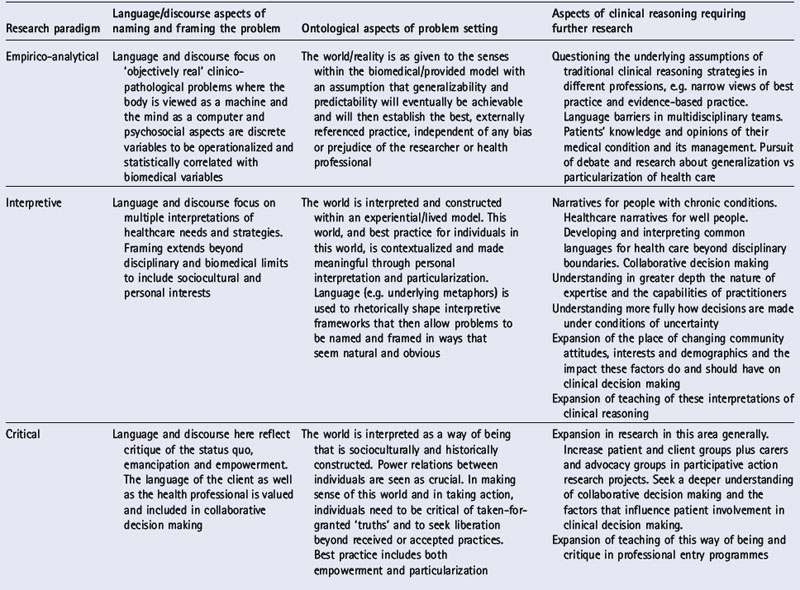
Naming and framing clinical problems depends to a large extent on the model of rationality underlying the particular health professions and the sciences they claim to be founded upon. The empirico-analytical paradigm uses a Cartesian approach to rationality. Descartes (trans. Clarke, 1999) claimed that the only rationality to be trusted was based upon mathematics and mathematical axioms. Despite the successes of the sciences built upon this form of rationality, it is increasingly recognized that Cartesianism demonstrates its limitations when applied to patient care. Wittgenstein (1958) argued that mathematical axioms are themselves conventions of language. From this viewpoint, language is more fundamental than mathematics. In fact, it can be argued that the way forward is, in a sense, a return to the past, provided we are willing to reconsider the ideas of such thinkers as Aristotle. Aristotle (trans. Lawson-Tancred, 1991) maintained that there was more than one way to be rational, claiming that rhetoric and argumentation were important ways of being rational. He further stated that different problems needed different types of rationality if they were to be adequately dealt with. Some debates and differences of opinion are best settled with persuasive argument rather than by numbers and measurements. The interpretive and critical paradigms both embody important alternative ways of being rational.
FACTORS INFLUENCING RESEARCH DIRECTIONS IN CLINICAL REASONING
THE CONTEXT OF CLINICAL DECISION MAKING
A key aspect of planning future clinical reasoning research is understanding the context of healthcare practice and decision making. Challenges facing health care today include the need to:
THE CONTEXT OF THE PROFESSION(S)
Another key factor influencing the directions of clinical reasoning research is the state of development of professions. Research into professional practice (e.g. Higgs & Titchen 2001) provides valuable insights into the nature of practice and factors influencing practice and reasoning. The professions are being shaped by external and internal forces such as demands for professional accountability and cost efficiency, driven by such factors as escalating healthcare costs, increasing public education and access to health-related information, technological advances and evidence-based practice. It is important to recognize that the outcomes of the clinical decisions practitioners make rest in their commitment to quality, relevant and accountable decision making. Such commitment is shaped by these contextual influences and also by the experiences of professionals and novices/students during their education and socialization. Research in education that is linked to clinical reasoning often examines the merits and challenges of problem-based learning. Medicine has the longest history of researching clinical reasoning, while nursing has a long history of workplace-based education. Further research into the context and education of professionals and their changing workplaces continues to be needed in support of quality health care and decision making.
THE NATURE OF THE PHENOMENON
Chapter 1 described clinical reasoning as both a simple and a complex phenomenon. Those researching clinical reasoning specifically and professional practice more generally must recognize the central role of clinical reasoning in practice. Clinical reasoning directs and informs the whole of clinical practice. Thus students of clinical reasoning must consider its nature and complexities. The following view of clinical reasoning demands research beyond the laboratory and involving multiple perspectives of the various participants in clinical decision making. Clinical reasoning is predominantly a human and social phenomenon that requires greater exploration through the human and social research paradigms.
Clinical reasoning (or practice decision making) is a context-dependent way of thinking and decision making in professional practice to guide practice actions. It involves the construction of narratives to make sense of the multiple factors and interests pertaining to the current reasoning task. It occurs within a set of problem spaces informed by practitioners’ unique frames of reference, workplace contexts and practice models, as well as by patients’ or clients’ contexts. It utilizes core dimensions of practice knowledge, reasoning and metacognition and draws upon these capacities in others. Decision making within clinical reasoning occurs at micro-, macro- and meta-levels and may be individually or collaboratively conducted. It involves the metaskills of critical conversation, knowledge generation, practice model authenticity and reflexivity (Higgs 2006).
INTERPRETING DIRECTIONS OF CUTTING EDGE CLINICAL REASONING RESEARCH
A paradigm shift, as defined by Kuhn (1996), is a major and radical change in the conceptual basis underlying a discipline. Paradigm shifts are inevitable in response to changing circumstances which demand different ways of understanding and exploring these new realities. There have been a number of distinct paradigm shifts in clinical reasoning research, from early behaviourism which was superseded by cognitivism and the development of the separate paradigm of medical decision theory. These are discussed in more detail in Chapter 18. In this section we reflect on emerging changes of direction in research. These ‘paradigm shifts’ are also called ‘turns’ or ‘moments’, and we see three emerging turns in clinical reasoning research and practice.
The first of these turns we describe as the ‘interdisciplinary turn’. In a previous edition of this book, Elstein & Schwarz (2000) recognized that the phenomenon we refer to as clinical reasoning is complex and multidimensional. They called for research into clinical reasoning that was informed by a range of academic disciplines. Social constructionism is one school of thought that synthesizes ideas from disciplines as diverse as philosophy, sociology and anthropology (Lupton 2003). Some research into clinical reasoning has been conducted from within the social constructionist worldview (e.g. Loftus 2006), with insights that would simply not have been possible with research from a strictly Cartesian point of view. Interdisciplinary research also includes investigation of emerging and potential trends in clinical decision making that transcend professional groups (with their diverse backgrounds) and include patients as members of multidisciplinary teams (see Chapters 26, 27, 32, 34).
The second turn we see starting to emerge in clinical reasoning research relates to ‘the linguistic turn’. The linguistic turn is the simple but profound recognition that our use of language is fundamental to what and who we are as human beings. Language is not merely a means of representing the world. Our use of language permits us, in a sense, to bring the world into being. As Gadamer (1989, p. 443) observed, ‘Language is not just one of man’s possessions in the world; rather, on it depends the fact that man has a world at all’. We are now beginning to appreciate the extent to which linguistic and discursive forms such as metaphor and narrative form a part of the phenomenon of clinical reasoning (Loftus 2006). An excellent and recent example of such an approach is Charon’s (2006) study of narrative medicine, in which she argues that narratology can provide insights that enable practitioners to come to a deeper understanding of their patients’ problems, and equip them with the cognitive tools to accompany those same patients on their journeys through illness and its treatment (see also Chapter 32).
Our third turn we call ‘the meta turn’. It reflects cutting edge research which calls for clinical reasoning research and practice to be grounded in an understanding of reasoning as occurring within practice models and clinical reasoning models (see e.g. Trede 2006, Trede & Higgs 2003). This proposition calls for informed practice, that is, practice informed by these understandings. Practice, we contend, should seek to embody authentically the practitioner’s chosen practice model, interests and clinical decision-making strategies. One such approach is the adoption of the critical social sciences as the basis for emancipatory practice (Trede et al 2003).
CONCLUSION
Clinical reasoning research is rapidly changing. While such research is still in the process of breaking away from and challenging the reductionist assumptions of much past research, the acceptance of new academic disciplines with different assumptions holds promise of providing exciting new insights into the ways in which clinical reasoning forms the basis of healthcare practice. As mentioned above, Elstein & Schwarz (2000) have called for research into clinical reasoning from different disciplines. We hope that they would be both pleased and surprised at the extent to which their call has been answered. We stand on the verge of a vital expansion in the scope of research in clinical reasoning that can go in many directions. There is much more to discover about clinical reasoning by pursuing promising new directions in research and by sharing across disciplines the findings of such research. This book is one means to that end.
Alder S. Beyond the restitution narrative. Sydney: University of Western Sydney, 2003. Unpublished PhD thesis
Aristotle. Lawson-Tancred HC, editor. The art of rhetoric. London: Penguin Books. 1991.
Benner P. From novice to expert: excellence and power in clinical nursing practice. Menlo Park, CA: Addison Wesley, 1984.
Borkan JM, Quirk M, Sullivan M. Finding meaning after the fall: injury narratives from elderly hip fracture patients. Social Science and Medicine. 1991;33:947-957.
Charles C, Gafni A, Whelan T, et al. Treatment decision aids: conceptual issues and future directions. Health Expectations. 2005;8(2):114-125.
Charon R. Narrative medicine: honoring the stories of illness. Oxford: Oxford University Press, 2006.
Crepeau EB. Achieving intersubjective understanding: examples from an occupational therapy treatment session. American Journal of Occupational Therapy. 1991;45:1016-1025.
Descartes R. Clarke DM, editor. Discourse on method and related writings. London: Penguin Books. 1999.
Elstein AS, Schwartz A. Clinical reasoning in medicine. In: Higgs J, Jones M, editors. Clinical reasoning in the health professions. 2nd edn. Oxford: Butterworth-Heinemann; 2000:95-106.
Feuerstein M, Beattie P. Biobehavioral factors affecting pain and disability in low back pain: mechanisms and assessment. Physical Therapy. 1995;75:267-280.
Fleming MH. Clinical reasoning in medicine compared with clinical reasoning in occupational therapy. American Journal of Occupational Therapy. 1991;45:988-996.
Gadamer H-G. Truth and method, 2nd revised edn. New York: Continuum, 1989.
Higgs J. The complexity of clinical reasoning: exploring the dimensions of clinical reasoning expertise as a situated, lived phenomenon. Seminar presentation at the Faculty of Health Sciences, University of Sydney, Australia, May 5. 2006.
Higgs J, Titchen A. Professional practice in health, education and the creative arts. Oxford: Blackwell Science, 2001.
Jensen GM, Shepard KF, Hack LM. Attribute dimensions that distinguish master and novice physical therapy clinicians in orthopedic settings. Physical Therapy. 1992;72:711-722.
Jensen GM, Gwyer J, Hack LM, et al. Expertise in physical therapy practice: applications in practice, education and research, 2nd edn. Philadelphia: Elsevier, 2007.
Kuhn T. The structure of scientific revolutions, 3rd edn. Chicago: University of Chicago Press, 1996.
Loftus S. Language in clinical reasoning: learning and using the language of collective clinical decision making. Australia: PhD thesis, University of Sydney, 2006. Online. Available: http://ses.library.usyd.edu.au/handle/2123/1165 7 July 2007
Lupton D. Medicine as culture: illness, disease and the body in Western societies, 2nd edn. London: Sage, 2003.
McCormack B. An exploration of the theoretical framework underpinning the autonomy of older people in hospital and its relationship to professional nursing practice. England: University of Oxford, 1998. DPhil thesis
Malt UF, Olafson OM. Psychological appraisal and emotional response to physical injury: a clinical, phenomenological study of 109 adults. Psychiatric Medicine. 1995;10:117-134.
Nietzsche F. Kaufman W, Hollingdale RJ, editors. The will to power. New York: Vintage Books. 1968. [Opening chapter quotation based on Book 3, quotation no 481, p. 267]
Reason P, Rowan J, editors. Human inquiry: a sourcebook of new paradigm research. London: John Wiley, 1981.
Schön DA. Educating the reflective practitioner: toward a new design for teaching and learning in the professions. San Francisco: Jossey-Bass, 1987.
Shotter J. Seeing historically: Goethe and Vygotsky’s ‘enabling theory-method’. Culture and Psychology. 2000;6(2):233-252.
Trede F. A critical practice model for physiotherapy. Australia: University of Sydney, 2006. Unpublished PhD thesis
Trede F, Higgs J. Re-framing the clinician’s role in collaborative clinical decision making: re-thinking practice knowledge and the notion of clinician–patient relationships. Learning in Health and Social Care. 2003;2(2):66-73.
Trede F, Higgs J, Jones M, et al. Emancipatory practice: a model for physiotherapy practice? Focus on Health Professional Education: A Multidisciplinary Journal. 2003;5(2):1-13.
Vygotsky LS. Mind in society: the development of the higher psychological processes. Cambridge, MA: Harvard University Press, 1978.
Wittgenstein L. 3rd edn. Anscombe GEM, editor. Philosophical investigations. Upper Saddle River, NJ: Prentice Hall. 1958.