Gastrointestinal and Digestive Care Plans
Bariatric Surgery
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans, go to http://evolve.elsevier.com/Gulanick/.
Overweight; Obesity; Gastric Banding; Gastric Bypass
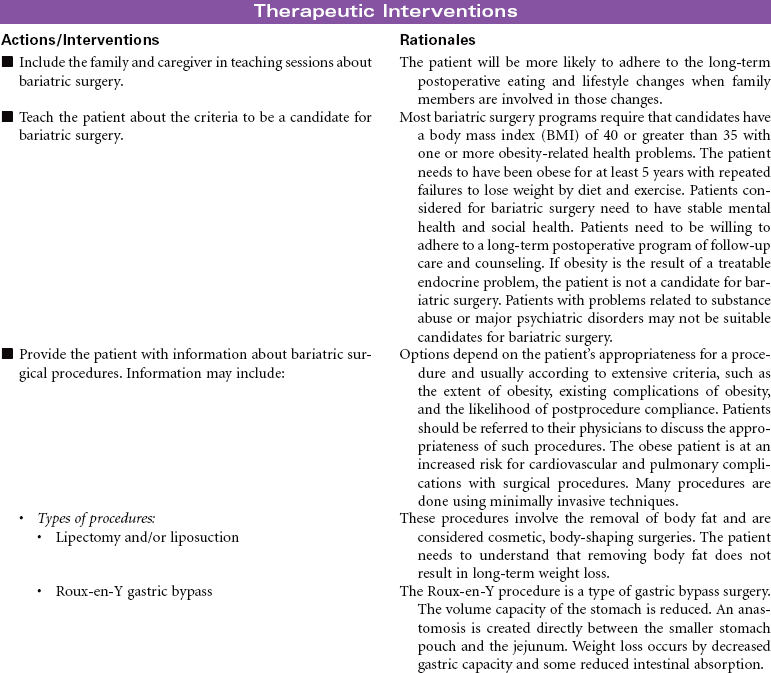
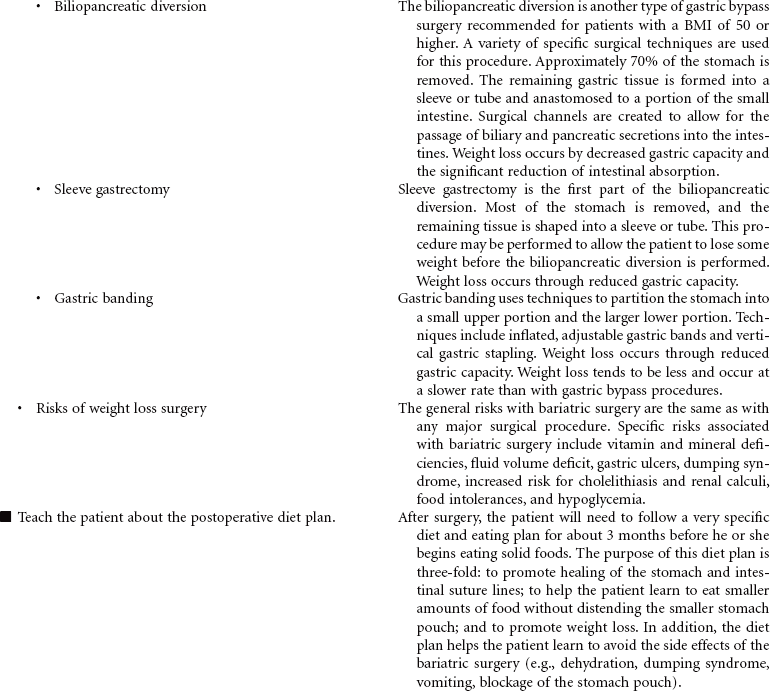
Overweight and obesity are major health problems in the United States, and their prevalence is growing globally. Bariatric surgical procedures are usually used for those patients considered morbidly obese with a body mass index (BMI) greater than 40. Patients with a BMI between 35 and 40 may be candidates for this type of surgery if they have other chronic health problems related to their obesity, such as diabetes mellitus, sleep apnea, hypertension, or heart failure. Evidence indicates that these surgical approaches to weight management provide the patient with more long-lasting weight loss compared to nonsurgical approaches such as diet and exercise. In addition, patients usually experience significant improvement in their obesity-related health problems. Gastric banding or stapling surgical techniques restrict the volume of the stomach and therefore decrease the amount of food the patient consumes. Gastric bypass procedures reroute the passage of food through the small intestine to reduce the absorption of food intake. Most bariatric surgery programs include a long-term postoperative program of lifestyle modifications such as eating habits, physical activity, and psychological support.
 Deficient Knowledge
Deficient Knowledge
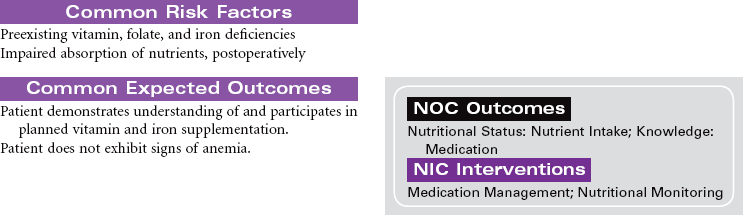
 Risk for Ineffective Therapeutic Regimen Management
Risk for Ineffective Therapeutic Regimen Management
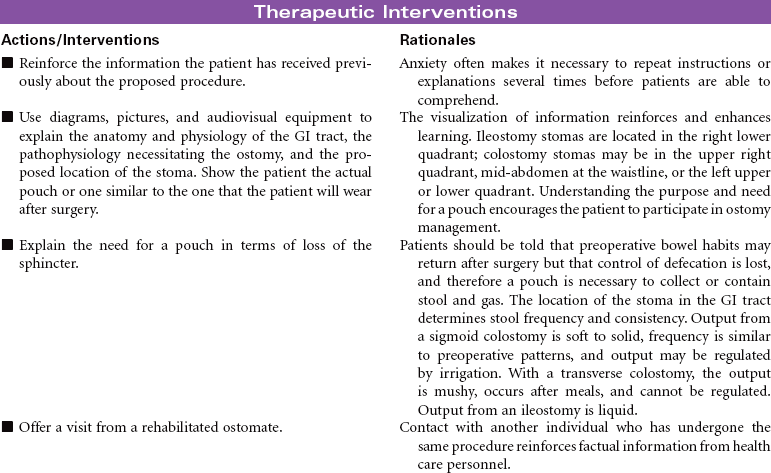
Bowel Diversion Surgery: Colostomy, Ileostomy
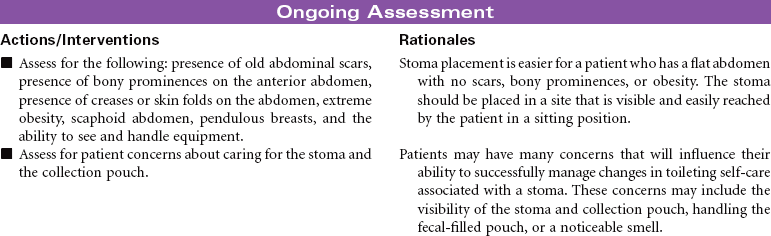
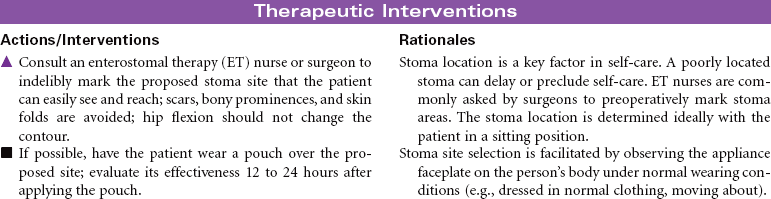
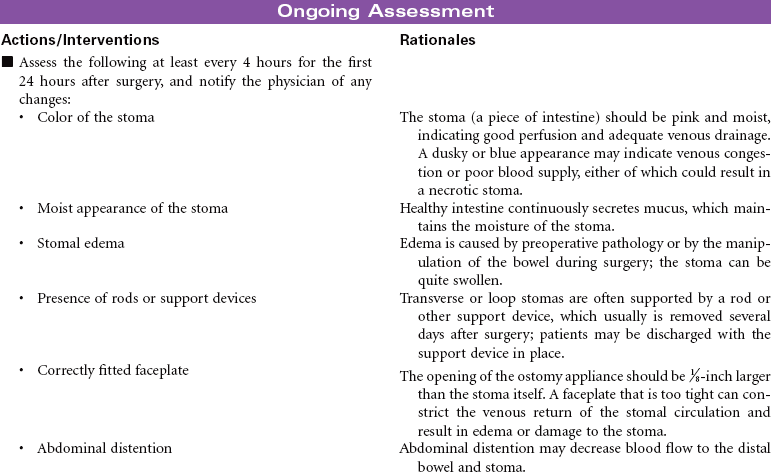
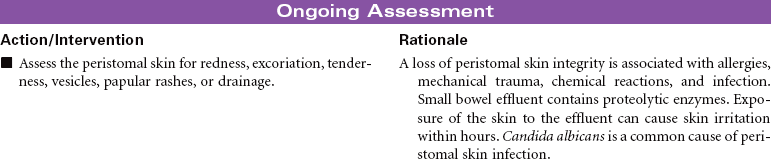
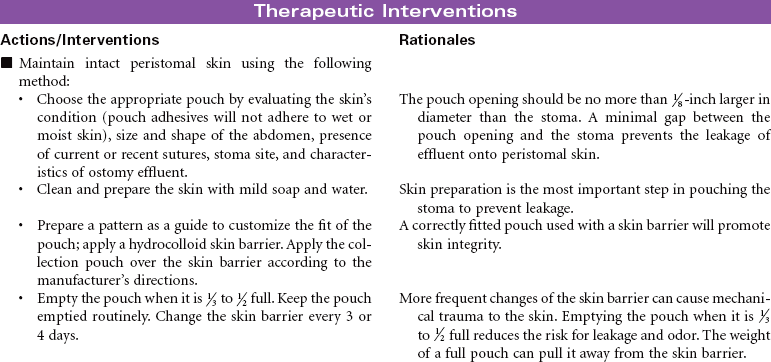
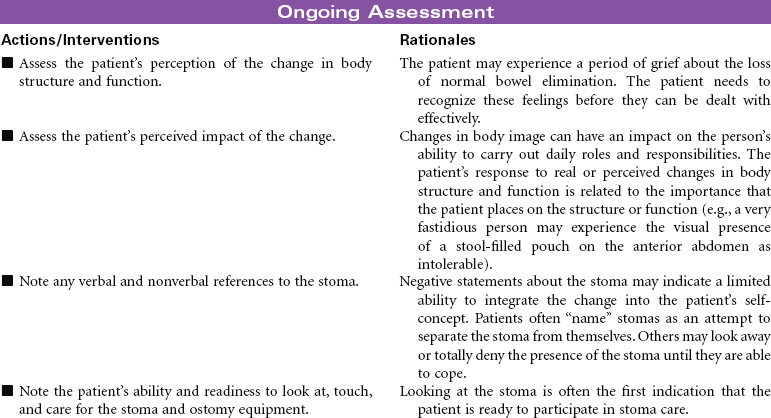
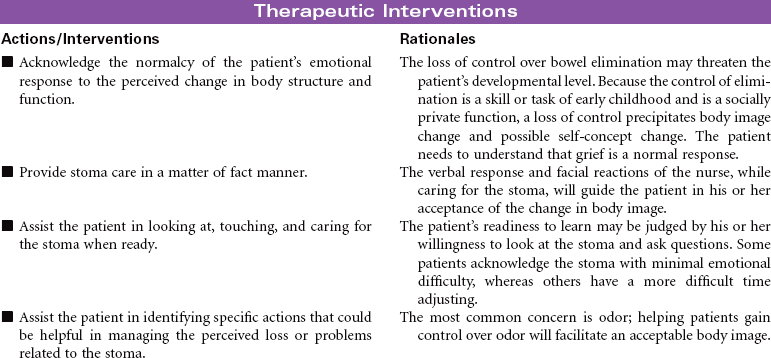
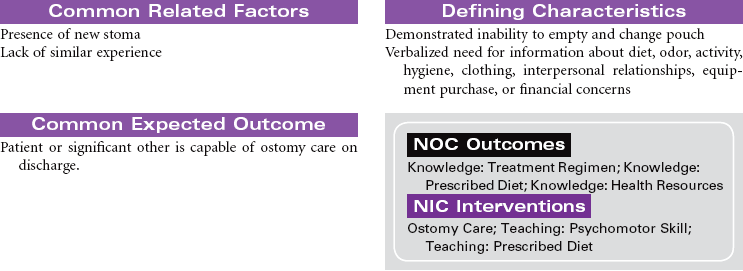
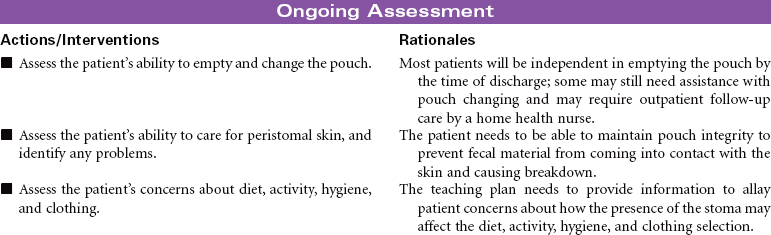
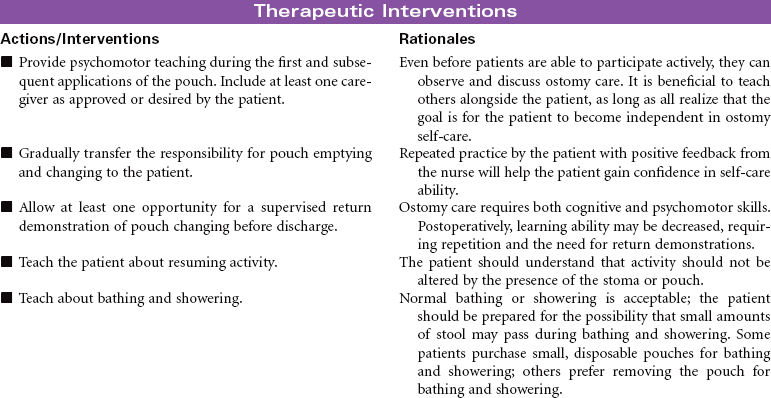
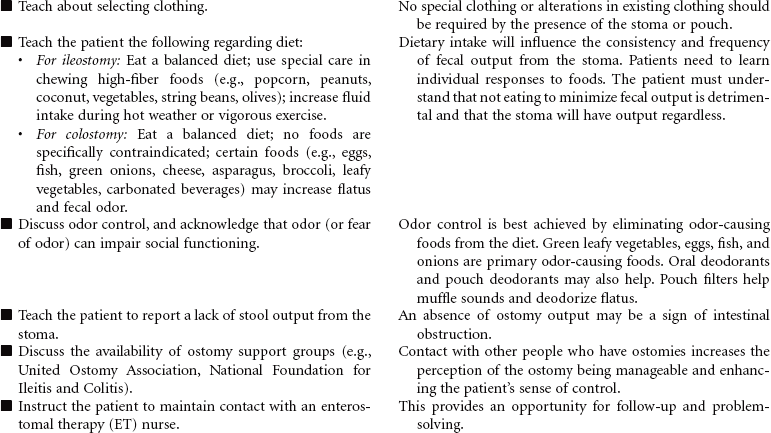
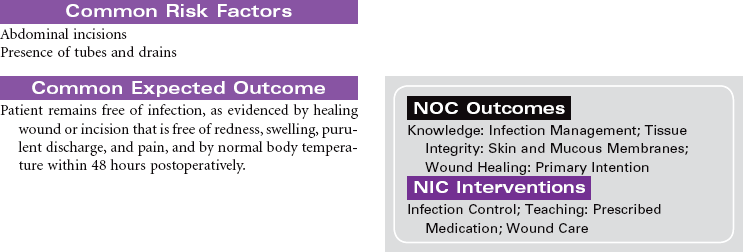
Bowel diversion surgery creates an opening into the small or large intestine that is brought to the external surface of the abdominal wall (stoma). These surgeries are done for the purpose of diverting the fecal stream past an area of obstruction or disease, protecting a distal surgical anastomosis, or providing an outlet for stool in the absence of a functioning intact rectum. The procedures may be performed to promote wound healing of an intestinal injury such as a gunshot wound. Diverted fecal material is directed away from the wound to promote wound healing. Depending on the purpose of the surgery and the integrity and function of anatomical structures, stomas may be temporary or permanent. Peristomal irritation, body image, self-care, and knowledge deficit are important nursing concerns. This care plan focuses primarily on the person with a new stoma who is being cared for in the hospital environment.





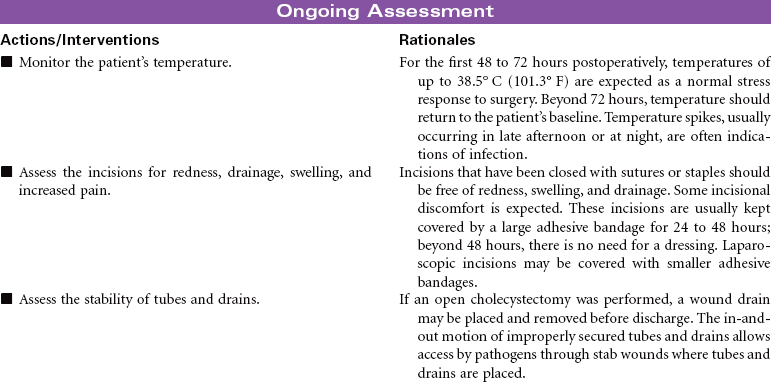
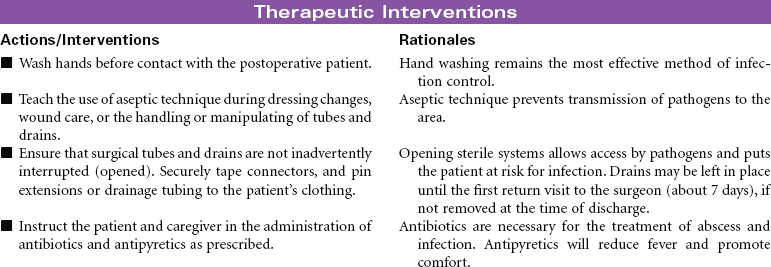
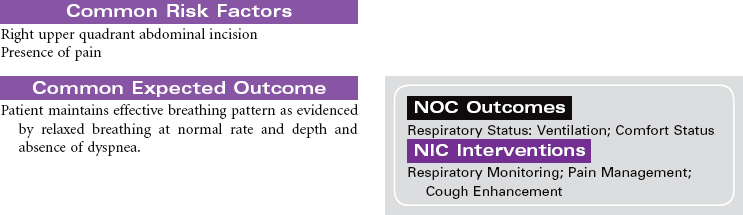
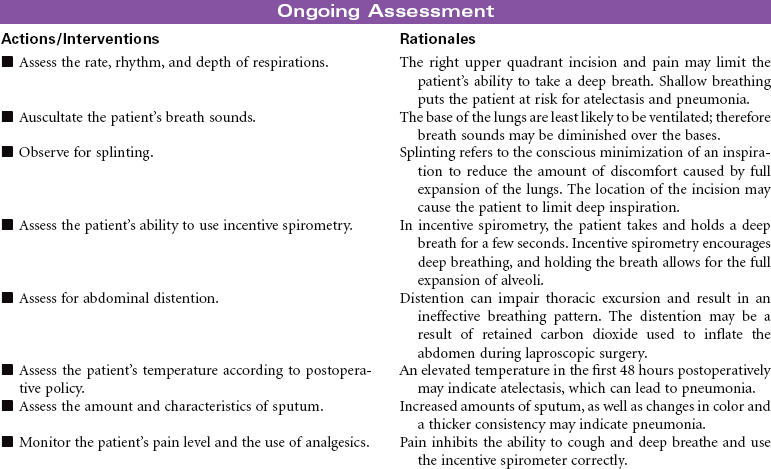
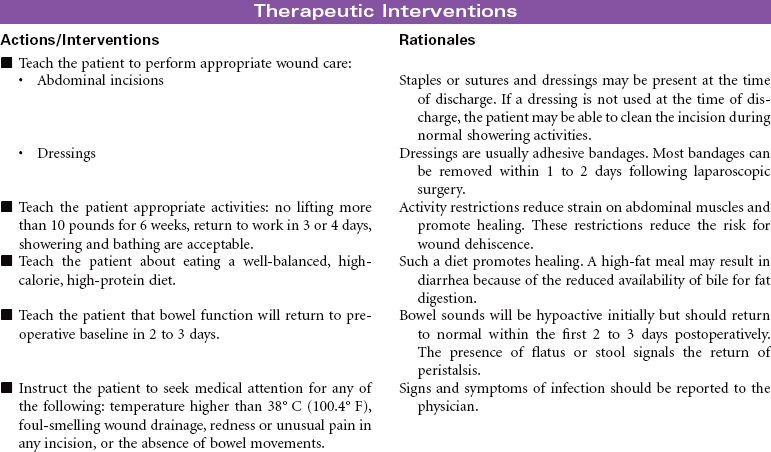
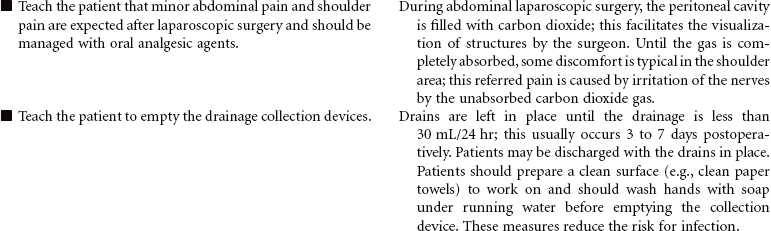
Cholecystectomy: Laparoscopic/Open, Postoperative Care
Cholecystitis is an inflammation of the gallbladder. Most patients who develop cholecystitis have cholelithiasis or gallstones. The most common manifestation of acute cholecystitis is right upper quadrant pain that occurs after eating a high-fat meal. Although eating a fat-free diet will decrease the patient’s symptoms temporarily, surgical removal of the gallbladder and gallstones (cholecystectomy) is usually recommended. The preferred method for cholecystectomy is laparoscopic surgery using small abdominal incisions in combination with telescopic visualization of the abdominal cavity. The abdominal cavity is inflated with carbon dioxide to facilitate visualization of the abdominal organs generally and the gallbladder specifically. Once the gallbladder is dissected away from surrounding tissue, it is removed through one of the puncture wounds. The carbon dioxide is evacuated, and the multiple puncture wounds are closed. If the surgeon is not able to successfully remove the gallbladder using a laparoscopic approach, a larger open incision is made in the right upper quadrant for direct visualization and removal of the gallbladder.

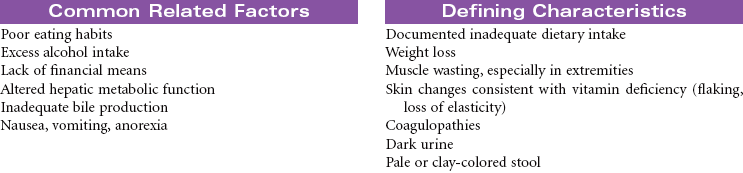
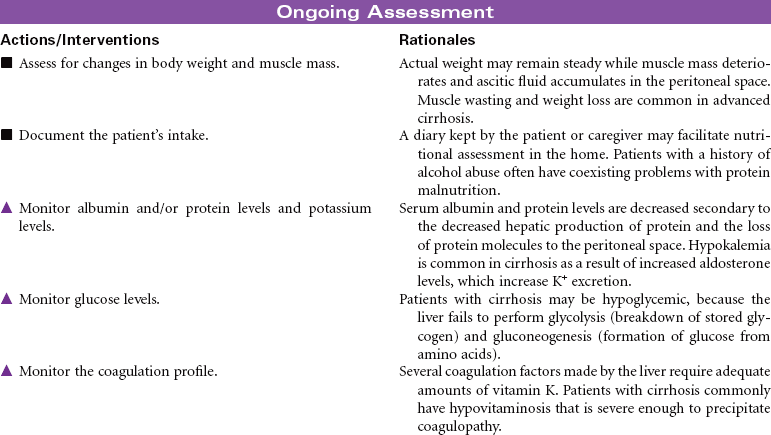
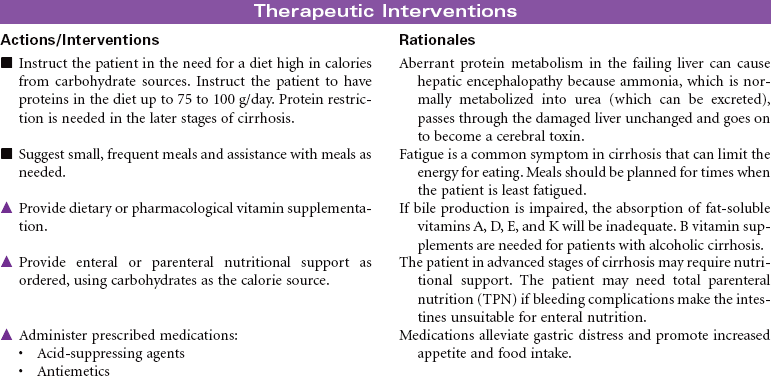
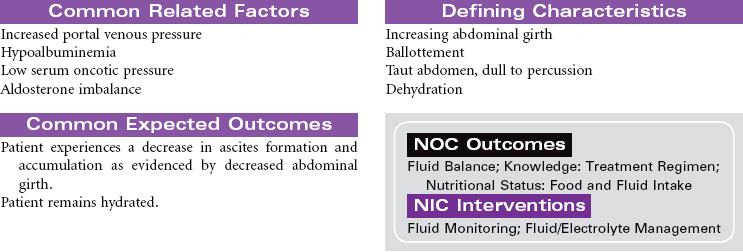
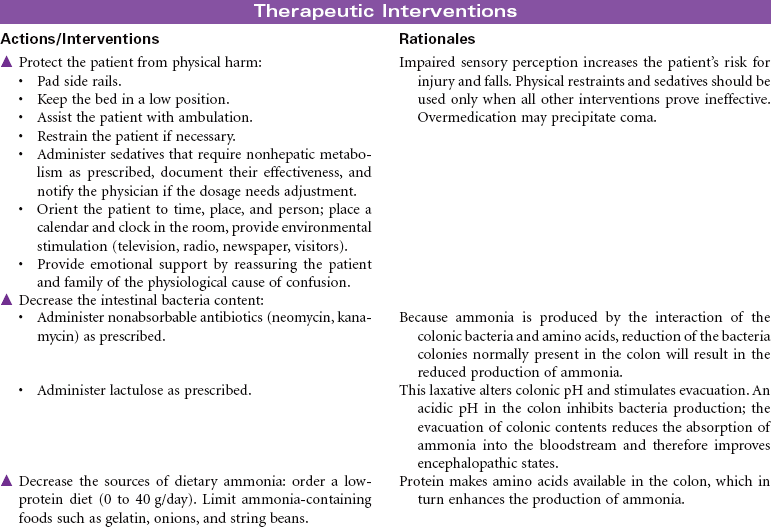
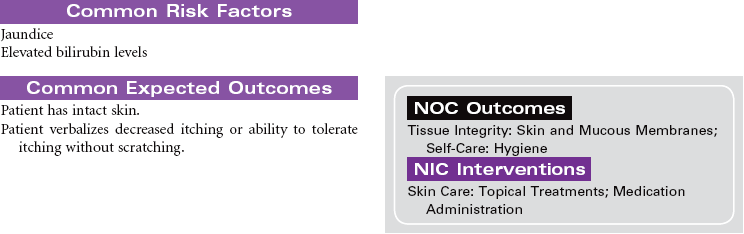
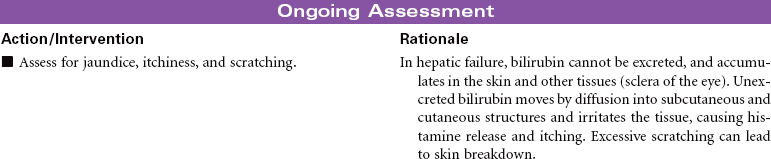
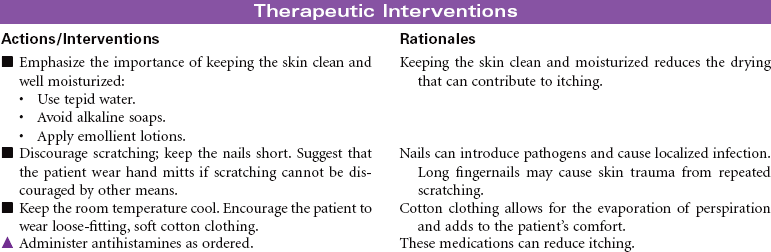
Cirrhosis
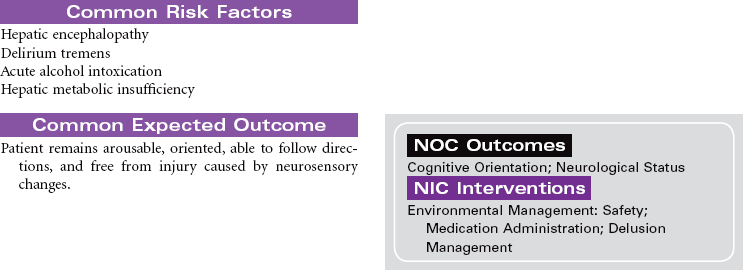
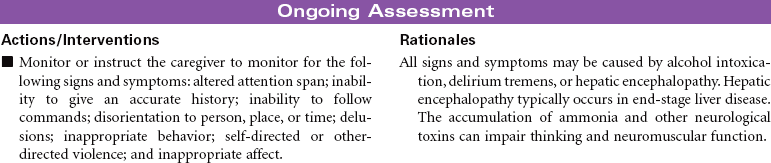
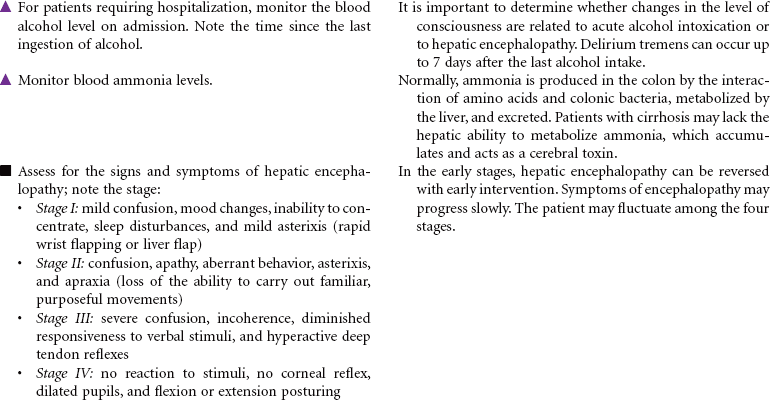
Laënnec’s Cirrhosis; Hepatic Encephalopathy; Ascites; Liver Failure
Cirrhosis is a chronic and progressive inflammatory disease of the liver. The inflammatory process results in irreversible fibrosis and scarring of hepatic tissue. The scarring produces changes not only in the size and shape of the liver but also in its function and blood flow. Worldwide the most common cause of cirrhosis is viral infection such as hepatitis B and C. Alcohol abuse is the primary cause of Laënnec’s cirrhosis. Other causes include biliary obstruction, prolonged right-sided heart failure, and metabolic defects such as alpha-1 antitrypsin deficiency. The incidence of cirrhosis is highest in men between 40 and 60 years old. The development of cirrhosis occurs over many years before the person presents with characteristic symptoms. Malnutrition contributes to the development of cirrhosis in people who abuse alcohol. The disruption of hepatic function in cirrhosis can lead to the development of end-stage liver disease with ascites, portal hypertension, hepatic encephalopathy, and liver failure.


Colorectal Cancer
Large Bowel Cancer; Rectal Cancer; Bowel Resection; Hemicolectomy; Colectomy
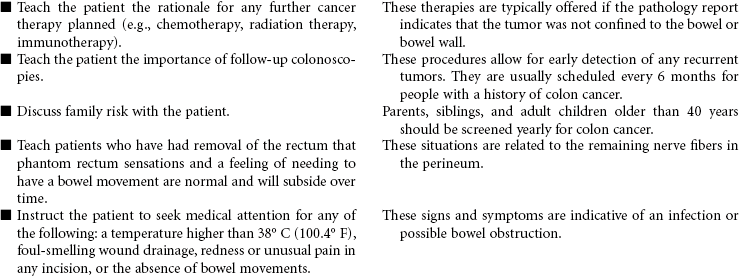
Colorectal cancer is the second most common cancer death in the United States. Colon cancer occurs more often than rectal cancer. Risk factors for colorectal cancer include familial polyposis, family history of colorectal cancer, and a personal history of colorectal cancer, colorectal polyps, or chronic bowel inflammatory disease. Other risk factors include physical inactivity, obesity, and a diet that is high in fat and low in fiber, smoking, and alcohol consumption. Overall, men and women are affected about equally. Early colorectal cancer often has no symptoms, which is why screening is so important. Most colorectal cancers begin as a polyp, a small growth in the wall of the colon. However, over time some polyps grow and become malignant. Signs of colorectal cancer include bleeding from the rectum, blood in the stool or in the toilet after having a bowel movement, a change in the shape of the stool, cramping pain in the lower stomach, and a feeling of discomfort or an urge to have a bowel movement when there is no need to have one. The tumor, node, metastasis (TNM) staging system indicates tumor depth, node involvement, and presence of tumor metastasis, which have been shown to be the most significant variables in determining the prognosis of colon cancer. Colorectal cancer may metastasize through direct extension to adjacent tissues or by hematological-lymphatic spread. Surgical removal is the preferred treatment for colorectal cancer, although irradiation may be used preoperatively. Postoperative chemotherapy has proven beneficial in treatment of colon cancer. Irradiation and immunotherapy are used, but with limited success. This care plan addresses the preoperative stage, care of the patient who has undergone colon resection, and self-care teaching.

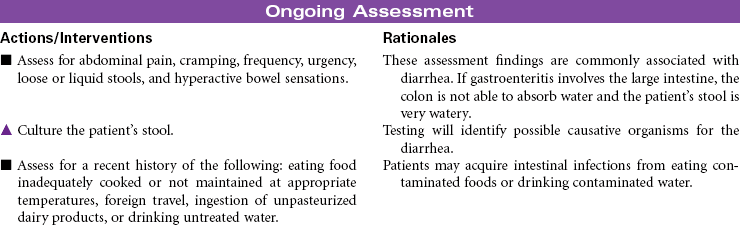
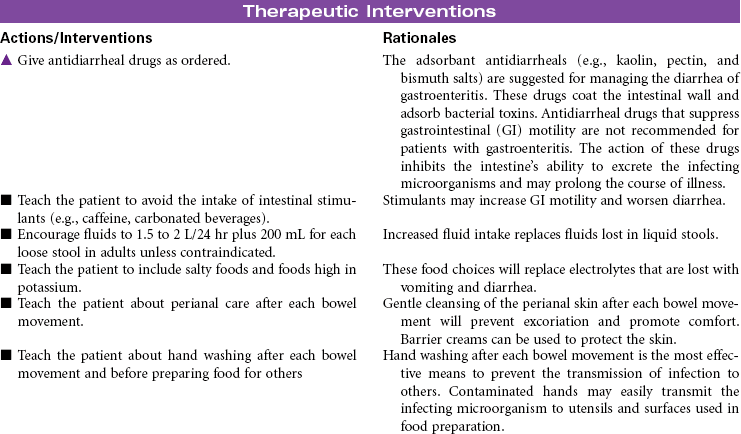
Gastroenteritis
Food Poisoning; Stomach Flu; Traveler’s Diarrhea
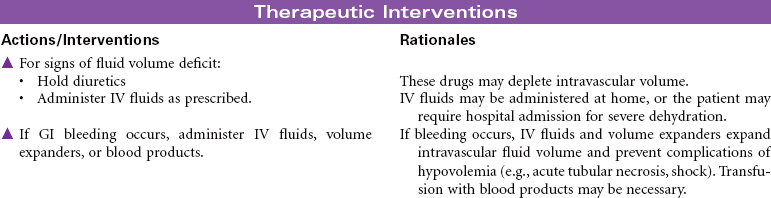
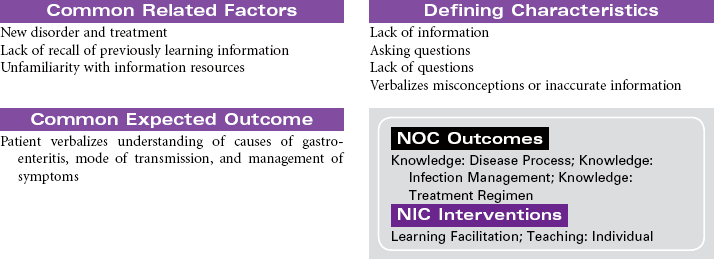
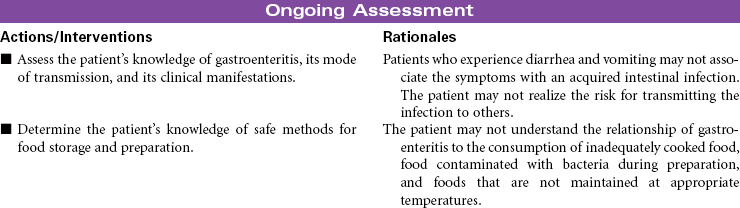
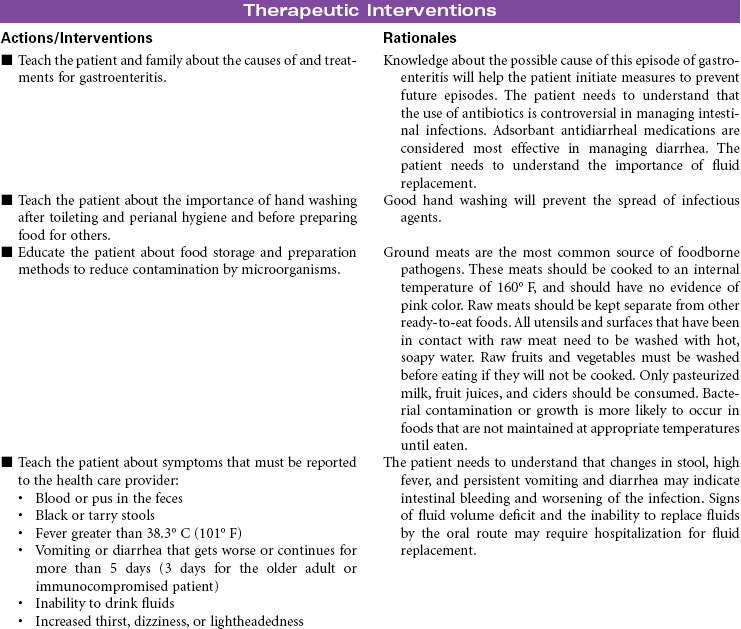
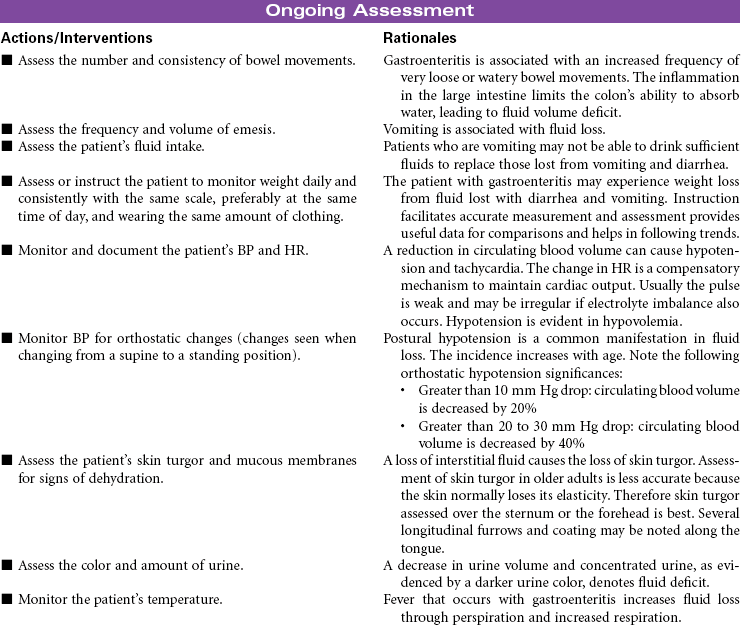
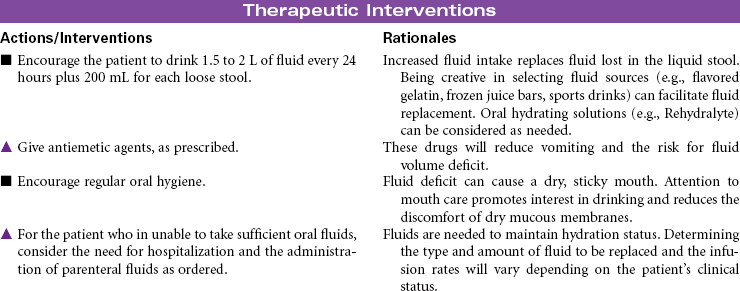
Gastroenteritis is the inflammation of the stomach and small intestine. The most common cause of this disorder is infection acquired from consuming contaminated food or water. A wide variety of viruses, bacteria, and parasites are associated with gastroenteritis. Viral gastroenteritis is often called stomach flu but it is not caused by the influenza virus. This form of gastroenteritis is very contagious. Food-borne gastroenteritis, often called food-poisoning, is associated with specific strains of bacteria such as Escherichia coli (e.g., O157:H7), salmonella, campylobacter, and clostridium (e.g., perfringens and botulinum), in addition to viruses and parasites. The ingestion of foods contaminated with chemicals such as mercury or the ingestion of plant toxins such as those found in certain types of mushrooms have been known to cause gastroenteritis. The clinical manifestations that occur in the patient with gastroenteritis include nausea, vomiting, diarrhea, fever, and abdominal pain. The disorder is usually self-limiting, with the resolution of symptoms in a week to 10 days. Symptom management and the prevention of recurrence is the focus of treatment for patients with gastroenteritis. Hospitalization may be required for patients who develop fluid volume deficit as a result of the vomiting and diarrhea. This care plan focuses on the initial treatment in a nonacute care setting.


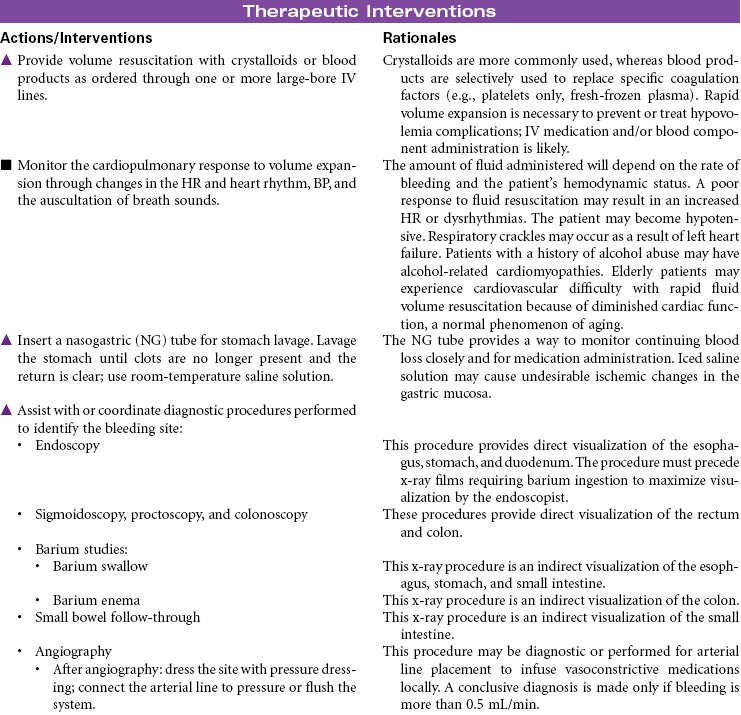
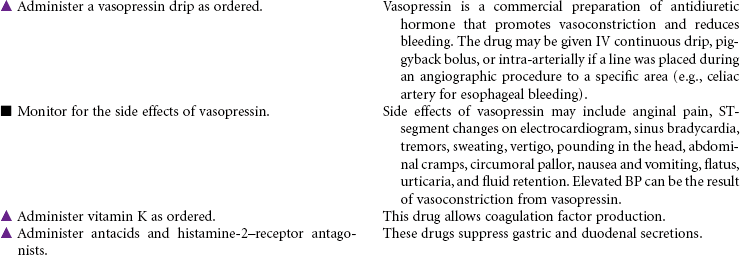
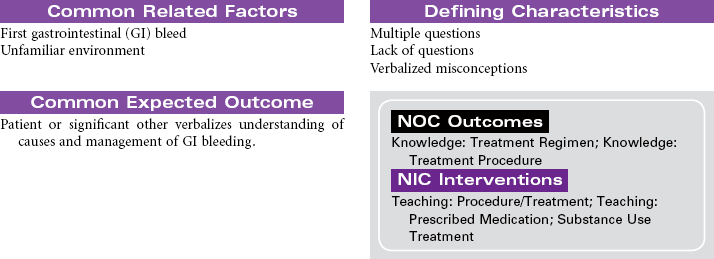
Gastrointestinal Bleeding
Lower Gastrointestinal Bleed; Upper Gastrointestinal Bleed; Esophageal Varices; Ulcers
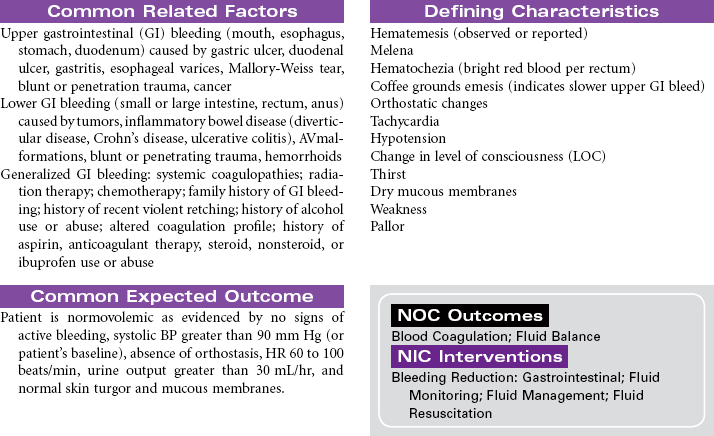
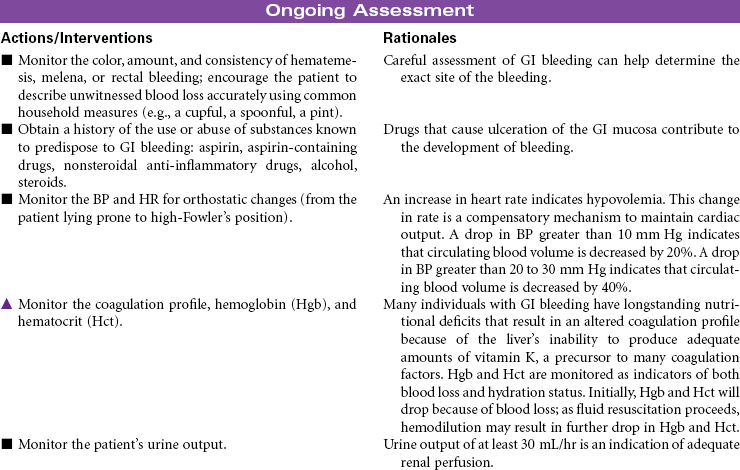
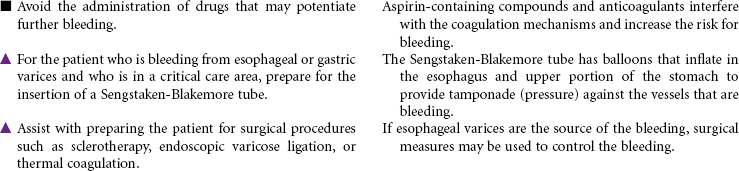
Loss of blood from the gastrointestinal (GI) tract is most often the result of erosion or ulceration of the mucosa, but it may also be the result of arteriovenous (AV) malformation or malignancies, increased pressure in the portal venous bed, or direct trauma to the GI tract. Alcohol abuse is a major etiological factor in GI bleeding. Varices, usually located in the distal third of the submucosal tissue of the esophagus or the fundus of the stomach, can also cause life-threatening GI hemorrhage. Upper GI bleeding may manifest as blood tinged, bright red, or coffee grounds emesis. The patient with upper GI bleeding may also experience dark, tarry stools. Lower GI bleeding may occur as bright red blood from the rectum. This type of bleeding is often associated with the presence of hemorrhoids. Tumors of the colon may cause bleeding detected as occult blood in the feces rather than visible bleeding. Inflammatory bowel disease may cause lower GI bleeding characterized as bloody diarrhea. Factors that alter coagulation or cause generalized inflammation of the intestinal mucosa can contribute to bleeding anywhere in the GI tract. Treatment may be medical or surgical or may involve mechanical tamponade. Acute GI bleeding may be life threatening without prompt treatment. In patients with GI bleeding, stabilization of BP and restoration of intravascular volume is the highest priority. The focus of this care plan is the acute hospital management phase of a patient with active GI bleeding.

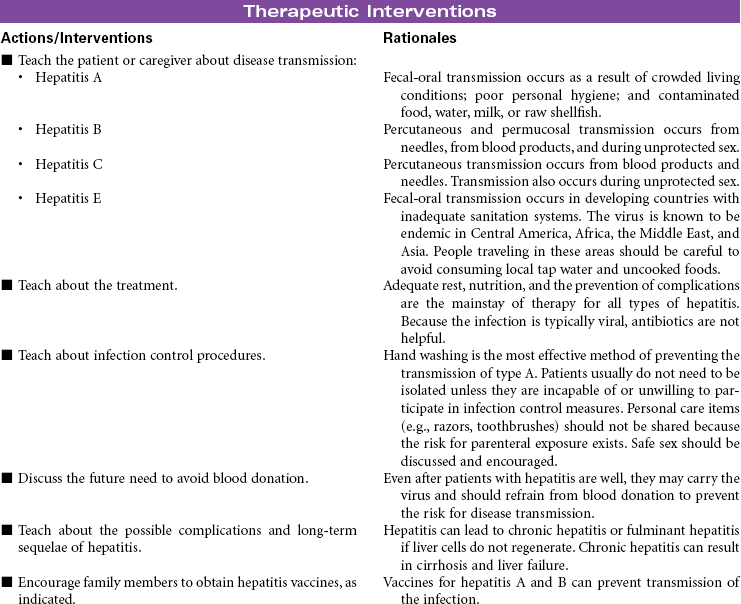
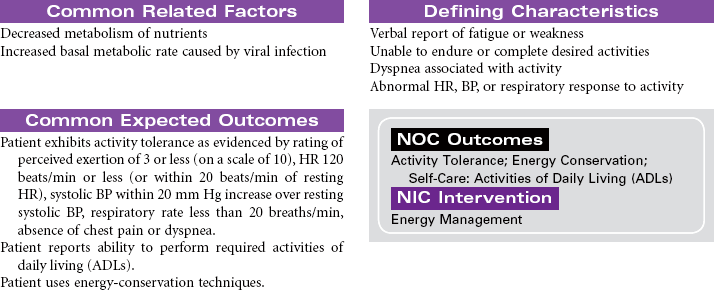
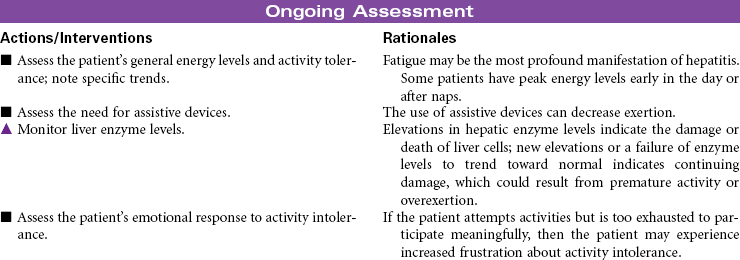
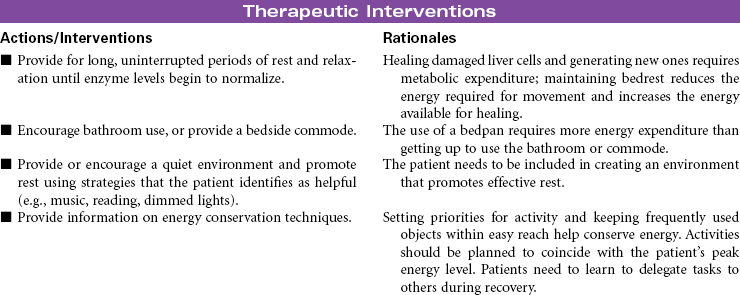
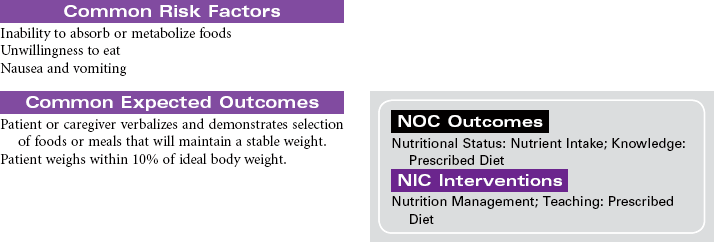
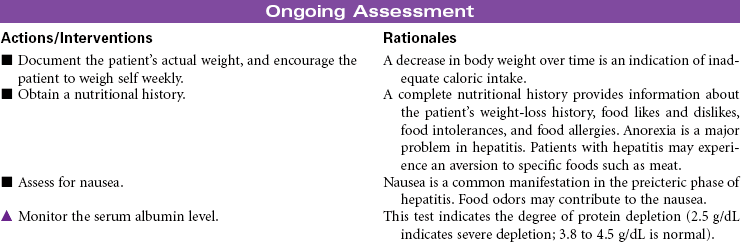
Hepatitis
Serum Hepatitis; Infectious Hepatitis; Viral Hepatitis
Hepatitis is inflammation of the liver, usually caused by a virus. Hepatitis may also result from adverse drug reactions or ingestion of other chemicals. Hepatitis may develop in response to viral infections with rubella, varicella, Epstein-Barr, cytomegalovirus, and herpes simplex virus. Viral hepatitis types A and E are transmitted via the fecal-oral route or through poor sanitation; person-to-person contact; or consumption of contaminated food, water, or shellfish. Hepatitis E infections are associated with contaminated water and occur most commonly in developing countries. Cases of hepatitis E in the United States are seen in patients who have traveled to areas in which the virus is endemic. There is no specific treatment for this form of hepatitis, and immune globulin is not useful in prophylaxis after exposure. Types B and C (formerly called non-A, non-B) are transmitted by blood, semen, and vaginal secretions. These types of hepatitis are often classified as sexually transmitted infections. They also can be transmitted via contaminated needles and renal dialysis (parenterally) or through intimate contact with carriers. Hepatitis B and C may progress to a chronic active form of the disease. As a result, the patient is at risk for liver failure that may require liver transplantation. Hepatitis D occurs only in the presence of hepatitis B. Hepatitis D develops as a co-infection or superimposed infection with hepatitis B. A co-infection with hepatitis D tends to increase the severity of the hepatitis B infection. Hepatitis G is not common but may exist in patients with other viral infections such as hepatitis B or C and human immunodeficiency virus (HIV). Vaccine for the prevention of hepatitis B is widely available. The Occupational Safety and Health Administration requires that employers offer the hepatitis B vaccine to health care workers, who are at risk for all types of hepatitis. A vaccine is also available for hepatitis A, although its use is not as widespread as hepatitis B vaccine. Some cases of hepatitis remain subclinical, and most are managed in the home. Fulminant hepatitis can result in massive destruction of liver tissue and can be fatal. This care plan addresses nursing concerns that may be managed in the hospital or at home.



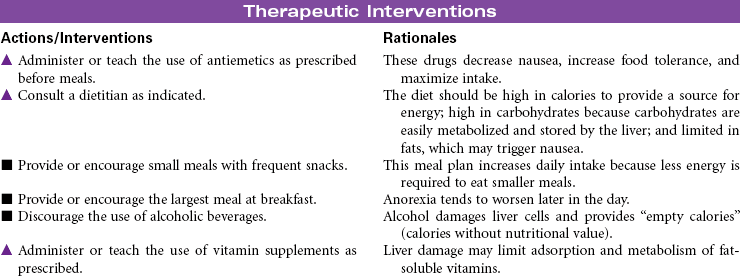
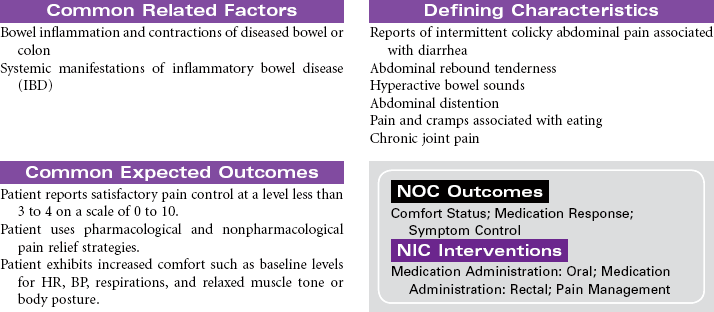
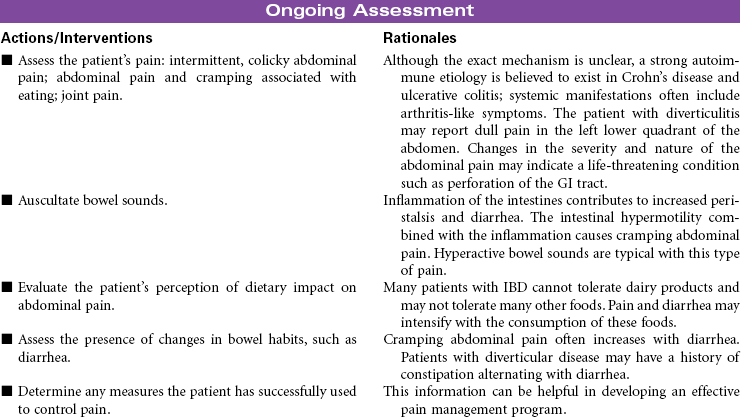
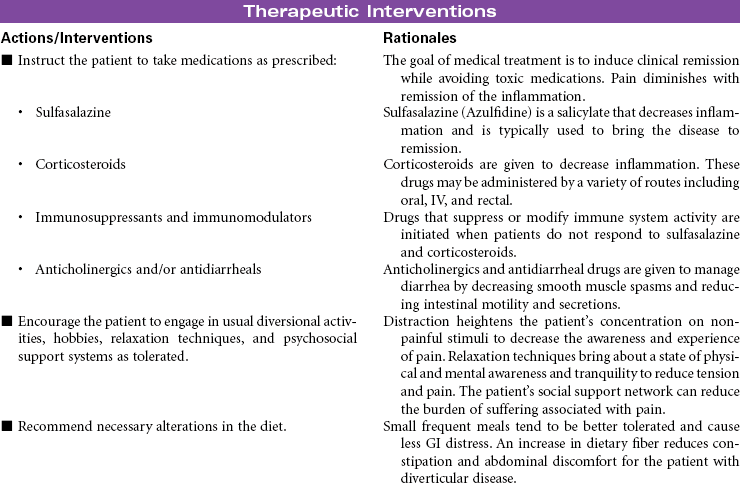
Inflammatory Bowel Disease
Crohn’s Disease; Ulcerative Colitis; Diverticulitis
Inflammatory bowel disease (IBD) refers to a cluster of specific bowel abnormalities whose symptoms are often so similar as to make diagnosis difficult and treatment empirical. Crohn’s disease is associated with involvement of all four layers of the bowel and may occur anywhere in the gastrointestinal (GI) tract, although it is most common in the small bowel at the terminal ileum. Ulcerative colitis occurs only in the colon and involves the mucosal and submucosal layers. Cause is unknown for both diseases, but a familial history of IBD is found in patients who develop Crohn’s disease and ulcerative colitis. Specific genetic mutations have been identified in people with Crohn’s disease. The incidence of Crohn’s disease is higher in people of Ashkenazi Jewish heritage than other ethnic groups. Incidence is usually in the 15- to 30-year-old age-group. Both Crohn’s disease and ulcerative colitis are associated with the development of diarrhea and nutritional deficiencies. Systemic manifestations can involve the liver, joints, skin, and eyes. Diverticulitis is inflammation of a diverticulum in the colon. The diverticulum is a herniation of the mucosal layer of the colon through the muscle layer. Obstruction of the diverticulum with hardened fecal material or undigested food particles causes the inflammation. Diverticular disease often occurs in people older than 40 years of age; it seems to be etiologically related to high-fat, low-fiber diets and occurs almost exclusively in the colon. IBD is treated medically. Bowel diversion surgery may be indicated if medical management fails or if the patient develops complications. This care plan focuses on chronic, ambulatory care.


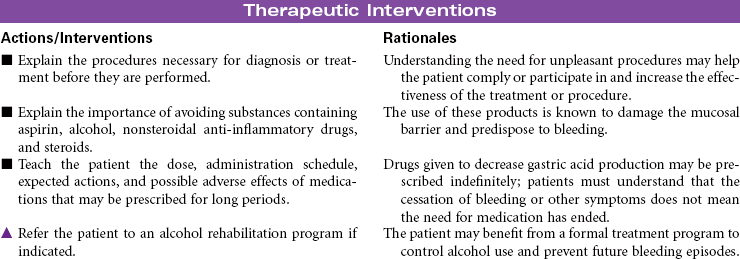
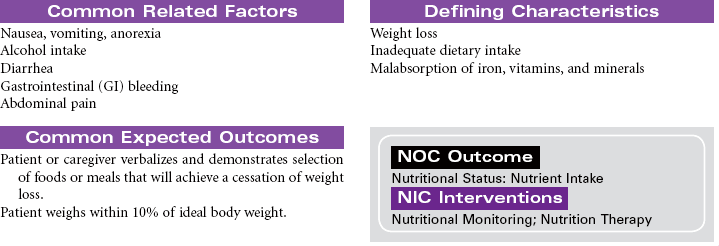
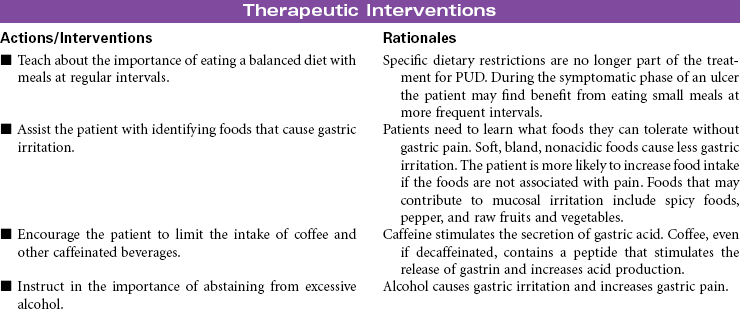
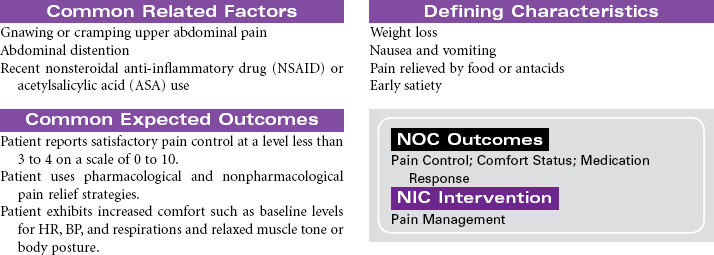
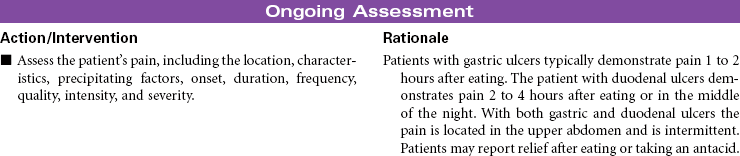
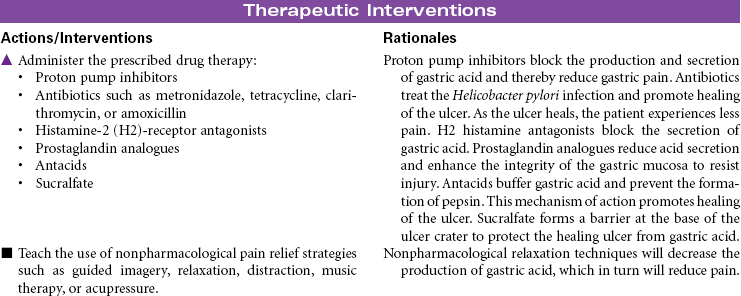
Peptic Ulcer Disease
Duodenal Ulcers; Gastric Ulcers; Stress-Induced Ulcers
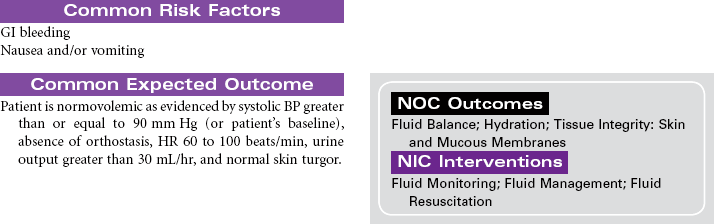
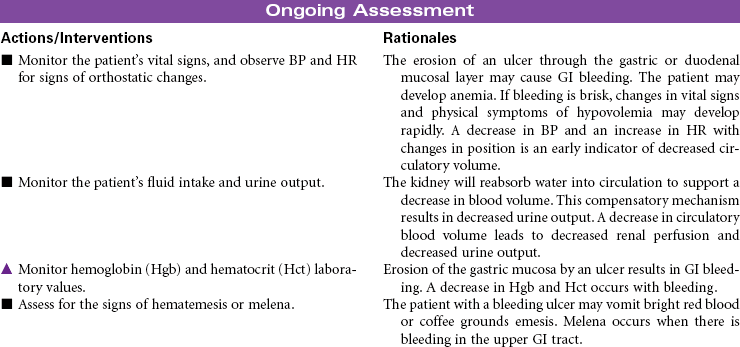
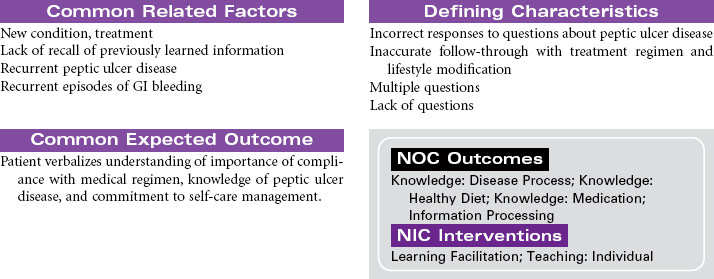
Peptic ulcer disease (PUD) is characterized by mucosal erosions or ulcers that develop from a weakening in the lining of the mucosa that surrounds the upper gastrointestinal (GI) tract. These ulcerations may develop in the lower esophagus, stomach, or duodenum. PUD can be caused by hyperacidity, pepsin, bile salts, ischemia, aspirin, and nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs cause a weakening in the lining of the GI tract by decreasing the protective function of the mucosal layer. This decrease in the protective layer is attributed to the inhibition of cycloxygenase-1 (COX-1) by the NSAIDs. Prostaglandins stimulate the secretion of mucus and bicarbonate, which helps in making the mucosa more resistant to acid penetration. Prostaglandins also increase mucosal blood flow and play a role in healing. Helicobacter pylori is a common cause of duodenal ulcers, although the mechanism is not fully understood. Current evidence suggests that the bacteria produce enzymes that cause direct injury to the mucosal lining. Indirectly, the bacteria stimulate release of hydrogen ions that increase acidity and further contribute to mucosal erosion. Gastric ulcers develop when the protective mucosal layer becomes more permeable to hydrogen ions. This type of ulcer is associated with bile reflux and use of NSAIDs. Other factors that contribute to the development of PUD include altered gastric emptying (delayed or too rapid), bile reflux through an incompetent pyloric sphincter, or increased stress associated with critical illness, surgery, or acute trauma. Stress-induced ulcers are thought to be caused by the effects of elevated cortisol levels as part of the normal stress response. Increased serum cortisol impairs the rate of mucosal cell replacement. Ulcerative or erosive diseases in the upper GI tract can cause GI bleeding, abdominal pain, anorexia, nausea and vomiting, or diarrhea.




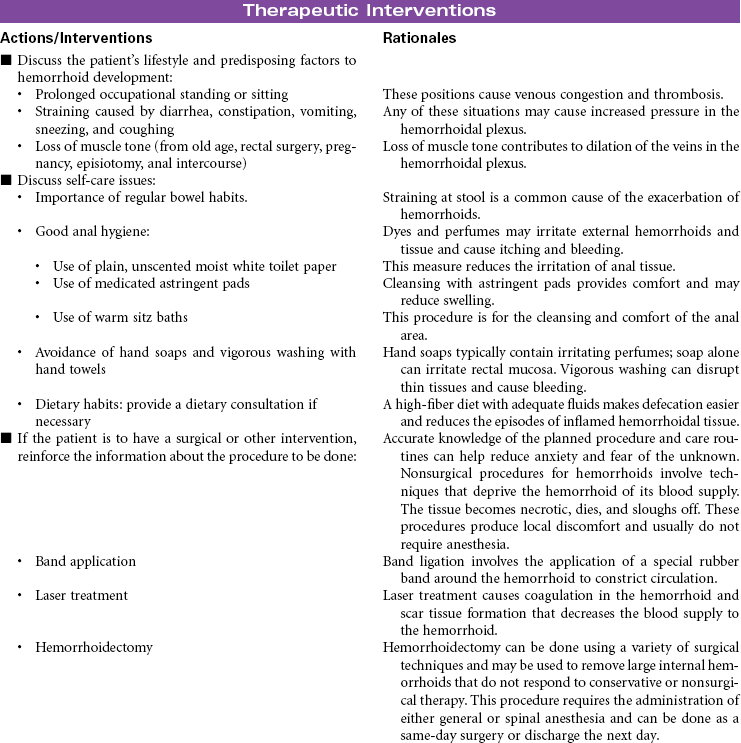
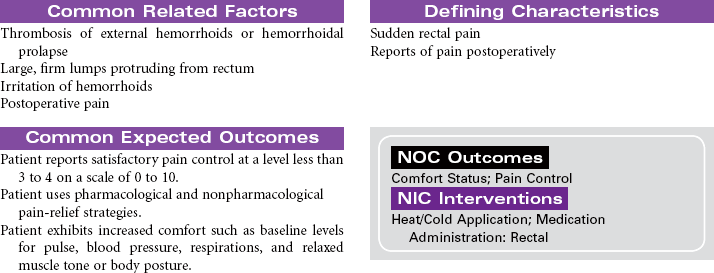
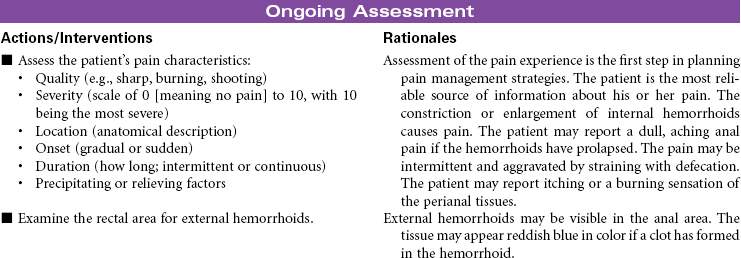
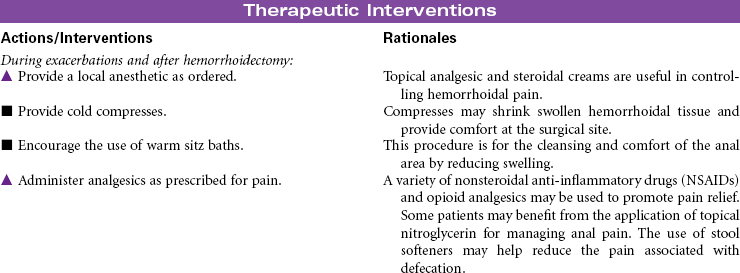
Hemorrhoids/Hemorrhoidectomy
Hemorrhoids are varicosities of veins in the rectal mucosa usually caused by the combined effects of shearing force and increased intra-abdominal pressure. Straining with defecation produces the shearing force that weakens muscles that support the rectal tissues. Prolonged or repeated increased pressure results in permanent dilation of the veins in the perianal area. Factors contributing to the development of hemorrhoids include chronic constipation, obesity, pregnancy, prolonged sitting or standing, and portal hypertension. Internal hemorrhoids develop in veins above the internal rectal sphincter. External hemorrhoids develop below the anal sphincter and are visible around the anus. Symptoms of hemorrhoids include local protrusion and swelling, discomfort related to protruding or swollen masses, and bleeding that may be significant enough to cause anemia. All patients with rectal bleeding should have a sigmoidoscopy for complete evaluation. Internal hemorrhoids are more likely to bleed than external hemorrhoids. Initial treatment for hemorrhoids should be conservative, including stool bulking (adequate intake of fiber and water) and topical treatment with ointment and suppositories. Nonsurgical removal of internal hemorrhoids may include band ligation or laser therapy. Hemorrhoidectomy is indicated for surgical removal of large internal hemorrhoids. This procedure may be done when internal hemorrhoids cause excessive bleeding or prolapse.
Pancreatitis, Acute
Pancreatitis is an inflammatory disorder of the pancreas that results in the self-destruction of the pancreas by its own enzymes, causing varying degrees of edema, necrosis, and hemorrhage. Activation of these proteases and lipases before they are excreted into the intestine causes inflammation and damage to the pancreatic tissue. The mechanism responsible for causing this abnormal enzyme activity in the pancreas is unknown. The patient may develop jaundice from obstruction of the common bile duct by an edematous pancreas. Damage to insulin-secreting cells of the pancreas produces episodes of hyperglycemia. The two most common causes are alcohol abuse and biliary obstruction by gallstones. The disease is equally common in middle-aged men and women. The highest incidence occurs in African Americans compared to those of other ethnic or racial backgrounds. In severe cases, pancreatitis can be life-threatening, as a result of hypovolemic shock, septic shock, or acute respiratory distress syndrome. Repeated episodes of acute pancreatitis can lead to the development of chronic pancreatitis and diabetes mellitus. The focus of this care plan is the care of the acutely ill person with pancreatitis.