Physical examination
At the end of the subjective examination it is often important to first summarize the main information of the interview, to clarify open questions and to find agreement with the patient on activity limitations which need to be rehabilitated and coping strategies regarding pain control.
The subsequent physical examination should be considered and communicated as the examination of movement impairments which often, but not always, are prerequisites to the restoration of optimum functional capacity. From a clinical reasoning perspective the physical examination is one of the stages in the therapeutic process in which hypotheses may be confirmed and/or modified.
Planning the physical examination procedures
As already stated, regular planning in critical phases of the therapeutic process is essential to comprehensive clinical practice. Regular planning may have become an automatic, implicit process for the more experienced MSK-physiotherapist, as they will be able to ‘reflect in action’ more frequently (Schön 1983). However, novices may actively enhance their path to professional expertise if they explicitly go through reflection and planning phases after having performed certain procedures of the physiotherapy process (‘reflection on action’). In this learning process it is essential not only to document the results of examination procedures and therapeutic interventions, but also to record the reflections and the planned procedures.
After completion of the subjective examination, it is often useful to summarize its main points and the goals of treatment agreed with the patient so far. It may also be necessary to explain to the patient the objectives of the next stage of the initial assessment – the physical examination.
Planning after the subjective examination as a preparation for the physical examination has three phases:
• Reflection on the subjective examination process – the physiotherapist needs to verify that the subjective examination is sufficiently complete in order to be able to perform a comprehensive physical examination, respecting precautions and contraindications, as well as performing subjective reassessment procedures in subsequent sessions (see Reflection on the subjective examination process, below).
• Expressing hypotheses which will influence the physical examination process. Hypotheses regarding pathobiological mechanisms, sources, contributing factors, precautions and contraindications and management in particular need to be made explicit (see Hypotheses, below).
• Planning the procedures of examination, including anticipation on possible findings, the kind of examination (dosage or extent of examination procedures), sequence of testing and reassessment procedures (see Planning of the physical examination procedures, below).
Precautions to examination procedures
Hypotheses with regard to precautions and contraindications to physical examination and treatment procedures serve to determine the extent of the physical examination that can be safely undertaken. Furthermore, they aid in the decision if contraindications to examination procedures or treatment interventions are present.
The precautions and contraindications are mostly determined by hypotheses with regard to pathobiological processes and neurophysiological pain mechanisms and may include the following factors:
Physical examination and the lumbar spine
Physical examination procedures should follow a structured, integrated format, but they should be flexible enough to be individualized to the patient's needs. This includes precautions to the test-procedures as well as the patient's preferences to move. Sometimes a phenomenological perspective with salutogenic approach to examination may be more beneficial than a therapist-directed approach to testing (see Chapters 1 and 2 of Volume 2 and Chapter 8 of this volume).
The scope of practice of a physiotherapist is reflected in the examination procedures. Making a movement diagnosis is a key issue, rather than making a structural diagnosis (although this hypothesis of pathobiological is an important element in clinical reasoning) and to design examination around safety, interventions and outcomes. In cases where the pain and disability are based on peripheral nociceptive and/or neurogenic processes, one of the goals of examination procedures will be reproduction of the patient's symptoms. However, other information regarding motor control patterns, habitual movement patterns, joint-position sense and proprioceptive feedback, as well as neurological conduction tests, may also be integrated into the examination procedures.
During the physical examination process, it needs regular phases of ‘brief appraisal’, in which the therapist reflects on the findings so far and if the examination procedures can be carried on as planned, or if they have to be adjusted and adapted to the patient's situation.
The physical examination should aim to confirm the hypotheses established through clinical evidence gathering in the subjective examination.
The main aim therefore, using movement analysis and manual examination, is to establish:
• The level of functioning of the movement system, including an impression of the movement potential
• The movement impairments and evidence for the need for movement therapy interventions
• Measures of the effectiveness of such interventions [P/E ASTERISKS***]
• Patient's confidence to move, at times in spite of the pain.
Specific aims of the physical examination should include (Higgs et al. 2008):
• Reproduce the patient's symptoms
• Find comparable signs-adaptive, protective, restrictive
• Find the source/cause of the source/contributing factors
• Establish components, mechanisms, dimensions for each symptom area
• Identify movement impairments (range, symptom response, quality of movement)
• Establish functional activity limitations
• Examine relative to the severity, irritability and nature of the symptoms (movement to P1 or limit with overpressure if necessary)
• Screen other potential components, predisposing factors
• Carry out special testing where appropriate
• Establish the role and desired effects of mobilization/manipulation.
Physical examination procedures place an emphasis on range, symptom response and quality of movements. They are mainly, but not exclusively, impairments based. However, functional demonstration tests may encompass all activities from daily life, which patients have been avoiding.
It is essential to link the therapeutic interventions to the physical examination findings, expressed in reassessment procedures after the application of the intervention. Furthermore, they need to be linked to the results from the subjective examination, which usually are compared at the beginning of subsequent sessions.
Table 6.8 provides an overview of the general test procedures related to the examination of the lumbar spine and related structures. It should be noted that reassessment procedures are part of the overall physical examination, even if not all planned tests may have been performed. If there is a pain sensation at the beginning of the physical examination (‘present pain’), this needs to be reassessed regularly to ascertain whether this present pain is changing as a result of, for example, active tests. Furthermore, it is possible that examination procedures, e.g. for accessory movements of the spine, may have a therapeutic effect, which has to be evaluated before, for example, hip movements are passively examined.
Table 6.8
Possible physical examination procedures of the lumbar spine and associated movement components
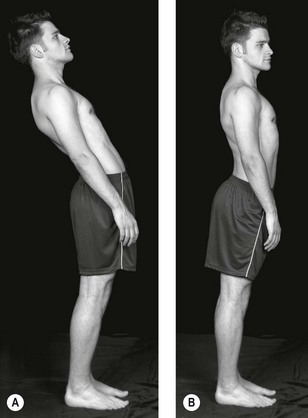
Observation
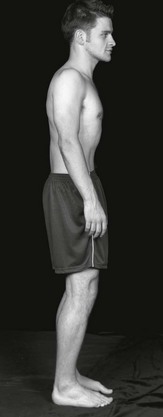
Observing the patient in a variety of positions and a variety of views while standing, sitting and/or lying will enable the clinician to start to identify structural faults, signs of impairment such as wasting or bruising, adaptive and protective mechanisms resulting in postural asymmetry, balance and alignment of body parts, including common faults associated with the risk of developing low back pain (such as sway back, flat back and kypholordosis).
• Furthermore, the therapist gains an impression about the willingness and confidence to move.
• The therapist's in-depth knowledge of alignment, pelvis neutral position, neutral zone, tone etc. will enhance an ability to recognize motor control faults, which could be contributing to deficits in movement (Sahrmann 2011)
• Present pain: any symptoms at resting postures need to be established before embarking on active examination procedures
• Correction of faults will clarify whether or not these faults are related to the current patient's symptoms. With the reproduction of symptoms on correction, the posture can be considered as an antalgic posture or protective deformity. See pelvic shift correction in Figure 6.4.
Functional demonstration
Functional demonstration testing may serve different purposes:
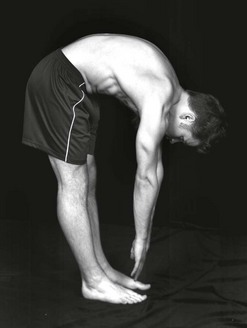
• The patient will often be able to demonstrate a movement or activity, involving the lumbar spine, which reproduces his symptoms. This may be a daily activity that he knows hurts his back, such as bending forwards to tie his shoelaces. He may also be able to demonstrate the movement he was doing when his back was strained – for instance, a backhand at tennis. By asking the patient to demonstrate such an activity to the onset on pain (P1), or to the limit, the therapist can analyze the range of movement, symptom response and quality of movement. This test movement may serve as a parameter (‘asterisk’) for reassessment procedures.
• Differentiation at this stage may help to confirm the movement components at fault if there is any doubt. For example, the patient may be able to reproduce his left buttock pain by demonstrating the backhand tennis shot that injured him. This movement principally involves rotation of the spine and hip. By using the lumbar spine/ hip differentiation test involvement of the spine rather than the hip may be revealed (or vice versa) (Fig. 6.5).
• Further brief appraisal of the spine with active movements and hip with for example the observation of squatting and one-leg hip extension will confirm the need to examine the spine or hip in more detail. Treatment should then reinforce the initial hypothesis.
Further differentiation of the functional demonstration or injuring movement may be of value when improvement has slowed or stopped. For example, after several sessions of treatment, the patient may have to stretch a lot further into the backhand shot to reproduce his pain. Further differentiation may reveal that lumbar extension and lateral flexion to the painful side adds to the buttock pain being reproduced by rotation of the spine during the backhand shot. Therefore a lumbar rotation treatment technique in lumbar extension and ipsilateral lateral flexion will be a valuable technique as a progression of treatment.
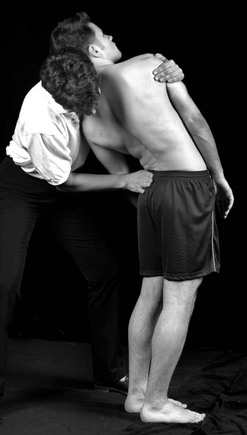
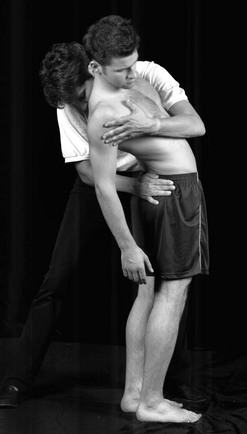
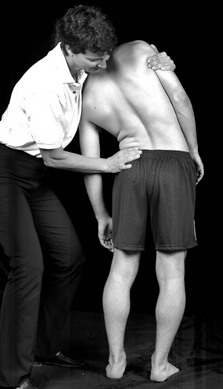
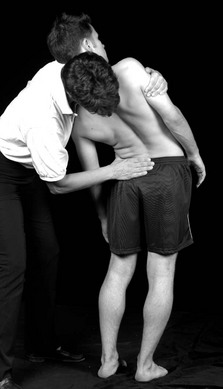
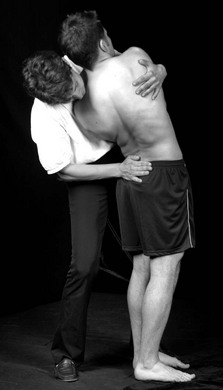
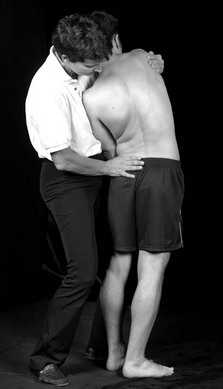
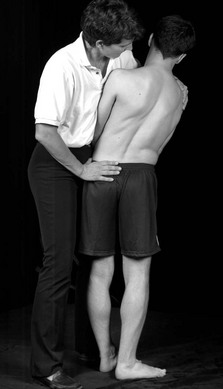
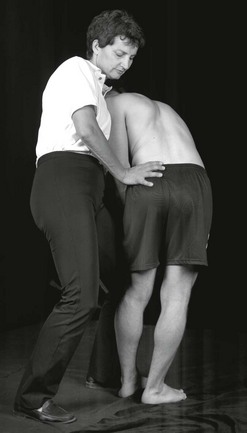
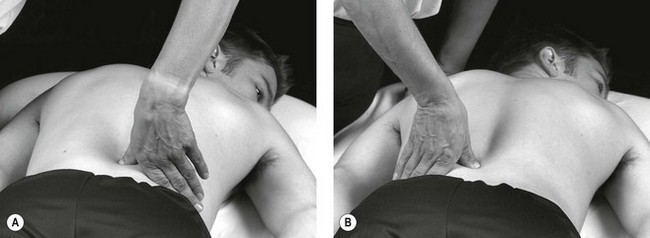
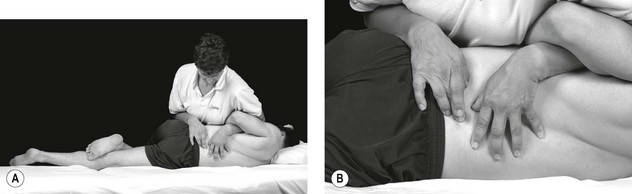
Pelvic shift correction
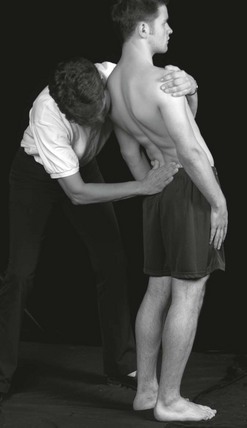
Patient starting position: patient presents with pelvic shift to right / trunk list to left
Therapist starting position: standing at patient's left side
Localization of forces: both forearms dorsally and ventrally of pelvis with hands on patient's right iliac crest; therapist's shoulder/ clavicle supports patient's left arm in patient's side
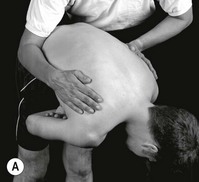
Correction a. Therapist pulls patient's pelvis towards herself. Observe range, quality of movement and symptom-response (Fig. 6.4A).
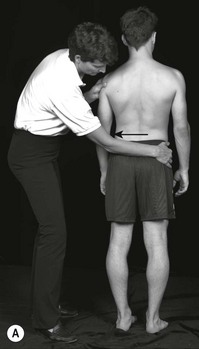
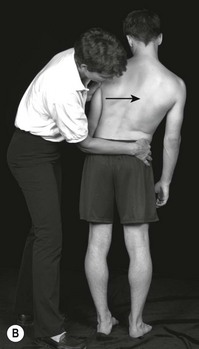
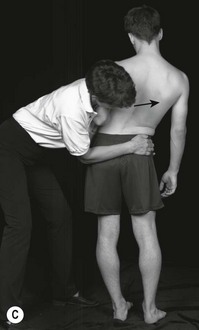
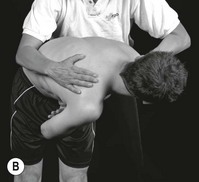
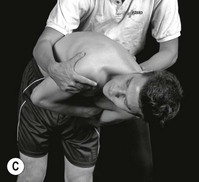
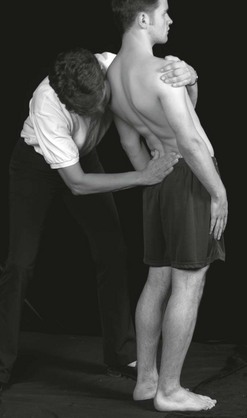
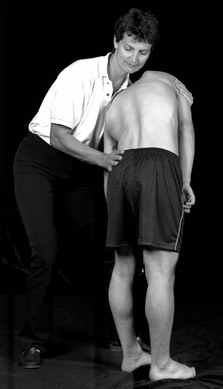
Figure 6.4 A Pelvic shift correction to the left; B Trunk list correction to the right; C Combination of pelvic shift to the left and trunk list to the right.
Correction b. Therapist pushes patient's trunk away from herself. Observe range, quality of movement and symptom-response (Fig. 6.4B)
Correction c. As a progression of testing: combination of (a) and (b) (Fig. 6.4C).
Remarks: the therapist ensures that with each hand an equal force is applied. The trunk/pelvis have to move in a horizontal line (avoid sideflexion to the right).
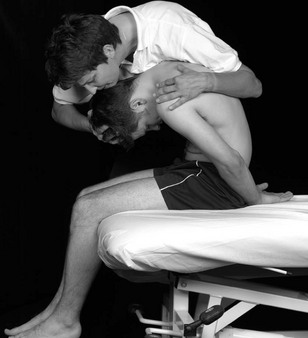
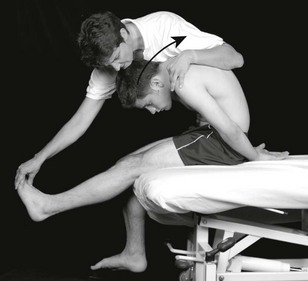
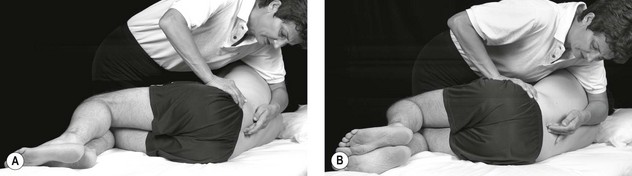
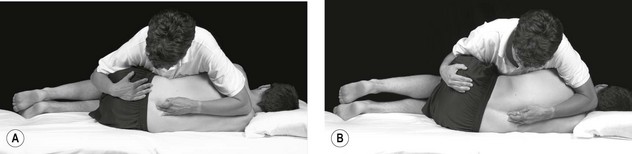
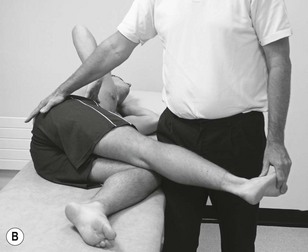
Lumbar spine/hip differentiation test
rotation
Patient starting position: standing, twisting the trunk to right until the onset of pain (symptom reproduction), then – if possible – balances on the right leg (refer to Fig. 6.5A and B)
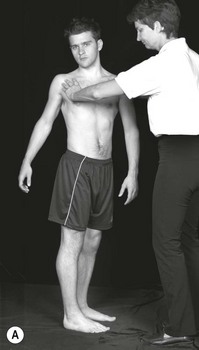
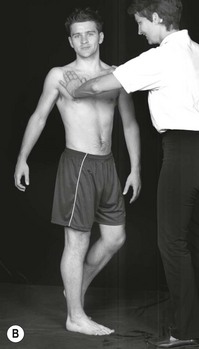
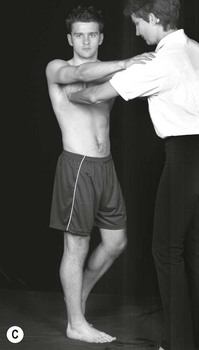
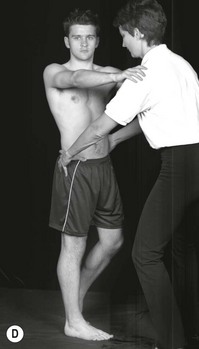
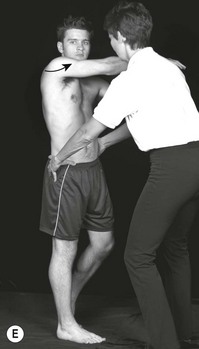

Figure 6.5 A Differentiation test, spinal and peripheral joint pain, part 1. A Rotation to the right. B Patient balancing on right leg and over-pressure added; C Patient balanced; D Stabilizing the pelvis; E Retaining hip rotation and releasing lumbar rotation; F Part 2: retaining released lumbar rotation and increasing hip rotation.
Therapist starting position: in front of patient.
• Patient places both hands on both shoulders of therapist for balance (refer to Fig. 6.5C)
• Therapist stabilizes patient's pelvis with both hands (refer to Fig. 6.5D).
Step 1: Patient derotates lumbar spine, by moving right hand from the left shoulder to the right shoulder of the therapist (refer to Fig. 6.5E) – therapist maintains pelvis in position to prevent rotation
Step 2: Patient's hands again on both shoulders of therapist: patient is asked to move the right hand further into right trunk rotation (therapist stabilizes pelvis)
Step 3: Patient's hands again on both shoulders – ensure that the pain is still reproduced. Therapist moves patient's pelvis into further right rotation: this increases hip rotation, decreases lumbar rotation (refer to Fig. 6.5F)
Step 4: As step 3, therapist moves patient's pelvis towards left rotation – thus releasing hip rotation and increasing lumbar rotation.
Active tests lumbar spine
Active testing of the lumbar spine includes flexion, extension, rotation and sideflexion of the trunk.
Initially the gross spinal range and pain response to the movement should be noted. Furthermore it is important to notice the quality of the local intervertebral movement and the pain response. These three aspects serve as parameter for reassessment-procedures (‘asterisks’).
If, for example lateral flexion is limited, the statement may be recorded that the limitation occurs mainly from L3 downwards. Watching the movements from these two aspects (i.e. the gross movements and the local movements) can be likened to taking a photograph with a wide-angle lens for the gross movement, and a second movement using a telephoto lens to highlight the localized limited movement.
However, if these movements do not reproduce any symptoms of the patient, additional stress may be added to the movement, as for example:
• Applying overpressure at the end of the available active ROM. Frequently more range will be gained, when the structures are moved further into the movement in a passive or assisted active way. Overpressure should be applied in a light oscillatory manner, while progressing further into the end of the range of the movement. Any symptom-response by the patient as well as the quality of the resistance perceived by the therapist has to be noted:
 overpressure may be applied to the overall movement
overpressure may be applied to the overall movement
overpressure may be applied locally to the intervertebral segments in E, LF and/or rotation.
• Application of the movements F, E, LF or Rot:
repeated: do the symptoms increase? Then the movement serves as a parameter for reassessment procedures
do the symptoms decrease with the repetition of the movement? Then the movement may be adapted to serve as a self-management exercise to control the pain
moving from one extreme position to the other. This is frequently useful in later treatment sessions, to check if the structures have been cleared sufficiently
sustained: maintaining the movement into end-of-range position, with a slight overpressure. This test variation may be particularly helpful in those cases, where symptoms occur only in sustained daily life positions.
• Most movements of the trunk in lumbar spine testing occur from a cephadad to caudad direction. However, at times it is more informative to test the movements from caudad to cephadad upwards
• Combination of movement directions. These combinations may give almost endless variations, as two directions, three movement directions may be combined. In some exceptional cases even an accessory movement has to be applied to the movement combination, before symptoms may be reproduces.
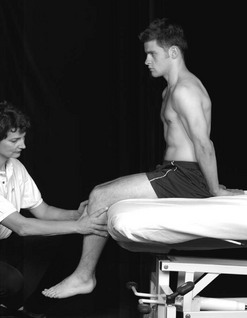
• Changing position of the patient: some symptoms may only be reproduced if the tests are being performed while the patient is sitting or lying.
The active tests, including a selection of test variations, are described below.
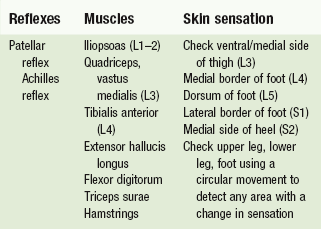
Neurological conduction testing
Neurological conduction testing is the manual testing of reflexes, muscle reactivity and skin sensation to support in clinical decision-making processes.
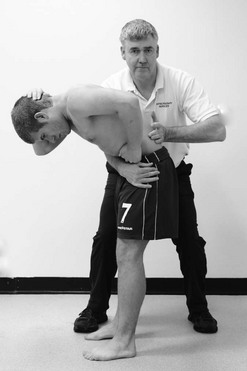
Lumbar flexion and variations
Patient starting position: standing.
Therapist starting position: therapist stands at the right side of patient.
• Overpressure (Fig. 6.6): left forearm of therapist stabilizes patient' pelvis, therapist's right hand is positioned between patient's scapulae
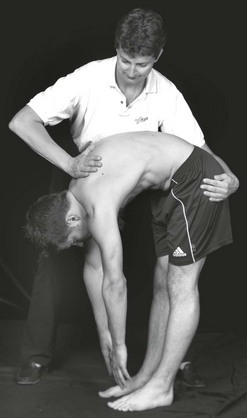
• Test combinations: patient folds arms in front of chest; therapist supports patient's pelvis with legs, trunk and right arm to control flexion position. Therapist's left arm assists the patient's movement.
Application of forces: active movement
• Observe active test: normal movement should be unrolling smoothly during downward
• Movement and during recovery from flexion (Fig. 6.7)
• Observe any deviations in the movement, e.g. during flexion sideflexion to the right
• Correction of the deviation may lead to a more limited range of movement and pain reproduction
• Overpressure (Fig. 6.6): therapist's right hand pushes patient's trunk towards stabilizing forearm at the patient's pelvis.
Test combinations: therapist keeps the patient in end of range flexion, any added movement as e.g. LF or rotation is done in an assisted active way: patient is asked to rotate the head and trunk up (Fig. 6.8AB) or to move the trunk sideways towards lateral flexion (Fig. 6.9A). Also combinations of three directions is at time possible (Fig. 6.9B & C)
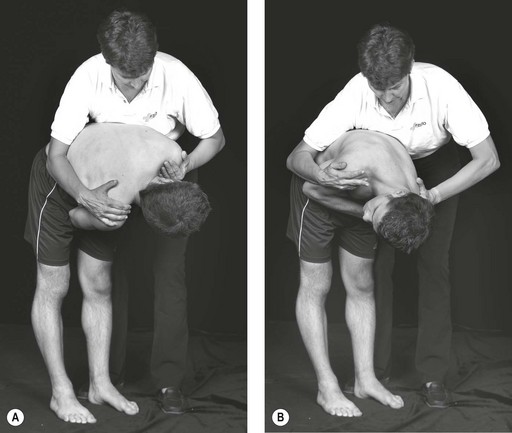
Figure 6.8 Lumbar flexion over-pressure adding rotation with over-pressure. A Rotation left; B Rotation right.
 ; B F + LF
; B F + LF  + Rot L; C F + LF
+ Rot L; C F + LF  + Rot R.
+ Rot R.• Application of neck flexion at the end of range of lumbar flexion (Fig. 6.10)

• Active flexion from caudad to cephadad upwards (Fig. 6.11)
• Test combinations e.g. flexion + LF ; flexion + rotation (Fig. 6.8AB)
• Test combinations are also possible in  flexed position (depending on the daily life activity which provokes the symptoms e.g. pain occurs while brushing teeth)
flexed position (depending on the daily life activity which provokes the symptoms e.g. pain occurs while brushing teeth)
Note: test combinations in flexion should only be performed in stable clinical situations, in which the pain is recuperating quickly after being provoked.
Change position of patient to sitting, sidelying, supine if necessary
Lumbar extension and variations
Patient starting position: standing
• Most tests: at the side of the patient
• In some test combinations: therapist may stand behind patient (as in lumbar quadrant)
• Overpressure generalized movement: therapist's left hand grasps around patient's chest and contralateral should; therapist's right hand is placed on patient's sacrum (Fig. 6.12)
• Localized overpressure: instead of placing the right hand on the sacrum, the therapist's thumb-pad and bent index fingers are gently placed around the spinous process of L5, L4, L3, L2 subsequently (Fig. 6.13)
• Combined movements, incl. lumbar quadrant (e.g. quadrant left: extension/sideflexion left/ rotation left):
• Overpressure: therapist's right hand on the sacrum stabilizes patient's pelvis; left hand moves gently towards the stabilizing hand (Fig. 6.12)
• Before applying overpressure, encourage the patient to arch the back further. It is important that the patient maintains his own balance
• Localized overpressure: the therapist moves the patient's trunk gently around the stabilizing fingers at the patient's spinous process (Fig. 6.13)
• Combined test movements: is possible in numerous directions.
• Localization of forces is the same as in extension & overpressure (Fig. 6.14); Extension + Rot (r): therapist pushes patient's left shoulder forward and right shoulder backwards with her left hand. Therapist's right index finger supplies counter pressure to the movement (Fig. 6.15).
 .
.a. lumbar quadrant may be build up as in normal extension: first apply extension, add left sideflexion, then left rotation (as in Fig. 6.14)
b. While standing behind the patient therapist's hands placed on patient's shoulder for control, after patient moved towards extension. Through her hands the therapist applies some pressure to the extension. By using the hands on patient's shoulders, the therapist guides the patient's trunk into the corner by laterally flexing and rotating his trunk away from her. Move until the limit of range (Fig. 6.16)

a. Extension from caudad-cephadad upwards; particularly if the extension while arching backwards is pain-free and a lumbosacral movement disorder is suspected (Fig. 6.17AB)
b. Change position of patient to sitting, sidelying, supine/prone if necessary
Lumbar sideflexion and variations
Patient starting position: standing.
Therapist starting position: at the side of the patient.
• Overpressure generalized movement: therapist's left axilla rests on patient's left shoulder; therapist's left arm grasps around patient's trunk towards patient's left upper arm. Therapist's right hand stabilizes patient's left crista iliaca (Fig. 6.18)
 generalized overpressure.
generalized overpressure.• Localized overpressure: therapist's left arm is position as in generalized overpressure, therapist's right thumb, supported by index finger is place laterally against spinous process of L5, L4, L3, L2 subsequently.
• Combined movements: as in generalized overpressure (Figs 6.19–6.22).
 + E
+ E• Overpressure of generalized and localized movement: hand at patient's crista /spinous process stabilizes the movement, which is initiated by the therapist's pressure on the patient's left shoulder towards the stabilizing hand at the pelvis. Overpressure is only applied after the patient moved actively towards the limit of the movement
• Combined movements: as in generalized overpressure. Therapist's hand at crista iliace may change anteriorly or posteriorly on the crista to stabilize the movements (Figs 6.19–6.22).
 + F.
+ F.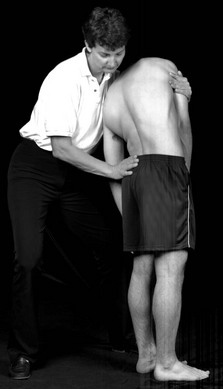
 + Rot
+ Rot  .
.
 + Rot
+ Rot  .
.a. Sideflexion from caudad–cephalad upwards (Fig. 6.23ABC)
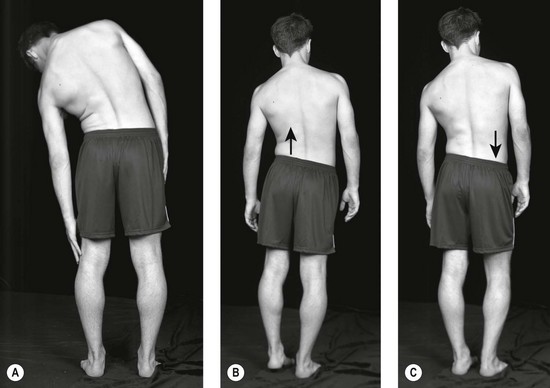
Figure 6.23 Lumbar spine lateral flexion left. A From above downwards; B from below upwards, hitching left hip; C dropping the right hip.
b. Change position of patient to sitting, sidelying, supine if necessary.
Lumbar rotation and variations
Patient starting position: standing
Therapist starting position: standing on patient's left side
• Generalized overpressure: therapist grasps patient's right shoulder posteriorly, and gently grasps left shoulder anteriorly (Fig. 6.24A)
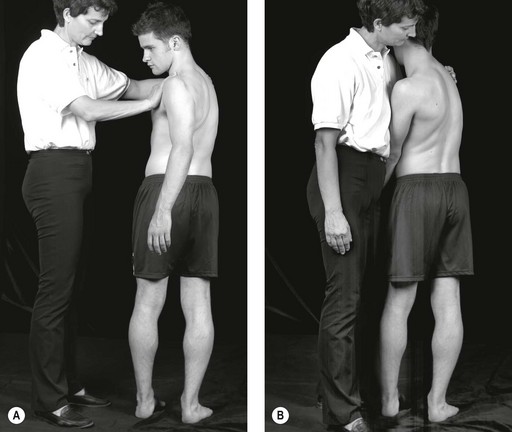
Figure 6.24 Combined movements in rotation left. A Initial adopting position; B End-position before adding other movements.
• Combined movements: after taking patient's trunk into full rotation, therapist changes her grasp to hold full range of rotation with her left axilla and hand (Fig. 6.24B)
• Generalized overpressure: ensure that the thorax remains straight, gently rotate the trunk until full range of movement, then oscillating overpressure is applied towards the whole movement
• Combined movement, depending on the additional movement directions, the therapist's right hand changes position on the patient's pelvis to stabilize the overall movement at the lumbar spine (Figs 6.25–6.29)
 + E.
+ E.
 + LF
+ LF  .
.
 + LF
+ LF  .
.
 + F + LF
+ F + LF  .
.a. If generalized overpressure provokes symptoms in the buttock area, differentiation testing may be considered (see Fig. 6.5 differentiation testing)
b. Rotation from caudad–cephadad upwards (Fig. 6.30AB)
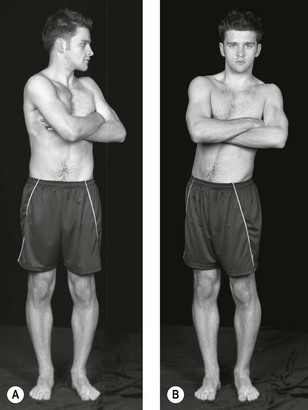
Figure 6.30 Lumbar spine rotation, commonly referred to as rotation to the left. A From above downwards; B from below upwards.
c. Change position of patient to sitting, sidelying, supine if necessary
If recent changes occur, the tests should be monitored regularly during the therapeutic process.
They are indicative of numerous processes in the nervous system (Butler 2000), but they may be particularly helpful in hypothesis generation regarding precautions to examination and treatment procedures and sources of the movement dysfunction, provided that the tests are placed within the overall context of subjective and physical examination findings.
Neurodynamic testing
See Table 6.9 for neurological conduction tests of the lower extremity.
SLR (sciatic nerve)
Patient starting position: supine
Therapist starting position: standing next to the patient's knee, facing the leg
One hand controls the knee extension, the other hand controls the lower leg (holding around the distal part of the tibia) (Fig. 6.31)
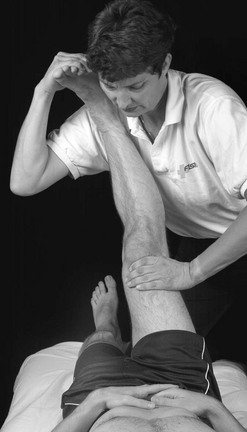
Figure 6.31 Straight leg raising (SLR  ). Reproduced with permission from Banks & Hengeveld (2010).
). Reproduced with permission from Banks & Hengeveld (2010).
In midposition between MR/LR and Ab/Ad of the hip the leg is raised until the onset of pain /resistance. Depending on the symptom localization, differentiation may take place by adding dorsiflexion of the foot, neckflexion, hip adduction or medial rotation of the hip (Fig. 6.32)


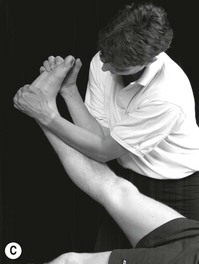
Figure 6.32 Straight leg raise: A inclined to the deep and superficial peroneal nerve; B inclined to the tibial nerve; C inclined to the sural nerve. Reproduced with permission from Banks & Hengeveld (2010).
Remarks/variations: may add inversion or eversion of the foot
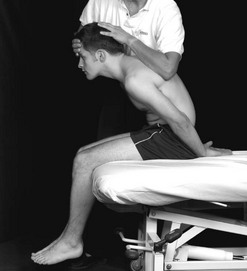
Slump test
Patient starting position: patient is sitting, well back at the short side of the bed (Fig. 6.33)
Therapist starting position: standing at the patient's side
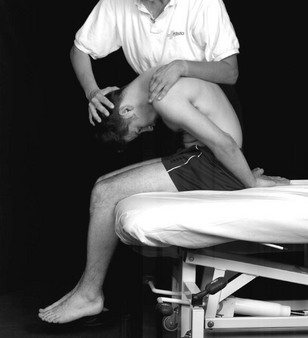
• Whilst controlling the patient's neck, the patient flexes the trunk fully (Fig. 6.34)
• The sacrum is placed in a vertical position whilst maintaining the flexed position of the trunk
• Neck flexion is added with gentle overpressure (Figs 6.35, 6.36)
• Knee extension is added whilst gently controlling the patient's trunk flexion and neck position (Fig. 6.37)

• alternative grip: therapist's elbow at the upper part of the patient's thorax and the web of the hand is placed under the patient's occiput to control the flexion position of the neck)
• If necessary dorsiflexion may be added to the procedure (Fig. 6.38)

• To differentiate any symptoms in the lumbar area or the leg, the neck will be raised from flexion to neutral position (Fig. 6.39)
• A pain-free lack of 30° knee extension can be normal, as can pain be felt at the T9–10 level of the spine (Maitland 1980)
• When firmer overpressure may be required the test may be performed in long-sitting position (Fig. 6.40)

Palpation
Manual diagnosis of the spine, including soft tissue palpation and passive intervertebral testing, has been found to be a reliable means in identifying symptomatic lumbar segmental levels. This is the case when manual diagnosis is compared with spinal anaesthetic block procedures (Jull et al. 1988, Phillips & Twomey 1996). Studies like these demonstrate that inter-tester reliability coefficients may be very high if a reference standard other than the comparison between individual therapist's palpating is chosen. Furthermore, it shows that training enhances the discriminative qualities of palpation skills (Jull et al.1997).
It is suggested to perform palpation examination as follows:
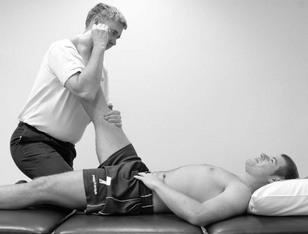
Slump in sidelying (femoral nerve)
Sidelying, pelvis at the side of the bed; lower leg in hip flexion. Patient stabilizes the knee of the lower leg with the hands (Fig. 6.41). Trunk is fully flexed, head in neutral position
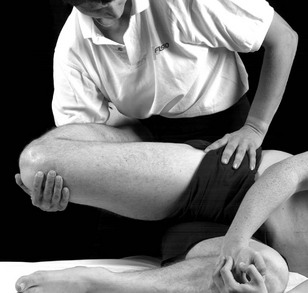
Figure 6.41 Slump in sidelying. Reproduced with permission from Banks & Hengeveld (2010).
Therapist starting position: standing behind patient, at the level of the pelvis.
One hand stabilizes the pelvis; the other hand supports the knee. Patient's foot may be placed on the side of the therapist's trunk (Fig. 6.41) or the lower leg may be carried by the therapist's forearm (Fig. 6.42)

Figure 6.42 Prone knee bend, leg free. Reproduced with permission from Banks & Hengeveld (2010).
Application of forces: The hip is extended until the onset of symptom /end of available range. Knee is kept in 90° F. Differentiation by neck flexion
Remarks/variations: Variation: patient may start in full neck flexion – differentiation will take place by moving out of the neck flexion
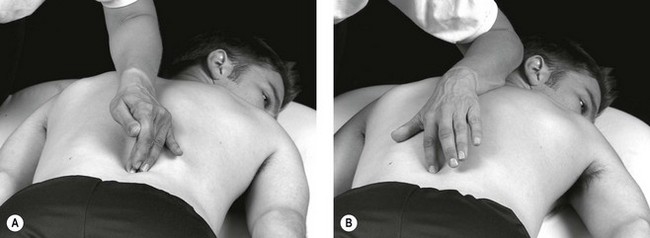
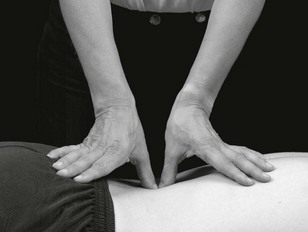
Small differences in temperature can be detected by the skilled therapist (Lando 1994). A small increase in temperature, sweating and skin tone may be indicating the spinal level at fault. All lumbar interspinous processes should be palpated with discernment, as should the lateral surface of the spinous processes. Thickening can occur on one or both sides of the process or in the space, event to the extent where the interspinous process can be completely obliterated by thickened hard tissue.
Figure 6.43 shows how this can be performed without the examiner having to move her position. She stands alongside the patient facing his feet, and uses her middle fingertip to probe into the right space and her index finger to dig medially into the left space. She can change rapidly from side to side, and equally rapidly from one level to the next, upwards or downwards.
It is also necessary to use the index and middle fingers to palpate into the interspinous space. When doing so, the fingers are held tightly together and oscillated back and forth sideways in an attempt to sink deeply into the space (Fig. 6.44).

Deeper palpations of the interspinous area are illustrated in Figure 6.45. By using the tip of the thumb a greater depth, even as deep as the lamina, can be reached. An assessment of this depth should be carried out if the more superficial area is normal.
Palpation of the paravertebral soft-tissue structures is illustrated in Figure 6.46. Both thumb tips are utilized, and the probing deep palpation should be carried out in many different directions – medially, lateral, caudally and cephalad. Also, the palpation should not be limited to the interlaminar area but should be extended to the adjacent upper and lower borders of the lamina and over the lamina itself.

B Passive movement testing, as passive intervertebral movement (PAIVMs), and if needed, passive physiological intervertebral movements (PPIVMs). See below.
Nerve palpation may be a diagnostic aid in the assessment of mechanosensitivity of the neural system (Butler 2000). Under normal circumstances peripheral nerves are painless to non-noxious stimuli. However, in cases such as nerve inflammation, gentle provocation, e.g. palpation, can cause pain, protective muscles responses or abnormal tingling-responses (Hall & Quintner 1996).
A comparative study investigating reliability of nerve palpation clinical examination in comparison to pain pressure threshold demonstrated excellent validity, reliability and diagnostic accuracy of nerve palpation in clinical examination at three different sites in the leg (Walsh & Hall, 2009).
Nerves can be palpated at various sites of the buttock and leg, as for example (Butler 2000):
Passive testing
Passive physiological intervertebral movements (PPIVMs): Passive physiological intervertebral movements are performed to examine the intervertebral mobility of one segment of the spine in relation to the neighbouring segment in more detail. Particularly discrepancies in mobility between mobile and stiff neighbouring segments are of interest, which may be indicative of a stability dysfunction of the motion segment.
Over many years it has been debated that the reliability coefficients of intervertebral movement examination may be insufficient; however, it is essential to consider the results from these tests within the overall information of subjective examination findings and other physical examination tests. There are various studies available which demonstrate an increase in reliability values if combinations of test procedures are being used in physical examination (Cibulka et al. 1988). It has been suggested not to condemn examination procedures without offering meaningful clinical alternatives and research from different perspectives with different reference standards (Bullock-Saxton 2002).
PPIVMs T10–L5/S1: flexion–extension
Patient starting position: sidelying, hips and knee flexed. A little pillow may be positioned under the lower waist, if the lumbar spine would sag into sideflexion
Therapist starting position: in front of the patient
Therapist supports both lower legs of the patient with both legs in the groin area (Fig. 6.47); the other hand palpates the interspinous space from below (Fig. 6.48)


Movement is performed either in flexion or extension direction by movement of the patient's pelvis (in a circular manner around the palpating finger).
• Single leg technique: as an alternative the test may be performed with one leg (Fig. 6.49)

• PA–AP shunt: if a movement seems more mobile at one segment in comparison to the neighbouring segment, a gentle PA glide may be added at the end of range of flexion by pulling at the thighs; or a gentle AP movement at the end of range of extension by pushing through the thighs. A normal feeling is that a sense of tissue-resistance should be perceived immediately at the application of the AP or PA movement.
PPIVMs T10–L5/S1: rotation
Patient starting position: patient is positioned on the couch
Therapist starting position: in front of the patient
Palpating finger as above (Fig. 6.48), lower arm is positioned paravertebral; other hand is positioned on crista iliaca an anterior spinous process of the ilium
Rotation is performed by gently rocking the pelvis posteriorly towards the palpating finger (Fig. 6.50AB)
Remarks/variations: in order to test the other direction, the patient is positioned on the other side
PPIVMs T10 – L5/S1: sideflexion
Patient starting position: patient is positioned on the couch
Therapist starting position: in front of the patient
Palpating finger as above (Fig. 6.48), lower arm is positioned paravertebral; other arm grasps around the upper pelvis/tuber pelvis
In order to test the other direction, the patient is positioned on the other side
Alternative grip: the therapist grasps around the pelvis, by holding the lower large trochanter and stabilizing the patient's pelvis between the arm and shoulder (Fig. 6.51AB)
Passive accessory intervertebral movements (PAIVMs)
Movement testing with intervertebral accessory movements should be carried out in the posteroanterior, unilateral posteroanterior and transverse directions of the spine. Additionally, anteroposterior movement of the lumbar spine may be performed.
On the one hand accessory movements are essential test procedures in physical examination, but on the other hand all accessory movements may be performed as a treatment technique as well.
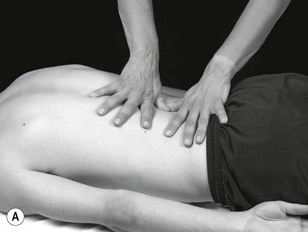
Central PA movement 

Patient starting position: prone lying, arms by the side
Therapist starting position: at the side of the plinth, facing the patient's lumbar spine. Hands or thumbs are used as the contact points; elbows relaxed, but stable. Sternum is over the hands
• Unilateral PA: both thumbs are placed in direct contact with each other adjacent to the spinous process in the intervertebral lamina (Fig. 6.52)

• Central PA: soft pad distally of hamate bone of the wrist is placed on the spinous process, hand is in a more or less vertical position; the soft pad of the other wrist is placed on top of the lower hand in the area of the anatomical snuffbox, 2nd and 3rd fingers grasp around the fingers of the lower hand to maintain the vertical position. Sternum of therapist is over the hand, elbows are relaxed (Figs 6.53–6.55)



• Gentler central PA movements may be produced by using the thumbs, as in unilateral PA techniques (Fig. 6.56)
Application of forces: movement is produced by the therapist's body
• In supine, do PA or unilateral PA movement (with pads of middle fingers; Fig. 6.57)

• In sideflexion right, do PA or unilateral PA movement (Fig. 6.58)

Figure 6.58 Posteroanterior central vertebral movement as a combined movement, in lateral flexion right (in LF  Do ).
Do ).
• In flexion, do PA, or unilateral PA movement (Fig. 6.59)
Transverse movements 
Patient starting position: prone lying, arms by the side
Therapist starting position: at the side of the table; height about at level of therapist's thorax
Localization of forces: therapist stands with one leg in front of the other, the pads of both thumbs are placed laterally against the spinous process; fingers are spread over the contralateral side of the thorax. Elbows are relaxed
Movement is produced by the therapist's body, transferring the weight back and forth over both legs (Fig. 6.60A)
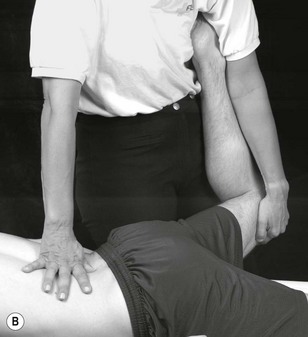
The technique may be intensified by holding the leg of the patient in abduction, resulting in sideflexion of the lumbar spine.
1. in sideflexion: do transverse movements
2. in transverse movement: do sideflexion of lumbar spine (by moving the leg into more / less abduction (Fig. 6.60B)
Anteroposterior movement 
Patient starting position: supine, legs resting on a pillow in a flexed position
Therapist starting position: at patient's side, facing the patient's abdomen
Pads of the second to fourth fingers are placed on top of each other and gently placed into the abdominal area, caudad of the umbilical area for L4 (Fig. 6.61)

Examination of motor control impairment
Comprehensive strategies for motor control of the lumbar spine are widely available in companion texts and supporting references: Sahrmann (2011), O'Sullivan (2005), Richardson et al. (2004). Furthermore, examples of techniques integrating motor control strategies with mobilization techniques are detailed on page 313 of this chapter in the subsection entitled ‘integrated treatment techniques’.
Mobilization and manipulation treatment techniques
As stated before, accessory movements of the spine can be used as treatment techniques. It is a special feature of the clinical reasoning processes of this concept of NMS-physiotherapy that the techniques may be applied in any physiological position of the spine, depending on the symptoms of patient. Also, physiological movements may be applied as a treatment technique. Furthermore, both accessory movements and physiological movements may be combined in an active of passive manner.
For example if the objective of treatment is the mobilization of sideflexion, it is possible to position the patient in sideflexion and then to apply accessory movement techniques and vice versa (see Fig. 6.68).
In this way a clinical rehabilitative approach to the normalization of movement impairments may be pursued. Next to the variations of active and passive arthrogenic techniques, integrated approaches of joint oriented techniques with neurodynamic treatment or motor control strategies often aid in the optimization of treatment results.
In this way almost endless variations of the treatment are possible. Hence the selection, the progression and adaption of treatment techniques must be based upon thorough examination procedures and the effects need to be monitored with disciplined reassessment procedures (see Box 6.5).
More details regarding selection and progression of treatment techniques can be found in Chapter 8 Management of knee disorders (Hengeveld & Banks 2014).
Physiological movements and variations: mobilizations, manipulations
Flexion techniques
Therapist starting position: as displayed in Figures 6.62–6.66


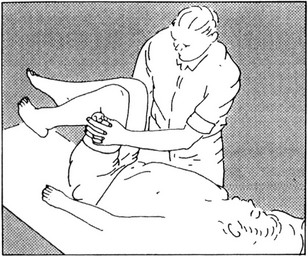

Figure 6.65 Starting position for flexion, extension, lateral flexion, rotation from below upwards and ‘coupled’ by using the femur and pelvis.

Figure 6.66 Flexion in sidelying. Reproduced with permission from Banks & Hengeveld (2010).
Movement is produced by the therapist's body
Adaptation of techniques towards E, SF


Rotation mobilization
Patient starting position: Sidelying, knees on top of each other, about 5–10 cm over side of plinth
• Grade I: upperlying forearm is gently placed in front of trunk (Fig. 6.69A)



• Grade II. Arm is placed on side (Fig. 6.69B)
• Positioning Grade IV, III (Fig. 6.69C):
a. pelvic rotation: maintain upper leg in neutral position between F/E for the treated segment; lower leg is extended, while palpating the lumbar, foot of the upper leg may be placed behind the knee fold of the patient
b. Rotation of the trunk until the onset of movement of the lumbar segment. To achieve this, the patient places the hand of the upper arm lightly on the therapist's shoulder. Therapist hold the patient in the interscapular area while gently turning the patient's trunk into rotation
Standing at back of the patient, level with the pelvis
For grades III, IV: may place lower leg on plinth, behind patient's pelvis
Grade I, II: both hands are placed over the ilium, next to each other/behind each other
Grade III, IV: one hand grasps around the pelvis, ensuring the control of the forward and backward movements of the pelvis during the application of the technique; other hand is placed gently over the pectoralis major area to stabilize the trunk rotation (gently holding – no pressure of the hand)
Application of forces: movement is produced by the therapist's body, towards the pelvis
• As a gentle grade I, II technique: see Figs 6.68 & 6.70.

• Localized rotation as end of range mobilization: as in IV (manipulation); however, performed in an oscillatory manner as a grade IV or III technique (refer to the figure of localized rotation manipulation (Fig. 6.71AB)
• Combined rotations as a progression of treatment in stable movement disorders (Figs 6.72–6.74)

 , do
, do  x axis).
x axis).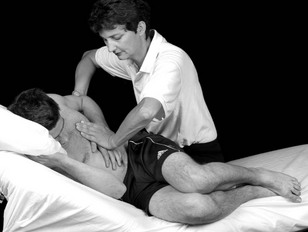
 , do Th).
, do Th).
 , do
, do  )
)Often the movement combination which provokes the patient's symptoms may be selected as a treatment technique, provided the problem is of a stable, nociceptive nature.
Neurodynamic techniques
The neurodynamic system can be treated in different ways. On the one hand the direct surroundings of the nerves may be treated, for example with passive mobilizations or soft tissue techniques, or directly in which it is distinguished between ‘slider’ and ‘tensioner’ techniques (Butler 2000, Coppieters & Butler 2008, Shacklock 2005)
Combination of arthrogenic techniques and neurodynamic mobilizations (example)
Lumbar rotation mobilization with neurodynamic emphasis
Patient starting position: (left) sidelying, same position as for lumbar rotation mobilization, grades III and IV
1. Patient's upper leg is hanging loosely over the side of the treatment table (Fig. 6.75)

2. As in (a) (Fig. 6.76)

1. Same position as for lumbar rotation mobilization, grades III and IV.
2. As a progression of (a). Therapist is standing in front of the patient; stabilizes the patient's leg between the knee
1. Same as for lumbar rotation mobilization, grades III and IV.
2. Therapist's (left) hand stabilizes patient's shoulder in the pectoral area, therapist's right hand is placed posteriorly at patient's left pelvis
1. Same as for lumbar rotation mobilization, grades III and IV
2. Therapist stabilizes the patient's leg in the chosen position of SLR, stabilizes the patient's shoulder and performs the rotation movement at the pelvis
These techniques are possible as a progression of treatment. It is crucial to consider the stability of the (neurogenic) pain mechanisms: the pain should be stable and behave in a more ‘on-off’ character during daily life activities.
Direct neurodynamic mobilization techniques
‘Slider’ techniques for the sciatic nerve (example)
Patient starting position: side lying, hipflexion (evt. adduction) short of onset of pain (P1)
Therapist starting position: standing next to the patient, on the level of the hip. Facing the patient's thigh
a. Therapist teaches patient to extend cervical spine (ensuring that this is possible without pain provocation)
b. Therapist extends the patient's knee, establishing the point of onset of pain in buttock or leg. The therapist's thigh block the patient's lower leg in a position of knee F/E shortly before P1
One hand stabilizes the pelvis, the other hand holds the patient's tibia
While the therapist gently moves the patient's knee back and forth into extension, short of P1, the patient extends and flexes the cervical spine in the rhythm of the knee movements. In this way a ‘slider’ technique to the neurodynamic system may be applied (Fig. 6.77)


• The technique may carefully be progressed into a ‘tensioner’ technique in which the patient stops moving the cervical spine, especially if the SLR is limited by resistance and the pain behaves in an ‘on-off’ manner
• Similar techniques as described above may be performed in supine lying, and sitting as well
Lumbar spine mobilization and manipulation techniques linked to clinical and supporting research evidence
In a number of studies it has been demonstrated that the grade, rhythm and direction of movement in which treatment techniques are being performed have an important influence on treatment outcomes. This has been demonstrated in a number of studies with treatment techniques in other joints such as the shoulder (Johnson et al. 2007a, Vermeulen et al. 2006), knee (Moss et al, 2007), elbow (Paungmali et al. 2003), ankle (Yeo & Wright 2011) or hip (Makofsky et al. 2007)
An increasing number of studies demonstrate physiological effects of lumbar mobilization techniques, such as accessory movements or rotation mobilization techniques:
• Perry and Green (2008), in a randomized controlled trial on normal male subjects, found that a grade III oscillatory mobilization applied at 2Hz to the left L4/5 facet joint had an effect on sympathetic activity in the left lower extremity over and above the effects produced in a control and placebo group (see Fig. 6.52).
• Krouwel et al. (2010), in a single blind randomized within subject repeated measurement study design, found in 30 asymptomatic subjects that a posteroanterior mobilization applied to L3 using a force platform to regulate force and frequency of oscillation (1.5Hz) had a significant (p= 0.013) effect on raising measured pressure pain threshold but this was independent of whether the amplitude of the mobilization was large (50–200N) or small (150–200N) (see Figs 6.55 & 6.56).
• Adams et al. (2010), in a review of intervertebral disc healing, suggest that a rotational mobilization might facilitate inter-lamella movements and prevent extensive scarring. In clinical practice, controlled mobilization of a recently-injured spinal level can be difficult due to pain and muscle spasm, but manual therapy can help to reduce pain and normalize muscle tone (Boal & Gillette 2004) and thereby decrease stress concentrations in the disc. Gentle early mobilization could also benefit the bony endplate, because repetitive micromovement stimulates fracture healing in adult long bones (Kenwright et al. 1991; see Fig. 6.69).
• Perry et al. (2011) in a quasi-experimental random design on 50 healthy participants, found that there was a significant (0.0005) increase in lower extremity sympathetic activity after grade V rotation manipulation, compared with extension exercises (see Fig. 6.71A).
Integrated treatment
In clinical practice, physiotherapists have established competencies and skills to deal with impairments of segmental mobility (arthrogenic), motor control and postural stability (myogenic) and nerve mechanosensitivity.
Physiotherapists should design individualized treatment programmes, collaboratively with the patient, based on the contemporary scope of practice, including an understanding of contextual mediators of the pain and disability and a comprehension of whether they would be modifiable or not. All impairment oriented treatments should follow up with an emphasis on restoring functional capacity, and guiding patients in the transition from health care needs to healthy life-styles/healthy living.
It is important that the treatment interventions, being arthrogenic, myogenic and/or neurodynamic oriented, are linked to examination findings. If possible clinical predictor rules may be applied to the selection of low back pain interventions and validated outcome measures such as Measure Yourself Medical Outcome Profile† (MYMOP; Paterson 1996) may be incorporated in the reassessment processes. Assessment during the application of an intervention and retrospective assessment are outlined in Box 6.8.
Research and best practice clinical guidelines have demonstrated that segmental mobilization and manipulation have a role to play in the treatment of patients with low back pain originating from the lumbar spine (NICE 2009).
Advances in knowledge in neuromuscular function have informed therapists how to fine tune movement, activate muscles and utilize motor control strategies to help patients recover from episodes of back pain (Macedo et al. 2009).
Clinical studies have demonstrated that restoration of ideal nerve gliding and tensioning after nerve injury or entrapment are important therapeutic considerations (Schafer et al. 2011).
What is not well known is the impact on recovery and outcome if these strategies are used in combinations and integrated into functional activities. The following example may illustrate this principle:
What if an SLR is mobilized whilst activating transverse abdominus muscles (TrAb).Will functional recovery be enhanced? The answers to such questions are beyond the scope of this text and the domain of the researcher. The next logical step, however, in selection of manual and movement therapy interventions for movement related NMS disorders of the lumbar spine is the merging of examination findings with treatment. For example, a patient may feel low back pain and neurogenic type symptoms in the back of the leg when bending forwards. The leg symptoms increase when the patient is asked to flex his cervical spine, in addition a posteroanterior glide on L4 reduces the leg pain and with a further addition of abdominal bracing the pain is less still, allowing greater range of cervical flexion. The logical treatment technique must be based on these findings, given that there is no nerve conduction loss and the leg symptoms settle quickly after provocation. The treatment technique is designed around the clinical evidence (supported by C/O evidence that the patient is troubled by leg pain when sitting or bending, the back feels stiff and the whole trunk feels weak).
A possible treatment technique in this case is:
In forward bending to pain + a posteroanterior pressure to L4 + activation of TAb
Active cervical flexion from neutral to full flexion (Fig. 6.78)
The challenge for the therapist is to take manual therapy and movement therapy interventions for low back pain into the domain of impairment interrelationships. Recovery may be enhanced by a lumbar accessory movement in PA-direction, abdominal activation or neural gliders alone; however, the challenge to clinical reasoning and handling skills is to merge integrated examination findings with treatment and design treatment techniques which address the relationship between movement impairments.
Below is a selection of such techniques. The reader is encouraged to reason how and why such techniques have been designed.
Where there is evidence of neurogenic and myogenic impairments coexisting
Position: standing+SLR+ TAb activation

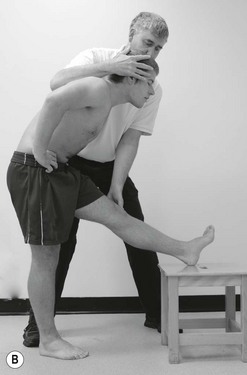
Figure 6.79 A Cervical flexion with ankle PF; B cervical extension with ankle DF. Reproduced with permission from Banks & Hengeveld (2010).
Purpose: sciatic-type leg symptoms restricting bending (pain and protection) when putting on socks; pain provoked with cervical flexion. Provocation less when abdominals activated to enhance neutral zone (Panjabi 1992) of lumbar segments
Standing with left heel resting on a stool and bending to point of leg symptom onset. Abdominals activated
Starting position of therapist
Standing by the left side of the patient facing forward.
Therapist's left hand stabilizing and monitoring patient knee. Right hand spread over the crown of the patient's head with the right forearm resting along the patients thoracic spine
Whilst monitoring the patient's knee in extension, the therapist flexes the patient's cervical spine at the same time as the patient performs active ankle plantarflexion [P/F]. Grade II+ or III- for both ankle P/F and cervical flexion
As the therapist brings the patient's head back to neutral, the patient's ankle is actively dorsiflexed
Where bending is impaired by painful protected sciatic-type leg symptoms without major conduction block
Where there is evidence of a need for restoring neural gliding supported by activation of stabilizing muscles to enhance postural stability
Position: sidelying+ TAb activation

Purpose: if the patient has sciatic-type leg symptoms, is comfortable in side lying, and needs neural gliding techniques to reduce neural mechanosensititvity. In addition, if the gliding techniques are facilitated by abdominal bracing and a greater pain free range of neural mobility is possible
Starting position of patient: side lying in the middle of the bed, painful leg uppermost (on most occasions). Spine parallel with the edge of the bed, hips flexed, knees together
Starting position of therapist: standing in front of the patient facing across the bed at the level of the pelvis
Localization of forces: therapist's right hand stabilizes the pelvis behind the iliac crest. Left hand holds the patients foot and ankle. Therapist's left thigh stabilizes the patient's knee
The patient is asked to activate transverse abdominus, and then actively flex the head. As the patient's head returns to neutral, the therapist extends the patient's knee and dorsiflexes [DF] the ankle. This rhythmical slider is continued
Uses: grade II or III to effect neural gliding supported by postural control of the spine with the desired effect of reducing sciatic nerve sensitivity to movement and increase movement capacity supported by motor control strategies
Position: supine lying+ TAb activation
Purpose: where a patient has sciatic-type symptoms and needs neural mobilization to reduce nerve mechanosensitivity and where the SLR+ DF has a greater available range when the abdominal muscles are activated to effect improved foraminal dynamic roominess (hypothesis)
Starting position of patient: Supine lying in the middle of the bed
Starting position of therapist: Standing by the patients right side (for right leg symptoms), right knee on the bed facing the patients opposite shoulder
Localization of forces: therapist supports the patient's heel on the therapist's right shoulder in a position of SLR for treatment. The therapist holds the patient's foot at the toes with the right hand and stabilizes the knee in SLR with the left hand
With abdominal muscles activated the patient's ankle is dorsiflexed through a range of movement to effect reduction in neurodynamic mechanosensitivity
Grade III to IV where there is a need for increase in range of SLR and where a component of lumbar segmental stability is inhibiting recovery of nerve mobility
Position: supine lying+ SLR + ankle DF + cervical flexion
Method: TAb activation exercises

Purpose: activation in neural loading where capacity to activate is impaired at the limit of neural mobility
Starting position of patient: Supine lying
Starting position of therapist: Sitting on the side of the bed facing the patient's head at the level of the patient's pelvis
Localization of forces: both of the therapist's hands facilitate activation of abdominals
Abdominals activated in progressive amounts of neural loading (left knee flexed to 90°, foot on bed), right leg resting on left flexed knee and relaxed foot, in SLR, in SLR+ DF, neck flexed chin to chest
Activation of abdominals for motor control acquisition in progressive amounts of neural loading so that the patient has the capacity to activate muscles selectively (dissociation) in neural loaded positions. Activation should be pain-free in all instances
Where there is evidence of arthrogenic and neurogenic impairments coexisting

Purpose: to regain end of range lumbar rotation in a neural loaded position – maximize segmental and neurodynamic capacity
Starting position of patient: Sidelying and maximum rotation of the trunk, neurodynamic restricted leg uppermost. Upper leg in tolerable extreme of SLR position, resting on the edge of the bed, left forearm resting on the lower rib cage
Starting position of therapist: standing behind the patient at the level of the pelvis
Localization of forces: therapist's left hand (for right rotation and right SLR) is spread over the patient's left greater trochanter and iliac crest. The therapist's right hand stabilizes the trunk over the anterior pectoral area adjacent to the left shoulder
Whilst the therapist's right hand stabilizes the trunk, the left hand and body working together produce rotation of the pelvis to the right in relation to the stabilized trunk
Grade IV in a direction localized to a specific spinal segment (e.g. L4/5) where there is segmental restriction in rotation and this restriction is increased when the leg is in an end of range SLR+DF position
Position: side lying + lumbar rotation

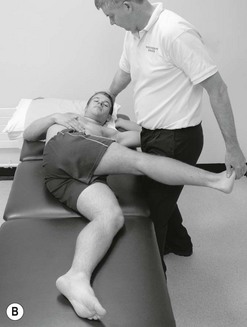
Figure 6.84 In side lying: A cervical flexion with knee flexion; B cervical extension with knee extension.
Purpose: to create a position of dynamic roominess and an ideal interface environment for the neural tissues to be ‘flossed’ (Butler 2000)
Starting position of patient: side lying in lumbar rotation
Starting position of therapist: standing in front of the patient facing across the bed at the level of the patients pelvis
Therapist's left hand (for patient in right side lying in lumbar rotation to the left) cradles the patient's occipital area. The therapist's right hand holds the patient's right foot. The therapist's right thigh stabilizes the patient's right thigh just above the knee
Whilst the patient's lumbar spine is in rotation the therapist flexes the patient's cervical spine at the same time as flexing the patient's right knee. The therapist then extends the patient's cervical spine at the same time as extending the patient's right knee. This sliding action is repeated at a smooth rhythm
As a grade II or III – where the patient has sciatic type symptoms restricting SLR with end of range segmental stiffness
Position: supine lying + PA L4


Purpose: where a PA on L4 is shown to enhance the range of SLR and dorsiflexion (neural tensioning) (right)
Starting position of patient: supine lying, left knee bent and right leg (back of the knee) resting on the left knee
Starting position of therapist: standing on the patient's right side facing the patient head at the level of the pelvis
Localization of forces: therapist's index fingers make contact with the spinous process of L4, hands resting on the patient's back adjacent to the spine
Therapist applies a PA pressure on L4 with the index fingers at the same time as the patient actively extends the right knee and dorsiflexes the ankle. As the PA pressure is released, the patient relaxes the right leg
Grade II, III – range of active SLR and DF with grade III– PA where back and leg symptoms are quite painful and the patient is comfortable lying supine
Where there is evidence of arthrogenic and myogenic impairments coexisting
Position: prone lying + TrAb activation

Purpose: if activation of TAb reduces pain responses and helps modulate pain effects of PA mobilization in acute LBP
Starting position of patient: prone lying, neutral pain-free
Starting position of therapist: standing by the side of the patient at the level of L4, leaning over so that the therapist's sternum is over L4 segmental level
Localization of forces: therapist's hands are interlocked so that the area between the pisiform and hook of hamate of the therapist's contact hand is against the L4 spinous process. Therapist's elbows slightly bent
Whilst asking the patient to activate TAb to 20%, the therapist performs a PA mobilization on L4
Grade I and II for episode of LBP where pain and protection with movement are the predominant features
Position: prone lying + PA pressure on L4 +TrAb activation
Method: active control of hip medial rotation in 90° of knee flexion (dissociation activity)
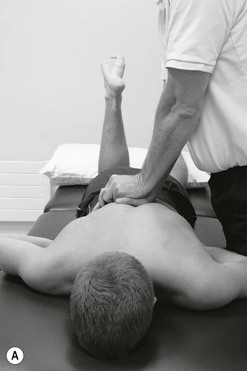

Figure 6.87 A In prone lying + posteroanterior pressure on L4 +TrAb activation: active control of hip medial rotation in 90° of knee flexion (dissociation activity); B in prone lying + posteroanterior pressure on L4 +TrAb activation: active control of hip medial rotation in 90° of knee flexion (dissociation activity).
Purpose: PA pressure on L4 to reduce pain inhibition of activation and maximize motor control strategy
Starting position of patient: prone lying with one knee bent to 90°
Starting position of therapist: standing by the side of the patient at the level of L4, leaning over so that the therapist's sternum is over L4 segmental level
Localization of forces: therapist's hands are interlocked so that the area between the pisiform and hook of hamate of the therapist's contact hand is against the L4 spinous process. Therapist elbows slightly bent
Whilst the therapist applies a PA pressure grade II, III to L4 the patient is asked to activate abdominals and at the same time dissociate hip rotation from pelvic movement
Where segmental mobilization reduces pain inhibition of activated muscles to support effective dissociation strategies
Position: standing + TrAb activation
Method: PA L4 with lumbar FF (MWM – mobilization with movement)


Figure 6.88 A, B in standing + TrAb activation: posteroanterior L4 with lumbar FF (MWM – mobilization with movement).
Purpose: when bending forwards or sustained bending is painful due to segmental restriction and motor control impairment
Starting position of patient: standing
Starting position of therapist: standing behind the patient and just to one side
Localization of forces: the therapist's left hand stabilizes the patient's trunk using the forearm against the patient's abdomen below the segmental level to be mobilized. The heel of the therapist's right hand is placed over the spinous process of L4 (for example) and directed upwards slightly
Whilst the patient bends forwards to P1 or limit with the abdominal muscles activated, the therapist, whilst stabilizing the patient's trunk, applies a posteroanterior pressure directed cephalad to the spinous process of L4
To improve pain free range and restriction of forward bending where the patients feels more stable with abdominal activation and can move further with PA pressure grade III, IV therefore allowing the patient to stretch further into range to increase forward flexion range
Where there is evidence of arthrogenic, myogenic and neurogenic impairments coexisting
Position: lumbar machine traction (supine, prone, sidelying)
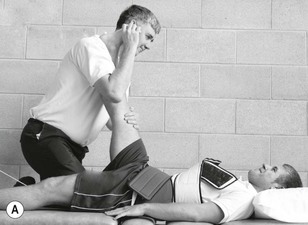
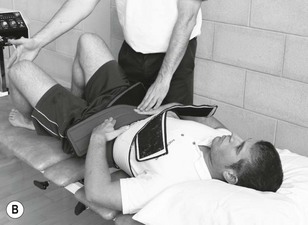
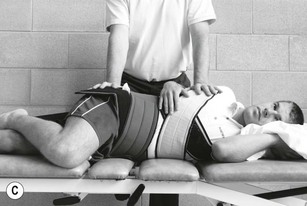

Figure 6.89 A In machine traction: SLR+ ankle DF; B in machine traction + TAb activation: hip AB and LR control; C in machine traction: lumbar rotation; D in machine traction: posteroanterior pressure.
Purpose: using machine traction as an interface mobilization, an enhancer of muscle activation or as a segmental mobilization
Starting position of patient: supine, prone, sidelying
Starting position of therapist: standing by the side of the traction bed
Traction harnesses applied to thorax and pelvis
Apply appropriate traction force to effect symptom reduction along with:
A The therapist mobilized ankle dorsiflexion in SLR
B In crook lying, the patient activates abdominals and then dissociates hip abduction and lateral rotation for trunk rotation or extension
C The therapist performs lumbar rotation mobilization by holding onto each iliac crest
D The therapist performs a posteroanterior mobilization of L4 with the patient in supine lying and the therapist's index fingers applying a mobilization pressure against the spinous process of L4
Where there is protective muscle spasm coexisting with arthrogenic, other myogenic and neurogenic impairments
Position: flexion over the bed
A Traction with sustained unilateral PA mobilization of L4
B Traction with TAb activation
C Traction with TAb activation and knee extension as a neural mobilization
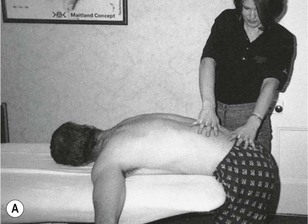
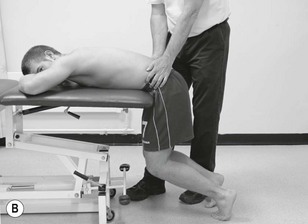

Figure 6.90 A In flexion over the bed; B in flexion with traction: TAb activation; C in flexion with traction + TAb activation: knee extension.
Purpose: where protective spasm is inhibiting effects of mobilization, co-contraction or nerve gliding and where the flexed position over the bed allows sustained stretching to reduce protective spasm
Starting position of patient: flexed over the bed with knees bent under the bed and feet resting on the floor
Starting position of therapist: standing by the side of the patient
Localization of forces: therapist places one hand over the mid-thoracic area and the other over the sacrum or L4
The patient is asked to flex their knee under the bed to allow the pelvis to flex thus producing a traction effect on the lumbar spine and a sustained stretch to the erector spinae muscles in particular.
A The therapist uses one hand to apply a unilateral PA mobilization to L4
B The patient is asked to activate the abdominal muscles and extend each hip in turn to facilitate dissociation and trunk stability
C The patient is asked to activate the trunk muscles and at the same time rhythmically extend one knee to produce a neural gliding effect
Where this starting position effects a relief of protective spasm to allow more effective mobilization, more effective activation and more effective neural gliding
Case studies
The following two case examples are included in this chapter to demonstrate:
• The gathering and analysis of patient reported problems and information
• The use of clinical reasoning strategies to enable open-minded and effective sorting out of the clinical information
• Linking patient problems to examination and interventions driven by the patient's functional and cognitive needs
• Evidence informed selection of the most appropriate interventions and treatment techniques
• The use of evaluation to drive progression of treatment towards patient reported outcomes.
 Case study 6.1 The 45-year-old joiner with a stiff back
Case study 6.1 The 45-year-old joiner with a stiff back
Question 1. My back feels stiff after I have been sitting for a while and then I get up. It's uncomfortable  if I have walked for half an hour so I have to sit down
if I have walked for half an hour so I have to sit down
Successful outcome? To be able to move around without discomfort and to be able to do my job without stiffness.
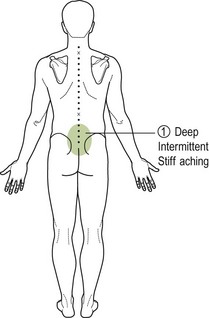
Areas of symptoms.  An area from just above the iliac crests to the mid-sacral area, in the middle of the spine, deep, intermittent stiff and aching. Radiating both sides but more to the left (Fig. 6.91).
An area from just above the iliac crests to the mid-sacral area, in the middle of the spine, deep, intermittent stiff and aching. Radiating both sides but more to the left (Fig. 6.91).
Behaviour of symptoms. I am a bit stiff in the morning when I get up but this eases after 5 minutes moving around. I do struggle to put my socks on  when I have to bend and twist when sitting. I am a bit worried about going back to work because I have to do a lot of bending and twisting.
when I have to bend and twist when sitting. I am a bit worried about going back to work because I have to do a lot of bending and twisting.
When I am sitting down, I am fine, just a bit achy, but if I have been sitting for an hour or so and I come to get up I move slowly because of stiffness in my back.
If I have been walking round the shops with my wife, after an hour, I start to stiffen up and my back gradually aches  more and more. If I sit down for a while, I am ok after 10 minutes.
more and more. If I sit down for a while, I am ok after 10 minutes.
Sometimes I wake up at night if I roll over awkwardly and it just gets my back in the wrong position, usually turning over onto my right side [pain and stiff] 
History of symptoms. I pulled my back at work 4 weeks ago  . It is a lot better now but still not fully better, so the Doctor has sent me here. I was lifting a plank of wood and it slipped in my hand. This jarred my back
. It is a lot better now but still not fully better, so the Doctor has sent me here. I was lifting a plank of wood and it slipped in my hand. This jarred my back  as I bent and twisted to catch it before it fell on my leg.
as I bent and twisted to catch it before it fell on my leg.
I have had twinges and a stiff back in the past but it always goes off in a day or so. It comes with the work.
I have had a few knee and ankle injuries playing football on the right side but nothing major.
Special questions/medical and health screening. My general health is fine, I just get tired if I am working away from home and I have to drive a long way. I do not think this helps my back. I do get acid reflux and I take medication for this. I had a back X-ray and it just came back as slight wear and tear in the lower back. I try not to take any tablets although the doctor gave me some anti-inflammatory tablets. They did not help much.
Hypotheses from subjective examination
• Likely to be segmental hypomobility related to strain
• Possible P/E findings: dysfunction in combined movements at end of range (flexion and rotation causing pain)
• There will be some motor control issues after 4 weeks, so screen for this
• No evidence of maladaptive protective mechanisms or central sensitization
• Nature of work may be a factor in risk and injury reduction/recurrence
• Check for contributing factors in lower extremity related to old injuries (hip, knee and ankle)
• Being clear regarding outcome measures for return to work and daily activities.
Sway back, over activity in left erector spinae (T8–L2) [protective response], contralateral protective shift [correct, stiff  increased in intensity].
increased in intensity].
*Sitting, reach forward as to put sock on left  when stretches [lumbar flexion and rotation, hip flexion 90° and lateral rotation 30°, reaches ankle].
when stretches [lumbar flexion and rotation, hip flexion 90° and lateral rotation 30°, reaches ankle].  ISQ with activation of abdominal muscles, lateral glide of the hip and neural loading [cervical flexion in lumbar flexion and left lateral flexion].
ISQ with activation of abdominal muscles, lateral glide of the hip and neural loading [cervical flexion in lumbar flexion and left lateral flexion].
**FF 40' + LLF 20'  . ISQ with activation of abdominals and neural loading.
. ISQ with activation of abdominals and neural loading.

E 30+ LLF 20+ LR 20  . ISQ with activation of abdominal and neural loading.
. ISQ with activation of abdominal and neural loading.
*PPIVMs and PAIVMs reveal hypomobility at L3/4 more on the left (lateral flexion, rotation and ULPA). Local pain provoked at end range.
*Stiff hip flexion /adduction on left and weak gluteus medius.
• Restore pain-free, resistance free segmental mobility at site of injury at L3/4
• Mobilize stiff hip and activate gluteus medius in the functional positions that reproduce 
• Recondition for work including self-management strategies with repeated movements towards extension and contralateral rotation/LF
• Main outcome measure- FF + LLF + LOAD (PAIN FREE): to enable restoration of functional performance (sitting without stiffness, carry out job related tasks without pain and stiffness).
• Clues from subjective examination and from knowledge of clinical, functional and behavioural sciences support the use of mobilization and physical activity in health and well-being (CSAG 1994)
• There is evidence for the effectiveness of hip mobilization for early osteoarthritis along with exercises (Sims 1999, Van Baar et al. 2000)
• PPIVMs help to localize segmental impairment (Cook & Hegedus 2010)
• PAIVMs – posteroanterior segmental stiffness is a prediction rule for the effectiveness of lumbar manipulation (Flynn et al. 2002)
• Loss of motor control is known to contribute to hip and back pain (Macedo et al. 2012)
• Behavioural and physical conditioning are key to sustainable physical and mental performance (Main & Spanswick 2000)
• NICE guidelines recommend mobilization and manipulation to enhance recovery from NSLBP (NICE 2009)
• Yeris et al. (2002) and Makofsky et al. (2007) noted that passive hip mobilizations demonstrated immediate effect on gluteus maximus contraction force.
Thinking: start by trying to reduce segmental stiffness and pain with mobilization techniques as movement related pain and stiffness are most evident and there seems little influence on symptoms with neural loading or trunk motor control in functional positions.
Treatment: in lumbar extension+ left lateral flexion+ left rotation mobilize L3/4 with a  unilateral posteroanterior pressure grade III+ for 3 minutes, repeated twice. Grade III+: with slight pain in rhythm of the movement. The aim is to reduce the pain and restriction in a compression pattern which is occurring through the active range of movement. Assessment during treatment. After 2–3 minutes sense of resistance changing (‘freer’) and patient felt less pain.
unilateral posteroanterior pressure grade III+ for 3 minutes, repeated twice. Grade III+: with slight pain in rhythm of the movement. The aim is to reduce the pain and restriction in a compression pattern which is occurring through the active range of movement. Assessment during treatment. After 2–3 minutes sense of resistance changing (‘freer’) and patient felt less pain.
Effects: reaching forward in sitting, FF+ LLF isq, hip F/ADD isq, gluteus medius control isq. Lumbar E+ LLF+ ROT better.
Home automobilization: sent home with a self-mobilization of L3/4 unilaterally on the left into lumbar extension/left lateral flexion and left rotation in standing as per treatment dosage. With instructions to do the exercise every 4 hours 10 × 3 and ensure symptoms reduce with repeated movements.
Follow up appointment 1 week later
Therapist's thinking: mobilization of L3/4 in combined movements in extension eased an old facet restriction and compression pattern but did not change the more recent pain and restriction into flexion. This is qualified by the fact that the patient felt better standing for longer and was less stiff after sitting but still had problems with bending and twisting and putting his socks on. The hip and gluteus medius impairments are likely to be separate components, as they did not change with lumbar mobilization.
Repeat the first treatment to clear the extension pattern and confirm this has little effect on flexion and hip components then add in mobilization in flexion to reduce aching and stiffness with bending and twisting (standing and sitting).
Treatment: in lumbar extension+ left lateral flexion+ left rotation mobilize L3/4 with a  unilateral posteroanterior pressure inclined medially grade IV+ for as a progression of treatment 3 minutes, repeated twice. The aim is to reduce the pain and restriction compression pattern. During treatment pain was provoked with the stiffness at end of range. The pain reduced as the stiffness reduced and full range was achieved.
unilateral posteroanterior pressure inclined medially grade IV+ for as a progression of treatment 3 minutes, repeated twice. The aim is to reduce the pain and restriction compression pattern. During treatment pain was provoked with the stiffness at end of range. The pain reduced as the stiffness reduced and full range was achieved.
Effects: reaching forward in sitting, FF+ LLF isq., hip F/ADD isq., gluteus medius control isq. Lumbar E+ LLF+ ROT no pain or restriction.
Therapist's thinking: it is clear now that the old extension pattern has cleared up sufficiently with mobilization but the flexion and hip components will need other interventions. Flexion and sideflexion is the painful stiff functional movement so use this as a treatment technique incorporating lumbar rotation
Treatment: in lumbar flexion and left lateral flexion: did right pelvis rotation grade III to L3/4 stretching into discomfort  for 3 minutes repeated once. Effects during treatment – after 2 minutes each time discomfort settled, resistance improved.
for 3 minutes repeated once. Effects during treatment – after 2 minutes each time discomfort settled, resistance improved.
Effects: improvement in flexion and lateral flexion and reaching in sitting to put socks on but hip flexion/adduction and gluteus medius control remain unchanged.
Home programme: as extension is now pain-free, automobilization can be stopped but advised patient to restart if stiffness and aching with sitting and standing starts to creep back in.
Advised to try to maintain the gains from mobilization into flexion combined movements using the functional activities that remain stiff and painful. Instructions given were to move into the functional direction until slight sense of pulling during every functional opportunity to maintain treatment gains.
Therapist's thinking: the patient feels as though his mobility has improved but he still gets sore after repeated bending and twisting so he is wary about returning to work, as he feels weak still. He is not as stiff after sitting or standing but still feels restricted putting his socks on.
This information suggests that the segmental pain and stiffness is settling but motor control has not fully recovered. The hip is still stiff so will need mobilizing to ensure contributing factors are addressed effectively.
On examination of unilateral posteroanterior pressure of L3/4 there is no loss of range just a deep soreness when pushing at the limit of the range. When asked to contract gluteal muscles actively the soreness on palpation diminishes significantly. When asked to flex and left side flex the lumbar spine there is a feeling of discomfort and weakness in this position that needs to be discomfort free and strong for work. When asked to contract the gluteal muscles in lumbar flexion and lateral flexion the discomfort reduced significantly. The same response to gluteal activation occurred in the functional position of reaching to put socks on as in sitting.
The important intervention now is to work towards sustainable functional capacity and return to work. To mobilize the hip and see if this reduces pain inhibition of gluteus medius and improve its stabilizing capacity.
Treatment: hip flexion/add grade III mobilization for 3 minutes repeated twice. During treatment the stiffness and discomfort gradually reduced over the 3 minutes of treatment time.
Effects: this helped the range of hip flexion when reaching to put socks on but did not improve the activation ability of gluteus medius.
Treatment: active exercises to activate gluteus medius in side lying 3 × 10 daily
Home programme: patient shown automobilization of hip flexion/add as per treatment and, as well as gluteus medius exercises, activation of gluteal muscles when performing functional tasks such as bending and twisting or putting socks on.
Thinking: the patient has mastered the gluteus medius activation. This has also improved forward bending, as the hamstrings are less tight. The hip is more flexible and the bending and twisting with loads equivalent to work is pain-free. Use this last session as an information session to explain to the patient: the importance of regular physical activity: the need to maintain strength and mobility to reduce risk of injury again at work: the role of pain in protection but also how pain can lead to maladaptive and chronic deconditioning.
Treatment: advice and information on physical activity and pain. Review exercises and functional capability.
Effects: patient has better understanding of the importance of physical activity, maintaining functional capability for his job and understanding pain and its role in protecting and ensuring recovery from injury.
Home programme: staged return to work, hand over to occupational health staff and discharge from health care to return to healthy living.
Case study 6.2
It is useful to include here an example of how the manipulative physiotherapist thinks her way through a patient's difficulty and atypical spinal problem. This particular example demonstrates how to link the theory with the clinical presentation. It also demonstrates the different components a patient's problem may have, and how one component may improve and another not. This patient's disorder demonstrates how the therapist must adapt her techniques to the expected and unexpected changes in the symptoms and signs. The example also demonstrates how open-minded she must be, and how detailed and inquiring her mind must be in making assessments of changes and interpreting them.
Eighteen months ago, a 34-year-old fit, well-built man (Mr L) with no history of previous back problems, wakened with pain in his left buttock area. Over the previous 2 days he had suffered very bad low lumbar backache, which his doctor had diagnosed as being viral because he also had general aching in other parts of his body. Mr L did say that, although he had ‘flu-like aches all over’, his lower back was the worst area. He had been on holiday during the previous week and had done a lot of lifting and been wind-surfing (a new experience for him). Two days after the onset of his buttock pain it spread, overnight, down the left leg with tingling into the big toe area of his left foot (? L5 radicular symptom). Some days later, the big toe tingling alternated with tingling along the lateral border of his foot and into the lateral two toes (? S1 radicular symptom). At no time prior to 18 months ago had he ever had any back symptoms, and there was no familial component. He had undergone numerous forms of treatment (orthodox and unorthodox) over 6 months, but without success. Over a period of time the symptoms eased, but he did not become symptom free.
Following a fall 3 weeks ago, which exacerbated his disorder, he had a lumbar puncture (which proved negative) and hospital traction for a week. Following this, his low back pain increased. When he first went for physiotherapy his symptoms were as follows (Fig. 6.92):
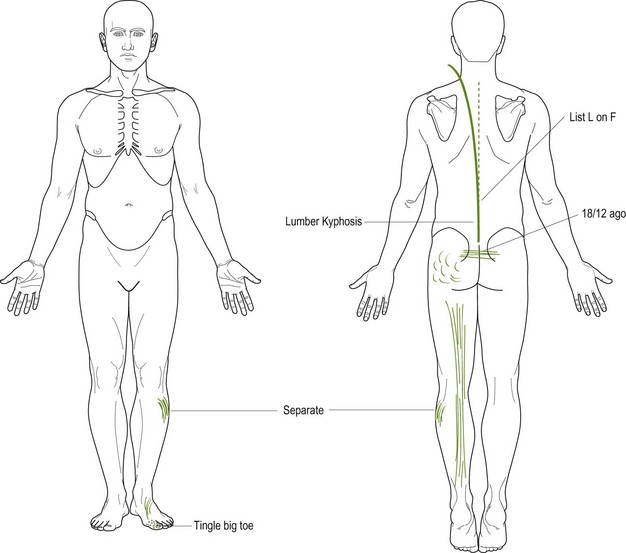
1. He would waken in the morning with back pain and back stiffness, and the stiffness would last for a few hours. (Unusual for a non-inflammatory musculoskeletal disorder.)
2. Coughing caused both back pain and left calf pain.
3. He was using indomethacin (Indocid) suppositories every night, and he felt that these were essential to lessen the level of his pain. (Perhaps this means there must be an inflammatory component.)
4. Bending caused him severe back and leg pain, both of which eased immediately on standing upright. (This latter fact indicates that a treatment technique that provokes leg pain may not be a contraindication to its use; the technique, to be effective, may in fact need to provoke leg pain.)
5. On standing for 1 minute, the pain would increase in his back and would spread down his leg. (This indicates that a sustained technique may be required.)
The initial physiotherapy treatment, which he had undergone elsewhere, had improved all of his symptoms marginally. The first three of these treatments consisted of PAs on L5 and unilateral PAs to the left of L4. The latter, he said, provoked calf pain in rhythm with the technique. On the third treatment intermittent traction had been introduced, but this did not help him.
I saw him for the first time 5 days later.
1. On more positive questioning to determine his area of pain, it was interesting to note that, although his main lower leg pain was posterior, he had what he described as ‘a different pain’ in the upper posterolateral calf. These two pains were sometimes present at the same time, but were more frequently felt separately. (This tends to indicate that they may arise from two different sources – two components.)
2. Standing (and he could not stand erect, in fact he had a lumbar kyphosis) provoked pain in his left leg, and he was unable to bend backwards because of increased leg pain.
3. He had an ipsilateral list on flexion. (Items (2) and (3) seem to indicate that he has a disc disorder, which is provoking possible radicular pain. The offending part of the disc is probably medial to the nerve root and its sleeve, and will therefore be harder to help by passive movement techniques.) Neck flexion while he was flexed was limited by increased leg pain. (There must be a canal component in his disorder.) It did not increase his back pain. (The cause of his back pain is probably not causing his leg pain. Two aspects of the one structure perhaps? The disc?)
4. While still in the flexed position, rotation to the left increased his leg pain by about 100%. Rotation to the right in flexion decreased the leg symptoms, slightly but definitely. (It is very helpful from a treatment point of view to have different responses with the different directions of rotation.) In this man's circumstances it is wise, when considering the selection of technique, to choose the relieving position while performing the relieving direction for the rotation.
5. In the upright position, performing a lateral shift of his trunk towards the left decreased his pain; shift to the right slightly increased the symptoms. (Because of this pain response, the list must be directly related to his disorder.)
6. Straight leg raise on the left was 35°, causing posterior leg pain. On the right it was 70°, and he said it caused an uncomfortable tight feeling, plus tingling, in the left foot laterally. (Crossed SLR response – treatment may need to include mobilizing the right SLR.)
7. Testing the power of his calf in standing demonstrated some weakness, which may have been a neurological weakness but may also have been a pain inhibition reaction.
8. Attempting to stand, from sitting only a short time (half a minute), he had back pain and a severe lumbar kyphosis, which took some 15 seconds or more (a long time) to dissipate. (Because the kyphosis developed so quickly, this meant that the disorder causing his back pain was very mobile.)
9. His leg pain was minimal on first standing but then gradually increased in intensity and also in the length of the pain referral down his leg. (This meant that the disorder causing his leg pain had a latent component.)
10. His leg pain and his back pain could be provoked separately. (This meant that there were at least two components to his disorder. With the added information in number (1) above, he has at least three components. Number (4) above makes it four components.)
11. Tingling was felt either in the big toe or the lateral border of his foot. (This indicated the possibility of two nerve roots being involved. This could mean that two intervertebral discs may be involved, or the patient may have an anatomically abnormal formation of the nerve roots.)
12. He also had canal movement abnormalities as well as intervertebral joint movement abnormalities.
Mr L's disorder was obviously atypical. The disc component seemed to be causing him more disability than the radicular aspect, but obviously the radicular aspect took higher priority. Being atypical means that one has to be very quick to notice the changes in the examination signs of the separate components, and to react with appropriate technique changes.
Because it seemed to be discogenic (getting up from sitting) with a nerve-root irritation:
1. The choice of technique would be rotation, as the symptoms and signs are clearly unilateral
2. The rotation would be performed in the ‘symptom-relieving’ position and direction to avoid provoking pain
3. Thinking ahead to further treatment techniques, it seemed possible that the canal signs would not improve in parallel with the joint signs, and that therefore SLR stretching may be required later.
Mr L was positioned lying on his left side with a support (folded towel) under his iliac crest to gain a lateral shift to the left position (his comfortable shift position, see item (5) above). He was also positioned in a degree of flexion to keep his lumbar spine away from the painful and markedly limited extension position. A rotation of this thorax to the right in relation to the pelvis was also adopted, and his right leg was kept up on the couch to avoid any canal tensioning (which would occur if his right leg were allowed to hang over the edge). The technique was to rotate his pelvis to the left (that is, the same direction as thoracic rotation to the right, but performed from below upwards) as a sustained (sustained because of the latent component) grade IV.
• During the performing of the technique he felt an easing of his leg symptoms, which was a favourable indication.
• On reassessing his movements after the technique, the joint movements were improved but SLR was unchanged.
• The technique was repeated, but more firmly and for a longer sustained period. During the performing of this technique all tingling in his foot disappeared. Following the technique movements had further improved, but
After four such treatments Mr L was greatly improved, but SLR, although improved, was nowhere near as much improved as were the joint movements. Sitting was also improved. His calf power was normal. During this stage of treatment, a scan revealed posterior disc protrusions slightly lateral to the left of the posterior longitudinal ligament at both the L4/5 and L5/S1 levels.
Because the, ?discogenic?, component was improved, and also the radicular symptoms were less (plus calf power improvement), left SLR was used as a technique and after four treatment sessions of this his left SLR became full range and pain free. However, the right SLR still felt tight and did provoke minimal left leg symptoms. It was decided to do right SLR as the treatment technique. The tightness cleared and remained clear for 4 hours.
The next treatment session consisted of performing SLR on each leg and ending the session with a repeat of the previous positioning and rotation technique. It was decided to stop treatment (unless he had an exacerbation) and review all aspects in a month.
The assessment after a month revealed that he had not only retained all of the improvement from treatment but also found he could sit, stand and be much more active. His movements were full and almost free of any discomfort. He was reviewed again after 2 months and discharged. Aspects of ‘back care’, especially in relation to the ‘weak link’, the capacity for harm to accumulate painlessly and the need to be aware of predisposing factors (see Appendix 4) were forcibly emphasized.
This presentation emphasizes that the manipulative physiotherapist must understand the pathology that may be involved in such a patient's disorder, yet she must take most notice of the changes in symptoms and signs. For example, the fact that his disorder may have been progressing towards a nerve-root compression did not prevent SLR being used as treatment, because the possible nerve condition signs were improving and the possible radicular symptoms were also improving. Nevertheless, the first SLR mobilization had to be done only once, and that once was a mild stretch. The 24-hour assessment indicated that it should be continued with care.
References
Adams, MA, Dolan, P. Spine biomechanics. J Biomech. 2005;38(10):1972–1983.
Adams, MA, Stefanakis, M, Dolan, P. Healing of a painful intervertebral dis should not be confused with reversing disc degeneration: Implications for physical therapies for discogenic pain. Clin Biomech. 2010.
Airaksinen, O, Hildebrandt, J, Mannion, AF, et al. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2004;15(Suppl 2):S192–S300.
Abenhaim, L, et al. The role of activity in the treatment of low back pain. Spine. 2000;25(4):1S–31S.
Apkarian, AV, Robinson, JP. Low back pain. IASP Pain Clinical Updates. VXIII(Issue 6), 2010.
Asenlöf, P, Denison, E, Lindberg, P. Individually tailored treatment targeting activity, motor behaviour and cognition reduces pain-related disability: a randomised controlled trial in patients with musculoskeletal pain. J Pain. 2005;6:588–603.
Asenlöf, P, Denison, E, Lindberg, P. Long-term follow-up of tailored behavioural treatment and exercise based physical therapy in persistent musculoskeletal pain: a randomised clinical trial in primary care. Eur J Pain. 2009;13:1080–1088.
Banks, K, The Maitland Concept as a clinical practice framework of NMS disorders, Maitland's Peripheral Manipulation. ed 5. Hengeveld, E, Banks, K, eds. Maitland's Peripheral Manipulation. Edinburgh:Elsevier; 2014;vol 2.
Banks, K, Hengeveld, E. Maitland's Clinical Companion: An Essential Guide for Students. Churchill Livingstone; 2010.
Billis, EV, McCarthy, CJ, Oldham, J. Subclassification of low back pain: a cross-country comparison. Eur Spine J. 2007;16:865–879.
Boal, RW, Gillette, RG. Central Neuronal Plasticity, Low Back Pain and Spinal Manipulative Therapy. J Manipulative Physiol Ther. 2004;27(5):314–326.
Bogduk, N. On the definitions and physiology of pain, referred pain and radicular pain. Pain. 2009;147:17–19.
Borkan, JM, Koes, B, Reis, J, et al. A report from the second international forum for primary care research on low back pain. Spine. 1998;23:1992–1996.
Briggs, AM, Buchbinder, R. Back pain; a national health priority area in Australia. Med J Aust. 2009;190:499–502.
Bruton, A, Conway, JH, Holgate, ST. Reliability: what is it and how is it measured? Physiotherapy. 2000;86(2):94–99.
Bullock-Saxton, J. The palpation reliability debate – the experts respond. J Bodyw Mov Ther. 2002;6(1):19–21.
Bunzli, S, Gillham, D, Esterman, A. Physiotherapy-provided operant conditioning in the management of low back pain disability: a systematic review. Physiother Res Int. 2011;16(2011):4–19.
Burton, K, Muller, G, Balagne, F, et al. Chapter 2: European Guidelines for the prevention of low back pain November 2004. Eur Spine J. 2009;15(Suppl. 2):S136–S168.
Butler, D. The sensitive nervous system. Adelaide: NOI-Group publications; 2000.
Butler, D, Moseley, L. Explain pain. Adelaide, Australia: Noi Group Publications; 2003.
Chartered Society of Physiotherapy. Scope of Practice. CSP. 2008:1–17.
Cibulka, M, Delitto, A, Koldehoff, R. Changes in innominate tilt after manipulation of the sacroiliac joint in patients with low back pain. Phys Ther. 1988;68:1359–1363.
Cleland, JA. Foreword. In: Glyn PE, Weisbach PC, eds. Clinical Prediction Rules. A Physical Therapy Reference Manual. Massachusetts: Jones and Bartlett Publisher Sudbury, 2011.
Coaz, W. Paradigmenwechsel – auch in der Physiotherapie? Physiother Bull. 1993;33:1–12.
Cook, C, Hegedus, E. Systematic review.Diagnostic utility of clinical tests for spinal dysfunction. Man Ther. 2010.
Coppieters, M, Butler, DS. Do ‘sliders’ slide and ‘tensioners’ tension? Man Ther. 2008;13:213–221.
Cott, CA, Finch, E, Gasner, D, et al. The movement continuum theory for physiotherapy. Physiother Can. 1995;47:87–95.
CSAG. Report on Back Pain. London: Clinical Standards Advisory Group. HMSO; 1994.
Dankaerts, W, O'Sullivan, P. The validity of O'Sullivan classification system (CS) for a subgroup of NS-CLBP with motor control impairment (MCI): Overview of a series of studies and review of the literature. Man Ther. 2011;16:9–14.
Davies, P. Starting again: early rehabilitation after traumatic brain injury. Berlin: Springer Verlag; 1994.
De Groot, AD. Het denken van den schaker. Eenexperimenteelpsychologischestudie. Amsterdam: Noord-HollandseUitgeversmaatschappij; 1946.
Edwards, I. Clinical Reasoning in three different fields of physical therapy - A qualitative case study. Adelaidem: School of Physiotherapy, Division of Health Sciences, University of South Australia; 2000.
Fishbain, DA. Secondary gain concept. Definition problems and its abuse in medical practice. APS Journal. 1994;3:264–273.
Flynn, T, Fritz, J, Whitman, J, et al. A Clinical Prediction Rule for Classifying Patients with Low Back Pain Who Demonstrate Short-Term Improvement With Spinal Manipulation. Spine. 2002;27(24):2835–2843.
Ford, JJ, Hahne, J. Pathoanatomy and classification of low back disorders. Man Ther. 2012.
Fordyce, WE. A behavioural perspective on pain. Br J Clin Psychol. 1982;21:313–320.
Fordyce, WE. On pain, illness and disability. J Back Musculoskeletal Res. 1995;5:259–264.
Gifford, L. Pain, the tissues and the nervous system: a conceptual model. Physiotherapy. 1998;84:27–36.
Glynn, PE, Weisbach, PC. Clinical prediction rules.a physical therapy reference manual. Massachusetts: Jones and Bartlett Publishers Sudbury; 2011.
Gowers, WR. Lumbago: Its lessons and analogues. Br Med J. 1904;1:117–121.
Greenhalgh, T, Hurwitz, B. Why study narratives. In: Greenhalgh T, Hurwitz B, eds. Narrative Based Medicine. London: British Medical Journal Press, 1998.
Hadler, NM. If you have to prove you are ill, you can't get well. Spine. 1996;20:2397–2400.
Hall, T, Quintner, J. Responses to mechanical stimulation of the upper limb in painful cervical radiculopathy. Aust J Physiother. 1996;42(4):277–285.
Hall, AM, Ferreira, PH, Maher, CC, et al. The Influence of the Therapist-Patient Relationship on Treatment Outcome in Physical Rehabilitation: A Systematic Review. Phys Ther. 2010;90:1099–1110.
Hancock, MJ, Maher, CG, Laslett, M, et al. Discussionpaper: what happened to the ‘bio’ in the bio-psycho-social model of low back pain? Eur Spine J. 2011;20:2105–2110.
Hayden, JA, van Tulder, MW, Tomlinson, G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann Intern Med. 2005;142:776–785.
Heath, J. Following the story: continuity of care in general practice. In: Greenhalgh T, Hurwitz B, eds. Narrative Based Medicine. London: British Medical Journal Press, 1998.
Hengeveld, E. Clinical Reasoning in Manueller Therapie – eine klinische Fallstudie. Manuelle Therapie. 1998;2:42–49.
Hengeveld, E. Gedanken zum Indikationsbereich der Manuallen Therapie. Teil 1, Teil 2. Manuelle Therapie. 1999;2(3):176–181.
Hengeveld, E. Psychosocial issues in physiotherapy in Switzerland: manual therapists’ perspectives and observations. London: University of East London; 2001.
Hengeveld, E. A behavioural perspective on severity and irritability. IMTA Newsletter. 2002;7:5–6.
Hengeveld, E, Banks, K. Maitland's Peripheral manipulation (vol 2), ed 5. Edinburgh, UK: Elsevier; 2014.
Hides, J, Stanton, WR, Wilson, J, et al. 2010. Retraining motor control of abdominal muscles among elite cricketers with low back pain. Scand J Med Sci Sports. 2010;20:834–842.
Higgs, J, Jones, M, Loftus, S, et al. Clinical Reasoning in the Health Professions, ed 3. Amsterdam: Elsevier Butterworth Heinemann; 2008.
Hodges, PW. Pain and motor control: from laboratory to rehabilitation. J Electromyogr Kinesiol. 2011;21:220–228.
Huijbregts, PA. Introduction. In: Glyn PE, Weisbach PC, eds. Clinical Prediction Rules. A Physical Therapy Reference Manual. Massachusetts: Jones and Bartlett Publishes Sudbury, 2011.
IFOMPT (International Federation of Orthopaedic Manipulative Physiotherapists). Educational Standards in Orthopaedic Manipulative Physical Therapy. www.ifompt.com, 2008.
Jensen, GM, Gwyer, J, et al. Expertise in Physical Therapy Practice. Boston: Butterworth-Heinemann; 1999.
Johnson, AJ, Godges, JJ, Zimmerman, GJ, et al. The effect of anterior versus posterio glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthop Sports Phys Ther. 2007;37(3):88–99.
Johnson, RE, Jones, GT, Wiles, NJ, et al. Active exercise, education and cognitive behavioral therapy for persistent disabling low back pain. A randomised clinical trial. Spine. 2007;32(15):1578–1585.
Jones, M. Clinical reasoning and pain. Man Ther. 1995;1:17–24.
Jull, G, Bogduk, N, Marsland, A. The accuracy of manual diagnosis for cervical zygapophysial joint pain syndromes. Med J Aust. 1988;148:233–236.
Jull, G, Zito, G, Trott, P, et al. Inter-examiner reliability to detect painful upper cervical joint dysfunction. Aust J Physiother. 1997;43:125–129.
Kamper, SJ, Maher, CG, Hancock, MJ, et al. Treatment-based subgroups of low back pain: A guide to appraisal of research studies and a summary of current evidence. Best Pract Res Clin Rheumatol. 2010;24:181–191.
Keating, J, Matyas, T. Unreliable inferences from reliable measurements. Aust J Physiother. 1998;44:5–10.
Kendall, NAS, Linton, SJ, Main, CJ, et al. Guide to assessing psychosocial yellow flags in acute low back pain: risk factors for long-term disability and work loss. Wellington, New Zealand: Accident Rehabilitation & Compensation Insurance Corporation of New Zealand and the National Health Committee; 1997.
Kent, PM, Keating, J. Do primary-care clinicians think that nonspecific low back pain is one condition? Spine. 2004;29(9):1022–1031.
Kent, PM, Kjaer, P. The efficacy of targeted interventions for modifiable psychosocial risk factors of persistent nonspecific low back pain. A systematic review. Man Ther. 2012.
Kent, PM, Keating, JL, Buchbinder, R. Searching for a conceptual framework for nonspecific low back pain. Man Ther. 2009;14:387–396.
Kent, PM, Keating, JL, Taylor, NF. Primary care clinicians use variable methods to assess acute nonspecific low back pain and usually focus on impairments. Man Ther. 2009;14:88–100.
Kenwright, J, Richardson, JB, Cunningham, JL, et al. Axial movement and tibial fractures – a controlled randomized trial of treatment. J Bone Joint Surg. 1991;73-B:654–659.
Kleinmann, A. The illness narratives: suffering, healing and the human condition. New York: Basic Books Harpers; 1988.
Krouwel, O, Hebron, C, Willett, E. An investigation into the potential hypoalgesic effects of different amplitudes of PA mobilisations on the lumbar spine as measured by pressure pain thresholds (PPT). Man Ther. 2010;15:7–12.
Lando, A. Temperature testing by manipulative physiotherapists in spinal examination. In Boyling JD, Palastanga N, eds.: Grieve's Modern Manual Therapy, ed 2, Edinburgh: Churchill-Livingstone, 1994.
MacDermid, JC, Walton, D, Avery, S, et al. Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther. 2009;39(5):400–417.
Macedo, LG, Maher, CG, Latimer, J, et al. Motor control exercises for persistent, nonspecific low back pain: a systematic review. Phys Ther. 2009;89(1):9–25.
Macedo, LG, Latimer, J, Maher, CG, et al. Effect of motor control exercises versus graded activity in patients with chronic nonspecific low back pain: A randomiszed controlled trial. Phys Ther. 2012;92(3):363–377.
Makofsky, H, Panicker, S, Abbruzzese, J, et al. Immediate effect of Grade IV inferior hip joint mobilisation on hip abductor torque: a pilot study. J Man Manipulative Ther. 2007;15(2):103–111.
Maher, C, Latimer, J, Refshauge, K. Prescription of activity for low back pain: what works? Aust J Physiother. 1999;45:121–132.
Main, CJ, Spanswick, CS. Pain management – a multidisciplinary approach. Edinburgh: Churchill Livingstone; 2000.
Maitland, GD. Movement of pain-sensitive structures in the vertebral canal in a group of physiotherapy students. S Afr J Physiother. 1980;36:4–12.
Maitland, GD. Vertebral Manipulation, ed 5. Oxford: Butterworth-Heinemann; 1986.
Maitland, GD. The development of manipulative physiotherapy. SVMP-Bulletin. 1995;10:3–5.
Maitland, GD, Hengeveld, E, Banks, K, et al. Maitland's Vertebral manipulation, ed 7. Edinburgh: Elsevier. Butterworth-Heinemann; 2005.
Maluf, KS, Sahrmann, SA, Van Dillen, LR. Use of a classification system to guide nonsurgical management of a patient with chronic low back pain. Phys Ther. 2000;80:1097–1111.
Mattingly, C. What is clinical reasoning? Am J Occup Ther. 1991;45:998–1005.
McGill, SM. The biomechanics of low back injury: implications on current practice in industry and in the clinic. J Biomech. 1997;30(5):465–475.
May, S, Aina, A. Centralization and directional preference: a systematic review. Man Ther. 2012.
McCarthy, CJ, Arnall, FA, Strimpakos, N, et al. The biopsychosocial classification of nonspecific low back pain: a systematic review. Phys Ther Rev. 2004;9:17–30.
McKenzie, R. The lumbar spine. Mechanical diagnosis and therapy. New Zealand: Spinal Publications; 1981.
Mead, J. Patient partnership. Physiotherapy. 2000;86:282–284.
Moseley, L. Evidence for the direct relationship( between cognitive and physical change during an education intervention in people with chronic low back pain. Eur J Pain. 2004;8(1):39–45.
Moss, P, Sluka, K, Wright, A. The initial effects of knee joint mobilisation on oateoarthritic hyperalgesia. Man Ther. 2007;12:109–118.
Nachemson AL, Jonsonn E, eds. Back and neck pain: Scientific evidence of Cause, diagnosis and treatment. Swedish Council of technology assessment and health care (SBU). Philidelphia: Lippincott Willams and Wilkins, 2000.
Nakao, M, Shinozaki, Y, Nolido, N, et al. Responsiveness of hypochondriacal patients with chronic low-back pain to cognitive-behavioral therapy. Psychosomatics. 2012;53:139–147.
NICE. Low back pain: early management of persistent non-specific low back pain. National Institute for Health and Clinical Excellence (UK). 2009:1–10.
O'Neill, CW, Kurgansky, ME, Derby, R, et al. Disc stimulation and patterns of referred pain. Spine. 2002;27(4):2776–2781.
O'Sullivan, P. 2005. Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanisms. Man Ther. 2005;10(4):242–255.
O'Sullivan, P. It's time for change with the management of non-specific chronic low back pain. Editorial. Br J Sports Med. 2011:4–6.
Paterson, C. 1996. Measuring outcomes in primary care: a patient generated measure, MYMOP, compared with the SF-36 health survey. BMJ. 1996;312:1016–1020.
Panjabi, M. The stabilising system of the spine: Part II Neutral zone and instability hypothesis. J Spinal Disord. 1992;5(4):390–396.
Paungmali, A, O'Leary, S, Souvlis, T, et al. Hypoalgesic and sympathoexcitatory effects of mobilisation with movement for lateral epicondylalgia. Phys Ther. 2003;83:374–383.
Perry, J, Green, A. An investigation into the effects of a unilateral mobilisation techniques on peripheral sympathetic nervous system activity in the lower limbs. Man Ther. 2008;13:492–499.
Perry, J, Green, A, Watson, P. A preliminary investigation into the magnitude of effect of lumbar extension exercises and a segmental rotatory manipulation on sympathetic nervous system activity. Man Ther. 2011;16(2):190–195.
Phillips, DR, Twomey, LT. A comparison of manual diagnosis with a diagnosis established with a lumbar block procedure. Man Ther. 1996;2:82–87.
Pilowsky, I. Abnormal illness behaviour. Chichester: John Wiley; 1997.
Pincus, T, Vlaeyen, JWS, Kenall, NAS, et al. Cognitive behavioral therapy and psychosocial factors in low back pain – directions for the future. Spine. 2002;27(5):E133–E138.
Prochaska, J, DiClemente, C. Stages of change and decisional balance for twelve problem behaviours. Health Psychol. 1994;13(1):39–46.
Quebec Task Force on Spinal Disorders. Scientific approach to the assessment and management of activity-related spinal disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal Disorders. Spine. 1987;12(Suppl 7):S1–S59.
RCGP. Clinical Guidelines for the Management of Acute Low Back Pain. London: Royal College of General Practitioners; 1999.
Richardson, C, Hodges, P, Hides, J. Therapeutic exercise for motor control and lumbopelvic stabilisation: a motor control approach for the treatment and prevention of low back pain. Edinburgh: Elsevier Churchill Livingstone; 2004.
Sahrmann, S. Movement system impairment syndromes of the extremities, Cervial and Thoracic Spine, ed 2. St Louis: Elsevier Mosby; 2011.
Sayres, LR. Defining irritability: the measure of easily aggravated symptoms. Br J Ther Rehabil. 1997;4:18–20.
Schafer, A, Hall, T, Muller, G, et al. Outcomes differ between subgroups of patients with low back and leg pain following neural manual therapy: a prospective cohort study. Eur Spine J. 2011;20:482–490.
Schön, DA. The reflective practitioner. How professionals think in action. Aldershurt: Arena; 1983.
Schmidt, H, Boshuyzen, H. On acquiring expertise in medicine. Educ Psych Rev. 1993;5(3):205–221.
Shacklock, M. Clinical neurodynamics: a new system of musculoskeletal treatment. Edinburgh: Elsevier. Churchill Livingstone; 2005.
Sheehan, NJ. Magnetic resonance imaging for low back pain: indications and limitations. Ann Rheum Dis. 2010;69:7–11.
Sims, K. Assessment and treatment of hip osteoarthritis. Man Ther. 4(3), 1999. [136–114].
Slater, SL, Ford, JJ, Richards, MC, et al. The effectiveness of sub-group specific manual therapy for low back pain: a systematic review. Man Ther. 2012;17(2012):201–212.
Smart, K, Blake, C, Staines, A, et al. Self-reporting pain severity, quality of life, disability, anxiety and depression in patients classified with ‘nociceptive’, ‘peripheral neurogenic’ and ‘central sensitisation’ pain. The discriminant validity of mechanism- based classification of low back (+/− leg) pain. Man Ther. 2012;17:119–125.
Stier-Jarmer, M, Cieza, A, Borchers, M, et al. How to apply the ICF and ICF core sets for low back pain. Clin J Pain. 2009;25:29–38.
Thomas-Edding D: Clinical problem solving in physical therapy and its implications for curriculum development. Proceedings of the 10th International Congress of the World Confederation of Physical Therapy, Sydney, 1987.
Thomson, D. Counseling and clinical reasoning: the meaning of practice. Br J of Therapy and Rehabilitation. 1998;5:88–94.
Turner, JA, LeResche, L, Korff Von, M, et al. Backpain in primary care – patient characteristics, content of initial visit and short-term outcome. Spine. 1998;23:463–469.
Van Baar, ME, Assendelft, WJ, Dekker, J, et al. Effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee. A systematic review of randomized clinical trials. Arthritis Rheum. 2000;42:1361–1369.
Van Tulder, M, Becker, A, Bekkering, T, et al, European Guidelines for the management of acute low back pain. Eur Spine J. 2006;(Suppl 15):131–300.
Vermeulen, HM, Rozing, PM, Obermann, WR, et al. Comparison of high-grade and low grade mobilisation techniques in the managemnt of adhesive capsulitis of the shoulder: randomized controlled trial. Phys Ther. 2006;86(3):355–368.
Vlaeyen, JWS, Crombez, G. Fear of movement/(re)injury, avoidance and pain disability in chronic low back pain patients. Man Ther. 1999;4:187–195.
Vleeming, A, Albert, HB, Östgaard, HC, et al. European Guidelines for the diagnosis and treatment of pelvic girdle pain. Eur Spine J. 2008;17:794–819.
Waddell, G. A new clinical model for the treatment of low back pain. Spine. 1987;12:632–644.
Waddell, G. The Back Pain Revolution. Edinburgh: Elsevier. Churchill Livingstone; 1998.
Waddell, G. The back pain revolution, ed 2. Edinburgh: Elsevier. Churchill-Livingstone; 2004.
Walsh, J, Hall, T. Reliability, validity and diagnostic accuracy of palpation of the sciatic, tibial and common peroneal nerves in the examination of low back related leg pain. Man Ther. 2009;14(2006):623–629.
Wand, BM, O'Connell, NE. Chronic non-specific low back pain – subgroups or a single mechanism? MBC Musculoskelet Disord. 2008;9:11.
Watson, P, Kendall, N. Assessing psychosocial yellow flags. In Gifford LS, ed.: Topical Issues in Pain, ed 2, Swanpool, UK: CNS Press, 2000.
Watters, W, Baisdenn, J, et al. Degenerative lumbar spinal stenosis: an evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar pinal stenosis. Spine J. 2008;8:305–310.
WHO. ICF – International Classification of Functioning, Disability and Health. Geneva: WHO; 2001.
WHO. WHO global strategy on diet, physical activity and health – A framework to monitor and evaluate implementation. Geneva: World Health Organization; 2008.
WHO/EUROPE, What is the best way to treat low back pain?. Health Evidence Network/Publications; 2000. www.euro.who.int.
Yeris, S, Makofsky, H, Byrd, C, et al. Effect of mobilisation of the anterior hip capsule on gluteus maximus strength. J Man Manipulative Ther. 2002;10(4):218–224.
Yeo, H, Wright, A. Effects of performing a passive accessory mobilization technique in patients with lateral ankle pain. Man Ther. 2011;16:373–377.
†MYMOP is a patient-generated, or individualized, outcome questionnaire. It is problem-specific but includes general wellbeing. It is applicable to all patients who present with symptoms, and these can be physical, emotional or social. On the first occasion the questionnaire is completed within the consultation, or with some confidential help. The patient chooses one or two symptoms that they are seeking help with, and that they consider to be the most important. They also choose an activity of daily living that is limited or prevented by this problem. These choices are written down in the patient's own words and the patient scores them for severity over the past week on a seven-point scale. Lastly, wellbeing is scored on a similar scale. On follow-up questionnaires the wording of the previously chosen items is unchanged, and follow-up questionnaires may be administered by post if required. (Source: www.sites.pcmd.ac.uk/mymop/)