Musculoskeletal System
Outline

http://evolve.elsevier.com/Jarvis/
• Bedside Assessment Summary Checklist
• Physical Examination Summary Checklist
• Quick Assessment for Common Conditions
Structure and Function
The musculoskeletal system consists of the body’s bones, joints, and muscles. Humans need this system (1) for support to stand erect and (2) for movement. The musculoskeletal system also functions (3) to encase and protect the inner vital organs (e.g., brain, spinal cord, heart), (4) to produce the red blood cells in the bone marrow (hematopoiesis), and (5) as a reservoir for storage of essential minerals, such as calcium and phosphorus in the bones.
Components of the Musculoskeletal System
The skeleton is the bony framework of the body. It has 206 bones, which support the body like the posts and beams of a building. Bone and cartilage are specialized forms of connective tissue. Bone is hard, rigid, and very dense. Its cells are continually turning over and remodeling. The joint (or articulation) is the place of union of two or more bones. Joints are the functional units of the musculoskeletal system because they permit the mobility needed for activities of daily living.
Nonsynovial orSynovial Joints
In nonsynovial joints, the bones are united by fibrous tissue or cartilage and are immovable (e.g., the sutures in the skull) or only slightly movable (e.g., the vertebrae). Synovial joints are freely movable because they have bones that are separated from each other and are enclosed in a joint cavity (Fig. 22-1). This cavity is filled with a lubricant, or synovial fluid. Just like grease on gears, synovial fluid allows sliding of opposing surfaces, and this sliding permits movement.
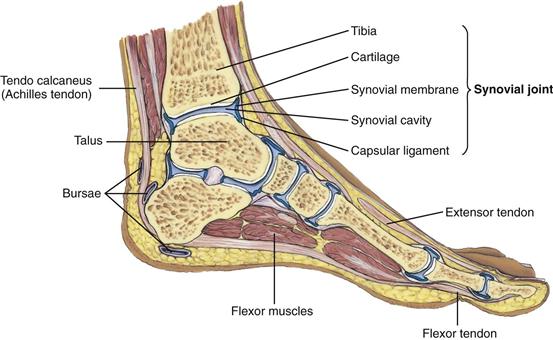
In synovial joints, a layer of resilient cartilage covers the surface of opposing bones. Cartilage is avascular; it receives nourishment from synovial fluid that circulates during joint movement. It is a very stable connective tissue with a slow cell turnover. It has a tough, firm consistency, yet is flexible. This cartilage cushions the bones and gives a smooth surface to facilitate movement.
The joint is surrounded by a fibrous capsule and is supported by ligaments. Ligaments are fibrous bands running directly from one bone to another that strengthen the joint and help prevent movement in undesirable directions. A bursa is an enclosed sac filled with viscous synovial fluid, much like a joint. Bursae are located in areas of potential friction (e.g., subacromial bursa of the shoulder, prepatellar bursa of the knee) and help muscles and tendons glide smoothly over bone.
Muscles
Muscles account for 40% to 50% of the body’s weight. When they contract, they produce movement. Muscles are of three types: skeletal, smooth, and cardiac. This chapter is concerned with skeletal, or voluntary, muscles—those under conscious control.
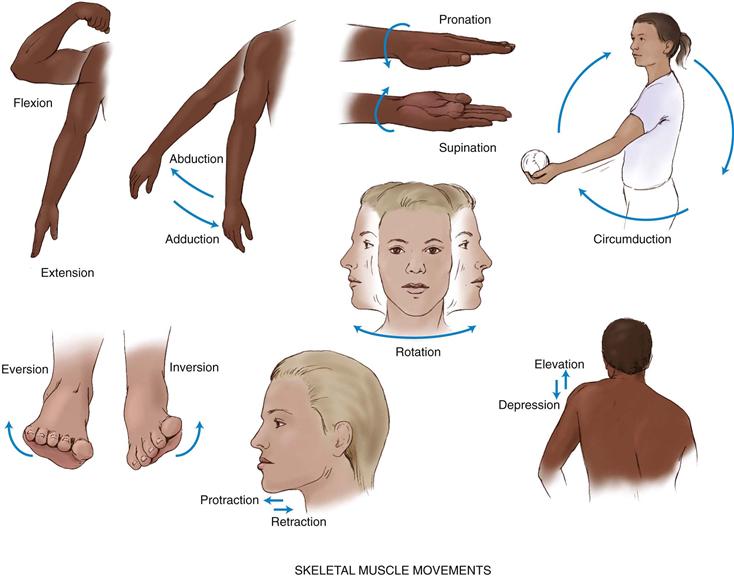
Each skeletal muscle is composed of bundles of muscle fibers, or fasciculi. The skeletal muscle is attached to bone by a tendon—a strong fibrous cord. Skeletal muscles produce the following movements (Fig. 22-2):
1. Flexion—bending a limb at a joint
2. Extension—straightening a limb at a joint
3. Abduction—moving a limb away from the midline of the body
4. Adduction—moving a limb toward the midline of the body
5. Pronation—turning the forearm so that the palm is down
6. Supination—turning the forearm so that the palm is up
7. Circumduction—moving the arm in a circle around the shoulder
8. Inversion—moving the sole of the foot inward at the ankle
9. Eversion—moving the sole of the foot outward at the ankle
10. Rotation—moving the head around a central axis
11. Protraction—moving a body part forward and parallel to the ground
12. Retraction—moving a body part backward and parallel to the ground
22-2 Copyright © (2006) © Pat Thomas, 2006.
Temporomandibular Joint
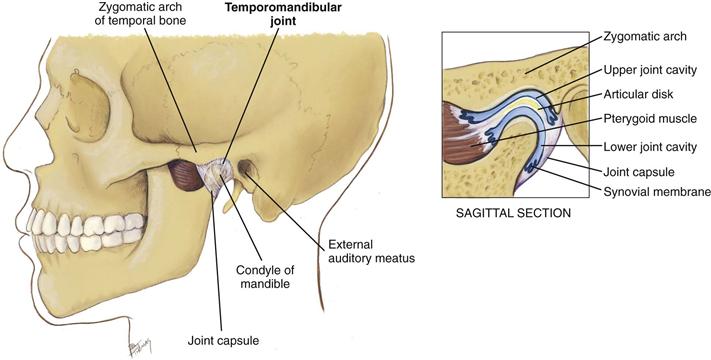
The temporomandibular joint (TMJ) is the articulation of the mandible and the temporal bone (Fig. 22-3). You can feel it in the depression anterior to the tragus of the ear. The TMJ permits jaw function for speaking and chewing. The joint allows three motions: (1) hinge action to open and close the jaws; (2) gliding action for protrusion and retraction; and (3) gliding for side-to-side movement of the lower jaw.
22-3
Spine
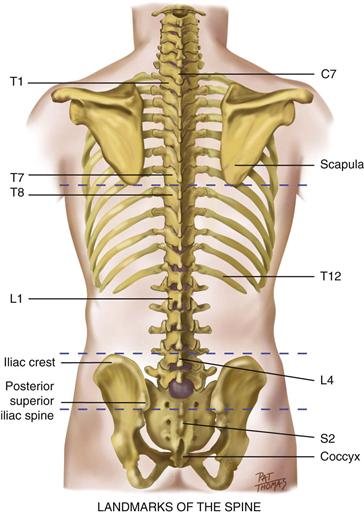
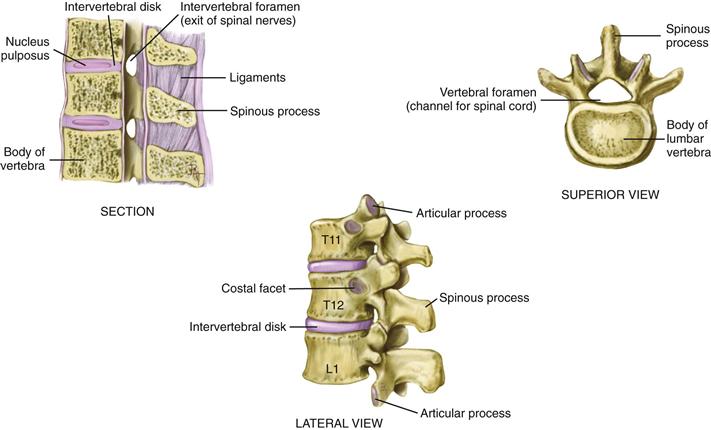
The vertebrae are 33 connecting bones stacked in a vertical column (Fig. 22-4). You can feel their spinous processes in a furrow down the midline of the back. The furrow has paravertebral muscles mounded on either side down to the sacrum, where it flattens. Humans have 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 3 or 4 coccygeal vertebrae. The following surface landmarks will orient you to their levels:
• The spinous processes of C7 and T1 are prominent at the base of the neck.
• The inferior angle of the scapula normally is at the level of the interspace between T7 and T8.
• An imaginary line connecting the highest point on each iliac crest crosses L4.
• An imaginary line joining the two symmetric dimples that overlie the posterior superior iliac spines crosses the sacrum.
22-4
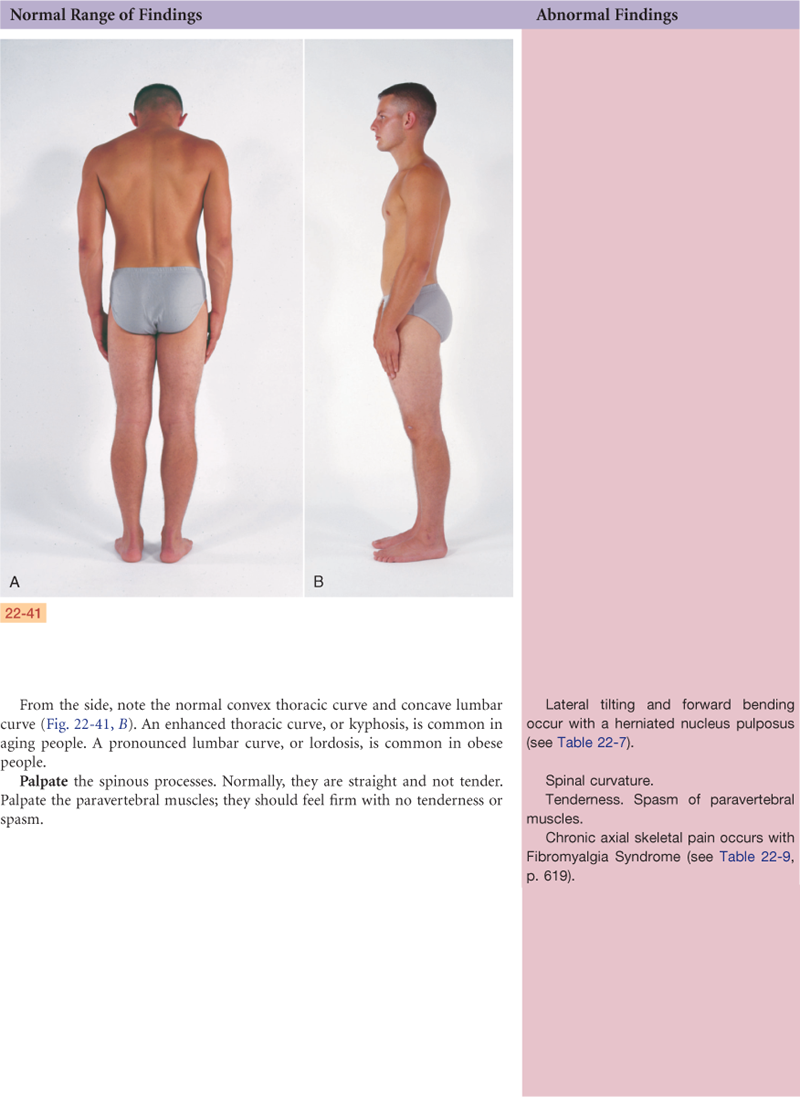
A lateral view shows that the vertebral column has four curves (a double-S–shape) (Fig. 22-5). The cervical and lumbar curves are concave (inward or anterior), and the thoracic and sacrococcygeal curves are convex. The balanced or compensatory nature of these curves, together with the resilient intervertebral disks, allows the spine to absorb a great deal of shock.
22-5
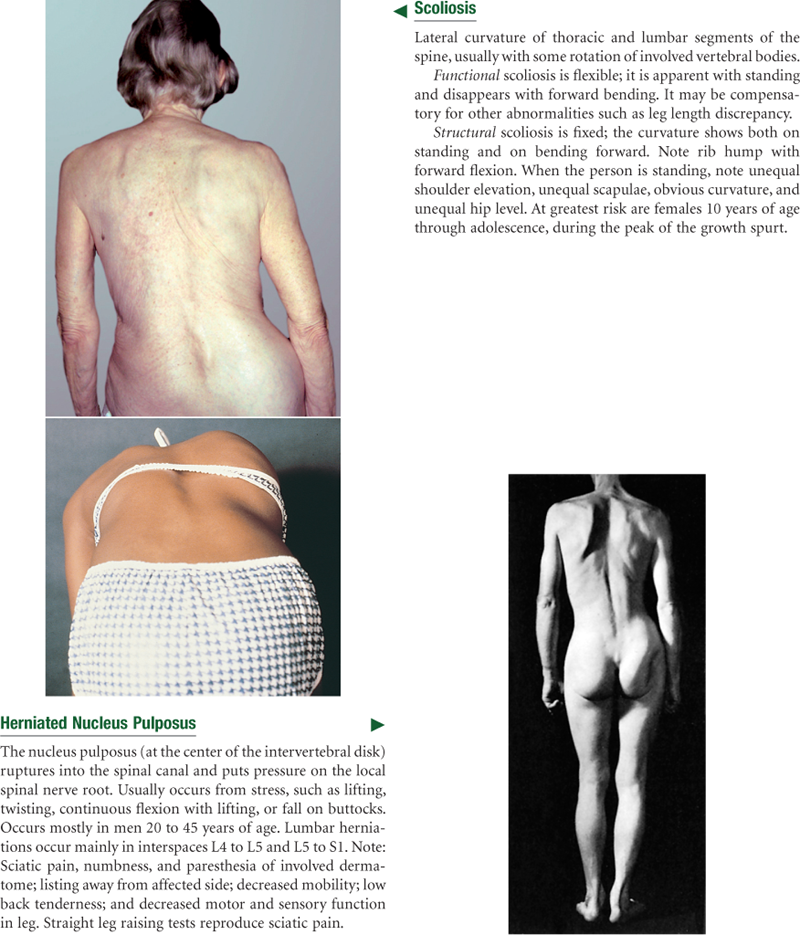
The intervertebral disks are elastic fibrocartilaginous plates that constitute one fourth of the length of the column (Fig. 22-6). Each disk center has a nucleus pulposus made of soft, semifluid, mucoid material that has the consistency of toothpaste in the young adult. The disks cushion the spine like a shock absorber and help it move. As the spine moves, the elasticity of the disks allows compression on one side, with compensatory expansion on the other. Sometimes compression can be too great. The disk then can rupture and the nucleus pulposus can herniate out of the vertebral column, compressing on the spinal nerves and causing pain.
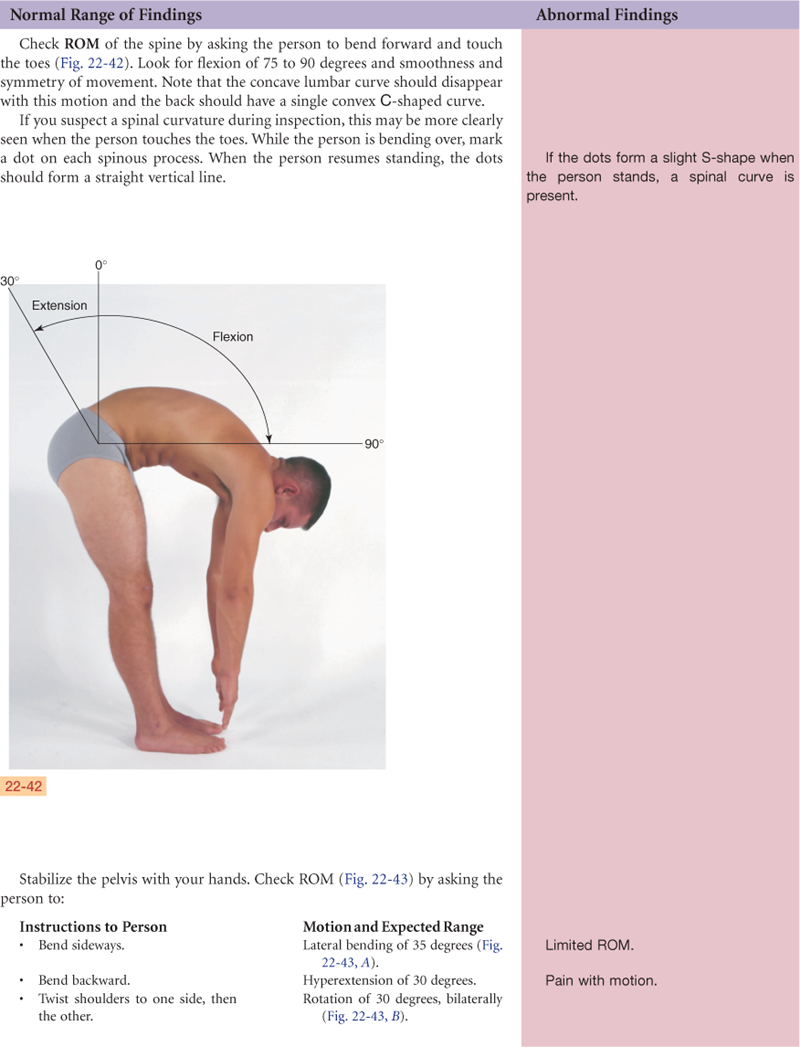
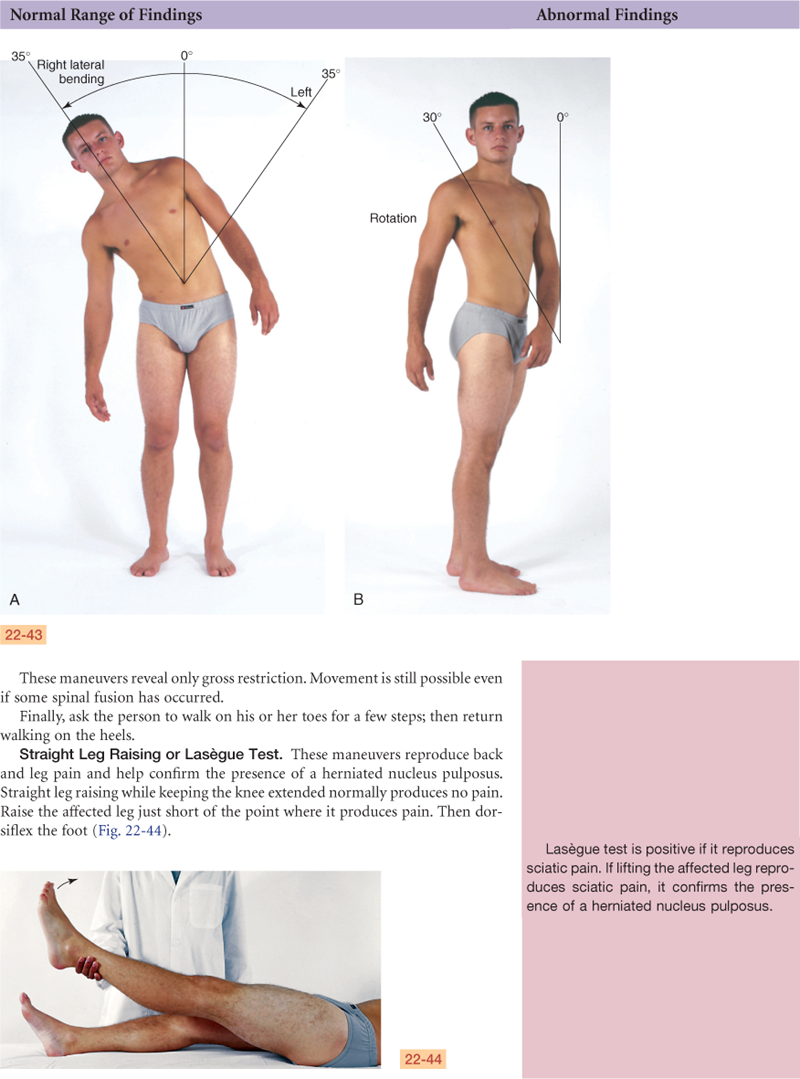
The unique structure of the spine enables both upright posture and flexibility for motion. The motions of the vertebral column are flexion (bending forward), extension (bending back), abduction (to either side), and rotation.
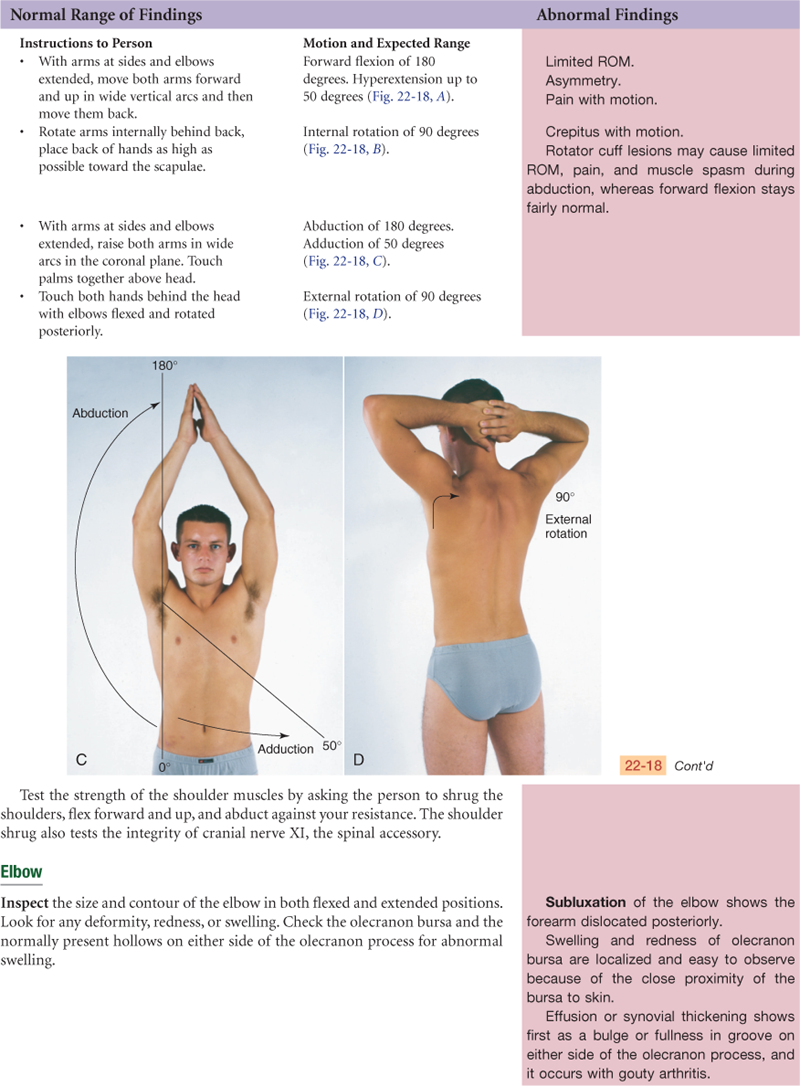
Shoulder
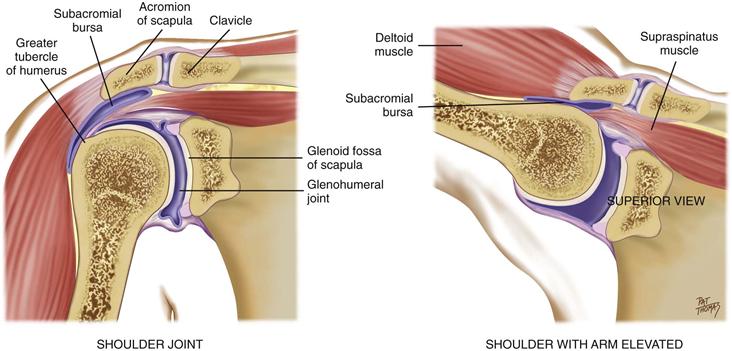
The glenohumeral joint is the articulation of the humerus with the glenoid fossa of the scapula (Fig. 22-7). Its ball-and-socket action allows great mobility of the arm on many axes. The joint is enclosed by a group of four powerful muscles and tendons that support and stabilize it. Together these are called the rotator cuff of the shoulder. The large subacromial bursa helps during abduction of the arm, so that the greater tubercle of the humerus moves easily under the acromion process of the scapula.
22-7
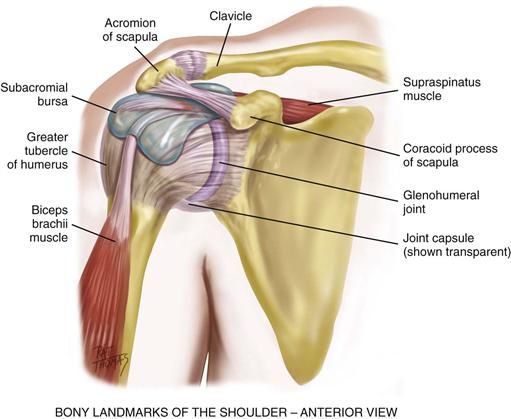
The bones of the shoulder have palpable landmarks to guide your examination (Fig. 22-8). The scapula and the clavicle connect to form the shoulder girdle. You can feel the bump of the scapula’s acromion process at the very top of the shoulder. Move your fingers in a small circle outward, down, and around. The next bump is the greater tubercle of the humerus a few centimeters down and laterally, and from that the coracoid process of the scapula is a few centimeters medially. These surround the deeply situated joint.
22-8
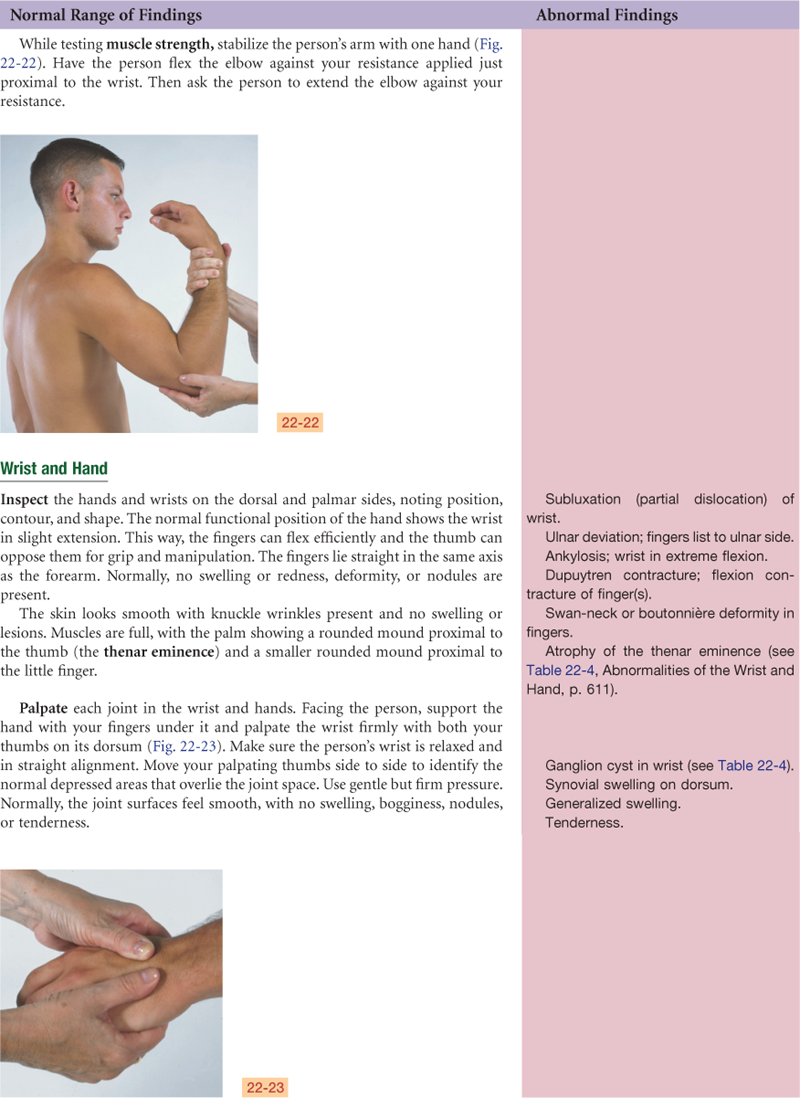
Elbow
The elbow joint contains the three bony articulations of the humerus, radius, and ulna of the forearm (Fig. 22-9). Its hinge action moves the forearm (radius and ulna) on one plane, allowing flexion and extension. The olecranon bursa lies between the olecranon process and the skin.
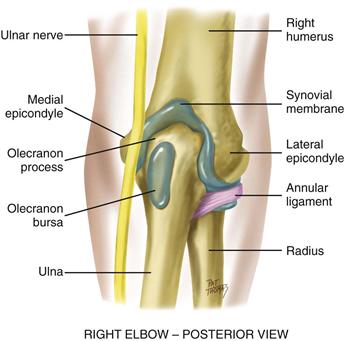
22-9
Palpable landmarks are the medial and lateral epicondyles of the humerus and the large olecranon process of the ulna in between them. The sensitive ulnar nerve runs between the olecranon process and the medial epicondyle.
The radius and ulna articulate with each other at two radioulnar joints, one at the elbow and one at the wrist. These move together to permit pronation and supination of the hand and forearm.
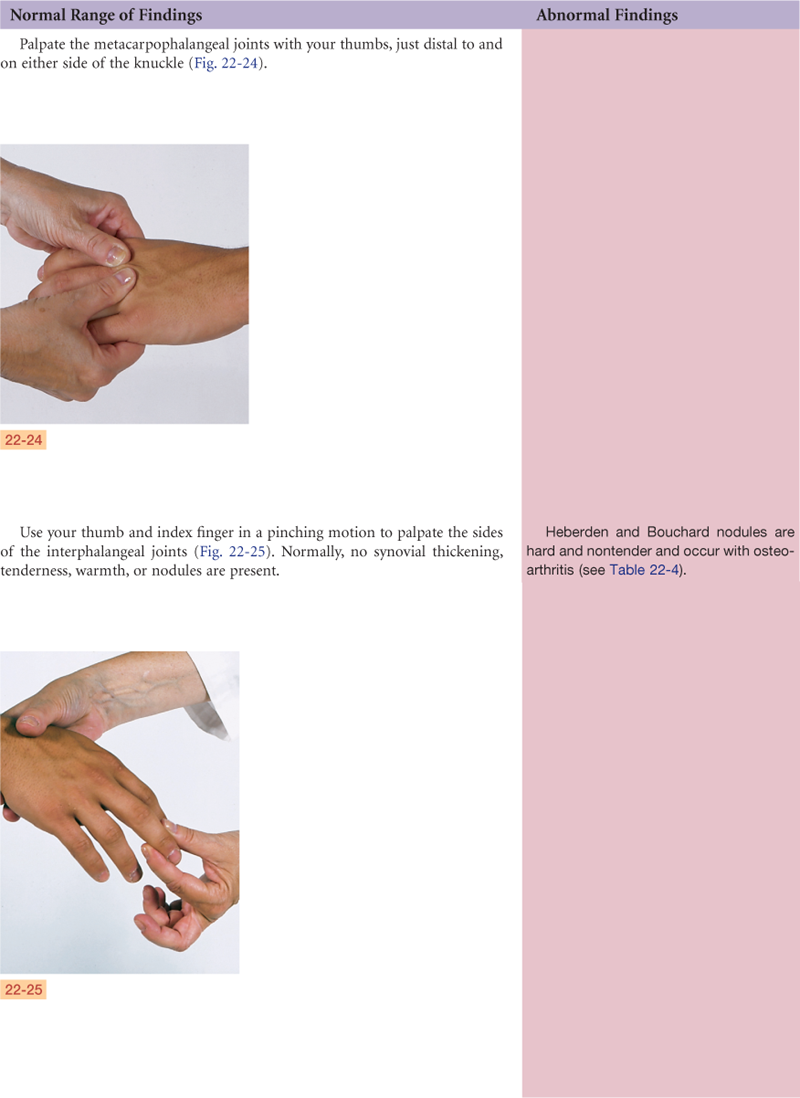
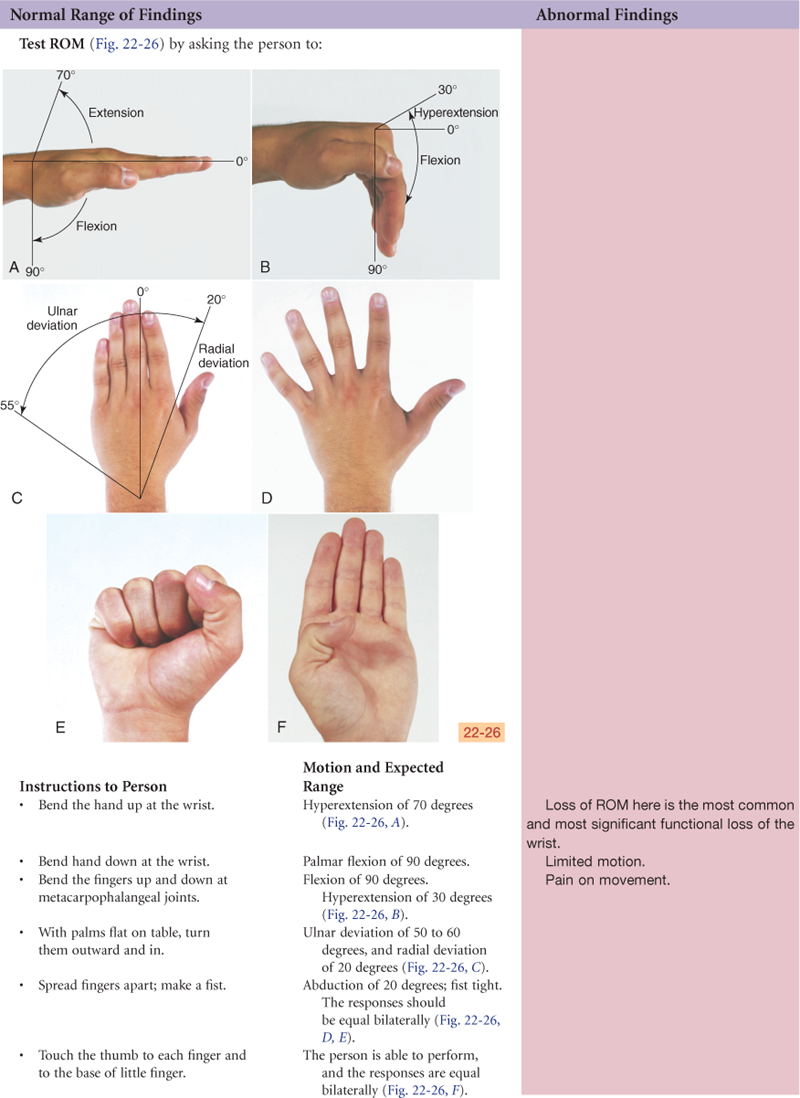
Wrist and Carpals
Of the body’s 206 bones, over half are in the hands and feet. The wrist, or radiocarpal joint, is the articulation of the radius (on the thumb side) and a row of carpal bones (Fig. 22-10). Its condyloid action permits movement in two planes at right angles: flexion and extension, and side-to-side deviation. You can feel the groove of this joint on the dorsum of the wrist.
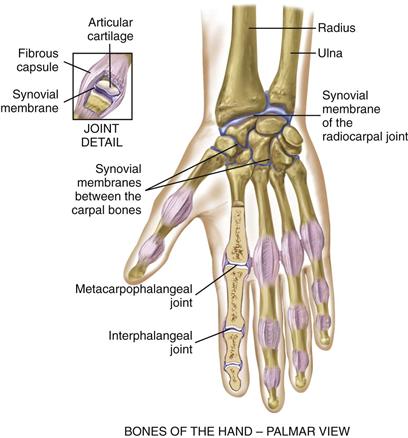
22-10
The midcarpal joint is the articulation between the two parallel rows of carpal bones. It allows flexion, extension, and some rotation. The metacarpophalangeal and the interphalangeal joints permit finger flexion and extension. The flexor tendons of the wrist and hand are enclosed in synovial sheaths.
Hip
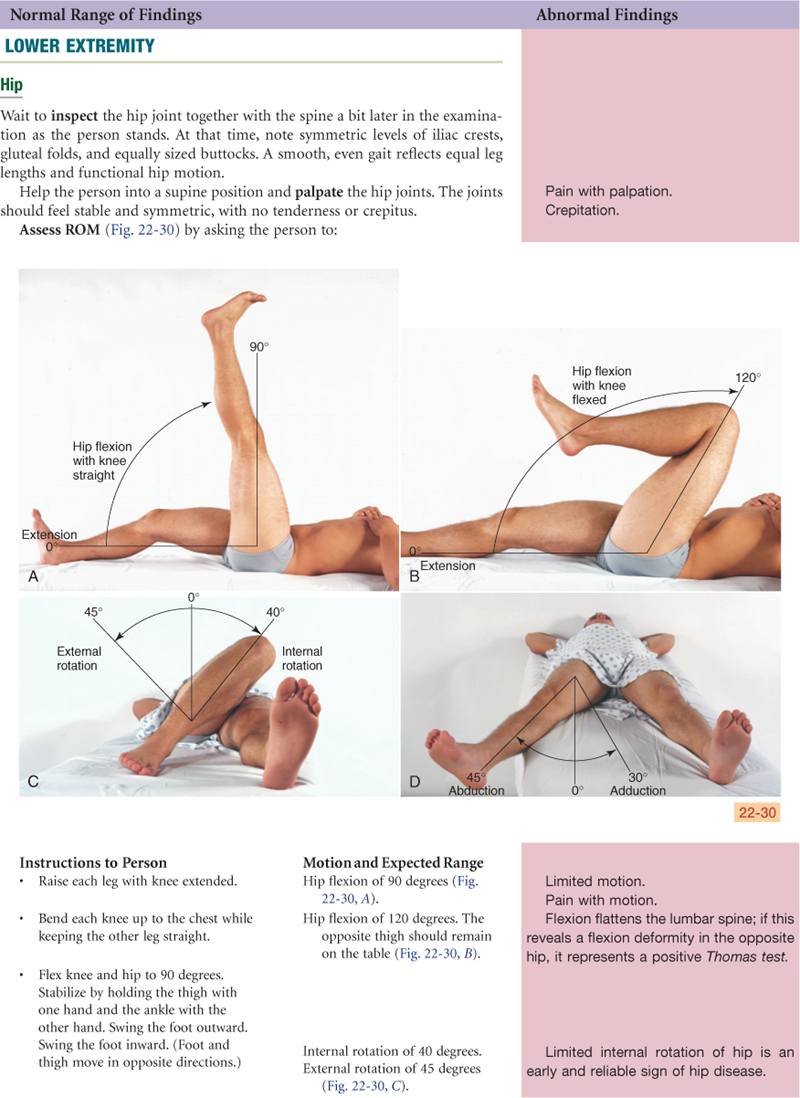
The hip joint is the articulation between the acetabulum and the head of the femur (Fig. 22-11). As in the shoulder, ball-and-socket action permits a wide range of motion (ROM) on many axes. The hip has somewhat less ROM than the shoulder, but it has more stability as befits its weight-bearing function. Hip stability is due to powerful muscles that spread over the joint, a strong fibrous articular capsule, and the very deep insertion of the head of the femur. Three bursae facilitate movement.
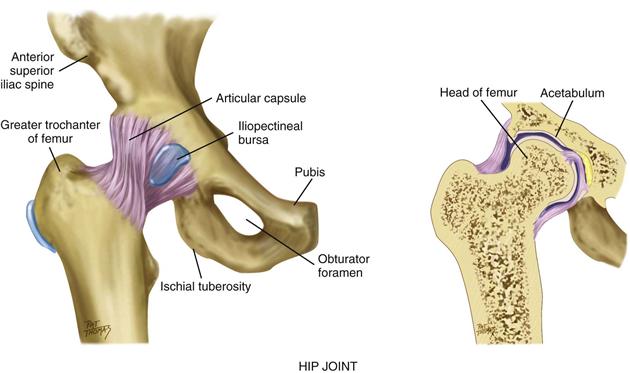
22-11
Palpation of these bony landmarks will guide your examination. You can feel the entire iliac crest, from the anterior superior iliac spine to the posterior. The ischial tuberosity lies under the gluteus maximus muscle and is palpable when the hip is flexed. The greater trochanter of the femur is normally the width of the person’s palm below the iliac crest and halfway between the anterior superior iliac spine and the ischial tuberosity. Feel it when the person is standing, in a flat depression on the upper lateral side of the thigh.
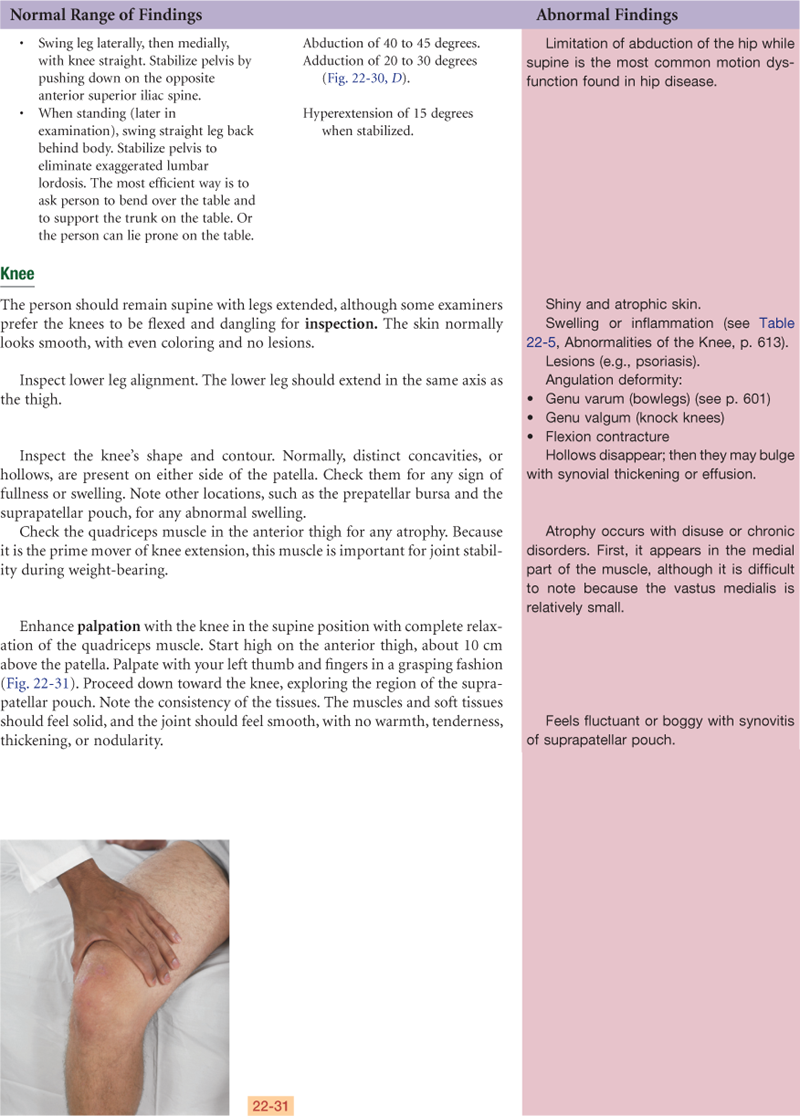
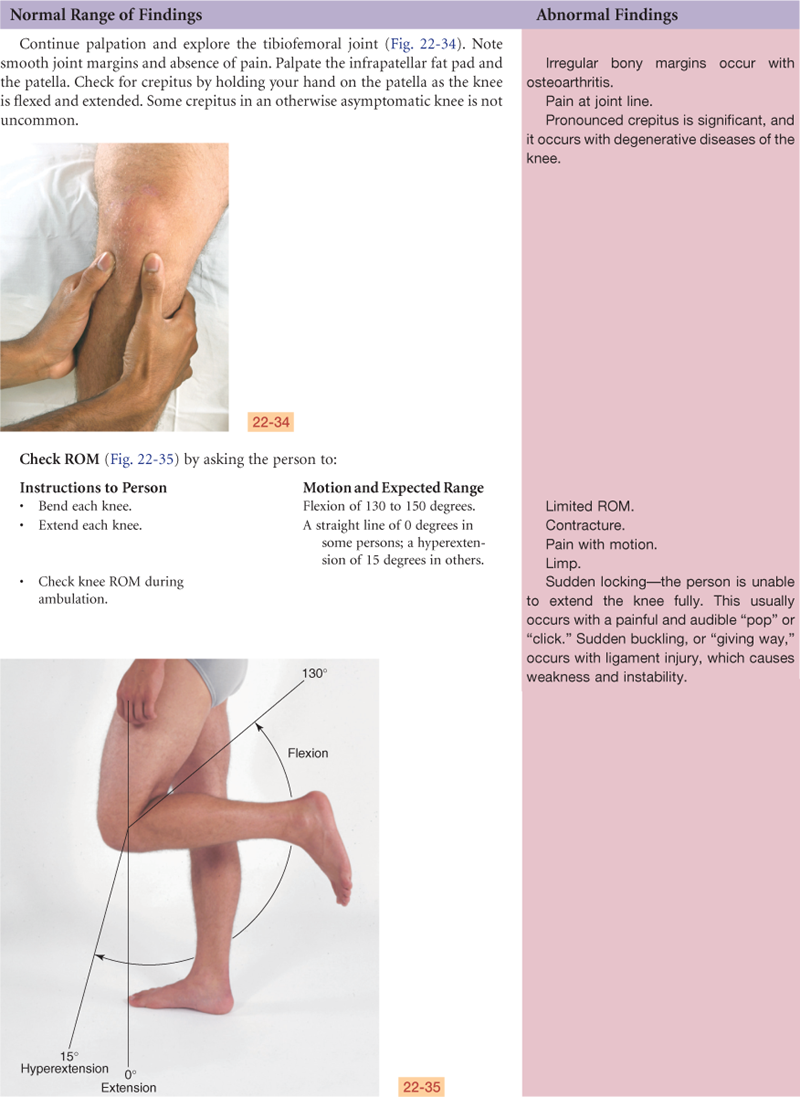
Knee
The knee joint is the articulation of three bones—the femur, the tibia, and the patella (kneecap)—in one common articular cavity (Fig. 22-12). It is the largest joint in the body and is complex. It is a hinge joint, permitting flexion and extension of the lower leg on a single plane.
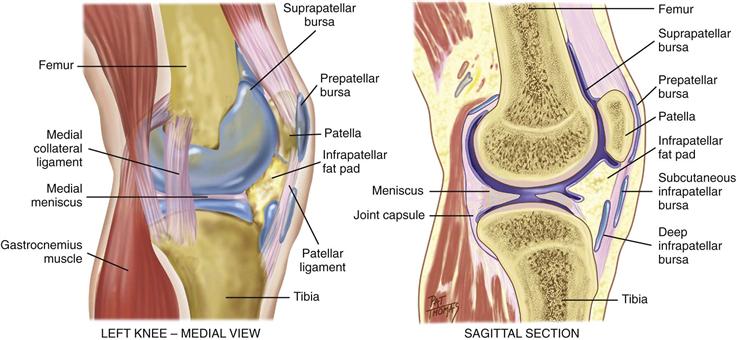
22-12
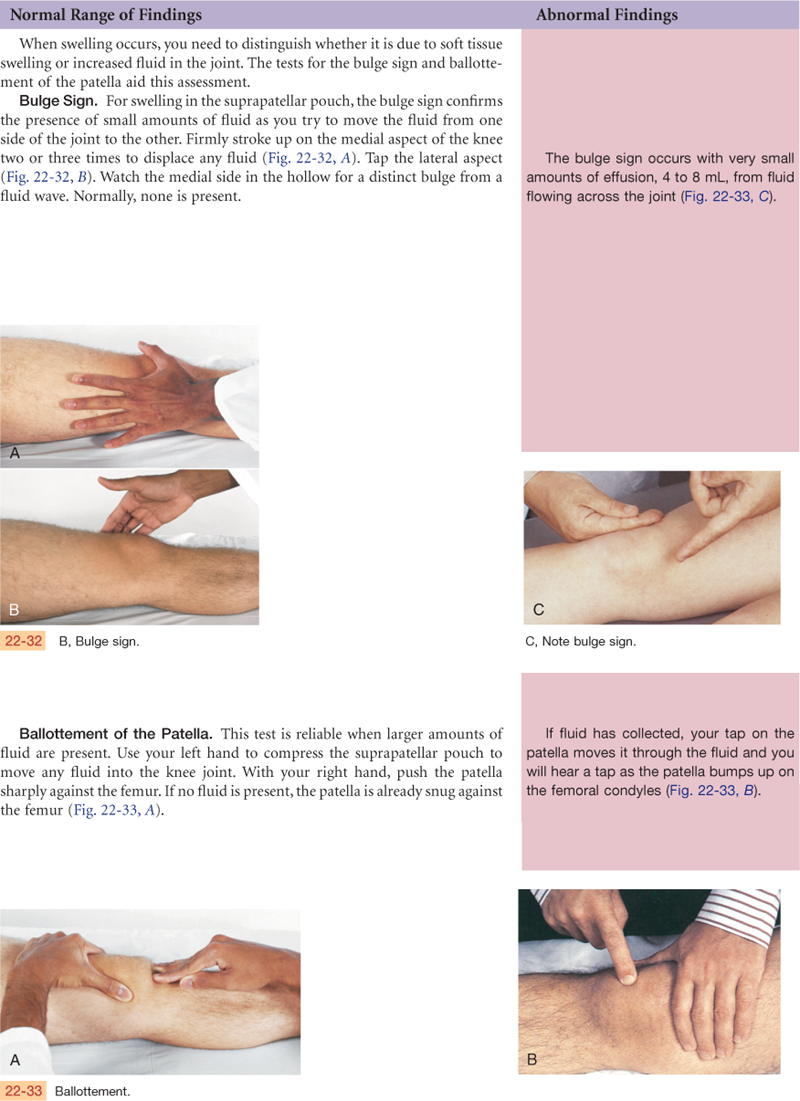
The knee’s synovial membrane is the largest in the body. It forms a sac at the superior border of the patella, called the suprapatellar pouch, which extends up as much as 6 cm behind the quadriceps muscle. Two wedge-shaped cartilages, called the medial and lateral menisci, cushion the tibia and femur. The joint is stabilized by two sets of ligaments. The cruciate ligaments (not shown) crisscross within the knee; they give anterior and posterior stability and help control rotation. The collateral ligaments connect the joint at both sides; they give medial and lateral stability and prevent dislocation. Numerous bursae prevent friction. One, the prepatellar bursa, lies between the patella and the skin. The infrapatellar fat pad is a small, triangular fat pad below the patella behind the patellar ligament.
Landmarks of the knee joint start with the large quadriceps muscle, which you can feel on your anterior and lateral thigh (Fig. 22-13). The muscle’s four heads merge into a common tendon that continues down to enclose the round bony patella. Then the tendon inserts down on the tibial tuberosity, which you can feel as a bony prominence in the midline. Move to the sides and a bit superiorly and note the lateral and medial condyles of the tibia. Superior to these on either side of the patella are the medial and lateral epicondyles of the femur.
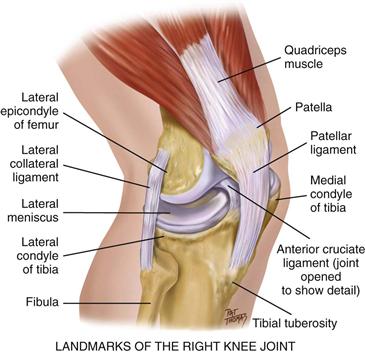
22-13
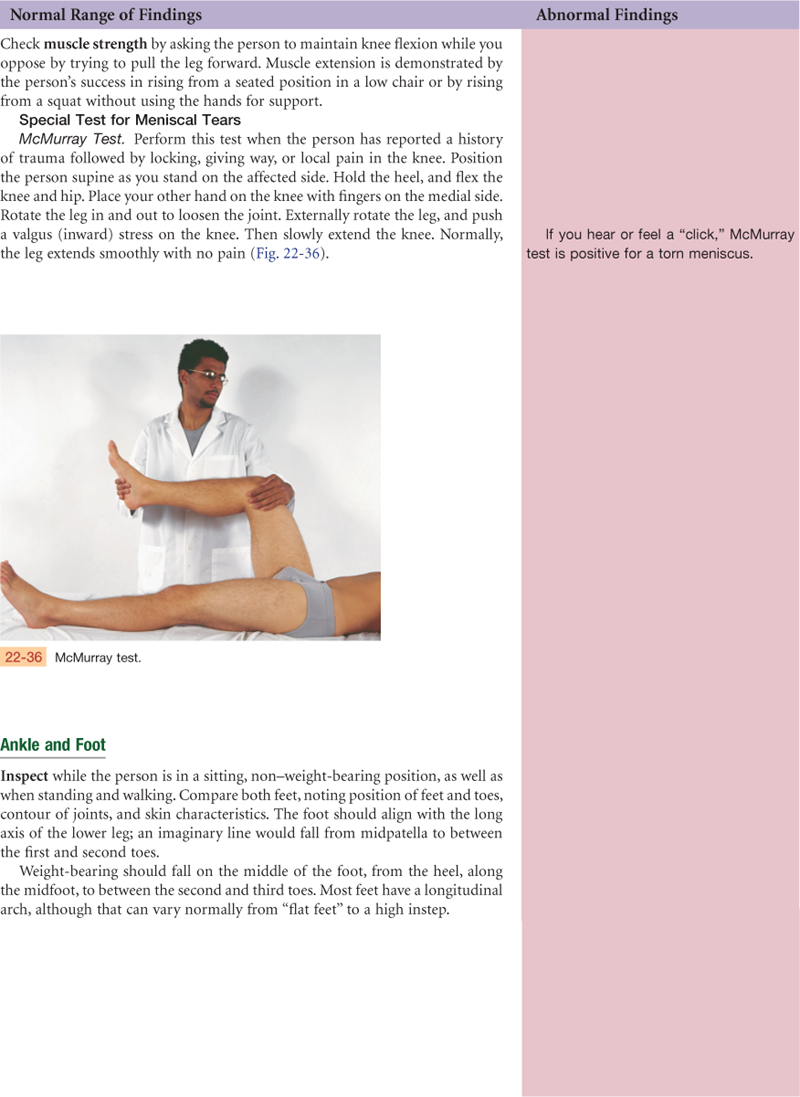
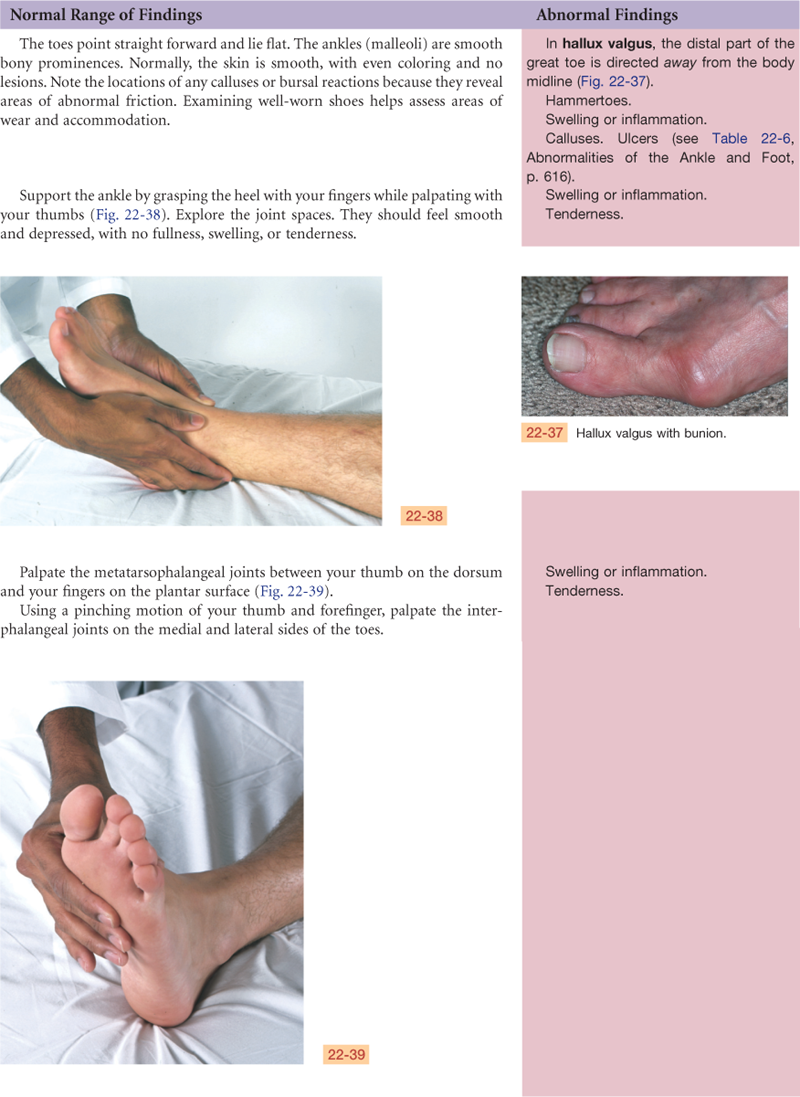
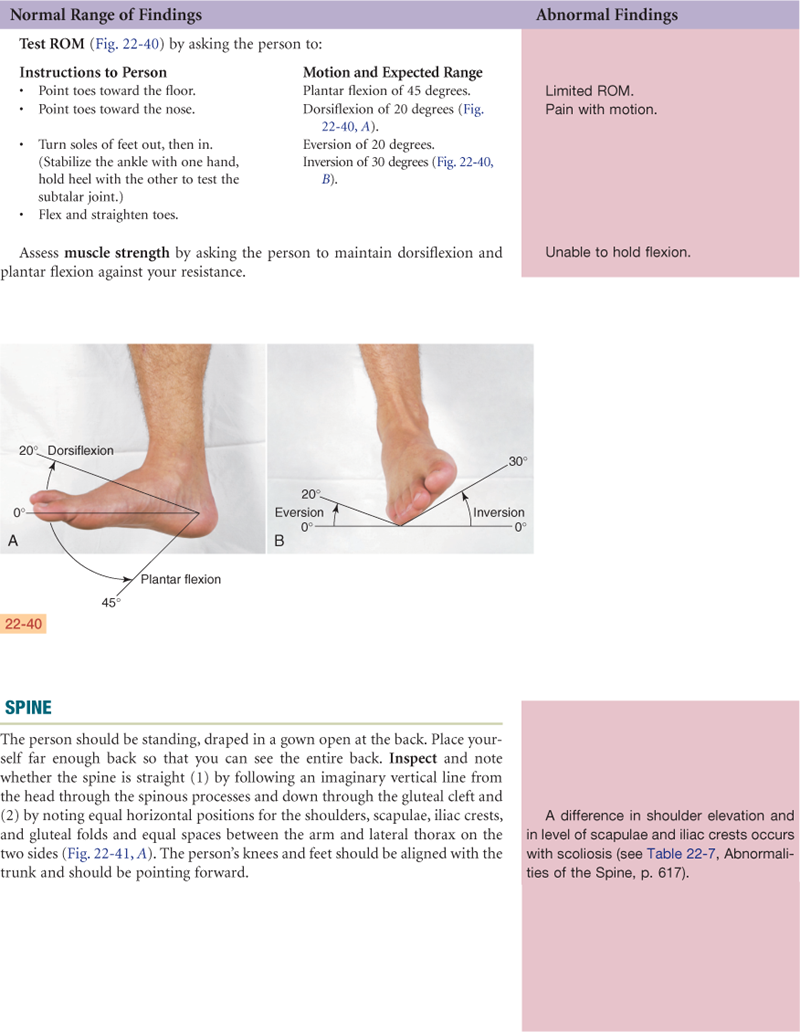
Ankle and Foot
The ankle, or tibiotalar joint, is the articulation of the tibia, fibula, and talus (Fig. 22-14). It is a hinge joint, limited to flexion (dorsiflexion) and extension (plantar flexion) on one plane. Landmarks are two bony prominences on either side—the medial malleolus and the lateral malleolus. Strong, tight medial and lateral ligaments extend from each malleolus onto the foot. These help the lateral stability of the ankle joint, although they may be torn in eversion or inversion sprains of the ankle.
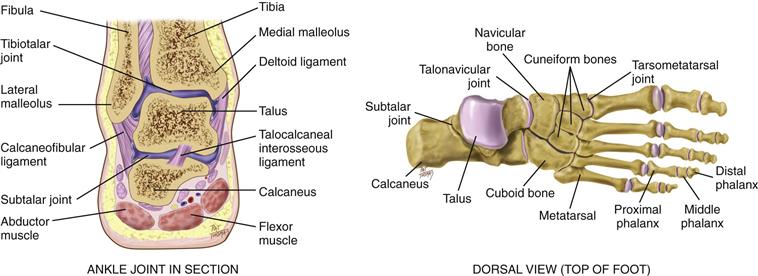
22-14
Joints distal to the ankle give additional mobility to the foot. The subtalar joint permits inversion and eversion of the foot. The foot has a longitudinal arch, with weight-bearing distributed between the parts that touch the ground—the heads of the metatarsals and the calcaneus (heel).
 Developmental Competence
Developmental Competence
Infants and Children
By 3 months’ gestation, the fetus has formed a “scale model” of the skeleton that is made up of cartilage. During succeeding months in utero, the cartilage ossifies into true bone and starts to grow. Bone growth continues after birth—rapidly during infancy and then steadily during childhood—until adolescence, when both boys and girls undergo a rapid growth spurt.
Long bones grow in two dimensions. They increase in width or diameter by deposition of new bony tissue around the shafts. Lengthening occurs at the epiphyses, or growth plates. These specialized growth centers are transverse disks located at the ends of long bone. Any trauma or infection at this location puts the growing child at risk for bone deformity. This longitudinal growth continues until closure of the epiphyses; the last closure occurs at about age 20 years.
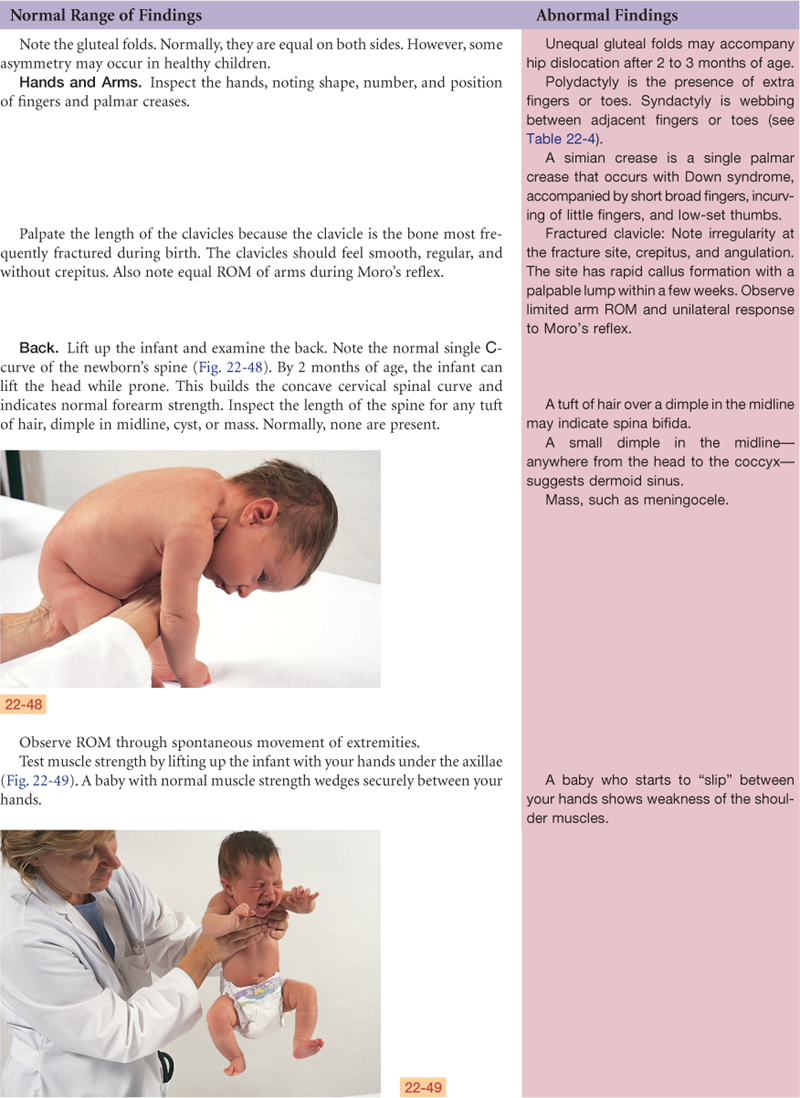
Skeletal contour changes are apparent at the vertebral column. At birth, the spine has a single C-shaped curve. At 3 to 4 months, raising the baby’s head from prone position develops the anterior curve in the cervical neck region. From 1 year to 18 months, standing erect develops the anterior curve in the lumbar region.
Although the skeleton contributes to linear growth, muscles and fat are significant for weight increase. Individual muscle fibers grow throughout childhood, but growth is marked during the adolescent growth spurt. Then muscles respond to increased secretion of growth hormone, to adrenal androgens, and in boys, to further stimulation by testosterone. Muscles vary in size and strength in different people. This is due to genetic programming, nutrition, and exercise. All through life, muscles increase with use and atrophy with disuse.
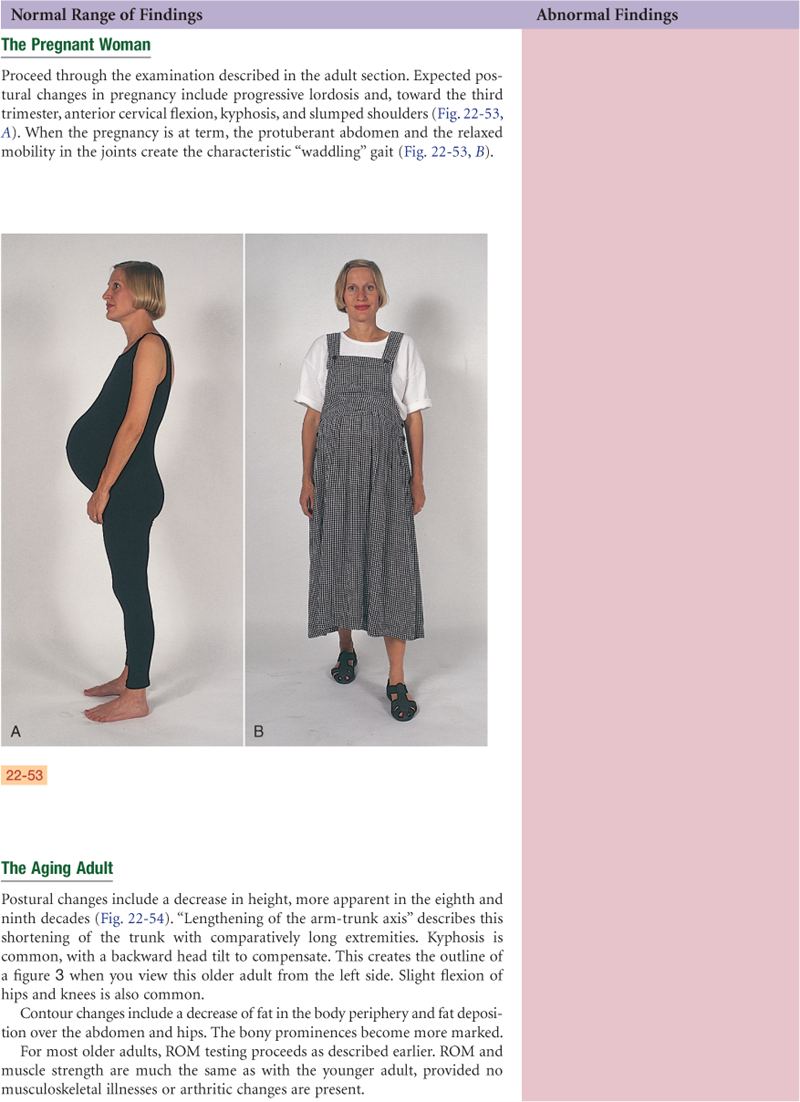
The Pregnant Woman
Increased levels of circulating hormones (estrogen, relaxin from the corpus luteum, and corticosteroids) cause increased mobility in the joints. Increased mobility in the sacroiliac, sacrococcygeal, and symphysis pubis joints in the pelvis contributes to the noticeable changes in maternal posture. The most characteristic change is progressive lordosis, which compensates for the enlarging fetus; otherwise, the center of balance would shift forward. Lordosis compensates by shifting the weight farther back on the lower extremities. This shift in balance in turn creates strain on the low back muscles, which, in some women, is felt as low back pain during late pregnancy.
Anterior flexion of the neck and slumping of the shoulder girdle are other postural changes that compensate for the lordosis. These upper back changes may put pressure on the ulnar and median nerves during the third trimester. Nerve pressure creates aching, numbness, and weakness in the upper extremities in some women.
The Aging Adult
Bone remodeling is a cyclic process of bone resorption and deposition. The balance favors deposition until skeletal maturity at 25 to 35 years when bones mass reaches its peak.17 After age 40, loss of bone matrix (resorption) occurs more rapidly than new bone formation. The net effect is a gradual loss of bone density, or osteoporosis. Although some degree of osteoporosis is nearly universal, women have more than men because for 5 years after menopause, the lack of estrogen leads to accelerated bone loss.
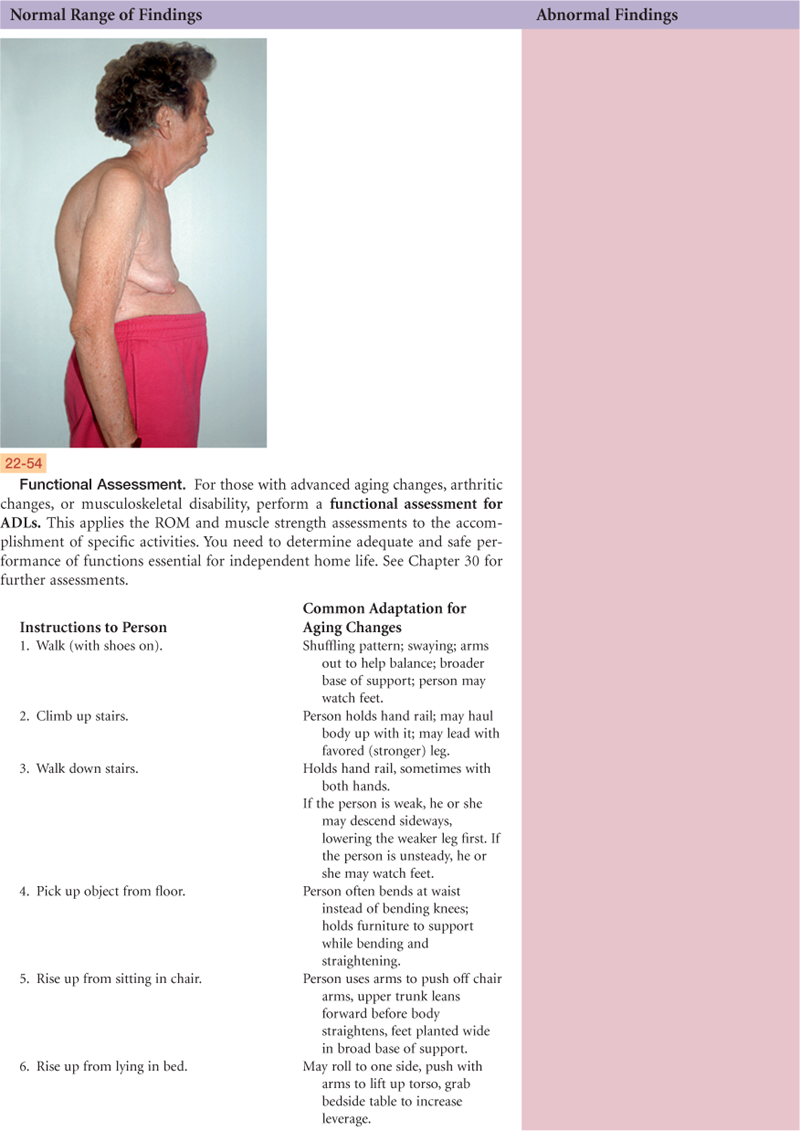
Postural changes are evident with aging, and decreased height is the most noticeable. Long bones do not shorten with age. Decreased height is due to shortening of the vertebral column. This is caused by loss of water content and thinning of the intervertebral disks and by a decrease in the height of individual vertebrae from osteoporosis.
Both men and women can expect a progressive decrease in height beginning at age 40 years in males and age 43 years in females, although this is not significant until age 60 years.6 A greater decrease occurs in the 70s and 80s as a result of osteoporotic collapse of the vertebrae. The result is a shortening of the trunk and comparatively long extremities. Other postural changes are kyphosis, a backward head tilt to compensate for the kyphosis, and a slight flexion of hips and knees.
The distribution of subcutaneous fat changes through life. Usually, men and women gain weight in their 40s and 50s. The contour is different, even if the weight is constant. They begin to lose fat in the face and deposit it in abdomen and hips. In the 80s and 90s, fat further decreases in the periphery, which is especially noticeable in the forearms and apparent over the abdomen and hips.
Loss of subcutaneous fat leaves bony prominences more marked (e.g., tips of vertebrae, ribs, iliac crests) and body hollows deeper (e.g., cheeks, axillae). An absolute loss in muscle mass occurs; some muscles decrease in size, and some atrophy, producing weakness. The contour of muscles becomes more prominent, and muscle bundles and tendons feel more distinct.
Lifestyle affects musculoskeletal changes; a sedentary lifestyle hastens musculoskeletal changes of aging. However, physical exercise increases skeletal mass and helps prevent or delay osteoporosis. Physical activity delays or prevents bone loss in postmenopausal women in a dose-dependent manner.19 Fast walking is the best prevention for osteoporosis; the faster the pace, the higher the preventive effect on the risk for hip fracture. The other positive effects of physical activity are improving muscle strength to prevent falls, balance and posture control, decrease in back pain, increase in quality of life, and prevention of cardiovascular disease, cancer, and depression.19
 culture and genetics
culture and genetics
There are racial/ethnic differences in bone strength and mineral density that may explain the incidence in hip fracture in older adults. African-American adults have a decreased risk for fracture when compared with white adults, and Hispanic women have a decreased risk for fractures than white women have.2 The differences in fracture rates may be traced to childhood, in which African-American and Hispanic children have shown significantly higher bone strength than white children. This is due to structural properties—greater bone density at specific bone sites in African-American and Hispanic children.26
Similar results have been demonstrated in adults: greater bone mass and bone mineral density (BMD) among African-American men than among their white counterparts.22 Younger Hispanic men had similar bone strength as African Americans, but older Hispanic men had more rapid loss of BMD and strength. The increased bone strength helps explain fracture risk.
Women have been studied regarding age at attaining peak bone mineral density. In the spine, women of all races gained BMD up to 30 to 33 years of age.3 But at the femoral neck in the hip joint, BMD peaked earlier among white women (≤16 years) than among African Americans (21 years) and Hispanics (20 years). An earlier peak BMD and a more rapid decline following is a trend that may explain the increased fracture risk for white women later in life. These data plus physical activity data discussed earlier suggest that weight-bearing physical activity (e.g., fast walking) is imperative during the reproductive and middle adult years to slow the process of decline in BMD.
Subjective Data
Trauma (fractures, sprains, dislocations)
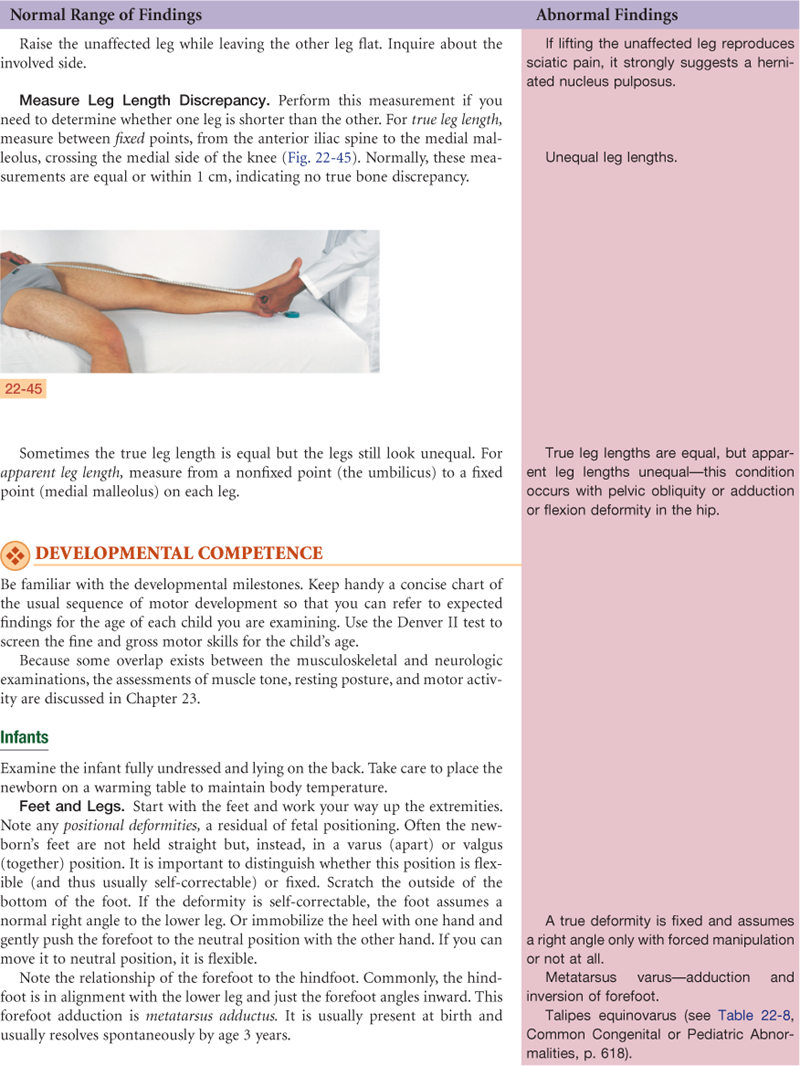
4. Functional assessment (activities of daily living [ADLs])
| Examiner Asks | Rationale |
| 1. Joints. | |
| • Any problems with your joints? Any pain? | Joint pain and loss of function are the most common musculoskeletal concerns that prompt a person to seek care. |
| • Location: Which joints? On one side or both sides? | Rheumatoid arthritis (RA) involves symmetric joints; other musculoskeletal illnesses involve isolated or unilateral joints. |
| • Quality: What does the pain feel like: aching, stiff, sharp or dull, shooting? Severity: How strong is the pain? • Onset: When did this pain start? | Exquisitely tender with acute inflammation. |
| • Timing: What time of day does the pain occur? How long does it last? How often does it occur? | RA pain is worse in morning when arising; osteoarthritis is worse later in the day; tendinitis is worse in morning, improves during the day. |
| • Is the pain aggravated by movement, rest, position, weather? Is the pain relieved by rest, medications, application of heat or ice? | Movement increases most joint pain except in RA, in which movement decreases pain. |
| • Is the pain associated with chills, fever, recent sore throat, trauma, repetitive activity? | Joint pain 10 to 14 days after an untreated strep throat suggests rheumatic fever. Joint injury occurs from trauma, repetitive motion. |
| • Any stiffness in your joints? | RA stiffness occurs in morning and after rest periods. |
| • Any swelling, heat, redness in the joints? | Suggests acute inflammation. |
| • Any limitation of movement in any joint? Which joint? • Which activities give you problems? (See Functional Assessment below and on p. 605.) |
Decreased ROM may be due to joint injury to cartilage or capsule or to muscle contracture. |
| 2. Muscles. | |
| • Any problems in the muscles, such as any pain or cramping? Which muscles? | Myalgia is usually felt as cramping or aching. |
| • If in calf muscles: Is the pain with walking? Does it go away with rest? | Suggests intermittent claudication (see Chapter 20). |
| • Are your muscle aches associated with fever, chills, the “flu”? | Viral illness often includes myalgia. |
| • Any weakness in muscles? • Location: Where is the weakness? How long have you noticed weakness? |
Weakness may involve musculoskeletal or neurologic systems (see Chapter 23). |
| • Do the muscles look smaller there? | Atrophy. |
| 3. Bones. | |
| • Any bone pain? Is the pain affected by movement? • Any deformity of any bone or joint? Is the deformity due to injury or trauma? Does the deformity affect ROM? • Any accidents or trauma ever affected the bones or joints: fractures; joint strain, sprain, dislocation? Which ones? |
Fracture causes sharp pain that increases with movement. Other bone pain usually feels “dull” and “deep” and is unrelated to movement. |
| • When did this occur? What treatment was given? Any problems or limitations now as a result? | |
| • Any back pain? In which part of your back? Is pain felt anywhere else, like shooting down leg? | |
| • Any numbness and tingling? Any limping? | |
| 4. Functional assessment (ADL). Do your joint (muscle, bone) problems create any limits on your usual activities of daily living (ADLs)? Which ones? (Note: Ask about each category; if the person answers “yes,” ask specifically about each activity in category.) | Functional assessment screens the safety of independent living, the need for home health services, and quality of life (see Chapter 30). |
| • Bathing—getting in and out of the tub, turning faucets? | Assess any self-care deficit. |
| • Toileting—urinating, moving bowels, able to get self on/off toilet, wipe self? | |
| • Dressing—doing buttons, zipper, fasten opening behind neck, pulling dress or sweater over head, pulling up pants, tying shoes, getting shoes that fit? | |
| • Grooming—shaving, brushing teeth, brushing or fixing hair, applying makeup? | |
| • Eating—preparing meals, pouring liquids, cutting up foods, bringing food to mouth, drinking? | |
| • Mobility—walking, walking up or down stairs, getting in/out of bed, getting out of house? | Impaired physical mobility. |
| • Communicating—talking, using phone, writing? | Impaired verbal communication. |
| 5. Self-care behaviors. Any occupational hazards that could affect the muscles and joints? Does your work involve heavy lifting? Or any repetitive motion or chronic stress to joints? Any efforts to alleviate these? | Assess risk for back pain or carpal tunnel syndrome. |
| • Tell me about your exercise program. Describe the type of exercise, frequency, the warm-up program. | Self-care behaviors. |
| • Any pain during exercise? How do you treat it? | |
| • Have you had any recent weight gain? Please describe your usual daily diet. (Note the person’s usual caloric intake, all four food groups, daily amount of protein, calcium.) | |
| • Are you taking any medications for musculoskeletal system: aspirin, anti-inflammatory, muscle relaxant, pain reliever? | |
| • If person has chronic disability or crippling illness: How has your illness affected: Your interaction with family Your interaction with friends The way you view yourself |
Assess for: • Self-esteem disturbance • Loss of independence • Body image disturbance • Role performance disturbance • Social isolation |
| Additional History for Infants and Children | |
| 1. Were you told about any trauma to infant during labor and delivery? Did the baby come head first? Was there a need for forceps? | Traumatic delivery increases risk for fractures, (e.g., humerus, clavicle). |
| 2. Did the baby need resuscitation? | Period of anoxia may result in hypotonia of muscles. |
| 3. Were the baby’s motor milestones achieved at about the same time as siblings or age-mates? | |
| 4. Has your child ever broken any bones? Any dislocations? How were these treated? | |
| 5. Have you ever noticed any bone deformity? Spinal curvature? Unusual shape of toes or feet? At what age? Have you ever sought treatment for any of these? | |
| Additional History for Adolescents | |
| 1. Involved in any sports at school or after school? How frequently (times per week)? | Assess safety of sport for child. Note if child’s height and weight are adequate for the particular sport (e.g., football). |
| 2. Do you use any special equipment? Does any training program exist for your sport? | Use of safety equipment and presence of adult supervision decrease risk for sports injuries. |
| 3. What is the nature of your daily warm-up? | Lack of adequate warm-up increases risk for sports injury. |
| 4. What do you do if you get hurt? | Students may not report injury or pain for fear of limiting participation in sport. |
| 5. How does your sport fit in with other school demands and other activities? | |
| Additional History for the Aging Adult | |
| Use the functional assessment history questions in Chapter 4 (pp. 49 to 70) to elicit any loss of function, self-care deficit, or safety risk that may occur as a process of aging or musculoskeletal illness. (Review the complete functional assessment in Chapter 30.) | |
| 1. Any change in weakness over the past months or years? | |
| 2. Any increase in falls or stumbling over the past months or years? | |
| 3. Do you use any mobility aids to help you get around: cane, walker? |


 Documentation and Critical Thinking
Documentation and Critical Thinking
Sample Charting
Subjective
States no joint pain, stiffness, swelling, or limitation. No muscle pain or weakness. No history of bone trauma or deformity. Able to manage all usual daily activities with no physical limitations. Occupation involves no musculoskeletal risk factors. Exercise pattern is brisk walk 1 mile 5×/week.
Objective
Joints and muscles symmetric; no swelling, masses, deformity; normal spinal curvature. No tenderness to palpation of joints; no heat, swelling, or masses. Full ROM; movement smooth, no crepitus, no tenderness. Muscle strength—able to maintain flexion against resistance and without tenderness.
Assessment
Muscles and joints—healthy and functional
Focused Assessment: Clinical Case Study
M.T. is a 45-year-old white female salesperson with a diagnosis of rheumatoid arthritis 3 years PTA, who seeks care now for “swelling and burning pain in my hands” for 1 day.
Subjective
M.T. was diagnosed as having rheumatoid arthritis at age 41 years by staff at this agency. Since that time, her “flare-ups” seem to come every 6 to 8 months. Acute episodes involve hand joints and are treated with aspirin, which gives relief. Typically experiences morning stiffness, lasting  to 1 hour. Joints feel warm, swollen, tender. Has had weight loss of 15 pounds over past 4 years and feels fatigued much of the time. States should rest more, but “I can’t take the time.” Daily exercises have been prescribed but doesn’t do them regularly. Takes aspirin for acute flare-ups, feels better in a few days, decreases dose by herself.
to 1 hour. Joints feel warm, swollen, tender. Has had weight loss of 15 pounds over past 4 years and feels fatigued much of the time. States should rest more, but “I can’t take the time.” Daily exercises have been prescribed but doesn’t do them regularly. Takes aspirin for acute flare-ups, feels better in a few days, decreases dose by herself.
Objective
Body joints within normal limits with exception of joints of wrist and hands. Radiocarpal, metacarpophalangeal, and proximal interphalangeal joints are red, swollen, tender to palpation. Spindle-shaped swelling of proximal interphalangeal joints of third digit right hand and second digit left hand; ulnar deviation of metacarpophalangeal joints.
Assessment
Acute pain R/T inflammation
Impaired physical mobility R/T inflammation
Deficient knowledge about aspirin treatment R/T lack of exposure
Noncompliance with exercise program R/T lack of perceived benefits of treatment
Noncompliance with advised rest periods R/T lack of perceived benefits of treatment
Summary Checklist: Musculoskeletal Examination
 For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
For a PDA-downloadable version, go to http://evolve.elsevier.com/Jarvis/.
Bibliography
1. Alexander IM. Pharmacotherapeutic management of osteoporosis and osteopenia. Nurse Practitioner. 2009;34(6):30–42.
2. Barrett-Connor E, Siris ES, Wehren LE, et al. Osteoporosis and fracture risk in women of different ethnic groups. Journal of Bone and Mineral Research. 2005;20:185–194.
3. Berenson AB, Rahman M, Wilkinson G. Racial difference in the correlates of bone mineral content/density and age at peak among reproductive-aged women. Osteoporosis International. 2009;20(8):1439–1449.
4. Broy SB, Myers AK. Identifying and managing osteoporosis: an update Journal of Musculoskeletal. Medicine. 2010;27(1):11–19.
5. Bunout D, Barrera G, Pia M, et al. Height reduction, determined using knee height measurement as a risk factor or predictive sign for osteoporosis in elderly women. Nutrition. 2007;23(11-12):794–797.
6. Cline MG, Meredith KE, Boyer JT, et al. Decline of height with age in adults in a general population sample: estimating maximum height and distinguishing birth cohort effects from actual loss of stature with aging. Human Biology. 1989;61:415–425.
7. Cruz AI, Smith BG. Scoliosis in children and adolescence: an update. Contemporary Pediatrics. 2010;27(1):42–52.
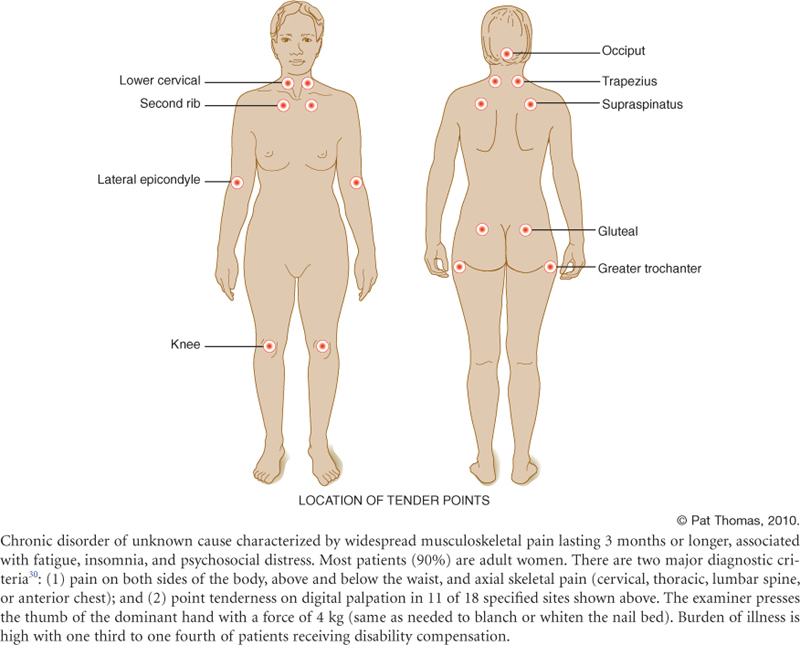
8. Dadabhoy D, McCarberg B, Hassett AL. Managing fibromyalgia in primary care. Primary Psychiatry. February 2010;17(2):2–16.
9. D’Arcy Y. Is low back pain getting on your nerves? Nurse Practitioner. 2009;34(5):10–20.
10. Davidson J, Randall GK, Getz MA. Self-reported height, calculated height, and derived body mass index in assessment of older adults. Journal of Nutrition for the Elderly. 2009;28(4):359–371.
11. Hart L. Primary care for patients with neurofibromatosis 1. Nurse Practitioner. 2005;30:38–43.
12. Jacobson AF, Myerscough RP, DeLambo K, et al. Patients’ perspectives on total knee replacement: a qualitative study sheds light on pre- and postoperative experiences. American Journal of Nursing. 2008;108(5):54–64.
13. Lee SG. Little arms, big league injuries. American Journal of Nursing. 2008;33(4):24–32.
14. Lewiecki EM. Current and emerging pharmacologic therapies for the management of postmenopausal osteoporosis. Journal of Women’s Health. 2009;18(10):1615–1624.
15. Looker AC, Melton III LJ, Harris T, et al. Age, gender, and race/ethnic differences in total body and subregional bone density. Osteoporosis International. 2009;20(7):1141–1149.
15a. McGee S. Evidence-based physical diagnosis. 2nd ed. St. Louis: Saunders; 2007.
16. Olson AF. Osteoporosis detection: is BMD testing the future? Nurse Practitioner. 2007;32(6):20–28.
17. Pigozzi E, Rizzo M, Giombini A, et al. Bone mineral density and sport: effect of physical activity. Journal of Sports Medicine and Physical Fitness. 2009;49(2):177–183.
18. Scanlon A, Maffei J. Carpal tunnel syndrome. The Journal of Neuroscience Nursing. 2009;41(3):140–147.
19. Schmitt NM, Schmitt J, Doren M. The role of physical activity in the prevention of osteoporosis in postmenopausal women: an update. Maturitas. 2009;63(1):34–38.
20. Seed SM, Dunican KC, Lynch AM. Osteoarthritis: a review of treatment options. Geriatrics. 2009;64(10):20–29.
21. Svara J. Weekend warriors: men’s sports-related knee injuries. Nurse Practitioner. 2009;34(7):13–24.
22. Travison TG, Beck TJ, Esche GR, et al. Age trends in proximal femur geometry in men: variation by race and ethnicity. Osteoporosis International. 2008;19(3):277–287.
23. U.S. Preventive Services Task Force. Screening for osteoporosis in postmenopausal women: recommendations and rationale. American Journal of Nursing. 2003;103:73–81.
24. U.S. Preventive Services Task Force. Screening for idiopathic scoliosis for adolescents: recommendation statement. American Family Physician. 2005;71:1975–1976.
25. Vondracek SF. Managing osteoporosis in postmenopausal women. American Journal of Health-System Pharmacy. 2010;67(7):S9–S19.
26. Wetzsteon RJ, Hughes JM, Kaufman BC, et al. Ethnic differences in bone geometry and strength are apparent in childhood. Bone. 2009;44(5):970–975.
27. Whyte MP. Paget’s disease of bone. New England Journal of Medicine. 2006;335(6):593–599.
28. Wick JM, Konze J, Alexander K, et al. Infantile and juvenile scoliosis: the crooked path to diagnosis and treatment. AORN Journal. 2009;90(3):347–380.
29. Wilson C. Rotator cuff versus cervical spine: making the diagnosis. Nurse Practitioner. 2005;30:45–50.
30. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis and Rheumatism. 1990;33:160–172.