Prenatal Care and Adaptations to Pregnancy
1 Define each key term listed.
2 List the goals of prenatal care.
3 Discuss prenatal care for a normal pregnancy.
4 Explain the nurse’s role in prenatal care.
5 Calculate the expected date of delivery and duration of pregnancy.
6 Differentiate among the presumptive, probable, and positive signs of pregnancy.
7 Describe the physiological changes that occur during pregnancy.
8 Identify nutritional needs for pregnancy and lactation.
9 Discuss the importance and limitations of exercise in pregnancy.
10 Describe patient education related to travel and common discomforts of pregnancy.
11 Discuss nursing support for emotional changes that occur in a family during pregnancy.
12 Identify special needs of the pregnant adolescent, the single parent, and the older couple.
13 Apply the nursing process in developing a prenatal teaching plan.
14 Identify the effects of medication ingestion on pregnancy and lactation.
 , p. 53)
, p. 53) , p. 52)
, p. 52) , p. 47)
, p. 47) , p. 52)
, p. 52) , p. 47)
, p. 47) , p. 48)
, p. 48) , p. 47)
, p. 47) , p. 47)
, p. 47) , p. 47)
, p. 47) , p. 53)
, p. 53) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Pregnancy is a temporary, physiological (that is, normal) process that affects the woman physically and emotionally. All systems of her body adapt to support the developing fetus. There are three phases of pregnancy: antepartum or prenatal (before birth), intrapartum (during birth), and postpartum (after birth). The focus of nursing care during pregnancy is to teach the mother how to maintain good health or, in the case of a mother with a condition that places her or her fetus at risk, to improve her health as much as possible. This chapter reviews prenatal care, the physiological and psychological changes of pregnancy, and nursing care to meet the needs of women and families.
Goals of Prenatal Care
Early and regular prenatal care is the best way to ensure a healthy outcome for both mother and child. Obstetricians, family practice physicians, certified nurse-midwives (CNMs), and nurse practitioners provide prenatal care. Unlike other health care providers, the nurse practitioner does not usually attend the woman at birth. The office or clinic nurse assists the health care provider in evaluating the expectant family’s physical, psychological, and social needs and teaches the woman self-care. These are the major goals of prenatal care:
• Ensure a safe birth for mother and child by promoting good health habits and reducing risk factors.
• Teach health habits that may be continued after pregnancy.
To achieve these goals, health care providers must do more than offer physical care. Health care providers must work as a team to create an environment that allows for cultural and individual differences while also being supportive of the entire family.
Prenatal Visits
Ideally, health care for childbearing begins before conception. Preconception care identifies risk factors that may be changed before conception to reduce their negative impact on the outcome of pregnancy. For example, the woman may be counseled about how to improve her nutritional state before pregnancy or may receive immunizations to prevent infections that would be harmful to the developing fetus. An adequate folic acid intake before conception can reduce the incidence of congenital anomalies (see Chapter 14). Some risk factors cannot be eliminated, such as preexisting diabetes, but preconception care helps the woman to begin pregnancy in the best possible state of health.
Prenatal care should begin, if not before conception, then as soon as a woman suspects that she is pregnant. A complete history and physical examination will help identify problems that may affect the woman or her fetus. The history should include the following:
• Obstetric history: Number and outcomes of past pregnancies; problems in the mother or infant
• Menstrual history: Usual frequency of menstrual cycles and duration of flow; first day of the last normal menstrual period (LNMP); any “spotting” since the LNMP
• Contraceptive history: Type used; whether an oral contraceptive was taken before the woman realized she might be pregnant; whether an intrauterine device is still in place
• Medical and surgical history: Infections such as hepatitis or pyelonephritis; surgical procedures; trauma that involved the pelvis or reproductive organs
• Family history of the woman and her partner: To identify genetic or other factors that may pose a risk for the pregnancy
• Health history of the woman and her partner: To identify risk factors (e.g., genetic defects or the use of alcohol, drugs, or tobacco) and possible blood incompatibility between the mother and the fetus
• Psychosocial history of the woman and her partner: To identify stability of lifestyle and ability to parent a child; significant cultural practices or health beliefs that may affect the pregnancy
The woman has a complete physical examination on her first visit to evaluate her general health, determine her baseline weight and vital signs, evaluate her nutritional status, and identify current physical or social problems. A pelvic examination is performed to evaluate the size, adequacy, and condition of the pelvis and reproductive organs and to assess for signs of pregnancy (see Box 4-3).
Her estimated date of delivery (EDD) is calculated based on the LNMP. An ultrasound examination may be done at this visit or at a later visit to confirm the EDD. An assessment for risk factors that may affect the pregnancy is performed during the first visit and updated at subsequent visits.
Several routine laboratory tests are performed on the first or the second prenatal visit. Others are done at specific times during pregnancy and may be repeated at certain intervals. Several tests are done for all pregnant women; others are based on the presence of various risk factors. The U.S. Preventive Services Task Force (USPSTF) has updated its recommendations concerning obtaining urine cultures at 12 to 16 weeks of gestation to screen for asymptomatic bacteruria. Early treatment of this condition can prevent preterm births. Table 4-1 lists prenatal laboratory tests. To prevent unnecessary fears or stress, it is important that the nurse explain that most tests are used to establish a baseline normal for comparison throughout pregnancy.
Table 4-1
Prenatal Laboratory Tests*
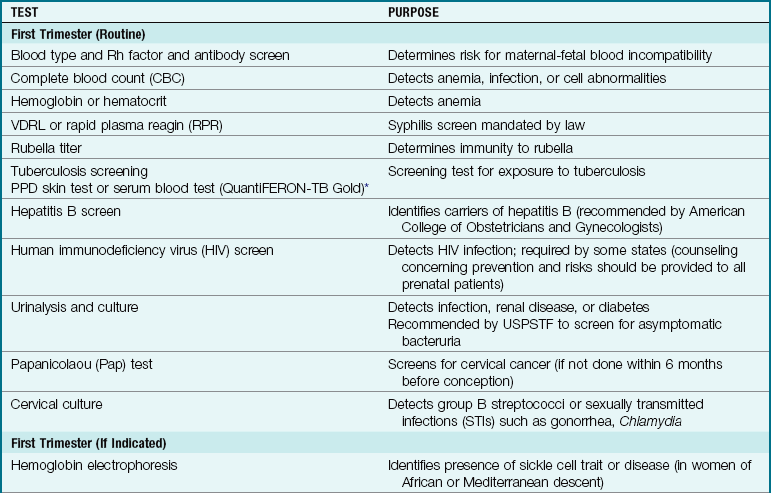
EDD, Estimated date of delivery; PPD, purified protein derivative; USPSTF, U.S. Preventive Services Task Force; VDRL, Venereal Disease Research Laboratory (test).
*Additional prenatal diagnostic tests are described in Table 5-1 (pp. 80-82).
The development of human genome mapping has expanded the prenatal detection of genetic disorders and provides the basis for future therapeutic interventions. The future direction of prenatal testing is to provide early, accurate, noninvasive screening tests.
The recommended schedule for prenatal visits in an uncomplicated pregnancy is as follows:
 Safety Alert!
Safety Alert!
Early and regular prenatal care is important for reducing the number of low-birth-weight infants born and for reducing morbidity and mortality for mothers and newborns.
The pregnant woman is seen more often if complications arise. Routine assessments made at each prenatal visit include the following:
• Review of known risk factors and assessment for new ones
• Vital signs: The woman’s blood pressure should be taken in the same arm and in the same position each time for accurate comparison with her baseline value.
• Weight to determine if the pattern of gain is normal: Low prepregnancy weight or inadequate gain are risk factors for preterm birth, a low-birth-weight infant, and other problems. A sudden, rapid weight gain is often associated with gestational hypertension.
• Urinalysis for protein, glucose, and ketone levels.
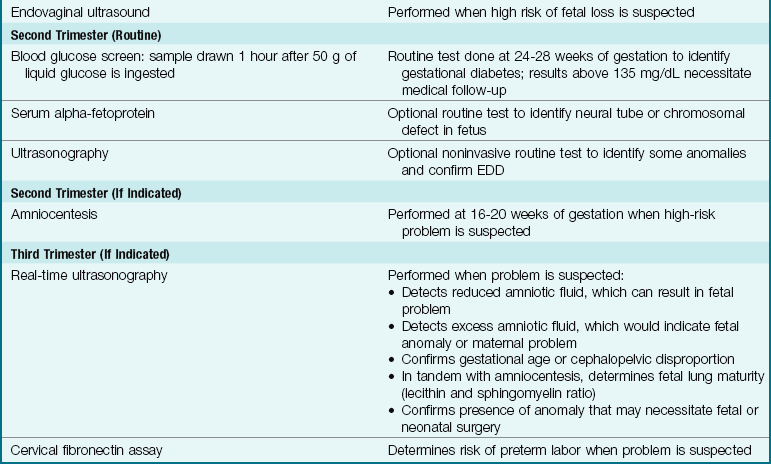
• Blood glucose screening between 24 and 28 weeks of gestation: Additional testing is done if the result of this screening test is 135 mg/dL or higher.
• Fundal height to determine if the fetus is growing as expected and the volume of amniotic fluid is appropriate (see Figure 4-3).
• Leopold’s maneuvers to assess the presentation and position of the fetus by abdominal palpation.
• Fetal heart rate: During very early pregnancy, the fetal heart rate is measured with a Doppler transducer; in later pregnancy, it may also be heard with a fetoscope. Beating of the fetal heart can be seen on ultrasound examination as early as 8 weeks after the LNMP.
• Review of nutrition for adequacy of calorie intake and specific nutrients.
• Discomforts or problems that have arisen since the last visit.
 Nursing Tip
Nursing Tip
The nurse listens to concerns and answers questions from the expectant family during each prenatal visit. This is a prime time for teaching good health habits, because most women are highly motivated to improve their health.
The nurse establishes rapport with the expectant family by conveying interest in their needs, listening to their concerns, and directing them to appropriate resources. The health care team must show sensitivity to the family’s cultural and health beliefs and incorporate as many as possible into care. For example, Muslim laws of modesty dictate that a woman be covered (hair, body, arms, and legs) when in the presence of an unrelated male, and therefore a female health care provider is often preferred. Latino families expect a brief period of conversation during which pleasantries are exchanged before “getting to the point” of the visit. An Asian woman may nod her head when the nurse teaches her, leading the nurse to believe that she understands and will use the teaching. However, the woman may be showing respect to the nurse rather than agreement with what is taught. Eye contact, which is valued by many Americans, is seen as confrontational in some cultures.
Definition of Terms
The following terms are used to describe a woman’s obstetric history:
• Gravida: Any pregnancy, regardless of duration; also, the number of pregnancies, including the one in progress, if applicable.
• Nulligravida: A woman who has never been pregnant.
• Primigravida: A woman who is pregnant for the first time.
• Multigravida: A woman who has been pregnant before, regardless of the duration of the pregnancy.
• Para: A woman who has given birth to one or more children who reached the age of viability (20 weeks of gestation), regardless of the number of fetuses delivered and regardless of whether those children are now living.
• Primipara: A woman who has given birth to her first child (past the point of viability), regardless of whether the child was alive at birth or is now living. The term is also used informally to describe a woman before the birth of her first child.
• Multipara: A woman who has given birth to two or more children (past the point of viability), regardless of whether the children were alive at birth or are presently alive. The term is also used informally to describe a woman before the birth of her second child.
• Nullipara: A woman who has not given birth to a child who reached the point of viability.
• Abortion: Termination of pregnancy before viability (20 weeks of gestation), either spontaneous or induced.
• Gestational age: Prenatal age of the developing fetus calculated from the first day of the woman’s LNMP.
• Fertilization age: Prenatal age of the developing fetus as calculated from the date of conception; approximately 2 weeks less than the gestational age.
• Age of viability: A fetus that has reached the stage (usually at 20 weeks) where it is capable of living outside of the uterus.
The word gravida indicates the number of pregnancies. The word para indicates the outcome of the pregnancies. The gravida number increases by 1 each time a woman is pregnant, whereas the para number increases only when a woman delivers a fetus of at least 20 weeks of gestation. For example, a woman who has had two spontaneous abortions (miscarriages) at 12 weeks of gestation, has a 3-year-old son, and is now 32 weeks pregnant would be described as gravida 4, para 1, abortions 2. The TPALM system (Box 4-1) is a standardized way to describe the detailed outcomes of a woman’s pregnancies on her prenatal record.
Box 4-1 TPALM System to Describe Parity

Determining the Estimated Date of Delivery
The average duration of a term pregnancy is 40 weeks (280 days) after the first day of the LNMP, plus or minus 2 weeks. Nägele’s rule is used to determine the EDD. To calculate the EDD, one identifies the first day of the LNMP, counts backward 3 months, and then adds 7 days (Box 4-2). The year is updated if applicable. The EDD is an estimated date, and many normal births occur before or after this date. The EDD may also be determined with a gestation wheel, an electronic calculator designed for this purpose, a physical examination, an ultrasound, or a combination of these methods.
Pregnancy is divided into three 13-week parts called trimesters. Predictable changes occur in the woman and the fetus in each trimester. Understanding these developments helps to better provide anticipatory guidance and identify deviations from the expected pattern of development.
Diagnosis of Pregnancy
The signs of pregnancy are divided into three general groups: presumptive, probable, and positive, depending on how likely they are to be caused by factors other than pregnancy (Box 4-3).
Presumptive Signs of Pregnancy
The presumptive indications of pregnancy are those from which a definite diagnosis of pregnancy cannot be made. These signs and symptoms are common during pregnancy but can often be caused by other conditions.
Amenorrhea, the cessation of menses, in a healthy and sexually active woman is often the first sign of pregnancy. However, strenuous exercise, changes in metabolism and endocrine dysfunction, chronic disease, certain medications, anorexia nervosa, early menopause, or serious psychological disturbances may also be the cause.
Nausea and sometimes vomiting occur in at least half of all pregnancies. “Morning sickness” describes the symptoms, but they may occur at any time of day. A distaste for certain foods or even their odors may be the main complaint. The nausea begins about 6 weeks after the LNMP and usually improves by the end of the first trimester. Emotional problems or gastrointestinal upsets may also cause nausea and vomiting.
Breast changes include tenderness and tingling as hormones from the placenta stimulate growth of the ductal system in preparation for breastfeeding. Similar breast changes also occur premenstrually in many women. Striae are pink to brown lines that may develop as the breasts enlarge (Figure 4-1).

FIGURE 4-1 Striae and pigmentation of breasts. Note the darkened pigmentation of areolae and the pink-white lines at the base of the breasts that are caused by stretching of the elastic tissue as the breasts enlarge. Pigmentation will disappear after pregnancy, and striae will fade into silvery strands.
Pigmentation changes occur primarily in dark-skinned women. They include increased pigmentation of the face (chloasma, or “mask of pregnancy”), breasts (darkening of the areolae), and abdomen (linea nigra, a line extending in the midline of the abdomen from just above the umbilicus to the symphysis pubis). See Figure 4-2 for common skin changes of pregnancy.

FIGURE 4-2 Abdominal striae are pinkish white or purple-gray lines that may occur in pregnancy. They may be found on the breasts, abdomen, and thighs. The dark line at the midline is the linea nigra, an area of increased pigmentation most noticeable in dark-skinned women.
Frequency and urgency of urination are common in the early months of pregnancy. The enlarging uterus, along with the increased blood supply to the pelvic area, exerts pressure on the bladder. Urinary frequency occurs in the first trimester until the uterus expands and becomes an abdominal organ in the second trimester. The pregnant woman experiences frequency of urination again in the third trimester when the presenting part descends in the pelvis in preparation for birth. Causes of urinary disturbances other than pregnancy are urinary tract infections and pelvic masses.
Fatigue and drowsiness are early symptoms of pregnancy. Fatigue is believed to be caused by increased metabolic needs of the woman and fetus. In an otherwise healthy young woman, it is a significant sign of pregnancy. However, illness, stress, or sudden changes in lifestyle may also cause fatigue.
Quickening, fetal movement felt by the mother, is first perceived at 16 to 20 weeks of gestation as a faint fluttering in the lower abdomen. Women who have previously given birth often report quickening at an earlier stage because they know how to identify it. This is an important event to record because it marks the approximate midpoint of the pregnancy and is another reference point to verify gestational age. Abdominal gas, normal bowel activity, or false pregnancy (pseudocyesis) are other possible causes.
Probable Signs of Pregnancy
The probable indications of pregnancy provide stronger evidence of pregnancy. However, these also may be caused by other conditions.
Goodell’s sign is the softening of the cervix and the vagina caused by increased vascular congestion. Chadwick’s sign is the purplish or bluish discoloration of the cervix, vagina, and vulva caused by increased vascular congestion. Hormonal imbalance or infection may also cause both Goodell’s and Chadwick’s signs. Hegar’s sign is a softening of the lower uterine segment. Because of the softening, it is easy to flex the body of the uterus against the cervix, which is known as McDonald’s sign.
Abdominal and uterine enlargement occurs rather irregularly at the onset of pregnancy. By the end of the twelfth week, the uterine fundus may be felt just above the symphysis pubis, and it extends to the umbilicus between the twentieth and twenty-second weeks (Figure 4-3). Uterine or abdominal tumors may also cause enlargement.
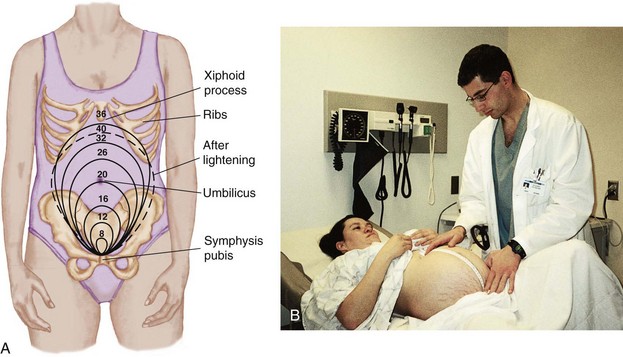
FIGURE 4-3 Height of fundus during gestation. A, The numbers represent the weeks of gestation, and the circles represent the height of the fundus expected at that stage of gestation. Note: The fortieth week is represented by a dotted line to indicate lightening has occurred. B, A health care provider measures the height of the fundus during a clinic visit. (B courtesy Pat Spier, RN-C.)
Braxton Hicks contractions are irregular, painless uterine contractions that begin in the second trimester. These contractions give the sensation of the abdomen being hard and tense. They become progressively more noticeable as term approaches and are more pronounced in multiparas. They may become strong enough to be mistaken for true labor. Uterine fibroids (benign tumors) may also cause these contractions.
Ballottement is a maneuver by which the fetal part is displaced by a light tap of the examining finger on the cervix and then rebounds quickly. Uterine or cervical polyps (small tumors) may cause the sensation of ballottement on the examiner’s finger.
Fetal outline may be identified by palpation after the twenty-fourth week. It is possible to mistake a tumor for a fetus.
Abdominal striae (stretch marks) are fine, pinkish white or purplish gray lines that some women develop when the elastic tissue of the skin has been stretched to its capacity (see Figure 4-2). Increased amounts of estrogen cause a rise in adrenal gland activity. This change in addition to the stretching is believed to cause breakdown and atrophy of the underlying connective tissue in the skin. Striae are seen on the breasts, thighs, abdomen, and buttocks. After pregnancy the striae lose their bright color and become thin, silvery lines. Striae may occur with skin stretching from any cause, such as weight gain.
Pregnancy tests use maternal urine or blood to determine the presence of human chorionic gonadotropin (hCG), a hormone produced by the chorionic villi of the placenta. Home pregnancy tests based on the presence of hCG in the urine are capable of greater than 97% accuracy, but the instructions must be followed precisely to obtain this accuracy. Professional pregnancy tests are based on urine or blood serum levels of hCG and are more accurate. A highly reliable pregnancy test is the radioimmunoassay (RIA). The RIA is a blood test that accurately identifies pregnancy as early as 1 week after ovulation. Pregnancy tests of all types are probable indicators because several factors may interfere with their accuracy: medications such as antianxiety or anticonvulsant drugs, blood in the urine, malignant tumors, or premature menopause.
Positive Signs of Pregnancy
Positive signs of pregnancy are caused only by a developing fetus. They include demonstration of fetal heart activity, fetal movements felt by an examiner, and visualization of the fetus with ultrasound.
Fetal heartbeat may be detected as early as 10 weeks of pregnancy by using a Doppler device. The examiner can detect the fetal heartbeat using a fetoscope between the eighteenth and twentieth weeks of pregnancy. When the fetal heartbeat is heard with a fetoscope, it is important because it provides another marker of the approximate midpoint of gestation. When assessing the fetal heartbeat with a Doppler device or fetoscope, the woman’s pulse rate must be assessed at the same time to be certain that the fetal heart is what is actually heard. The fetal heart rate at term ranges between a low of 110 to 120 beats/min and a high of 150 to 160 beats/min. The rate is higher in early gestation and slows as term approaches.
Additional sounds that may be heard while assessing the fetal heartbeat are the uterine and funic souffles. Uterine souffle is a soft blowing sound heard over the uterus during auscultation. The sound is synchronous with the mother’s pulse and is caused by blood entering the dilated arteries of the uterus. The funic souffle is a soft swishing sound heard as the blood passes through the umbilical cord vessels.
Fetal movements can be felt by a trained examiner in the second trimester. Fetal activity must be distinguished by the examiner because, to a prospective mother, normal intestinal movements can appear similar to the faint fetal movements typical of early pregnancy. Fetal movements can be seen with ultrasonography.
Identification of the embryo or fetus by means of ultrasound photography of the gestational sac is possible as early as 4 to 5 weeks of gestation with 100% reliability. This noninvasive method is the earliest positive sign of a pregnancy. An ultrasound is often routinely done around the twentieth week of gestation (Figure 4-4).

Physiological Changes in Pregnancy
The woman’s body undergoes dramatic changes as she houses and nourishes her growing child. Most of these changes reverse shortly after birth.
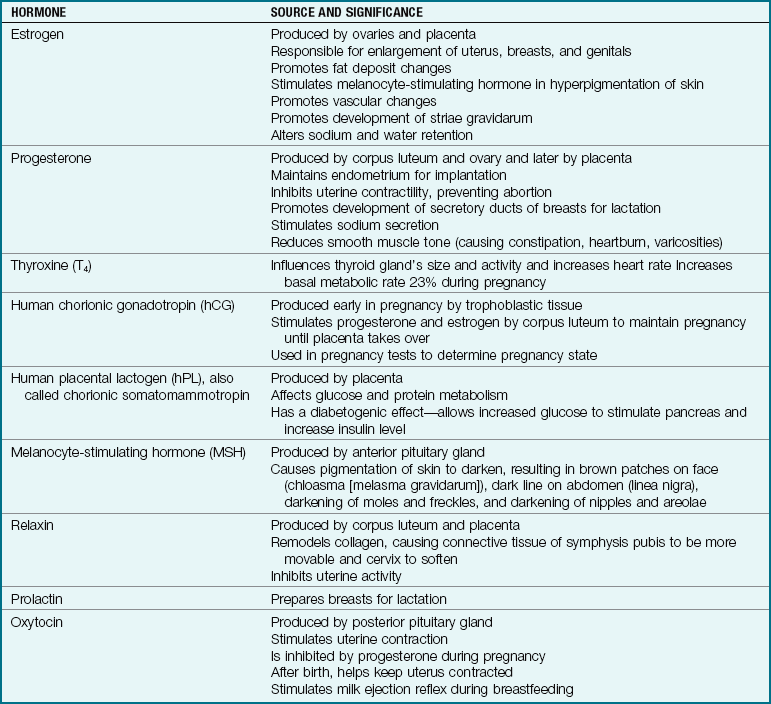
Endocrine System
Hormones are essential to maintain pregnancy, and the dramatic increase in hormones during pregnancy affects all body systems. Most hormones are produced by the corpus luteum initially and later by the placenta. The most striking change in the endocrine system during pregnancy is the addition of the placenta as a temporary endocrine organ that produces large amounts of estrogen and progesterone to maintain the pregnancy (as well as hCG and human placental lactogen [hPL]). hPL increases maternal insulin resistance during pregnancy, providing the fetus with glucose needed for growth (Table 4-2).
Reproductive System
The uterus undergoes the most obvious changes in pregnancy. Before pregnancy it is a small, muscular, pear-shaped pelvic organ that weighs about 60 g (2 oz), measures 7.5 cm (3 inches) × 5 cm (2 inches) × 2.5 cm (1 inch), and has a capacity of about 10 mL ( oz). The uterus expands gradually during pregnancy by increasing both the number of myometrial (muscle) cells during the first trimester and the size of individual cells during the second and third trimesters. The uterus becomes a temporary abdominal organ at the end of the first trimester. At term the uterus reaches the woman’s xiphoid process and weighs about 1000 g (2.2 lb). Its capacity is about 5000 mL (5 quarts), enough to house the term fetus, the placenta, and amniotic fluid.
oz). The uterus expands gradually during pregnancy by increasing both the number of myometrial (muscle) cells during the first trimester and the size of individual cells during the second and third trimesters. The uterus becomes a temporary abdominal organ at the end of the first trimester. At term the uterus reaches the woman’s xiphoid process and weighs about 1000 g (2.2 lb). Its capacity is about 5000 mL (5 quarts), enough to house the term fetus, the placenta, and amniotic fluid.
Cervix
Soon after conception the cervix changes in color and consistency. Chadwick’s and Goodell’s signs appear. The glands of the cervical mucosa increase in number and activity. Secretion of thick mucus leads to the formation of a mucous plug that seals the cervical canal. The mucous plug prevents the ascent of vaginal organisms into the uterus. With the beginning of cervical thinning (effacement) and opening (dilation) near the onset of labor, the plug is loosened and expelled.
Ovaries
The ovaries do not produce ova (eggs) during pregnancy. The corpus luteum (empty graafian follicle; see Chapter 2) remains on the ovary and produces progesterone to maintain the decidua (uterine lining) during the first 6 to 7 weeks of the pregnancy until the placenta can perform this function.
Vagina
The vaginal blood supply increases, causing the bluish color of Chadwick’s sign. The vaginal mucosa thickens, and rugae (ridges) become prominent. The connective tissue softens to prepare for distention as the child is born. Secretions of the vagina increase. In addition, the vaginal pH becomes more acidic to protect the vagina and uterus from pathogenic microorganisms. However, the vaginal secretions also have higher levels of glycogen, a substance that promotes the growth of Candida albicans, the organism that causes yeast infections.
The most common cause of vaginal discharge is bacterial vaginosis (BV), in which there is a decrease in normal lactobacilli and an increase in bacteroids and other anaerobic microorganisms. There may be a milky-white vaginal discharge, but often there are no other clinical symptoms. Bacterial vaginosis has been associated with preterm labor, and many obstetricians routinely screen pregnant women for BV early in pregnancy. Treatment with antimicrobials between 12 and 20 weeks of gestation is common.
Breasts
Hormone-induced breast changes occur early in pregnancy. High levels of estrogen and progesterone prepare the breasts for lactation. The areolae of the breasts usually become deeply pigmented, and sebaceous glands in the nipples (tubercles of Montgomery) become prominent. The tubercles secrete a substance that lubricates the nipples.
In the last few months of pregnancy, thin yellow fluid called colostrum may be expressed from the breasts. This “premilk” is high in protein, fat-soluble vitamins, and minerals but is low in calories, fat, and sugar. Colostrum contains the mother’s antibodies to diseases and is secreted for the first 2 to 3 days after birth in the breastfeeding woman.
Respiratory System
The pregnant woman breathes more deeply, but her respiratory rate increases only slightly, if at all. These changes increase oxygen and carbon dioxide exchange because she moves more air in and out with each breath. Oxygen consumption increases by 15% during pregnancy. The expanding uterus exerts upward pressure on her diaphragm, causing it to rise about 4 cm (1.6 inch). To compensate, her rib cage flares, increasing the circumference of the chest about 6 cm (2.4 inches). Dyspnea may occur until the fetus descends into the pelvis (lightening), relieving upward pressure on the diaphragm.
Increased estrogen levels during pregnancy cause edema or swelling of the mucous membranes of the nose, pharynx, mouth, and trachea. The woman may have nasal stuffiness, epistaxis (nosebleeds), and changes in her voice. A similar process occurs in the ears, causing a sense of fullness or earaches.
Cardiovascular System
The growing uterus displaces the heart upward and to the left. The blood volume gradually increases (hypervolemia) to about 45% greater than that of the prepregnant state by 32 to 34 weeks of gestation, at which time it levels off or declines slightly. This increase provides added blood for these purposes:
• Exchange of nutrients, oxygen, and waste products within the placenta
Cardiac output increases because more blood is pumped from the heart with each contraction, the pulse rate increases by 10 to 15 beats/min, and the basal metabolic rate (BMR) may increase 20% during pregnancy.
Blood pressure does not increase with the higher blood volume because resistance to blood flow through the vessels decreases. A blood pressure of 140/90 mm Hg or a significant elevation above the woman’s baseline measurement calls for attention. Supine hypotension syndrome, also called aortocaval compression or vena cava syndrome, may occur if the woman lies on her back (Figure 4-5). The supine position allows the heavy uterus to compress her inferior vena cava, reducing the amount of blood returned to her heart. Circulation to the placenta may also be reduced by increased pressure on the woman’s aorta, resulting in fetal hypoxia. Symptoms of supine hypotension syndrome include faintness, lightheadedness, dizziness, and agitation. Displacing the uterus to one side by turning the patient (preferably to the left) is all that is needed to relieve the pressure. If the woman must remain flat for any reason, a small towel roll placed under one hip will also help to prevent supine hypotension syndrome.
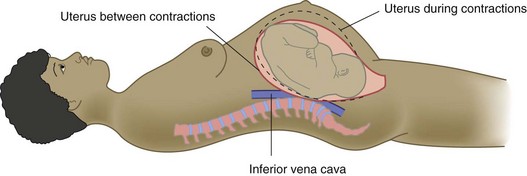
FIGURE 4-5 Supine hypotension syndrome. When a pregnant woman lies on her back (supine), the weight of the uterus with its fetal contents presses on the vena cava and the abdominal aorta. Placing a wedge pillow under the woman’s right hip helps to relieve compression of these vessels.
Orthostatic hypotension may occur whenever a woman rises from a recumbent position, resulting in faintness or lightheadedness. Cardiac output decreases because venous return from the lower body suddenly drops. Palpitations (sudden increase in heart rate) may occur from increases in thoracic pressure, particularly if the woman moves suddenly.
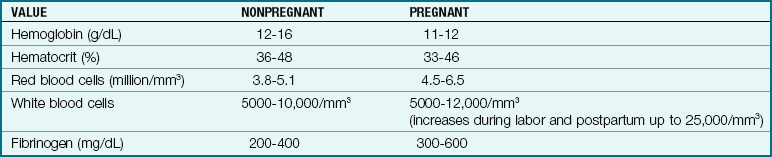
Although both plasma (fluid) and red blood cells (erythrocytes) increase during pregnancy, they do not increase by the same amount. The fluid part of the blood increases more than the erythrocyte component. This leads to a dilutional anemia or pseudoanemia (false anemia). As a result, the normal prepregnant hematocrit level of 36% to 48% may fall to 33% to 46%. Although this is not true anemia, the hematocrit count is reevaluated to determine patient status and needs. The white blood cell (leukocyte) count also increases about 8% (mostly neutrophils) and returns to prepregnant levels by the sixth day postpartum (Table 4-3).
There are increased levels of clotting factors VII, VIII, and X and plasma fibrinogen during the second and third trimesters of pregnancy. This hypercoagulability state helps prevent excessive bleeding after delivery when the placenta separates from the uterine wall. However, these changes increase the possibility of thrombophlebitis during pregnancy and are the reason the pregnant patient requires careful assessment for this risk and specific teaching to prevent the venous stasis that can lead to thrombophlebitis.
The current increased interest in physical fitness has resulted in many pregnant women continuing to exercise during pregnancy. The effects of exercise on the cardiovascular system that already has an increased blood volume, increased cardiac output, and increased coagulability during pregnancy must be reviewed before an exercise plan is carried out. Venous pressure may increase in the femoral veins as the size and weight of the uterus increase, resulting in varicose veins in the legs of some women.
Gastrointestinal System
The growing uterus displaces the stomach and intestines toward the back and sides of the abdomen (Figure 4-6). Increased salivary secretion (ptyalism) sometimes affects taste and smell. The mouth tissues may become tender and bleed more easily because of increased blood vessel development caused by high estrogen levels. Contrary to popular belief, teeth are not affected by pregnancy.
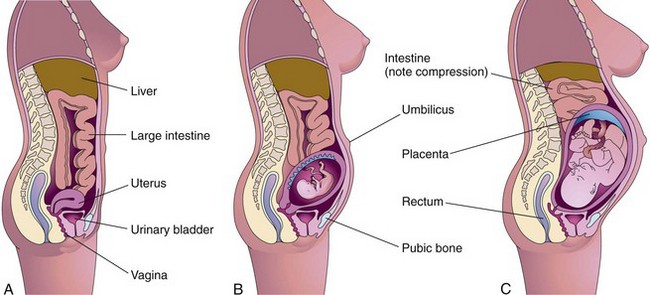
FIGURE 4-6 Compression of abdominal contents as uterus enlarges. The nonpregnant state (A) shows the relationship of the uterus to the abdominal contents. As the uterus enlarges at 20 weeks of gestation (B) and 30 weeks of gestation (C), the abdominal contents are displaced and compressed.
The demands of the growing fetus increase the woman’s appetite and thirst. The acidity of gastric secretions is decreased; emptying of the stomach and motility (movement) of the intestines are slower. Women often feel bloated and may experience constipation and hemorrhoids. Pyrosis (heartburn) is caused by the relaxation of the cardiac sphincter of the stomach, which permits reflux (backward flow) of the acid secretions into the lower esophagus.
Glucose metabolism is altered because of increased insulin resistance during pregnancy. This allows more glucose utilization by the fetus but also places the woman at risk for the development of gestational diabetes mellitus. Progesterone and estrogen relax the muscle tone of the gallbladder, resulting in the retention of bile salts, and this can lead to pruritus (itching of the skin) during pregnancy.
Urinary System
The urinary system excretes waste products for both the mother and the fetus during pregnancy. The glomerular filtration rate of the kidneys increases. The renal tubules increase the reabsorption of substances that the body needs to conserve but may not be able to keep up with the high load of some substances filtered by the glomeruli (e.g., glucose). Therefore glycosuria and proteinuria are more common during pregnancy. Water is retained because it is needed for increased blood volume and for dissolving nutrients that are provided for the fetus.
The relaxing effects of progesterone cause the renal pelvis and ureters to lose tone, resulting in decreased peristalsis to the bladder. The diameter of the ureters and the bladder capacity increase because of the relaxing effects of progesterone, causing urine stasis. The combination of urine stasis and nutrient-rich urine makes the pregnant woman more susceptible to urinary tract infection. Consuming at least eight glasses of water each day reduces the risk for urinary tract infection. Although the bladder can hold up to 1500 mL of urine, the pressure of the enlarging uterus causes frequency of urination, especially in the first and third trimesters. Changes in the renal system may take 6 to 12 weeks after delivery to return to the prepregnant state.
Fluid and Electrolyte Balance
The increased glomerular filtration rate in the kidneys increases sodium filtration by 50%, but the increase in the tubular resorption rate results in 99% reabsorption of the sodium. Sodium retention is influenced by many factors, including elevated levels of the hormones of pregnancy. Although much of the sodium is used by the fetus, the remainder is in the maternal circulation and can cause a maternal accumulation of water (edema). This fluid retention may cause a problem if the woman in labor is given intravenous fluids containing oxytocin (Pitocin), which has an antidiuretic effect and can result in water intoxication. Agitation and delirium—possible signs of water intoxication—should be recorded and reported, and an accurate intake and output record should be kept during labor and the immediate postpartum phase.
In pregnancy, blood is slightly more alkaline than in the nonpregnant state, and this mild alkalemia is enhanced by the hyperventilation that often occurs during pregnancy. This status does not affect a normal pregnancy.
Integumentary and Skeletal Systems
The high levels of hormones produced during pregnancy cause a variety of temporary changes in the integument (skin) of the pregnant woman. In addition to the pigmentary changes discussed under the presumptive signs of pregnancy, the sweat and sebaceous glands of the skin become more active to dissipate heat from the woman and fetus. Small red elevations of skin with lines radiating from the center, called spider nevi, may occur. The palms of the hands may become deeper red. Most skin changes are reversed shortly after giving birth.
The woman’s posture changes as her child grows within the uterus. The anterior part of her body becomes heavier with the expanding uterus, and the lordotic curve in her lumbar spine becomes more pronounced. The woman often experiences low backaches and, in the last few months of pregnancy, rounding of the shoulders may occur along with aching in the cervical spine and upper extremities.
The pelvic joints relax with hormonal changes during late pregnancy and entry of the fetal presenting part into the pelvic brim in the last trimester. A woman often has a “waddling” gait in the last few weeks of pregnancy because of a slight separation of the symphysis pubis.
Nutrition for Pregnancy and Lactation
Good nutrition is vital to good health and essential for normal growth and development. It is also essential to establish and maintain a healthy pregnancy and give birth to a healthy child. Good nutritional habits begun before conception and continued during pregnancy promote adaptation to the maternal and fetal needs. In a joint effort, the U.S. Department of Agriculture (USDA) and the U.S. Department of Health and Human Services created MyPyramid, which offers dietary guidelines for Americans (Figure 4-7). An example of how a food pyramid can be modified to fit Latin American dietary preferences is shown in Figure 4-8.
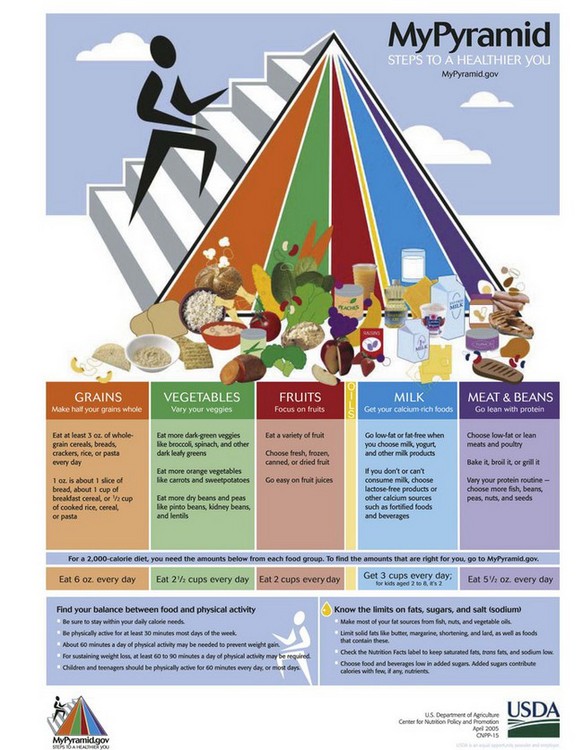
FIGURE 4-7 The 2005 Food Guide Pyramid is a guide to healthful eating for all people. The colors represent the basic food groups in the diet, and approximate recommended amounts to consume in relation to the total diet plan are indicated. Portion size can be individualized to the consumer by accessing the Internet site www.mypyramid.gov and entering the individual’s weight, sex, and activity level. The orange color represents whole grains; green represents vegetables; red represents fruit; the tiny white section represents healthy oils such as those from fish, nuts, and vegetable oil; blue represents a calcium source such as milk; and purple represents meat, poultry, eggs, and beans.
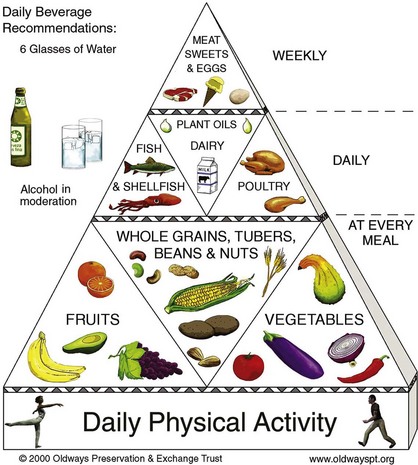
FIGURE 4-8 The Traditional Healthy Latin American Diet Pyramid. This diet pyramid is a modification of the North American diet and has daily physical activity as its base. It contains foods common to the Latin American diet.
 Nutrition Considerations
Nutrition Considerations
Maternal Diet and Fetal Health
There is a high correlation between maternal diet and fetal health. To ensure that deficiencies do not occur during the critical first weeks of pregnancy, the nurse explains to women of childbearing age the value of eating well-balanced meals so they may start pregnancy in a good nutritional state.
A healthy, balanced, nutrient-dense diet combined with adequate physical activity is the core of the revised dietary guidelines. A personalized portion-sized diet plan that includes individualized activity level advice is available online at www.MyPyramid.gov. Additional recommendations for specific populations can be found at www.healthierus.gov/dietaryguidelines. Women who follow this guide before pregnancy will be well nourished at the time of conception. Before and during pregnancy, women should read food labels carefully to promote the intake of calories that are nutrient dense rather than empty.
During pregnancy and lactation, an adequate dietary intake of docosahexaenoic acid–omega 3 fatty acid (DHA) is essential for optimal brain development of the fetus and infant. The World Health Organization (WHO) recommends that a full-term infant receive 20 mg of DHA per kilogram per day. Maternal dietary sources of DHA include fish such as mackerel, Atlantic and sockeye salmon, halibut, tuna, flounder, egg yolk, red meat, poultry, canola oil, and soybean oil; two to three servings per week are recommended. Frying these foods detracts from DHA content. Refer to Table 15-6 for culturally diverse food patterns.
Nursing Care Plan 4-1 on p. 58 lists common nursing diagnoses and interventions related to nutrition during pregnancy and lactation.
4-1  Nursing Care Plan
Nursing Care Plan
Nutrition During Pregnancy and Lactation
Mrs. Switzer is seen in the clinic. She is 35 years old, in the first trimester of her first pregnancy, and appears interested in learning how to “start a healthy diet” in order to have a healthy pregnancy outcome.
Deficient knowledge related to importance of nutrition in pregnancy and lactation
1. Mrs. Switzer says she is anxious to complete the clinic appointment because she wants to “light up a cigarette.” What is your major concern about her smoking? What interventions would be appropriate?
2. Mrs. Switzer states that her dietary pattern is heavily influenced by her perceived “food cravings,” which have occurred increasingly in the past month. What would be your approach to this problem?
Recommended Dietary Allowances and Recommended Dietary Intakes
In the United States, the Food and Nutrition Board of the Institute of Medicine (IOM), the National Academy of Science in cooperation with the USDA, and the U.S. Department of Health and Human Services developed recommended dietary allowances (RDAs) of nutrient intake required to maintain optimal health. In the past, RDAs reflected the fact that nutrients were primarily supplied by foods, in particular, nonfortified ones. Research by the Food and Nutrition Board showed an increasing use of dietary supplements and fortified foods, resulting in the need to describe upper limits of intake levels in order to prevent toxicity. Adverse responses (toxicity) can occur if the combination of intake in the form of supplements and food, whether fortified or not, exceeds the present upper limits of safety. When scientific evidence is insufficient to determine RDA, an adequate intake is likely provided by an adequate diet. Consuming dietary supplements of trace elements can result in toxicity if upper limits of intake are consistently exceeded.
The Committee of the USDA Human Nutrition and Research Center published recommended dietary intakes (RDIs) focusing on specific nutrients (see http://fnic.nal.usda.gov). Research is ongoing. Future nutrient recommendations will be expressed as dietary reference intakes (DRIs). DRI is an umbrella term that includes the RDA and tolerable upper levels of intake. The RDA will be retained for any nutrient for which revision to the new DRI has not been made, and both RDAs and RDIs will be used until research is completed. Current RDAs and RDIs of nutrients for various age-groups, including those for pregnant and lactating women, can be found on the Evolve website or in a nutrition textbook.
Weight Gain
In the past a woman’s weight gain was restricted during pregnancy. It was thought that minimal weight gain would keep the fetus small and therefore easier to deliver. More recently, low weight gain was thought to reduce the risk for gestational hypertension, a theory that has been disproved (Creasy et al., 2009).
Low maternal weight gain is associated with complications such as preterm labor, and recommendations for weight gain during pregnancy have gradually increased. Guidelines for weight gain during pregnancy are based upon the woman’s prepregnant weight and BMI. (The BMI considers the height and weight of the average American adult.) Women with a BMI of 18.5 to 24.9 are considered normal weight; women with a BMI of less than 18.5 are considered underweight; women with a BMI of 25 to 25.9 are considered overweight; and, women with a BMI greater than 30 are considered obese. A BMI calculator is available at www.nhlbisupport.com/bmi. Current IOM (2009) recommended weight gains during pregnancy with a single fetus are as follows:
• Normal-weight women: 25 to 35 lb (11.5 to 16 kg)
• Underweight women: 28 to 40 lb (12.5 to 18 kg)
Women carrying twins should gain more weight:
The adolescent should gain in the upper part of the range currently recommended for adult women.
The pattern of weight gain is also important. The general recommendation is that a woman gain up to 4.4 lb (2 kg) during the first trimester and approximately 1 lb (0.44 kg) per week during the rest of pregnancy. Nausea and vomiting and some transient food dislikes often limit weight gain or cause weight loss during the first trimester, but the weight is usually regained when the gastrointestinal upsets subside.
Women often want to know why they should gain so much weight when their infant weighs only 7 or 8 lb. The nurse can use the distribution of weight gain during pregnancy shown in Table 4-4 to teach women about all the factors that contribute to weight gain.
Table 4-4
Distribution of Weight Gain in Pregnancy
| SOURCE OF WEIGHT GAIN | WEIGHT GAIN IN POUNDS (kg) |
| Uterus | 2.5 (1.1) |
| Fetus | 7.0-7.5 (3.2-3.4) |
| Placenta | 1.0-1.5 (0.5-0.7) |
| Amniotic fluid | 2.0 (0.9) |
| Breasts | 1.5-3.0 (0.7-1.4) |
| Blood volume | 3.5-4.0 (1.6-1.8) |
| Extravascular fluids | 3.5-5.0 (1.6-2.3) |
| Maternal reserves | 4.0-9.5 (1.8-4.3) |
| Total | 25.0-35.0 (11.4-15.9) |
Modified from McKinney, E., James, S., Murray, S., & Ashwill, J. (2009). Maternal-child nursing (3rd ed.). Philadelphia: Saunders.

Nutritional Requirements During Pregnancy
A calorie increase of about 300 kcal/day is recommended to provide for the growth of the fetus, the placenta, amniotic fluid, and maternal tissues; 300 kcal is not a large increase. A banana, a carrot, a piece of whole wheat bread, and a glass of low-fat milk total about 300 kcal. A half of a roast beef sandwich on whole wheat bread and a fresh green salad added to a healthy diet would also meet the added caloric requirement. Caloric intake must be nutritious to have beneficial effects on pregnancy. Four nutrients are especially important in pregnancy: protein, calcium, iron, and folic acid. The amounts required are specified in Table 4-5.
Table 4-5
Daily Food Pattern for Pregnancy
| FOOD | AMOUNT |
| Milk, nonfat or low-fat, yogurt, cheese | 3-4 cups |
| Meat (lean), poultry, fish, egg | 2 servings (total 4-6 oz) |
| Vegetables, cooked or raw: dark green or deep yellow; starchy, including potatoes, dried peas, and beans; all others | 3-5 servings, all types, often |
| Fruits, fresh or canned, dark orange, including apricots, peaches, cantaloupe | 2-4 servings, all types, often |
| Whole-grain and enriched breads and cereals | 7 or more servings |
| Fats and sweets | In moderate amounts |
| Fluids | 8-10 glasses (8 oz) |
Modified from Mahan, L.K., & Escott-Stump, S. (2008). Krause’s food, nutrition, and diet therapy (12th ed.). Philadelphia: Saunders.
The pregnant woman should use MyPyramid to choose her daily diet. Servings that will supply enough of the additional nutrients needed are presented in Table 4-5.
Nutrition Considerations
Sample Menu for a Pregnant Woman*
 cup)
cup) cup)
cup) cup)
cup) cup)
cup) cup)
cup)*This menu assumes that the woman is of normal prepregnancy weight, that her weight gain is appropriate, that her activity is moderate, and that she is carrying only one fetus. Changes would be needed for the underweight or overweight woman, the adolescent, or a woman with a multifetal pregnancy.
Modified from Mahan, L.K., & Escott-Stump, S. (2008). Krause’s food, nutrition, and diet therapy (12th ed.). Philadelphia: Saunders.
Protein
Added protein is needed for metabolism and to support the growth and repair of maternal and fetal tissues. An intake of 60 g/day is recommended during pregnancy. The best sources of protein are meat, fish, poultry, and dairy products. Beans, lentils, and other legumes; breads and cereals; and seeds and nuts in combination with another plant or animal protein can provide all the amino acids (components of protein) needed.
Examples of complementary plant protein combinations are corn and beans, lentils and rice, and peanut butter and bread. Plant proteins are also complemented with animal proteins, such as in grilled cheese sandwiches, cereal with milk, and chili made of meat and beans. The complementary foods must be eaten together because all the amino acids necessary for building tissues (essential amino acids) must be present at the same time.
Information about nonmeat sources of protein should be given to women who are vegetarians to ensure that their protein needs are met. The information can also help reduce the family’s food budget because many plant protein sources are less expensive than animal sources. Fish containing high mercury levels such as albacore tuna and mackerel should be eaten with caution. Raw meat and raw eggs can be contaminated and should be avoided during pregnancy and lactation.
Calcium
Pregnancy and lactation increase calcium requirements by nearly 50%. The Dietary Reference Intake (DRI) of calcium for pregnant women is 1200 mg. Dairy products are the single most plentiful source of this nutrient. Other sources of calcium include enriched cereals, legumes, nuts, dried fruits, broccoli, green leafy vegetables, and canned salmon and sardines that contain bones. Calcium supplements are necessary for women who do not drink milk (or eat sufficient amounts of equivalent products). Supplements are also necessary for women under 25 years of age because their bone density is not complete. Calcium supplements should be taken separately from iron supplements for best absorption.
Iron
Pregnancy causes a heavy demand for iron because the fetus must store an adequate supply to meet the needs in the first 3 to 6 months after birth. In addition, the pregnant woman increases her production of erythrocytes. The DRI is 15 mg/day for nonpregnant adult women and 30 mg/day for pregnant women. Women who have a known iron deficiency may need more.
It is difficult to obtain this much iron from the diet alone, and most health care providers prescribe iron supplements of 30 mg/day beginning in the second trimester, after morning sickness decreases. Taking the iron on an empty stomach improves absorption, but many women find it difficult to tolerate without food. It should not be taken with coffee or tea or with high-calcium foods such as milk. Vitamin C (ascorbic acid) may enhance iron absorption (Mahan & Escott-Stump, 2008).
Iron comes in two forms, heme (found in red and organ meats) and nonheme (found in plant products). Heme iron is absorbed by the body best. Nonheme plant foods that are high in iron include molasses, whole grains, iron-fortified cereals and breads, dried fruits, and dark-green, leafy vegetables.
Folic Acid
Folic acid (folacin or folate) is a water-soluble B vitamin essential for the formation and maturation of both red and white blood cells in bone marrow. This vitamin can also reduce the incidence of neural tube defects such as spina bifida and anencephaly. The DRI for a pregnant woman is 400 mcg (0.4 mg) per day. Food sources of folic acid are liver, lean beef, kidney and lima beans, dried beans, potatoes, whole-wheat bread, peanuts, and fresh, dark-green, leafy vegetables.
Because adequate intake of folic acid at conception has a large impact on reducing the incidence of neural tube defects, the Centers for Disease Control and Prevention (CDC, 2010) recommends that all fertile American women consume 400 mcg (0.4 mg) of folic acid daily. A higher level of 4 mg/day is recommended for women who have previously had an infant with a neural tube defect, such as spina bifida, and plan to become pregnant again.
Fluids
The pregnant woman should drink 8 to 10 8-oz glasses of fluid each day, most of which should be water. Caffeinated drinks and drinks high in sugar should be limited. Caffeine acts as a diuretic, which counteracts some of the benefit of the fluid intake. The woman should limit her daily caffeine consumption to two cups of coffee or their equivalent. Women at risk for insufficient amniotic fluid (oligohydramnios) should drink 8 to 12 8-oz glasses of fluid daily (Fowles, 2006).
Sodium
In the past, sodium intake of pregnant women was restricted in an attempt to prevent edema and gestational hypertension. However, sodium intake is essential for maintaining normal sodium levels in plasma, bone, brain, and muscle because both tissue and fluid expand during the prenatal period. Sodium should not be restricted during pregnancy, but foods high in sodium, such as lunch meats and chips, should be avoided during pregnancy.
Diuretics to rid the body of excess fluids are not recommended for the healthy pregnant woman because they reduce fluids necessary for the fetus. The added fluid during pregnancy supports the mother’s increased blood volume.
Special Nutrition Considerations
Pregnant Adolescent: Gynecological age is the number of years between the onset of menses and the date of conception. The adolescent who conceives soon after having her first period has greater nutritional needs than one who is more sexually mature. The nurse must consider the adolescent’s characteristics of resistance, ambivalence, and inconsistency when planning nutritional interventions (see Chapter 20). The nurse must also remember that the girl’s peer group is of utmost importance to her and should help the adolescent find nutritious foods that allow her to fit in with her friends.
Inadequate weight gain and nutrient deficits are more likely in the pregnant adolescent. The girl’s continuing growth plus the growth of the fetus may make it difficult for her to meet her nutritional needs. In addition, a body image in which she sees herself as “fat” at a time when appearance is a high priority, combined with peer pressure to eat “junk” foods, places the pregnant adolescent at special risk.
Even a moderate positive change in diet helps, and the nurse should give the girl positive reinforcement for her efforts. Fast foods with poor nutritional content are often the adolescent’s foods of choice. However, the nurse can point out to the adolescent that many fast food restaurants offer salads, chicken, tacos, baked potatoes, and pizza. These foods provide many important nutrients and allow her to socialize with her peers at mealtime.
Nutritional intervention is necessary early in prenatal care to ensure a healthy mother and child. The younger and smaller teenage adolescent may need an additional 200 kcal/day in addition to the recommended increase of about 300 kcal/day for a normal pregnancy in order to meet her own growth needs and that of the developing fetus (Fowles, 2006). Many communities offer programs for adolescents that provide social support, education about prenatal care, and nutritional advice. Adolescents often respond well in these peer groups. The nurse often refers these young women to programs such as Women, Infants, and Children (WIC) and food stamp programs if needed.
Vegetarian or Vegan Diets: Women who follow vegetarian or vegan diets should focus on protein-rich foods such as soy milk, tofu, tempeh, and beans and supplement the diet with prenatal vitamins in order to meet the dietary needs of pregnancy. See Chapter 15, Figure 15-7, for an example of a healthy vegetarian diet.
Pica: The craving for and ingestion of nonfood substances such as clay, starch, raw flour, and cracked ice is called pica. Ingestion of small amounts of these substances may be harmless, but frequent ingestion in large amounts may cause significant health problems. Starch can interfere with iron absorption, and large amounts of clay may cause fecal impaction. Any other nonfood substance ingested in large quantities may be harmful because the necessary nutrients for healthy fetal development will not be available.
Pica is a difficult habit to break, and the nurse often becomes aware of the practice when discussing nutrition, food cravings, and myths with the pregnant woman. The nurse should educate the pregnant woman in a nonjudgmental way about the importance of good nutrition so the pica habit can be eliminated or at least decreased.
Lactose Intolerance: Intolerance to lactose is caused by a deficiency of lactase, the enzyme that digests the sugar in milk. Some women cannot digest milk or milk products, which increases their risk for calcium deficiency. Native Americans, Latinos, and persons of African, Middle Eastern, and Asian descent have a higher incidence of lactose intolerance than Caucasians. Signs and symptoms of lactose intolerance include abdominal distention, flatulence, nausea, vomiting, and loose stools after ingestion of dairy products. In such cases, a daily calcium supplement can be taken.
Substitutes for dairy products are listed in the section on calcium. Lactose-intolerant women may tolerate cultured or fermented milk products such as aged cheese, buttermilk, and yogurt. The enzyme lactase (LactAid) is available in tablet form or as a liquid to add to milk. Lactase-treated milk is also available commercially and can be used under a physician’s direction.
Cultural Preferences: People of varied cultures believe that specific foods have a dominant trait that affects the “humoral balance” in the body when ingested. Classification of food as “hot” or “cold” has nothing to do with the actual temperature. Examples of hot foods include peanuts, mangoes, ice cream, tea, cereal grains, and hard liquor. Examples of cold food include milk, green leafy vegetables, fresh water fish, chicken, bananas, and citrus fruits. In this belief framework, several health problems are classified as hot or cold, requiring a cold or hot food for balance.
To support the nutritional needs of patients from various cultures, teachings must consider these cultural beliefs and practices. See Chapter 15 for more details concerning food and culture.
Gestational Diabetes Mellitus: Gestational diabetes mellitus is first diagnosed during pregnancy rather than being present before pregnancy (see Chapter 5). Calories should be evenly distributed during the day among three meals and three snacks to maintain adequate and stable blood glucose levels. Pregnant diabetic women are susceptible to hypoglycemia (low blood glucose level) during the night because the fetus continues to use glucose while the mother sleeps. It is suggested that the final bedtime snack be one of protein and a complex carbohydrate to provide more blood glucose stability. Dietary management may be supervised by a registered dietitian. Glycemic control during the first and second trimesters is most important in preventing complications such as macrosomia (abnormally large newborn). Women with uncontrolled diabetes and fasting blood glucose levels greater than 500 mg/dL in the last trimester have an increased risk of stillbirth (Fowles, 2006).
Nutritional Requirements During Lactation
The caloric intake during lactation should be about 500 calories more than the nonpregnant woman’s RDA. An indicator of adequate caloric intake is a stable maternal weight and a gradually increasing infant weight. The maternal protein intake should be 65 mg/day so the growing infant has adequate protein. Calcium intake and iron intake are the same as during pregnancy to allow for the infant’s demand on the mother’s supply. Vitamin supplements are often continued during lactation. Fluids sufficient to relieve thirst should be taken. Drinking 8 to 10 glasses of liquids other than those containing caffeine is adequate.
Some foods should be omitted during lactation if they cause gastric upset in the mother or child. The mother will often identify foods that seem to upset her child. Caffeine should be restricted to the equivalent of two cups of coffee each day. Lactating mothers should be instructed that many types of drugs she may take can be secreted in varying amounts in the breast milk. Drugs should be taken only with the health care provider’s advice. Alcohol intake should be restricted to an occasional single serving for breastfeeding women.
Exercise During Pregnancy
There is evidence that mild to moderate exercise is beneficial during normal pregnancy, but vigorous exercise should be avoided. The nurse should guide the patient concerning exercise during pregnancy based on the understanding that the maternal circulatory system is the lifeline to the fetus and any alteration can affect the growth and survival of the fetus. The maternal cardiac status and fetoplacental reserve should be the basis for determining exercise levels during all trimesters of pregnancy. Current health and fitness lifestyles mandate the inclusion of information concerning exercise during pregnancy in prenatal education programs (Lewis et al., 2008).
A history of the exercise practices of the patient is important, and gathering such data is the first step in the nursing process. Women who have had prior training may have a higher tolerance for exercise than women who have led a sedentary lifestyle. The goal of exercise during pregnancy should be maintenance of fitness, not improvement of fitness or weight loss (Figure 4-9). The following are some basic factors that should be evaluated and discussed.
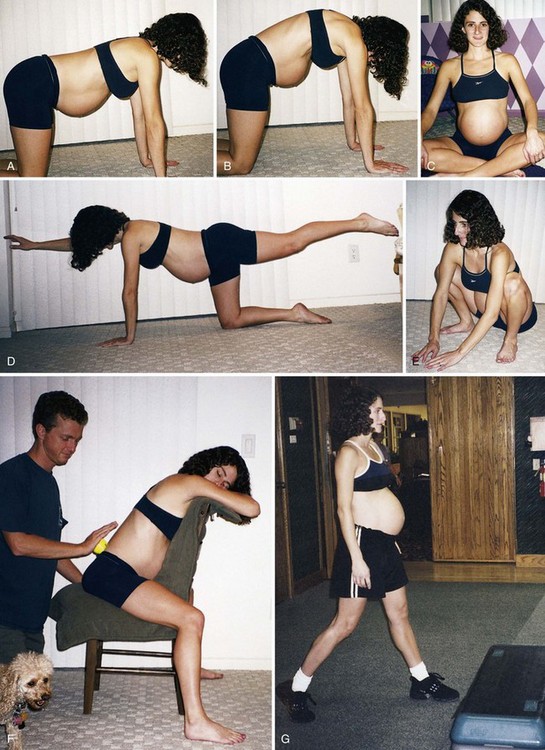
FIGURE 4-9 Exercises during pregnancy. A and B, The pelvic tilt. C, Tailor sitting position. D, Proper stretch position. E, Proper squat position. F, Back massage with a tennis ball used as pressure. G, A pregnant woman participating in step aerobics class for moderate exercise.
Elevated Temperature
Exercise can elevate the maternal temperature and result in decreased fetal circulation and cardiac function. Maternal body temperature should not exceed 38° C (100.4° F), which rules out the use of hot tubs and saunas during pregnancy. Maternal heat exposure during the first trimester of pregnancy has been associated with neural tube defects and miscarriage (Lewis et al., 2008). Exercise-related increases in body temperature are somewhat more easily tolerated because of the normal physiology of pregnancy as it pertains to increased peripheral blood flow, thermal inertia from weight gain, and peripheral venous pooling. Monitoring the body temperature in addition to the exercise intensity is essential.
Hypotension
When the flat supine position is assumed and the uterus presses on the vena cava, the increasing size and weight of the uterus can cause poor venous return and result in supine hypotension syndrome. Orthostatic hypotension can also reduce blood flow to the fetus. Certain exercise positions may need to be modified during pregnancy to avoid these problems, which can cause fetal hypoxia.
Cardiac Output
Pregnancy increases the workload of the heart. The increase in peripheral pooling during pregnancy results in a decrease in cardiac output reserves for exercise. When exercise is allowed to exceed the ability of the cardiovascular system to respond, blood may be diverted from the uterus, causing fetal hypoxia. Exercise increases catecholamine levels, which the placenta may not be able to filter, resulting in fetal bradycardia and hypoxia. Strenuous and prolonged exercise causes blood flow to be distributed to the skeletal muscles and skin and away from the viscera, uterus, and placenta. If the reduction in uterine blood flow exceeds 50%, serious adverse effects to the fetus may occur. For this reason, moderate exercise is preferred for pregnant women as opposed to strenuous or prolonged exercise. Exercise increases maternal hematocrit levels and uterine oxygen uptake, so moderate exercise will not cause decreased oxygen supplies to the fetus.
Hormones
Exercise can cause changes in oxygen consumption and epinephrine, glucagon, cortisol, prolactin, and endorphin levels. In early pregnancy these hormonal changes can negatively affect implantation of the zygote and vascularization of the uterus. In late pregnancy the increases in catecholamines during exercise can trigger labor. However, studies have not shown increased rates of preterm deliveries in pregnant women who exercise (Lewis et al., 2008). Joint instability caused by hormonal changes can result in injury if the woman engages in deep flexion or extension of joints. Range of motion (ROM) should not be extended beyond prepregnancy abilities.
Other Factors
In general, moderate exercise several times a week from the eighth week through delivery is advised during pregnancy, with avoidance of vigorous activity and competitive sports. Moderate exercise during pregnancy has many beneficial effects including a more positive self-image, a decrease in musculoskeletal discomforts during pregnancy, and a more rapid return to prepregnant weight after delivery (Lewis et al., 2008). The American Diabetes Association supports moderate exercise during pregnancy. Vigorous exercise in hot, humid weather should be avoided by even the trained woman. Safety measures are advisable because of the changes in the body’s center of gravity as the uterus enlarges. Liquid and calorie intake should be adjusted to meet the needs of pregnancy as well as the demands of exercise. Women who have complications or medical conditions such as hypertension or multiple gestation should consult a health care provider before engaging in any exercise program during pregnancy.
Nursing guidance should include the following:
• The woman should start with a warm-up and end with a cool-down period.
• Women who are beginning an exercise program should not exceed the American College of Obstetricians and Gynecologists (ACOG, 2007) recommendations for moderate exercise. Women who have exercised regularly at higher levels before pregnancy may follow more liberal guidelines of weight-bearing exercise for no more than 1 hour three to five times a week.
• Exercise combined with a balanced diet rich in unprocessed, nonroot vegetables, nuts, fruits, and whole-grain breads is beneficial during pregnancy. Eating 2 to 3 hours before exercise and immediately after exercise is recommended.
• The woman should avoid scuba diving below a depth of 30 feet or exercising in altitudes above 8000 feet during pregnancy.
• The woman should avoid getting overheated and should drink plenty of water during exercise.
• Intensity of exercise should be modified according to the “talk test” (should be able to complete a conversational sentence without taking an extra breath).
Travel During Pregnancy
Many women choose to maintain a normal lifestyle and travel during a normal pregnancy. Air travel is generally safe for the pregnant woman, but the availability of medical care at the destination should be checked online at www.cdc.gov/travel. Because of the increased levels of clotting factors and plasma fibrinogen that normally occur during pregnancy, the woman should be counseled to avoid long periods of sitting because there is an increased risk of developing thromboembolism (Steffen et al., 2007). She should also avoid locations that pose a high risk for exposure to infectious diseases. A copy of obstetric records should be taken, and the location of medical facilities in the area to be visited should be identified.
Guidance concerning hand hygiene and dietary precautions to prevent diarrhea are essential. If needed, special oral rehydration solutions may be available or bottled drinks may provide the fluid, sugar, and electrolytes needed. An oral rehydration formula recommended by the WHO is to combine and drink 1 L of water, 1 teaspoon of salt, 4 teaspoons of cream of tartar,  teaspoon of baking soda, and 4 tablespoons of sugar (CDC, 2010). The woman should be advised to wear comfortable shoes and long-sleeved clothing and use mosquito nets around the bed in insect-prone areas. Insect repellants that contain the chemical abbreviated as DEET are usually safe after the first trimester. Sunblock should be applied as appropriate.
teaspoon of baking soda, and 4 tablespoons of sugar (CDC, 2010). The woman should be advised to wear comfortable shoes and long-sleeved clothing and use mosquito nets around the bed in insect-prone areas. Insect repellants that contain the chemical abbreviated as DEET are usually safe after the first trimester. Sunblock should be applied as appropriate.
Common Discomforts in Pregnancy
Various discomforts occur during normal pregnancy as a result of physiological changes. The nurse should teach the woman measures to relieve these discomforts. The nurse should also explain signs of problems that can be confused with the normal discomforts of pregnancy. Providing information written in the woman’s primary language gives her a reference if she has questions later.
Nausea is a problem chiefly in the first trimester. Persistent nausea with vomiting that significantly interferes with food and fluid intake is not normal and should be reported. Relief measures include the following:
• Eating dry toast or crackers before getting out of bed in the morning
• Drinking fluids between meals instead of with meals
• Eating small, frequent meals
• Avoiding fried, greasy, or spicy foods and foods with strong odors, such as cabbage and onions
Vaginal discharge is more noticeable because of the increased blood supply to the pelvic area. A discharge that is yellow, has a foul odor, or is accompanied by itching and inflammation suggests vaginal infection and should be reported. Measures to manage the discharge and reduce the risk for infection include the following:
• Wearing loose-fitting cotton panties
• Not douching unless specifically ordered by the health care provider
• Wiping the perineal area from front to back after toileting
Fatigue may be difficult in the early months of the pregnancy if the mother is working or has other small children. Measures to cope with fatigue include the following:
• Getting at least 8 to 10 hours of sleep at night
• Taking a nap during the day if possible
• Using relaxation techniques, meditation, or a change of scenery
Extreme exhaustion usually diminishes in the second trimester, and often women then feel exhilarated and full of energy. The tired feeling may return again during the last 4 to 6 weeks of the pregnancy. Again, daytime naps and as much restful nighttime sleep as possible help to provide the energy needed for labor.
Backache occurs because of the spine’s adaptation to the back’s changing contour as the uterus grows. Relief measures include the following:
• Maintaining correct posture with the head up and the shoulders back
• Avoiding exaggerating the lumbar curve
• Wearing low-heeled shoes to help maintain better posture
• Squatting rather than bending over when picking up objects
• When sitting, supporting the arms, feet, and back with pillows as needed
• Exercising using tailor sitting, shoulder circling, and pelvic rocking (see Figure 4-9)
Constipation occurs because of slowed peristalsis, the use of iron supplements, and pressure of the growing uterus on the large intestine. Relief measures include the following:
• Drinking at least eight glasses of water each day, not counting coffee, tea, or carbonated drinks
• Adding dietary fiber to foods, such as unpeeled fresh fruits and vegetables, whole-grain cereals, bran muffins, oatmeal, potatoes with skins, and fruit juices
• Limiting cheese consumption if this tends to be constipating
• Limiting sweet foods if they cause flatulence
• Consulting the health care provider if iron supplements cause constipation. Do not stop taking the iron, because a change in the supplement may help
• Getting plenty of exercise (a brisk 1-mile walk is good to stimulate peristalsis)
• Establishing a regular time each day for having a bowel movement; defecate as soon as the urge occurs rather than delaying
• Taking laxatives or enemas only under the direction of the health care provider
Varicose veins are common in the pregnant woman because the large uterus slows venous return, causing the blood to pool, especially in the leg veins. This pooling may eventually break down the competence of the valves within the veins, resulting in varicosities. Varicose veins are seen most often on the back of the calves and behind the knees. Excessive weight gain and genetic predisposition affect the occurrence of varicosities and their persistence after the pregnancy. Varicosities may occur on the vulva, especially after the twentieth week of pregnancy. They are usually temporary and subside after the delivery. Measures to relieve the discomfort of varicosities include the following:
• Avoiding constricting clothing or crossing the legs at the knees
• Elevating the legs above hip level when resting
• Wearing support hose or elastic stockings, which increase venous blood flow; for best results, apply them before getting out of bed each morning
Hemorrhoids are varicosities of the rectum and anus that become more severe with constipation and with descent of the infant’s head into the pelvis. They generally decrease or disappear after birth, when pressure is relieved. Relief measures include the following:
Heartburn causes discomfort mainly in late pregnancy, when the uterus presses against the esophagus where it enters the stomach. This pressure may cause a reflux of gastric acids into the esophagus, resulting in a burning feeling in the chest and a bitter taste in the mouth. Suggestions to reduce heartburn include the following:
• Eating small, frequent meals and avoiding fatty foods
• Sitting upright and sleeping with an extra pillow under the head
• Using deep breathing and taking sips of water, both of which may relieve the burning
• Using antacids if recommended by the health care provider (those high in sodium [Alka-Seltzer, baking soda] should be avoided)
Nasal stuffiness may occur. Edema of the nasal mucosa is caused by high estrogen levels. Relief can be obtained by saline nasal drops or use of a humidifier.
Dyspnea is often encountered in late pregnancy as the uterus exerts pressure on the diaphragm. Even with mild exercise, many women are unable to breathe deeply. Most women notice improvement in dyspnea with “lightening” (about 2 weeks before birth with the first child). Suggestions for relief include the following:
Leg cramps may occur in the first 6 weeks of pregnancy but are more often experienced during the third trimester. The superficial calf muscles of the legs involuntarily contract, causing severe pain. Increased uterine weight, increased circulatory load, inadequate rest, and imbalance of the calcium-to-phosphorus ratio are implicated as causes. Intake of phosphorus may exceed the calcium intake, resulting in a calcium-to-phosphorus imbalance. Measures to relieve leg cramps include the following:
• Extending the affected leg, keeping the knee straight, and flexing the foot
• Standing and applying pressure on the affected leg to stretch the muscles in spasm
• Elevating the legs periodically during the day to improve circulation
• Consulting the health care provider about reducing milk intake or using aluminum hydroxide capsules to restore an ideal calcium/phosphorus ratio
Edema of the lower extremities is common, especially after the twentieth week of pregnancy. It is caused by the increased circulatory load and slower venous return of blood from the legs. Edema in the face and the hands may be a sign of gestational hypertension and should be reported to the health care provider. Temporary relief measures for lower extremity edema include the following:
• Elevation of legs above the heart
• Avoidance of tight restrictive bands around the legs, such as garters, knee-highs, or thigh-high stockings
Water aerobics in healthy women can relieve edema because the hydrostatic pressure forces fluid into the circulation, stimulating glomerular filtration and excretion of water. Care should be taken to avoid excessive water temperatures during water aerobics (see Exercise During Pregnancy on pp. 62-64).
Psychosocial Adaptation to Pregnancy
Pregnancy creates a variety of confusing feelings for all members of the family, whether or not the pregnancy was planned. Both parents may feel ambivalence about the pregnancy and being a parent. First-time parents may be anxious about how the infant will affect their relationship as a couple. Parents who already have a child may wonder how they can stretch their energies, love, and finances to another infant and how the infant will affect their older child or children. The nurse who provides prenatal care helps families to work through this phase in their lives. Identifying and managing psychosocial problems is essential to the positive outcome of pregnancy.
Identifying barriers to accessing care is a primary nursing responsibility. Inadequate health insurance coverage, financial problems, knowledge deficit concerning community resources, lack of transportation, and need for day care for other children or older adult parents are examples of problems that can be referred to a social service worker. Frequent housing relocation may indicate domestic violence, legal problems, or financial difficulties that may need attention to ensure compliance with regular prenatal care. Nutritional needs and patterns relating to age, ethnicity, or financial constraints should be discussed. Tobacco or substance abuse should be assessed. Stress in the life of the mother should be reviewed, and appropriate referrals to mental health professionals or educational programs should be made to reduce the levels of stress that can affect pregnancy outcome.
Impact on the Mother
In 1984, researcher Reva Rubin noted four maternal tasks that the woman accomplishes during pregnancy as she becomes a mother:
1. Seeking safe passage for herself and her fetus: This involves both obtaining health care by a professional and adhering to important cultural practices.
2. Securing acceptance of herself as a mother and for her fetus: Will her partner accept the infant? Does her partner or family have strong preferences for a child of a particular sex? Will the child be accepted even if he or she does not fit the ideal?
3. Learning to give of self and to receive the care and concern of others: The woman will never again be the same carefree girl she was before her infant’s arrival. She depends on others in ways she has not experienced before.
4. Committing herself to the child as she progresses through pregnancy: Much of the emotional work of pregnancy involves protecting and nurturing the fetus.
Pregnancy is more than a physical event in a woman’s life. During the months of pregnancy, she first accepts the fetus as part of herself and gradually moves to acceptance of the child as an independent person. She evolves from being a pregnant woman to being a mother. The woman’s responses change as pregnancy progresses. These changes will be discussed here within the framework of the three trimesters of pregnancy.
First Trimester
The woman may have difficulty believing that she is pregnant during early pregnancy because she may not feel different. If a home pregnancy test was positive, the woman often feels “more pregnant” after a professional confirms it. An early sonography examination helps the woman to see the reality of the developing fetus within her. Women (and their partners) often show off their sonogram photos just as they will show their infant pictures later.
Most women have conflicting feelings about being pregnant (ambivalence) during the early weeks. Many, if not most, pregnancies are unplanned. The parents may have wanted to wait longer so they could achieve career or educational goals or to have longer spacing between children. Women who have planned their pregnancies, or even worked hard to overcome infertility, also feel ambivalence. They wonder if they have done the right thing and at the right time. Moreover, the woman often feels that she should not have these conflicting feelings. The nurse can help the woman to express these feelings of ambivalence and reassure her that they are normal.
The woman focuses on herself during this time. She feels many new physical sensations, but none of them seem related to a child. These physical changes and the higher hormone levels cause her emotions to be more unstable (labile). The nurse can reassure the woman and her partner (who is often confused by her moods) about their cause, that they are normal, and that they will stabilize after pregnancy.
Second Trimester
The fetus becomes real to the woman during the second trimester. Her weight increases, and the uterus becomes obvious as it ascends into the abdomen. If she has not already heard the fetal heartbeat or seen it beating on a sonogram, the woman usually will have an opportunity to hear it early in the second trimester. She feels fetal movement, and this is a powerful aid in helping her to distinguish the fetus as a separate person from herself.
The second trimester is a more stable time during pregnancy during which most women have resolved many of their earlier feelings of ambivalence and begin to take on the role of an expectant mother. The woman becomes totally involved with her developing child and her changing body image (narcissism). She often devotes a great deal of time to selecting just the right foods and the best environment to promote her health and that of her infant. She welcomes the solicitous concern of others when they caution her not to pick up a heavy package or work too hard. She may lose interest in work or other activities as she devotes herself to the project of nurturing her fetus. The nurse can take advantage of her heightened interest in healthful living to teach good nutrition and other habits that can benefit the woman and her family long after the child is born.
The woman “tries on” the role of mother by learning what infants are like. She wants to hear stories of what she and her mate were like when they were infants. She often fantasizes about how her child will look and behave or what sex the child will be. She may or may not want to know the sex of the infant if it is apparent on a sonogram, sometimes preferring to be surprised at the birth. The woman who has had a child before undergoes a similar transition as she imagines what this specific child will be like and how he or she will compare to any siblings.
The body changes of pregnancy become evident during the second trimester. The woman may welcome them as a sign to all that her fetus is well protected and thriving (Figure 4-10). However, these same changes may be unwelcome to her because they can be perceived as unattractive and cause discomfort.

FIGURE 4-10 The body changes of pregnancy are evident, and the woman may welcome them as a sign to all that her pregnancy is real and her fetus is thriving.
The body changes may alter her sexual relationship with her partner as well. Both partners may fear harming the developing fetus, particularly if there has been a previous miscarriage. Her increasing size, discomforts, and the other changes of pregnancy may make one or both partners have less interest in intercourse. The nurse can assure them that these changes are temporary and help them explore other expressions of love and caring.
Third Trimester
As her body changes even more dramatically, a woman alternates between feeling “absolutely beautiful and productive” and feeling “as big as a house and totally unloved” by her partner. These mood swings reflect her sense of increased vulnerability and dependence on her partner. She becomes introspective about the challenge of labor that is ahead and its outcome. Her moods may again be more labile.
The woman begins to separate herself from the pregnancy and to commit herself to the care of an infant. She and her partner begin making concrete preparations for the infant’s arrival. They buy clothes and equipment the infant will need. Many take childbirth preparation classes. The woman’s thinking gradually shifts from “I am pregnant” to “I am going to be a mother.”
The minor discomforts of pregnancy become tiresome during the last weeks before delivery, and the woman may feel that the pregnancy will never end. With the understanding and support of her family and health care professionals, she can develop inner strength to accomplish the tasks of birth.
Impact on the Father
Responses of fathers vary widely. Some want to be fully involved in the physical and emotional aspects of pregnancy. Others prefer a management role, helping the woman adhere to recommendations of her physician or nurse-midwife. Some fathers want to “be there” for the woman, but prefer not to take an active role during pregnancy or birth. Cultural values influence the role of fathers because pregnancy and birth are viewed exclusively as women’s work in some cultures. The nurse should not assume that a father is disinterested if he takes a less active role in pregnancy and birth.
Fathers go through phases similar to those of expectant mothers. Pregnancy is considered the beginning of a separate developmental stage called “Growth and Development of a Parent” (see Table 15-5). Fathers who do not anticipate changes specific to the normal event of pregnancy may be confused or concerned by new feelings or behaviors and the changes that occur in family dynamics.
For fathers, the announcement phase begins when pregnancy is confirmed. Initially they may also have difficulty perceiving the fetus as real. Ambivalence and self-questioning about their readiness for fatherhood are typical. Fathers who attend prenatal appointments with the woman can see the fetus on ultrasound or hear the fetal heartbeat, making the child seem more like a real person (Figure 4-11). Acceptance of the pregnancy results in strengthening of the family support system and expansion of the social network. Rejection of the pregnancy may result in lack of communication and resentment.

FIGURE 4-11 The father begins to develop a relationship with the fetus as he hears the fetal heartbeat and feels fetal movement.
The second phase of the father’s response is the adjustment phase. The father may revise financial plans, become involved in planning the child’s room or furniture, and actively listen to the fetal heartbeat and feel fetal movement (see Figure 4-11). Lack of adjustment may result in an increase in outside interests, or development of various symptoms in a struggle to regain attention he may feel has been lost to the fetus.
The third phase of the father’s response is the focus phase, where active plans for participation in the labor process, birth, and change in lifestyle result in the partner “feeling like a father” (Box 4-4). The nurse’s role is to help the father achieve positive outcomes in each phase (see Table 4-6 on pp. 73-75).
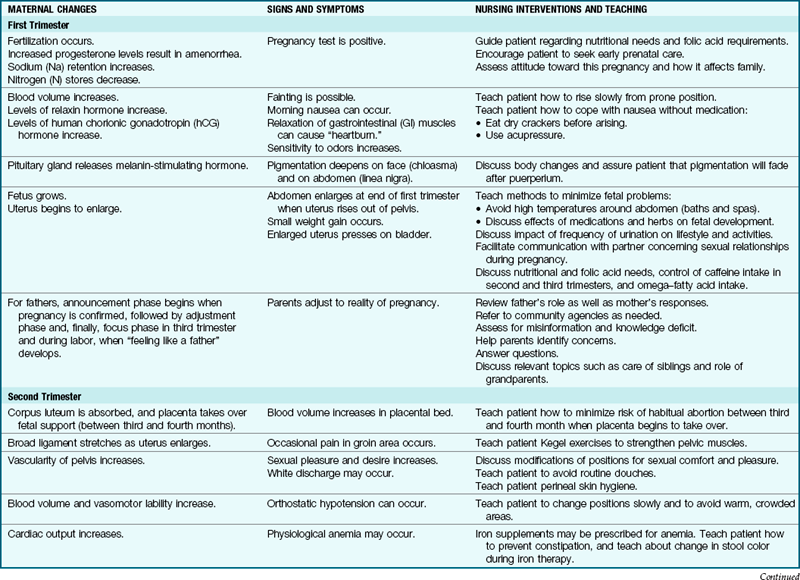
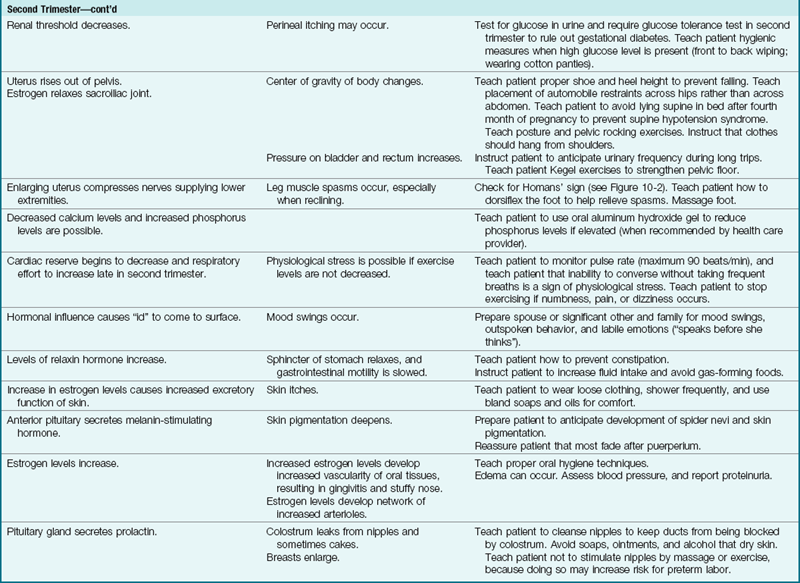
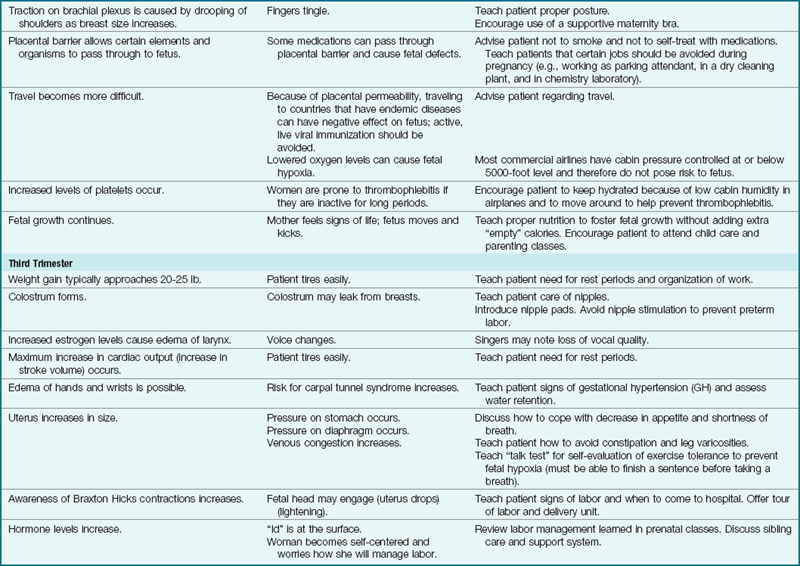
The father is often asked to provide emotional support to his partner while struggling with the issue of fatherhood himself. Too often, he receives the message that his only job is to support the pregnant woman rather than being a parent who is also important and has needs. The nurse should explore the father’s feelings and encourage him during prenatal appointments, childbirth preparation classes, and labor and birth. He is trying to learn the role of father, just as the woman is trying to learn the role of mother.
Impact on the Pregnant Adolescent
Pregnant adolescents often have to struggle with feelings they find difficult to express. They are fraught with conflict about how to handle an unplanned pregnancy. Initially, they must face the anxiety of breaking the news to their parents and the father of the child. Denial of the pregnancy until late in gestation is not uncommon. There may be financial problems, shame, guilt, relationship problems with the infant’s father, and feelings of low self-esteem. Alcoholism and substance abuse may be a part of the complex picture.
The nurse must assess the girl’s developmental and educational level and her support system to best provide care for her. A critical variable is the girl’s age. Young adolescents have difficulty considering the needs of others, such as the fetus. The nurse helps the adolescent girl to complete the developmental tasks of adolescence while assuming the new role of motherhood. Ideally, separate prenatal classes tailored to their needs help adolescent girls learn to care for themselves and assume the role of mother.
The nurse must anticipate resistive behavior, ambivalence, and inconsistency in the adolescent. The nurse must consider the girl’s developmental level and the priorities typical of her age, such as the importance of her peer group, focus on appearance, and difficulty considering the needs of others. The pregnant adolescent must cope with two of life’s most stress-laden transitions simultaneously: adolescence and parenthood.
Impact on the Older Couple
Women who become pregnant for the first time after age 35 years are described as “elderly primips” or “advanced maternal age” because they are at a later stage in their childbearing cycle, and they may face special problems during pregnancy and labor. Many factors contribute to the trend of postponing pregnancy until after age 35 years:
• Effective birth control alternatives
• Increasing career options for women
• High cost of living (delays childbearing until financial status is secure)
• Development of fertilization techniques to enable later pregnancy
The “older couple” usually adjusts readily to pregnancy because they are often well-educated, have achieved life experiences that enable them to cope with the realities of parenthood, and are ready for the lifestyle change. Although the older couple may adjust to the process of pregnancy and parenthood, they may find themselves “different” from their peers, and this can result in impaired social interaction. Concerns of the older parent relate to age and energy level as the child grows, confronting the issues of their own mortality, and child care requirements. Meeting financial needs of a college-age child at retirement is a special issue that may require discussion and planning. Many older parents are placed in a “high-risk” prenatal group that may limit their options for selecting a birth center. However, the pregnancy should be treated as normal unless problems are identified.
Advances in maternal care and delivery practices have decreased the risk of unfavorable pregnancy outcomes, although special problems exist. Women over age 35 years may have a decreased ability to adjust their uterine blood flow to meet the needs of the fetus (Creasy et al., 2009). There also may be an increase in multiple pregnancies if fertility drugs were used, which increases fetal risk. The increased risk of a congenital anomaly usually results in the offering of special tests during pregnancy (chorionic villi sampling, amniocentesis), which increases the cost factor of prenatal care.
Impact on the Single Mother
Whether an adolescent or a mature woman, the single mother has special emotional needs. Some single mothers can turn to their parents, siblings, or close friends for support. Women who do not have emotional support from significant others will have more difficulty completing the tasks of pregnancy. Their uncertainty in day-to-day living competes with mastering the emotional tasks of pregnancy.
Some single mothers may have conceived by in vitro fertilization because of a strong desire to have a child even in the absence of a stable relationship. These women often are nearing the end of their childbearing years and perceive a “now or never” view of motherhood. Single women who plan pregnancies often prepare for the financial and lifestyle changes. Achieving social acceptance is not as difficult today as it was many years ago when single motherhood was taboo and considered a distinct disgrace to the maternal family. The nurse should maintain a nonjudgmental attitude and assist the single mother to successfully achieve the psychological tasks of pregnancy.
Impact on the Single Father
The single father may take an active interest in and financial responsibility for the child. The couple may plan marriage eventually, but it is often delayed. A single father may provide emotional support for the mother during the pregnancy and birth. He often has strong feelings of surprise and accomplishment when he becomes aware of his partner’s pregnancy. He may want to participate in plans for the child and take part in infant care after birth. However, his participation is sometimes rejected by the woman.
Impact on Grandparents
Prospective grandparents have different reactions to a woman’s pregnancy as well. They may eagerly anticipate the announcement that a grandchild is on the way, or they may feel that they are not ready for the role of grandparent, which they equate with being old. The first grandchild often causes the most excitement in grandparents. Their reaction may be more subdued if they have several grandchildren, which may hurt the excited pregnant couple.
Grandparents have different ideas of how they will be involved with their grandchildren. Distance from the younger family dictates the degree of involvement for some. They may want to be fully involved in the plans for the infant and help with child care, and they often travel a great distance to be there for the big event. Other grandparents want less involvement because they welcome the freedom of a childless life again. Many grandparents are in their 40s and 50s, a time when their own career demands and care of their aging parents compete with their ability to be involved with grandchildren.
If grandparents and the expectant couple have similar views of their roles, little conflict is likely. However, disappointment and conflict may occur if the pregnant couple and the grandparents have significantly different expectations of their role and involvement. The nurse can help the young couple understand their parents’ reactions and help them to negotiate solutions to conflicts that are satisfactory to both generations.
Impact on Siblings
Preparation for arrival of a new baby in the family should start before the arrival of the newborn and before the sibling feels the change that a new family member brings. All siblings will be affected by the arrival of a new baby into the family. Young children may lack resources to cope with their feelings of being displaced, and some behavior changes may be expected. Special time and effort is needed to make the siblings feel they are loved as they were before.
Prenatal Education
Prenatal education is an interactive process that requires input from the patient concerning individual needs and assessment of outcome: a healthy mother and child and an intact family unit. A plan for prenatal education is based on the desired outcome and includes the development of positive attitudes and perceptions, achievement of knowledge of facts, and the learning of skills to cope with pregnancy, labor, and the transition into parenthood. Examples include the perception that pregnancy is a normal process that is enhanced by good nutrition and a healthy lifestyle; the knowledge to select the proper diet; and the learning of skills to perform exercises, breathing, and relaxation techniques to prepare the woman for labor.
Prenatal education should progress according to the nursing process, as follows:
• Assess the history and cultural needs.
• Diagnose the knowledge deficit.
• Plan the goals and priorities.
• Outcomes identification clarifies expected outcomes.
Collecting data to assess cultural needs can be individualized to the patient with the use of a birth plan (Figure 4-12). The birth plan can be presented in multiple languages, and the nurse can compare answers to the tool written in the nurse’s primary language. Prenatal teaching can be planned according to the nursing process. Teaching can occur in formal childbirth education classes or informally during a clinic visit. Every contact a nurse has with a pregnant patient is an opportunity for teaching.
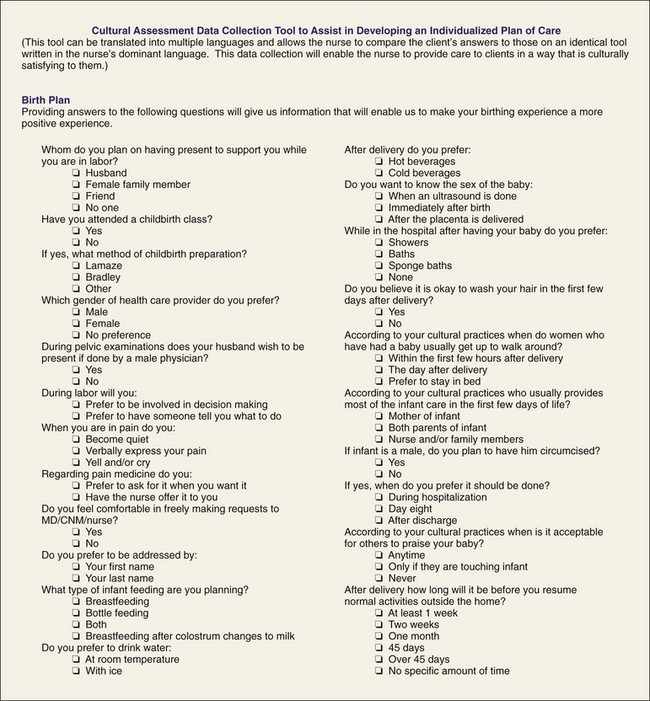
FIGURE 4-12 A birth plan is a cultural assessment data collection tool that is used to assist in developing an individualized plan of care. This tool can be translated into multiple languages and allows the nurse to compare the patient’s answers to an identical tool in the nurse’s dominant language, thus enabling the nurse to provide care that is culturally sensitive.
The Effect of Pregnancy and Lactation on Medication Metabolism
The physiological changes in pregnancy affect the metabolism of medications administered to the mother. Subtherapeutic drug levels may occur because of the increased plasma volume, cardiac output, and glomerular filtration that occur during pregnancy. A decreased gastric emptying time during pregnancy changes absorption of drugs and can delay onset of action. Parenteral medication may be absorbed more rapidly because of increased blood flow and may have a faster onset of action than in the nonpregnant state. The increased levels of estrogen and progesterone may alter hepatic (liver) function, resulting in drug accumulation in the body.
Drugs can cross the placenta and have an impact on fetal development, especially in the first trimester, and have increased absorption levels in the developing fetus in the third trimester. The mother should be instructed to check with her health care provider before taking over-the-counter medications. Taking ibuprofen in the third trimester can cause early closure of the ductus arteriosus, resulting in fetal distress.
Drugs can pass into breast milk by diffusion and be ingested by the neonate during breastfeeding. If the lactating mother must take a medication, it should be administered immediately after the infant breastfeeds to minimize passage to the infant. The U.S. Food and Drug Administration (FDA) has established a series of risk categories for medication use during pregnancy, and it is published in most drug books nurses can use as a reference. All women of childbearing age should be counseled about the risk of ingesting drugs during pregnancy and lactation. Pregnancy risk categories allow for some assessment of risk to the fetus when a drug is prescribed in a pregnant woman (Box 4-5).
Immunizations During Pregnancy
Live-virus vaccines are contraindicated during pregnancy because of possible adverse effects on the fetus. The Immunization Action Coalition (2010) has developed a screening questionnaire to determine if a vaccination is contraindicated or appropriate for a patient. Products containing thimerosal should not be given to pregnant women because of the risk of mercury poisoning. Most vaccines are available in an alternative thimerosal-free form to be used for women who are pregnant. Vaccines contraindicated during pregnancy include bacille Calmette-Guerin (BCG), human papillomavirus (HPV), live attenuated influenza vaccine (LAIV) in nasal spray form because it is a live virus (CDC, 2008), and measles, mumps, and rubella (MMR). A woman is advised to avoid pregnancy for at least 1 month following an MMR immunization.
When exposure to or high risk of infection is present, vaccinations allowable during pregnancy include hepatitis A and B; inactivated influenza; meningococcal (MCV-4), only if the patient is at high risk for disease; pneumococcal polysaccharide vaccine (PPV) in high-risk women; inactivated polio vaccine when immediate protection is required; rabies if risk for infection is high; and tetanus-diphtheria (Td) after 29 weeks of gestation. Pregnant women at high risk of infection can also be given the vaccine for Japanese encephalitis and anthrax (CDC, 2008). The H1N1 flu vaccination is also recommended to protect pregnant women. Vaccines in vials with natural rubber tops should not be administered to women who are allergic to latex.
Nursing Care During Pregnancy
Table 4-6 describes the physiological and psychological changes that occur during pregnancy, the related signs and symptoms noted in the patient, and some suggested nursing interventions or teaching points appropriate to that phase. The rationales for a nursing care plan can be based on the information within this table. Teaching for the prenatal patient should include the risks of smoking, alcohol use, and illicit drug use as well as the advantages of breastfeeding and good nutrition during pregnancy.
Get Ready for the NCLEX® Examination!
Key Points
• Early and regular prenatal care promotes the healthiest possible outcome for mother and infant.
• The woman’s estimated date of delivery is calculated from her last normal menstrual period.
• The length of a pregnancy is 40 weeks after the last normal menstrual period plus or minus 2 weeks. The expected date of delivery is determined by using Nägele’s rule.
• Presumptive signs of pregnancy often have other causes. Probable signs more strongly suggest pregnancy, but can still be caused by other conditions. Positive signs have no other cause except pregnancy. The three positive signs of pregnancy include detection of a fetal heartbeat, recognition of fetal movements by a trained examiner, and visualization of the embryo or fetus on ultrasound.
• The optimal weight gain during pregnancy is 55 to 77 kg (25 to 35 lb).
• The uterus undergoes the most obvious changes in pregnancy: it increases in weight from approximately 60 g (2 oz) to 1000 g (2.2 lb); it increases in capacity from about 10 mL ( oz) to 5000 mL (5 quarts). Pregnancy affects all body systems.
oz) to 5000 mL (5 quarts). Pregnancy affects all body systems.
• The mother’s blood volume is about 45% greater than her prepregnant volume to enable perfusion of the placenta and extra-maternal tissues. Her blood pressure does not increase because resistance to blood flow in her arteries decreases. The fluid portion of her blood increases more than the cellular portion, resulting in a pseudoanemia.
• The common discomforts of pregnancy occur as a result of hormonal, physiological, and anatomical changes normally occurring during pregnancy. The nurse should teach relief measures and abnormal signs to report to the health care provider.
• Supine hypotension syndrome, also known as aortocaval compression or vena cava syndrome, may occur if the pregnant woman lies flat on her back. Turning to one side or placing a small pillow under one hip can help relieve this hypotension.
• To provide for the growth of the fetus and maternal tissues, the mother needs 300 extra, high-quality calories daily. Important nutrients that must be increased are protein, calcium, iron, and folic acid. Five hundred extra calories a day are needed for lactation.
• Adequate folic acid intake before conception can reduce the incidence of neural tube defects such as anencephaly or spina bifida. The CDC (2009) recommends that all fertile women consume 400 mg (0.4 mcg) of folic acid daily.
• Fathers should be included in prenatal care to the extent they and the woman desire.
• Adaptation to pregnancy occurs in the mother, the father, and other family members. Prenatal care involves physical and psychological aspects and should be family centered.
• Childbirth education includes formal classes and informal counseling. Education should include nutrition, prenatal visits, exercise, breathing and relaxation techniques, the birth process, safety issues, and beginning parenting skills.
• Live virus vaccines are contraindicated during pregnancy.
• The physiological changes during pregnancy influence the metabolism of ingested medications.
• Medications ingested during pregnancy can affect fetal development.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish translations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• The Alexander Technique: www.alexandertechnique.com/articles
• The Bradley Method of natural childbirth: www.bradleybirth.com/cc.htm
• Exercise during pregnancy: http://csep.ca/forms.asp
• Lamaze International: www.lamaze.org
• MyPyramid: www.mypyramid.gov/
• Patient care updates: www.patientcareonline.com
• Pregnancy and childbirth prenatal care: www.makewayforbaby.com/prenatalcare.htm
Review Questions for the NCLEX® Examination
1. A woman is having a prenatal visit at 18 weeks of gestation. Why is it important to ask her about fetal movement?
1. Absence of fetal movement at this time suggests that the pregnancy is more advanced than her dates indicate.
2. Denial of fetal movement at this stage in pregnancy may indicate that the woman is not accepting her pregnancy.
3. If she has started feeling fetal movement, the fetal heartbeat will be checked with a fetoscope to confirm that the fetus is living.
4. Fetal movement is first felt by the mother about this time and provides a marker for approximate gestational age.
2. A pregnant woman complains that she has a large amount of vaginal secretions. The next most appropriate nursing action is to:
1. consult her nurse-midwife for a cream or douche.
2. ask her if the discharge is irritating or causes itching.
3. During a prenatal examination at 30 weeks of gestation, a woman is lying on her back on the examining table. She suddenly complains of dizziness and feeling faint. The most appropriate response of the nurse would be to:
1. reassure the woman and take measures to reduce her anxiety level.
2. offer the woman some orange juice or other rapidly absorbed form of glucose.
4. A woman being seen for her first prenatal care appointment has a positive home pregnancy test, and her chart shows a TPALM recording of 40120. The nurse would anticipate that:
1. minimal prenatal teaching will be required because this is her fourth pregnancy.
2. the woman will need help in planning the care of her other children at home during her labor and delivery.
3. the woman should experience minimal anxiety because she is familiar with the progress of pregnancy.
4. this pregnancy will be considered high risk, and measures to reduce anxiety will be needed.
Critical Thinking Questions
1. A 35-year-old primipara woman in her twentieth week of pregnancy states she does not want to drink the liquid glucose for the routine blood glucose screen because it does not taste good. She states she is not a diabetic and does not think the test is necessary for her. What is the best response by the nurse?
2. A woman entering her second trimester of pregnancy states that she is noticing increasing stretch marks on her abdomen. She is afraid these marks will remain prominent after pregnancy and wants to go on a low-calorie diet to prevent her abdomen from getting too large. What information should the nurse include in her teaching plan for this patient?