An Overview of Growth, Development, and Nutrition
1 Define each key term listed.
2 Explain the differences between growth, development, and maturation.
3 Recognize and read a growth chart for children.
4 List five factors that influence growth and development.
5 Discuss the nursing implications of growth and development.
6 Discuss the importance of family-centered care in pediatrics.
7 Recognize the influence of the family and cultural practices on growth, development, nutrition, and health care.
8 Describe three developmental theories and their impact on planning the nursing care of children.
9 Discuss the nutritional needs of growing children.
10 Differentiate between permanent and deciduous teeth, and list the times of their eruption.
11 Understand the characteristics of play at various age levels.
12 Describe the relationship of play to physical, cognitive, and emotional development.
13 Understand the role of computers and computer games in play at various ages.
 , p. 350)
, p. 350) , p. 364)
, p. 364) , p. 380)
, p. 380) , p. 381)
, p. 381) , p. 364)
, p. 364) , p. 350)
, p. 350) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Growth and Development
The main difference between caring for the adult and caring for the child is that the latter is in a continuous process of growth and development. This process is orderly and proceeds from the simple to the more complex (Box 15-1). Although the process is orderly, it is not steadily paced. Growth spurts are often followed by plateaus. One of the most noticeable growth spurts is at the time of puberty. The rate of growth varies with the individual child. Each infant has an individual timetable that revolves around established norms. Siblings within a family vary in growth rate. Growth is measurable and can be observed and studied. This is done by comparing height, weight, increase in vocabulary, physical skills, and other parameters. There are variations in growth within the systems and the subsystems. Not all parts mature at the same time. Skeletal growth approximates whole-body growth, whereas the brain, lymph, and reproductive tissues follow distinct and individual sequences.
Box 15-1
Emerging Patterns of Behavior from Age 1 to 5 Years
Motor: Walks with one hand held; rises independently; takes several steps
Adaptive: Picks up pellet with pincer action of thumb and forefinger; releases object to another person on request
Language: Says “mama,” “dada,” and a few similar words
Social: Plays simple ball game; makes postural adjustment to dressing
Motor: Runs stiffly; sits on small chair; walks up stairs with one hand held; explores drawers and wastebaskets
Adaptive: Makes tower of four cubes; imitates vertical stroke; imitates scribbling; dumps pellet from bottle
Language: 10 words (average); names pictures; identifies one or more parts of body
Social: Feeds self; seeks help when in trouble; may complain when wet or soiled; kisses caregivers with pucker
Motor: Runs well; walks up and down stairs, one step at a time; opens doors; climbs on furniture; jumps
Adaptive: Tower of seven cubes (six at 21 months); circular scribbling; imitates horizontal stroke; folds paper once imitatively
Language: Puts three words together (subject, verb, object)
Social: Handles spoon well; often tells immediate experiences; helps to undress; listens to stories with pictures; plays in parallel with other children
 Years
YearsMotor: Rides tricycle; stands momentarily on one foot
Adaptive: Tower of 10 cubes; imitates construction of “bridge” of three cubes; copies a circle; imitates a cross
Language: Knows age and sex; counts three objects correctly; repeats three numbers or a sentence of six syllables
Social: Plays simple games (cooperative play is highly imaginative); helps in dressing (unbuttons clothing and puts on shoes); washes hands
Motor: Hops on one foot; throws ball overhand; uses scissors to cut out pictures; climbs well
Adaptive: Copies bridge from model; imitates construction of “gate” of five cubes; copies cross and square; draws a man with two to four parts besides head; identifies longer of two lines
Language: Counts four pennies accurately; tells a story
Social: Plays with several children with beginning of social interaction and role playing; goes to toilet alone
Adaptive: Draws triangle from copy; identifies heavier of two weights
Language: Names four colors; repeats sentence of 10 syllables; counts 10 pennies correctly
Social: Dresses and undresses; asks questions about meaning of words; domestic role playing
Note: After 5 years the Stanford-Binet, the Wechsler-Bellevue, and other scales offer the most precise estimates of developmental level. To have the greatest value they should be administered only by an experienced and qualified person.
Modified from Kliegman, R., Behrman, R., Jenson, H., & Stanton, B. (2007). Nelson’s textbook of pediatrics (18th ed.). Philadelphia: Saunders. Data are derived from those of Gesell (as revised by Knobloch), Shirley, Provence, Wolf, Bailey, and others.
The Impact of Growth and Development on Nursing Care
Pediatrics is a subspecialty of medical-surgical nursing. Adult acute care units in a hospital may contain a separate neurology unit, a separate cardiac unit, a separate medical unit, and a separate surgical unit. On the pediatric acute care unit in the general hospital, all medical-surgical specialties are usually housed on one unit—for patients from newborn to adolescent. The developmental needs of the child have an impact on his or her response to illness and on the approach the nurse must take in developing a plan of care. Choosing the right words to explain to a child what will happen is essential. For example, if the nurse states that the child will be “put to sleep” before the operation, will the child relate that to a pet at home being “put to sleep” and never heard from again? The fractured jaw of an 8-month-old after a motor vehicle accident may affect his developmental process more seriously than the same injury in a 4-year-old, because the 8-month-old is in the oral phase of development.
Because the child differs from the adult both anatomically and physiologically, differences in response to therapy as well as in manifestations of illness can be anticipated. The nurse must understand the normal to recognize deviations within any age-group and to plan care that takes these developmental differences into consideration (Box 15-2).
 Nursing Tip
Nursing Tip
The nursing approach should be governed by the developmental level of the child and family values, with choices and active participation offered when appropriate.
An understanding of growth and development, including its predictable nature and individual variation, has value in the nursing process. Such knowledge is the basis of the nurse’s anticipatory guidance of parents. For example, the nurse who knows when the infant is likely to crawl can, at the appropriate age, expand teaching on safety precautions. The nurse also incorporates these precautions into nursing care plans in the hospital. Age-appropriate care cannot be administered without an understanding of growth and development.
While explaining various aspects of child care to families, the nurse stresses the importance of individual differences. Parents tend to compare their children’s development and behavior with those of other children and with information in popular magazine articles. This may relieve their anxiety or cause them to impose impossible expectations and standards. In addition, many parents had poor role models who influenced their own experiences as children. Lack of knowledge about parenting can be recognized by the nurse and suitable interventions begun.
The nurse who understands that each child is born with an individual temperament and “style of behavior” can help frustrated parents cope with a newborn who has difficulty settling into the new environment. Specific parameters can be used to determine whether an infant is merely on an individual timetable or whether the infant varies from normal.
The nurse must also recognize when to intervene to prevent disease and/or accidents. For example, a brief visit with a caregiver may reveal that the child’s immunizations are not up to date. A review with a teenage mother of the characteristics of a 2-year-old may prevent the ingestion of poisons. Complications of the newborn can be avoided by advising the expectant mother to avoid alcohol and cigarettes. Other threats to health may likewise be anticipated. Knowing that specific diseases are prevalent in certain age-groups, the nurse maintains a high level of suspicion when interacting with these patients. This approach, based on developmental knowledge, experience, and effective communication, helps to ensure a higher level of family care. Finally, the nurse must understand how to provide nursing care to children of various ages to enhance their physical, mental, emotional, and spiritual development according to their specific needs and comprehension.
Terminology
The following stages of growth and development are referred to throughout this text:
Growth refers to an increase in physical size and is measured in inches and pounds. Development refers to a progressive increase in the function of the body. These two terms are inseparable. Maturation (maturus, “ripe”) refers to the total way in which a person grows and develops, as dictated by inheritance (Box 15-3). Although maturation is independent of environment, its timing may be affected by environment.
Directional Patterns
Directional patterns are fundamental to all humans. Cephalocaudal development proceeds from head to toe. The infant is able to raise the head before being able to sit, and he or she gains control of the trunk before walking. The second pattern is proximodistal, or from midline to the periphery. Development proceeds from the center of the body to the periphery (Figure 15-1). These patterns occur bilaterally. Development also proceeds from the general to the specific. The infant grasps with the hands before pinching with the fingers.

Some Developmental Differences Between Children and Adults
Height refers to standing measurement, whereas length refers to measurement while the infant is in a recumbent position. At birth the newborn has an average length of about 50 cm (20 inches). Linear growth is caused mainly by skeletal growth. Growth fluctuates until maturity is reached. Infancy and puberty are both rapid growth periods. Height is generally a family trait, although there are exceptions. Good nutrition and general good health are instrumental in promoting linear growth. Height is measured during each well-child visit (Skill 15-1). The length of the infant usually increases about 2.5 cm (1 inch) per month for the first 6 months. By age 1 year, the birth length increases by 50% (mostly in the trunk area).
Skill 15-1 Assessing the Length and Height of Infants and Children








To determine height in order to calculate body surface area (BSA) measurement and to determine status on growth chart
Infants from Birth Until 2 Years
1. Measure infants from birth until age 2 years in the recumbent position.
2. Exert mild pressure on the knee to straighten the leg for crown-to-heel measurement. Use a tape measure or measuring mat (the leg should not be “pulled” to straighten by exerting pressure on the ankle.)

1. Measure children ages 2 to 18 years in the standing position. The body should be in alignment, with the head erect and the child looking straight ahead and shoulders, buttocks, and heels touching the wall. The child should not be wearing shoes and should stand on a paper barrier.
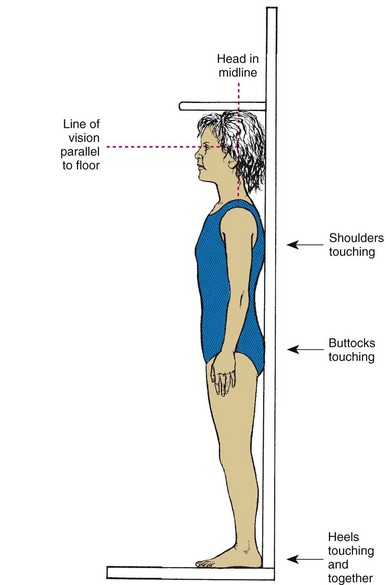
Children from 2 to 18 years are measured in the standing position. The body should be in alignment with the child looking straight ahead and shoulders, buttocks and heels touching the wall. The child should not be wearing shoes and should stand on a paper barrier. The height should be measured accurately and recorded.
Weight
Weight is another good index of health. However, the weight of a newborn infant does not always imply gestational maturity (see Chapter 13 and Figure 13-1). The average full-term newborn weighs 2.72 to 4.08 kg (6 to 9 lb), with an average of 3.4 kg (7.5 lb). Approximately 5% to 10% of the birth weight is lost by age 3 or 4 days as the result of the passage of stools and a limited fluid intake. The infant usually regains his or her birth weight by age 10 to 12 days. Birth weight usually doubles by age 5 to 6 months and triples by age 1 year. After the first year, weight gain levels off to approximately 1.81 to 2.72 kg (4 to 6 lb) per year, until the pubertal growth spurt begins.
Weight is determined at each office visit. A marked increase or decrease necessitates further investigation. The body weight of a newborn is composed of a higher percentage of water than in the adult. This extracellular fluid falls from 40% in the newborn to 20% in the adult. The high proportion of extracellular fluid in the infant can cause a more rapid loss of total body fluid, and therefore every infant must be closely monitored for dehydration. (See technique of weighing infants in Chapter 12 and Figure 12-11.)
Body Proportions
Body proportions of the child differ greatly from those of the adult (Figure 15-2). The head is the fastest-growing portion of the body during fetal life. During infancy the trunk grows rapidly, whereas during childhood, growth of the legs becomes the predominant feature. At adolescence, characteristic male and female proportions develop as childhood fat disappears. Alterations in proportions in the size of head, trunk, and extremities are characteristic of certain disturbances. Routine measurements of head and chest circumference are important indices of health.
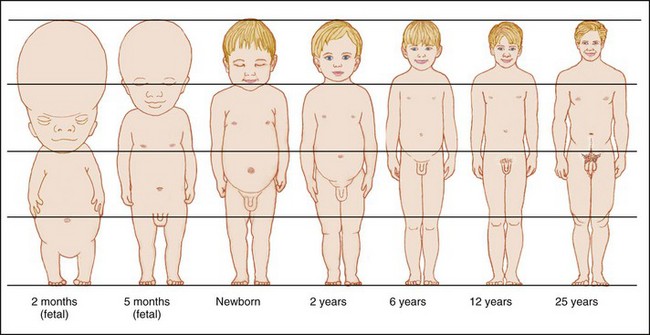
FIGURE 15-2 Changes in body proportions. Approximate changes in body proportions from fetal life through adulthood are shown. These changes in body proportions affect calculations of body surface area that are used to determine the percentages of body burns in burn injuries. (See the “rule of nines” in Chapter 30, Figure 30-15.)
Metabolic Rate
The metabolic rate (energy utilization and oxygen consumption) is higher in children than in adults. Infants require more calories, minerals, vitamins, and fluid in proportion to weight and height than adults. Higher metabolic rates are accompanied by an increased production of heat and waste products. The body surface area (BSA) of young children is far greater in relation to body weight than that of adults. The young child loses relatively more fluid from the pulmonary and integumentary systems.
Respirations
The respirations of infants are irregular and abdominal. Small airways can become easily blocked with mucus. The short, straight eustachian tube connects with the ear and predisposes the infant to middle ear infections. The chest wall is thin, and the muscles are immature, and therefore pressure on the chest can interfere with respiratory efforts.
Cardiovascular System
In neonates, the muscle mass of the right and left ventricles of the heart is almost equal. An increased need for cardiac output is often met by an increase in heart rate. Newborns have a high oxygen consumption and require a high cardiac output in the first few months of life. The presence of fetal (immature) hemoglobin in the first months of life also contributes to the need for a high cardiac output. The disappearance of fetal hemoglobin along with the loss of maternal iron stores contributes to the development of physiological anemia in infants after 3 or 4 months of age.
Immunity
For the first 3 months of life, the newborn is protected from illnesses to which the mother was exposed. The infant gradually produces his or her own immunoglobulin, until adult levels are reached by puberty. Therefore the infant and child must be protected from health care–associated infections in the hospital and from unnecessary exposure to pathogens. Immunizations against common childhood communicable diseases are discussed in Chapter 32.
Kidney Function
Kidney function is not mature until the end of the second year of life. Therefore drugs that are eliminated via the kidney can accumulate in the body to dangerous levels before age 2 years. Immature kidney function also predisposes the infant to dehydration. Nursing responsibilities for children under age 2 years include monitoring for dehydration and observing closely for toxic effects of drug therapy.
Nervous System
Maturation of the brain is evidenced by increased coordination, skills, and behaviors in the first years of life. Primitive reflexes, such as the grasp reflex, are replaced by purposeful, controlled movement. Head circumference increases 1.5 cm (0.6 inch) per month to an approximate total of 43 cm (17 inches) at age 6 months. During the second 6 months of life, head circumference increases 0.5 cm (0.2 inch) per month to an approximate total of 46 cm (18 inches) at 1 year of age. The age-appropriate toy is correlated with nervous system maturation. When selecting play activities, the nurse should consider the diagnosis and the child’s developmental level and abilities to be sure the toy is safe.
Sleep Patterns
Sleep patterns vary with age. The neonate sleeps 8 to 9 hours per night and naps an equal amount of time during the day. The 2-year-old may sleep 10 hours during the night and have only one short daytime nap. The 7-year-old usually requires 11 to 13 hours of sleep and rarely has a daytime nap. These patterns may be altered by cultural practices. For example, Israeli kibbutzim often have all family members nap after work or school, before dinner.
Bone Growth
Bone growth provides one of the best indicators of biological age. Bone age can be determined by x-ray studies. In the fetus, bones begin as connective tissue, which later is converted to cartilage. Cartilage is converted to bone through ossification. The rate of bone growth and the age of maturity vary within individuals, but the progression remains the same. Growth of the long bones continues until epiphyseal fusion occurs. Bone is constantly synthesized and resorbed. In children, bone synthesis is greater than bone destruction. Calcium reserves are stored in the ends of the long bones. Vitamin A, vitamin D, sunlight, and fluorine are necessary for the growth and development of skeletal and soft tissue.
Critical Periods
There appear to be certain periods when environmental events or stimuli have their maximum impact on the child’s development. The embryo, for example, can be adversely affected during times of rapid cell division. Certain viruses, drugs, and other agents are known to cause congenital anomalies during the first 3 months after conception. It is believed that issues such as developing a sense of trust during the first year of life and learning readiness are also subject to these periods of particular sensitivity.
Integration of Skills
As the child learns new skills, they are combined with those previously mastered. The child who is learning to walk may sit, pull the body up to a table by grasping it, balance, and take a cautious step. Tomorrow the child may take three steps! Children connect and perfect each skill in preparation for learning a more complex one.
Growth Standards
Growth is measured in dimensions such as height, weight, volume, and thickness of tissues. Measurement alone, without any standard of comparison, limits the interpretation of the data. A number of standards have been developed to make it possible to compare (1) the measurement of a child to others of the same age and sex (and, ideally, race), and (2) the child’s present measurements with the former rate of growth and pattern of progress. These standards, available as growth charts, are among the tools that have been used to assess the child’s overall development (Figure 15-3).
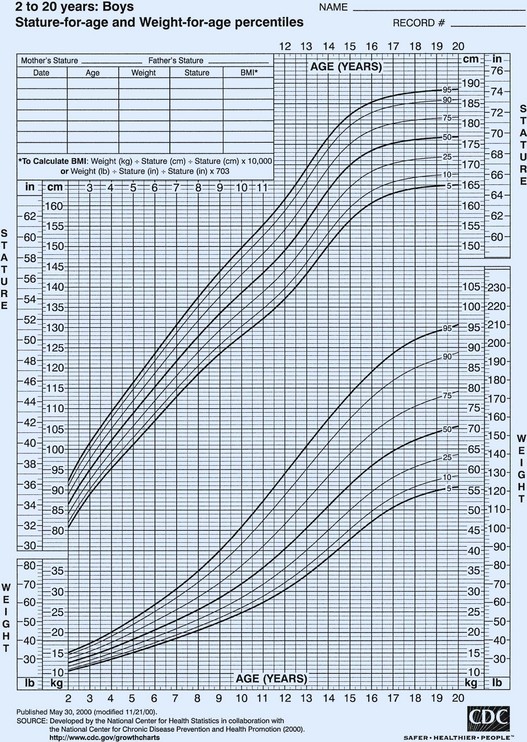
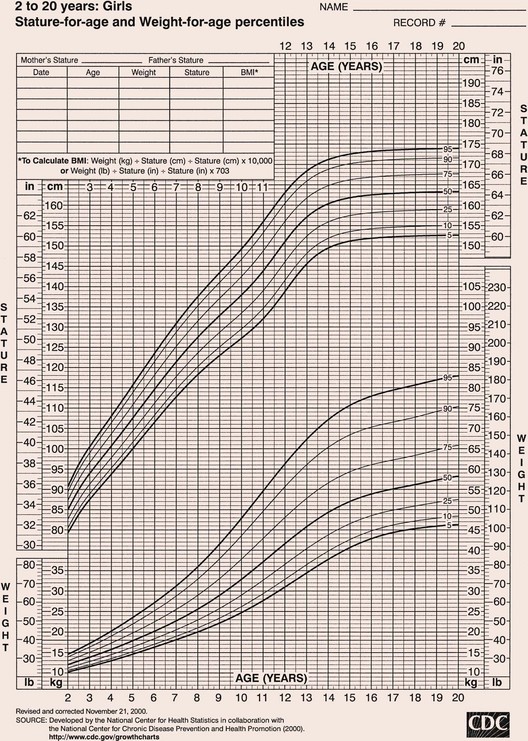
FIGURE 15-3 Sample of a complete growth chart, United States. Note the percentiles for height and weight. BMI, Body mass index.
Length refers to horizontal measurement; it is used before a child can stand, usually from birth to 2 years. Height is measured with the child standing, usually between 2 and 18 years. Some pointers in reading and interpreting growth charts are as follows:
• Children who are in good health tend to follow a consistent pattern of growth.
• At any age, there are wide individual differences in measured values.
• Percentile charts are customarily divided into either seven or eight percentile levels designated by lines. In general, these lines are labeled 95th, 90th, 75th, 50th, 25th, 10th, and 5th; or 97th, 95th, 90th, 75th, 50th, 25th, 10th, and 3rd.
• The median (middle), or 50th percentile, is designated by a solid black line. Percentile levels show the extent to which a child’s measurements deviate from the 50th percentile or middle measurement. A child whose weight is at the 75th percentile line is one percentile above the median. A child whose height is at the 25th percentile is one percentile below the median.
• A difference of two or more percentile levels between height and weight may suggest an underweight or overweight condition and prompts further investigation.
• Deviations of two or more percentile levels from an established growth pattern necessitate further evaluation.
Developmental Screening
Developmental screening is a vital component of child health assessment. One widely used tool is the Denver II, a revision of the Denver Developmental Screening test. This tool assesses the developmental status of children during the first 6 years of life in four categories: personal-social, fine motor-adaptive, language, and gross motor. It is not an intelligence test. Its purpose is to identify children who are unable to perform at a level comparable to their age-mates. A low score merely indicates a need for further evaluation. It is designed for use by both professionals and paraprofessionals. Proper administration and interpretation will aid in developing an individualized plan of care for the child.
Influencing Factors
Growth and development are influenced by many factors, such as heredity, nationality, race, ordinal position in the family, gender and environment. These factors are closely related and dependent on one another in their effect on growth and development. They make each person unique. If a child is ill, physically or emotionally, the developmental processes may be delayed.
Hereditary Traits
Characteristics derived from our ancestors are determined at the time of conception by countless genes within each chromosome. Each gene is made of a chemical substance called deoxyribonucleic acid (DNA), which plays an important part in determining inherited characteristics. Examples of inherited traits are eye color, hair color, and physical resemblances within families.
Nationality and Race
Many physical differences among people of various nationalities and races, who were formerly distinguished with ease, have become less apparent in our age of common environment and customs. For instance, a person of Japanese origin might be thought of as being of short stature. However, Japanese children living in the United States are comparable in height to other children in this country. Nevertheless, ethnic differences extend into many areas including speech, food preferences, family structure, religious orientation, and code of conduct. The nurse should ascertain cultural beliefs and practices when collecting data for nursing assessment (see Table 15-2 on pp. 358-364).
Ordinal Position in the Family
Whether the child is the youngest, the middle, or the oldest in the family has some bearing on growth and development. The youngest and middle children learn from their older sisters and brothers. However, motor development of the youngest may be prolonged if the child is babied by the others in the family. The only child or the oldest child may excel in language development because his or her conversations are mainly with adults. These children are often the object of greater parental expectations.
Gender
The male infant often weighs more and is slightly longer than the female. He grows and develops at a slightly different rate. Parents and relatives may treat boys differently from girls by providing “gender-appropriate” toys and play and by having different expectations of them. Current trends promote unisex activities in play and career development.
Environment
The physical condition of the newborn is influenced by the prenatal environment. The health of the mother at the time of conception and the amount and quality of her diet during pregnancy are important for proper fetal development. Infections or diseases may lead to malformations of the fetus. A healthy and strong newborn can easily adapt to its surroundings.
The home greatly influences the infant’s physical and emotional growth and development. If a family is financially strained by an added member and the parents are unable to provide nourishing foods and suitable housing, the infant is directly affected. An uneducated mother may not know how to properly cook foods to preserve their nutritional value. Immunizations and other medical attention may be neglected. The infant senses tension within the family and is affected by it.
In contrast, energies can be directed toward positive development when the surroundings are secure and stable and the infant feels secure, wanted, and loved. Most environments are neither completely positive nor completely negative but fall somewhere between the two extremes. Intelligence plays an important role in social and mental development. Potential intelligence is thought to be inherited but greatly affected by the environment.
The Family
The family has been defined in many different ways and fulfills many different purposes. Generally, a family is defined as two or more person’s living and interacting together. Traditionally, the nuclear family, or biological family, has been the basic unit of structure in American society (mother, father, siblings). Today many nuclear families do not share the same household because of single parenthood, divorce, and remarriage. Kinship lines have become blurred, and fundamental changes from what was once perceived as standard are occurring in the family. The extended family refers to three generations: grandparents, parents, and children. Because of an increasing life span, however, there are a greater number of living grandparents and great-grandparents, and the proportion of them living in the family home may increase. Table 15-1 lists the various types of families and gives a description of each.
Table 15-1
| TYPE OF FAMILY* | DESCRIPTION |
| Nuclear | Traditional—husband, wife, children (natural or adopted) |
| Extended | Grandparents, parents, children, relatives |
| Single-parent | Women or men establish separate households through individual preference, divorce, death, illegitimacy, or desertion |
| Foster-parent | Parents who care for children requiring parenting because of a dysfunctional family, no family, or individual problems |
| Alternative | Communal family |
| Dual-career | Both parents work outside the home because of desire or need |
| Blended | Remarriage of persons with children |
| Polygamous | More than one spouse |
| Homosexual | Two persons of the same sex adopt children or have children from a previous marriage |
| Cohabitation | Heterosexual or homosexual couples live together but remain unmarried |
*Not all family types may be legally sanctioned. A family is two or more persons who live and interact together.
The interactions of family unit members are by far the most influential aspect of family life in the growth and development of the child. The nurse must understand the interaction of the family unit to be able to effect a positive change that may be necessary to prevent or treat childhood illnesses. Some families have solid support systems and use available community resources to maintain health. Other families may lack support systems and require closer follow-up care and encouragement by the health team. Parenting is a learned behavior, often modeled by past experience and modified by the acceptance of specific roles and responsibilities. A family that does not provide for the optimum physical, psychological, and emotional health of the children is called a dysfunctional family. A dysfunctional family does not necessarily imply that its members are not loving and caring. A dysfunctional family does not know how to be successful in its efforts and interactions and requires intervention.
Historically, in middle-class families the father was the breadwinner and the mother managed the home and raised the children. This model has shifted. Because of changing economic conditions, both parents’ earnings may be necessary to maintain the family’s standard of living. In dual-career families both the father and the mother are often absent for most of the day because of long commutes or the demands of the working environment. Both parents may share child care and domestic chores. The parents may need to transfer to different locations to maintain their careers. This decreases extended family support and makes it necessary for children to change schools frequently.
Divorce, separation, death, and pregnancy outside marriage create many one-parent families. The percentage of children living in single-parent families has more than doubled since the 1970s. Most single-wage families have an economic disadvantage, but families with women as the sole wage earner often have considerably lower incomes than those in which men are the sole wage earner. The problem of providing good, affordable child care is a serious one for both dual-career families and single parents. Relatives and the noncustodial parent may assist in raising the child. Many single parents remarry, creating the blended family. The addition may be merely a stepfather or stepmother, or two families may unite. These family units must make many adjustments. To succeed, parents and children have to learn problem-solving techniques, communication skills, and flexibility.
A family APGAR, first described by Smilkstein and colleagues (1984), is a tool that can be used as a guide to assess family functioning. This assessment is valuable in determining the approach to home care needs:
• Adaptation: How the family helps and shares resources
• Partnership: Lines of communication and partnership in the family
• Growth: How responsibilities for growth and development of child are shared
• Affection: Overt and covert emotional interactions among family members
• Resolve: How time, money, and space are allocated to prevent and solve problems
Questions concerning each of these areas should be posed and evaluated. The goal in family assessment is to enable the nurse to develop interventions that aid the family to achieve a healthier adaptation to the child’s health needs or problems.
Nursing Tip
An infant who is hypersensitive to noise or touch needs the parent to understand the need for quiet surroundings. A chronically depressed parent may interpret fussiness or lack of smiling as rejection. Therefore an assessment of parent-child interaction is essential in the home, clinic, or hospital setting.
Nursing Tip
Special care may be required to assist in the growth and development of infants who are blind or whose parents are chronically depressed.
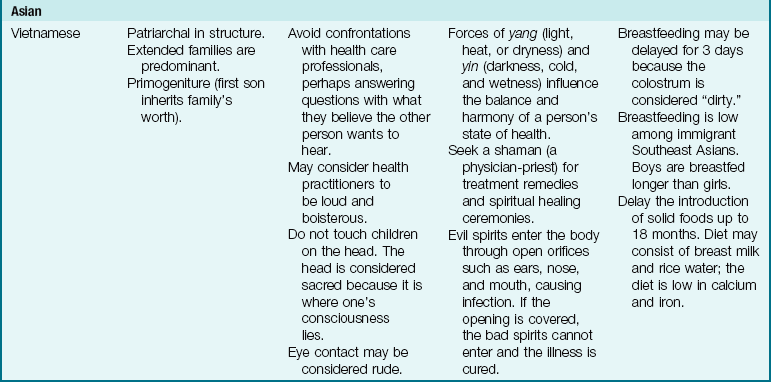
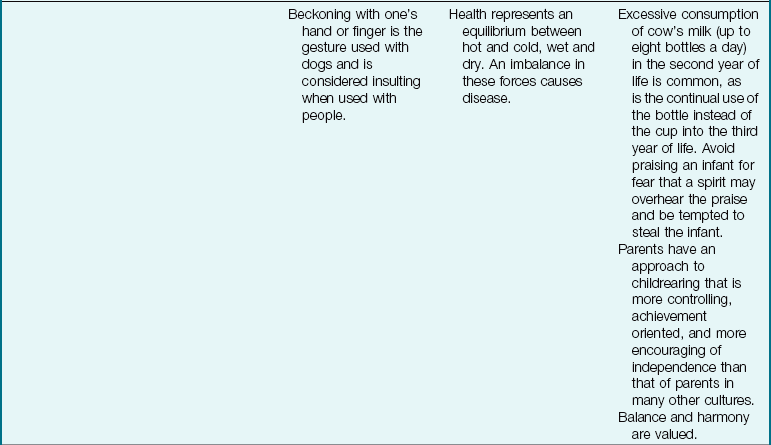
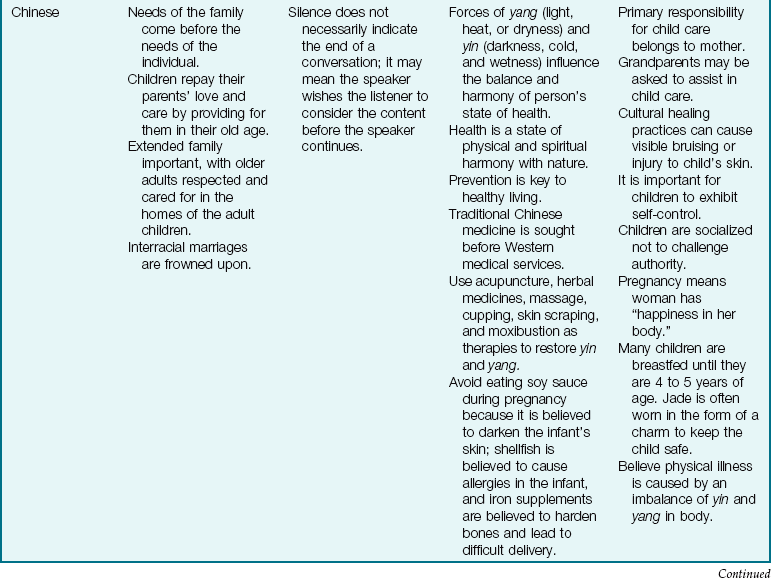
The Family as Part of a Community: The term community is defined in many ways, but here it is used to refer to the immediate geographical area in which the family lives and interacts (e.g., “I come from the South Side”). Families are greatly influenced by the communities in which they reside. Nurses must understand the culture of the community in which they work or to which the patient will return (Table 15-2). Assessment of the community is particularly important in creating discharge plans for families from various cultures. Their lives may be broadened or restricted depending on the facilities within the community. A few factors to consider are housing, access to public transportation, city services, safety, and health care delivery systems. The nurse has immediate access to the patient and therefore becomes an important liaison between various agencies that address specific needs.
Table 15-2
Cultural Influences on the Family
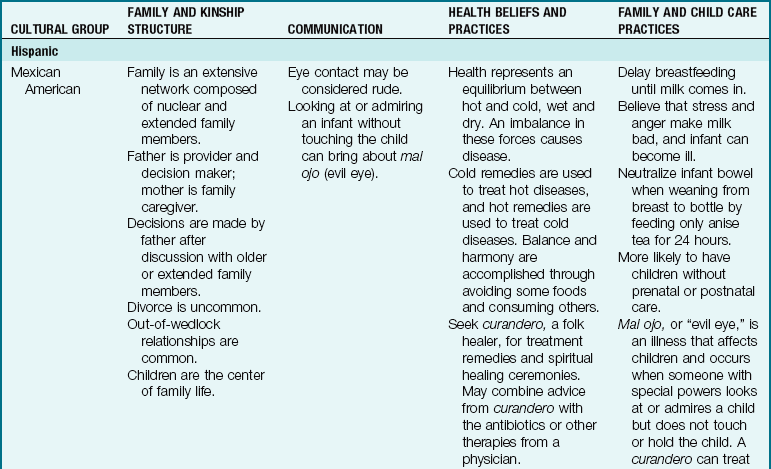
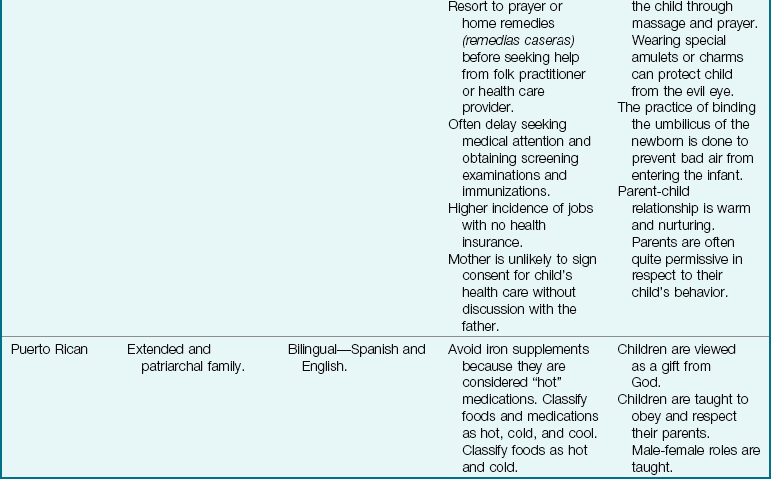
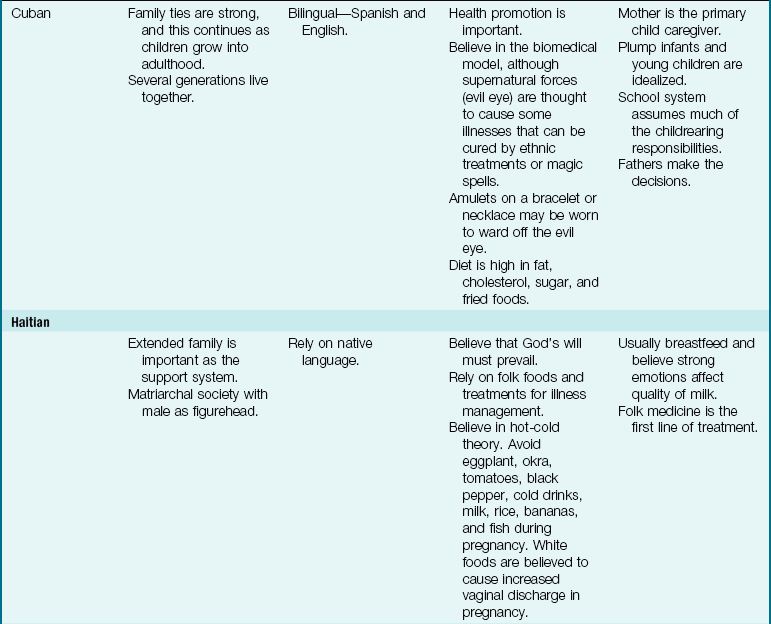
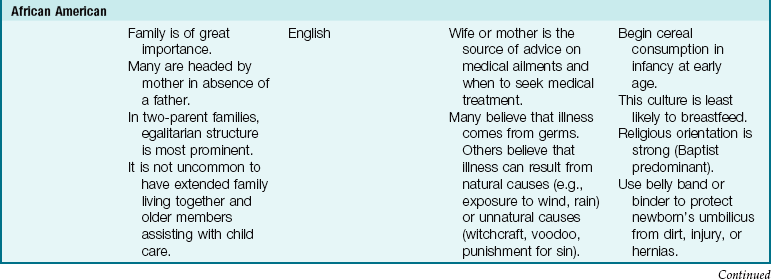
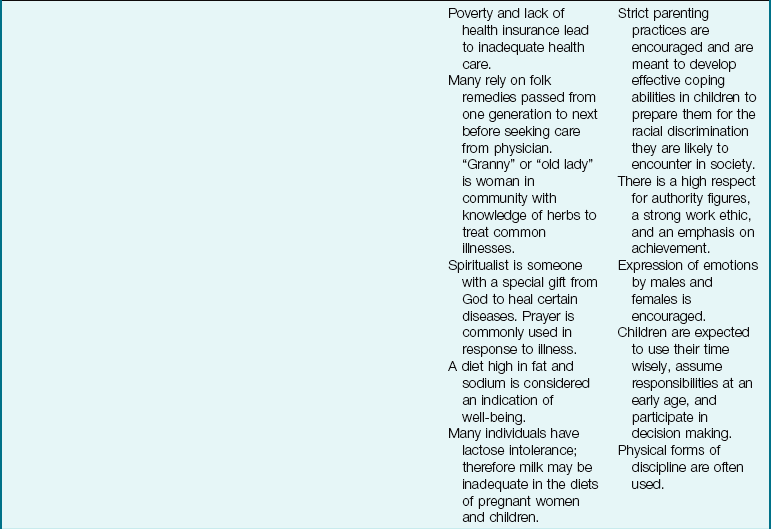
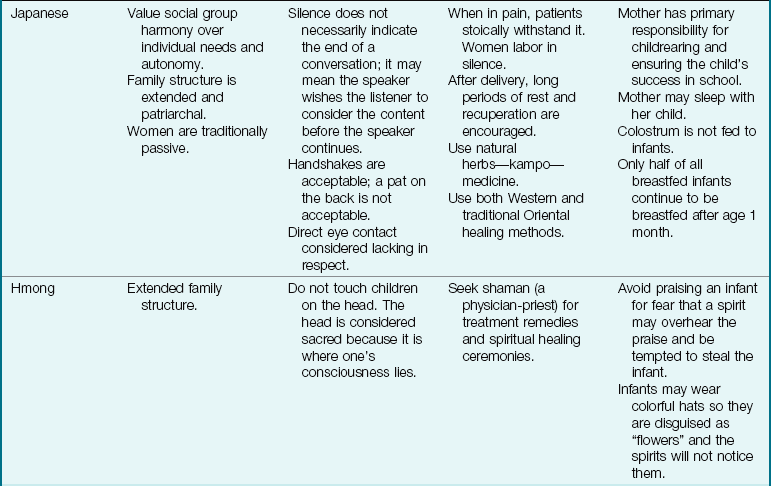
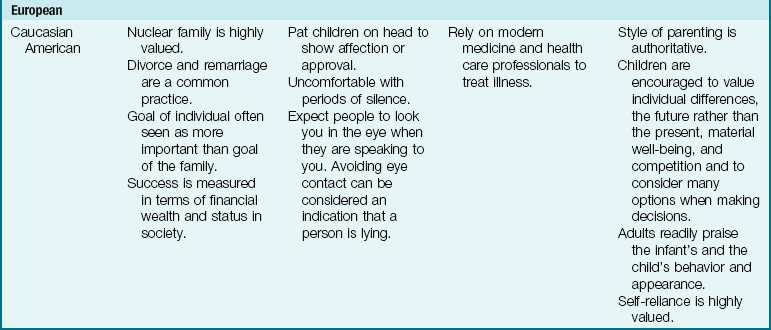
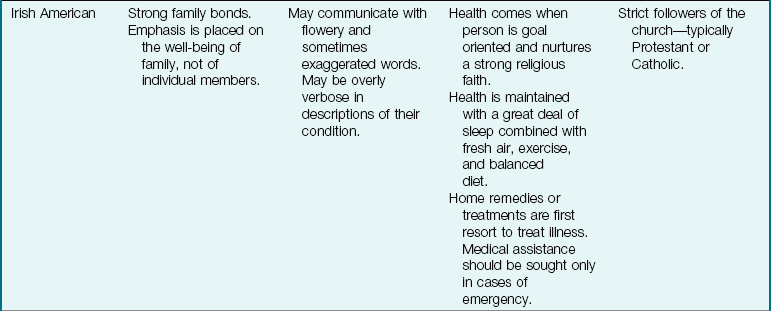
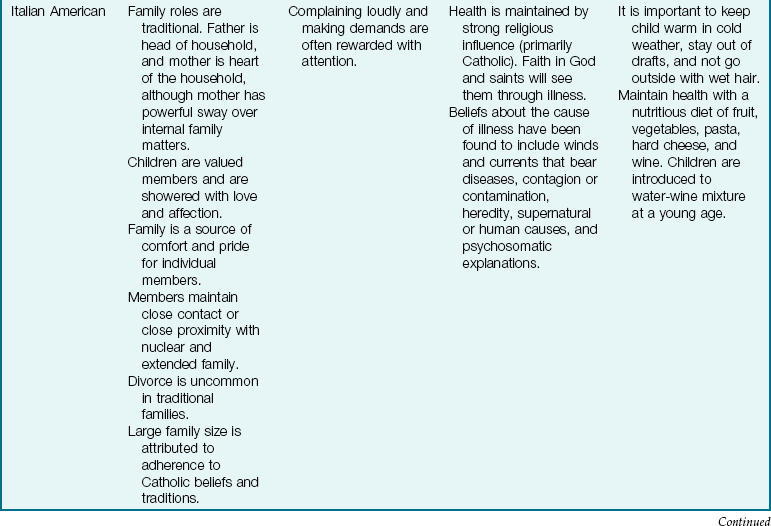
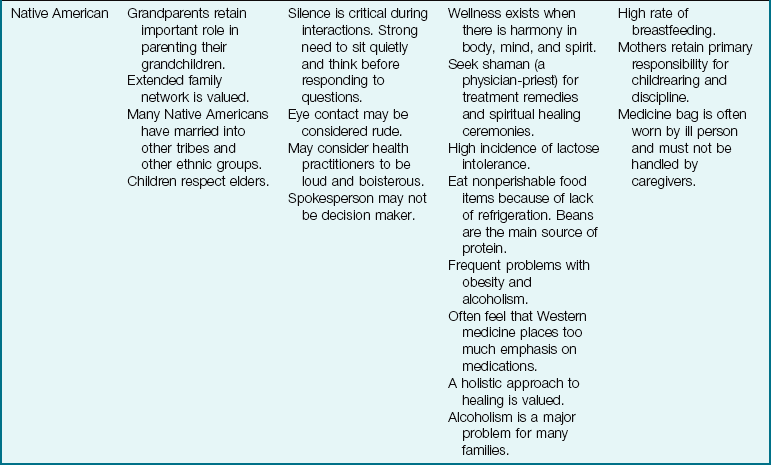
Modified from Bowden, V., Dickey, S., & Greenberg, C. (1998). Children and their families: The continuum of care. Philadelphia: Saunders; Lipson, J., & Dibble, S. (2005). Culture and nursing care (2nd ed.). San Francisco: University of California–San Francisco Nursing Press; and Leifer, G., & Hartston, H. (2004). Growth and development across the lifespan: A health promotion focus. Philadelphia: Saunders.
The Homeless Family: The homeless family with children is a modern-day problem that has an impact on the growth, development, and health of the child. Support systems and financial resources are often lacking, and the school nurse or emergency department nurse may be the first to identify the status of this family. Community referrals to provide shelter, food, education, and financial aid are primary needs that must be met before health teaching can be effective.
It is imperative that nurses take advantage of the strengths of the family while attending to its weaknesses. Nurses are in an excellent position to help the health profession move toward truly contemporary models of family-centered care. The nuclear family of the past is no longer dominant. Pediatric nursing research and care must reflect this phenomenon.
Personality Development
Most people tend to equate personality with social attractiveness: “She has a lot of personality, and he has no personality”; or “There’s an example of personality plus.” The term personality is more broadly defined by psychologists. One definition states that personality is a “unique organization of characteristics that determine the individual’s typical or recurrent pattern of behavior.” No two persons are exactly alike. An individual’s personality is the result of interaction between biological and environmental heritages.
Although no one group of theories can explain all human behavior, each can make a useful contribution to it. Many experts have devoted their lives to understanding why children and families behave as they do. Some experts, called systems theorists, believe that everyone in the family or system is affected by each of its members. This theory focuses on the interrelatedness of the various persons as opposed to an analysis of an individual in the group. Nurses using systems theory focus on caring for the child by caring for the whole family. They see the family as protector, educator, resource, and health provider for the child. In turn, they see the child’s health as having an impact on each member of the family as a whole.
Many experts see human development through a composite lens of various theories. The hierarchy of needs developed by Abraham Maslow is depicted in Figure 15-4, and the developmental theories of Erik Erikson, Sigmund Freud, Lawrence Kohlberg, Harry Stack Sullivan, and Jean Piaget are presented in Table 15-3. Other theorists are briefly contrasted within appropriate chapters devoted to specific age-groups. Theories provide a framework for the practitioner; however, humans are not a gathering of isolated parts to be disassembled and reassembled according to some theoretical set of instructions, even when these parts must be examined for investigative purposes.
Table 15-3
Comparison of the Developmental Theories of Erikson, Freud, Kohlberg, Sullivan, and Piaget
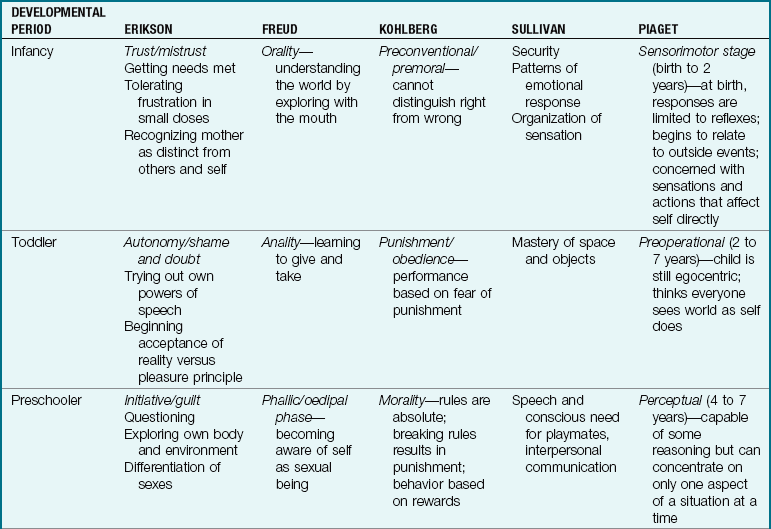
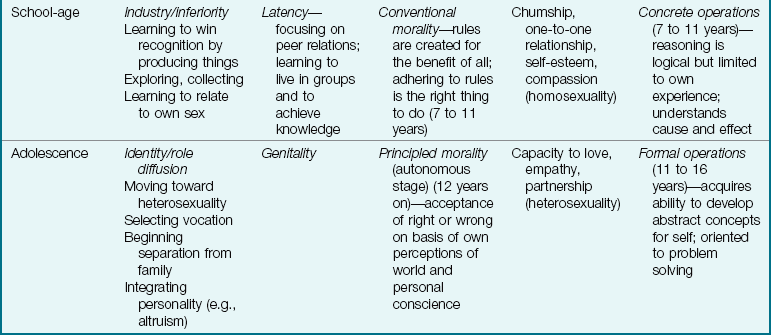
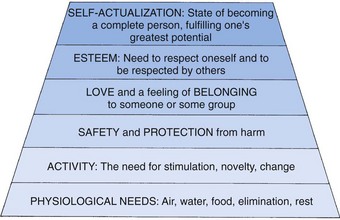
FIGURE 15-4 Maslow’s hierarchy of basic needs. The needs at the bottom of the pyramid must be met before one can fulfill needs at the next higher level.
Cognitive Development
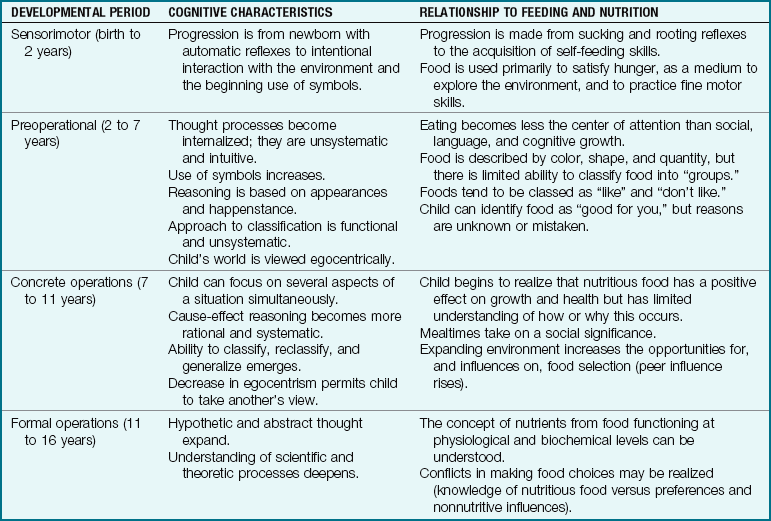
Cognition (cognoscere, “to know”) refers to intellectual ability. Children are born with inherited potential, but the potential must be developed. “It requires opportunities for exploration that are neither too easy nor too hard” (Levine et al., 2003). The development of logical thinking and conceptual understanding is a complex process. One outstanding authority on cognitive development was Piaget, a Swiss psychologist. He proposed that intellectual maturity is attained through four orderly and distinct stages of development, all of which are interrelated: sensorimotor (up to 2 years), preoperational (2 to 7 years), concrete operations (7 to 11 years), and formal operations (11 to 16 years). The ages for each stage are approximate, and each stage builds on the preceding one.
Piaget believed that intelligence consists of interaction and coping with the environment. Infants begin their interaction by reflex response. As they grow older, their use of symbolism (particularly language) increases. Gradually they acquire a here-and-now orientation (concrete operations) and finally a fully abstract comprehension of the world (formal operations). Table 15-4 relates Piaget’s theory to feeding and nutrition. It is a good example of how knowledge of development can help in understanding the behavior of a child at a particular time.
Moral Development
Lawrence Kohlberg, a childhood theorist, suggests that moral development in children is sequential. His theories on moral development are based on Piaget’s cognitive development investigations. He describes three levels: preconventional, conventional, and postconventional. Each level contains two stages. In the preconventional stage (4 to 7 years), children try to be obedient to their parents for fear of punishment. During the conventional phase (7 to 11 years), children show conformity and loyalty, and they focus on obeying rules. In the postconventional level (12 years and older), moral values are developed to solve complex problems. There is an emphasis on the conscience of the individual within the society. Although rules are still important, changing them to meet the needs of a culture is considered.
The Growth and Development of a Parent
Table 15-5 shows the tasks of the parent as they relate to the child’s developmental tasks in Erikson’s system of stages, as well as some suggestions for nursing interventions that can aid the growth and development of a parent and a child.
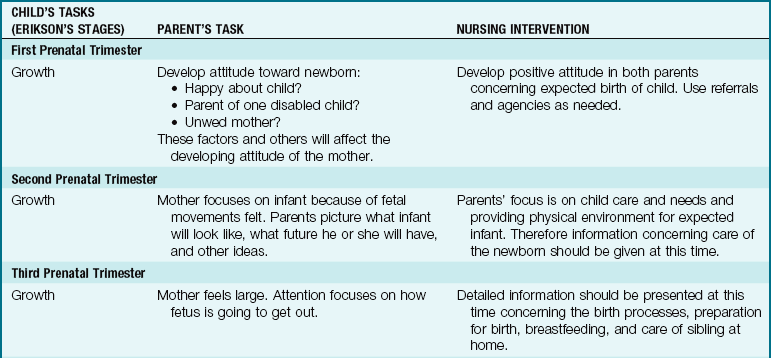
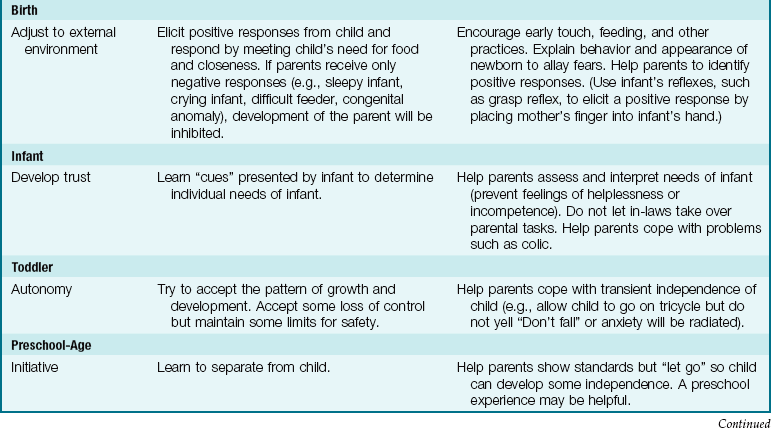
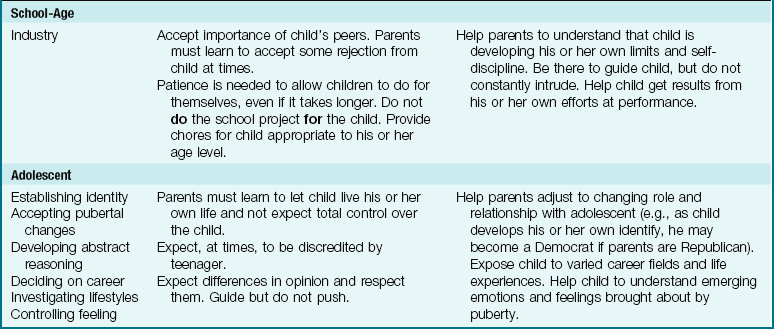
Erikson’s stages of child development demonstrate the various tasks that must be mastered at each age to achieve optimum maturity. Each stage builds on the successful completion of the previous stage. Achievement of the tasks of childhood do not occur in isolation. Parents must interact appropriately to assist the child to achieve successfully at his or her developmental level (Figure 15-5). For example, if the parent constructs a school project for a child, the child will not achieve a sense of industry. If the parent does not accept a positive attitude toward the pregnancy and unsuccessfully attempts to abort, the parent may become overly protective or abusive to the newborn infant, and bonding will not occur.

FIGURE 15-5 Infant carriers enable face-to-face interaction between young infant and parent. An older infant can be turned in the carrier to face outward and interact with the environment.
Parents should be guided not to attempt to prevent frustration in the lives of their children. Experiences in dealing with challenges and disappointments prepare the child to function independently in adulthood. Parents should encourage a child to deal with successes and failures, provide socially acceptable outlets, and intervene only if the frustrations become overwhelming. The parent’s task is to provide the child with the skills and tools appropriate at each age level to deal with events. Many websites provide tips concerning parenting skills.
Nutrition
Good nutrition begins before conception. Nutritional needs during pregnancy are discussed in Chapter 4. The dependent child is fed for many years by adults whose eating habits may be based on misinformation, income level, folklore, fads, or religious, cultural, and ethnic preferences. Table 15-6 describes some common food patterns of various cultures found in the United States. Many families are poor, others have inadequate knowledge of how to prepare foods, and many rely on convenience foods to save time.
Table 15-6
Culturally Diverse Food Patterns of Americans
| CULTURE | HISTORICAL DIETARY PATTERN* |
| African American | All meats, fish, and chicken; pork is often consumed (spareribs, bacon, and sausage). Vegetables are cooked in salt pork for long periods of time; grits and cornbread muffins. There is some lactose intolerance. Popular vegetables include collard greens, beet greens, and sweet potatoes. |
| Chinese American | Rich in vegetables (bean sprouts, broccoli, bamboo shoots, and mushrooms). Vegetables are cooked until crisp; meat is consumed in small portions with other food. Soy sauce, tofu, peanut butter; limited milk and cheese; fish baked with native spices; soups with egg, meat, and vegetables. Tea is China’s national beverage. Rice is staple of diet. |
| Jewish American | Diet varies according to whether family is Orthodox, Conservative, or Reform. For an Orthodox family, food must be kosher (must conform to dietary laws); meat is soaked in salt water to remove blood; only meat eaten is that of divided-hoofed animals that chew a cud; fish without scales (shellfish) and pork are prohibited; milk and meat cannot be combined. Favorites are gefilte fish, lox (smoked salmon), herring, eggs, bagels, cream cheese, and matzo. |
| Laotian American | Numerous varieties of freshwater fish and shellfish (eaten fresh, dried, or salted); pork, beef, chicken, and rabbit, often mixed with vegetables and spices; eggs, peanuts, black-eyed peas; vegetables eaten raw, as juice, or cooked with meat or fish and preserved by drying or pickling; sticky rice, rice or bean thread noodles, and legumes often used in desserts; soybean drink, sugar cane drink, tea, and coconut juice. Popular seasonings include padek, chilies, curry, tamarind, and red and black pepper. |
| Italian American | All meats, fish, and chicken, including cold cuts (salami, mortadella) and Italian pork sausage; pasta (staple of diet), breads, olive oil, wine, cheese, and all varieties of fruits and vegetables. |
| Japanese American | Fish and seafood (fresh, smoked, and raw) and beef. Food is cut into small portions. Principal fruit is nasi, which tastes much like a pear. Many vegetables are eaten, such as seaweed, bamboo shoots, onions, beans, and dried mushrooms (shitake); enjoy pickled vegetables. Rice is national staple. Beverages include tea and sake. Little cheese, milk, butter, or cream is consumed. Chief cooking fat is soybean oil or rice oil. |
| Mexican American | Chicken, pork chops, wieners, cold cuts, hamburger, eggs (used frequently), beans (eaten mashed or refried with lard), potatoes (basic item, usually fried), chilies, fresh tomatoes, corn (maize—often used as basic grain), tortillas, packaged cereals; little milk because of lactose intolerance. |
| Native American | Acorn flour, a staple food made into mush or bread; salmon, fresh or dried; other varieties of fish, deer, duck, geese, and other small game; nuts such as buckeye and hazel; wild berries, seeds, and roots. |
| Puerto Rican American | Meat cooked in stews; poultry, pork, fish, dried beans or peas mixed with rice; milk in combination with coffee (cafe con leche), variety of fruits, starchy vegetables (plantains, cassava, sweet potatoes), salad, soft drinks. |
| Vietnamese American | Pork—most common meat; meats cut into small pieces and fried, boiled, or steamed; fish—all types of freshwater and saltwater fish and shellfish, often fried and dipped in fish sauce; eggs, soybeans, legumes, and wide variety of fruits and vegetables; rice often eaten with every meal; seasonings including oyster sauce, soy sauce, monosodium glutamate, ginger, garlic, nuoc mam sauce; tea, coffee, soft drinks, soybean milk. |
*More diverse eating patterns occur as future generations of a culture become assimilated.
Data from Mahan, L.K., & Escott-Stump, S. (2008). Krause’s food, nutrition and diet therapy (12th ed.). Philadelphia: Saunders; Wetter, A.C., Goldberg, J.P., King, A.C., Sigman-Grant, M., Baer, R., Crayton, E., et al. (2001). How and why do individuals make food and activity choices? Nutrition Reviews, 59(3), 11-21; and Booth, S., Sallis, J., Ritenbaugh, C., Hill, J., Birch, L., Frank, L., et al. (2001). Environmental and societal factors affect food choice and physical activity: Rationale, influences, and leverage points. Nutrition Reviews, 59(2), S21-S39.
Some families do not consider food a priority in the home. However, optimum nutrition is essential for the child to reach his or her growth potential. A lack of adequate nutrition can lead to mental retardation. The obese child may be subject to decreases in motor skills and peer rejection, leading to low self-esteem.
The nurse is in a position to identify children at risk and to help families modify eating habits to ensure proper nutrition. An important resource for the nurse is the nutritionist in the community or on the staff of the health agency where the nurse is employed. Formula feeding and breastfeeding are discussed in Chapter 9 and Chapter 16.
Family Nutrition
The U.S. Department of Agriculture (USDA), in a joint effort with the U.S. Department of Health and Human Services (USDHHS), offers dietary guidelines for Americans; these were updated in 2005. Good nutrition is vital to good health and essential for normal growth and development. A healthy, balanced, nutrient-dense diet, combined with adequate physical activity, is the core of the new dietary guidelines. The 2005 Dietary Guidelines can be designed to meet the individual needs of the consumer. Personalized, portion-sized diet plans that include advice on activity level can be found online, along with additional recommendations for specific populations.
Examples of culturally diverse food pyramids can be found in Chapter 4. The dietary guidelines are intended to help Americans make informed decisions about what they eat. Families who practice such principles are educating their children by good example. Figure 15-6 shows a suggested food pyramid for children 2 to 6 years of age. Many families are vegetarian, and the use of teaching tools that respect the dietary limitations will encourage compliance. Figure 15-7 demonstrates a modification of the food pyramid for vegetarians. This food pyramid is directed toward vegetarian families and applies to children as young as age 2 years. The nurse should assess restricted foods in the vegetarian diet and ensure that the diet is adequate in protein, vitamins, and minerals to promote growth and development in children. Children on vegetarian diets often consume large amounts of high-fiber foods.
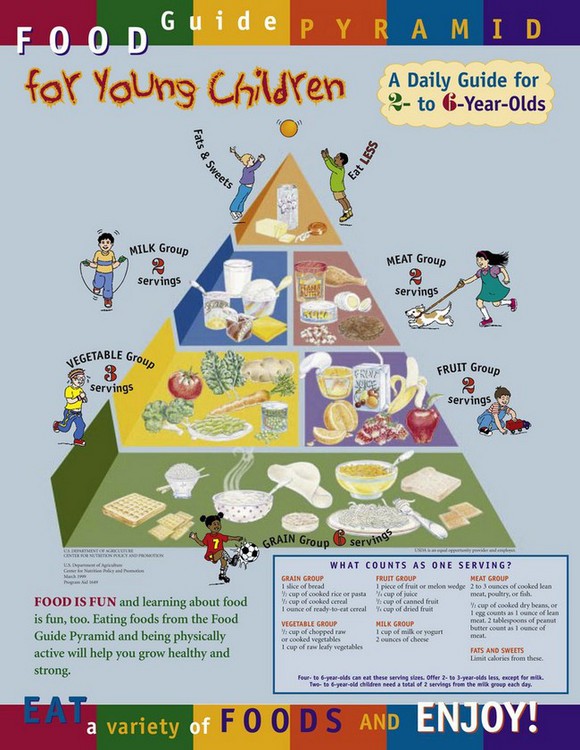
FIGURE 15-6 The Food Guide Pyramid for Young Children. This food pyramid can be used to teach children about a balanced diet that will promote growth and development.
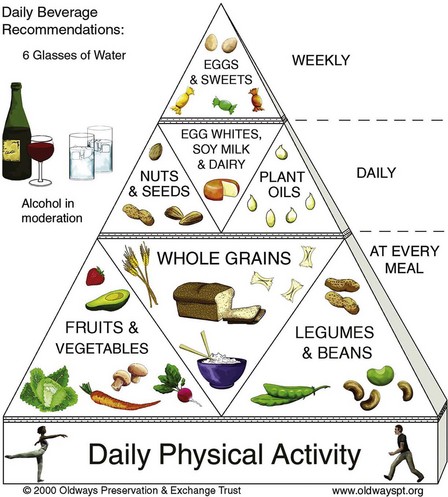
FIGURE 15-7 The Vegetarian Diet Pyramid. The vegetarian diet pyramid is a modification, designed for vegetarians, of the U.S. Department of Agriculture (USDA) food pyramid. Using food guidelines that respect dietary limitations or restrictions may increase compliance when teaching parents and children concerning a balanced diet that promotes optimum health.
High-fiber foods cause increased losses of calcium, zinc, magnesium, and iron in the stool and may necessitate the intake of supplements. A diet containing meat, poultry, or fortified foods lessens this nutrient deficiency (see Nutrition Considerations box).
 Nutrition Considerations
Nutrition Considerations
Fiber Needs of the Young Child
The American Academy of Pediatrics recommends intake of 0.5 g of fiber per kilogram of body weight in childhood, gradually increasing to adult levels of 20 to 35 g/day by the end of adolescence. High-fiber foods can fill the small stomach capacity and provide few of the nutrients and calories needed by the active, growing child.
Different types of fiber are contained in foods (Table 15-7). The water-soluble fiber found in oats, apples, and citrus fruits delays intestinal transit and decreases serum cholesterol levels. The water-insoluble fiber found in whole-grain breads, wheat bran, and some cereals accelerates intestinal transit and slows starch digestion.
Table 15-7
High-Fiber Foods for Relief of Mild Constipation in Children Over 12 Months of Age
*All products indicated are registered trademarks of their respective companies.
Modified from Baker, S. (1994). Introduce fruits, vegetables, and grains but do not overdo high-fiber foods. Pediatric Basics, 69(Summer), 2-4.
A well-balanced diet supplies all essential nutrients in the necessary amounts. Food provides heat and energy, builds and repairs tissues, and regulates body processes. A given food is a mixture of elements such as minerals (e.g., calcium, phosphorus, sodium, iron), compounds (carbohydrates, fats, proteins, some vitamins), and water. The body needs approximately 50 nutrients, which it absorbs at various sites (Figure 15-8). See the table on USDA Dietary Guidelines for Americans on the Evolve website.
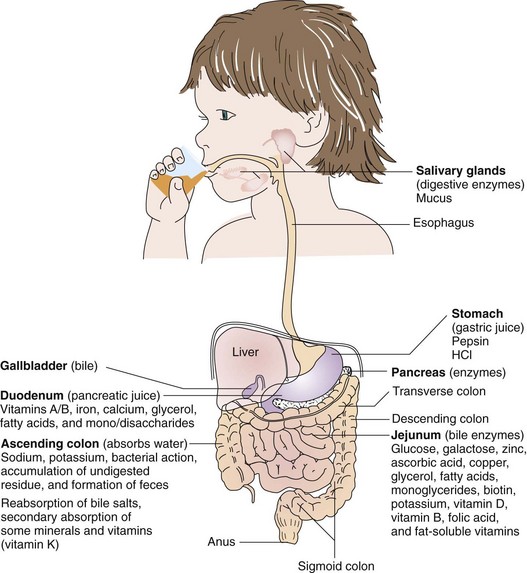
FIGURE 15-8 Nutrient digestion. The sites of absorption of major nutrients are shown in this illustration. Most nutrient absorption occurs in the duodenum and jejunum of the small intestine. Most water absorption occurs in the large intestine. Absorption of nutrients depends on adequate secretion of digestive enzymes, normal motility, and normal villi on the mucosal surface of the intestines. Portal circulation, lymphatic circulation, and hormones also play a role in the digestion and absorption of nutrients.
Nutrition Considerations
Enhancing Absorption of Minerals
Foods containing essential minerals such as iron, zinc, and calcium should be combined with citrus, fish, or poultry to enhance absorption of the minerals. Vitamin D and lactose sugars also enhance mineral absorption in the body.
Children are susceptible to nutritional deficiencies because they are growing and developing. Infants require more calories, protein, minerals, and vitamins in proportion to their weight than do adults. Fluid requirements are also higher for infants. Eating a variety of foods selected from the basic food groups ensures good health for children. The amount and size of portions are important in maintaining a reasonable weight. There are no known advantages to consuming excessive amounts of any nutrients, and there are risks for overdoses.
Nutritional Care Plan
The nutritional care plan can be used in the hospital, home, or outpatient department. Parts of the care plan may already have been collected by other professionals, and the nurse should refer to the patient’s chart for pertinent data. The nutritional care plan provides information and stores it in one place. It can also be put on a computer for easy retrieval.
Nutrition and Health
The digestive system of the newborn is immature and functions minimally during the first 3 months. Saliva is minimal; hydrochloric acid and rennin in the stomach and trypsin in the intestines aid in the digestion of milk. Amylase (a pancreatic enzyme) and lipase are not present in adequate quantity before age 4 months, and therefore complex carbohydrates and fats cannot be digested effectively. Excess fiber intake in the young infant results in loose, bulky stools. The ability of the liver to function is limited in the first year of life. The teeth are not present for chewing before 6 to 8 months of age.
 Safety Alert!
Safety Alert!
Raw fruits that contain seeds or some raw vegetables and nuts may not be appropriate foods for infants and young children because of the risk of choking. Beans and vegetables should be well cooked.
The physiology of digestion is the basis for food introduction in the first year of life. Breast milk or iron-fortified formula is the food of choice for the first 6 months to 1 year of life. Introducing baby food before age 5 to 6 months does not serve any nutritional purpose. Overnutrition and its link to obesity in adults have been explored. The effects of childhood nutrition on adult health and illness patterns, such as heart disease, have been established. Home preparation of food for infants is discussed in Chapter 16.
Nutrition and Health Promotion
Therapeutic diets, such as the diabetic diet, are well established in medical care. Some foods can promote dental caries, and others contain protective fibers that are known to prevent some diseases. Atherosclerosis can be prevented by starting healthy dietary patterns in childhood. However, restrictive diets are not advised for infants and young children. Fat and cholesterol are needed for calories and the development of the central nervous system. The sodium content of baby foods has been decreased because the average diet contains adequate sodium. Some food additives, such as aspartame (an artificial sweetener), may be harmful to children with phenylketonuria. Food additives that prolong the shelf life of foods and food dyes that make food look more attractive should be minimized in the child’s diet. Fast-food chains, often depended on by working parents and preferred by adolescents, make available to the consumer the nutrient content of the foods they serve. The caloric content of the menu often depends on the foods selected and the toppings added. Therefore a “salad bar” is not necessarily synonymous with a low-calorie meal.
Height and weight should be plotted on a growth chart at each clinic visit to enable early identification of health problems related to dietary intake. The weight or triceps skinfold thickness greater than the 75th percentile or below the 3rd percentile indicates a need for further evaluation. The role of the grandparents in providing a diet that may lead to obesity must often be addressed, because the principles of good nutrition that were adhered to 20 or 30 years ago may no longer be valid. Concern is expressed over the level of cholesterol in children. Methods to reduce cholesterol in families are listed in the Health Promotion box below, and the National Cholesterol Education Program’s recommendations are cited in Box 15-4.
 Health Promotion
Health Promotion
Methods to Reduce Cholesterol in School-Age Children
• Exercise more with your children.
• Provide fresh fruits and vegetables rather than empty calories such as those found in doughnuts and store-bought pastries.
• Decrease trips to fast-food restaurants.
• Switch to low-fat foods; use vegetable oil cooking sprays in place of butter; bake or broil foods instead of frying them.
• Seek the advice of a nutritionist.
• If there is a family history of heart disease, have the child’s as well as your levels of cholesterol tested.
Dietary supplements, formulas, and nutritional support techniques for preterm infants, children with cancer, and those with long-term disorders (e.g., cystic fibrosis) have become sophisticated and are used successfully. Total parenteral nutrition allows the physician to choose preparations ranging from amino acids and intravenous fats to complete multivitamins. Total parenteral nutrition and enteral feedings allow children who need nutritional support to be cared for at home, thus greatly enhancing the quality of life.
In the 1990s an oral rehydration solution (ORS) used by third-world populations for treating acute diarrhea in children gained acceptance and is now produced and distributed by the World Health Organization. It is composed mainly of electrolytes, glucose, and water. Health care workers are able to teach parents how to save the lives of their infants by using this simple solution. Medicine women, the respected leaders of some tribes, are being incorporated into the educational process. One example of a commercial preparation available in the United States is Pedialyte. See Chapter 28 for detailed discussion of oral rehydrating solutions.
Feeding the Healthy Child
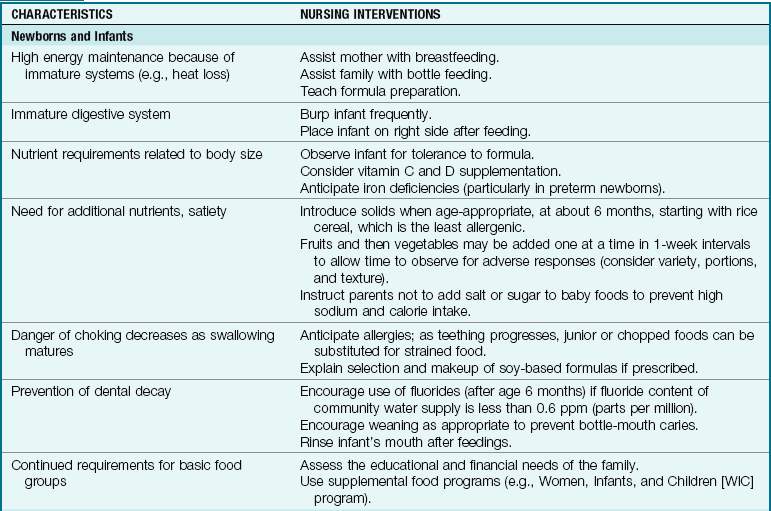
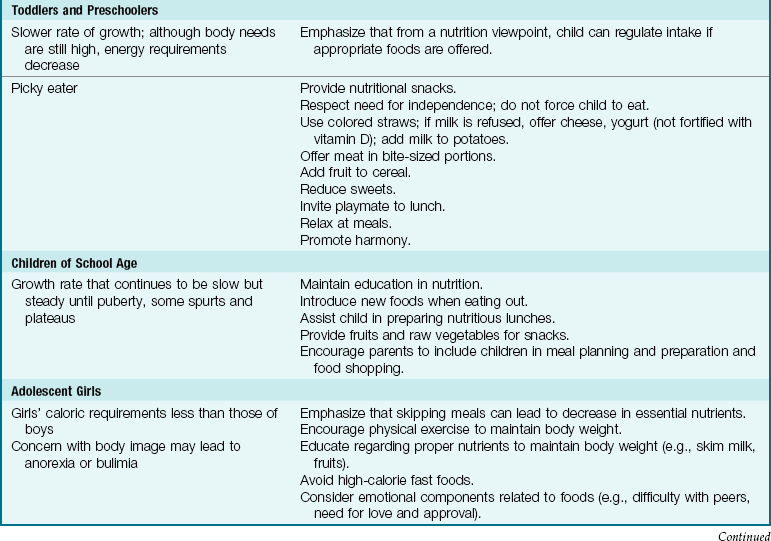
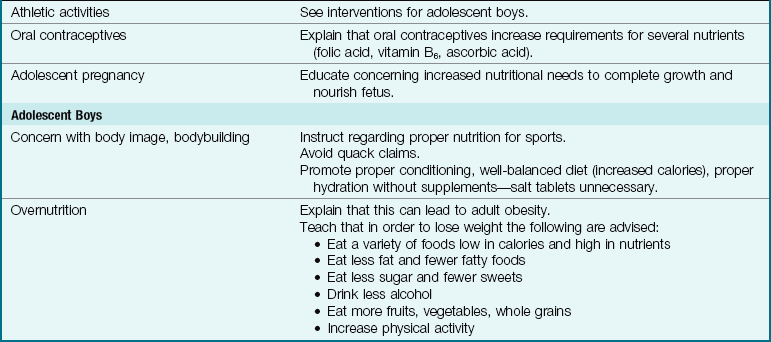
Table 15-8 specifies the nursing interventions that help to meet the nutritional needs of children from infancy to adolescence.
The Infant
Infants require more calories, protein, minerals, and vitamins in proportion to their weight than do adults. Their fluid requirements are also high. Breast milk is excellent in all these regards, and a nursing mother may continue this even when her infant is hospitalized. The nurse stresses that the mother should avoid fatigue, because it affects milk production. Breast milk can be manually expressed and refrigerated at the hospital and then given in the mother’s absence.
Some infants cannot tolerate milk because of intestinal bleeding, allergy, or other negative reactions. Many milk substitutes are available for therapeutic use. Among these are soybean mixtures (such as ProSobee and Isomil) for infants with milk-protein sensitivity. Most products come in dry and liquid forms, and parents must be made aware of what concentrations the physician recommends. Rice cereal is the first solid food introduced at age 6 months (Figure 15-9).
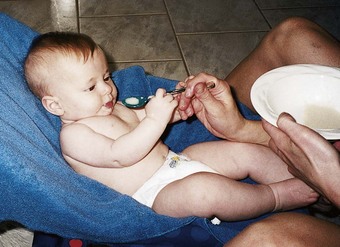
FIGURE 15-9 Spoon feeding. Solid foods should be introduced at age 6 months and fed by spoon to the infant. Cereal should not be mixed into the formula bottle when feeding the healthy infant.
The nurse must be aware of the problems of underfeeding and overfeeding infants. Underfeeding is suggested by restlessness, crying, and failure to gain weight. Overfeeding is manifested by symptoms such as regurgitation, mild diarrhea, and too rapid a weight gain. Diets high in fat delay gastric emptying and cause abdominal distention. Diets too high in carbohydrates may cause distention, flatus, and excessive weight gain. Constipation may be the result of too much fat or protein or a deficiency in bulk. Increased amounts of cereals, vegetables, and fruits can often correct this problem.
If the parents plan to prepare their own baby food at home, the nurse should discuss the choice of foods, their preparation, and safe storage. Blenders, strainers, and mashers are equipment often used, and ice cube trays may be used to freeze portions for storage. Spinach, broccoli, and beets should not be pureed at home because of their nitrite content, which can cause methemoglobinemia in young infants (Akers & Groh-Wargo, 2005) but most fresh and frozen unsalted foods are appropriate. Water or juice used in cooking can also be used to thin blended food, but overblending should be avoided since it can cause over oxidation of nutrients (Akers & Groh-Wargo, 2005). Prepared foods can be stored in the refrigerator for 48 hours or frozen for several months. Home-prepared foods are less expensive, contain less salt and sugar, and help the infant become familiar with the cultural tastes of the family.
Most infants naturally adapt to a schedule of three meals a day by the first birthday. At this time the appetite fluctuates as the growth rate slows somewhat. The child may not be interested in eating. Spills are frequent. At age 1 year, children cannot manipulate a spoon, but hand-to-mouth coordination is good enough that they enjoy holding a piece of toast while the nurse assists. In the hospital, children in highchairs are secured with safety belts. The nurse remains in constant attendance. Developmental advancements that change eating patterns are explained to parents to prevent feeding difficulties.
The Toddler
Toddlers can feed themselves by the end of the second year (Figure 15-10). This is important in developing a sense of independence. The toddler may be rebellious at times, and food may be pushed away or completely refused. Toddlers benefit from the caregivers’ presence at mealtime. Feeding difficulties may result from the anxieties of parents and a lack of time planned for meals.

The Preschool Child
Preschoolers and toddlers like finger foods. Dawdling and regression are common in this age-group. In general, preschoolers are more vulnerable to protein-calorie deficiencies; their younger siblings receive priority at home, and older brothers and sisters may receive the benefits of school lunch programs.
The School-Age Child
School-age children need food from the basic food groups but in increased quantities to meet energy requirements. Their attitudes toward food are unpredictable. Intake of protein, calcium, vitamin A, and ascorbic acid tends to be low. The intake of sweets decreases the appetite and provides empty calories.
The Adolescent
Nutrition is particularly important during the adolescent years. Teenagers grow rapidly and expend large amounts of energy. Their food needs are great. The nurse attempts to involve the teenager in selecting foods that are nutritious and appetizing. This may be done by reviewing choices made on the daily menu. Sometimes it helps to stress how important good nutrition is to physical appearance and fitness. The need for peer approval is at its height during adolescence, and food fads and skipped meals may result in malnutrition, even in families of means. Fatigue is a common complaint at this age. If it is accompanied by a lack of appetite and irritability, anemia should be suspected. Some adolescents consult computer chat rooms for weight loss information, and this can lead to anorexic behavior. Parental guidance of computer use is necessary. The Health Promotion box on nutrition resources in the community lists nutrition services in the community available to children.
Childhood Obesity
Approximately one third of all children in the United States are overweight, with about 30% to 40% considered obese (Snow & Van Hemel, 2008). Excessive weight in childhood is related to obesity in adulthood. Obesity can cause health problems such as increased cholesterol, orthopedic problems, sleep apnea, high blood pressure, type 2 diabetes mellitus, and devastating social isolation that can lead to depression. The instrument to determine obesity is the body mass index (BMI) percentile (Skill 15-2).
Skill 15-2 Calculating Body Mass Index (BMI)
To estimate a healthy body weight for an individual based on height and indirectly measure body fat percentage to determine obesity or underweight status
A child over 2 years of age should be weighed and measured at every health checkup to determine growth and nutritional status. Any deviation from the trend that is plotted on the growth chart may indicate a developing health problem. The following formulas can be used to obtain a BMI:
Note: Assistance in using formulas to obtain the BMI is available at www.cdc.gov/healthyweight/assessing/bmi/index.html. This site will calculate the BMI for individual data supplied. The nurse has the responsibility for measuring the growth of a child and understanding growth charts.
A BMI over 18 in children aged 5 to 9 years, or over 22 to 24 for 13- to 17-year-olds, evidences an overweight status (Bartlett et al., 2005). The cause of obesity is most often related to diet and inactivity, although some causes can include illness syndromes. Monitoring, counseling, and follow-up are essential.
Parents and school-age children need guidance concerning appropriate portions of foods to have at each meal. Supersized portions are advertised on TV in a positive way and are difficult to resist at the fast food restaurant or the store. Healthy food choices and appropriate portion sizes are an important part of weight control. One type of assistance available to parents and children is the Portion Plate for kids, a two-sided reusable placemat that compares the appropriate portion size for school-age children with common objects such as a deck of cards or a baseball (Figure 15-11). The reverse side of the placemat offers tips on selection of healthy foods and refers the parent and child to myPyramid.gov for individual guidance.
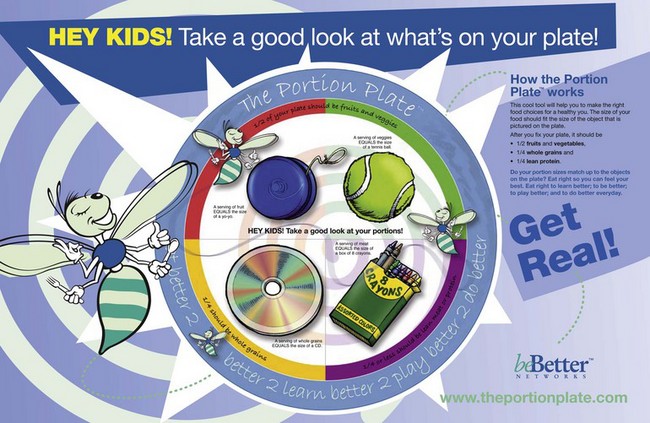
FIGURE 15-11 The Portion Plate for Kids is an educational placemat that can be used to guide portion amounts in terms children can understand, such as making the serving portion of vegetables in one meal about the size of a baseball. The reverse side of the mat offers tips on food selection. Preventing the supersizing of portions is an important step in preventing obesity.
Feeding the Ill Child
Children in the hospital continue in the process of growing. Well-nourished children can be characterized as follows:
• Nearly always show steady gains in weight and height
• Have no fatigue circles beneath the eyes
• Have a skin color within normal limits
• Have mouth and gum mucous membranes that are firm and pink, not swollen or bleeding
• Have no mouth or tongue lesions
• Have teeth that are erupting on schedule
• Have a generally good appetite and eliminate regularly
• Sleep well at night, have energy and vitality, and are not irritable
This picture changes somewhat during illness, but the child who is basically well nourished can easily be distinguished from one who is malnourished.
Many hospitalized children have poor appetites. This may be due to age, the nature of the illness, the type of diet, sudden exposure to strange foods and a strange environment, a reaction to hospitalization, or the degree of satisfaction obtained during mealtimes. The child may also refuse to eat in an attempt to manipulate the parents, particularly if lack of appetite was a concern in the past.
The nurse observes the patient’s tray to determine if the food is of the right consistency. Does the child have any teeth? Do lesions in the mouth prevent chewing? Can the child use a knife and fork? Children with bandaged limbs or those receiving intravenous fluids require assistance. The size of servings is important.
One should serve less than one hopes will be eaten. A tablespoonful of food (not heaping) for each year of age is a good guide to follow. More is given if the patient appears hungry. One item at a time is placed before small children who feed themselves, so they do not become overwhelmed. The nurse avoids showing personal dislikes because negative attitudes are easily transmitted. The nurse proceeds slowly with unfamiliar children to determine their level of mastery. Food is served warm, and sufficient time is allotted. Sweet drinks and snacks should not be served just before meals. Treatments such as chest physiotherapy should not be scheduled immediately after a meal.
Infants who are placed on “nothing by mouth” (NPO) status should be provided with a pacifier to meet their sucking needs. Some children prefer to use their thumb for nonnutritive sucking (Figure 15-12).
FIGURE 15-12 Nonnutritive sucking. Nonnutritive sucking involving the finger or a pacifier is common in infants under age 1 year and fulfills the needs of the oral phase of development. In general, malocclusion from nonnutritive sucking will not be a problem if the habit is discontinued by age 3 years. Frequency, duration, and intensity of sucking influence the occurrence of malocclusion associated with finger or pacifier use. Behavior modification can help to decrease thumb sucking (e.g., a dental appliance or substances placed on the finger). The child must be physically and emotionally “ready” to discontinue thumb sucking, and appropriate rewards should be predetermined.
Food-Drug Interactions
Whenever a child is ill and treated with prescription medications, the nurse is responsible for monitoring drug-drug interactions, drug-food interactions, and drug-environment interactions. Monitoring drug-drug interactions involves knowledge of the side effects of each drug prescribed. Drug-environment interactions involve the effects of a drug on the response of the patient to his or her environment. For example, certain antibiotics have photosensitivity as a side effect. Nurses armed with this knowledge advise the patient or parent to avoid prolonged exposure to sunlight. Drug-food interactions are often overlooked but can have an impact on treatment and/or the growth and development of the child. The nurse should remain alert to food-drug interactions while dealing with the sick child.
The Teeth
The development of the 20 deciduous, or baby, teeth begins at about the fifth month of intrauterine life. The health and diet of the expectant mother affect their soundness. Primary teeth erupt during the first 2.5 years of life. It is a normal process and is generally accompanied by little or no discomfort. Wide individual differences in tooth eruption occur in normal, healthy infants. Occasionally an infant is born with teeth; neonatal teeth are removed to prevent the possibility of choking should they fall out. A delay in teething is significant if other forms of immaturity or illness are present. The physician evaluates the process of teething during the infant’s regular health checkups.
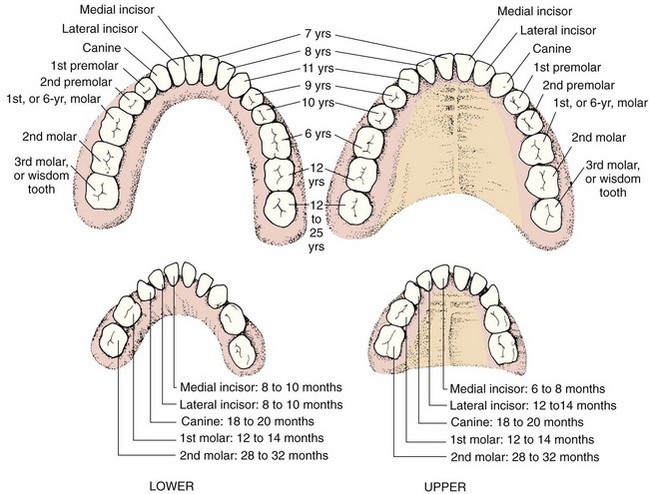
The first tooth generally appears at about the sixth or seventh month. The 1-year-old has about six teeth, four above and two below. The order in which the teeth appear is almost always the same (Figure 15-13). They are shed in about the same order in which they appear (i.e., lower central incisors first, and so forth). Although the Academy of Pediatric Dentistry recommends that the first dental visit occur by 1 year, the majority of children begin seeing a dentist between ages 2 and 3 years. Tetracycline antibiotics stain developing teeth a yellowish brown and therefore are to be avoided during pregnancy and in the first 8 years of life.
Parents and nurses must not neglect baby teeth, thinking that they will eventually be lost. A 2-year-old who wants to brush his teeth when Mommy does is encouraged to do so. The deciduous teeth serve not only in the digestive process but also in the development of the jaw. When the deciduous teeth are lost early because of neglect, the permanent teeth become poorly aligned. The nurse checks that all patients ages 1 year and older have toothbrushes. Children sometimes must be reminded of oral hygiene at bedtime. Parental supervision of toothbrushing is necessary until age 7 years.
Permanent Teeth
The 32 permanent teeth develop just before birth and during the first year of life. They do not erupt through the gums, however, until the sixth year. Nutrition and general health during the first year of life affect the formation of permanent teeth. This process is not completed until the wisdom teeth appear at about age 18 to 25 years. The first permanent teeth do not replace any of the deciduous teeth but appear behind the deciduous molars. Cavities in them are often neglected because they are mistaken for baby teeth. The most common site of decay in children is the fissures of the molar teeth. These areas can be protected by the professional application of plastic sealants.
Oral Care in Health and Illness
Good dental care begins with a proper diet that supplies adequate nutrients while the teeth are developing in the jaws, especially during the prenatal period and the first year. The many essential elements found in milk include calcium, phosphorus, vitamins A and B complex, and protein. Vitamin D (the “sunshine vitamin”) and vitamin C (found in citrus fruits) are also valuable. Dietary practices influence the development of cavities, and parents are encouraged to limit the frequency of fermentable carbohydrate intake.
Health Promotion
Developmental Dental Hygiene
Infant’s gums are wiped daily after 2 months of age with a moist cloth or xylitol wipe.
Gentle brushing is performed each night with a soft, small toothbrush.
Use of anticaries fluoride toothpaste (amount equivalent to a grain of rice) is begun between 1 and 2 years of age.
Child is not put to bed with bottle of milk or juices. If infant must have a bottle, water is used.
Deciduous teeth erupt, and baby teeth start to exfoliate (fall out) toward the end of this period.
Parents assist children and remind them to brush and floss until at least age 8 years. A small, soft toothbrush is used.
Bedtime routine of brushing is established, since salivary flow rates slow during sleep, reducing natural protective mechanisms.
Parents are advised to brush for the child at least once a day and to clean teeth that are in contact with each other with dental floss.
Sweets are limited to daytime meals, when saliva content is high.
First permanent molars appear. The pits and fissures of molars make them the primary site for caries. Sealants (plastic coating) professionally applied to molars provide a mechanical barrier against bacteria.
Parents continue with fluorides and flossing, and reducing frequency of exposure to fermentable carbohydrates. Adolescent gingivitis (gingiv, “gum,” and itis, “inflammation of”), characterized by redness, swelling, and bleeding, is common in children and adolescents and may be aggravated by hormonal changes at puberty.
Motivating the adolescent to assume responsibility for dental care may be complicated by rebellion against authority and some incapacity to appreciate long-term consequences.
Topical fluorides and fluoride toothpastes are available.
Orthodontic treatments place adolescent at high risk for gingivitis and caries around appliances or braces.
Mouth protectors should be used to prevent dental injuries from contact sports.
Data from Griffen, A. (2000). Pediatric oral health. Pediatric Clinics of North America 47(5), 975-1000. Philadelphia: Saunders. Galganny-Almeida, A., & Queiroz, M. (2007). The effectiveness of a novel infant tooth wipe in high caries-risk babies 8 to 15 months old. Pediatric Dentistry, 29(4), 337-42.
In the past, total carbohydrate consumption was thought to be the most important dietary consideration for dental health. Today more attention is given to the frequency with which sweets are eaten and how long they stick to the teeth. Sticky foods have more potential to cause caries (cavities) than do sugared drinks that are quickly cleared from the mouth. Oral care after eating sticky foods is recommended. Recommended snack foods include cheese, peanuts, milk, sugarless gum, and raw vegetables. Items to be avoided include sugared gum, dried fruits, sugared soft drinks, cakes, and candy.
Of most importance in preventing caries is the administration of fluoride by mouth after age 6 months. Ideally, fluorides are present naturally in the water supply or are added to it. The fluoride content of city water or prepared formula may decrease the need for fluoride supplements. When necessary, systemic fluorides can be offered until the last permanent tooth erupts at about age 13 years. Many fluoride preparations are available and are often incorporated with vitamins. These tablets are obtained by prescription and should not be interchanged among children of various ages, because too much fluoride may cause the teeth to become “mottled” (fluorosis). Fluoride may also be applied directly to the teeth by the dentist.
Another aspect of tooth care is the prevention of bottle-mouth caries (nursing caries) (Figure 15-14). This condition occurs when an infant falls asleep while breastfeeding or is put to bed with a bottle of milk or sweetened juice. Sugar pools within the oral cavity, causing severe decay. It is seen most often in children between 18 months and 3 years of age. Eliminating the bedtime bottle or substituting water is recommended. Bottles and sippy cups, if used, should only contain water, except at mealtimes. “Read, don’t feed, at bedtime” should be the teaching motto (Hofman, 2008). Early childhood caries is defined by the American Academy of Pediatric Dentistry as one or more decayed or filled tooth surface in any primary tooth in a child under 6 years of age (Wagner & Oskouians, 2008). Severe childhood caries is defined as smooth surface caries in a child younger than 3-years of age. According to the USDHHS, severe childhood caries are more prevalent than obesity or asthma in children (USDHHS, 2008). Signs of early decay include chalky white spots on tooth enamel near the gum line of maxillary incisors. Brown discoloration signals more advanced decay. Tooth decay can cause dental abscesses, which can result in brain infections.
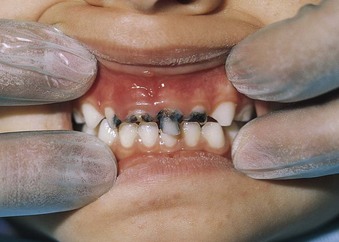
FIGURE 15-14 Nursing caries. During sleep, saliva production decreases and the teeth become more vulnerable to decay. When the infant is put to sleep with a bottle containing milk or sweetened juice, the sugar combines with the bacterial flora in the mouth to cause tooth decay. This is known as “milk caries.” Parents should be taught to use unsweetened water as the only liquid in a bottle at bedtime.
The maintenance of good oral health is an integral portion of comprehensive care for a sick or disabled pediatric patient. Education, prevention, and referral in the home, school, or hospital setting must be part of the child’s plan of care. Untreated dental caries or malposition of the erupting teeth can cause periodontal disease in later years if not treated promptly. Delayed or early eruption of teeth can be indicative of certain endocrine disorders or other pathological conditions and should be recorded and reported. Parents and caregivers should avoid “tasting” baby food fed to infants and young children, because the transmission of acid-producing bacteria from their mouths can be passed on to the food or feeding utensils and contribute to tooth decay in the infant. The use of xylitol chewing gum by the parent can reduce cross-contamination of mouth bacteria with the infant (Galganny-Almeida & Queiroz, 2007). Regular toothbrushing can start with tooth eruption. Children should brush before bedtime because the protective bacteriocidal effects of saliva decrease during sleep, and bacterial growth can cause tooth decay. Fever (body temperature exceeding 38.1° C [100.6° F]) is not associated with teething and should be evaluated for other causes (Douglas et al., 2004).
Parents and children should be educated concerning the care of the toothbrush to provide maximum effectiveness of the toothbrushing activity:
• Replace toothbrush every 3 months.
• Replace toothbrush after a viral illness.
• Avoid rinsing bristles in hot water.
A properly sized toothbrush will aid in developing good toothbrushing technique. A soft brush with a small amount of toothpaste, about the size of a pencil eraser, is appropriate. Dental flossing should be done with an up-and-down motion. A back-and-forth “sawing” motion can cause injury to gingival tissues. Children need assistance and supervision with flossing until at least age 7 years.
Trauma to the teeth often occurs in school-age children. Appropriate protective devices can prevent injury during sports activities. If a primary tooth is knocked out (avulsed) because of trauma, the child should be referred to a dentist for a “spacer” that will maintain tooth alignment until the permanent tooth erupts. If a permanent tooth is avulsed because of trauma, the tooth should be immersed in milk and brought with the child to the dentist for immediate care. Open wounds to oral tissues may require tetanus prophylaxis or antibiotics. All tooth fractures should be referred to a dentist for evaluation and treatment.
Dental problems that occur often with adolescents include puberty gingivitis, gingivitis associated with oral contraceptive use, drug-related gingivitis, and hyperplastic gingivitis associated with orthodontic therapy. Temporomandibular joint problems (TMJ) and malocclusion caused by missing teeth necessitate a dental referral. Orthodontic appliances such as fixed braces can trap plaque and food and increase tooth decay. Meticulous oral hygiene, brushing, flossing, and fluoride applications are part of comprehensive orthodontic care.
A team approach to dental care for the child receiving chemotherapy or radiation therapy includes the dentist, the physician, the nurse, the parent, and the patient. Brushing and flossing when the platelet count is more than 20,000/mm3 and using moist gauze when the platelet count is under 20,000/mm3 is advised to prevent infection and bleeding. The use of chlorhexidine may be prescribed to reduce oral lesions. Table 15-9 reviews medical problems that have an effect on dental health.
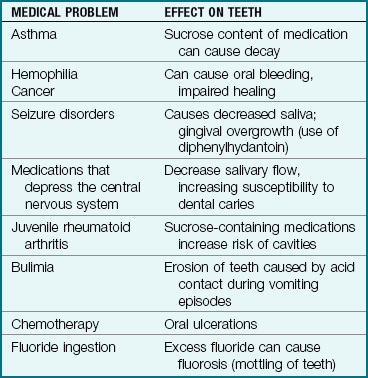
Disabled children can master independent toothbrushing by modifying the toothbrush. Using padded tongue depressors to visualize the oral cavity and an aspirating catheter attached to the toothbrush and connected to a suction machine can assist in providing dental care for a severely disabled child. Battery-operated toothbrushes can help to achieve optimum brushing technique.
In the year 2000, the U.S. Surgeon General issued a report concerning oral health in America (USDHHS, 2000). Preventive oral health was considered to be vital to the maintenance of general health. The principal goals established were to urge health care providers to integrate oral health concepts into education and general health care and to increase the accessibility of oral care for children. Parents can find a local pediatric dentist by searching online.
Play
Play is the business of children. Observing the child at play can aid in assessing growth and development and understanding the child’s relationship with family members. Any plan of care for a hospitalized child of any age should include a play activity that either encourages growth and development or encourages the expression of thoughts and feelings. Playrooms in the hospital pediatric unit can be used for children who have conditions that are not communicable. Medications and treatments should not be carried out in the playroom setting. Play can also be therapeutic and aid in the recovery process. An example of therapeutic play is the game of having the child “blow out” the light of a flashlight as if it were a candle to promote deep breathing. Table 15-10 reviews age-appropriate play behaviors.
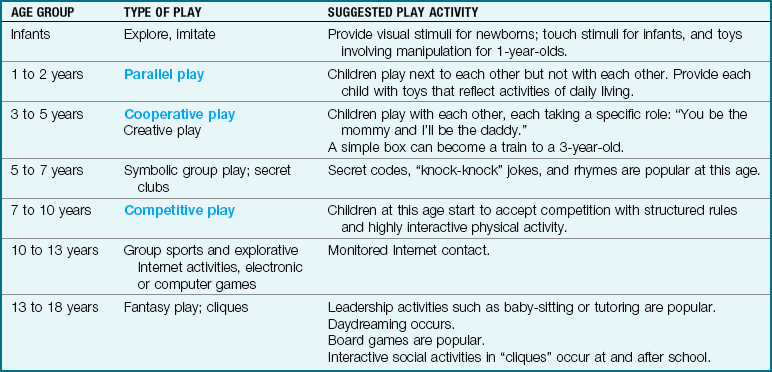
Art is an appropriate play activity at almost any age and provides an avenue for experimentation as well as for creative expression and a feeling of accomplishment in the child. Computer programs are popular with all age-groups, providing problem-solving games, manipulative skills, and opportunities for new learning. Both of these activities must be balanced with active play experiences.
Nursing interventions should focus on encouraging optimal play activities and experiences that are age-appropriate. Parents need guidance concerning the value of play that may not always be a neat and clean activity. Helping parents to select appropriate toys that are safe as well as appropriate to the age and illness is essential. For example, a stuffed animal may not be the toy of choice for an asthmatic child. In the health care setting a blood pressure cuff can give the child a “hug.” Children can play with the equipment they see in their environment to provide stress relief.
Ongoing Health Supervision
Children of all ages should receive ongoing health checkups. Specific health care recommendations are discussed in Chapters 16 through 20. The American Academy of Pediatrics, in partnership with the Academy of State Health Policy, provides a federally sponsored children’s health insurance program (SCHIP) for uninsured children. Information concerning SCHIP for each state can be obtained online.
Get Ready for the NCLEX® Examination!
Key Points
• Growth and development are orderly and sequential, although there are spurts and plateaus.
• Cephalocaudal development proceeds from head to toe.
• Children are susceptible to nutritional deficiencies because they are in the process of growth and development.
• Maslow depicted human development on the basis of a hierarchy of needs.
• Freud’s theories portray personality development as phases of psychosexual development.
• Piaget describes phases of cognitive development.
• Erikson described eight stages of psychosocial development from birth to adulthood.
• Developmental theories can serve as guides to nursing intervention; however, each child grows and develops at an individual pace.
• A family is two or more persons that interact together.
• Parent-child interactions affect positive growth and development.
• Deciduous teeth are baby teeth. The proper care of the teeth depends on caregiver supervision according to the child’s physical level of development and mastery.
• Optimal nutrition is essential to physical and neurological growth and development.
• Motor development follows a predictable sequence.
• Nutritional practices of early childhood tend to persist through adulthood.
• The nurse is responsible for counseling and teaching positive nutritional practices that are acceptable to the family’s culture, religion, and lifestyle.
• The availability of age-appropriate toys enhances physical, emotional, and mental development in infants, children, and adolescents.
• Computer games can foster problem solving, cognitive development, and motor coordination but should be balanced with active play activities.
• Many hospitals have playrooms, which must be kept safe from painful or invasive experiences.
• A nurse is an advocate, educator, and collaborator in a family-centered care environment.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• 2000 CDC Growth Charts: www.cdc.gov/growthcharts
• American Academy of Pediatric Dentistry: www.aapd.org
• Children’s Health Insurance Program (CHIP): www.ncsl.org/programs/health/chiphome.htm
• Dietary Guidelines for Americans: www.healthierus.gov/dietaryguidelines
• Gerber: www.gerber.com
• Inheritance and development: www.ncbi.nlm.nih.gov/omim
• Institute of Medicine: www.iom.edu
• MyPyramid: www.myPyramid.gov
• National Cholesterol Education Program: www.nhlbi.nih.gov/chd
• Parenting skills: http://store.parentsactionstore.org/prostores/servlet/storefront
• Portion Plate for kids: www.theportionplate.com
Review Questions for the NCLEX® Examination
1. How many erupted teeth would the nurse expect a healthy 8-month-old infant to have?
2. During the first week of life, the newborn’s weight:
3. The nurse should encourage the parent to introduce toothbrushing to her child by age:
4. To meet the needs (as described by Erikson) of a school-age child diagnosed with diabetes, the nurse should:
1. explain carefully to the mother the need to rigidly adhere to dietary modifications.
2. allow the child to eat whatever he or she wants and administer insulin to maintain optimum glucose levels.
3. allow the child to perform his own Accuchecks and administer his own insulin.
5. It is most appropriate to first introduce competitive games at age: