The Adolescent
1 Define each key term listed.
2 List major physical changes that occur during adolescence.
3 Identify two major developmental tasks of adolescence.
4 Discuss three major theoretical viewpoints on the personality development of adolescents.
5 List five life events that contribute to stress during adolescence.
6 Describe Tanner’s stages of breast development.
7 Describe menstruation to a 13-year-old girl.
8 Identify two ways in which a person’s cultural background might contribute to behavior.
9 Discuss the importance of peer groups, cliques, and best friends in the developmental process of an adolescent.
10 List three guidelines of importance for the adolescent participating in sports.
11 Summarize the nutritional requirements of the adolescent.
12 Discuss two main challenges during the adolescent years to which the adolescent must adjust.
13 List a source for planning sex education programs for adolescents.
14 Discuss the common problems of adolescence and the nursing approach.
 , p. 456)
, p. 456) , p. 455)
, p. 455) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
General Characteristics
Adolescence is defined as the period of life beginning with the appearance of secondary sex characteristics and ending with cessation of growth and emotional maturity. The term comes from the Latin word adolescere, meaning “to grow up.” Adolescence is often divided into early, middle, and late periods because the 13-year-old adolescent differs a great deal from the 18-year-old adolescent. Middle adolescence appears to be the time of greatest turmoil for most families. Perhaps one of the most characteristic features of adolescence is its uncertainty. It is a period of life that in our culture lasts a comparatively long time and involves a great number of adjustments. The major tasks of adolescence include establishing an identity, separating from family, initiating intimacy, and developing career choices for economic independence. Some of the major theories of development are summarized in Box 20-1. Life is never dull when there are adolescents in the family. The surge toward independence becomes more and more pronounced, making it practically impossible for adolescents to get along with their parents, who represent authority. When adolescents submit to parental wishes, they may feel humiliated and childish. If they revolt, conflicts arise within the family. Parents and adolescents must weather the storm together and try to discover solutions that are relatively satisfactory to all.
Numerous other factors account for the restlessness of adolescents. Their bodies are rapidly changing, and they experience intense sexual drives. They want to be accepted by society, but they are not sure how to attain this goal. Adolescents question life and search to find what psychologists call their sense of identity; they ask, “Who am I?” “What do I want?” This is followed by the intimacy stage, in which adolescents must learn to avoid emotional isolation. They must face the fear of rejection in shared activities such as sports, in close friendships, and in sexual experiences. The older adolescent thinks about the future and is generally idealistic. Jean Piaget and other investigators indicate that during this time adolescents reach the final stages of abstract reasoning, logic, and other symbolic forms of thought, which increases sophistication in moral reasoning.
These facts sound complicated in themselves, but they are intensified by a world that is constantly changing. Gender roles are less well-defined in many households, and parents may not be traditional role models for their children. Many adolescents live in single-parent homes or with working relatives where little, if any, supervision is available.
Conformity is one of the strongest needs of the adolescent in society. Today, with electronic technology bringing common experiences to people all over the world via radio, television, and computers, the combined pressure to conform often overrides cultural or traditional practices. Assimilation is beginning to occur via technology.
The needs of the family often compete with the needs of the adolescent when parents try to push the adolescent into an activity or career that meets the parent’s own personal need or dreams. Parents must be guided to enjoy the interests and activities of the adolescent without imposing their personal desires. The main challenges of the adolescent years include adjusting to rapid physical and physiological changes, maintaining privacy, coping with social stresses (Figures 20-1 and 20-2) and pressures, maintaining open communication, and developing positive health care practices and lifestyle choices.
Growth and Development
Preadolescence is a short period immediately preceding adolescence. In girls it comprises the ages of 10 to 13 years and is marked by rapid changes in the structure and function of various parts of the body. It is distinguished by puberty, the stage in which the reproductive organs become functional and secondary sex characteristics develop. Both sexes produce male hormones (androgens) and female hormones (estrogens) in comparatively equal amounts during childhood. During puberty the hypothalamus of the brain signals the pituitary gland to stimulate other endocrine glands—the adrenals and the ovaries or testes—to secrete their hormones directly into the bloodstream in differing proportions (more androgens in the boy and more estrogens in the girl).
The age of puberty varies and is somewhat earlier for girls than for boys. The final 20% of mature height that is achieved during adolescence is called the growth spurt and usually occurs by 18 years of age. The major cause of weight gain is the increase in skeletal mass. The implications of growth and development for nursing assessments are illustrated in Figure 20-3.
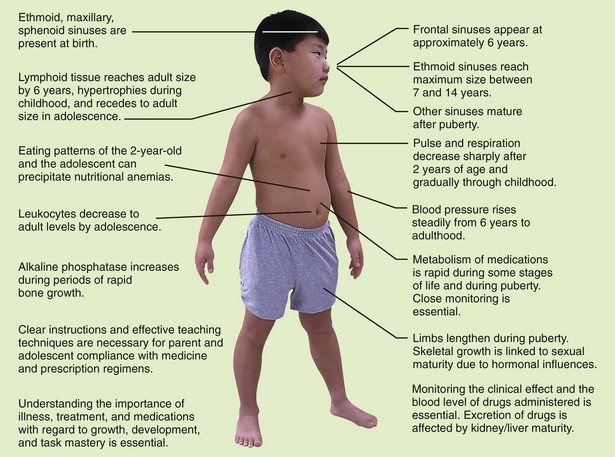
FIGURE 20-3 Many developmental changes occur between infancy and adolescence. The nurse must understand the implications of growth and development for nursing assessments.
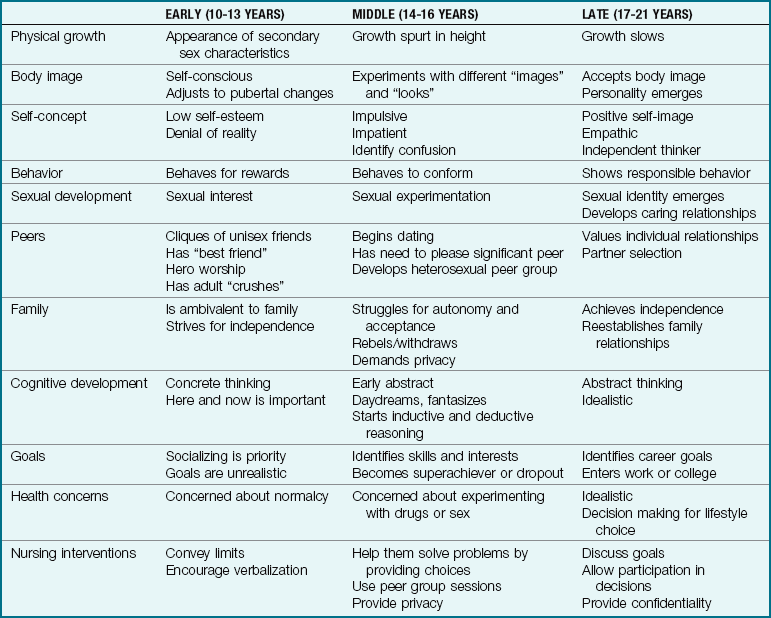
The general appearance of the adolescent tends to be awkward, that is, long-legged and gangling; this growth characteristic is termed asynchrony because different body parts mature at different rates. The sweat glands are very active, and oily skin and acne are common. Both sexes mature earlier and grow taller and heavier than in past generations. Because of the gross motor development that occurs during adolescence, teenagers can gain satisfaction from sports. Table 20-1 outlines the growth and development of adolescents.
 Nursing Tip
Nursing Tip
A rapid period of growth in which the body reaches adult height and weight before age 18 years is known as a growth spurt.
Boys
During fetal life the placental chorionic gonadotropin stimulates Leydig cells to secrete testosterone. Thus weeks 8 to 12 of fetal life are important in the sexual development of the male (XY) child. Luteinizing hormone (LH) maintains testosterone levels. Serum levels of LH increase during sleep 1 to 2 years before puberty. The secretion of gonadotropin stimulates gonad enlargement and the secretion of sex hormones. The interaction among the hypothalamus, pituitary, and gonads supports the development of puberty.
In boys, puberty begins with hormonal changes between 10 and 13 years of age. The shoulders widen, the pectoral muscles enlarge, and the voice deepens. Hair begins to grow on the face, chest, axillae, and pubic areas (Figure 20-4 and Box 20-2). Enlargement of the testicles and of internal structures and pigmentation of the scrotum are followed by enlargement of the penis. Erections and nocturnal emissions take place. The production of sperm begins between 13 and 14 years of age. An athletic scrotal support device (jockstrap) is necessary for boys participating in sporting events or for any activity in which support and protection of the genitalia are required. Athletic supporters not only support and protect the genitalia but also prevent embarrassment from exposure. Athletic supporters are purchased by size. Good personal hygiene is necessary because heat and friction may lead to jock itch, a fungal infestation of the groin. Sharing athletic supporters is discouraged.
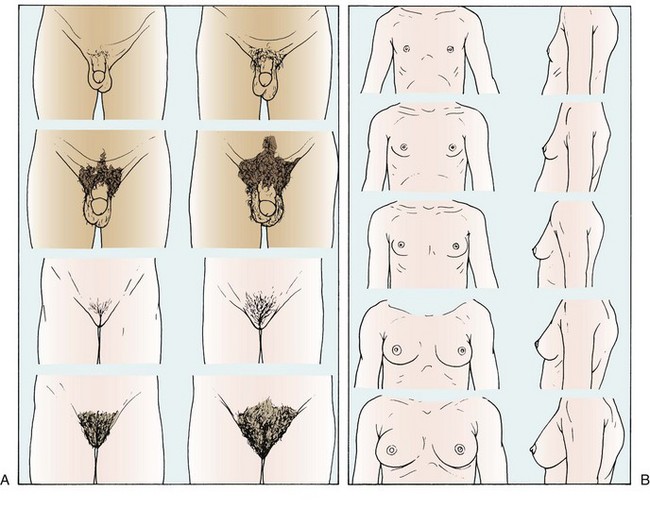
FIGURE 20-4 A, Sexual maturity ratings (SMRs) of pubic hair changes in adolescent boys and girls. B, SMRs of breast changes in adolescent girls. Bone growth is closely correlated with SMR because epiphyseal closure is controlled by hormones.
Some experts recommend that after puberty boys examine their testes during or after a hot bath or shower. Each testicle is examined using the index and middle fingers of both hands on the underside of the testicle and the thumbs on the top of the testicle. The testicles are gently rolled between the thumb and the fingers to feel for abnormalities. Testicular and scrotal self-examinations are performed once a month. If a lump is discovered, it should be reported immediately to a health care provider (American Cancer Society, 2010).
Girls
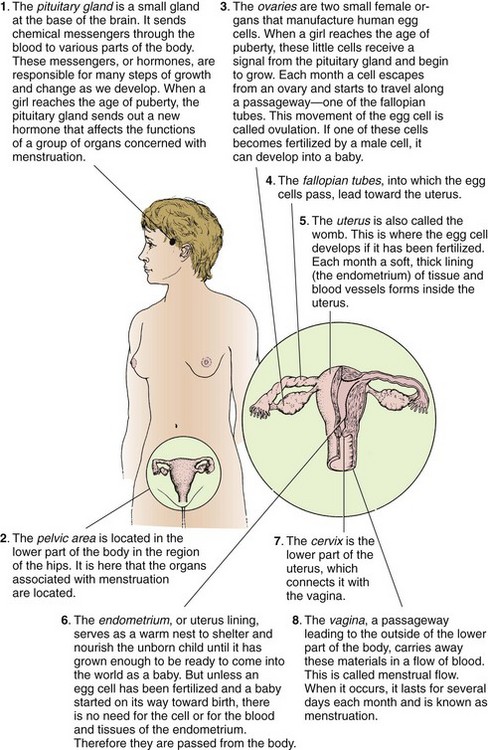
Pubertal changes in girls occur 6 months to 2 years before they occur in boys. Puberty is easily recognized in girls by the onset of menstruation (Figure 20-5). The first menstrual period is called the menarche. It commonly occurs about age 12 or 13 years, but this varies. It may occur as early as age 10 years or as late as age 15 years. Secondary sex characteristics become more apparent before the menarche. Fat is deposited in the hips, thighs, and breasts, causing them to enlarge (see Box 20-2).
At this time the adolescent girl may need to be fitted for a bra. Measurements must be ascertained and various styles tried on for comfort. Straps should fit so that they do not continually fall from the shoulders. Cups need to be large enough to support fullness near the underarms. The garment must fit across the back so that it is not uncomfortably tight. Adolescents generally like attractive undergarments that have some type of lace trim. Sports bras are available for girls who participate in active sports. Puberty is a good time to begin teaching breast self-examination (see Skill 11-1). Instructional materials are available through the American Cancer Society.
The external genitalia grow. Hair develops in the pubic area (see Figure 20-4 and Box 20-2) and the underarms. It is important to note that in ballet dancers, runners, gymnasts, and adolescents engaged in other athletic activities that involve a lean body and high level of physical activity, the mechanisms affecting puberty can be altered and cause a delay in the onset of menarche. Energy balance, activity, and nutrition are important factors to evaluate when menstruation is delayed. Further growth can no longer take place when the ends of the long bones knit securely to their shafts (epiphyseal closure). See Chapter 2 for a detailed discussion of the physiology of reproductive organs.
Psychosocial Development
Physical growth and sexual interest correlate with sexual maturity. Cognitive growth and social changes correlate with chronological age and placement in school. Stress can increase when physical growth and cognitive growth occur at different rates in the same adolescent. Although the early-maturing male often finds positive social adjustment and acceptance, early-maturing females are often embarrassed and develop low self-esteem. The adolescent’s desire for freedom and independence is extremely important and necessary for developing individuality. To accomplish this, young persons must reject their childhood self and often the people most closely associated with it. Erikson identifies the major task of this group as identity versus role confusion. Emancipation is a critical element in the establishment of identity.
Adolescents want to be people in their own right, and they “try on” different roles. Self-concept (one’s view of oneself) fluctuates during this time and is molded by the demands of parents, peers, teachers, and others. Interaction with others helps adolescents determine who they are and in what direction they want to proceed. This process is more difficult for low-income minorities and is complicated by many factors, such as illness, broken homes, and the extent of formal education. Young persons who are unable to master confusion and establish an identity may become rigid in their actions, bewildered, or depressed, or they may cling to the conformity of peer groups long after the need should have passed. Some show an inordinate need for something “new and exciting.” They may experience low self-esteem and alienation, and they may confront many other difficulties on entering the adult world.
Nursing Tip
In adolescence, dependency creates hostility. Parents who foster dependence invite unavoidable resentment. Wise parents make themselves increasingly dispensable. Their language is sprinkled with such statements as “The choice is yours,” “You decide about that,” “If you want to,” and “It’s your decision.”
Sense of Intimacy
Developing intimacy is closely entwined with the resolving of a person’s sense of identity. As adolescents move toward young adulthood, they become ready to take the risks of close affiliations and friendships and to establish relationships with the opposite sex (Figure 20-6). Avoidance of building these relationships may lead to a deep sense of isolation. Adolescence is a period of trying and testing. Disagreements with parents often revolve around dating, the family car, money, chores, school grades, choice of friends, smoking, sex, and the use of illicit drugs. The young person questions parental values and morals and is particularly sensitive to hypocrisy.

FIGURE 20-6 As adolescents move toward young adulthood, they become ready to take the risks of close affiliations and friendship and to establish relationships with members of the opposite sex.
Adults who associate with adolescents should try to create an atmosphere of interest and understanding. Adolescents must know that adults care. Adolescents need practice in making decisions that must be respected even if they have made a mistake. Parents should set limits and expect them to be challenged but not exceeded. Parents and nurses who see other people’s intrinsic worth, feel good about themselves, and do not see the adolescent’s behavior as a reflection on their parenting or nursing provide a more secure environment for growth. Loving detachment is not easy, but it is an effective tool in dealing with adolescents.
Cultural and Spiritual Considerations
Americans are multiethnic, multicultural, and multilingual. The value of independence as a goal of maturational and emotional development may not be adopted by all. The traditional Chinese do not recognize the period of adolescence; there is no word for it in their language. Many immigrants and Americans of Asian descent come from societies that are patriarchal and highly structured and have distinct social roles. The good of the family takes precedence over personal goals. The protection of family image and neighborhood reputation is essential.
As part of a search for their identity, adolescents focus on the values and ideals of the family and decide either to embrace them or to separate from them. Adolescents often perceive their feelings and thoughts as unique and therefore do not express their feelings freely. Adolescents can understand abstract concepts and symbols, and exposure to religion and religious practices other than those experienced within their own traditional family can help them stabilize their group identity (Figure 20-7). The nurse’s awareness of these and other cultural influences on the adolescent’s behavior will help in the effort to provide holistic care.

Body Image
In early adolescence the young person must adjust to the dramatic changes of puberty. Focusing on body development during early and middle adolescence is one factor that contributes to egocentrism, or self-centeredness. Young persons create what has been termed an “imaginary audience.” They believe everyone is looking at them. This preoccupation with self is normal and accounts for the constant hair combing and makeup repairing often observed in a group of adolescents. Young adolescents may try to hide their changing body or may advertise it. They may take pride in their abilities or feel frustrated when their actual abilities do not match their perceived abilities.
In early adolescence teens make every effort to be just like their peers. A pimple on the skin or a disability is disastrous to the young adolescent. By late adolescence, most have completed their growth, are less self-conscious, and enjoy their individual skills, abilities, and interests. Chronic illness or eating disorders (see Chapter 33) may complicate or exacerbate unresolved problems of body image.
Peer Relationships
Peer groups help adolescents to feel that they “belong” and make it possible to experiment with social behaviors (Figure 20-8). School assumes an important role in the psychological development of the adolescent by providing the focus for initiating social interaction. Small, exclusive groups called cliques form. These unisex groups are made up of adolescents with similar interests, values, and tastes. Belonging to the group is of utmost importance to the young adolescent.
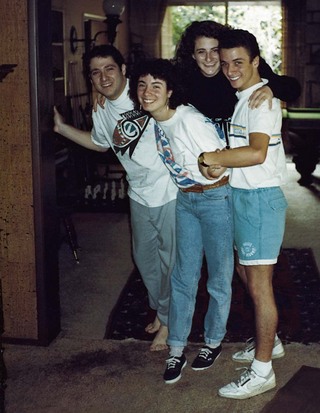
FIGURE 20-8 Immersion into a peer group helps adolescents free themselves from childhood dependence.
Within the clique, the adolescent often develops a close personal relationship with one peer of the same sex. This best friend interaction supports social development by enabling adolescents to experiment with behaviors together and listen to and care about each other (Figure 20-9). Stable “best friend” experiences often precede successful heterosexual relationships in later life.

FIGURE 20-9 Adolescents practice facial expressions and try out new hair styles. “Best friend” interaction supports social development by enabling the adolescent to experiment with behavior and care about others.
The peer group serves as a mirror for “normality” and helps to determine where one “fits in.” It is vitally important in helping adolescents define themselves. Acceptance by one’s friends helps to decrease the loneliness and sense of loss many adolescents experience on the road to adulthood.
The social norms and pressures exerted by the group may cause problems. The selection of friends and allegiance to them may bring about confrontations within the family. Parents need help in understanding that the adolescent’s exaggerated conformity is necessary to moving away from dependence and obtaining approval from persons outside the nuclear family. Failure to develop social competence may produce feelings of inadequacy and low self-esteem.
Nurses can assist the family by supporting and educating them in the dynamics of this age-group. Parents can be directed to groups such as peer helpers (for the adolescent) and community educational programs sponsored by various agencies. Organizations such as Parents Without Partners might be another resource.
Career Plans
Some adolescents graduate from high school with a definite idea of what they would like to do. Many, however, are unsure of what they want. To choose a career that is best suited for them, adolescents must first know themselves. What particularly interests them? What are they good at? What are their shortcomings?
By this time, adolescents have already taken some definite steps toward a goal. Choice of high school curriculum and grades determine eligibility for college or preparation for a specific vocation. Parents should observe the interests of their children and encourage them to take advantage of their talents (Figure 20-10). Whenever possible, an adolescent should investigate various fields by talking to people who are involved in them.
FIGURE 20-10 Parents should encourage adolescents to take advantage of their talents. Singing, playing a musical instrument, or developing mechanical skills is part of adolescent life.
Valuable information can also be obtained by career exploration, which is available at most colleges, and by pamphlets from professional organizations, the government, Internet sites, and other sources. The school guidance counselor administers aptitude tests as an additional guide and can work with adolescents to expose them to as wide a selection of careers as possible. The adolescent must make the final decision. To be happy in a career, the adolescent must choose it of his or her own free will and not because parents expect him or her to follow in their footsteps.
The job market today is extremely competitive and almost nonexistent for some people without skills or higher education. Productive employment must fit young people’s life framework and offer an opportunity for personal growth. Some positive aspects of employment include helping to build self-esteem, promoting responsibility, testing new skills, constructively channeling energies, providing money for increased independence, engaging the young person in interactions with adults, and allowing the adolescent to assume an active rather than a passive role. In contrast, when adolescents are forced to take a job because of economic or personal pressures, they may need to drop out of school. With few skills and no experience, they may remain locked into low-level employment. This is often perpetuated from one generation to another.
Responsibility
Adolescents look forward to challenges. Parents must encourage their children to take on new responsibilities. The adolescent is often humiliated by being placed in a dependent role, such as when a parent or sibling drives them to school. Driving a car, riding a bicycle, or walking provides a sense of independence and responsibility. Even routine jobs can be made more inspiring if youths are taught to see them in relation to a longer-term objective.
Young adolescents must also be taught the value of money. An allowance helps them to learn financial management. If money is simply handed out as requested, it is more difficult to develop responsibility for finances. Allowances should be increased from time to time to comply with the age and needs of the adolescent.
Middle and older adolescents who have jobs can be taught to use a checkbook and a savings account. Many find satisfaction in purchasing their own clothes. An adolescent who buys an old car soon discovers that it takes money to insure, run, and repair it. Such experiences provide valuable lessons in finance. Baby-sitting is a common means of earning money among younger adolescents. Many boys and girls begin to assist with baby-sitting at about 12 or 13 years of age. Baby-sitting courses are valuable because young people need to be prepared for this important responsibility.
Cognitive Development
Piaget’s theory of cognitive development states that development is systematic, sequential, and orderly. Young adolescents are still in the concrete phase of thinking. They take words literally. A young adolescent girl, if asked by the nurse, “Have you ever slept with anyone?” may not connect the question with a vaginal infection or sexual intercourse. By middle adolescence the ability to think abstractly has increased. Piaget calls this the stage of formal operations. Older adolescents can see a situation from many viewpoints and can imagine or organize unseen or unexperienced possibilities. Abstract thinking and reasoning emerges.
Therefore when teaching early adolescents about menstruation, the nurse focuses on concrete issues and concerns. When abstract thinking emerges in later adolescence, the abstract meaning of menstruation relating to womanhood or motherhood can be discussed. Empowering young adolescent girls by educating them according to their intellectual and emotional developmental level can increase their self-image. Adolescents are able to sympathize and empathize. They can understand their own values and actions and can also understand and accept differing values and actions of people from other cultures.
Daydreams
Adolescents spend a lot of time daydreaming in the solitude of their rooms or during a class lecture. Most of this behavior is normal and natural for this age-group. Daydreaming is usually considered harmless if the young person continues the usual active pursuits. It also serves several purposes. Adolescence is a lonely, in-between age; daydreaming helps to fill the void. Imaginatively acting out what will be said or done in various situations prepares adolescents to deal with others so they can better cope with real situations. Daydreams are also a valuable safety valve for the expression of strong feelings.
Sexual Development
Adolescents must meet and become acquainted with members of the opposite sex. This may begin with admiration from afar, which is accompanied by daydreams as the young person attempts to attract the other’s attention.
Group dates for structured school or church functions are followed by double dating and then single-couple dating. Dancing provides an opportunity for the symbolic expression of sexual urges without physical contact. Slow dancing provides a mode of close physical contact in public that is socially acceptable. Long telephone or text messaging conversations link the adolescent to peers when they are at home or feeling alone. “Crushes”—feelings of attachment to a person of the opposite sex who is popular or possesses qualities important to the adolescent—are a common occurrence. Competition and rivalry may be keen, but long-term commitment and deep romantic attachments are not often present.
Sexual experimentation often occurs as a response to peer pressure, as a means for momentary pleasure, as a learning experience to satisfy curiosity, or as a means of gaining a feeling of being loved and cared about. Sexual behavior can affect the growth and development of the adolescent. Unplanned pregnancies or sexually transmitted infections (STIs) are two major complications of adolescent sexual interaction, because few adolescents responsibly use protection (Kliegman et al., 2007).
The adolescent’s cultural background influences patterns of dating. Conflict often arises when the adolescent wants to be independent and quickly adopts American norms of dating while parents insist on strict traditional values. This is particularly noticeable with daughters.
Dating is one of the early social aspects of growing up. Attending the high school prom is a rite of adolescence. As such, it may become a battleground for the struggle for independence. Parents’ opposition is often based on their unspoken fears. Parents may also fear sexual experimentation, pregnancy, or acquired immunodeficiency syndrome (AIDS). They may respond by imposing strict restrictions, such as curfews, chaperones, and limitations on use of the car. When these problems are not discussed openly, the adolescent may react by rebelling sexually or by other means to test general parental control, rather than for the sake of the prohibited act itself.
Sexual curiosity and masturbation are common among adolescents. There is also a need for the intimacy of close personal friendships. Seeking one person of the opposite sex to share confidences and feelings may lead to sexual intimacies. This may produce guilt feelings and can lead to isolation from friends and family. The breaking up of such romances is often a source of great emotional pain.
Most of our knowledge about the sexual behavior of Americans comes from the pioneering efforts of Alfred Kinsey. Although his studies had flaws, they provided much in-depth information. A wide variety of sexual behavior is freely discussed and depicted in movies, in magazines, online, and on television. Music directed toward young people often centers on sexual themes. Premarital sexual activity has become much more widespread, and adolescents are initiating their sexual activity at increasingly younger ages. Thirty percent of girls and 45% of boys report having had sexual intercourse by 18 years of age (Kliegman et al., 2007).
Sex Education
Sex education for the adolescent is a challenge. Nurses must put aside their own attitudes and biases; understand society, cultural, and moral values; and incorporate a broad understanding of physical and psychological growth and development to prepare an effective school or clinic program. Television, movies, magazines, and computer chat rooms or websites provide a source of information for sex education for the adolescent that may or may not be accurate and helpful to the young adult.
The prevalence of human immunodeficiency virus (HIV) exposure, AIDS, and other STIs was a factor that resulted in the formalized incorporation of sex education in schools. This education focuses on the physiology of sex, the reproductive systems, and STIs as well as personal values concerning sexuality, facts about contraception, safe sex, and peer pressure. Formal structured comprehensive sex education programs are available from the Sexuality Information and Education Council of the United States (SIECUS) and other community agencies. These types of programs are geared to kindergarten through grade 12 and present information about all aspects of health, such as nutrition, dental care, avoidance of drugs, and STIs. These courses should be presented as age appropriate. The physiology of the reproductive systems can be taught at about grade 5. By grade 8 topics such as coping skills for dating and sexuality, pregnancy, and birth can be reviewed. Abstinence and contraception are also discussed.
Decision making is emphasized. Flowcharts should show the possible consequences of certain actions. The high school units can include how to handle adolescent pregnancy, prenatal and postnatal care, and effective parenting techniques. A unit on intimate relationships can be presented as a series of discussions and activities designed to help students think about the nature of love. It can cover ideas such as compromise, problem solving, and communication skills. It should emphasize the many reasons why adolescents should say “no” to casual sex.
Factual and sensitive information provided by concerned parents is, of course, the ideal. However, too often peers provide erroneous material or parents postpone education until a crisis arrives. Children must be told what body changes to expect and why these changes occur. Two years too soon is better than 1 day too late! Parents who have answered their children’s questions truthfully throughout childhood offer a secure and natural foundation on which to build. Studies have shown that adolescents who obtain early sex education information from caring parents or well-informed adults do not have a higher rate of sexual activity.
Concerns About Being “Different”
Adolescents have certain concerns that are specific to puberty. The girl who begins to experience physical changes at about 10 years of age may feel self-conscious because she towers over her friends or needs to wear a bra. She may be teased because she is different. The other extreme is the latecomer who feels abnormal and unattractive because her friends look more feminine.
Such problems are not limited to girls. Of particular concern is the boy on a slow schedule of development. Still short at age 15 years, he is unable to compete for placement on school teams because of his size. He sees his male friends being admired for their height and strength, and this is a threat to him. Such fears are natural and usually are alleviated by reassurances that, although boys begin to grow later than girls, their growth spurt lasts longer. During data collection, the nurse has an opportunity to support the adolescent who is concerned about normal growth and development.
Traditional gender stereotypes define being “male” by activity and achievement and being “female” by sensitivity and interpersonal competence. Society’s current trends toward equality of the sexes may affect these roles. Nevertheless, few adolescents escape the social pressures that dictate acceptable sexual attitudes and behavior for each sex.
Homosexuality
When a person has an attraction for a person of their own sex, that person is referred to as homosexual. A lesbian is a female who prefers other females as sexual partners. A male is called gay when he prefers another male as his sexual partner. Homosexual behavior in adolescence is not uncommon. This experimentation is not a positive predictor of adult sexual preference; it may merely indicate a desire to explore alternative lifestyles. Homosexuality occurs in about 5% of men and women (Kliegman et al., 2007) but is no longer listed as a mental disorder by the American Psychiatric Association (2000). It is thought that a combination of cultural, biological, and psychological factors contribute to sexual orientation and development. The nursing role is not to change homosexual behaviors but to help the child understand how to cope with the reaction of others.
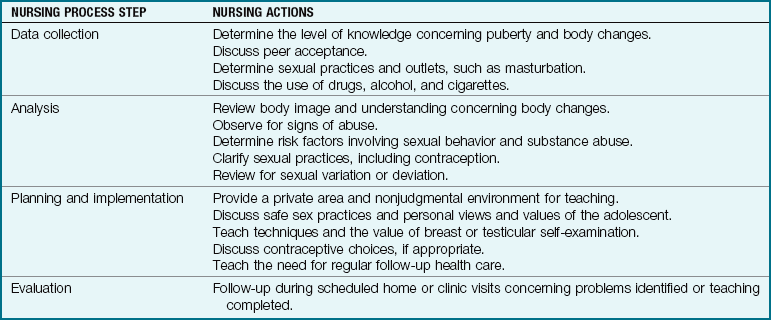
Nurses must be sensitive to these issues when obtaining histories and working with young adolescents. They must also be aware of their personal biases to determine their potential effectiveness with this population. Support groups for parents and friends of gays and lesbians are available. Those who question their sexual orientation are referred to counselors and health agencies that can respond to their needs. Table 20-2 provides an example of the use of the nursing process in planning sex education for the adolescent.
Parenting the Adolescent
Parenting an adolescent requires major adaptations on the part of the parents. At times it is difficult for parents to cope with adolescents. The shift in parenting philosophies from the rigid rules of discipline to permissiveness or the current middle-of-the-road position often leads to confusion. Some parents are unsure of their own opinions and may hesitate to exert authority. Others refuse to “let go” or change any of their beliefs to accommodate today’s youth. Issues of privacy and trust abound, and conflict occurs as the adolescent desires more adult liberties. Adolescents may need time alone to separate themselves from family and search for their identity.
Adolescents need to talk about their fears, such as school examinations or how they will look with a certain haircut. They need assistance in sorting out confused feelings. A confidential, accepting atmosphere will promote quality communications (Figure 20-11). Physical symptoms, such as stomachaches, insomnia, and headaches, surface in relation to anxiety. Bizarre behavior may be a call for long-overdue help.

FIGURE 20-11 Listening is an important tool for establishing rapport. A confidential, accepting atmosphere will promote good communication.
Some approaches to such problems are presented in the Health Promotion box below. As adolescents try to separate themselves from their family, they may reject some family traditions such as family outings or dress codes. When parents respond to this behavior negatively, the separation widens and tension grows. Often adolescents search for adults outside of the family as role models and confidants. Coaches or scout leaders can fulfill this role and serve as positive outlets for gaining a sense of “belonging” when there are conflicts at home.
 Health Promotion
Health Promotion
Effective Approaches to Problems
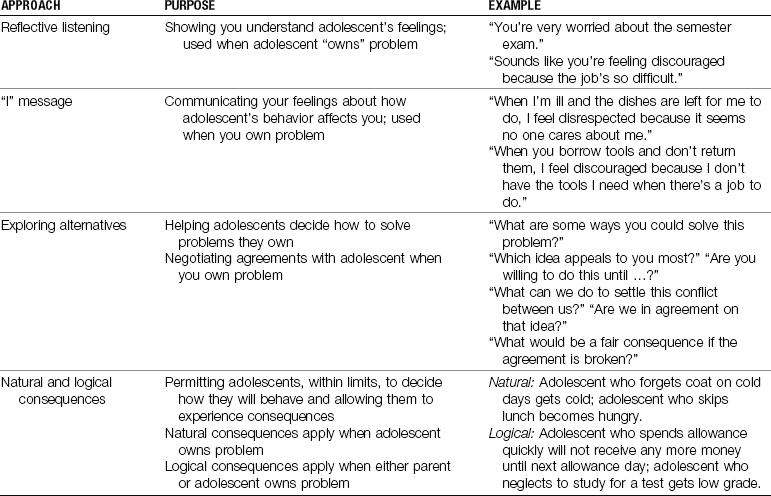
From Systematic training for effective parenting of teens: Parenting teenagers. Circle Pines, Mich: American Guidance Service. © 1990 by Don Dinkmeyer and Gary D. McKay
Nurses should help parents keep the lines of communication open, promote respect and trust, and provide confidentiality and a sense of privacy. Despite the problems parents face with their adolescents, the family continues to play a major role in socialization.
Health Promotion and Guidance
Adolescents grow rapidly; therefore they need foods that provide for their increase in height, body cell mass, and maturation. Adolescents appear to be “always hungry” because their stomach capacity is too small to meet the increased caloric and protein requirements of their rapid growth spurt. Frequent meals are needed. Dietary deficiencies are more likely to occur at this age because of this growth acceleration and because eating patterns become more irregular. Nutritional requirements are more strongly correlated with sexual maturity ratings (SMRs) (see Box 20-2) than with age. For example, girls at SMR 2 and boys at SMR 3 are close to their peak growth velocities. They require adequate intake of nutrients and calories, regardless of their chronological age.
The most noticeable changes in the adolescent’s eating habits are skipped meals, more between-meal snacks, and eating out more often. Breakfast and lunch are often omitted. Part-time jobs, school activities, and socialization may result in the adolescent eating little or nothing during the day and then “catching up” in the evening. Fast-food restaurants are inexpensive and provide food quickly for the busy adolescent. These foods tend to be high in calories, fat, protein, sugar, and sodium and low in fiber. In general, to determine the dietary fiber intake needs in children, add 5 g (0.2 oz) to the age in years (Dartmouth-Hitchcock, 2010). Most food chains have added salads and other healthier foods, which is applauded. Carbonated drinks often replace milk, resulting in low intakes of calcium, riboflavin, and vitamins A and D.
Foods should be selected from the basic food pyramid (see Figure 4-7). In estimating calories, variables such as physical activity and sex must also be considered. The elements most likely to be inadequately supplied in the adolescent’s diet are calcium, iron, and vitamin B12. Zinc is known to be essential for growth and sexual maturation and is therefore of great importance in adolescence. The recommended dietary allowances (RDAs) for adolescents are listed in the Evolve resources for Chapter 15.
Vegetarian Diets
Foods and eating fads are often the main conflict between adolescents and their parents. However, adolescents are now a growing segment of the vegetarian population. Ninety percent of adolescent vegetarian diets include eggs and milk. Iron-rich foods include fortified grain products. However, a high intake of whole grains, bran, and foods rich in oxalic acid (e.g., spinach) can impair the absorption of iron. Tofu, nuts, wheat germ, and legumes can provide the zinc necessary for cognitive development. If animal products are totally excluded in the diet, a vitamin B12 supplement may be necessary. The nursing role is to understand the eating pattern, identify fad diets, and understand the reason the diet was selected, and then evaluate and discuss any deficiencies or needs within that diet. Developing a partnership with the adolescent in meeting growth needs and allowing the adolescent to take responsibility for meeting his or her own health needs are the cornerstones for success in nutritional education.
Vegetarians who eat no animal protein, eggs, or dairy products (vegans) are at particular risk of developing deficiencies in protein, vitamin B12, calcium, iron, iodine, and possibly zinc. A total vegetarian diet is adequate only if it is carefully planned.
Sports and Nutrition
The best training diet is one that contains foods from each of the basic food groups in sufficient quantities to meet energy demands and nutrient requirements. What to eat and when to eat it in relation to muscle exercise are vital to successful athletic performance. Athletes exhaust reserves of muscle glycogen. Carbohydrates that can be rapidly converted to blood glucose and transported to muscles will provide the rapid recovery of muscle glycogen necessary for maintaining prolonged intense muscle activity. Eating a slowly absorbed glucose source will prevent the development of chronically low muscle energy stores. To hasten muscle energy recovery, the young athlete should consume at least 50 g of a rapidly used carbohydrate within 4 hours after exercise. Foods high in fat and protein will prolong carbohydrate metabolism.
Carbohydrates that provide both energy and other nutrients are best for athletes. Therefore fruits and fruit juices are a better choice than sugar-rich soft drinks and candy. The fat content in candy will slow carbohydrate absorption. Some foods that provide a rapid supply of carbohydrates to muscles include corn flakes, bagels, raisins, maple syrup, potatoes, and rice. Some foods that supply a slow release of carbohydrates to muscles include apples, pears, green peas, chickpeas, skim milk, and plain yogurt.
Fluids lost by sweat must be replaced by drinking small amounts of fluid during a workout. Thirst is one guide for intake. Caffeine and alcohol deplete body water and are to be avoided.
Anabolic steroids, used by some athletes to gain weight and increase strength, are detrimental to bone growth. Iron is particularly necessary for female athletes, who may be borderline or deficient in their intake of this mineral.
Nutrition and School Examinations
The role of diet in the management of illness has become traditional practice. The role of diet in maintaining health is becoming prominent in health education today. Nutritional practices are the focus of weight control programs, and special nutritional supplements are available for athletes, pregnant women, and older adults. Studies have shown that foods can affect behavior, moods, and alertness.
For the adolescent who is scheduled to take an important school examination, the nurse can offer nutritional guidance as part of the examination preparation. Carbohydrates such as pancakes and syrup, breakfast pastries, or a muffin and jelly increase serotonin in the brain, resulting in a soothing, sleepy response. Bacon and eggs are high in fat and cholesterol and are therefore slow to digest, diverting blood from the brain during the digestion process and causing decreased alertness. Drinking more than 4 cups of a caffeine-containing beverage such as coffee can cause overstimulation and nervousness. However, protein-rich meals increase amino acids and tyrosine, which will break down into norepinephrine in the brain and result in increased alertness. Fish, soy, peanuts, and rice increase choline and acetylcholine in the brain, which result in increased memory. Therefore a “proper” meal before a big school test may help the adolescent’s achievement as well as his or her health.
Personal Care
The adolescent needs personal hygiene information because body changes require more frequent bathing and the use of deodorants. The nurse can help the young person sort out the various claims of reliability for hair removal, menstrual hygiene, and cosmetic products and procedures. Body piercing, a popular adolescent fad, should be performed only by an experienced person using sterile instruments. The skin around the point of insertion of the body ring should be regularly inspected for signs of infection. Swapping of body rings is discouraged. Adolescents are warned not to use another’s razor or toothbrush, particularly in light of the risk of HIV infection.
Dental Health
The prevalence of tooth decay has substantially decreased. This is believed to result from the widespread use of fluorides, including community fluoridation, dental sealants, and dental products containing fluorides. Adolescents are nonetheless at risk for dental caries because of inadequate dental maintenance and frequent snacking on sucrose-containing candies and beverages. When dental hygiene is neglected, the period of greatest tooth decay in the permanent teeth is from ages 12 to 18 years. Lack of oral hygiene (inadequate brushing, flossing, and rinsing, particularly after meals) fosters the accumulation of plaque and food debris. Missing, aching, or decayed teeth contribute to poor nutrition. Young people with unattractive teeth may suffer from low self-esteem. Corrective orthodontic appliances are often worn during adolescence, and meticulous oral hygiene is essential to prevent discoloration of tooth enamel and other complications.
According to media hype, healthy, white teeth are synonymous with popularity and sex appeal. Regular dental visits during adolescence must be maintained as a priority in the health care teaching of adolescents and their families. See Chapter 15 for a detailed discussion of dental health.
Sunbathing
Adolescents respond to movie and magazine pictures of the ideal “healthy suntanned body” as an attractive aspect of a body image. The young adult looks forward to sunbathing on the beach or at the pool during summer vacations and often prepares his or her body by trying to obtain a tanned appearance using artificial means. The nurse plays a vital role in educating the adolescent concerning the danger of the sun’s rays and the need for skin protection with a sun protective factor (SPF) of at least 15. Protection of the eyes from the sun is also essential. Excessive sunlight and the use of artificial tanning machines can cause serious long-term reactions such as early aging of the skin or skin cancer (see Chapter 30).
Safety
The chief hazard to the adolescent is the automobile (Figure 20-12). Road and off-road vehicle accidents kill and cripple adolescents at alarming rates. Some schools now offer driver training courses as an integral part of the educational program. Students learn how to drive and the accompanying responsibilities; however, this does not ensure compliance. Preventing motor vehicle accidents is of utmost importance to every community. Adolescents who ride motorcycles, motor scooters, or motorbikes should know the rules of the road and wear special safety equipment, such as helmets.

FIGURE 20-12 Adolescents look forward to getting their driver’s license. The search for independence also brings responsibilities.
Young people should learn how to swim and practice swimming safety. Accidents result from diving into unsafe areas, from using alcohol or drugs while swimming, and from unsafe use of jet skis. If adolescents are interested in hunting or similar sports that require a gun, they must be instructed in the proper safeguards.
Sports Injuries
Sports involving body contact can be hazardous to the adolescent. Sports teams separated by age only are a special problem, because adolescents of one specific age-group can vary in size, weight, and muscle strength. Protective gear should be worn by all team players in any contact sport. The feeling of strength and the need to show off can motivate the adolescent to participate in risky behavior. Assessment of the female athlete in training should include identification of the “female athlete triad,” which includes an eating disorder, amenorrhea, and osteoporosis. Coaches, parents, and health care providers must be vigilant for this condition, which has serious long-term complications (Loman, 2009).
All student athletes should have comprehensive cardiovascular screening before participating in competitive sports activities. Each year, many high school athletes die in a nontraumatic sports-related death. Most deaths result from cardiac problems that are not obvious. The American Academy of Pediatrics Committee on Sports Medicine has established guidelines for medical clearance for sports activities (Saglimbeni, 2010). There may be a future role for genetic testing for cardiac disease in athletes with a family history of cardiac problems. The school nurse can play a key role in safety education by working closely with school coaches and parents.
Common Problems of Adolescence
The growing drug trade and the increase in vandalism and crime expose adolescents to unprecedented assaults in their schools and neighborhoods. Gang-related deaths from guns and knife wounds have escalated greatly. This growing menace is a source of great frustration and concern to parents and to all who provide services to children.
When adolescents experiment with different types of behavior in a search for their identity, they may experiment with drugs. The best weapon against illicit use of drugs is education. Drugs are often made available in the schools and in the streets of the neighborhood where adolescents congregate. The need to conform, the need to be accepted, peer pressure, and the emotional depression often occurring in the turmoil of adolescent adjustments are strong influences promoting drug use. Education concerning the dangers of drug experimentation and use is essential in the home and in the school.
Adolescents are prone to mood swings as they try to adjust to the many physical and psychological changes occurring in their lives. The present may feel overwhelming, and the future blurs. The PACE interview (Schwartz, 1997) can assist in distinguishing the drug-free adolescent from one who may be experimenting with drugs and requires a follow-up referral.
 Memory Jogger
Memory Jogger
P—Parents, peers, and pot: Question the adolescent concerning his or her parents, relationships with peers, and attitude toward and exposure to marijuana.
A—Alcohol, automobiles: Question the adolescent concerning alcohol use (e.g., alcohol at parties) and his or her driving record.
C—Cigarettes: Discuss the adolescent’s smoking history.
E—Education: Discuss the adolescent’s attitude and performance in school.
If two or more of the PACE letters are problem areas, the adolescent may be at high risk for drug abuse and require a professional referral. Follow-up care may involve making a contract with the adolescent to be drug free, educating the adolescent, teaching coping skills, and referring the parents to a support group such as Tough Love Groups or the National Family Partnership.
Depression
Sometimes an adolescent who appears to be adjusted and performing well in school may become depressed. Drug use can precede the development of depression. Working parents and busy teachers can easily overlook slowly changing behaviors. A change in school performance, in appearance, or in behavior can be a warning sign of depression, which can lead to suicide if left untreated. A threat of suicide is a call for help that must be taken care of without delay. Suicide is the third leading cause of death in the adolescent group age 15 to 19 years (Centers for Disease Control and Prevention, 2009). The school nurse can help the adolescent by recognizing the depression, encouraging open communication, posting the numbers of available hotlines, identifying appropriate coping mechanisms, and providing professional referrals.
Adolescent Pregnancy
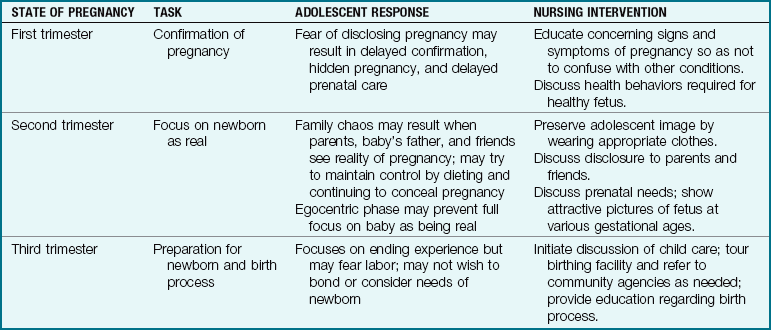
Adolescent pregnancy continues to be a social and health concern in the United States. Nurses must be familiar with the tasks of the adolescent years and recognize that adolescent pregnancy occurs while the adolescent is still struggling to deal with developmental issues. There are many psychosocial factors that influence sexual activity during the adolescent years. The developmental and physiological impact of pregnancy on the adolescent, the tasks and adolescent responses, and the appropriate nursing interventions are described in Tables 20-3 and 20-4. Nutritional needs and nursing care of the pregnant adolescent are discussed in Chapter 4, and nursing care of the adolescent during labor and delivery is discussed in Chapters 7 and 9.
Table 20-3
Developmental and Physiological Impact of Pregnancy on the Adolescent
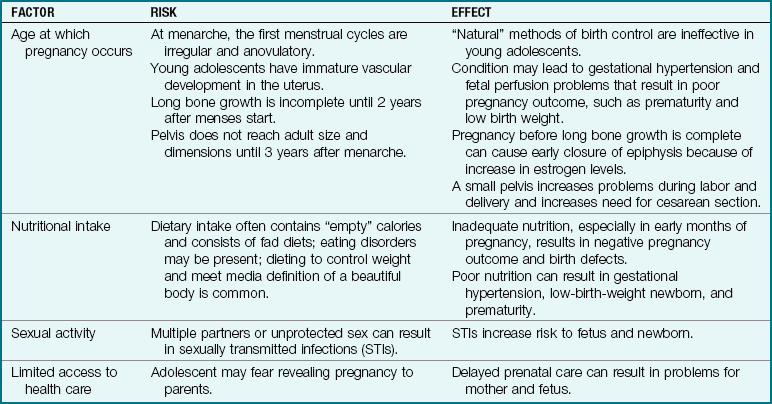
Note: Studies have shown that pregnancy in late adolescence accompanied by good prenatal care does not pose as high a risk for physiological problems as it does in early and middle adolescence. A multidisciplinary approach is essential because teen pregnancy is a complex problem.
From Leifer, G. (2008). Maternity nursing (10th ed.). Saunders: Philadelphia.
The Nursing Approach to Adolescents
The nurse must open the lines of communication with adolescents and enable them to feel at ease before initiating care or teaching. A sense of humor is helpful. Providing privacy and ensuring confidentiality and respect are basic to adolescent communication. The nurse must be careful not to behave like an adolescent, because the adolescent may perceive that behavior as “phony.” Adolescent hostility may be evidence of fear of the unknown, and rebellion may be an effort at grasping independence. The nurse should guide the parents concerning the need to listen, understand, and share with adolescents. Helping parents distinguish between normal problems of adolescence and problems that necessitate referral and follow-up is essential. For example, demands for privacy are normal, but overall withdrawal necessitates referral and follow-up care.
Health care teaching should include nutrition, dental care, personal care, body piercing, accident prevention, substance abuse, self-control, risk-taking behavior, money, and time management. Open-ended questions concerning common problems of adolescence may encourage the discussion of a topic that adolescents may not initiate by themselves.
Graduation from high school is self-actualization for the adolescent (Figure 20-13). Getting a job that will provide for self-support or going to college, which may involve leaving home, is the first step of entrance into independent adulthood (Figure 20-14).

Get Ready for the NCLEX® Examination!
Key Points
• Adolescence is defined as the period of life that begins with the appearance of secondary sex characteristics and ends with emotional maturity and the cessation of growth.
• According to Erikson, the major developmental task of adolescence is to establish a sense of identity. Other major tasks of adolescence include separating from family, initiating intimacy, and making career choices.
• Freud considered adolescence as the last stage of psychosexual development. He termed this the genital stage.
• Jean Piaget suggests that the cognitive development during adolescence reflects abstract reasoning and logic. He calls this stage the period of formal operations.
• The physical development seen during this period is distinguished by puberty, the stage at which the reproductive organs become functional and secondary sex characteristics develop.
• Adolescents vary in their rate of physical and social maturation and their ability to resolve conflicts concerning self-esteem and autonomy.
• A nonjudgmental adult role model who can maintain a confidence can help avoid a crisis for the adolescent.
• The Sexuality Information and Education Council of the United States (SIECUS) is an example of a national organization that assists in the development and implementation of sex education programs.
• Some main challenges of the adolescent years include adjusting to rapid physical changes, maintaining privacy, coping with stresses and pressures, maintaining open communication, and developing positive lifestyle choices.
• Peer groups help the adolescent to separate from the family and experiment with social behaviors.
• A clique affords the adolescent the opportunity to “belong” and to develop close personal relationships with others who have similar interests and values.
• The first menstrual period is called menarche.
• The adolescent struggles with the development of a realistic body image.
• Accurate, safe, and timely sex education can help prevent STIs and HIV.
• Adolescence is a time of conflict with parental authority and values. The influence of peers and heterosexual relationships increases.
• Motor vehicle accidents, homicide, and drownings are the leading causes of mortality in this age-group.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• American Academy of Pediatrics: http://aappolicy.aappublications.org/cgi/reprint/pediatrics;108/4/1030.pdf
• Bicycle Helmets: www.aap.org/policy/0103.html
• MTV, It’s Your Sex Life: www.itsyoursexlife.com
• National Family Partnership: http://cmnfp.pictco.org/default.asp
• Parents Without Partners: www.parentswithoutpartners.org
• Sexuality Information and Education Council of the United States (SIECUS): www.siecus.org
• Suicide prevention: www.cdc.gov/ncipc/dvp/Suicide/youthsuicide.htm
Review Questions for the NCLEX® Examination
1. One of the tasks of adolescence as defined by Erikson is:
2. When communicating with an adolescent about safety concerns, which concept of adolescent behavior should be considered?
1. The typical adolescent understands teaching and respects and usually follows the advice of adults.
2. Growth and development are complete in the adolescent, and muscle coordination and skills lessen the risks for injury.
3. Safety concerns at this age mostly focus on sports injuries.
4. Adolescents are risk takers and tend to experiment with potentially dangerous outcomes.
3. Puberty can most accurately be defined as the period of life characterized by the:
1. occurrence of sexual maturity and appearance of secondary sex characteristics.
2. substitution of adult interests and value systems for child interests.
3. most rapid rate of physical and mental growth and development.
4. awakening of sexual feelings and the initiation of sexual experience.
4. A 16-year-old female towers over her companions, which bothers her. She confides in the nurse and says, “I just hate school—everyone is always staring at me.” The nurse’s best response would be:
1. “Don’t pay any attention to it.”
2. “You just don’t know how lucky you are to be tall.”
5. Which action is most important when planning nutrition management for the adolescent?
Critical Thinking Question
1. A high school senior expresses her concern to the nurse about taking her college entrance examination. The examination is given early in the morning, which is when she often feels sleepy and less alert and has trouble concentrating. She states that she usually studies hard the night before an examination and tries to eat a good breakfast on the day of the test. The breakfast usually consists of bacon and eggs, a muffin, and chocolate milk. What is the appropriate response of the nurse?