Nursing Management of Pain During Labor and Birth
1 Define each key term listed.
2 List the common types of classes offered to childbearing families.
3 Describe factors that influence a woman’s comfort during labor.
4 Describe the methods of childbirth preparation.
5 Discuss the advantages and limitations of nonpharmacological methods of pain management during labor.
6 Explain nonpharmacological methods of pain management for labor, including the nursing role for each.
7 Discuss the advantages and limitations of pharmacological methods of pain management.
8 Explain each type of pharmacological pain management, including the nursing role for each.
 , p. 162)
, p. 162) , p. 159)
, p. 159) , p. 165)
, p. 165) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Pregnant women are usually interested in how labor will feel and how they can manage the experience. Preparation for childbirth is important.
Education for Childbearing
Various classes are offered to women during pregnancy by most hospitals and freestanding birth centers to help women adjust to pregnancy, cope with labor, and prepare for life with an infant (Figure 7-1). Women who plan a home birth usually prepare intensely because they want to avoid medications and other interventions associated with hospital births.

FIGURE 7-1 The nurse teaching this prenatal class discusses the movement of the fetus through the pelvis.
Types of Classes Available
Classes during pregnancy focus on topics that contribute to good outcomes for the mother and infant (see Health Promotion box). Special classes prepare other family members for the birth and the new infant. Other classes are sometimes available, including:
 Health Promotion
Health Promotion
Types of Prenatal Classes
Maintaining the woman’s fitness during pregnancy (see Chapter 4)
Variations of Basic Childbirth Preparation Classes
Refresher classes consist of one to three sessions to review the material learned during a previous pregnancy. Ways to help siblings adjust to the new baby and a review of infant feeding are often included.
Cesarean Birth Classes
Classes for women who expect a cesarean birth help the woman and her support person to understand the reasons for this method of delivery and anticipate what is likely to occur during and after surgery.
Vaginal Birth after Cesarean Classes
Women in vaginal birth after cesarean (VBAC) classes may need to express unresolved feelings about their previous cesarean birth. Depending on the reason for the cesarean delivery, they may be more anxious about the forthcoming labor.
Adolescent Childbirth Preparation Classes
A pregnant adolescent’s needs are different from those of an adult. Adolescents are therefore usually uncomfortable in regular childbirth preparation classes. They are often single mothers and have a more immature perception of birth and child rearing. Some are not old enough to drive or do not have access to a car. They cannot attend classes that target working adults. The content of classes for adolescents is tailored to their special needs. Because acceptance by their peer group is important to adolescents, the girls are a significant source of support for each other. Classes may be held in the school setting. Expectant fathers may be included.
Basic Content of All Childbirth Preparation Classes
Regardless of the specific method taught, most classes are similar in basic content (see the Health Promotion box). Many of the techniques covered can also be used to help the unprepared woman during labor. The woman who learns about the changes produced by pregnancy and childbirth is less likely to respond with fear and tension during labor. Information about cesarean birth is usually included.
Benefits of Exercise
Conditioning exercises such as the pelvic rock, tailor sitting, and shoulder circling prepare the woman’s muscles for the demands of birth (see Chapter 4). These exercises also relieve the back discomfort common during late pregnancy.
Pain Control Methods for Labor
The woman and her partner learn a variety of techniques that may be used during labor as needed (Figure 7-2). These are some examples:

FIGURE 7-2 The partner massages the foot of the pregnant woman. Massage can provide an effective technique for pain relief during labor (see also Chapter 34).
• Skin stimulation, such as effleurage (see Figure 7-3)

FIGURE 7-3 Effleurage. This woman is practicing effleurage, stroking the abdomen with the fingertips in a circular motion. This technique stimulates large-diameter nerve fibers, thus interfering with pain transmission. Fingertip pressure should be firm enough to prevent creating a tickling sensation.
These techniques are most effective if learned before labor begins. See Box 7-1 for selected nonpharmacological pain relief techniques.
Childbirth and Pain
Pain is an unpleasant and distressing symptom that is personal and subjective. No one can feel another’s pain, but empathic nursing care helps to alleviate pain and helps the woman cope with it.
How Childbirth Pain Differs from Other Pain
Several factors distinguish childbirth pain from other types of pain:
• It is part of a normal birth process.
• The woman has several months to prepare for pain management.
Pain is usually a symptom of injury or illness, yet pain during labor is an almost universal part of the normal process of birth. Although excessive pain is detrimental to the labor process, pain also can be beneficial. It may cause a woman to feel vulnerable and seek shelter and help from others. Pain often motivates her to assume different body positions, which can facilitate the normal descent of the fetus. Birth pain lasts for hours, as opposed to days or weeks. Labor ends with the birth of an infant, followed by a rapid and nearly total cessation of pain.
Factors That Influence Labor Pain
Several factors lead to pain during labor and influence the amount of pain a woman experiences. Other factors influence a woman’s response to labor pain and her ability to tolerate it.
Pain Threshold and Pain Tolerance
Two terms are often used interchangeably to describe pain, although they have different meanings. Pain threshold, also called pain perception, is the least amount of sensation that a person perceives as painful. Pain threshold is fairly constant, and it varies little under different conditions. Pain tolerance is the amount of pain one is willing to endure. Unlike the pain threshold, one’s pain tolerance can change under different conditions. A primary nursing responsibility is to modify as many factors as possible so that the woman can tolerate the pain of labor.
Physical Factors That Modify Pain
Several physical factors influence the amount of pain a woman feels or is willing to tolerate during labor.
Central Nervous System Factors:
Gate control theory: The gate control theory explains how pain impulses reach the brain for interpretation. It supports several nonpharmacological methods of pain control. According to this theory, pain is transmitted through small-diameter nerve fibers. However, the stimulation of large-diameter nerve fibers temporarily interferes with the conduction of impulses through small-diameter fibers. Techniques to stimulate large-diameter fibers and “close the gate” to painful impulses include massage, palm and fingertip pressure, and heat and cold applications.
 Nursing Tip
Nursing TipEndorphins: Endorphins are natural body substances similar to morphine. Endorphin levels increase during pregnancy and reach a peak during labor. Endorphins may explain why women in labor often need smaller doses of an analgesic or anesthetic than might be expected in a similarly painful experience.
Maternal Condition
Cervical Readiness: The mother’s cervix normally undergoes prelabor changes that facilitate effacement and dilation in labor (see Chapter 6). If her cervix does not make these changes (ripening), more contractions are needed to cause effacement and dilation.
Pelvis: The size and shape of the pelvis significantly influences how readily the fetus can descend through it. Pelvic abnormalities can result in a longer labor and greater maternal fatigue. In addition, the fetus may remain in an abnormal presentation or position, which interferes with the mechanisms of labor.
Labor Intensity: The woman who has a short, intense labor often experiences more pain than the woman whose birth process is more gradual. Contractions are intense and frequent, and their onset may be sudden. The cervix, vagina, and perineum stretch more abruptly than during a gentler labor. Contractions come so fast that the woman cannot recover from one before another begins. In addition, a rapid labor limits the woman’s choices for pharmacological pain control.
Fetal Presentation and Position
The fetal presenting part acts as a wedge to efface and dilate the cervix as each contraction pushes it downward. The fetal head is a smooth, rounded wedge that most effectively causes effacement and dilation of the round cervix. The fetus in an abnormal presentation or position applies uneven pressure to the cervix, resulting in less effective effacement and dilation and thus prolonging the labor and delivery process.
The fetus usually turns during early labor so that the occiput is in the front left or right quadrant of the mother’s pelvis (occiput anterior positions) (see Figures 6-7 and 6-8). If the fetal occiput is in a posterior pelvic quadrant, each contraction pushes it against the mother’s sacrum, resulting in persistent and poorly relieved back pain (back labor). Labor is often longer with this fetal position.
Interventions of Caregivers
Although they are intended to promote maternal and fetal safety, several common interventions may add to pain during labor. These are some examples:
Psychosocial Factors That Modify Pain
Several psychosocial variables alter the pain a woman experiences during labor. Many of these variables interrelate with one another and with physical factors.
Culture influences how a woman feels about pregnancy and birth and how she reacts to pain during childbirth. See Table 6-1 for selected traditional cultural practices during labor and delivery.
Nonpharmacological Childbirth Preparation and Pain Management
Nonpharmacological pain control methods are important, even if the woman receives medication or an anesthetic. Most pharmacological methods cannot be instituted until labor is well-established because they tend to slow the progress of labor. Nonpharmacological methods help the woman to cope with labor before it has advanced far enough for her to be given medication. In addition, most medications for labor do not eliminate pain, and the woman will need nonpharmacological methods to manage the discomfort that remains. Nonpharmacological methods are usually the only realistic option if the woman comes to the hospital in advanced labor.
Advantages
There are several advantages to nonpharmacological methods if pain control is adequate. Poorly relieved pain increases fear and anxiety, thus diverting blood flow from the uterus and impairing the normal labor process. It also reduces the pleasure of this extraordinary experience. Nonpharmacological methods do not harm the mother or fetus. They do not slow labor if they provide adequate pain control. They carry no risk for allergy or adverse drug effects.
Limitations
For best results, nonpharmacological measures should be rehearsed before labor begins. They can be taught to the unprepared woman, preferably during early labor, when she is anxious enough to be interested yet comfortable enough to learn. The nurse may help the woman use several key techniques of nonpharmacological pain control during labor. If the woman and her partner attended childbirth preparation classes, the nurse builds on their knowledge during labor (Box 7-1).
Childbirth Preparation Methods
Most childbirth preparation classes are based on one of several methods. The basic method is often modified to meet the specific needs of the women who attend.
Dick-Read Method: Grantly Dick-Read was an English physician who introduced the concept of a fear-tension-pain cycle during labor. He believed that fear of childbirth contributed to tension, which resulted in pain. His methods include education and relaxation techniques to interrupt the cycle.
Bradley Method: The Bradley method was originally called “husband-coached childbirth” and was the first to include the father as an integral part of labor. It emphasizes slow abdominal breathing and relaxation techniques.
Lamaze Method: The Lamaze method, also called the psychoprophylactic method, is the basis of most childbirth preparation classes in the United States. It uses mental techniques that condition the woman to respond to contractions with relaxation rather than tension. Other mental and breathing techniques occupy her mind and limit the brain’s ability to interpret labor sensations as painful. The Lamaze breathing technique should be no slower than half of the woman’s baseline respiratory rate and no faster than twice the baseline rate.
Nonpharmacological Techniques
Relaxation Techniques: The ability to release tension is a vital part of the expectant mother’s “tool kit.” Relaxation techniques require concentration, thus occupying the mind while reducing muscle tension. Promoting relaxation is basic to all other methods of pain management and birth preparation, both nonpharmacological and pharmacological. The nurse should adjust the woman’s environment and help her with general comfort measures as discussed in Chapter 6. For example, water in a tub or shower helps to refresh her and promotes relaxation.
To reduce anxiety and fear, the woman is oriented to the labor area, any procedures that are done, and what is happening in her body during the normal process of birth. A partnership style of nurse-patient–labor partner is usual in maternity settings.
Looking for signs of muscle tension and teaching her partner to do so helps the woman who is not aware of becoming tense. She can change position or guide her partner to massage the area where muscle tension is noted. The laboring woman is guided to release the tension specifically, one muscle group at a time, by saying, for example, “Let your arm relax; let the tension out of your neck … your shoulders. …” Specific instructions are repeated until she relaxes each body part.
The woman should change methods at intervals because constant use of a single technique reduces its effectiveness (habituation).
Skin Stimulation: Several variations of massage are often used during labor. Most can be taught to the woman and partner who did not attend childbirth preparation classes.
Effleurage: Effleurage is a technique that stimulates the large-diameter nerve fibers that inhibit painful stimuli traveling through the small-diameter fibers. The woman strokes her abdomen in a circular movement during contractions (Figure 7-3 and Chapter 34). If fetal monitor belts are on her abdomen, she can massage between them or on her thigh, or she can trace circles or a figure eight on the bed. She can use one hand when on her side.
Sacral pressure: Firm pressure against the lower back helps relieve some of the pain of back labor. The woman should tell her partner where to apply the pressure and how much pressure is helpful (Figure 7-4).

FIGURE 7-4 Sacral pressure. The partner applies firm pressure on the lower back of the woman in labor. Using a tennis ball enhances the effect (see also Chapter 34).
Thermal stimulation: Heat can be applied with a warm blanket or a glove filled with warm water. Warmth can also be applied in the form of a shower if there is no contraindication to doing so. Most women appreciate a cool cloth on the face. Two or three moistened washcloths are kept at hand and changed as they become warm.
Positioning: Frequent changing of position relieves muscle fatigue and strain. In addition, position changes can promote the normal mechanisms of labor.
Diversion and Distraction: Several methods may be used to stimulate the woman’s brain, thus limiting her ability to perceive sensations as painful. All these methods direct her mind away from the pain.
Focal point: The woman fixes her eyes on a picture, an object, or simply a particular spot in the room. Some women prefer to close their eyes during contractions and focus on an internal focal point.
Imagery: The woman learns to create a tranquil mental environment by imagining that she is in a place of relaxation and peace. Preferred mental scenes often involve warmth and sunlight, although some women imagine themselves in a cool environment. During labor the woman can imagine her cervix opening and allowing the infant to come out, as a flower opens from bud to full bloom. The nurse can help to create a tranquil mental image, even in the unprepared woman (see Chapter 34).
Breathing: Like other techniques, breathing techniques are most effective if practiced before labor. The woman should not use them until she needs them, generally when she can no longer walk or talk through a contraction. She may become tired if she uses them too early or if she moves to a more advanced technique sooner than she must. If the woman has not had childbirth preparation classes, each technique is taught as she needs it.
Each breathing pattern begins and ends with a cleansing breath, which is a deep inspiration and expiration, similar to a deep sigh. The cleansing breaths help the woman to relax and focus on relaxing.
Slow-paced breathing: The woman begins with a technique of slow-paced breathing. She starts the pattern with a cleansing breath, then breathes slowly, as during sleep (Figure 7-5, A). A cleansing breath ends the contraction. An exact rate is not important, but about six to nine breaths a minute is average. The rate should be at least half her usual rate to ensure adequate fetal oxygenation and prevent hyperventilation.
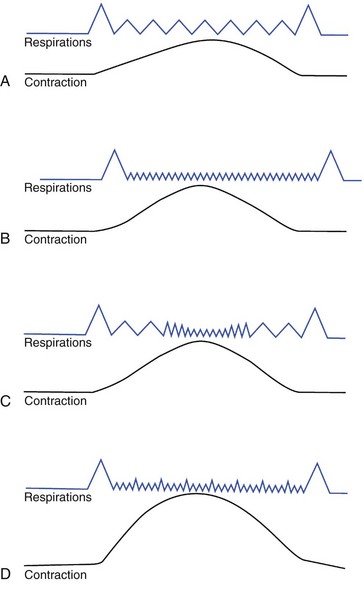
FIGURE 7-5 Breathing patterns. A, Slow-paced breathing. The pattern starts with a cleansing breath as the contraction begins. The woman breathes slowly, at about half her usual rate, and ends with a second cleansing breath at the end of the contraction. B, As labor intensifies, the woman may need to use modified paced breathing. The pattern begins and ends with a cleansing breath. After the opening cleansing breath, the woman breathes rapidly during the contraction, no faster than twice her usual respiratory rate, and makes the closing cleansing breath as the contraction subsides. C, In this variation of modified paced breathing, the woman begins with slow-paced breathing at the beginning of the contraction, switching to faster breathing during its peak. A cleansing breath also begins and ends this pattern. D, Patterned paced breathing begins and ends with a cleansing breath. During the contraction the woman emphasizes the exhalation of some breaths. She may use a specific pattern or may randomly emphasize the blow.
Modified paced breathing: This pattern begins and ends with a cleansing breath. During the contraction the woman breathes more rapidly and shallowly (see Figure 7-5, B and C). The rate should be no more than twice her usual rate. She may combine slow-paced with modified paced breathing. In this variation she begins with a cleansing breath and breathes slowly until the peak of the contraction, when she begins rapid, shallow breathing. As the contraction abates, she resumes slow, deep breathing and ends with a cleansing breath. Hyperventilation is sometimes a problem when the woman is breathing rapidly. She may complain of dizziness, tingling, and numbness around her mouth and may have spasms of her fingers and feet. Box 7-2 lists measures to combat hyperventilation.
Patterned paced breathing: The technique of patterned paced breathing is more difficult to teach the unprepared laboring woman because it requires her to focus on the pattern of her breathing. It begins with a cleansing breath, which is followed by rapid breaths punctuated with an intermittent slight blow (see Figure 7-5, D), often called pant-blow, or “hee hoo” breathing. The woman may maintain a constant number of breaths before the blow or may vary the number in a specific pattern, as follows:
• Constant pattern: Pant-pant-pant-blow, pant-pant-pant-blow, and so on.
• Stairstep pattern: Pant-blow, pant-pant-blow, pant-pant-pant-blow, pant-pant-pant-pant-blow
In another variation her partner calls out random numbers to indicate the number of pants to take before a blow. If she feels an urge to push before her cervix is fully dilated, the woman is taught to blow in short breaths to avoid bearing down. Pushing before full cervical dilation may cause cervical edema or lacerations, especially with a woman’s first child, because the cervix is not as stretchable as it is after one or more births.
The Nurse’s Role in Nonpharmacological Techniques: When a woman is admitted, the nurse determines whether she had childbirth preparation classes and works with what the woman and her partner learned. The nurse helps them to identify signs of tension so the woman can be guided to release it.
If the woman did not have childbirth preparation classes, the nurse teaches simple breathing and relaxation techniques. If the woman is extremely anxious and out of control, she will not be able to comprehend verbal instructions. It may be necessary to make close eye contact with her and to breathe with her through each contraction until she can regain control.
The nurse minimizes environmental irritants as much as possible. The lights should be lowered and the woman kept reasonably dry by regularly changing the underpads on the bed. The temperature should be adjusted; the nurse provides a warm blanket if that offers the most comfort. (See Chapter 6 for other general comfort measures during labor.)
The nurse should be cautious not to overestimate or underestimate the amount of pain a woman is experiencing. The quiet, stoic woman may need analgesia yet be reluctant to ask. A tense body posture or facial grimacing may indicate that she needs additional pain relief measures.
Pharmacological Pain Management
Pharmacological pain management methods include analgesics, adjunctive drugs to improve the effectiveness of analgesics or to counteract their side effects, and anesthetics. Analgesics are systemic drugs (affecting the entire body) that reduce pain without loss of consciousness. Anesthetics cause a loss of sensation, especially of pain. Regional anesthetics block sensation from a localized area without causing a loss of consciousness. General anesthetics are systemic drugs that cause a loss of consciousness and sensation of pain. Tables 7-1 and 7-2 summarize intrapartum analgesics, adjunctive drugs, and methods of anesthesia.
Anesthetics are administered by various clinicians depending on the type of drug. Local anesthetics are given by the physician or the nurse-midwife at the time of birth. Other anesthetics may be given by a specialist in anesthetic administration.
There are two types of anesthesia clinicians:
1. An anesthesiologist: a physician who specializes in giving anesthesia
2. A certified registered nurse anesthetist (CRNA): a registered nurse who has advanced training in anesthetic administration. State licensing laws and individual facility policies affect which methods of anesthesia each clinician may use.
Physiology of Pregnancy and Its Relationship to Analgesia and Anesthesia
Specific factors in the physiology of pregnancy affect the pregnant woman’s response to analgesia and anesthesia:
• The pregnant woman is at a higher risk for hypoxia caused by the pressure of the enlarging uterus on the diaphragm.
• The sluggish gastrointestinal tract of the pregnant woman can result in increased risk for vomiting and aspiration.
• Aortocaval compression (pressure on the abdominal aorta by the heavy uterus when the woman is in supine position) increases the risk of hypotension and the development of shock.
Advantages
Methods that use drugs for reducing pain during birth can help the woman to be a more active participant in birth. They help her relax and work with contractions. Drugs do not usually relieve all pain and pressure sensations.
The pain of labor may cause a “stress response” in the mother that results in an increase in autonomic activity, a release of catecholamines, and a decrease in platelet perfusion. This stress response results in fetal acidosis. The pain can also cause maternal hyperventilation and lead to respiratory alkalosis, and then a compensating metabolic acidosis. Metabolic acidosis in the woman results in further fetal acidosis. Therefore appropriate pain relief during labor can play an important role in the positive outcome of pregnancy for mother and infant.
Limitations
Pharmacological methods are effective, but they do have limitations. One important factor to consider is that two persons are medicated—the mother and her fetus. Any drug given to the mother can affect the fetus, and the effects may be prolonged in the infant after birth. The drug may directly affect the fetus, or it may indirectly affect the fetus because of effects in the mother (such as hypotension).
Several pharmacological methods may slow labor’s progress if used early in labor. Some complications during pregnancy limit the pharmacological methods that are safe. For example, a method that requires the infusion of large amounts of intravenous (IV) fluids might overload the woman’s circulation if she has heart disease. If she takes other medications (legal or illicit), they may interact adversely with the drugs used to relieve labor pain.
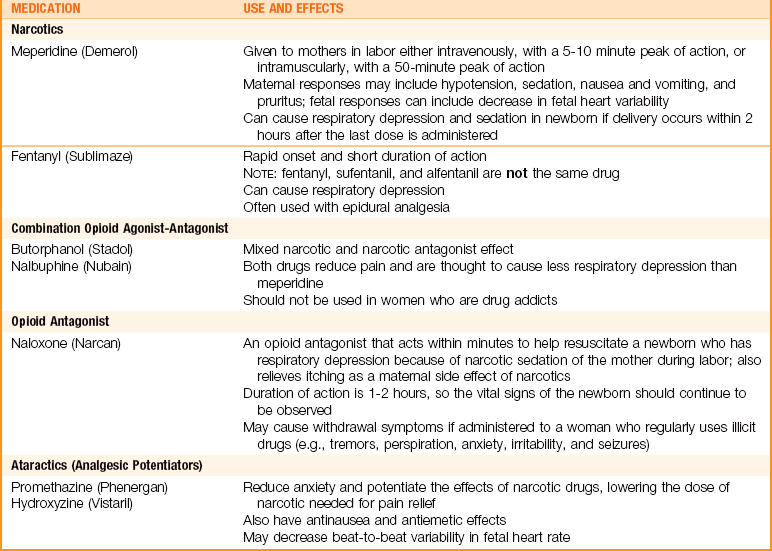
Analgesics and Adjunctive Drugs
Narcotic (Opioid) Analgesics: Systemic opioids are the most common means of labor analgesia in the United States. They are used in small doses to avoid causing fetal respiratory depression. Opioids do not provide complete pain relief during labor, but they do help the woman cope with a tolerable level of intermittent labor pains. Drugs used are listed in Table 7-1.
In general, use of narcotic analgesics is avoided if birth is expected within an hour. An attempt is made to time administration so the drug does not reach its peak at the time of birth. However, small doses are sometimes given in late labor if the fetus has no problems. The nurse must be prepared to support the respiratory efforts of all infants at birth, regardless of whether the mother received narcotics during labor.
Narcotic Antagonist: Naloxone (Narcan) is used to reverse respiratory depression, usually in the infant, caused by opioid drugs such as meperidine. It is not effective against respiratory depression from other causes, such as intrauterine hypoxia. It can be given by the IV route, or it may be given through the endotracheal tube during resuscitation. IV naloxone can be given to the neonate immediately after birth via the umbilical cord vein. The use of naloxone in a woman who is drug dependent can cause withdrawal syndrome in the mother or the neonate.
Regional Analgesics and Anesthetics
The membranes around the spinal cord are called the meninges. The meninges have three layers:
The epidural space is located between the dura mater and the inside bony covering of the brain or spinal cord. The subdural space is located between the dura mater and the arachnoid mater, and the subarachnoid space is located between the arachnoid mater and the pia mater. Regional anesthesia in obstetrics usually involves the placement of an anesthetic in the epidural or the subarachnoid space (see Figure 7-7).
An analgesic blocks pain, whereas an anesthetic blocks both pain and motor responses. For example, an epidural block may provide analgesia and allow the woman to ambulate with assistance, but spinal anesthesia prevents ambulation. The role of the nurse in caring for a woman with regional analgesia or anesthesia is to monitor her responses and the status of the fetus. Starting or managing intermittent dosages of a regional anesthetic is not within the nursing scope of practice for a licensed practical or vocational nurse (LPN/LVN).
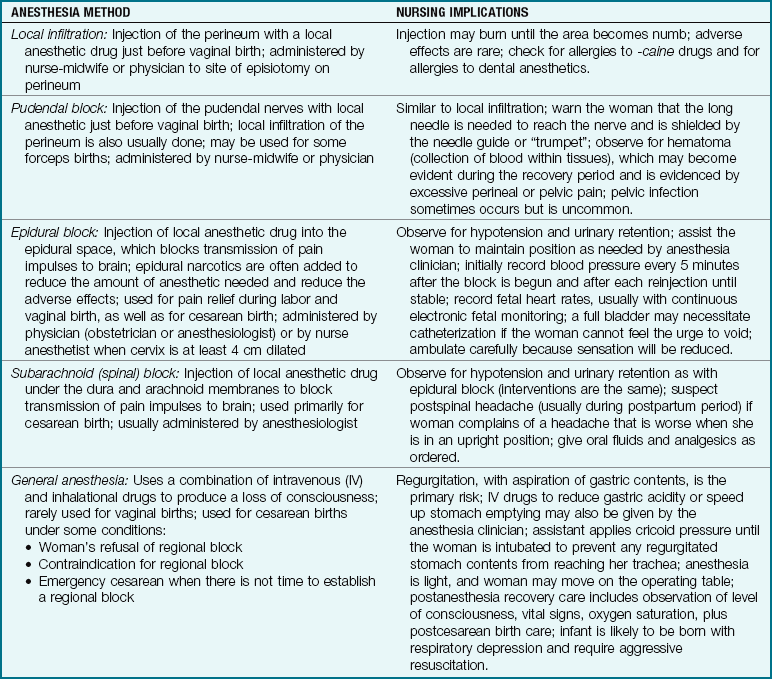
Regional anesthetics block sensation to varying degrees, depending on the type of regional block used, the quantity of medication, and the drugs injected. The woman still feels pressure and may feel some pain. The major advantage of regional anesthetics is that they provide satisfactory pain relief yet allow the woman to be awake and participate in the birthing process (Table 7-2).
Local and pudendal blocks are given in the vaginal-perineal area. Epidural and subarachnoid blocks and intrathecal narcotics are given by injecting anesthetic drugs so they bathe the nerves as they emerge from the spinal cord. The spinal cord and nerves are not directly injected.
Local anesthetic agents for childbirth are related to those used for dental work. On admission, the nurse should ask each woman if she is allergic to or has had problems with dental anesthesia. If so, her physician or nurse-midwife should be alerted so she can have the safest pain relief measures.
Local Infiltration: Injection of the perineal area for an episiotomy is done just before birth, when the fetal head is visible. It may also be done after placental expulsion to repair a perineal laceration. There is a short delay between injection of the anesthetic agent and the loss of pain sensation. The physician or nurse-midwife allows the anesthetic to become effective before beginning the episiotomy. There are virtually no risks if the woman is not allergic to the drug.
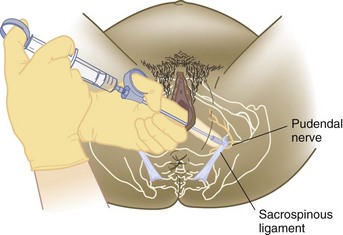
Pudendal Block: The pudendal block is used for vaginal births, although its use has become less common as the popularity of the epidural block has increased. It provides adequate anesthesia for an episiotomy and for most low forceps births. It does not block pain from contractions and, like local infiltration, is given just before birth. There is a delay of a few minutes between injection of the drug and the onset of numbness (paresthesia).
The physician or nurse-midwife injects the pudendal nerves on each side of the mother’s pelvis (Figure 7-6). The nerves may be reached through the vagina or by injection directly through her perineum. A long needle (13 to 15 cm [5 to 6 inches]) is needed to reach the pudendal nerves, which are near the mother’s ischial spines. If the injection is done through the vagina, a needle guide (“trumpet”) is used to protect the mother’s tissues. The needle is injected only about 1.3 cm (0.5 inch) into the woman’s tissues. The perineum is also infiltrated because the pudendal block alone does not completely anesthetize the perineum.
Epidural Block: The epidural space is a small space just outside the dura (outermost membrane covering the brain and spinal cord). The woman is in a sitting or side-lying position for the epidural block. Her back is relatively straight, rather than sharply curved forward, to avoid compressing the tiny epidural space, which is about 1 mm (the thickness of a dime).
The physician or nurse anesthetist penetrates the epidural space with a large needle (16- to 18-gauge). A fine catheter is threaded into the epidural space through the bore of the needle (Figure 7-7). A test dose (2 to 3 mL) of local anesthetic agent is injected through the catheter. The woman is not expected to have effects from the test dose if the catheter is in the right place. Numbness or loss of movement after the small test dose indicates that her dura mater was probably punctured and the drug was injected into the subarachnoid space (as in a subarachnoid block) rather than in the epidural space. Numbness around the mouth, ringing in the ears (tinnitus), visual disturbances, or jitteriness are symptoms that suggest injection into a vein. The test dose is small enough to prevent long-term adverse effects.
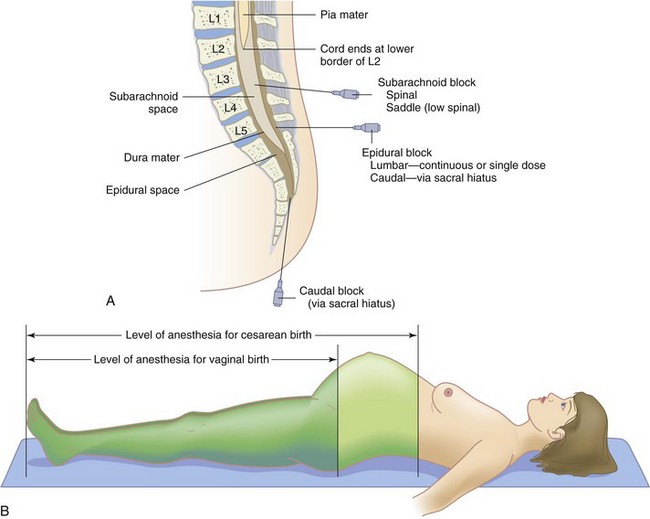
FIGURE 7-7 Epidural and spinal anesthesia. A, The insertion sites for the needle in epidural, subarachnoid, and spinal blocks. B, Levels of anesthesia for vaginal birth compared with minimum level required for cesarean birth.
If the test dose is normal (no effects), a larger amount of anesthetic agent is injected to begin the block. A few minutes are needed before the onset of the block. If an epidural block is being used for surgery, such as cesarean delivery or tubal ligation, the anesthesiologist or CRNA will test for the level of numbness before surgery begins.
Local anesthetic drugs are usually combined with a small dose of an opioid analgesic such as fentanyl (Sublimaze). The combination of drugs allows quicker and longer-lasting pain relief with less anesthetic agent and minimal loss of movement. An epidural block for labor is more accurately termed analgesia (reducing pain) than anesthesia (obliterating all sensation).
The woman can sometimes ambulate when a combination-drug epidural is used because the local anesthetic dose is much lower. She can assume any position with this type of block, although any pregnant woman should avoid the supine position.
To maintain pain relief during labor, the anesthetic drug is constantly infused into the catheter via an infusion pump. Alternatively, intermittently repeated injections of the drug may be given.
Dural puncture: The dura lies just below the tiny epidural space. This membrane is sometimes punctured accidentally (“wet tap”) with the epidural needle or the catheter that is inserted through it. If a dural puncture occurs, a relatively large amount of spinal fluid can leak from the hole, which may result in a headache.
Limitations of epidural block: Although it is a popular method of intrapartum pain relief, an epidural block is not used if the woman has any of the following:
Adverse effects of epidural block: The most common side effects are maternal hypotension and urinary retention. To counteract hypotension, which can compromise fetal oxygenation, a large quantity (500 mL to 1000 mL or more) of IV solution such as Ringer’s lactate is infused rapidly before the block is begun. The large quantity of IV fluids combined with reduced sensation may result in urinary retention. The nurse should palpate the suprapubic area for a full bladder every 2 hours or more often if a large quantity of IV solution was given. The woman will need catheterization if she is unable to void.
The woman may feel less of an urge to push in the second stage of labor when she has an epidural block, depending on the drugs used for her block. Therefore this stage may be longer if a woman has an epidural block. Maternal and fetal conditions are monitored closely.
Subarachnoid (Spinal) Block: The woman’s position for a subarachnoid block is similar to that for the epidural block except that her back is curled around her uterus in a C shape. The dura is punctured with a thin (25- to 27-gauge) spinal needle. A few drops of spinal fluid confirm entry into the subarachnoid space (see Figure 7-7). The local anesthetic drug is then injected. A much smaller quantity of the drug is needed to achieve anesthesia using the subarachnoid block than with the epidural block. Anesthesia occurs quickly and is more profound than the epidural block. The woman loses all movement and sensation below the block.
The subarachnoid block is a “one-shot” block because it does not involve placing a catheter for reinjection of the drug. It is not often used for vaginal births today but remains common for cesarean births. Its limitations are essentially the same as for an epidural block.
Adverse effects of subarachnoid block: Hypotension and urinary retention are the main adverse effects of subarachnoid block, as with the epidural block. They are managed as in the epidural block. Hypotension is often more severe with a subarachnoid block.
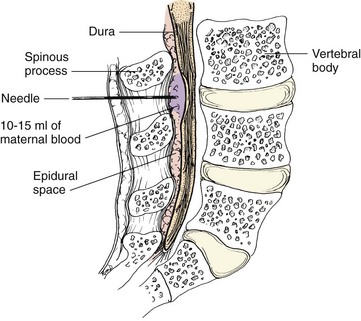
A postspinal headache sometimes occurs, most likely because of spinal fluid loss. The woman may be advised to remain flat for several hours after the block to decrease the chance of postspinal headache. However, there is no absolute evidence that this precaution is effective. Postspinal headache is worse when the woman is upright and often disappears entirely when she lies down. Bed rest, analgesics, and oral and IV fluids help to relieve the headache. A blood patch, done by the nurse anesthetist or anesthesiologist, may provide dramatic relief from postspinal headache. The woman’s blood (10 mL to 15 mL) is withdrawn from her vein and injected into the epidural space in the area of the subarachnoid puncture (Figure 7-8). The blood clots and forms a gelatinous seal that stops spinal fluid leakage. The clot later breaks down and is resorbed by the body.
General Anesthesia
General anesthesia is rarely used for vaginal births or for most cesarean births. Regional blocks are preferred for cesarean births, if possible. General anesthesia may be necessary in the following circumstances:
• Emergency cesarean birth, when there is not time to establish either an epidural or a subarachnoid block
• Cesarean birth in the woman who refuses or has a contraindication to epidural or subarachnoid block
Combinations of general anesthetic drugs (balanced anesthesia) allow for a quick onset of anesthesia, minimal fetal effects, and prompt maternal wakening once the drug is stopped.
Adverse Effects in the Mother: The major risk of general anesthesia is the same during birth as at any other time: regurgitation with aspiration (breathing in) of the acidic stomach contents. This results in a chemical injury to the lungs, aspiration pneumonitis, which can be fatal. Many women begin labor with a full stomach, and their gastric action slows during labor. In addition, the full uterus exerts upward pressure against the stomach. Therefore every pregnant woman is presumed to have a full stomach for purposes of anesthesia.
Adverse Effects in the Neonate: Respiratory depression is the main neonatal risk because drugs given to the mother may cross the placenta. To reduce this risk, the time from induction of anesthesia to clamping of the umbilical cord is kept as short as possible. The woman is prepped and draped for surgery, and all personnel are scrubbed, gowned, and gloved before anesthesia begins. In addition, the anesthesia is kept as light as possible until the cord is clamped. Aggressive resuscitation of the newborn may be necessary.
The Nurse’s Role in Pharmacological Techniques
The nurse’s responsibility in pharmacological pain management begins at admission (Nursing Care Plan 7-1). The woman should be closely questioned about allergies to foods, drugs (including dental anesthetics), and latex to identify pain relief measures that may not be advisable. She should be questioned about her preferences for pain relief. Factors that may have an impact on the choice of pain relief should be noted, such as a history of back surgery, infection in the area where an epidural block would be injected, or blood pressure abnormalities.
7-1  Nursing Care Plan
Nursing Care Plan
The Woman Needing Pain Management During Labor
A woman, para 1, gravida 2, is in active labor and is 4 cm dilated. She is thrashing in bed and is not cooperating with the coaching of her partner.
Risk for injury related to loss of sensation
| Goals | Nursing Interventions | Rationales |
| The woman will not have an injury, such as a muscle strain or fall, while her epidural block is in effect. The fetus will not be born in an uncontrolled delivery. | Check for movement, sensation, and leg strength before ambulating; ambulate cautiously with an assistant. Assist the woman to change positions regularly. | A fall is more likely if the woman does not have sensation and control over her movements. A change of position prevents muscle strain. |
| Observe for signs that birth may be near: increase in bloody show, perineal bulging, and/or crowning. | Loss of sensation varies among women having an epidural block. Labor may progress more rapidly than expected. These are signs associated with imminent birth that should be evaluated by the experienced nurse, the nurse-midwife, or the physician. |
1. A woman, para 1, gravida 2, is in active labor. The last examination revealed that her cervix was 7 cm dilated and 75% effaced. She states that her contraction pains are almost unbearable, even with the medication she has received. Because getting up and walking helped her earlier and she needs to go to the bathroom now, she asks the nurse to help her out of bed to walk to the nearby bathroom. What would be the best response of the nurse?
The nurse keeps the side rails up if the woman takes pain relief drugs. Narcotics may cause drowsiness or dizziness. Regional anesthetics reduce sensation and movement to varying degrees, and therefore the woman may have less control over her body. Side rails on the bed may be necessary for safety.
The nurse reinforces the explanations given by the anesthesia clinician regarding procedures and the expected effects of the selected pain management method. Women often receive these explanations when they are very uncomfortable and do not remember everything they were told. The woman is helped to assume and hold the position for the epidural or subarachnoid block. The nurse tells the anesthesia clinician if the woman has a contraction because it might prevent her from holding still. The anesthetic drug is usually injected between contractions.
The woman is observed for hypotension if an epidural or subarachnoid block is given. Hospital protocols vary, but blood pressure is usually measured every 5 minutes after the block begins (and with each reinjection) until her blood pressure is stable. An automatic blood pressure monitor is often used. Some facilities add a pulse oximeter to monitor oxygen saturation. At the same time the nurse observes the fetal monitor for signs associated with fetal compromise (see Chapter 5), because maternal hypotension can reduce placental blood flow.
The epidural block is given during labor and may reduce the mother’s sensation of rectal pressure. The nurse coaches her about the right time to start and stop pushing with each contraction if needed. The nurse also observes for signs of imminent birth, such as increased bloody show and perineal bulging, because the woman may not be able to feel the sensations clearly.
Nursing responsibilities related to general anesthesia include assessment and documentation of oral intake and administration of medications to reduce gastric acidity. The woman should be told that all preparations for surgery will be performed before she is put to sleep. The nurse should reassure her that she will be asleep before any incision is made. Having a familiar nurse in the operating room full of new people is reassuring to the woman before surgery.
The woman who has received a general anesthetic is usually awake enough to move from the operating table to her bed after surgery. Her respiratory status is observed every 15 minutes for 1 to 2 hours. A pulse oximeter provides constant information about her blood oxygen level. She is given oxygen by face mask or other means until she is fully awake. Her uterine fundus and vaginal bleeding are observed as for any other postpartum woman. Her urine output from the indwelling catheter should be observed for quantity and color at least hourly for 4 hours. The nurse should ambulate the woman cautiously and with assistance to prevent potential falling.
 Safety Alert!
Safety Alert!
The following are important admission assessments related to pharmacological pain management: last oral intake (time and type), adverse reactions to drugs (especially dental anesthetics), other medications taken, and any food allergies or latex allergy.
If the woman receives narcotic drugs, the nurse observes her respiratory rate for depression. Because respiratory depression is more likely to occur in the neonate than in the mother, the neonate is closely observed after birth. Narcotic effects in the infant may persist longer than in an adult. The nurse has naloxone on hand in case it is needed to reverse respiratory depression in the mother or neonate.
The nurse observes the woman for late-appearing respiratory depression and excessive sedation if she received epidural narcotics after cesarean birth. This may occur up to 24 hours after administration, depending on the drug given. The woman’s vital signs are monitored hourly, and a pulse oximeter may be applied. Facilities often use a scale to assess for sedation so all caregivers use the same criteria for assessment and documentation. Additional analgesics are given cautiously and strictly as ordered. If mild analgesics do not relieve the pain, the health care provider is contacted for additional orders.
Get Ready for the NCLEX® Examination!
Key Points
• Pain during childbirth is different from other types of pain because it is part of a normal process that results in the birth of an infant. The woman has time to prepare for it, and the pain is self-limiting.
• A woman’s pain threshold is fairly constant. Her pain tolerance varies, and nursing actions can increase her ability to tolerate pain. Irritants can reduce her pain tolerance.
• The pain of labor is caused by cervical dilation and effacement, uterine ischemia, and stretching of the vagina and perineum.
• Poorly relieved pain can be detrimental to the labor process.
• Childbirth preparation classes give the woman and her partner pain management tools they can use during labor. Some tools, such as breathing techniques and effleurage, can also be taught to the unprepared woman.
• The nurse should do everything possible to promote relaxation during labor because it enhances the effectiveness of all other pain management methods, both nonpharmacological and pharmacological.
• Any drug taken by the expectant mother may cross the placenta and affect the fetus. Effects may persist in the infant much longer than in an adult.
• The use of narcotic antagonist drugs for women who have a drug dependency can cause withdrawal syndrome in the mother or the neonate.
• Observe the mother and infant for respiratory depression if the mother received opioids, including epidural narcotics, during the intrapartum period.
• Regional anesthetics are the most common for birth because they allow the mother to remain awake, including for cesarean birth.
• Closely question the woman about drug allergies when she is admitted. Because drugs used for regional anesthesia are related to those used in dentistry, ask her about reactions to dental anesthetics.
• Observe the mother’s blood pressure and the fetal heart rate after epidural or spinal block to identify hypotension or fetal compromise. Urinary retention is also more likely.
Additional Learning Resources

Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Association of Women’s Health, Obstetric and Neonatal Nurses: www.awhonn.org
• Pain relief during birth: www.acog.org/publications/patient_education/bp086.cfm
Review Questions for the NCLEX® Examination
1. What is the narcotic drug of choice for pain relief during labor when the cervix is less than 4 cm dilated?
2. Which technique is likely to be most effective for “back labor”?
1. Stimulating the abdomen by effleurage
2. Applying firm pressure in the sacral area
3. Blowing out in short breaths during each contraction
4. Rocking from side to side at the peak of each contraction
3. What drug should be immediately available for emergency use when a woman receives narcotics during labor?
4. Choose the most important nursing assessment immediately after a woman receives an epidural block:
5. Spinal headache after epidural anesthesia may be relieved by: