The Toddler
1 Define each key term listed.
2 Describe the physical, psychosocial, and cognitive development of children from 1 to 3 years of age, listing age-specific events and guidance when appropriate.
3 Discuss speech development in the toddler.
4 Describe the task to be mastered by the toddler according to Erikson’s stages of growth and development.
5 List two developmental tasks of the toddler period.
6 Discuss the principles of guidance and discipline for a toddler.
7 Discuss how adults can assist small children in combating their fears.
8 Identify the principles of toilet training (bowel and bladder) that will help guide parents’ efforts to provide toilet independence.
9 Describe the nutritional needs and self-feeding abilities of a toddler.
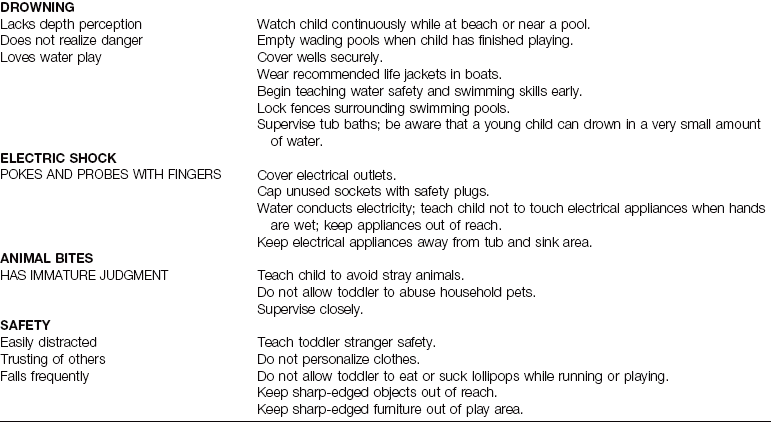
10 List two methods of preventing the following: automobile accidents, burns, falls, suffocation and choking, poisoning, drowning, electric shock, and animal bites.
11 Describe the characteristic play and appropriate toys for a toddler.
 http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
General Characteristics
Children between 1 and 3 years of age are referred to as toddlers. They are able to get about by using their own powers and are no longer completely dependent persons. By 1 year of age, they have generally tripled their birth weight and gained control of their head, hands, and feet. The remarkably rapid growth and development that took place during infancy begins to slow down. The toddler period presents different challenges for the parents and the child.
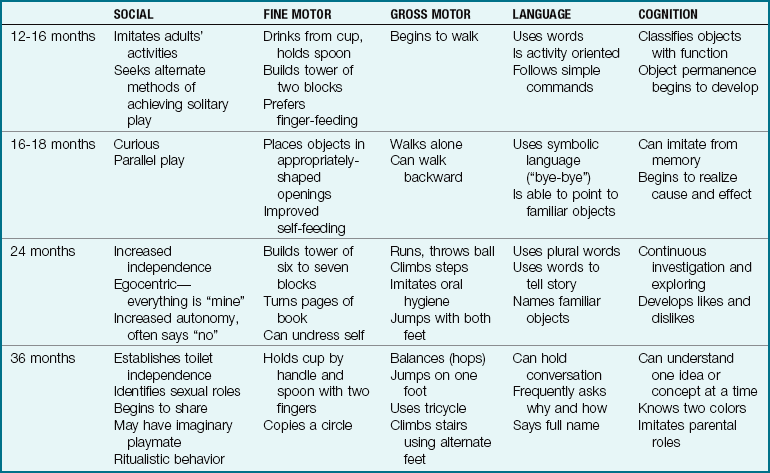
The toddler is in Erikson’s stage of autonomy versus shame and doubt, which is based on a continuum of trust established during infancy (see Chapter 15). Along with the toddler’s increasing independence and curiosity to explore the widening environment come many challenging tasks to be mastered, including toilet training, self-feeding, self-dressing, and speech development. One major parental responsibility is to maintain safety while allowing the toddler the opportunity for social and physical independence. Another major parental responsibility is to maintain a positive self-image and body image in the child whose behavior is inconsistent and often frustrating. Toddlers alternate between dependence and independence. They test their power by saying “no” frequently. This is called negativism. Offering limited choices and making use of distraction can be helpful strategies in handling toddlers (too many choices can cause confusion). Developing self-control and socially acceptable outlets for aggression and anger are important factors in the formation of personality and behavior. Ritualism is another characteristic of toddler behavior. Toddlers increase their sense of security by making compulsive routines of simple tasks, and therefore their rituals should be respected. Table 17-1 summarizes the toddler’s physical development, social behavior, and abilities at various ages.
Physical Development
The toddler’s body changes proportions (Figure 17-1). The legs and arms lengthen through ossification and growth in the epiphyseal areas of the long bones. The trunk and head grow more slowly. The toddler gains 1.8 to 2.7 kg (4 to 6 lb) per year. The birth weight has quadrupled by 2.5 years of age. The toddler grows 10 cm (4 inches) per year in height. The height of a 2-year-old is thought to be one half of the potential adult height of that child. The height and weight are plotted carefully on a growth chart during each clinic visit to reflect what should be a steady pace of growth and development (see Figure 15-3).
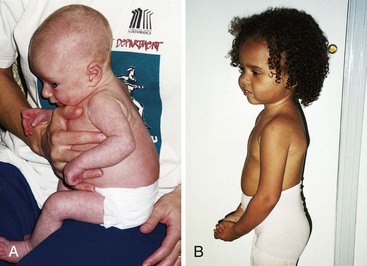
FIGURE 17-1 Change in body contour. A, The back of the infant is rounded. B, In the toddler, the exaggerated lumbar lordosis makes the abdomen protrude.
The rate of brain growth decelerates. The increase in head circumference during infancy is 10 cm (4 inches), whereas during the second year of life it is only 2.5 cm (1 inch). Chest circumference continues to increase. After the second year the child appears leaner because the chest circumference begins to exceed the abdominal circumference. The protuberant abdomen flattens when the muscle fibers increase in size and strength.
Myelination of the spinal cord is practically complete by age 2 years, allowing for control of anal and urethral sphincters. Bowel and bladder control is usually complete by 2.5 to 3 years of age.
Respirations are still mainly abdominal but shift to thoracic as the child approaches school age. The toddler is more capable of maintaining a stable body temperature than is the infant. The shivering process, in which the capillaries constrict or dilate in response to body temperature, has matured.
The skin becomes tough as the epidermis and dermis bond more tightly, which protects the child from fluid loss, infection, and irritation. The defense mechanisms of the skin and blood, particularly phagocytosis, work more effectively than they did during infancy. The lymphatic tissues of the adenoids and tonsils enlarge during this period. The eustachian tubes continue to be shorter and straighter than in the adult. Tonsillitis, otitis media, and upper respiratory infections are common problems. Eruption of deciduous teeth continues until completion at about 2.5 years of age (see Figure 15-13).
The blood pressure of a toddler may average 90/56 mm Hg; the respiratory rate slows to 25 breaths/min, and breathing continues to be abdominal. The pulse of a toddler slows to a range of 70 to 110 beats/min. Digestive processes and the volume capacity of the stomach increase to accommodate a three-meal-a-day schedule.
Sensorimotor and Cognitive Development
The senses and motor abilities of the toddler do not function independently of one another. Two-year-old toddlers reach, grasp, inspect, smell, taste, and study objects with their eyes. Their attention becomes centered on characteristics of their surroundings that capture their interest. Binocular vision is well established by age 15 months. Visual acuity is about 20/40 by 2 years of age.
As memory strengthens, toddlers can compare present events with stored knowledge. They assimilate information through trial and error plus repetition. They try alternative methods of accomplishing a goal. Thought processes advance, preparing the way for more complex mental operations. The sensorimotor and preconceptual phase of development described by Piaget develops rapidly between 1 and 3 years of age, and the toddler’s behavior reflects this.
Separation anxiety, which consists of protest, despair, and detachment, develops in infancy and continues throughout toddlerhood. Toddlers are able to tolerate longer periods of separation from parents to explore their environment. They become aware of cause and effect. Often they correlate a type of object with its function. For example, if their toys are stored in a paper bag, they will gleefully open any paper bag they see, expecting to find toys. If the bag contains garbage or drugs, they can be injured or may be punished. This can be confusing to the toddler and frustrating to the parents.
The concept of spatial relationships develops, and toddlers are able to fit square pegs in a square hole and round pegs in a round hole. Toys should be selected to promote this ability. Object permanence continues to develop, and the toddler becomes aware that there may be fun items behind closed doors and in closed drawers. The toddler’s curiosity and ability to explore make it important to educate parents to keep dangerous objects out of their reach. The toddler begins to internalize standards of behavior as evidenced by saying “no-no” when tempted to touch a forbidden object.
The toddler copies the words and the roles of the models seen in the home. The toddler may “help Mommy clean” or “help Daddy shave.” By 2 years of age there is recognition of sexual differences.
Toddlers may confuse essential with nonessential body parts. Expelling feces and flushing them down the toilet can be upsetting to some toddlers because they may feel they expelled a part of themselves that has disappeared. Toddlers’ body image and self-esteem may be impaired if they are scolded in a way that makes them feel they are bad rather than their behavior. The nurse must help the parents develop skills that will enable toddlers to feel they are loved even though the specific behavior is unacceptable.
Speech Development
Language development parallels cognitive growth. The increase in the level of comprehension is particularly striking and exceeds verbalization. By 3 years of age the child has a rather extensive vocabulary of about 900 words. Speech is more than 90% intelligible (Table 17-2). At about the end of the first year, the infant begins to make noises that sound like “bye-bye,” “ma-ma,” and “da-da.” When toddlers see the happy response to these sounds, they repeat them. This is true throughout the toddler period. To want to learn to talk, small children must have an appreciative audience.
Table 17-2
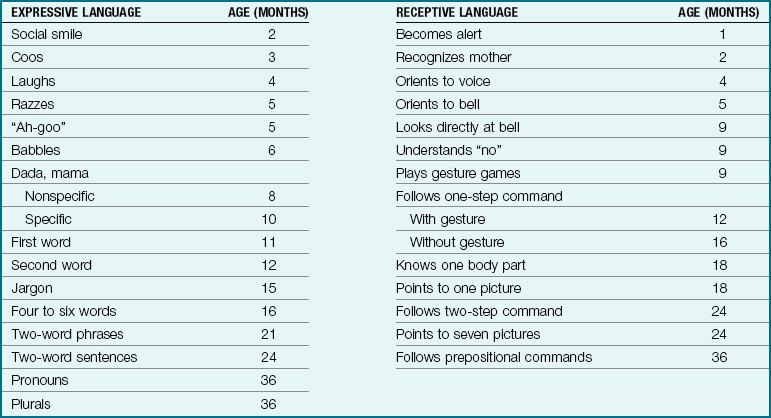
Note: This table of language milestones is a guide to assessing normal language development. Although most mentally handicapped children are language delayed, not all language-delayed children are mentally retarded. Some normal children also are late talkers.
Modified from Montgomery, T. (1994). When not talking is the chief complaint. Contemporary Pediatrics, 11(9), 49.
Children first refer to animals by the sounds the animals make. For example, before saying “dog,” the toddler repeats “bow-bow.” Soon the child can say short phrases such as “Daddy gone car.” Toddlers also respond to tone of voice and facial expression. If an adult sounds threatening, the toddler may answer “no” and then repeat it in a louder voice.
Sometimes adults scold the child merely for being too young to understand what is requested. However, imagine being punished in a foreign country because you could not speak or comprehend the language well enough to defend yourself. Adults who show empathy to the small child can help to minimize their frustrations.
Parents who are concerned about their child’s delayed speech can discuss it with their health care provider during a routine physical examination so it can be evaluated in light of total physical growth and development (Table 17-3). Many late talkers are perfectly normal children who prefer listening over active participation. Lead poisoning and hearing deficits should be ruled out before screening for other developmental problems such as autism (Box 17-1). Many common household items, such as vertical window blinds and decorative metal vases, contain lead. Autism is discussed in Chapter 33.
Table 17-3
When a Child with a Communication Disorder Needs Help
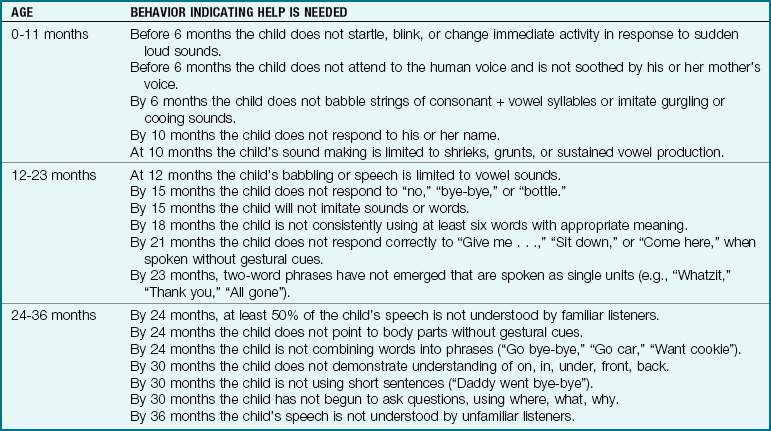
Note: At any age the child is consistently dysfluent (not clear) with repetitions, hesitations, or blocks, or struggles to say words. Struggle may be accompanied by grimaces, eye blinks, or hand gestures.
From Kliegman, R., Marcdante, K., Jenson, H., & Behrman, R. (2005). Nelson’s essentials of pediatrics (5th ed.). Philadelphia: Saunders.
Guidance and Discipline
Discipline for the toddler involves guidance. The goal is to teach, not to punish. Teaching the toddler self-control with positive self-esteem is more desirable than encouraging a completely submissive, “obedient” child. The toddler who scribbles on the wall must be given the opportunity to scribble on paper, a more socially acceptable outlet.
Temper tantrums (uncontrolled anger reactions) often occur during the toddler years, and parent responses reinforce to the child either the desirability or the risks involved with such behavior. Expectations must be commensurate with the child’s physical and cognitive abilities. Toddlers get into many situations that are over their heads. When adults make firm decisions, the problem is resolved, at least for the time being. The child feels secure.
Limit setting should include praise for desired behavior as well as disapproval for undesired behavior. A time-out period in a safe place helps the child to develop the ability to tolerate delayed gratification and self-regulation. Timing should not begin until the child has settled down. The child is praised once calm. Timing for time-out is usually based on 1 minute per year of age.
Children, like adults, seek approval. It is effective and helps to increase their self-confidence. The positive approach should be taken as often as possible. One assumes that the toddler is going to be good rather than bad. “Thank you, Johnny, for giving me the matches” will make them arrive in your hand more quickly than “Give me those matches right now,” said in a threatening tone. The use of fear or physical aggression should not be a part of discipline, because it does not foster self-control and can lead to physical or mental abuse of the child.
Fear is a valuable emotion to the child if it does not become too intense. Unfortunately, many children fear situations that are not in themselves dangerous, and this sometimes deprives them of activities that otherwise would be enjoyable. If the parent warns, “Be careful, don’t fall,” when a toddler begins to ride a tricycle, the toddler may develop a fear of the risk taking that may be involved in experiencing new activities.
The physical and mental health of the child at the time of a fear-provoking experience affects the extent of the reaction. If the child is alone, fear may be greater than if someone such as a parent or nurse is present. Once a fear has been learned, it is more difficult to eliminate. Clinging to favorite possessions and repetitive rituals are self-consoling behaviors for the toddler, particularly at bedtime and during separation from parents.
Stress increases fear of separation. Adults should attempt to control their own fears in the presence of young children. Respect and understanding should always be accorded to children who are afraid. Making fun of the fear or shaming the child in front of others is detrimental to self-esteem.
Many toddlers who independently explore the clinic examining room while waiting to be examined may cling to the parent when the stranger (the health care provider) enters the room and approaches the child. The toddler who does not seek the parent during stressful situations or turns to a stranger for comfort reflects a need for closer evaluation of the parent-child relationship.
The “terrible twos,” during which negativistic behavior is predominant, begin the disciplinary pattern of the family that will carry throughout childhood and affect the child’s personality. Corporal punishment, involving spanking, is accepted in many traditional cultures as the mainstay of discipline. However, regular spanking reflects a desperate effort by the parent to gain control over a toddler who is exercising his or her beginning autonomy (independent functioning) and developing negativism. Potential injury, child abuse, and reciprocal aggressive behavior in the child can be avoided with careful parental guidance concerning alternative techniques of discipline. Time-out, limit setting, clear communication, and frequent rewards and approval for positive behavior are effective noncorporal techniques of discipline.
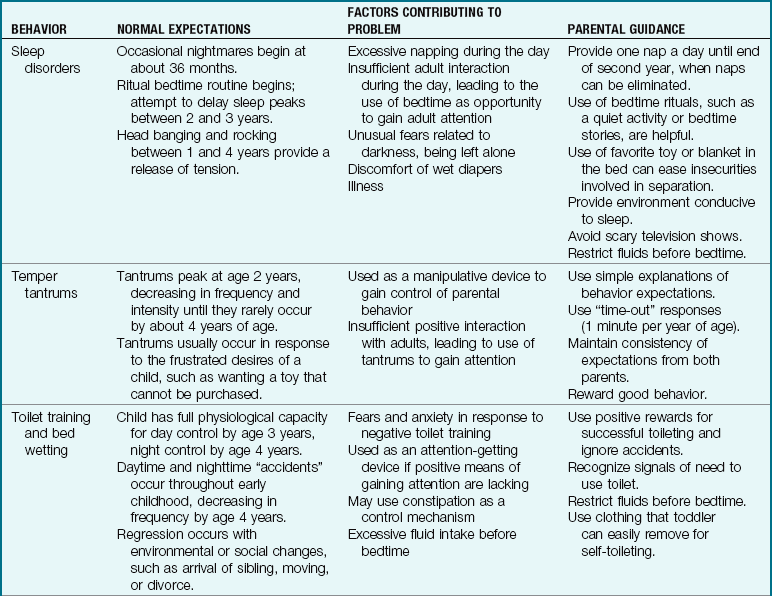
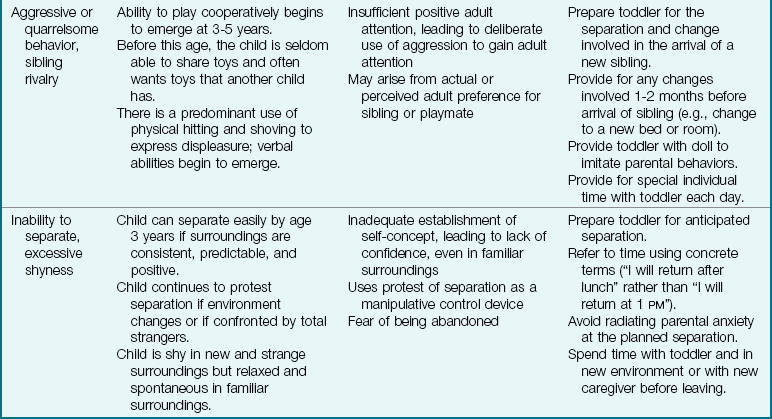
Communicating love and respect to the child with a clear message that it is the behavior, not the child, that is disapproved of by the adult are the keys to effective discipline. Behavior problems that can occur during early childhood are detailed in Table 17-4.
 Nursing Tip
Nursing TipDaily Care
Nutrition, dentition, and oral care are discussed in Chapter 15. When talking to the toddler, the adult should be at eye level with the child so the adult seems less overwhelming. This is of particular importance when the child is in a fear-provoking environment, such as the hospital. A flexible schedule organized around the needs of the entire household is best for the toddler. The toddler needs a consistent routine, but it can differ for special occasions.
The clothing of toddlers should be simple and easy for them to put on and take off. Pants with elastic waists are convenient for them to pull down when they use the toilet. All clothing must be fairly loose to provide freedom of movement for jumping and other strenuous activities. Sunburn protection with clothing or sunscreen is necessary to prevent skin damage.
The toddler wears shoes mainly for protection. They should fit the shape of the foot and be half an inch longer and a quarter of an inch wider than the foot. They must fit securely at the heel. Children should wear their usual shoes at their periodic checkups because these show how the shoes have been worn, which indicates to the health care provider how the children are using their bodies. The toddler may go barefoot whenever it is safe and possible, because this strengthens the foot muscles. Socks must be large enough that they do not flex the toes. The toddler should be taught to pull socks free from the toes before putting on shoes.
Good posture is the result of proper nutrition, plenty of fresh air and exercise, and sufficient rest. The toddler’s mattress must be firm. The chair and play table are adapted to size. In some cases, this can be easily accomplished by placing a rolled-up blanket or pad in the seat of the chair. A small, sturdy stool placed in the bathroom will bring the child to the proper height for brushing the teeth. As in all areas of learning, the child’s posture is greatly influenced by that of other members of the family. The toddler who is happy and is allowed gradually increasing independence develops a sense of security, which is reflected in the posture. Slouching is sometimes seen in children who are insecure and lack self-confidence.
Toilet Independence
There are many approaches to toilet training. Much depends on the temperament of both the individual child and the person guiding the child. Readiness is important. Voluntary control of anal and urethral sphincters begins at about 18 to 24 months. The child’s waking up dry in the morning or from naptime is an indication of maturity. Children must be able to communicate in some fashion that they are wet or need to urinate or defecate. They must be willing to sit on the potty for several minutes at a time.
Toddlers seek approval and like to imitate the actions of parents. They wander into the bathroom and are curious about what is taking place there. If a parent feels that the child will respond to training at this time, the child might first be put in training pants or pull-up diapers. These can be removed quickly and easily, and the child becomes more aware of being wet.
The use of a child’s potty-chair or a device that attaches to an adult toilet seat is a matter of personal preference (Figure 17-2). A potty-chair may make the toddler feel more secure because it is small. It should support the back and arms of the child. The feet should touch the floor. If a potty-chair is not available, the child can be placed on the standard-size toilet, facing the toilet tank. This method may increase feelings of security. The toddler can use a regular toilet with a bench to support the child’s feet.

FIGURE 17-2 Toilet training. Toilet training should be a nonstressful experience for the toddler. Nurses can help parents identify readiness for toilet independence. The nurse assesses the parents’ expectations, family and cultural preferences, and developmental readiness of the child when instructing parents. Sitting on the potty too long without supervision may result in bathroom playtime!
Bowel training is generally attempted first; however, some toddlers become bladder trained during the day because they enjoy listening to the “tinkle” in the potty. If toddlers have bowel movements at the same time each day, they may progress fairly rapidly. They should not be left on the potty-chair for more than a few minutes at a time.
Bladder training is begun when the toddler stays dry for about 2 hours at a time. The parent may discover that the toddler has gone the entire night without wetting. It is then logical to put the child on the potty-chair and to praise success. Bladder training varies widely, particularly during the night. Restricting fluids before bedtime may help. Placing the half-asleep child on the potty-chair accomplishes little.
Most children continue to have occasional accidents until age 4 years. If the toddler has a mishap, parents should accept it matter-of-factly and merely change the clothes. Children benefit when adults show continuous affection to them and accept both bad and good days.
The word that toddlers use to signal defecation or urination should be one that is recognized by others besides the immediate family. Sometimes a parent may forget to inform the baby-sitter or nursery school teacher of the word that the child uses. This causes the toddler unnecessary frustration because those about them cannot understand what they are trying to say.
Toddlers who are toilet trained at home should continue to use the potty in the hospital setting. They may be acutely embarrassed by wetting the bed. Although regression of bowel and bladder training is common during hospitalization, personnel often contribute to it by not taking time to investigate the child’s needs. Nurses regularly consult the child’s nursing care plan to maintain continuity of care as well as promote growth and development of the toddler.
Demands and threats do more damage than good. Life is smoother for all if the parent remains patient and keeps this new adventure pleasant. Training should not be undertaken when the family or child is under stress, such as during illness or a move to a new location.
Nutrition Counseling
Caloric requirements per unit of body weight decline in the toddler from 120 calories/kg per day during infancy to 100 calories/kg per day. Children need an adequate protein intake to cover maintenance needs and to provide for optimum growth. Milk should be limited to no more than 720 mL (24 oz) a day. Too few solid foods can lead to dietary deficiencies of iron. Children between 1 and 3 years of age are high-risk candidates for anemia.
The toddler who is well nourished shows steady proportional gains on height and weight charts and has good bone and tooth development. The diet history should be adequate, avoiding excessive calories and large amounts of vitamins.
The toddler is noted for having a fluctuating appetite with strong food preferences. The nurse reminds parents that any nutritious food can be eaten at any meal; for example, soup for breakfast and cereal for dinner are acceptable. Serving size is important (Table 17-5). Too-large servings are discouraged, because they may overwhelm the child and can lead to overeating problems. One tablespoon of solid food per year of age serves as a measurement guide. A quiet time before meals provides an opportunity for the child to “wind down.” The toddler’s refusal to eat may result from fatigue or not being particularly hungry. The toddler may eat one food with vigor one week and refuse it the next. A flexible schedule designed to meet the needs of the toddler and the rest of the family must be worked out by the individual family. Forcing toddlers to eat only creates further difficulties. They are quick to sense parents’ frustration and may use mealtime to obtain attention by behaving poorly and refusing to eat. Discipline and arguments during mealtime only upset everyone’s digestion.
Table 17-5
Approximate Serving Sizes per Meal
| AGE 1 YEAR | AGE 2-3 YEARS | |
| Bread | 1 slice | 1 slice |
| Cereal | 1 oz | 1 oz |
| Rice or pasta | 1 cup | 1 cup |
| Vegetables | 2 tablespoons | 3 tablespoons |
| Fruit | 1 cup | 1 cup |
| Milk | 1 cup | 1 cup |
| Meat, beans | 2 tablespoons | 3 tablespoons |
Note: Approximate serving sizes per meal for a toddler. For food pyramid, see Figure 15-6.
Toddlers are fond of ritual. This is often seen at mealtime. They want a particular dish, glass, and bib. It is best to go along with their wishes as long as they do not become too pronounced. It gives them a sense of security and, in the long run, saves time and energy for the adult.
Toddlers have a brief attention span. They may try to stand in the high chair or wander away from the table. They may be excused if they have eaten a fair amount of the meal; otherwise distraction of some type is necessary. Toddlers who regularly feed themselves may enjoy being helped by mommy or daddy. Some restaurants that cater to families provide crayons and special place mats to keep the small child occupied until adults finish their dinners. In the hospital the toddler who is fed in a high chair wears an appropriate safety restraint, and the nurse remains with the child.
The toddler’s food is chopped into fine pieces. Various foods are offered, and one should try to plan contrasts of colors and textures. A 2-year-old likes finger foods. Foods are served at moderate temperatures. Candy, cake, and soda between meals are to be avoided. (See Chapter 15 for a food guide.)
Children like colorful dishes, which must be made of an unbreakable substance. Washable plastic bibs, placemats, and protection for the floor around the high chair are advisable. Eating utensils should be small enough that they can be handled easily. Seating equipment should be adjusted so the child is comfortable and maintains good posture.
Day Care
Family life has changed dramatically since the 1970s. Today many more children are cared for in community settings outside of the home. In the last decade, the fastest-growing group of persons in the labor force has been women with infants. Not only were more mothers working, but they were also returning to the work force sooner after the child was born. It was clear that alternative methods of child care were necessary. These arrangements must meet families’ personal preferences, cultural perspectives, and financial and special needs. Parents must take an active role in ensuring high-quality care. Nurses need to be resource persons and family advocates, because finding adequate day care can be stressful.
The decision to place a toddler in the care of others while parents work can be difficult and produce feelings of guilt in the parent. The concept of such care is not new. Many cultures have some type of arrangement, for example the Israelis, who have traditionally placed toddlers in day care while working on a “kibbutz.” The hours of care extend from early morning to the dinnertime hour. Successful alternative child care arrangements depend on specific guidelines in selecting the facility (see Chapter 18), frequent visits to the facility, and close communication and conferences with the staff in the facility. Day care for the toddler differs somewhat from what is appropriate for the preschool child because of the toddler’s shorter attention span, the tendency to engage in parallel play rather than group play, and the need for closer supervision to maintain safety (Figure 17-3).

FIGURE 17-3 Beginning social skills, parallel play, and short attention spans of toddlers require them to have close supervision in day care settings.
There are various types of child care. Many children today can be cared for by relatives, friends, neighbors, or those who have advertised such services. However, there is little research on these types of home arrangements and few standards of quality control. Most licensed day care centers are private businesses run for profit. They are subject to state regulations about physical layout, number of children per caretaker, education of personnel, and other factors. Parents must plan ahead for times when the child is sick and unable to attend. A few innovative programs for the in-home care of sick children have been developed. Employer-supported child care is a rapidly growing area, and these programs are very diverse. Some companies provide family day care (care of the child in the provider’s home). Other employers assist parents through reimbursement, referral programs, or support of existing child care programs in the community.
For low- and some middle-income families, the cost of child care is difficult if not impossible to maintain. Some form of continued or expanded government assistance or private funding is necessary. Inspection and monitoring of child care facilities to ensure compliance with health (physical and mental) and safety standards are paramount. Ideally, all day care programs would include comprehensive health services and health education programs. Criteria for selecting a day care center are similar to those discussed for nursery schools (see Chapter 18).
Injury Prevention
Accidents kill and cripple more children than any disease known and are the leading cause of death in childhood. The best prevention is knowledge of age-appropriate risks and anticipatory guidelines. If parents understand their child’s activities at certain ages, they can prevent many serious injuries by taking necessary precautions (see Health Promotion box).
 Health Promotion
Health Promotion
How to Prevent Hazards Caused by the Behavioral Characteristics of Toddlers
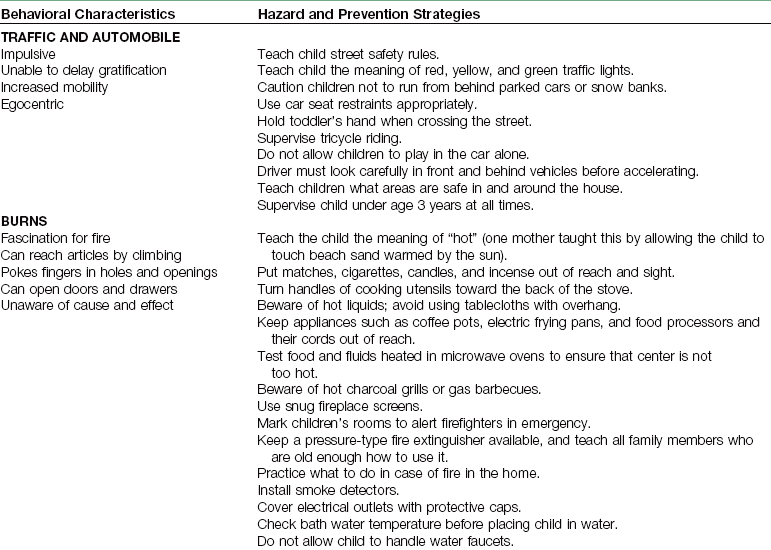
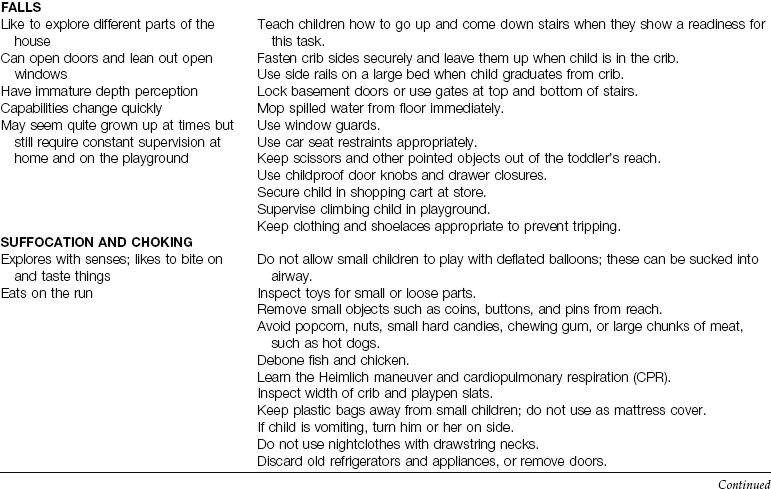
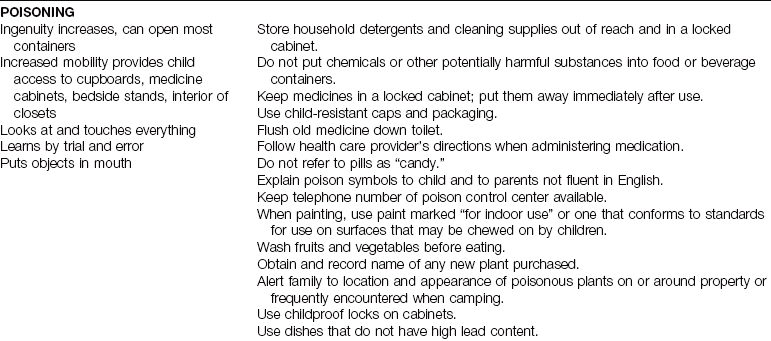
Note: Keep first aid chart and emergency numbers handy. Know location of and how to get to nearest emergency facility.
Nurses have an important responsibility to review injury prevention with parents during each clinic visit. The normal behavior characteristics of a toddler, including curiosity, mobility, and negativity, make the toddler prone to injuries, which often occur in and around the home (Figure 17-4).

FIGURE 17-4 The playful toddler needs close supervision during water play. Falling into a kiddie pool can result in serious injury.
Car safety is important. The use of seat belts is effective if they are worn properly. A shoulder strap that extends across the neck or a lap belt that fits high on the abdomen or waist area can be harmful rather then helpful. A child seat placed in the front car seat close to the passenger air bag can be dangerous.
Nurses demonstrate safety measures to their patients and their families. This is most effectively done by good example. Safety measures pertinent to the pediatric unit are discussed in Chapter 22. Nurses in the community can often contribute indirectly to the welfare of others by the example they set and by being aware of emergency medical facilities available in the community.
Consumer Education
The federal government and concerned private agencies have attempted to regulate some of the variables that cause injuries. A few examples are ensuring the use of nonflammable material for children’s sleepwear, mandating childproof caps on medicine bottles and certain household products, and establishing maximum temperatures for home hot-water heaters. Smoke detectors in homes and public places are commonplace. The United States Consumer Product Safety Commission has established regulations for crib slats, locks, and latches and crib mattress size and thickness. Safety warnings on the crib’s carton advise buyers to use a snug mattress only. The nurse should reinforce this type of information.
Laws have been passed in virtually all states that require infants and small children to be restrained while riding in automobiles (Figure 17-5). These restraints must follow standards established by the Federal Motor Vehicle Safety Department and follow American Academy of Pediatrics (AAP) guidelines. Rental car companies also lend child seat restraints to their customers. The use of car seats begins with the first ride home from the hospital. Once a child is large enough for a car safety belt to fit correctly (usually above 36.3 kg [80 lb] and above 142.5 cm [57 inches] tall), a shoulder and lap system belt is ideal. Incorrectly used safety belts can cause injury to a child (Biagioli, 2005).

FIGURE 17-5 A, The infant’s car seat faces the rear of the car to prevent the infant’s large and heavy head from falling forward when the car stops suddenly or in case of an accident. The driver can look through the rearview mirror of the car toward a mirror mounted on the rear window or the seat back to see the face of the infant in a rear-facing car seat. Note that the metal clip or lock of the car seat belt is not under the chin of the infant, but rests firmly on the chest. B, The toddler’s car seat can be front-facing in the center of the rear seat of the car and secured by the car’s seat belt. The infant’s car seat remains rear-facing behind the driver.
New homes are required to have smoke and carbon monoxide detectors when they are built. Consumers who live in older homes and apartment complexes are also encouraged to install them. Various other safety codes are mandatory for public buildings, with additional measures required for buildings specifically for the disabled. Nevertheless the problems of surveillance and upkeep are considerable. Many children live in substandard housing with little supervision. The education of parents is of monumental importance in decreasing death and disability.
Toys and Play
In 1970 the Child Protection and Toy Safety Act was passed in an effort to halt the distribution of unsafe toys. In addition, parents must be taught to routinely inspect toys for damage and to buy toys suitable for the age, skills, and abilities of the individual child. Some labels now give safety information and intended user age. In general, notification of recall for a specific toy is announced on radio and television and is published in newspapers and consumer journals.
Toy boxes and toy chests are another potential hazard. The most serious injuries caused by a box or chest are the result of the lid falling on a child or a child being trapped inside. A parent can report a product hazard by writing to the United States Consumer Product Safety Commission, Washington, DC, 20207.
Play is the work of a toddler. Through play, toddlers learn how to manipulate and understand their environment, socialize, and explore their world. High-priced toys are not necessary. Pots and pans from the kitchen, supervised water play, dancing to music, and crayons or finger paint and paper are preferred by toddlers. A picture book reviewed while on the lap of a family member can often be enjoyed over and over again. Tricycles can be adapted to the size and ability of the toddler. Objects that can be pushed or pulled are preferred to wind-up toys for this age-group. The sense of touch can be stimulated by providing materials such as fur, sandpaper, felt, and nylon. Colors can be taught while having the toddler help to sort the laundry. Memory can be stimulated by pointing to familiar pictures in a book, newspaper, or magazine. Counting can be taught while climbing stairs. Supervision and maintenance of safety are the keys to a positive play experience for the toddler. Particular attention should be given whenever a pet is part of the environment (Figure 17-6).

FIGURE 17-6 Close supervision is necessary when a child plays in any home where there is a pet, whether large or small. Both the toddler and the pet have unpredictable behavior.
As toddlers become aware of their expanding environment, their social development takes form. Egocentric thinking, in which children relate everything to themselves, predominates. They engage in parallel play, playing next to, but not with, their peers. They gradually develop cooperative play, which involves imagination and sharing skills.
Nurses must closely assess children with special needs for safety precautions. Caregivers of children with disabilities require extended instruction according to the child’s particular needs; these children include those with visual, motor, or intellectual impairments, convulsive disorders, or diabetes mellitus. Immobile children must be protected from sunburn and wind or rainy weather. Adults must also guard these children from mosquitoes and other disease vectors. Injury prevention involves some of the methods mentioned in the discussion of consumer education: the use of items such as electric outlet covers, cabinet locks, and drawer locks and the creation of a hazard-free or “childproof” environment for the child (Figure 17-7).

Get Ready for the NCLEX® Examination!
Key Points
• The birth weight has quadrupled by age 2.5 years.
• Physical changes of the toddler include the acquisition of fine and gross motor skills, among which is increased mobility and increased eye-hand coordination.
• The digestive volume and processes of the toddler increase to accommodate a three-meal-a-day schedule.
• Complete bowel and bladder control is usually achieved by age 2.5 to 3 years.
• Erikson refers to the toddler stage as one in which the child’s task is to acquire a sense of autonomy (self-control) while overcoming shame and doubt.
• The most evident cognitive achievements of the toddler involve language and comprehension.
• Some important self-regulatory functions mastered by the toddler include toilet independence, self-feeding, tolerating delayed gratification, separation from parents, and perfecting newfound physical skills and speech.
• Separation anxiety includes the stages of protest, despair, and detachment.
• Parental guidance is needed to deal with the negativism, temper tantrums, and sibling rivalry that is characteristic of this age-group.
• Discipline for the toddler should be designed to teach rather than punish.
• Some methods of dealing with the inconsistencies of the toddler include distraction, reward and praise, and time-out in a safe place.
• Accidents and poisoning are the leading causes of death in the toddler age-group.
• Infants and young children should ride in a car safety seat for all car trips.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Alliance for Children and Families: www.alliance1.org
• American Academy of Family Physicians: www.aafp.org
• Car Safety Seats: Information for Families: www.aap.org/family/Carseatguide.htm
• Resources for toddler development: www.zerotothree.org
Review Questions for the NCLEX® Examination
1. A parent states she is having a conflict with her toddler who seems to “always want to do things his way.” He insists on putting on his right sock and shoe before his left and has a tantrum if the parent tries to put on the left sock and shoe first. The parent asks the nurse why the child is acting this way. The best response of the nurse would be to:
1. explain to the child it really doesn’t make a difference which sock and shoe is donned first.
2. put the child in a “time-out” for the appropriate time.
3. explain that this is normal ritualistic behavior at this age and should be respected.
2. The nurse assesses the vital signs of a 2-year-old. A normal respiratory rate (per minute) would be:
3. Which statement by the parent would indicate a need for further guidance?
1. I use a car seat for my toddler whenever we are in the car, and he is right beside me as I drive so I can keep an eye on him.
2. I use a car seat for my toddler whenever we are in the car and secure it onto the rear seat of the car.
3. I use a car seat for my toddler that is designed to hold children up to 40 lb.
4. I use a car seat for my toddler that is designed to fasten with the seat belt.
4. A mother tells the nurse that her 2-year-old toddler often has temper tantrums at the family dinner table and asks how to handle the behavior. The best response of the nurse would be:
1. temper tantrums are normal for a 2-year-old, and the child will grow out of it.
2. the toddler should be removed from the family dinner table until he or she is old enough to behave.
3. strict discipline and corporal punishment are appropriate to help the child to gain self-control.
4. parents should agree on a method of discipline, such as time-out, and use it when the child misbehaves.
5. One of the developmental hallmarks of the toddler that most gives rise to safety hazards is:
Critical Thinking Question
1. The parents of a toddler discuss safety in the home with the nurse. The parents state they will use a car seat as required by law and safety gates on the stairs to prevent accidental falls. However, they believe no other safety “childproofing” is necessary, because their child is a good child and they plan to teach him to be obedient so he will learn what not to touch. What is the best response of the nurse?