The Preschool Child
1 Define each key term listed.
2 List the major developmental tasks of the preschool-age child.
3 Describe the physical, psychosocial, and spiritual development of children from age 3 to 5 years, listing age-specific events and guidance when appropriate.
4 Discuss the development of positive bedtime habits.
5 Discuss one method of introducing the concept of death to a preschool child.
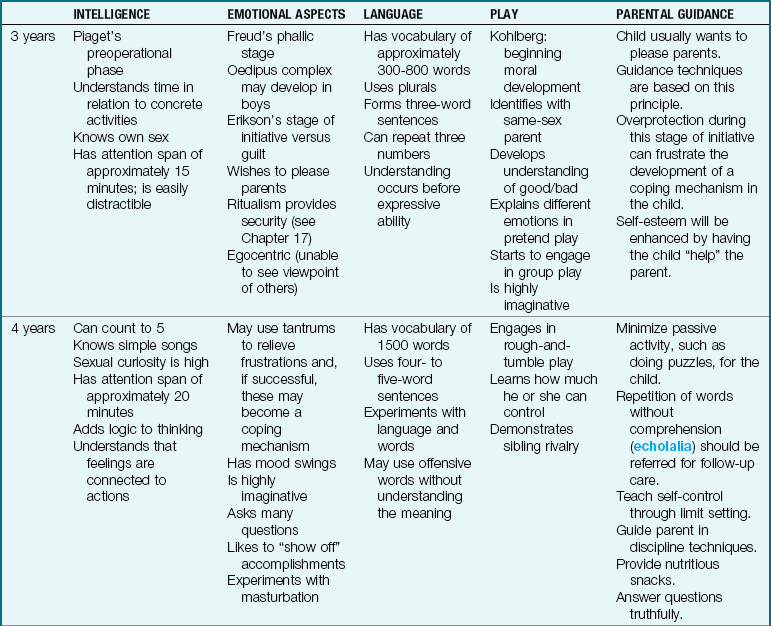
6 Describe the development of the preschool child in relation to Piaget’s, Erikson’s, and Kohlberg’s theories of development.
7 Discuss the characteristics of a good preschool.
8 Discuss the value of play in the life of a preschool child.
9 Designate two toys suitable for the preschool child, and provide the rationale for each choice.
10 Describe the speech development of the preschool child.
11 Discuss the value of the following: time-out periods, consistency, role modeling, and rewards.
12 Discuss the approach to problems such as enuresis, thumb sucking, and sexual curiosity in the preschool child.
13 Describe the developmental characteristics that predispose the preschool child to certain accidents, and suggest methods of prevention for each type of accident.
14 Explain the use of therapeutic play with a handicapped child.
 , p. 422)
, p. 422) , p. 428)
, p. 428) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
General Characteristics
The child from age 3 to 5 years is often referred to as the preschool child. This period is marked by slowing of the physical growth process and mastery and refinement of the motor, social, and cognitive abilities that will enable the child to be successful in his or her school years.
The major tasks of the preschool child include preparation to enter school, development of a cooperative type of play, control of body functions, acceptance of separation, and increase in communication skills, memory, and attention span.
Physical Development
The infant who tripled his or her birth weight at 1 year has only doubled the 1-year weight by 5 years of age. For instance, the infant who weighs 9 kg (20 lb) on the first birthday will probably weigh about 18 kg (40 lb) by the fifth birthday. The child between 3 and 6 years of age grows taller and loses the chubbiness seen during the toddler period. Between 3 and 5 years of age, there will be an increase of 7.6 cm (3 inches) in height, mostly in the legs, that contributes to the development of an erect, slender appearance. Visual acuity is 20/40 at 3 years of age and 20/30 at 4 years of age. The achievement of 20/20 vision may be accomplished by school age. All 20 primary teeth have erupted. Hand preference develops by 3 years of age, and efforts to change a left-handed child to a right-handed child can cause a high level of frustration. Appetite fluctuates widely. The normal pulse rate is 90 to 110 beats/min. The rate of respirations during relaxation is about 20 breaths/min. The systolic blood pressure is about 85 to 90 mm Hg, and the diastolic blood pressure is about 60 mm Hg.
Preschool children have good control of their muscles and participate in vigorous play; they become more adept at using already familiar skills as each year passes. They can swing and jump higher. Their gait resembles that of an adult. They are quicker and have more self-confidence than they did as toddlers.
Cognitive Development
The thinking of the preschool child is unique. Piaget calls this period the preoperational phase. It comprises children from 2 to 7 years of age and is divided into two stages: the preconceptual stage (2 to 4 years of age) and the intuitive thought stage (4 to 7 years of age). Of importance in the preconceptual stage is the increasing development of language and symbolic functioning. Symbolic functioning is seen in the play of children who pretend that an empty box is a fort; they create a mental image to stand for something that is not there.
Another characteristic of this period is egocentrism, a type of thinking in which children have difficulty seeing any point of view other than their own. Because children’s knowledge and understanding are restricted to their own limited experiences, misconceptions arise. One misconception is animism. This is a tendency to attribute life to inanimate objects. Another is artificialism, the idea that the world and everything in it is created by people.
The intuitive stage is one of prelogical thinking. Experience and logic are based on outside appearance (the child does not understand that a wide glass and a tall glass can both contain 4 oz of juice). A distinctive characteristic of intuitive thinking is centering, the tendency to concentrate on a single outstanding characteristic of an object while excluding its other features.
More mature conceptual awareness is established with time and experience. This process is highly complex, and the implications for practical application are numerous. Interested students are encouraged to explore these concepts through further study. Table 18-1 summarizes some major theories of personality development for the preschooler.
Effects of Cultural Practices
Cultural practices can influence the development of a sense of initiative in families who practice authoritarian types of parenting styles that put a great value on obedience and conformity. Parents and older siblings are models for language development, and the mastery of sounds proceeds in the same order around the world. Some parents speak both English and a native language in the home. Studies have shown that young children adapt quickly to a bilingual environment and cultural practices (Figure 18-1). Cultural preferences related to dietary practices are discussed in Chapter 15.

Language Development
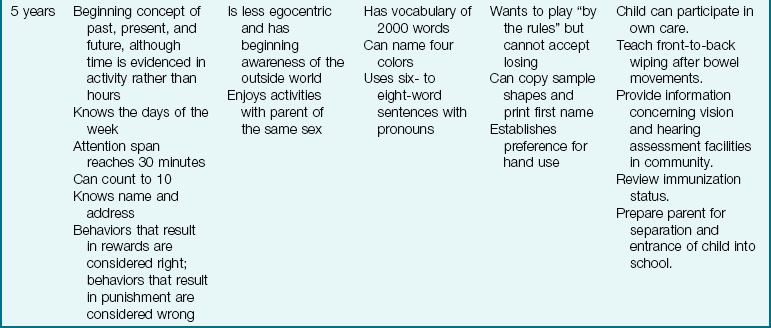
The development of language as a communication skill is essential for success in school (Figure 18-2). Delays or problems in language expression can be caused by physiological, psychological, or environmental stressors. Typically, in the preschool period between 2 and 5 years of age, the number of words in the child’s sentence should equal the child’s age (e.g., two words at 2 years of age). By  years of age, most children evidence possessiveness (my doll). By 4 years of age they can use the past tense, and by 5 years of age they can use the future tense. The development of language skills includes both the understanding of language and the expressing of oneself in language. Children who have difficulty expressing themselves in words often exhibit tantrums and other acting-out behaviors.
years of age, most children evidence possessiveness (my doll). By 4 years of age they can use the past tense, and by 5 years of age they can use the future tense. The development of language skills includes both the understanding of language and the expressing of oneself in language. Children who have difficulty expressing themselves in words often exhibit tantrums and other acting-out behaviors.
FIGURE 18-2 Grandpa reads to the children. Preschool language development depends on exposure to the written word and picture familiarity. In interactive reading the child is asked questions about the pictures she sees and receives immediate feedback. It is the ideal way to optimize the mastery of language.
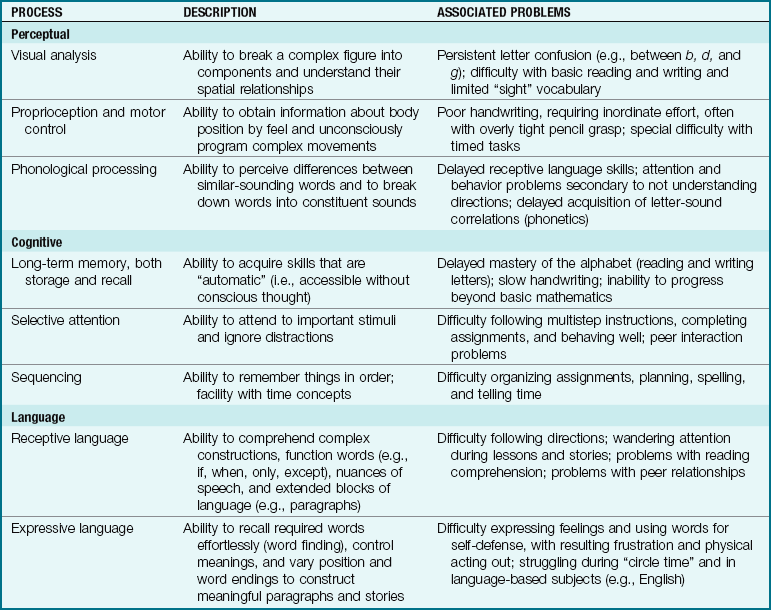
Table 18-2 lists the language, cognitive, and perceptual abilities required for success in school. Problems detected and treated during the preschool years can prevent many school problems in later years. Table 18-3 on p. 424 describes the clinical symptoms of typical language disorders. Evaluation of language development must be done together with an assessment of problem-solving skills.
Table 18-2
Selected Perceptual, Cognitive, and Language Processes Required for Elementary School Success
From Kliegman, R., Behrman, R., Jenson, H.B., & Stanton, B. (2007). Nelson’s textbook of pediatrics (18th ed.). Philadelphia: Saunders.
Table 18-3
Not Talking: A Clinical Classification
| WHEN PARENTS SAY | CLASSIFY THE SYMPTOMS AS |
| “I’m the only one who understands what she says.” | Articulation disorder |
| “She’ll do what I say, but when she wants something, she just points.” | Expressive language delay |
| “He can’t play ‘show me your nose,’ and the only word he says is ‘mama.’ ” | Global language delay |
| “He never made those funny baby sounds or said ‘mama’ and ‘dada,’ and now he just repeats everything I say.” | Language disorder |
| “He used to say things like ‘Joey go bye-bye,’ but now he doesn’t talk at all.” | Language loss |
From Montgomery, T. (1994). When children do not talk. Contemporary Pediatrics, 11(9), 49.
Development of Play
Play activities in the preschool child increase in complexity. At 2 to 3 years of age, the child imitates the activities of daily living of the parents (hammering, shaving, feeding the doll). By 4 years of age, the child may develop broader themes such as a trip to the zoo. By 5 years of age, a trip to the moon demonstrates the child’s imaginary abilities. Play enables the child to experience multiple roles and emotional outlets, such as the aggressor, the victim, the superpower, or the acquisition of toys or friends they desire. Appealing to the child’s magical thinking is the best approach to communication.
Spiritual Development
Preschoolers learn about religious beliefs and practices from what they observe in the home. Preschoolers cannot yet understand abstract concepts; their concept of God, sometimes treated as an imaginary friend, is concrete. Preschool children can memorize Bible stories and related rituals, but their understanding of the concepts is limited. Observing religious traditions practiced in the home during a period of hospitalization (e.g., before-meal or bedtime prayers) can help the preschool child deal with stressors.
Sexual Curiosity
When guiding parents concerning the sexual education of young children, the nurse should use the following common principles of teaching and learning:
• First assess the knowledge base of the child; then assess what specific information the child is seeking.
• Be honest and accurate in providing information at the child’s level. Although the child may not understand completely at first, the child’s repeated questions and explanations will form the basis of later learning and understanding.
• Use correct terminology so that misinformation or misinterpretation can be avoided.
• Provide sex education at the time the child asks the question. The asking of the question often indicates readiness to learn.
• Parents must understand that sexual curiosity starts as an inquiry into anatomical differences. Differences in how urination occurs may later become the focus. A general understanding of infants coming from “Mommy’s tummy” precedes the more mature concept of sexual organs and functioning.
Preschool children are as matter-of-fact about sexual investigation as they are about any other learning experience and are easily distracted to other activities. Sexual curiosity displayed in the form of masturbation or “playing doctor” should be approached in a positive manner. The appropriate touch or dress can be taught without generating a “bad” or “dirty” concept of the activity. Teaching socially acceptable behavior must be in the form of guidance rather than discipline.
Masturbation
Masturbation is common in both genders during the preschool years. The child experiences pleasurable sensations, which lead to a repetition of the behavior. It is beneficial to rule out other causes of this activity, such as rashes or penile or vaginal irritation. Masturbation in the preschool child is considered harmless if the child is outgoing, sociable, and not preoccupied with the activity.
Education of the parents consists of assuring them that this behavior is a form of sexual curiosity and is normal and not harmful to the child, who is merely curious about sexuality. The cultural and moral background of the family must be considered in assessing the degree of discomfort about this experience. A history of the time and place of masturbation and the parental response is helpful. Punitive reactions are discouraged. Parents are advised to ignore the behavior and distract the child with some other activity. The child should know that masturbation is not acceptable in public, but this must be explained in a nonthreatening manner. Children who masturbate excessively and who have experienced a great deal of disruption in their lives benefit from ongoing counseling.
Bedtime Habits
The development and reinforcement of optimal bedtime habits are important in the preschool years. Parents should be guided to engage the child in quiet activities before bedtime, to maintain specific rituals that signal bedtime readiness (such as storytelling), and to verbally state “after this story, it will be bedtime.” The use of a night-light, a favorite bedtime toy, or a glass of water at the bedside is an option. Attention-getting behavior that results in taking the child into the parent’s bed should be discouraged because it rewards the attention-getting behavior and defeats the objectives of the bedtime ritual. The nurse should be aware that specific cultures encourage “family beds,” where children regularly sleep with siblings and parents. Understanding cultural practices is essential before preparing a teaching plan.
Physical, Mental, Emotional, and Social Development
Three-year-olds are a delight to their parents. They are helpful and can assist in simple household chores. They obtain articles when directed and return them to the proper place. Three-year-olds come very close to the ideal picture that parents have in mind of their child. They are living proof that their parents’ guidance during the trying 2-year-old period has been rewarded. Temper tantrums are less frequent, and in general the 3-year-old is less erratic. They are still individuals, but they seem better able to direct their primitive instincts than previously. They can help to dress and undress themselves, use the toilet, and wash their hands. They eat independently, and their table manners have improved.
Three-year-olds talk in longer sentences and can express thoughts and ask questions. They are more company to their parents and other adults because they can talk about their experiences. They are imaginative, talk to their toys, and imitate what they see about them. Soon they begin to make friends outside the immediate family. Parallel play (playing independently within a group) and associative play are both typical of this period. Children play in loosely associated groups. Because they can now converse with playmates, they find satisfaction in joining their activities. Three-year-olds play cooperatively for short periods. They can ask others to “come out and play.” If 3-year-olds are placed in a strange situation with children they do not know, they commonly revert to parallel play because it is more comfortable.
Preschoolers begin to find enjoyment away from Mom and Dad, although they want them nearby when needed. They begin to lose some of their interest in their mother, who up to this time has been more or less their total world. The father’s prestige begins to increase. Romantic attachment to the parent of the opposite sex is seen during this period. A daughter wants “to marry Daddy” when she grows up. Children also begin to identify themselves with the parent of the same sex.
Preschool children have more fears than the infant or older child because of increased intelligence (which enables them to recognize potential dangers), memory development, and graded independence (which brings them into contact with many new situations). Toddlers are not afraid of walking in the street because they do not understand its danger. Preschool children realize that trucks can injure, and they worry about crossing the street. This fear is well-founded, but many others are not.
The fear of bodily harm, particularly the loss of body parts, is unique to this stage. The little boy who discovers that his infant sister is made differently may worry that she has been injured. He wonders if this will happen to him. Masturbation is common during this stage as children attempt to reassure themselves that they are all right. Other common fears include fear of animals, fear of the dark, and fear of strangers. Night wandering is typical of this age-group.
Preschool children become angry when others attempt to take their possessions. They grab, slap, and hang onto them for dear life. They become very distraught if toys do not work the way they should. They resent being disturbed from play. They are sensitive, and their feelings are easily hurt. Much of the unpleasant social behavior seen during this time is normal and necessary to the child’s total pattern of development.
The Four-Year-Old
Four-year-olds are more aggressive and like to show off newly refined motor skills. They are eager to let others know they are superior, and they are prone to pick on playmates. Four-year-olds are boisterous, tattle on others, and may begin to swear if they are around children or adults who use profanity. They recount personal family activities with amazing recall but forget where their tricycle has been left. At this age, children become interested in how old they are and want to know the exact age of each playmate. It bolsters their ego to know that they are older than someone else in the group. They also become interested in the relationship of one person to another, such as Timmy is a brother but is also Daddy’s son.
Four-year-olds can use scissors with success. They can lace their shoes. Their vocabulary has increased to about 1500 words. They run simple errands and can play with others for longer periods. Many feats are done for a purpose. For instance, they no longer run just for the sake of running. Instead, they run to get someplace or see something. They are imaginative and like to pretend they are doctors or firefighters. They begin to prefer playing with friends of the same sex.
The preschool child enjoys simple toys and common objects. Raw materials are more appealing than toys that are ready-made and complete in themselves. An old cardboard box that can be moved about and climbed into is more fun than a dollhouse with tiny furniture. A box of sand or colored pebbles can be made into roads and mountains. Parents should avoid showering their children with ready-made toys. Instead, they can select materials that are absorbing and that stimulate the child’s imagination.
Stories that interest young children depict their daily experiences. If the story has a simple plot, it must be related to what they understand to hold their interest. They also enjoy music they can march around to, music videos, and simple instruments they can shake or bang. (Make up a song about their daily life, and watch their reaction.)
The Concept of Death
Children between 3 and 4 years of age begin to wonder about death and dying. They may pretend to be the hero who shoots the intruder dead, or they may actually witness a situation in which an animal is killed. Their questions are direct. “What is ‘dead’? Will I die?” The view of the family is important to the interpretation of this complex phenomenon.
Children may become acquainted with death through objects with no particular significance to them. For instance, the flower dies at the end of the summer and does not bloom anymore. It no longer needs sunshine or water because it is not alive. Usually young children realize that others die, but they do not relate death to themselves. If they continue to pursue the question of whether or not they will die, parents should be casual and reassure them that people do not generally die until they have lived a long and happy life. Of course, as they grow older they will discover that sometimes children do die.
The underlying idea is to encourage questions as they appear and gradually help them accept the truth without undue fear. There are many excellent books for children about death. Two that are appropriate for the preschool child are Geranium Mornings by S. Powell and My Grandpa Died Today by J. Fassler. The dying child is discussed in Chapter 27.
The Five-Year-Old
Five is a comfortable age. Children are more responsible, enjoy doing what is expected of them, have more patience, and like to finish what they have started. Five-year-olds are serious about what they can and cannot do. They talk constantly and are inquisitive about their environment. They want to do things correctly and seek answers to their questions from those whom they consider to “know” the answers. Five-year-old children can play games governed by rules. They are less fearful because they believe their environment is controlled by authorities. Their worries are less profound than at an earlier age.
The physical growth of 5-year-olds is not outstanding. Their height may increase by 5 to 7.6 cm (2 to 3 inches), and they may gain 1.4 to 2.7 kg (3 to 6 lb). They may begin to lose their deciduous teeth at this time. They can run and play games simultaneously, jump three or four steps at once, and tell a penny from a nickel or a dime. They can name the days of the week and understand what a weeklong vacation is. They usually can print their first name.
Five-year-olds can ride a tricycle around the playground with speed and dexterity. They can use a hammer to pound nails. Adults should encourage them to develop motor skills and not continually remind them to “be careful.” The practice children experience will enable them to compete with others during the school-age period and will increase confidence in their own abilities. As at any age, children should not be scorned for failure to meet adult standards. Overdirection by solicitous adults is damaging. Children must learn to do tasks themselves for the experience to be satisfying.
The number and type of television or computer programs that parents allow the preschool child to watch is a topic for discussion. Although children enjoyed television at age 3 or 4 years, it was usually for short periods. They could not understand much of what was occurring. The 5-year-old, however, has better comprehension and may want to spend a great deal of time watching television or playing computer games. The plan of management differs with each family. Whatever is decided must be discussed with the child. For example, television and computers should not be allowed to interfere with good health habits, sleep, meals, and physical activity. Most parents find that children do not insist on watching television if there is something better to do.
Guidance
Much has been written on the subject of discipline, views of which have changed considerably over time. Today, authorities place much importance on the development of a continuous, warm relationship between children and their parents. They believe this helps to prevent many problems. The following is a brief discussion that may help the nurse in guiding parents.
Children need limits for their behavior. Setting limits makes them feel secure, protects them from danger, and relieves them from making decisions that they may be too young to formulate. Children who are taught acceptable behavior have more friends and develop good self-esteem. They live more enjoyably within the neighborhood and society. The manner in which discipline or limit setting is carried out varies from culture to culture. It also varies among different socioeconomic groups. Individual differences occur among families and between parents and vary according to the characteristics of each child.
The purpose of discipline is to teach and to gradually shift control from parents to the child, that is, to develop self-discipline or self-control. Positive reinforcement for appropriate behavior has been cited as more effective than punishment for poor behavior. Expectations must be appropriate to the age and understanding of the child. The nurse encourages parents to try to be consistent, because mixed messages are confusing for the learner.
Timing the Time-Out
Most researchers agree that to be effective, discipline must be given at the time the incident occurs. It should also be adapted to the seriousness of the infraction. The child’s self-worth must always be considered and preserved (Carey et al., 2009). Warning the preschool child who appears to be getting into trouble may be helpful. However, too many warnings without follow-up lead to ineffectiveness. For the most part, spankings are not productive. The child associates the fury of the parents with the pain rather than with the wrong deed because anger is the predominant factor in the situation. The real value of the spanking is therefore lost. Beatings administered by parents as a release for their own pent-up emotions are totally inappropriate and can lead to child abuse charges. In addition, the parent serves as a role model of aggression. Whether a parent is affectionate, warm, or cold (uncaring) also plays a role in the effectiveness of child rearing.
Time-out periods, usually lasting 1 minute per year of age, with the child sitting in a straight chair facing a corner are considered an effective discipline technique. There should be no interaction or eye contact during the time-out period, and a timer with a buzzer should be used. Often a child will attempt interaction during this period by asking, “How much more time is left?” The child should learn that any interaction restarts the timer at zero. Using the child’s room or a soft comfortable chair for time-out is not effective, because the child will either fall asleep or engage in another activity and the objective of time-out is defeated. Time-out should be preceded by a short (no longer than 10-word) explanation of the reason and followed by a short (no more than 10 words) restatement of why it was necessary. Longer explanations are not effective for young children. If the child knows the rules and the behavior that will precipitate a time-out and receives no more than one warning that there will be a time-out if the undesirable behavior continues, he or she will learn self-control. Consistency is the key to helping the child learn acceptable behavior. Parents must be taught to resist using power and authority for their own sake. As the child matures and understands more clearly, privileges can be withheld as a consequence for undesirable behavior. The reasons for such actions are carefully explained.
Reward
Rewarding the child for good behavior is a positive and effective method of discipline. This can be done with hugs, smiles, tone of voice, and praise. Praise can always be tied with the act, such as “Thank you, Zoe, for picking up your toys,” or “I appreciate your standing quietly like that.” The encouragement of positive behavior eliminates many of the undesirable effects of punishment.
Rewards should not be confused with bribes. The parent may offer a child a reward if he or she behaves in a specific situation before an incident occurs. For example, the parent may say, “You may pick out one small toy after we are finished shopping if you behave during this trip.” If this agreement is not made before an incident and the child misbehaves and then is offered one small toy to behave, this is a bribe that serves to reinforce the bad behavior and is not a desirable technique of behavior management.
Consistency and Modeling
Being consistent is difficult for parents. Realistically, it is only an ideal to strive for—no parent is consistent all the time. Consistency must exist between parents as well as within each parent. It is suggested that parents establish a general style for what, when, how, and to what degree punishment is appropriate for misconduct. Parents who are lax or erratic in discipline and who alternate it with punishment have children who experience increased behavioral difficulties.
The influence of modeling, or good example, has been widely explored. Studies show that adult models significantly influence children’s education. Children identify and imitate adult behavior, verbal and nonverbal. Parents who are aggressive and repeatedly lose control demonstrate the power of action over words. Those who communicate, show respect and encouragement, and set appropriate limits are more positive role models. Finally, parents need assistance in reviewing parental discipline during their own childhood to recognize destructive patterns that they may be repeating. Modeling also involves teaching a child how to be self-sufficient and responsible. Asking children to do simple chores around the house is a good way to make them feel good about themselves; it gives them an opportunity to please you and learn at the same time, as long as the chore is not expected to be performed with expertise! Some chores a preschooler can perform include setting the table, sorting colored and white laundry, and picking up toys. If the chore is associated with a positive outcome, the concept of consequences can be learned. For example,” If we pick up the toys quickly, then we will have time to read a story before bedtime.”
Jealousy
Jealousy is a normal response to actual, supposed, or threatened loss of affection. Both children and adults may feel insecure in their relationship with the person they love. The closer children are to their parents, the greater is their fear of losing them. Children envy the newborn. They love the sibling but resent his or her presence. They cannot understand the turmoil within themselves (Figure 18-3). Jealousy of a new sibling is strongest in children under 5 years of age and is shown in various ways. Children may be aggressive and may bite or pinch, or they may be rather discreet and may hug and kiss the infant with a determined look on their face. Another common situation is children’s attempt to identify with the infant. They revert to wetting the bed or want to be powdered after they urinate. Some 4-year-olds even try the bottle, but it is usually a big disappointment to them.
FIGURE 18-3 Child and new sibling. A new sibling is welcomed into the home. Both children need attention to minimize the development of jealousy.
Preschool children may be jealous of the attention that their mother gives to their father. They may also envy the children they play with if they have bigger and better toys. There is less jealousy in an only child, who is the center of attention and has a minimum number of rivals. Siblings of varied ages are apt to feel that the younger ones are “pets” or that the older ones have more special privileges.
Parents can help to reduce jealousy by the early management of individual occurrences. Preparing young children for the arrival of the new brother or sister minimizes the blow. They should not be made to think that they are being crowded. If the newborn is going to occupy their crib, it is best to settle the older child happily in a large bed before the infant is born. Children should feel they are helping with care of the infant. Parents can inflate their ego from time to time by reminding them of the many activities they can do that the infant cannot.
If it is convenient, the newborn is given a bath or a feeding while the older child is asleep. In this way, the older sibling avoids one occasion in which the mother shows the newborn affection for a relatively long time. Some persons think that it helps to give the child a pet to care for. Many hospitals offer sibling courses that assist parents in helping the child to overcome jealousy.
If the child tends to hit the infant or another child, both children must be separated. The child who has caused or is about to cause the injury needs as much attention as the victim, if not more. Similar aggressiveness is seen when the child is made to share toys. It is even more difficult to learn to share Mother, so the child must be given time to adjust to new situations. Children are assured that they are loved but are told that they cannot injure others.
Thumb Sucking
Thumb sucking is an instinctual behavioral pattern and is considered normal. It is seen by sonogram about the twenty-ninth week of embryonic life. Although the cause is not fully understood, it satisfies and comforts the infant. Nonnutritive sucking in the form of thumb sucking or use of a pacifier has several documented benefits in the first year of life—when the infant is in the oral phase of development. Increased weight gain, decreased crying, the development of self-consoling ability, and increased behavioral organization have been documented in infants who have been allowed to suck unrestrained. If a pacifier is used, safe construction is essential (see Figure 16-2). The pacifier causes fewer dental problems than the rigid finger and is more easily relinquished. Parents need guidance in the safe use of pacifiers. Cleanliness is essential, because the pacifier often falls onto a dirty surface.
Finger or thumb sucking will not have a detrimental effect on the teeth as long as the habit is discontinued before the permanent teeth erupt. Most children give up the habit by the time they reach school age, although they may regress during periods of stress or fatigue. Management includes education and support of the parents to relieve their anxiety and prevent secondary emotional problems in their children. The child who is trying to stop thumb sucking is given praise and encouragement.
Enuresis
Enuresis is involuntary urination after the age at which bladder control should have been established. The term enuresis is derived from the Greek word enourein, “to void urine.” Bed wetting has existed for generations and affects many cultures. There are two types: primary and secondary. Primary enuresis refers to bed wetting in the child who has never been dry. Secondary enuresis refers to a recurrence in a child who has been dry for a period of 1 year or more. Diurnal, or daytime, wetting is less common than nocturnal, or nighttime, episodes. It is more common in boys than in girls, and there may be a genetic influence. In many children a specific cause is never determined.
Approximately 92% of children achieve daytime dryness by 5 years of age. By 12 to 14 years of age, approximately 98% of children remain dry during the night. Sometimes enuresis is the result of inappropriate toilet training. Parents who demand early toilet training can cause a child to rebel and defy them by continuing to wet the bed. Parents who are not alert to the needs of the child may not recognize readiness to toilet train and therefore frustrate the child’s efforts to master this developmental task. Stressful events can precipitate bed wetting.
In some cases, organic causes of nocturnal enuresis include urinary tract infections, diabetes mellitus, diabetes insipidus, seizure disorders, obstructive uropathy, abnormalities of the urinary tract, and sleep disorders. Maturational delay of the nervous system and small bladder capacity have also been suggested as causes.
Treatment and Nursing Care
A detailed physical and psychological history is obtained. Factors such as the pattern of wetting, number of times per night or week, number of daytime voidings, type of stream, dysuria, amount of fluid taken between dinner and bedtime, family history, stress, and reactions of parents and child are documented. The nurse also determines any medications that the child may be taking and the extent to which his or her social life is inhibited by the problem, such as the inability to spend the night away from home. Developmental landmarks, including toilet training, are reviewed. If there appears to be an organic cause, appropriate blood and urine studies are undertaken. In most cases, the physical findings are negative.
Education of the family is extremely crucial to prevent secondary emotional problems. Parents are reassured that many children experience enuresis and that it is self-limited. Power struggles, shame, and guilt are fruitless and destructive. Reassurance and support by the nurse are of great help.
It is essential that the child be the center of the management program. The positive approach of rewarding dry nights and charting the progress is very helpful. Liquids after dinner should be limited, and the child should routinely void before going to bed.
When the child does not respond to routine management, other techniques include counseling, hypnosis, behavior modification, and pharmacotherapy. Moisture-activated conditioning devices are also commercially available (e.g., an alarm rings when the child wets). These have had limited success. Bladder-training exercises in which the child is asked to hold the urine for as long as possible may stretch the bladder and increase its size. The child’s bedroom should be as close to the bathroom as possible, and a night-light should be used.
The nurse prepares the parents for relapses, which are common. The response to various therapies is highly individual. Overzealous treatment is to be avoided. A nonpunitive, matter-of-fact attitude is most prudent. Imipramine hydrochloride (Tofranil) has been found to decrease enuresis. It is administered before bedtime. Imipramine has a variety of side effects, including mood and sleep disturbances and gastrointestinal upsets. Overdose can lead to cardiac dysrhythmias, which may be life threatening. Dosage and administration should be closely supervised. It is not recommended for children under age 6 years. Desmopressin (DDAVP) nasal spray has been used with some success but is expensive.
Preschool
The change from home to nursery school or preschool is a big step toward independence. At this age, children are adjusting to the outside world as well as to the family. Some children have the complicating factor of a new brother or sister in the house.
Many parents work outside the home and find it necessary to provide alternative care settings for their children. Some parents who have only one child seek preschool experiences for their child to enhance growth and development by providing experience with playmates. Nurses can provide guidance to parents in selecting an appropriate preschool to meet their child’s needs. A family day care center provides child care for small groups of children for 6 or more hours of a 24-hour day. Work-based group care may be provided by some employers as a convenience to their employees. Preschool programs provide structured activities that foster group cooperation and the development of coping skills. The child can gain self-confidence and positive self-esteem in a good preschool program. Qualified preschool teachers are objective in their interaction with the child and often can detect problems that can be followed up before the child enters kindergarten. Parents may need guidance in selecting a preschool for their child.
The following list of suggestions can guide the nurse in helping parents to select a facility appropriate for their child:
• The facility should be licensed by the state; contact a state licensing agency for a list of local day care centers or preschools.
• The accreditation criteria for preschools can be obtained by writing the National Association for the Education of Young Children, 1834 Connecticut Avenue NW, Washington, DC 20009.
• Teachers prepared in early childhood education should staff the preschool.
• The student-to-staff ratio should be reviewed.
• The philosophies of the facility, including discipline procedures, environmental safety, sanitary provisions, fee schedules, and facilities for snacks, meals, and rest time, should be reviewed.
• Schedules and facilities for active/passive and indoor/outdoor play should be reviewed.
• The school should routinely require a personal and health history of the child before admission to the program.
• The parent should visit the preschool and personally observe the environment. Talking with the parents of other children attending the school is helpful. Children are accepted into nursery schools between ages 2 and 5 years. Most sessions last about 3 hours.
Daily Care
The child between ages 3 and 6 years does not require the extensive physical care given to an infant but still needs a bath each day and a shampoo at least twice a week. It is best to keep hairstyles simple. Dental hygiene and nutrition are discussed in Chapter 15.
Clothing
Clothes should be loose enough so they don’t restrict movement but allow for active play without hems getting stepped on or tripped over. Clothes should be washable. Simple clothes make it easy for preschoolers to dress themselves. A hook within reach, nailed to the door perhaps, is helpful. Preschool children should dress and undress themselves as much as they can. The child’s mother or father can assist but should not take over.
Shoes should be sturdy and supportive. Protective gear such as helmets for bicycling should be a natural part of dressing for play activities. Dressing appropriately for the weather to be encountered is essential. Flame-retardant sleepwear is available in most stores.
Accident Prevention
Accidents are still a major threat during the years from 3 to 5. At this age, children may suffer injuries from a bad fall. Preschool children hurry up and down stairs. They climb trees and stand up on swings. They play hard with their toys, particularly those they can mount. Stairways must be kept free of clutter. Shoes should have rubber soles, and new ones should be purchased when the tread becomes smooth. When buying toys, parents must be sure they are sturdy and age appropriate. Preschool children should not be asked to do anything that is potentially dangerous, such as carrying a glass container or sharp knife to the kitchen sink.
Automobiles continue to be a threat. Children are taught where they can safely ride their tricycle and where they can play ball, and they should not be allowed to use sleds on streets that are not blocked off for this purpose. They must not play in or around the car or be left alone in the car. The use of car seats or seat belt restraints continues to be important.
Burns that occur at this age often result from the child’s experimentation with matches or lighters. Burns from hot coffee are also common. These items are common hazards for this age-group; they should be kept well out of reach, and their dangers should be explained to the child.
Poisoning is still a danger. Children try to imitate adults and are apt to sample pills, especially if they smell good. Their increased freedom brings them into contact with many interesting containers in the garage or basement.
Preschool children are also taught the dangers of talking to or accepting rides from strangers. If they are stopped by a driver, they should run to the house of people they know. Parents should make it clear to children in nursery school that they will never send a stranger to call for them. Children must know the dangers of playing in lonely places and of accepting gifts from strangers. Children should always know where to go if Mother or Father or the baby-sitter cannot be found. Preschool children still require a good deal of indirect supervision to protect them from dangers that arise from their immature judgment or social environment (Figure 18-4).

Play in Health and Illness
Play is important to the physical, mental, emotional, and social development of both healthy and sick children (Figure 18-5). Children climbing on a jungle gym develop muscles and coordination as they exercise all parts of their bodies. They use energy and develop self-confidence. Their imagination may take them to the jungle, where they swing from limb to limb. They may face imagined fears and solve problems that would be much more trying, if not impossible, in reality. They communicate with other children and take a further step in developing moral values, that is, taking one’s turn and considering others. Other types of play help children learn colors, shapes, sizes, and textures and can teach creativity. This natural and readily available outlet must be tapped by nursing and health care personnel. Children may be unfamiliar with every facet of the hospital, but they know how to play, and playing is a good way for the nurse to establish rapport with them.

The Nurse’s Role
Some hospitals have well-established playroom programs supervised by play therapists. Play therapy is an important part of every pediatric nursing care plan. It is not necessary to be an expert in manual dexterity, art, or music; rather, one must understand the needs of the child. Play is not just the responsibility of those assigned to it, nor is it confined to certain times or shifts.
Many factors are involved in providing suitable play for children of various ages in the hospital. The patient’s state of health affects the amount of activity in which he or she can participate. The nurse can facilitate many activities that relieve stress and provide enjoyment for the child who has been prescribed bed rest. Overstimulation would be hazardous for some severely ill children. Nurses are always on guard for signs of fatigue in patients and use their judgment accordingly.
The diagnosis of the hospitalized child should also be considered when choosing an appropriate toy. For example, a friction toy is inappropriate for a child in an oxygen-rich environment. Sparks from the toy can cause an explosion. A stuffed animal may not be an appropriate toy for a child with asthma, who may be allergic to the contents of the stuffing.
Safety must be considered in selecting an appropriate toy. Toys should be safe, durable, and suited to the child’s developmental level. Toys should not be sharp or have parts that are easily removed and swallowed. Too many toys at one time are confusing to the child. Complicated toys are frustrating and disappointing. Well-selected toys such as crayons, blocks, and dolls are useful throughout the years. A washable laundry bag tied to the bed of a hospitalized child can be used to store the child’s own toys neatly and safely. Toys may be taken home with the child or discarded after he or she is discharged from the hospital.
Each child needs sufficient time to complete an activity. In general, quiet play should precede meals and bedtime for both well and sick children. Investigations have shown that the toys enjoyed by boys and those enjoyed by girls are more similar than dissimilar.
During routine procedures the nurse can entertain the child with nursery rhymes, stories, nonsense games, songs, finger play, or puppets. Often the other children on the unit can be included for “I’m thinking of something blue, red, and green,” and so forth. Simple crafts are fun. The nurse may find various instructions from children’s magazines or the local public library. Scrapbooks are entertaining. Children may even enjoy making a storybook about their hospital experience. The nurse involved in enrichment programs for children can make a definite contribution. Surprise boxes in which a gift is opened every day provide anticipation for the patient. Collections of scraps can be started consisting of bright ribbons, bits of string, pipe cleaners, paper bags, newspapers, or bits of cotton. Because the turnover of patients is rapid, many projects can be repeated with different children.
Music is provided by radio, CDs, MP3 players, computers, and instruments. Older children enjoy sending emails and text messages to friends. Special children’s recordings and videos are available. The services of a music therapist are available in some institutions. Drawing materials, finger paints, and modeling clay foster expression and creativity. They require only a flat surface, such as the overbed table, and a particular medium. The bedridden child can participate in messy projects, too. The bed is simply protected with newspapers or plastic. Children in cribs require adequate back support for such projects. This is done by elevating the mattress or using pillows. Simple computer games may be available in the hospital setting.
Playmates may be limited in the hospital setting if the child has a condition that is communicable. However, surgical and orthopedic patients can play together in a playroom with appropriate supervision. The nurse should guide the parents to play for a child who is fatigued or weakened by illness. The child can maintain the role of observer.
Types of Play
Preschool children need playmates to promote social development. The play characteristics of each age-group are shown in Table 15-10. The preschool-age child gradually moves from parallel and associative play to cooperative play with playmates.
The play of preschool children should be noncompetitive. The healthy preschool child requires active play activities that are supervised for safety. Large construction sets, number or alphabet games, crayons, play tools, housekeeping toys, musical toys, pop-up books, large puzzles, and clay are examples of suitable toys for the preschool-age child. Active play can involve simple climbing, sliding, and running activities. Imaginary friends are common to the preschool-age child. They serve many purposes in helping the child adjust to an expanding world and increased independence. Parents can acknowledge the presence of the imaginary friend as part of pretend play, but the responsibilities of reality do not include the pretend friend. Parents should not intervene in play groups. Allowing the child to master frustration and develop social skills is essential to growth and development.
 Nursing Tip
Nursing Tip
Imaginary playmates are common and normal during the preschool period and serve many purposes, such as relief from loneliness, mastery of feats, and provision of a “scapegoat.”
Play and the Handicapped Child
The child who is mentally impaired needs more stimulation through play than the child who is not. The nurse must consider the mental age of the child rather than the chronological age when guiding parents about the selection of toys. The environment should be as colorful and bright as possible. The child may be introduced to objects of various sizes and textures. Play with other children must be supervised because the poorer judgment of mentally handicapped children may get them into difficulty. They may be aggressive and unaware of their own strength. Adequate space in which to run is necessary. These children should be brought into group play gradually. Materials are presented one at a time.
Mentally handicapped children may need to be taught how to play, because they may not have had the preschool play experience of the nonhandicapped child. Repetition of play experiences is necessary. Equipment and play materials must be altered to accommodate the child’s size and yet be suitable for the mental age. The nurse or teacher should improvise games and songs to meet the special needs of this group. (See Chapter 23 for a more complete discussion of the growth and development and care of the mentally handicapped child.)
Therapeutic Play
Play and toys can be of therapeutic value in retraining muscles, improving eye-hand coordination, and helping children crawl and walk (push-pull toys). A musical instrument such as the clarinet promotes flexion and extension of the fingers. Blowing is an excellent prerequisite for speech therapy. Therapists supervise such activities. They leave specific instructions if they wish their work to be reinforced on the unit. Blowing out the light of a flashlight as if it were a candle is therapeutic play for a postoperative preschool child.
Play Therapy
The nurse may also hear the term play therapy. This technique is used for the child under stress. A well-equipped playroom is provided. Children are free to play with whatever articles they choose. A counselor may be in the room observing and talking with the child, or the child may be observed through a one-way glass window. By using these as well as other methods, the therapist obtains a better understanding of the patient’s struggles, fears, resentments, and feelings toward self and others. When children act out their feelings through “dramatic play,” the feelings are externalized, which relieves tension. The interpretation of child behavior is complex, and a great deal of time, study, and sensitivity is required for full understanding.
Art Therapy
Art therapy is useful in communicating with children and adults. It is becoming more widely used. The art therapist is especially trained to assist children to express their feelings and communicate through drawings, clay, and other media. Some hospitals with inpatient mental health units have art therapy departments.
Nursing Implications of Preschool Growth and Development
The nurse should anticipate parental concern with nutritional problems in the preschool child. Daily appetites may fluctuate widely, but the weekly pattern will probably show stability to meet the child’s growth needs. During clinic visits the parents should be guided to provide age-appropriate foods at mealtimes in appropriate portions. The child’s developing self-regulatory mechanism will determine how much he or she will eat based on feelings of hunger or satiety. Efforts to control the preschool child’s intake may result in power struggles or patterns of overeating or undereating.
Safety is a high priority in this active age range. “Childproofing” the home and the need for adequate supervision and safety equipment during sports activities should be emphasized. Preschoolers who will be given immunizations via a “shot” can be calmed by giving pretend “shots” to their doll and having a parent present to comfort them. Explanations such as “the shot will hurt just a little but will prevent you from getting sick” are beyond the Piaget preoperational level of understanding of the preschool child. The ability to understand detailed explanations is not yet present in preschool-age children, even if verbal ability is high. The preschool-age child may have unfounded fears that respond best to reassurance and “protection” by parents, rather than reasoning about why the fear is unfounded.
The nurse should provide parental guidance concerning the changing behavior patterns of the preschool-age child. The characteristic alternating dependence and independence can be frustrating for parents. Parents who do not volunteer any positive comments about their child during conversations may require further investigation and interview. Problems with day care and discipline must be discussed. The use of corporal punishment (spanking) as a major disciplinary technique can lead to child abuse. The use of time-out and alternative methods of discipline should be stressed.
Hospitalization can be frightening to a preschool child who is egocentric and prone to magical thinking. Because the preschool child cannot fully understand cause and effect, he or she may perceive hospitalization as punishment for behavior. The preschool child may feel abandoned by the parents and continues to be subject to separation anxiety. Separation anxiety (see Chapter 21) is manifested by the stages of protest, despair, detachment, and regression to earlier behaviors. Bed wetting is common in the hospitalized preschool-age child, and parents should be encouraged to be patient and positive. Assigning a consistent caregiver and providing age-appropriate diversional activities are essential for a hospitalized preschool-age child.
The nurse who is with children daily can describe their behavior. It is important to describe good and poor behavior, conversations that seem pertinent, and the child’s relationships with other children in the hospital. What is the child’s approach to play? Does the child join in freely or linger outside the group? Does the child prefer active or quiet activities? Does the child seem to tolerate frustrations? Can the child talk with his or her playmates and convey ideas? What type of attention span does the child have? These observations and charting are meaningful and promote better understanding and appropriate interventions by nurses and other personnel.
Get Ready for the NCLEX® Examination!
Key Points
• The child age 3 to 5 years is often referred to as the “preschool child.” During this period, the child grows taller and loses the chubbiness of the toddler period.
• The major tasks of the preschool child include preparation to enter school, the development of a cooperative type of play, control of body functions, acceptance of separation, and increase in communication skills, memory, and attention span.
• Gross and fine motor skills become more developed, as evidenced by participation in running, skipping, and drawing pictures.
• Piaget refers to the preschool period as one in which symbolic thought processes and language emerge.
• Erikson’s preschool stage involves the development of initiative. Kohlberg’s theory concerning preschoolers refers to the moral development and the beginning awareness of the needs of others.
• Language ability develops rapidly, and the child is able to construct rather complicated sentences by the end of this period.
• The many questions of the preschool child must be listened to carefully and answered thoughtfully and truthfully.
• Play is the business of children. It contributes to physical and mental well-being by encouraging communication, socialization, and outlets for energy.
• Cooperative and highly imaginative play is characteristic of the preschool child.
• Social issues of the preschool period include learning to share and to control impulses.
• Common concerns of parents during this period include how to set limits, handle jealousy, and respond to thumb sucking and masturbation.
• Corporal punishment of the preschool child can nurture rebellion and aggression. Appropriate discipline techniques can assist the child to develop self-control.
• Careful evaluation of day care and nursery school programs is important to ensure high-quality care.
• Accidents are still a major hazard for preschool children because of their immature judgment and increased locomotive skills.
• During the preschool years the parents need guidance to understand the developmental road map of physical, emotional, and cognitive growth to help the child to meet life’s challenges and goals and to enrich family interaction.
• Primary enuresis refers to bed wetting in a child who has never been dry. Secondary enuresis refers to bed wetting in a child who has been dry for a period of 1 year or more.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• American Academy of Pediatrics, Children’s Health Topics: www.aap.org/topics.html
• Sexuality Information and Education Council of the United States: www.siecus.org
Review Questions for the NCLEX® Examination
1. When selecting play activities for a healthy 4-year-old, the parent should be guided to understand that the 4-year-old enjoys:
1. solitary play, sitting next to a friend.
2. cooperative play with friends.
2. An example of a therapeutic play activity for a preschool child who is recovering from an appendectomy would be:
3. The nurse is guiding a parent concerning techniques of dealing with a child with enuresis. The most appropriate suggestion by the nurse would be to:
1. wake the child often during the night and take him to the bathroom to void.
2. limit liquids after dinner and have the child void before going to bed.
3. use a consistent technique of discipline whenever the bed is wet.
4. keep the child in diapers until bed wetting is no longer a problem.
4. The appropriate amount of time to use in a time-out period for a 3-year-old child is:
Critical Thinking Question
1. The parents of a preschool child discuss the typical play activities of their child. They express concern that they have seen their child choose to play the role of “the aggressive bad guy” in play scenarios and are concerned that he may be developing aggressive behavior. They ask if they should stop him from assuming roles in play that are not acceptable behaviors. What is the best response of the nurse?