The Child with a Genitourinary Condition
1 Define each key term listed.
2 Name the functional unit of the kidney.
3 List four urological diagnostic procedures.
4 Recognize urinary tract anomalies in infants.
5 Differentiate between nephrosis and acute glomerulonephritis.
6 Discuss the skin care pertinent to the child with nephrosis.
7 Explain any alterations in diet applicable to the child with nephrosis.
8 Outline the nursing care for a child who is diagnosed as having Wilms’ tumor.
9 Discuss the impact of undescended testes on fertility.
10 Discuss the impact of genitourinary surgery on the growth and development of children at various ages.
 , p. 677)
, p. 677) , p. 685)
, p. 685) , p. 676)
, p. 676) , p. 676)
, p. 676) , p. 676)
, p. 676) , p. 676)
, p. 676) , p. 677)
, p. 677) , p. 680)
, p. 680) , p. 684)
, p. 684) , p. 678)
, p. 678) , p. 683)
, p. 683) , p. 681)
, p. 681) , p. 677)
, p. 677) , p. 676)
, p. 676) , p. 674)
, p. 674) , p. 681)
, p. 681) , p. 676)
, p. 676) , p. 677)
, p. 677) , p. 686)
, p. 686) , p. 677)
, p. 677) , p. 677)
, p. 677) , p. 677)
, p. 677) , p. 679)
, p. 679) , p. 686)
, p. 686) , p. 679)
, p. 679) , p. 679)
, p. 679) , p. 679)
, p. 679) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Development of the Urinary Tract
The urinary system consists of two kidneys, two ureters, the urinary bladder, and the urethra. Figure 29-1 depicts these structures and illustrates how they differ in the developing child and in the adult. The function of the kidneys is to rid the body of waste products and to maintain body fluid homeostasis (Figure 29-2). The kidneys also produce substances that stimulate red blood cell formation in the bone marrow (e.g., erythropoietin-stimulating factor [ESF]), as well as renin, which regulates blood pressure. Microscopically, the functional unit of the kidneys is the nephron. Each kidney contains more than 1 million nephrons. Although the newborn’s kidneys are immature, they function quite effectively. Nevertheless, the functional limitations must be considered carefully when the newborn is premature or ill. This applies especially to the administration of medications, formula, and parenteral fluids.
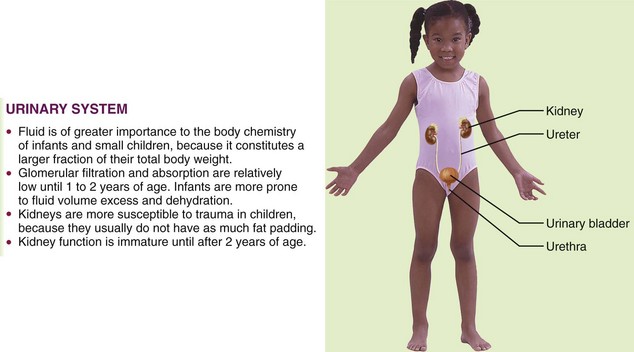
FIGURE 29-1 Summary of some urinary system differences between the child and the adult. The urinary system is the main excretory system. The kidneys remove wastes and excess materials from the blood and produce urine. This system helps to regulate blood chemistry.
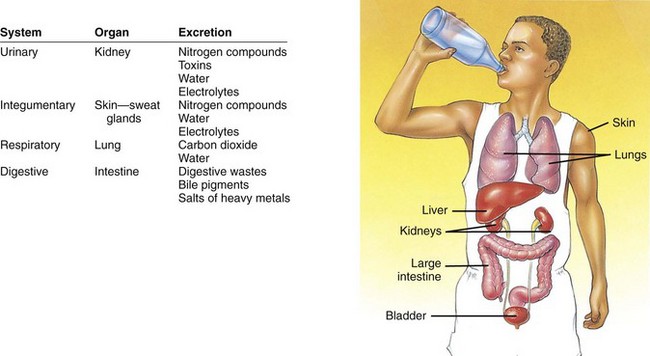
FIGURE 29-2 The urinary system’s chief function is to regulate the volume and composition of body fluids and excrete unwanted materials, but it is not the only system in the body that is able to excrete unneeded substances. The table in this figure compares the excretory functions of several systems. Although all of these systems contribute to the body’s effort to remove wastes, only the urinary system can finely adjust the water and electrolyte balance to the degree required for normal homeostasis of body fluids.
Soon after implantation, the embryonic mass differentiates into three distinct layers of cells: the ectoderm, mesoderm, and endoderm. The urinary and reproductive organs originate from the mesoderm. At approximately the third month of gestation the fetal kidney begins to secrete urine. The amount gradually increases as the fetus matures and comprises a portion of the amniotic fluid volume. An absence or small amount of amniotic fluid may indicate genitourinary difficulties.
The kidney and the urinary tract develop about the same time as the ears form during fetal life. There is an unexplained relationship between low-set ears in the newborn and urinary tract anomalies. When assessing the newborn, an imaginary line should be drawn between the outer canthus of the eye and the ear. The line should cross the tip of the auricle. If the tip of the auricle falls below this line, the assessment should be recorded and reported (see Figure 12-6).
Development of the Reproductive Systems
Figure 29-3 shows the female and male reproductive systems and lists some of the differences between children and adults. The reproductive system provides for perpetuation of the species. Members of each gender are equipped with gonads (which provide reproductive cells) and a set of accessory organs. The gonads (ovaries in the female and testes in the male) produce sex cells and hormones that affect the reproductive organs and other body systems.
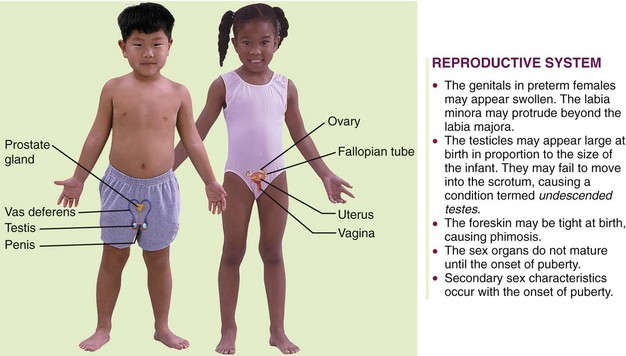
FIGURE 29-3 Summary of some reproductive system differences between the child and the adult male and female. Each reproductive system consists of gonads and associated structures. The reproductive system maintains sexual characteristics and provides for perpetuation of the species.
Sex is genetically determined at the time of fertilization. The presence of a Y chromosome is essential for the development of the testes and their hormones. Sex differentiation in the embryo occurs early. The organs specific to the male or female child develop. Before this, the embryo has neither male nor female characteristics. The development of the ovaries occurs later than that of the testes. By the twelfth week the external genitalia of the fetus are recognizably male or female.
Several tests are helpful in diagnosing conditions of the reproductive tract. These include a Papanicolaou (Pap) smear, serological blood tests, cultures, ultrasound procedures, pregnancy tests, and routine blood and urine tests. Sexual abuse in children may be manifested by behaviors such as urinary frequency, excessive masturbation, encopresis (fecal soiling beyond 4 years of age), severe nightmares, bedwetting, irritation or pain in the genital area, and a decrease in physical or emotional development. Suggestive posturing by young children or an explicit knowledge of sex acts shown by children under 8 years of age calls for further investigation. Menstrual disorders and premenstrual syndrome are discussed in Chapter 11. Sexually transmitted infections are discussed in Chapters 11 and 32.
 Nursing Tip
Nursing TipAssessment of Urinary Function
Urological diagnostic procedures include urinalysis, ultrasonography, intravenous (IV) pyelogram, and computed tomography (CT) scan of the kidneys. Renal biopsy is used to diagnose the extent of kidney disease. A uroflow is an assessment procedure used to determine the rate of urine flow. The child voids into a receptacle, and a uroflowmeter graphs the volume and pressure. This is useful in diagnosing stricture or scarring. Cytoscopy is useful for investigating congenital abnormalities or acquired lesions in the bladder and lower urinary tract. Radiographic examination of the bladder and urethra before and during micturition (voiding) is called voiding cystourethrography. The cystometrogram and urethral pressure profile assess bladder capacity and function. Both tests require catheterization and infusion of sterile water. The minimum urine output for infants and toddlers is 2 to 3 mL/kg/hr; for preschoolers and young school-age children, the minimum is 1 to 2 mL/kg/hr; and for school-age children and adolescents, the minimum is 0.5 to 1 mL/kg/hr. Common laboratory tests are reviewed in Table 29-1.
Table 29-1
Common Laboratory Tests for Urinary Tract Function
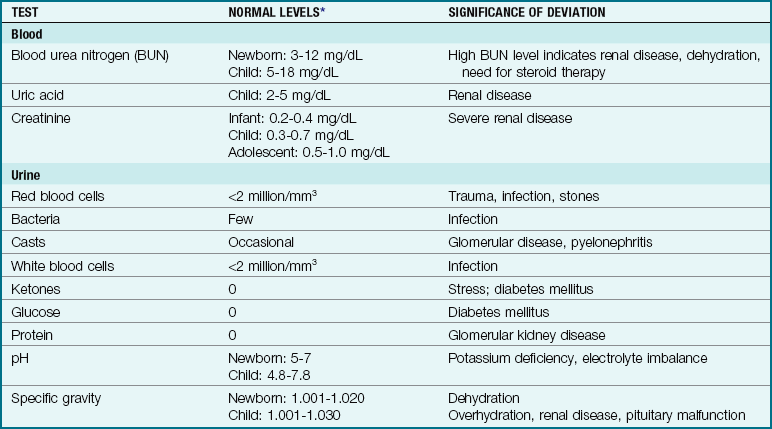
*Values for different age-groups are indicated only when relevant.
Terms commonly used to describe urinary dysfunction include the following:
• Dysuria: difficulty in urination
• Frequency: abnormal number of voidings in a short period
• Urgency: strong urges to void, often despite inability to do so
• Nocturia: awakening during the night to void
• Enuresis: uncontrolled voiding after bladder control has been established
Anomalies of the Urinary Tract
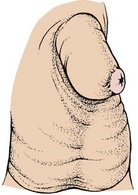
Pathophysiology: Phimosis is a narrowing of the preputial opening of the foreskin, which prevents the foreskin from being retracted over the penis (Figure 29-4). This is normal in newborns and usually disappears by 3 years of age. In some children this narrowing may obstruct the stream of urine, causing dribbling or irritation. The condition can be corrected by circumcision.
Treatment and Nursing Care: When circumcision is performed on an older boy, careful explanations and reassurance are provided. The nurse is sensitive to the child’s embarrassment and fear. Postoperatively the penis is covered with a petroleum gauze. The penis is tender and may burn on urination.
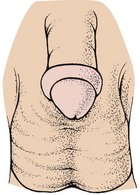
Cleansing of the uncircumcised penis and retraction of the foreskin are discussed in Chapter 12. Forcible retraction of a tight foreskin is avoided because it can lead to paraphimosis (Figure 29-5). When this occurs, the foreskin cannot be returned to its normal position. There may be swelling and impaired circulation caused by the constriction. This condition necessitates immediate evaluation by a physician.
Hypospadias and Epispadias
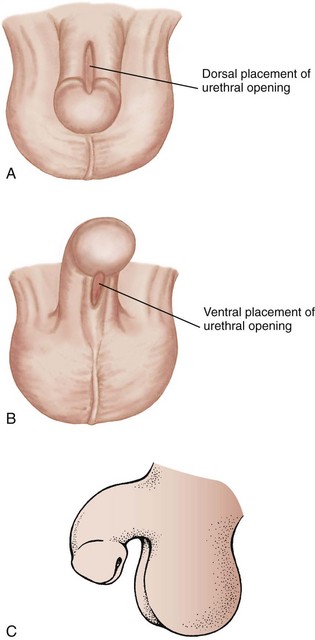
Pathophysiology: Hypospadias is a congenital defect in which the urinary meatus is located not at the end of the penis but on the lower shaft. In mild cases it lies just below the tip of the penis, but it may be found at the midshaft or near the penile-scrotal junction. With epispadias, the opening of the urinary meatus is on the upper surface of the penis. Unlike epispadias, hypospadias is fairly common, occurring in 1 out of 250 to 500 newborn boys. Hypospadias may be accompanied by chordee, a downward curvature of the penis caused by a fibrotic band of tissue (Figure 29-6).
Treatment and Nursing Care: The alert nurse may discover hypospadias or epispadias in the nursery during neonatal assessment. In many mild cases surgery is not necessary for either condition unless the location and extent of the defect are such that the child will not be able to stand to void or the defect would cause psychological problems or difficulties in future sexual relations. Treatment consists of surgical repair and is usually performed before age 18 months. It is sometimes done in stages depending on the associated defects. Most techniques can be performed during same-day surgery. Routine circumcision is avoided in these children, because the foreskin may be useful in the repair. A urinary catheter may be required after surgery. Parents are instructed in the home care of the catheterized child. Medication for bladder spasms may be required.
This condition is corrected at a time in childhood when fears of separation and mutilation are great, and therefore attention is directed to psychological considerations. In the older child, questions about virility and reproduction may surface and need to be addressed.
Exstrophy of the Bladder
Pathophysiology: In exstrophy of the bladder the lower portion of the abdominal wall and the anterior wall of the bladder are missing. As a result, the bladder lies open and exposed on the abdomen. Exstrophy is caused by a failure of the midline to close during embryonic development. Other congenital anomalies may also be present. This anomaly occurs in 1 out of 40,000 live births and is more common in boys than in girls.
Manifestations: This disorder is noticeable by fetal sonogram. The defect may range from a small cutaneous fistula in the abdominal wall to complete exstrophy (the turning inside out of an organ). Urine leaks continually from the bladder. The skin around the bladder becomes excoriated. Other anomalies are common.
Treatment and Nursing Care: The bladder is covered with a plastic shield or appropriate dressing to protect its mucosa but allow for urinary drainage. This also protects the bladder from irritation by bedclothes or diapers. The skin is protected by a suitable ointment. Diapers are generally placed under rather than around the infant. The infant is positioned on his or her back or side so that urine drains freely. Antibiotics are given to prevent infection. Surgical closure is ideally performed during the first 48 hours of life.
Obstructive Uropathy
Pathophysiology: Many conditions, such as calculi (stones), tumors, strictures, and scarring, may cause an obstruction of the normal flow of urine. These conditions may be congenital or acquired, and blockage may be either partial or complete. One or both kidneys may be affected. The pathological changes depend on the nature and location of the problem. Hydronephrosis (hydro, “water,” and nephro, “kidney”) is the distention of the renal pelvis as the result of an obstruction. The pelvis of the kidney becomes enlarged, and cysts form. This may eventually damage renal nephrons, resulting in deterioration of the kidneys. Polycystic kidney refers to a condition in which large, fluid-filled cysts form in place of healthy kidney tissue in the fetus. This is inherited as an autosomal recessive trait. Kidney damage can result in an inability of the kidney to concentrate urine, resulting in metabolic acidosis. Urine that is not excreted promptly can promote the growth of organisms that cause urinary tract infection.
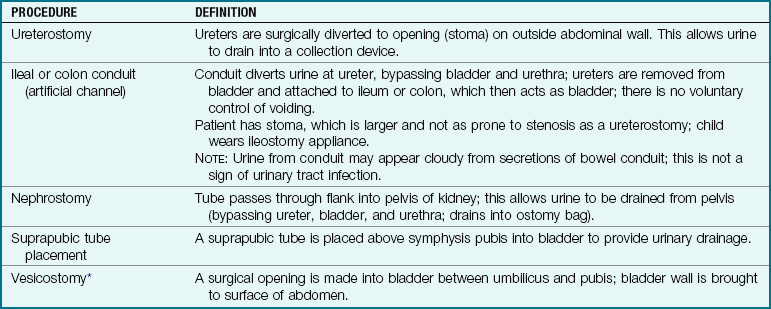
Treatment and Nursing Care: Urinary diversion is necessary in certain conditions and may be accomplished by several procedures (Table 29-2). This type of surgery is a source of great apprehension for parents. The physical care of the child with a urinary stoma (artificially created opening or passage) presents hygiene problems, skin problems, and difficulties in leaving the infant in the care of others. Frequent trips to the health care provider add to the strain of everyday life.
Stress from the urinary diversion is age related. The toddler may be unable to attain independence in toilet training. The school-age child suffers from being different and may have a distorted body image. The adolescent may have lowered self-esteem and is concerned about sexuality. Parents with affected newborns grieve for the loss of a perfect child and experience concerns about the length and quality of the infant’s life. The nurse anticipates the impact of this type of diagnosis and incorporates suitable psychological interventions into daily care. Providing emotional support and teaching parents how to prevent infection are priorities of care.

Acute Urinary Tract Infection
Pathophysiology: Urinary tract infections (UTIs) are common in children. They are more common in girls than in boys (except during the neonatal period) and occur predominantly in children 7 to 11 years of age. Of all infections, 75% to 90% are caused by Escherichia coli, followed by Klebsiella and Proteus (Kliegman et al., 2007). The nurse will see the following terms used to describe the location and nature of urinary tract disturbances:
• Urethritis: infection of the urethra
• Cystitis: inflammation of the bladder
• Bacteriuria: bacteria in the urine
• Pyelonephritis: infection of the kidney and the renal pelvis
• Ureteritis: infection of the ureters
• Vesicoureteral reflux: backward flow of urine into the ureters
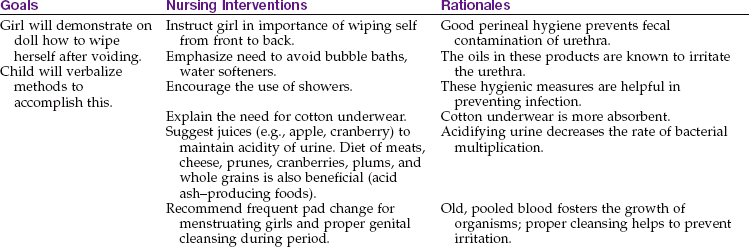
Several factors account for the preponderance of UTIs in girls. These include a shorter urethra, the location of the urethra closer to the anus, the wearing of close-fitting nylon underwear, the use of bubble baths, the retention of urine, and vaginitis. Incest or other sexual abuse should be considered in young girls with repeated infections. In boys, the longer male urethra and the antibacterial properties of prostatic secretions inhibit the entry of pathogens.
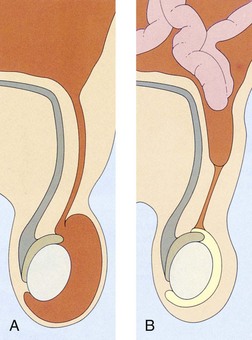
Certain chemical and physical factors are important. Normal urine is acidic. Alkaline urine favors pathogens. Urine that remains in the bladder for a prolonged time serves as an excellent medium for bacterial growth. In certain conditions such as vesicoureteral reflux, the urine is forced backward from the bladder and into the ureters during urination (Figure 29-7).
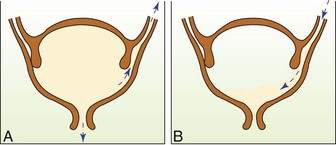
FIGURE 29-7 Vesicoureteral reflux. A, Congenital abnormalities of the junction between the bladder and the ureters can force urine to flow backward into the ureters during voiding. B, After voiding, residual urine from the ureter remains in the bladder.
Vesicoureteral reflux: Vesicoureteral reflux (VUR) refers to the abnormal retrograde flow of urine from the bladder to the ureters during a void (see Figure 29-7). After the void, urine flows back into the bladder, where urinary stasis occurs that allows growth of bacteria leading to UTI. The bacteria have access to the kidneys during subsequent reflux; pyelonephritis and renal scarring can result.
Manifestations and Diagnosis: The signs and symptoms of UTI are age dependent. The infant may be admitted with high fever, vomiting, and chills. A urine culture is done. Specimens must be processed promptly or refrigerated to prevent contamination. Urine specimens should not be collected from the diaper because the chemicals and gels contained in the diaper fabric may alter the results of some tests. In toilet-trained children, a midstream urine specimen is obtained after cleansing the urethral meatus and rinsing with sterile water. A voiding cystourethrogram (VCUG) may be ordered to diagnose structural abnormalities.
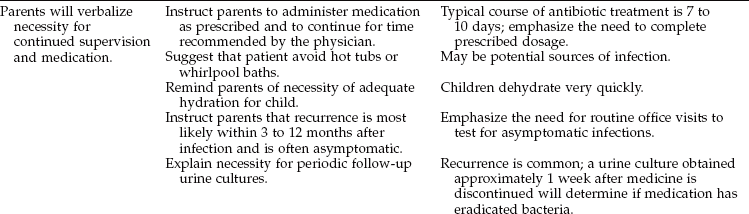
Treatment and Nursing Care: Infants under 1 year of age are usually hospitalized and observed. Treatment with daily low-dose antimicrobial medications may be required to keep the urine sterile and prevent kidney infection. In children with low-grade UTI, antimicrobial prophylaxis may not prevent the development of new renal scarring (Montini, 2008). Infants usually outgrow the reflux, but are monitored regularly as outpatients. For severe reflux, an endoscopic procedure injects a bulking agent via a subtrigonal injection (STING) into the mucous membrane of the ureter to prevent retrograde flow of urine. Open surgical intervention is reserved mostly for significant anatomical defects.
Acute cystitis is treated promptly to prevent development of pyelonephritis and kidney damage. Until the specific organism causing the infection is identified, broad-spectrum antibiotics are initially prescribed.
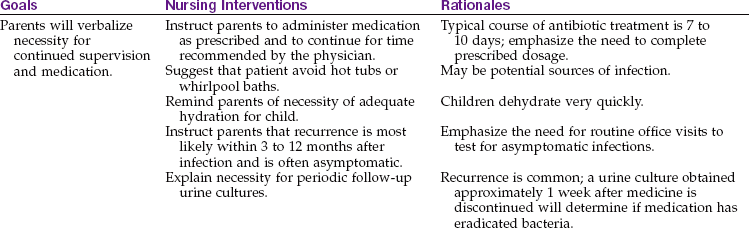
Methods of preventing UTIs are taught to parents and to the patient, if age appropriate. The nurse stresses the need for proper amounts of fluid to maintain sterility and flushing of the bladder. Nursing Care Plan 29-1 presents the nursing considerations appropriate for these patients. The prognosis is excellent with prompt treatment. Monitoring vital signs, including blood pressure, and providing anticipatory guidance help decrease the stress levels of the children and parents.
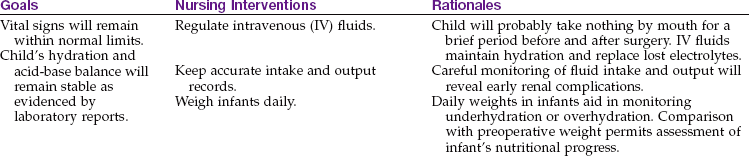
29-1  Nursing Care Plan
Nursing Care Plan
The Child with a Urinary Tract Infection
A school-age female child is brought to the clinic complaining of burning on urination. Her mother states the child fears going to the bathroom because “it will hurt.”
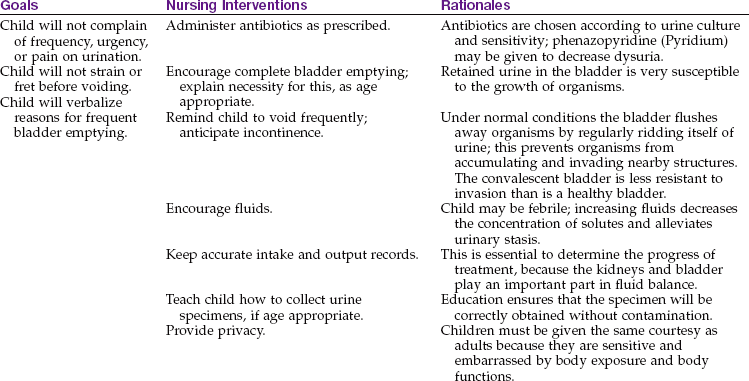
Deficient parental knowledge related to follow-up care
1. A mother comes to the clinic with her 5-year-old child who has a urinary tract infection for the second time in 3 months. You notice that the child is wearing spandex sports shorts and carrying a doll. She is holding a bottled water container that is filled with fruit punch. What teaching interventions could the nurse initiate?
Nephrotic Syndrome (Nephrosis)
Pathophysiology: Nephrotic syndrome refers to a number of different types of kidney conditions that are distinguished by the presence of marked amounts of protein in the urine, edema, and hypoalbuminemia. Minimal change nephrotic syndrome (MCNS), found in approximately 85% of cases, is discussed in this section.
Nephrosis is more common in boys than in girls and is seen most often in children 2 to 7 years of age. The specific cause is unknown but may be related to a thymus T-cell dysfunction. The prognosis is good in steroid-responsive patients. Most children have periods of relapse until the disease resolves itself. There is an 80% favorable prognosis over the long term.
Manifestations: The characteristic symptom of nephrosis is edema. This occurs slowly; the child does not appear to be sick. It is first noticed around the eyes and ankles and later becomes generalized. The edema shifts with the position of the child during sleep. The child gains weight because of the accumulation of fluid. The abdomen may become distended (ascites). The child is pale, irritable, and listless and has a poor appetite. Blood pressure is usually normal.
Urine examination reveals massive albumin (protein) and a few red blood cells. The glomeruli, the working units of the kidneys that filter the blood, become damaged and allow albumin and blood cells to enter the urine. The level of protein in the blood falls; this is termed hypoalbuminemia (hypo, “below,” albumin, and emia, “blood”).
Treatment: The goals of treatment include minimizing edema, preventing infection, reducing the loss of protein in the urine, and preventing toxicity from the medication prescribed.
Control of edema: The child with nephrosis is given medications designed to reduce proteinuria and, consequently, edema. Steroid therapy is currently used for this purpose. Oral prednisone is initially given. The dosage is reduced for maintenance therapy, which continues for 1 to 2 months. Because steroids mask signs of infection, the patient must be watched closely for more subtle symptoms of illness. Children are prone to infection when absolute granulocyte counts fall below 1000 cells/mm3. This is called neutropenia.
The child’s skin is examined at sites of punctures, wounds, pierced ears, body piercings, and catheters. The nurse watches for temperature variations and changes in behavior. Suspicions are promptly reported, because septicemia is life threatening. Prompt antimicrobial therapy is begun when an acute infection is recognized. Generally, diuretics have not been effective in reducing nephrotic edema. Immunosuppressive therapy (e.g., cyclophosphamide [Cytoxan] and chlorambucil) is used for some steroid-resistant children.
Nursing Care: The nursing care of the child with nephrosis is of the greatest significance because the disease necessitates long-term therapy. The child is periodically hospitalized and becomes a familiar personality to hospital personnel.
The nurse provides supportive care to the parents and child throughout the course of this disease. The child is treated at home whenever possible and is brought to the hospital for special therapy only. Parents are instructed to keep a daily record of the child’s weight, urinary protein levels, and medications. Signs of infection, abnormal weight gain, and increased protein in the urine must be reported promptly. Good skin care is especially important during periods of marked edema. After the acute stage of the illness subsides, the child is allowed to participate in normal childhood activities.
Positioning: The child is turned frequently to prevent respiratory tract infection. A pillow placed between the knees when the child is lying on the side prevents pressure on edematous organs. The child’s head is elevated from time to time during the day to reduce edema of the eyelids and to make him or her more comfortable. Swelling impairs the circulation of the lacrimal secretions. It may therefore be necessary to bathe the eyes to prevent the accumulation of exudate.
Monitoring intake and output: The child’s intake and output are strictly charted. This is the responsibility of the nurse, regardless of who feeds the patient. Parents are instructed to inform the nurse of how much fluid has been taken. The importance of keeping proper fluid balance sheets (i.e., intake and output records) for patients with diseases of the kidneys cannot be overemphasized.
As stated, the patient’s urine output must be carefully measured. Diapers may be weighed on a gram scale before application and after removal (1 g = 1 mL). The dry weights are marked on the diaper. A careful check of the number of voidings is of particular value. The character, odor, and color of the urine are also important. If a 24-hour urine collection is ordered, every voided specimen within that time must be saved, or the test will not be valid. The specimens are collected in a large bottle or container that is correctly labeled. Some tests require that certain preservatives be added to the container; this matter is clarified before the procedure begins.
Weight and protection from infection: The patient is weighed two or three times a week to determine changes in the degree of edema. The child is weighed on the same scale each time and at about the same time of day. Abdominal girth (circumference) should also be measured daily.
Nurses make every effort to protect the child from exposure to upper respiratory tract infections. Children who are active must not be allowed to wander into areas where they would be in danger of contracting an infection. No vaccinations or immunizations should be administered while the disease is active and during immunosuppressive therapy.
The vital signs of a patient with nephrosis are taken regularly. Ordinarily, there is no temperature elevation unless an infection is present. Blood pressure remains normal. Parental guidance and support are given by all members of the nursing team. The child with nephrosis is kept under close medical supervision over an extended period. Home care during remissions is preferred, with parents being taught monitoring skills.
Acute Glomerulonephritis
Pathophysiology: Acute glomerulonephritis (AGN), formerly called Bright’s disease, is an allergic reaction (antigen-antibody) to a group-A beta-hemolytic streptococcal infection. It may appear after the patient has had scarlet fever or skin infections. The body’s immune mechanisms appear to be important in its development. Antibodies produced to fight the invading organisms also react against the glomerular tissue. Glomerulonephritis is the most common form of nephritis in children, and it occurs most often in boys 3 to 7 years of age. Both kidneys are usually affected.
The nephron is the working unit of the kidneys. Nephrons number in the millions. Within the bulb of each nephron lies a cluster of capillaries called the glomerulus. It is these structures that are affected, as the name implies. They become inflamed and sometimes blocked, permitting red blood cells and protein (which are normally retained) to enter the urine. The kidneys become pale and slightly enlarged. Table 29-3 compares nephrosis with AGN.
Table 29-3
Comparison Between Nephrosis and Acute Glomerulonephritis
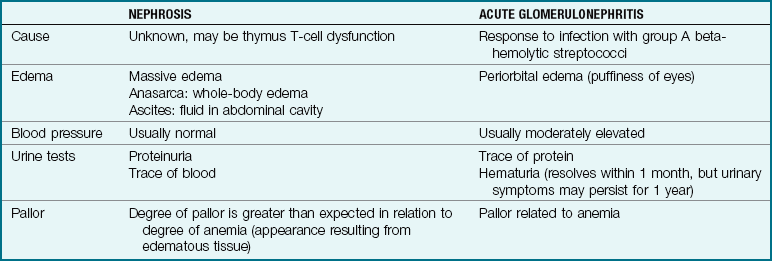
Note: The signs and symptoms of nephrosis and acute glomerulonephritis are similar. Careful analysis and comparisons reveal significant differences. Either condition can lead to renal failure and its consequences.
The prognosis for AGN is excellent. Patients with mild cases of the disease may recover within 10 to 14 days. Patients with protracted cases may show urinary changes for as long as 1 year but have complete recovery. The possibility of complications involving hypertensive changes such as brain ischemia necessitates careful monitoring and care of each patient.
Manifestations: From 1 to 3 weeks after a streptococcal infection has occurred, the parent may notice that the child has periorbital edema upon awakening in the morning and that the child’s urine is smoky brown or bloody. This is frightening to the parent and child, and most parents immediately seek medical advice. Urine output may be decreased. The urine specific gravity is high, and albumin, red and white blood cells, and casts may be found on examination. The blood urea nitrogen (BUN) level is elevated, as are the serum creatinine level and the sedimentation rate. The serum complement level (C3) is usually reduced. Hyperkalemia (excessive potassium in the blood) may produce cardiac toxicity. Hypertension may occur. An antistreptolysin (ASO) titer, if positive, evidences a recent streptococcal infection.
Treatment and Nursing Care: Although children may feel well, activity is limited until gross hematuria subsides. The urine is examined regularly. Every effort is made to prevent children from becoming overly tired, chilled, or exposed to infection. Because renal function is impaired, there is a danger of accumulating nitrogenous wastes and sodium in the body. Dietary sodium and fluid restrictions are based on the hypertension and edema present. Foods high in potassium, such as bananas, are restricted during periods of oliguria.
Nursing care is supportive: Prevention of infection and fatigue, maintenance of accurate intake and output records, and frequent monitoring of vital signs are essential.
Although glomerulonephritis is generally benign, it can be a source of anguish for the parents and child. If the patient is treated at home, the parents must plan activities to keep the child occupied with quiet activity. They must understand the importance of continued medical supervision, because follow-up urine and blood tests are necessary to assess progress toward recovery. All children with hypertension should be monitored for signs of increased intracranial pressure. Most children recover completely with no sequelae.
Wilms’ Tumor
Pathophysiology: Wilms’ tumor, or nephroblastoma (nephro, “kidney,” blasto, “bud,” and oma, “tumor”), is one of the most common malignancies of early life. It is an embryonal adenosarcoma (adeno, “glandular,” and sarcoma, “cancer of connective tissue”) that is now known to be associated with certain congenital anomalies, particularly of the genitourinary tract. It is thought to have a genetic basis.
About two thirds of these growths are discovered before the child is 3 years of age. As with some other malignancies, there are few or no symptoms during the early stages of growth. A mass in the abdomen is generally discovered by a parent or by the physician during a routine checkup. Radiographic examinations of the kidneys (most importantly, IV pyelograms) reveal a growth and verify that the remaining kidney is normal. The tumor compresses kidney tissue and is usually encapsulated. Renal damage may cause hypertension. Chest x-ray films, ultrasonography, bone surveys, liver scan, and CT may also be indicated. Wilms’ tumor seldom affects both kidneys.
Treatment and Nursing Care: Treatment of patients with Wilms’ tumor consists of a combination of surgery, radiation therapy, and chemotherapy. The kidney and tumor are removed as soon as possible after the diagnosis has been confirmed. It is important to prepare the parents and the child for the extent of the incision, which is considerable.
General nursing measures for the comfort of the patient are carried out. One important consideration pertaining to this condition is the avoidance of all unnecessary handling of the abdomen because it can cause the tumor to spread. The physician explains this to the parents, and in the hospital a sign is placed on the crib: “Do not palpate abdomen.” Nursing Care Plan 29-2 outlines care for a child undergoing surgery of the renal system. Chemotherapy and radiation therapy after surgery are usually completed at a specialized cancer center. Postoperatively, contact sport should be avoided to prevent damage to the remaining kidney.
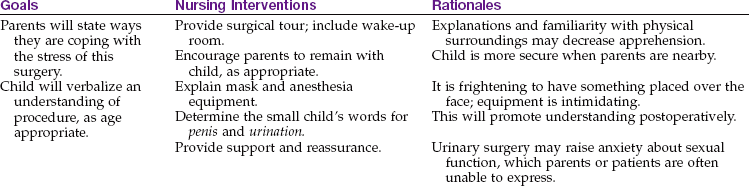
29-2 Nursing Care Plan
Child Undergoing Surgery of the Renal System
A preadolescent boy is admitted for elective kidney surgery. The child asks his parents to stay and asks the nurse many questions about the planned surgery.
High risk for ineffective airway clearance related to poor cough effort associated with postanesthesia, postoperative immobility, pain
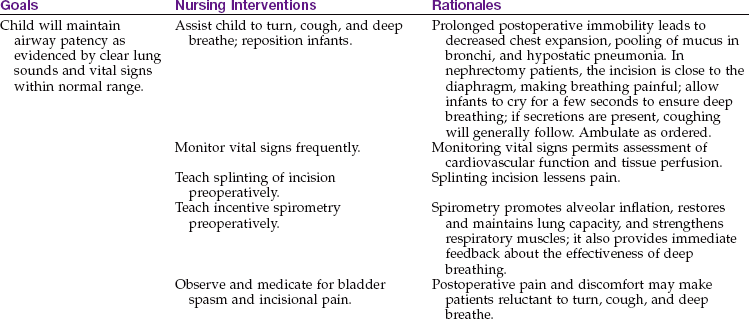
Fluid volume, high risk for deficient, related to patient’s age, surgery, catheters, or refusal to drink
1. The parents of a postoperative patient who has had renal surgery appear anxious and upset. When questioned, they state that they both work, cannot afford to take the time off from work to stay with their child, and are also worried that he will fail in school and no longer be able to travel with his friends in a carpool. They do not know how they will manage. What is the best response of the nurse?
 Safety Alert!
Safety Alert!Hydrocele
Pathophysiology: A hydrocele (hydro, “water,” and cele, “tumor”) is an excessive amount of fluid in the sac that surrounds the testicle and causes the scrotum to swell (Figure 29-8). When the testes descend into the scrotum in utero, the processus vaginalis (a fold of tissue) precedes them. This tissue ordinarily fuses, separating the peritoneal cavity from the scrotum. When this fusion does not take place, however, peritoneal fluid may enter the inguinal canal. Its appearance in the newborn is not uncommon, and in many cases the condition corrects itself by 1 year of age.
Treatment: A chronic hydrocele that persists beyond 1 year is corrected by surgery. Routine postoperative nursing care is given. This is outlined in Chapter 22. Same-day surgery may be arranged.
Cryptorchidism
Pathophysiology: The testes are the male sex glands. These two oval bodies begin their development in the embryo within the abdominal cavity, just below the kidneys. Their function is to produce spermatozoa (male sex cells) and male hormones, particularly testosterone. Toward the end of the seventh fetal month, the testes begin to descend along a pathway into the scrotum. If this descent does not take place normally, the testes may remain in the abdomen or the inguinal canal. This condition is common in approximately 30% of low-birth-weight infants (Ferlin et al., 2008). When one or both testes fail to lower into the scrotum, the condition is termed cryptorchidism (kryptos, “hidden,” and orchi, “testis”). The unilateral form is more common.
Because the testes are warmer in the abdomen than in the scrotum, the sperm cells begin to deteriorate. If both testes are affected, sterility results. Inguinal hernia often accompanies this condition. Secondary sex characteristics, such as voice change and growth of facial hair, are not affected because the testes continue to secrete hormones directly into the bloodstream. Acute scrotal pain may indicate a testicular torsion (twisting), which necessitates immediate surgery to preserve testicular function.
Treatment and Nursing Care: Occasionally, a testis or the testes spontaneously descend during the first year of life. Hormonal management before surgery consists of the administration of human chorionic gonadotropin (hCG). This hormone is useful as a diagnostic aid and may also precipitate the descent of the testes into the scrotal sac. If this does not occur, an operation called an orchiopexy (orchio, “testicle,” and pexy, “fixation”) is performed.
Although an orchiopexy improves the condition, the fertility rate among these patients may be reduced, even when only one testis is undescended. In addition, the incidence of testicular tumors is increased in these patients during adulthood. Parents are told to teach the growing child the importance of self-examination of the testes. When the child returns from surgery, care is taken to prevent contamination of the suture line, and scrotal support is maintained.
The psychological approach of the nurse to the patient and his family is important because of the embarrassment they may feel. People may ask the child why he is undergoing surgery when there is no visible evidence of trauma. This problem is often compounded by the fact that the older child may have been told not to discuss his condition; in addition, his understanding of his problem and just what is going to happen in surgery may be vague. Therefore the nurse caring for the child should know what he has been told and how he feels about his operation to give emotional support. Terminology is clarified. The nurse assures the child that his penis will not be involved in the surgery.
The parents, too, may have anxieties that they cannot verbalize. It is difficult for many of them to communicate with their child about such matters. A thoughtful, sensitive nurse who tries to anticipate related feelings and fears promotes the child’s adjustment.
Impact of Urinary or Genital Surgery on Growth and Development
Surgery of the urinary or genital tract affects growth and development. Preschoolers may perceive the treatment as punishment. Separation anxiety during hospitalization peaks, and preventive strategies should be explained to the parents. The body image of the child must be assertively maintained whenever surgery is delayed beyond infancy. Between 3 and 6 years of age, the child becomes curious about sexual differences and may masturbate. Surgical interventions during this stage of development necessitate guidance and preparation to minimize the negative impact on growth and development.
During home care, tub baths may be contraindicated, dressings to “private parts” of the body must be inspected daily, and restrictions on play activities that involve straddle toys (e.g., tricycles, rocking horses) are necessary. Adolescents may be concerned about the effects of surgery on their appearance and sexual abilities.
Get Ready for the NCLEX® Examination!
Key Points
• The functional unit of the kidney is the nephron.
• Children with hypospadias are born with the urethral opening on the undersurface of the penis.
• Bladder exstrophy is a serious congenital defect in which the bladder lies exposed on the lower portion of the abdominal wall. Surgical correction of this defect is lifesaving.
• Obstruction of the urinary tract may lead to hydronephrosis, a distention of the kidney pelvis. This is a serious condition because it could eventually lead to kidney failure if left untreated.
• To prevent fecal contamination of the urinary tract, girls are taught to wipe the perineal area from front to back after urination.
• Ascites is an abnormal collection of fluid in the peritoneal cavity. It is seen in advanced cases of nephrosis and in other conditions.
• The accurate charting of intake and output on patients with kidney problems is absolutely essential to their treatment and recovery. This includes ostomy and urinary drainage.
• Accurate blood pressure measurements will detect hypertension, a condition often associated with kidney problems.
• Normally urine flows from the ureters into the bladder, and almost no flow reenters the ureters.
• Repeated urinary tract infections or improper position of the ureters or sphincters in the bladder at birth may result in the reflux of urine into the ureters.
• Good health habits include assessing one’s own body, including the genitalia.
• Routine abdominal palpation is omitted with a child diagnosed with Wilms’ tumor.
• Early treatment of cryptorchidism is necessary to preserve testicular function.
• A hydrocele is an excessive amount of fluid in the sac that surrounds the testicle. It causes the scrotum to swell.
• Undescended testes (cryptorchidism) refers to a condition in which the testes do not lower into the scrotum during the fetal period but remain in the abdomen or the inguinal canal after birth.
• The minimum urine output for infants and toddlers is 2 to 3 mL/kg/hr; for preschoolers, the minimum is 1 to 2 mL/kg/hr; and for school-age children and adolescents, the minimum is 0.5 to 1 mL/kg/hr.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Hypospadias: www.urologychannel.com/pediatric/hypospadias.shtml
• Phimosis: www.healthscout.com/ency/68/360/main.html
• Urinary tract infections: www.pediatrics.org/cgi/content/full/103/4/e54
• Vesicoureteral reflux: www.findarticles.com/cf_dls/g2601/0014/2601001452/p1/article.jhtml
Review Questions for the NCLEX® Examination
1. The nurse understands that genitourinary surgery affects growth and development. When caring for a 4-year-old child postoperatively, a priority nursing responsibility would include:
1. strategies to preserve the child’s body image.
2. assurances that appearance and sexual function will not be affected.
3. providing age-appropriate toys such as tricycles.
4. preventing embarrassment by limiting visitation of family and friends.
2. The administration of prednisone to children with nephrosis creates the problem of:
3. Daily weights are obtained in children with nephrosis to monitor:
1. weight loss from a low-protein diet.
2. accuracy of fluid balance sheets.
4. A priority nursing responsibility in the care of a child with Wilms’ tumor is to:
1. maintain accurate intake and output records.
5. The nurse is caring for a child diagnosed with nephrosis. Symptoms that are characteristic of nephrosis include (select all that apply):