The Term Newborn
1 Define each key term listed.
2 Briefly describe three normal reflexes of the newborn, including the approximate age of their disappearance.
3 Demonstrate the steps in the physical assessment of the newborn.
4 State four methods of maintaining the body temperature of a newborn.
5 State the cause and describe the appearance of physiological jaundice in the newborn.
6 Define the following skin manifestations in the newborn: lanugo, vernix caseosa, mongolian spots, milia, acrocyanosis, and desquamation.
7 State the methods of preventing infection in newborns.
8 Interpret discharge teaching for the mother and her newborn.
 , p. 292)
, p. 292) , p. 281)
, p. 281) , p. 281)
, p. 281) , p. 290)
, p. 290) , p. 281)
, p. 281) , p. 293)
, p. 293) , p. 292)
, p. 292) , p. 297)
, p. 297) , p. 292)
, p. 292) , p. 292)
, p. 292) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The arrival of the newborn, or neonate, begins a highly vulnerable period during which many psychological and physiological adjustments to life outside the uterus must be made. The fetus that remains in the uterus until maturity has reached a major goal. The infant’s genetic background, the health of the recent uterine environment, a safe delivery, and the care during the first month of life further contribute to this adjustment.
The infant mortality rate is the ratio of the number of deaths of infants younger than age 1 year during any given year to the number of live births occurring in the same year. The rate is usually expressed as the number of deaths per 1000 live births. The infant death rate is highest in the first month and is referred to as the neonatal mortality rate. The first 24 hours of life are the most dangerous. The infant mortality rate is considered to be one of the best means of determining the health of a country. To obtain accurate figures, all births and deaths must be registered. In the United States this registration is required by law. Each birth certificate is permanently filed with the state bureau of vital statistics.
Morbidity (morbidus, “sick”) refers to the state of being diseased or sick. Morbidity rates show the incidence of disease in a specific population during a certain time frame. Perinatology is the study and support of the fetus and neonate. The term perinatal mortality designates fetal and neonatal deaths related to prenatal conditions and delivery circumstances. See Chapter 1 for details concerning statistics in the United States.
Low-birth-weight newborns and limited access to health care are major causes of infant morbidity. Reducing infant morbidity rates can reduce the resulting incidence of disability, which can have an impact on the growth and development of children. The nurse can play a vital role in educating new parents about health care and the developmental needs of their newborn.
Adjustment to Extrauterine Life
When a child is born, an orderly, continuous adaptation from fetal life to extrauterine life takes place. All the body systems undergo some change. Respirations are stimulated by chilling and by chemical changes within the blood. Sensory and physical stimuli also appear to play a role in respiratory function. The first breath opens the alveoli. The infant then enters the world of air exchange, at which time an independent existence begins. This process also initiates cardiopulmonary interdependence. The newborn’s ability to metabolize food is hampered by the immaturity of the digestive system, particularly deficiencies in enzymes from the pancreas and liver. The kidneys are structurally developed, but their ability to concentrate urine and maintain fluid balance is limited because of a decreased rate of glomerular flow and limited renal tubular reabsorption. Most neurological functions are primitive (see the discussion of the individual body systems in this chapter).
Phase 3: Care of the Newborn
Phase 3 care of the newborn covers the physical characteristics and nursing assessment of the normal term newborn, by body system. Refer to Chapter 6 for care of the newborn immediately after birth (Phase 1) and Chapter 9 for care of the newborn on admission to the nursery or postpartum unit (Phase 2).
Nervous System: Reflexes
The nervous system directs most of the body’s activity. Newborns can move their arms and legs vigorously but cannot control them. When the infant is lifted from the bed, the head will fall back because the newborn cannot maintain neutral position of the head. This is called a head lag (Figure 12-1). The reflexes full-term infants are born with, such as blinking, sneezing, gagging, sucking, and grasping (Figure 12-2), help to keep them alive. They can cry, swallow, and lift their heads slightly when lying on their abdomen.

FIGURE 12-1 Head lag. The newborn has some ability to control the head in some positions. When placed on the abdomen, the newborn may be able to raise the chin from the bed briefly. However, head lag and hyperextension normally occur when the newborn is raised from the bed in a supine position. Significant head lag after age 6 months indicates a need for follow-up care.
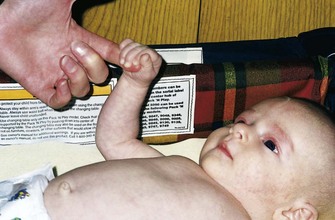
FIGURE 12-2 Grasp reflex. Touching the hands near the base of the fingers causes a reflex flexion of the hands. This grasp reflex is replaced after age 3 months by a voluntary grasp.
If the crib is jarred, infants draw their legs up and the arms fan out and then come toward midline in an embrace position. This is normal and is called the Moro reflex (Figure 12-3). Its absence may indicate abnormalities of the nervous system. The rooting reflex causes the infant’s head to turn in the direction of anything that touches the cheek, in anticipation of food. The nurse uses this when helping a mother to breastfeed her infant. A breast touching the cheek causes the infant to turn toward it to find the nipple (see Chapter 9).
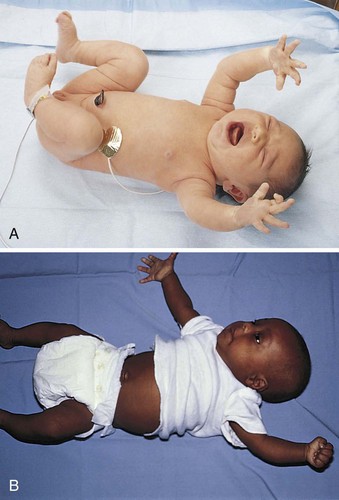
FIGURE 12-3 A, Moro reflex. Sudden jarring causes extension and abduction (an embracing motion) of the extremities and spreading of the fingers, with the index finger and the thumb forming a C shape. A unilateral (one-sided) Moro reflex may indicate a fractured clavicle. Absence of the Moro reflex may indicate a pathological condition of the central nervous system. B, Abnormal Moro reflex. Note the clenched fist of one hand that does not follow a symmetrical embracing motion. This infant requires follow-up care.
The tonic neck reflex is a postural reflex that is sometimes assumed by sleeping infants. The head is turned to one side, the arm and leg are extended on the same side, and the opposite arm and leg are flexed in a “fencing” position. This reflex disappears by the seventh month of life (Figure 12-4). Prancing movements of the legs, seen when an infant is held upright on the examining table, are termed the dancing reflex. Table 12-1 lists ages at which the neurological signs of infancy appear and disappear.
Table 12-1
Ages of Appearance and Disappearance of Neurological Signs Unique to Infancy
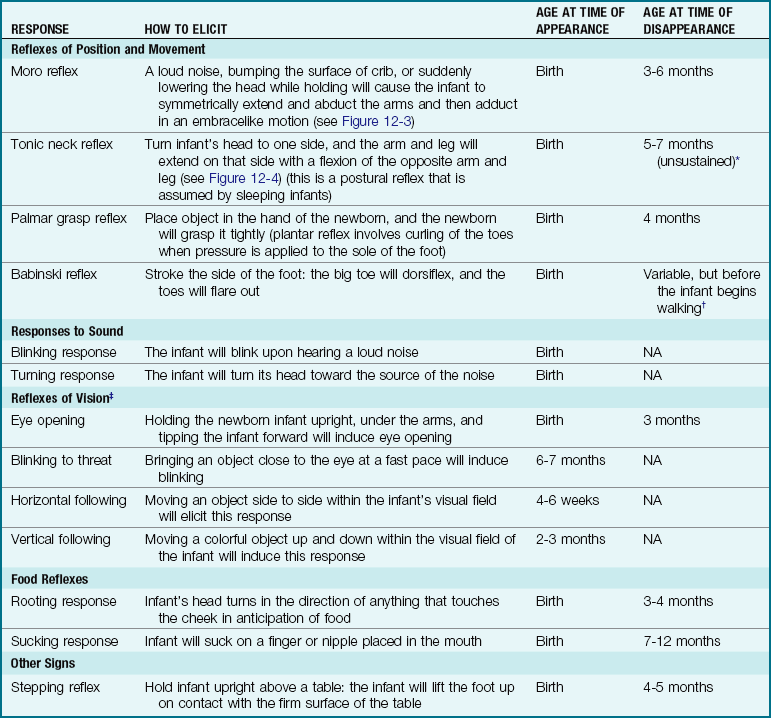
Note: Absence of these reflexes or prolonged appearance may indicate a neurological problem and requires further follow-up.
*Arm and leg posturing can be broken by infant after a few minutes, despite continued neck stimulus.
†Usually of no diagnostic significance until after age 2 years.
‡Holding the newborn infant upright under the arms will induce eye opening.

FIGURE 12-4 Spontaneous tonic neck reflex. The infant turns the head to one side, and the arm and leg are extended on that side. The opposite arm and leg flex. Often called the “fencing” reflex, it disappears by age 5 to 7 months as the central nervous system matures.
Head
The brain grows rapidly before birth, and therefore the newborn’s head is large in comparison with the rest of the body. The normal limits of head circumference range from 32 to 36 cm (12.5 to 14.1 inches) (Skill 12-1). The head may be out of shape from molding (the conforming of the fetal head to the size and shape of the birth canal) (Figure 12-5, A). There may also be swelling of the soft tissues of the scalp, which is termed caput succedaneum. It gradually subsides without treatment. Occasionally, a cephalhematoma (cephal, “head,” hemato, “blood,” toma, “tumor”) protrudes from beneath the scalp (see Figure 12-5, B and C). This condition is caused by a collection of blood beneath the periosteum of the cranial bone. It may be seen on one or both sides of the head but does not cross the suture line. This condition usually recedes within a few weeks without treatment.
Skill 12-1 Taking Head and Chest Measurements








1. The circumference of the head is measured from the top of the eyebrow to the widest part of the occiput.

2. The size of the fontanelle is obtained by measuring the widest point of the width and the widest point of the length, adding the measurements together, and dividing by 2.

3. The normal anterior fontanelle in a newborn measures between 3.6 and 6 cm. The fontanelles should appear flat with the contour of the skull. A bulging fontanelle may indicate increased intracranial pressure. A depressed fontanelle may indicate dehydration and should be reported to the health care provider.
4. When measuring the chest circumference, the measuring tape is placed at the nipple line.

5. Lift the infant to remove the paper tape in order to prevent paper cuts to the infant’s skin.
Note: The head circumference should be equal to and no more than 2 cm greater than the chest circumference until age 2. See normal growth charts to compare findings and to determine need for follow-up referral.
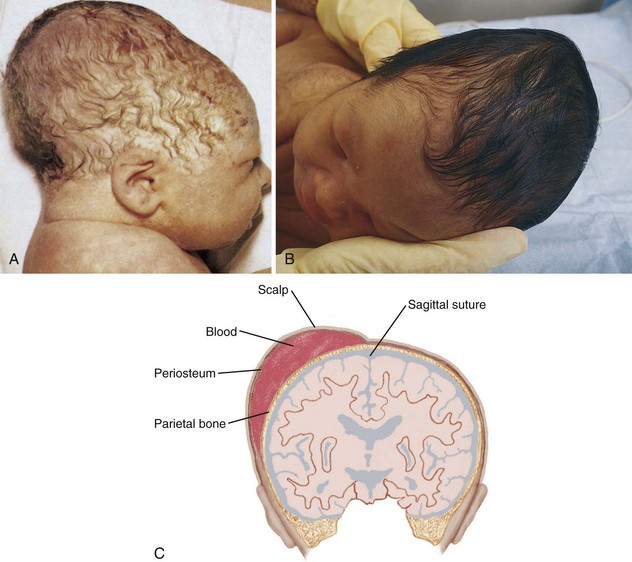
FIGURE 12-5 A, Molding of the head occurs as a result of the parietal bones overriding each other as the head passes through the birth canal. Often a collection of fluid under the scalp caused by edema of the presenting part (caput succedaneum) causes the head to appear longer than normal and soft to the touch. This condition disappears without treatment within a few weeks. B, Cephalhematoma appears as a lump on one side of the head. C, With a cephalhematoma, the blood collects between the surface of the cranial bone and the periosteal membrane. The swelling does not cross the suture lines.
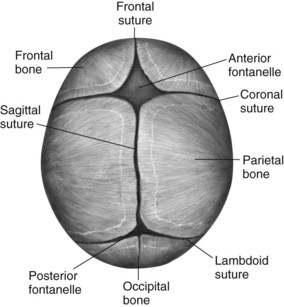
The fontanelles are unossified spaces or soft spots on the cranium of a young infant. They protect the head during delivery by permitting the process of molding and allow for further brain growth during the next  years. The anterior fontanelle is diamond shaped and is located at the junction of the two parietal and two frontal bones. It usually closes by age 12 to 18 months. The posterior fontanelle is triangular and is located between the occipital and parietal bones. It is smaller than the anterior fontanelle and is usually ossified by the end of the second month. These areas are covered by a tough membrane, and there is little chance of their being injured during ordinary care. The features of the newborn’s face are small. The mouth and lips are well developed because they are necessary to obtain food. The newborn can both taste and smell. In fact, the newborn can recognize the scent of the mother’s milk on the breast pad.
years. The anterior fontanelle is diamond shaped and is located at the junction of the two parietal and two frontal bones. It usually closes by age 12 to 18 months. The posterior fontanelle is triangular and is located between the occipital and parietal bones. It is smaller than the anterior fontanelle and is usually ossified by the end of the second month. These areas are covered by a tough membrane, and there is little chance of their being injured during ordinary care. The features of the newborn’s face are small. The mouth and lips are well developed because they are necessary to obtain food. The newborn can both taste and smell. In fact, the newborn can recognize the scent of the mother’s milk on the breast pad.
Eyes
The healthy newborn can see and can fixate on points of contrast. The newborn shows a preference for observing a human face and follows moving objects. Visual stimulation is thus an important ingredient in newborn care. Toys that make sounds and have contrasting colors attract the newborn.
Most newborns appear cross-eyed because their eye muscle coordination is not fully developed. At first, the eyes appear to be blue or gray; the permanent coloring becomes fixed between ages 6 and 12 months. The eyelids are closed most of the time. Tears do not appear until approximately age 1 to 3 months because of the immaturity of the lacrimal gland ducts.
Ears
The ears are well developed but small at birth. The ears are assessed for placement because low-set ears may indicate a congenital abnormality in another part of the body. An imaginary line drawn from the outer canthus of the eye should be even with the upper tip of the pinna of the ear (Figure 12-6). The hearing ability of the newborn is well developed at birth, but the sick or premature newborn may not respond to sounds that are heard. The presence of amniotic fluid in the ear canal can diminish hearing, but normal drainage and sneezing that occur shortly after birth help clear the ear canal.
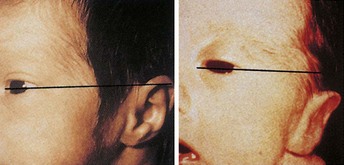
FIGURE 12-6 Ear position. The ears are assessed for placement because low-set ears may indicate a congenital abnormality. An imaginary line drawn from the outer canthus of the eye should be even with the upper tip of the pinna of the ear.
The newborn will react to sudden sound with an increase in pulse rate and respirations or a display of the startle reflex. Increased responses to vocal stimulation, particularly higher-pitched female voices, have been documented. The ability to discriminate between the mother’s voice and the voices of others may occur as early as age 3 days. Hearing is important to the development of normal speech. The nurse observes and records how the newborn reacts to sound, such as a rattle or the voice of the caretaker. The infant will respond to voices by decreasing motor activity and sucking activity and turning the head toward the sound.
One type of test used to measure infant hearing is the ALGO hearing screening test, which analyzes hearing by sending a series of soft clicks into the sleeping infant’s ear (Figure 12-7). The infant’s brain responds with a specific brain wave that is referred to as an auditory brainstem response (ABR). The response is compared by computer to normal responses, and a pass/fail score is recorded. Another type of test is the otoacoustic emissions test (OAE) that measures sounds from the cochlea in response to sound stimulation. Newborn hearing screening programs have become part of the protocol of care in hospital nurseries across the United States.

FIGURE 12-7 ALGO hearing screener shows how the test is accomplished. Immediate pass/fail results indicate whether the infant needs further audiological testing.
The ears and nose need no special attention except for cleansing with a soft cloth during the bath. Occasionally they may be externally cleansed with a cotton ball moistened slightly with water. The bony canal of the external ear is not well developed, and the tympanic membrane is vulnerable to injury. The nurse should not insert applicators. They may cause serious injury to the tympanic membrane if inserted too far into the ear canal or if the infant moves suddenly.
Sensory Overload: Sensory overload can occur if there is too much stimulation. This detrimental overload can occur in the hospital environment, where lights are bright and voices carry. The nurse can help to modify this situation by responding quickly to alarms and by speaking quietly when working near the infant.
Sleep
The neonate sleeps approximately 15 to 20 hours a day. There is a gradual change in the quantity and quality of sleep as the newborn matures. At birth the newborn passes through the phases of sleep-wake states as part of the adjustment to life outside of the uterus:
• First reactive phase: During the first 30 minutes of life the newborn is alert, and this is the best time to initiate bonding between the parent and newborn.
• Sleep phase: During the next few hours of life the infant gradually becomes sleepier and less responsive.
• Second reactive phase: After a deep sleep the infant again becomes responsive and alert.
• Stability phase: After age 24 hours the sleep-wake pattern becomes more stabilized. The pattern of sleep gradually develops into one in which the newborn is awake during the day and asleep during the night.
The environment plays a large role in the infant’s sleep behavior. The nurse can help the parent to understand that normal conversational tones can quiet a newborn, whereas high noise levels can cause increased crying. Wrapping an infant snugly can maintain temperature and promote sleep, as can gentle horizontal rocking. An infant held upright on the shoulder and rocked in a vertical fashion is likely to maintain an alert state. Newborns exhibit a specific pattern of reactivity that can influence the response to stimuli and bonding, as follows:
• Quiet sleep: Infant sleeps and does not move.
• Rapid eye movement (REM) sleep: Respirations are more irregular during REM sleep. Eye movements are evident beneath the eyelid, and limb and mouth movement may be seen.
• Active alert: The infant displays diffuse motor activity.
• Quiet alert: The infant is awake, relaxed, and quiet. In this state the infant is most responsive to testing and to bonding efforts.
• Crying: The infant’s cry is accompanied by vigorous motor activity of extremities.
• Transitional: The infant is moving between one of the previously described states. The infant may be quiet and relaxed but not very responsive to the environment.
Pain
In the past it was believed that newborns did not experience pain because of immaturity of the nerve pathways to the brain. It is now thought that fibers that conduct pain stimuli to the spinal cord are in place early in fetal life. These are called nociceptors (noci, “pain,” ceptus, “to receive”). The newborn also produces catecholamines and cortisol in response to stress. Heart rate and respiratory rates change. Blood pressure increases, and blood glucose levels rise. Newborns should be medicated for pain when discomfort is anticipated.
The nurse is responsible for understanding the physiological and behavioral responses to pain and providing appropriate pain relief measures. Untreated pain in early infancy can have long-term effects because the pain pathways and structures required for long-term memory are well developed by 24 weeks of gestation. Unrelieved pain can also cause exhaustion and irritability and slow the healing process. Some infants may be too weak to demonstrate a visible response to pain, and so behavioral responses and physiological changes must both be monitored. There are several pain assessment tools available for preterm and term infants. Pain assessment tools appropriate for the older child are discussed in Chapter 21. Examples of pain assessment tools for infants include the following:
• COMFORT scale: A 7-point scale that includes alertness, calmness, muscle tone, movement, facial tension, and respiratory response, and two physiologic items (heart rate and mean arterial blood pressure). Each item is scored from 1 to 5, with a high cumulative score indicating increased distress.
• CRIES: This 10-point scale (with each component being scored from 0 to 2) includes facial expression, cry, movement of the arms and legs, consolability, and oxygen saturation in its scoring. Letters of the acronym are defined as follows: C = cry, R = requires oxygen, I = increased vital signs, E = expression on face, S = sleeplessness.
• FLACC: This pain tool measures the pain of infants. The parameters include face, legs, activity, cry, and consolability. Each parameter is scored from 0 to 2, with a higher cumulative score indicating increased distress.
• PIPP: The Premature Infant Pain Profile is based on scales similar to the CRIES scale. This rates eye squeeze, nasal labial furrow, heart rate, oxygen saturation, and the brow furrow on a 0-to-3 scale, with 21 indicating the worst level of pain.
• NIPS: The Neonatal Infant Pain Scale is based on scales similar to the CRIES scale. This scale rates facial expression, arm movement, cry, leg movement, respiration, and arousal on a 0-to-2 scale with a score of 7 indicating the worst level of pain.
• NPASS: The Neonatal Pain, Agitation, and Sedation Scale considers the previous criteria in addition to behavior and is considered to be a very reliable and valid assessment tool, even for premature infants on ventilators. Scores are given for crying or irritability, behavioral state, facial expression, tone of extremities, vital signs, and oxygen saturation. Scores in each category range from −2 for sedated infants to +2 for agitated infants. A normal response indicating no pain or sedation is scored as 0 (zero).
The pain assessment findings should be documented and appropriate nursing interventions implemented.
Adequate pain relief in newborns who undergo painful procedures (e.g., circumcision) can reduce postoperative morbidity. Evaluation of pain in the neonate can be based on changes in vital signs and behavior of the infant and decreased oxygen saturation rates (Figure 12-8). Swaddling with the hand near the mouth, cuddling, rocking, nonnutritive sucking, and a quiet environment are noninvasive methods of pain relief for newborn infants. Oral sucrose is an effective pain reliever for minor procedures (Harrison et al., 2010). Morphine, fentanyl, and topical anesthetics can be used safely for severe pain. The nurse must be aware of safe dosage ranges and must observe infants closely for side effects or signs of withdrawal when the medication is gradually decreased and then discontinued.

FIGURE 12-8 Pain in the newborn. Note furrowed brow, clenched fist, irritability or cry, chin quiver, increased muscle tone and activity, tightly closed eyes, facial grimace, raised cheeks, deepened nasolabial fold, and open mouth. Diaphoresis; rapid, shallow respirations; and increased heart rate and blood pressure also can be observed in the neonate experiencing pain. Pain relief for the neonate during any medical procedure is very important.
Conditioned Responses
A conditioned response or reflex is one that is learned over time. It is an unconscious response to an external stimulus. An example is the hungry infant who stops crying merely at the sound of the caregiver’s footsteps, even though food is not yet available. Emotions are particularly subject to this type of conditioning. As an infant matures, the mere sight of an object that once caused pain can precipitate fear.
Neonatal Behavioral Assessment Scale
The Neonatal Behavioral Assessment Scale, developed by T. B. Brazelton (1973), has increased the understanding of the newborn’s capabilities. Among other areas of assessment, this scale measures the inherent neurological capacities of the newborn and responses to selected stimuli. Areas tested include alertness, response to visual and auditory stimuli, motor coordination, level of excitement, and organizational process in response to stress.
Respiratory System
The unborn fetus is completely dependent on the mother for all vital functions. The fetus needs oxygen and nourishment to grow. These nutrients are supplied through the bloodstream of the pregnant woman by way of the placenta and the umbilical cord. The fetus is relieved of the waste products of metabolism by the same route. The lungs are not inflated and are almost completely inactive. The circulatory system is adapted only to life within the uterus. Little blood flows through the pulmonary artery because of natural openings within the heart and vessels that close at birth or shortly thereafter.
When the umbilical cord is clamped and cut, the lungs take on the function of breathing oxygen and removing carbon dioxide. The first breath helps to expand the collapsed lungs, although full expansion does not occur for several days. The health care provider assists the first respiration by removing mucus from the passages to the lungs. The infant’s cry should be strong and healthy. The most critical period for the newborn is the first hour of life, when the drastic change from life within the uterus to life outside the uterus takes place.
Mucus may be seen draining from the nose or mouth, and it is wiped away with a sterile gauze square. Gently clearing mucus with a bulb syringe may also be indicated (Skill 12-2). When this procedure is done orally, the tip is inserted into the side of the mouth to avoid stimulating the gag reflex. Parents are taught how to use the bulb syringe and are instructed to keep one next to the newborn during the early weeks of life.
Skill 12-2 Bulb Suctioning
1. Compress the ball of the bulb syringe.
2. Insert the narrow portion of the bulb syringe into the side of the infant’s mouth to avoid stimulating the gag reflex. Suction the mouth first to prevent inhalation and aspiration of mucus during a gasp reflex, which is stimulated by nasal suctioning.
3. Release the pressure on the ball of the bulb syringe and listen for the sound of mucus being suctioned.
4. Remove the bulb syringe and empty the contents into a receptacle by compressing the bulb.
5. Compress the bulb syringe and insert into one nostril; then release pressure on the bulb to suction the mucus out.
6. Remove the bulb syringe and empty it into a receptacle. Repeat for the other nostril.
7. The nurse should demonstrate the technique of suctioning with a bulb syringe to parents and review cleaning and storage of the bulb syringe.

The nurse can assist newborns to maintain a patent airway by positioning them on their back or side and dressing them in clothing that maintains warmth while allowing expansion of the lungs. The nurse should record vital signs and suction mucus as needed, first from the mouth and throat and then from the nose.
Apgar Score
The Apgar score is a standardized method of evaluating the newborn’s condition immediately after delivery. Five objective signs are measured: heart rate, respiration, muscle tone, reflexes, and color. The score is obtained 1 minute after birth and again after 5 minutes (see Table 6-7 in Chapter 6). On admission of the newborn to the nursery, the Apgar score is reviewed to determine any particular difficulties encountered during the birth process. The health care provider’s orders are noted. The nurse must observe the newborn very closely. Respiratory distress may be evidenced by the rate and character of respirations, color (cyanosis), and general behavior (see Chapter 13). Sternal retractions are reported immediately.
Circulatory System
The mother’s blood carried essential oxygen to the placenta, which sent it to each cell of the fetus while in the uterus. The health care provider cuts off this supply by severing the umbilical cord. Thereafter the newborn depends on his or her own systemic circulation and pulmonary circulation (see Figure 3-7).
The newborn has approximately 300 mL of circulatory blood volume. The circulation of blood in the fetus differs from that in the newborn in that most fetal blood bypasses the lungs (see Chapter 3). Some of the blood goes from the right atrium to the left atrium of the heart through an opening (the foramen ovale) in the septum. Some passes from the pulmonary artery to the thoracic aorta by way of the ductus arteriosus. These normal openings close soon after birth. If they fail to close, the infant may be cyanotic because part of the blood continues to bypass the lungs and does not pick up oxygen.
Murmurs are caused by blood leaking through openings that have not yet closed. Murmurs may be functional (innocent) or organic (caused by improper heart formation). Functional murmurs result from the sound of blood passing through normal valves. Organic murmurs are caused by blood passing through abnormal openings. The majority of heart murmurs are not serious, but they should be checked periodically to rule out other pathological conditions.
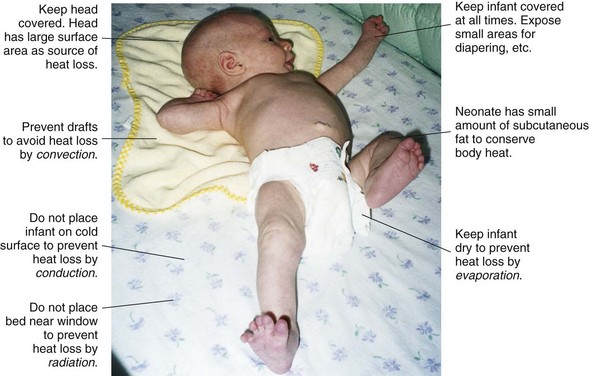
Providing Warmth
The newborn has an unstable heat-regulating system. Body temperature falls immediately after birth to about 35.5° C (96.0° F). Within a few hours, it climbs slowly to a range of 36.6° C to 37.2° C (97.8° F to 98.9° F). The body temperature is influenced by that of the room and by the number of blankets covering the infant. The temperature of the nursery, or of the mother’s room in the case of rooming-in, is kept at 21° C to 24° C (69° F to 75° F). The humidity should be between 45% and 55%. The air in the room must be fresh, but there should be no drafts.
The newborn’s hands and feet are not used as a guide to determine warmth because the infant’s extremities are cooler than the rest of the body. Acrocyanosis (acro, “extremity,” cyanosis, “blue color”) is also evident because of sluggish peripheral circulation. The newborn cannot adapt to changes in temperature. The nurse wraps the infant in a blanket whenever the infant leaves the nursery (Skill 12-3). The infant’s heat perception is poor, so the nurse must be careful when applying any form of external heat.
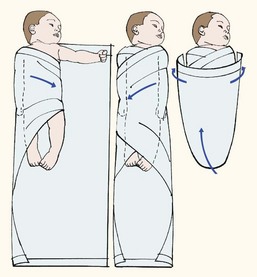
Skill 12-3 Swaddling the Newborn
1. Place a small blanket flat on the bed in the shape of a diamond, with the top corner folded down slightly.
2. Place the newborn with the shoulders at the upper edge of the blanket. The arm may be placed at the infant’s side or positioned so the hand is near the mouth. Wrap the right corner of the blanket around the newborn and tuck it under the left side of the infant. Fold the left corner of the blanket over the newborn and tuck it under the right side of the infant.
3. Pull the bottom of the blanket up to the infant’s chest and secure each corner around the newborn and under its back (snugly, not tightly).
Because the sweat glands do not function effectively during the neonatal period, the newborn infant is at risk for developing an elevated temperature if overdressed or if placed in an overheated environment. A red skin rash may develop in response to overheating. Maintaining body temperature in the newborn is summarized in Figure 12-9. See also Table 9-2.
Obtaining Temperature, Pulse Rate, and Respirations
Some birth facilities recommend that the initial temperature of the newborn be taken by rectum to determine that the rectum is patent. When the temperature is taken rectally, the nurse must be gentle to avoid injuring the rectal mucosa. Daily routine temperatures are taken by axilla. To obtain the axillary temperature, the thermometer is held firmly in the center of the newborn’s axilla. During this time, the arm is held against the infant’s side. Digital thermometers are read when the indicator sounds.
The newborn’s pulse rate and respirations are counted before the temperature is taken because the infant is apt to cry when disturbed. Figure 12-10 illustrates the apical pulse rate being obtained from a newborn infant. The newborn’s pulse is irregular and rapid and varies from 110 to 160 beats/min. Blood pressure is low and may vary with the size of the cuff used. The average blood pressure at birth is 80/46 mm Hg. The respirations are approximately 30 to 60 breaths/min. The nurse always reports the following changes:

Musculoskeletal System
The bones of the newborn are soft because they are composed mostly of cartilage, in which there is only a small amount of calcium. The skeleton is flexible, and the joints are elastic to accommodate the passage through the birth canal. Because the bones of the infant are easily molded by pressure, the infant’s position must be changed frequently. If the infant lies constantly in one position, the bones of the head can become flattened.
The movements of the newborn are random and uncoordinated. Most newborns appear cross-eyed because their eye muscle coordination is not fully developed. The newborn lacks the muscular control to hold the head steady. The development of muscular control proceeds from head to foot and from the center of the body to the periphery (see the discussion of cephalocaudal and proximodistal control in Chapter 15). Therefore the infant holds the head up before sitting erect. In fact, the head and neck muscles are the first ones to come under control. The newborn’s legs are small and short and may appear bowed. There should be no limitation of movement. Fingers clenched in a fist should be separated and observed.
An examination of the newborn for gestational maturity includes checking for the scarf sign (see Figure 13-3, D). This refers to the full-term infant’s resistance to attempts to bring one elbow farther than the midline of the chest. No resistance is observed in the preterm infant.
The infant needs freedom of movement. The infant stretches, sucks, and makes faces and vigorously moves the entire body when crying. Tremors of the lips and extremities during crying are normal. Constant tremors during sleep may be pathological. These are often accompanied by eye movements, are not related to particular stimuli, and should be reported to the health care provider. The morning bath provides excellent opportunities for the newborn to exercise and the nurse to inspect and assess the infant’s condition. When handled, the infant should not feel limp. General body proportions are observed in the following section. Bathing is also an excellent form of stimulation for the newborn.
Length and Weight
The length of the average newborn is 46 to 56 cm (19 to 21.5 inches). The weight varies from 2722 to 4082 g (6 to 9 lb). In general, girls weigh a little less than boys. African American, Asian American, and Native American infants may be somewhat smaller. In the first 3 to 4 days after birth, the infant loses about 5% to 10% of the birth weight. This loss may be as high as 15% for preterm infants. This may result from withdrawal from maternal hormones, fluid shifts, and the loss of feces and urine. Mothers should be prepared for this and reassured that the weight will normalize after 3 or 4 days and that the infant will regain his or her birth weight by 10 days of age. Newborns are weighed at the same time each day, when morning care is given. (Instructions for measuring and weighing the infant are provided in Figure 12-11 and Chapter 15.)

FIGURE 12-11 Weighing the infant. Note the barrier placed under the infant and the nurse’s hand held above the infant for safety and protection. The scale used may be a balance scale or digital scale that locks in and displays the weight in pounds and/or kilograms. Gloves should be worn when handling a nude infant. (Courtesy Pat Spier, RN-C.)
Genitourinary System
The kidneys function at birth but are not fully developed. The glomeruli are small. Renal blood flow is only about one third that of the adult. The ability to handle a water load is reduced, as is the excretion of drugs. The renal tubules are short and have a limited capacity for reabsorbing important substances such as glucose, amino acids, phosphate, and bicarbonate. There is a decrease in the ability to concentrate urine and to cope with fluid imbalances. It is important to note the first voiding of the newborn. This may occur in the delivery room or may not occur for several hours. If voiding does not occur within the first 24 hours, the health care provider is notified. The nurse must keep an accurate record of the frequency of urination. Anuria, changes in color, and any unusual findings are brought to the attention of the health care provider. The newborn should have about six wet diapers per day.
Male Genitalia
The genitalia of the male are developed at birth, although their maturation varies. The testes of the male descend into the scrotum before birth. Occasionally, they remain in the abdomen or the inguinal canal. This condition is called cryptorchidism, or undescended testes, and is described in Chapter 29. With proper surgical treatment, the prognosis is good. The location of the urethral opening should be at the tip of the penis in newborn boys. A white cheesy substance called smegma is found under the foreskin and is thought to be bacteriostatic. The school-age child can be taught to retract the foreskin gently about once a week during routine bathing. Full retraction may not be possible before puberty.
Circumcision: Circumcision is the surgical removal of the foreskin on the penis. Circumcision has both advantages and disadvantages. The disadvantages include infection and hemorrhage. Infants with congenital anomalies of the penis, such as hypospadias (the opening of the urethra is on the undersurface of the penis), should not be circumcised because the skin may be needed for surgery. The benefits of circumcision include possible prevention of cancer, fewer urinary tract infections, and fewer occurrences of sexually transmitted disease later in life.
A discussion of the pros and cons of this procedure is included as part of prenatal and postpartum education. The American Academy of Pediatrics (AAP) position on circumcision states, “Existing scientific evidence demonstrates potential medical benefits of newborn male circumcision, however, these data are not sufficient to recommend routine neonatal circumcision” (AMA, 2005). Regardless of whether the male is circumcised, at an appropriate age he is taught daily hygiene of the genitalia. This includes special attention to skin folds, retraction and replacement of the foreskin, cleansing of the penis, and examination for lumps or swelling of the penis or the scrotum.
The infant should be physiologically stabilized before circumcision. The newborn is restrained on a circumcision board (Figure 12-12, A). The Gomco clamp and the Plastibell clamp are two devices commonly used for performing circumcisions. If the Gomco clamp is used, a thin layer of petroleum jelly (Vaseline) or petroleum jelly–impregnated gauze may be applied to the end of the penis to protect it from moisture and from sticking to the diaper. The area is observed for bleeding, infection, and irritation. Voidings are recorded.

FIGURE 12-12 Circumcision. A, A circumcision board is used to restrain the newborn during circumcision in the hospital, which is usually done by the obstetrician without the family present. EMLA (eutectic mixture of local anesthetics) is a local skin anesthetic that may be used before the procedure. A sucrose-sweetened pacifier is a helpful pain relief measure during this procedure. B, A ritual circumcision. In the Jewish faith, a circumcision is called a bris milah and is performed at home on the eighth day of life. It is performed by a specially trained individual called a mohel (seen in this picture wearing a tollis, or religious scarf). The person who restrains the newborn during the procedure is known as the sandek (pictured on the left); this honor is often bestowed on an elder in the family. The presence of a minimum of 10 adults is customary, but not required, for the ceremony. A few drops of the wine in the foreground are fed to the newborn by a nipple for pain relief during the procedure. The naming ceremony is often combined with the circumcision ceremony. Understanding and respecting the rituals and traditions of others is an integral part of cultural competence. Written instructions concerning the care of the circumcised penis should be given to the parents in a language they understand.
When a Plastibell clamp is used, the foreskin is tied over a fitted plastic ring and the excess prepuce cut away. The rim usually drops off 5 to 8 days after circumcision. Parents are instructed not to remove it prematurely. No special dressing is required, and the infant is bathed and diapered as usual. A dark brown or black ring encircling the plastic rim is natural. This disappears when the rim drops off. Parents are instructed to consult their physician if there are any questions, if there is increased swelling, or if the ring has not fallen off within 8 days; parents should contact their physician immediately if the ring has slipped onto the shaft of the penis. The Jewish religious custom of circumcision, comparable to baptism in the Christian faith, is performed on the eighth day after birth if the newborn’s condition permits. The infant usually receives his Hebrew name at that time (see Figure 12-12, B). Families of the Muslim faith also favor circumcision, and it is considered to be a rite of passage for many African tribes.
The nurse’s role in circumcision includes assessing parental knowledge, checking to see that the surgical consent has been signed, and preparing the newborn. The infant is not fed for 1 to 2 hours before the procedure to prevent possible vomiting and aspiration. A bulb syringe is kept handy in case suctioning is required. A light blanket is placed under the infant on the “circ” board, and the diaper is removed. A heat lamp is positioned to prevent cold stress, or the infant may be placed in a radiant warmer. The physician may administer a local anesthetic to minimize pain during the procedure and to prevent irritability and sleep disturbances after it. Additional comfort measures include holding and soothing the infant and using a pacifier or a small amount of sucrose solution. If bleeding occurs, gentle pressure is applied to the site with a sterile gauze pad and the physician is notified. The amount and characteristics of the urinary stream are recorded, because edema could cause an obstruction. Parents should be provided with written instructions concerning the care of the circumcised or uncircumcised penis.
 Patient Teaching
Patient Teaching
Home Care of the Penis
Care of the Uncircumcised Penis
Avoid forcefully pulling back the foreskin over the glans (retraction).
Wash penis with water. White lumps (smegma) are normal.
At toddler age, gentle retraction after bathing prevents moisture collection; be sure to replace foreskin after retraction.
At school age, the child can be taught to gently retract foreskin for cleansing; this should be done once a week during bathing.
Female Genitalia
The female genitalia may be slightly swollen. A thin, white or blood-tinged mucus (pseudomenstruation) may be discharged from the vagina. This discharge is caused by hormonal withdrawal from the mother at birth. The nurse cleanses the vulva from the urethra to the anus, using a clean cotton ball or different sections of a washcloth for each stroke to prevent fecal matter from infecting the urinary tract. The importance of this is stressed to parents.
Integumentary System
Tissue turgor refers to the hydration or dehydration of the skin. To test tissue turgor (elasticity), the nurse gently grasps and releases the skin (Figure 12-13). It should spring back to place immediately in the well-hydrated infant. When the skin remains distorted (“tented”), tissue turgor is considered poor.

FIGURE 12-13 Testing tissue turgor. The term turgor refers to the elasticity of the skin, which is affected by the extent of hydration. The nurse tests skin turgor by gently grasping the skin. When the skin is released, it should instantly spring back into place; if it does not, tissue turgor is considered poor.
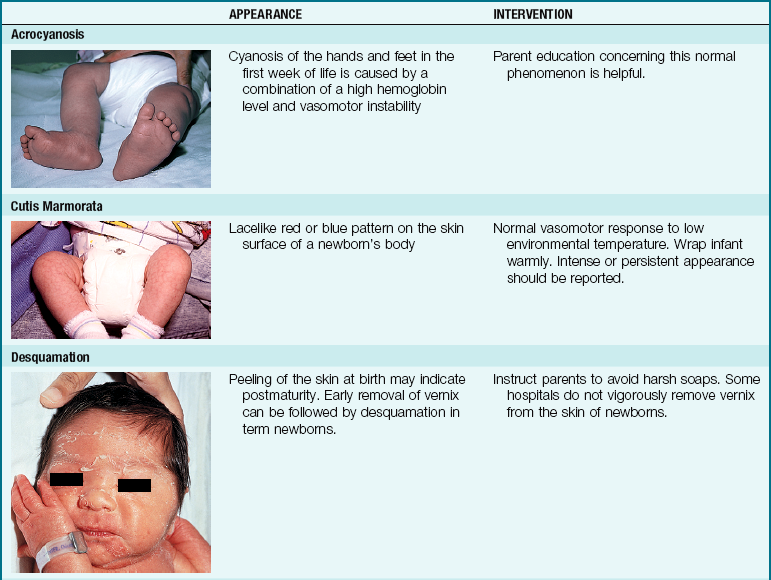
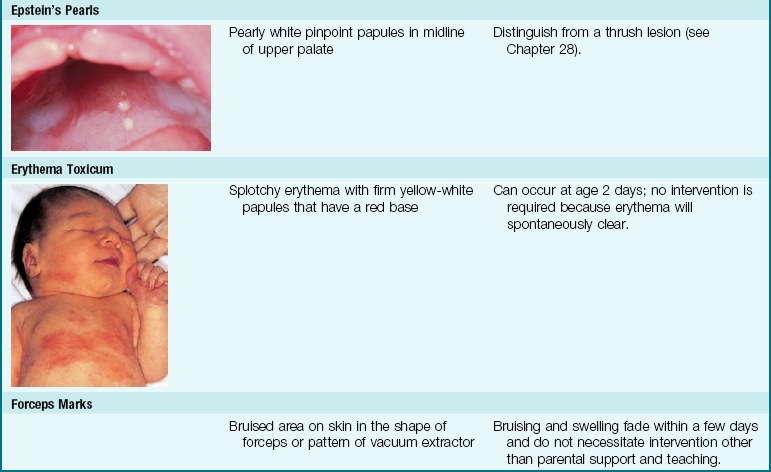
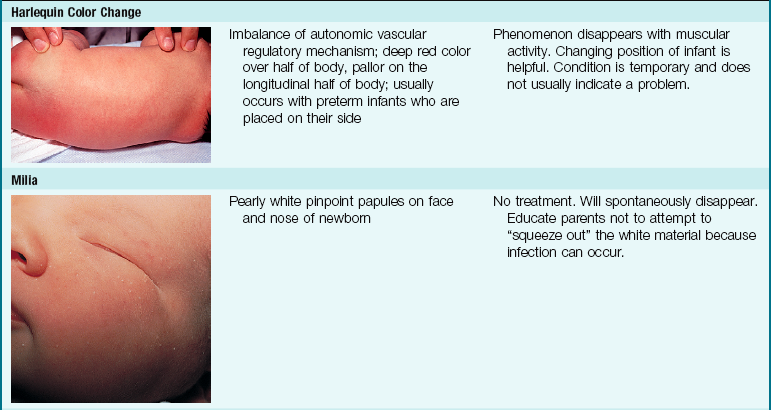
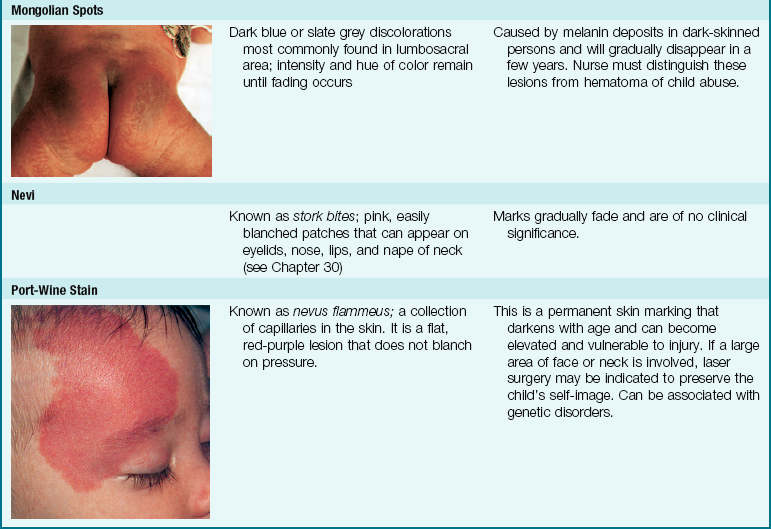
The skin of newborn Caucasian infants is red to dark pink. The skin of African American infants is reddish brown. Infants of Latin descent may appear to have an olive or yellowish tint. The body is usually covered with fine hair called lanugo, which tends to disappear during the first week of life. This is more evident in premature infants. Vernix caseosa, a cheeselike substance that covers the skin of the newborn, is made of cells and glandular secretions; it is thought to protect the skin from irritation and the effects of a watery environment in utero (Figure 12-14). White pinpoint “pimples” caused by the obstruction of sebaceous glands may be seen on the nose and chin. These are called milia and disappear within a few weeks. Lesions on the midline of the hard palate of the milia type are called Epstein’s pearls and are caused by a collection of epithelial cells. Stork bites (telangiectatic nevi) are flat, red areas seen on the nape of the neck and on the eyelids. They result from the dilation of small vessels. See Table 12-3 for other skin manifestations seen in the newborn.

FIGURE 12-14 Vernix is the thick, white, cheesy substance covering the skin of the newborn. Preterm newborns are heavily covered in vernix whereas postterm newborns have little vernix protection on their skin. Note the heavy covering of vernix on this newborn.
Mongolian spots, bluish discolorations of the skin, are common in infants of African American, Native American, and Mediterranean descent. They are usually found over the sacral and gluteal areas (see Table 12-3). They disappear spontaneously during the early years of life. Mongolian spots can be differentiated from a hematoma due to abuse because the hematoma will change color each day, but the Mongolian spot remains the same color and hue.
Acrocyanosis, or peripheral blueness of the hands and feet, is normal and results from poor peripheral circulation. The hands or feet should not be used to determine general body warmth in the newborn. Central body areas are not cyanotic in normal newborns. Pallor is not normal and should be reported because it may indicate neonatal anemia or another more serious condition.
Desquamation, or peeling of the skin, occurs during the early weeks of life. Skin in areas such as the nose, knees, elbows, and toes may break down because of friction from rubbing against the sheets. The involved area is kept dry, and the infant’s position is changed frequently. The buttocks need special attention. A wet diaper should be changed immediately to prevent chafing. The buttocks are washed and dried well.
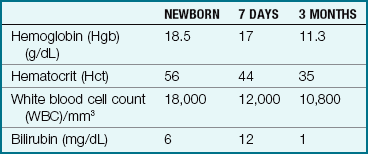
Physiological jaundice, also called icterus neonatorum, is characterized by a yellow tinge of the skin. It is caused by the rapid destruction of excess red blood cells, which the infant does not need now because he or she is in an atmosphere that contains more oxygen than was available during prenatal life. Plasma levels of bilirubin increase from a normal 1 mg/dL to an average of 5 to 6 mg/dL between the second and fourth days (Table 12-2). Physiological jaundice becomes evident between the second and the third days of life and lasts for about 1 week. This is a normal process and is not harmful to the infant. However, genetic and ethnic factors may affect its severity, resulting in pathological hyperbilirubinemia. Evidence of jaundice is reported and charted, and the newborn is evaluated frequently to ensure safety (Skill 12-4).
Skill 12-4 Assessing for Jaundice
1. Observe skin in a well-lit room.
2. Press skin over the nose or sternum with the thumb until the skin blanches (lightens).
3. Observe the level of jaundice. (Note: There is a cephalocaudal progression of jaundice in term infants. As the bilirubin level increases, the jaundice progresses from the head toward the feet [Slusher, 2004].)
4. Jaundice seen below the sternum or present in the arms, lower abdomen, or feet may indicate that a serum bilirubin test is required (Kliegman et al., 2007).
Two commonly used methods to assess jaundice are the following:
1. Icterometer: The icterometer is a plastic strip with increasingly deeper yellow stripes representing levels of jaundice. The strip is placed against the infant’s nose until the skin blanches. The underlying skin tone is matched to the corresponding shade of yellow.
2. Transcutaneous bilirubin measurement (TcB): Transcutaneous measurement of jaundice is noninvasive. The Colormate III bilirubinometer has been approved by the U.S. Food and Drug Administration (FDA) as a screening device to determine if a more accurate blood test is indicated. The machine is unaffected by the level of melanin in the skin (Maisels et al., 2004).
Table 12-3 discusses nursing interventions for common skin manifestations of the newborn infant.
The Interactive Bath
Initial skin care after the newborn is stable involves washing blood, amniotic fluid, and excessive vernix from the skin. Until the infant’s first bath and shampoo, the nurse wears gloves when handling the newborn, as described in Skill 12-5 on p. 296. The bath provides an opportunity for teaching as well as assessment of the infant and infant-parent interaction. The nurse should emphasize certain basic principles of care such as hand hygiene, cleansing the tub, organizing supplies to be within easy reach, safe water temperature, and techniques for holding the wet infant securely.
Skill 12-5 Bathing the Newborn
To cleanse the skin and interact with the newborn
A sponge bath may be given until the umbilical cord site and circumcision site are healed; however, tub baths can be given before the cord falls off without risk of infection (Association of Women’s Health, Obstetric and Neonatal Nurses [AWHONN], 2007).
• Give bath between feedings at most convenient time for baby and family.
• Complete baths are not necessary more than two or three times a week because specific areas are washed after diaper changes and when milk is spit up.
• After the bath, the baby will likely want to sleep.
• A bath should not be given immediately after feeding since excessive handling may cause regurgitation.
• Carefully wash and dry each area to prevent heat loss.
• Keep the baby warm by exposing only the area you are washing.
1. Test bath water. (It should be approximately 37.2° to 38° C [99° to 100.4° F]). A bath thermometer should be used; many have preset temperature alerts.
2. Proceed from the cleanest to the most soiled area of the body: from eyes and face to the trunk and extremities and finally to the diaper area. Shampooing of the hair is always done last to prevent excessive heat loss from the head.
a. Wash the baby’s face with clear water. Use a separate clean area of the washcloth (or use cotton ball) to wipe each eyelid. Use a clean area to wash outer ear (do not put anything inside ear or nose).
b. Wash behind ears, where milk that is spit up may accumulate.
c. If necessary, clean nose with a clean corner of the washcloth.
d. Put hand under the baby’s shoulders and lift slightly. This allows the creases of the neck to be washed.
e. Wash the vulva of a female newborn by wiping from front to back to prevent contamination of the vagina or urethra by rectal content. In the male newborn, do not force back the foreskin of the uncircumcised penis. Clean the penis and scrotal area gently. It is important to clean under the scrotum and the folds of the scrotum.
f. The easiest way to wash the hair is to hold the baby (wrapped in a towel to prevent chilling) in one arm using the football hold over the basin of water. Soap hair and rinse by pouring water from a container over the head. Then dry hair to prevent chilling.
1. Use a plastic tub or a clean sink for the bath.
2. Place a small blanket or pad at the bottom of the tub for comfort and to prevent slipping.
3. Place approximately 3 to 4 inches of warm water in the tub. The water temperature should be 36.6° to 37.2° C (98° to 99° F).
4. Using a clean, dampened washcloth, wash eyes and face with plain water.
5. Place the baby in the tub. The baby may seem frightened and cry when first put in the water. Holding the baby securely and talking with a soft voice will often help baby adjust to the bath, which is a new experience.
6. Be sure all soap is rinsed off the baby before removing him or her from the tub.
7. Remove newborn from the tub and immediately wrap in a dry towel.
8. With the baby wrapped in a towel and held in a football hold, gently shampoo the hair; rinse thoroughly with warm water and dry with a clean towel.

Principles of eye and ear care are reviewed. Cotton swabs should not be inserted into the ear or the nose. Alkaline soaps, oils, and lotions are not advised as they can alter the normal pH of the newborn’s skin, making it vulnerable to bacterial infection. Powders should be avoided because of the high risk of aspiration of small particles. Some health care providers advise giving sponge baths until the cord falls off and heals (about 1 to 2 weeks), but tub baths are acceptable. The infant need only be bathed 2 or 3 times a week using plain warm water during the neonatal period. Daily bathing with soap and water is no longer recommended (Association of Women’s Health, Obstetric and Neonatal Nurses [AWHONN], 2007). The bath is an excellent time to provide basic hygiene and to observe the naked newborn for behavior, muscle activity, and general well-being.
The temperature of the bath water should be approximately 37.8° C (100° F) in a warm room environment at 24° C to 27° C (75° F to 80° F). Special care should be taken to keep the infant covered to prevent chilling. Parents should be taught to start bathing the face and then proceed in a cephalocaudal (head-to-toe) direction, turning the surface of the washcloth as the bath progresses. The eyes should be cleansed with a moist cotton ball from the inner canthus to the outer canthus, using a clean cotton ball for each eye. The genitalia should be cleansed with a front-to-back motion to prevent urinary tract infection.
The nurse may wrap the infant in a towel and use a football hold to shampoo the hair. The shampoo is given last because the large surface area of the head predisposes the infant to heat loss. Observing the cues and responses of the infant to the warmth of the water and the touch of the washcloth, drying and dressing are discussed with the parent in relation to opportunities to promote parent-infant bonding during the bath experience. The general principles of the infant bath should be explained to parents to foster good techniques at home. Cord care is discussed in Chapter 9 (see Skill 9-6).
 Nursing Tip
Nursing TipGastrointestinal System
The intestinal tract functions as an outlet for amniotic fluid as early as the fifth month of fetal life. The normal functions of the gastrointestinal tract begin after birth. Food is digested and absorbed into the blood, and waste products are eliminated. Meconium, the first stool, is a mixture of amniotic fluid and secretions of the intestinal glands. It is dark greenish black, thick, and sticky (tarry) and is passed 8 to 24 hours after birth. The stools gradually change during the first week. They become loose and are greenish yellow with mucus. These are called transitional stools (Figure 12-15).
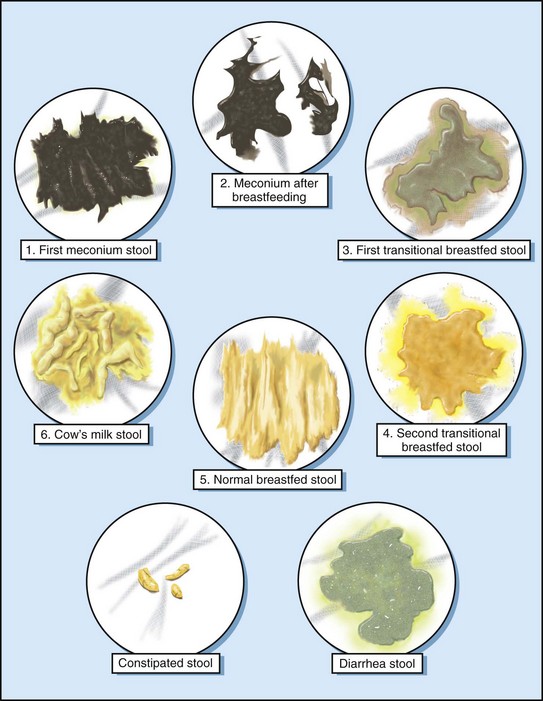
FIGURE 12-15 The normal infant stool cycle. The first meconium is dark, black, and tarry. It gradually changes to a greenish yellow transitional stool. The breastfed infant’s “milk” stool is golden yellow, whereas the bottle fed infant has a pale yellow stool. A green, watery stool is indicative of diarrhea and should be reported to the health care provider.
The stools of a breastfed infant are bright yellow, soft, and pasty. There may be three to six stools a day. The number of stools decreases with age. The bowel movements of a bottle fed infant are more solid than those of the breastfed infant. They vary from yellow to brown and are generally fewer in number. There may be one to four a day at first, but this gradually decreases to one or two a day. The stools are darker when an infant is receiving oral iron supplements, and they are green when an infant is under the phototherapy lamp. Small, puttylike stools or diarrhea and bloody stools are abnormal. When there is a question, the nurse saves the stool specimen for the physician to observe. The nurse keeps an accurate record of the number and characteristics of stools that each newborn passes daily.
Constipation
Constipation refers to the passage of hard dry stools. Newborns differ in regularity. Some pass a soft stool every other day. This is not constipation. The nurse explains to parents that straining in the newborn period results from undeveloped abdominal musculature. This is normal, and no treatment is required. In the first month of life, a breastfed infant will pass at least four stools a day. After the second month of life, the infant will increase stool volume and decrease stool frequency. Even if 5 to 6 days pass without a stool, it is not considered constipation if the stool passed is large in volume and soft or pasty in character. Constipation is sometimes seen as the infant matures and if a formula change is made. Increasing water intake may be all that is necessary to remedy this constipation. If the infant is eating solid foods, an increased intake of fruits, vegetables, and whole-grain cereals is usually sufficient. The nurse encourages mothers to telephone their health care provider’s office when questions arise and ask to speak to the nurse. This is particularly emphasized to new mothers, who may be afraid of appearing “ignorant.” Very often a simple solution can relieve hours of anxiety.
Hiccoughs
Hiccoughs appear frequently in newborns and are normal. Most disappear spontaneously. Burping the infant and offering warm water may help.
Digestion
Breastfeeding and formula feeding are discussed in Chapters 9 and 16. Breastfed infants may be put to the breast in the first hour after delivery for psychological benefits and to help stimulate milk production. Bottle feedings are begun in about 5 hours. An infant’s hunger is evidenced by crying, restlessness, fist sucking, and the rooting reflex. The capacity of the infant’s stomach is about 90 mL (3 oz). Emptying time is 2 to 3 hours, and peristalsis is rapid. Feeding the newborn often stimulates the gastrocolic reflex, which results in the infant passing a stool.
The immature cardiac sphincter of the stomach causes the young infant to be prone to regurgitation. For this reason parents should be educated to avoid overfeeding their infant and to position the infant on the right side after feeding. Deficiency of pancreatic enzymes such as lipase limits fat absorption. Breast milk contains some lipase enzyme that aids infant digestion. Whole cow’s milk does not contain this enzyme and therefore should not be fed undiluted to newborns or young infants.
The salivary glands do not secrete saliva until the infant is age 2 to 3 months. Drooling in the newborn is considered a sign of pathological disturbance and should be reported. The liver is immature, especially in its ability to conjugate bilirubin, regulate blood glucose, and coagulate blood.
Vitamins
Infants need extra vitamins C and D. Breast milk contains sufficient vitamin C if the mother’s diet is rich in citrus fruits and certain vegetables. Vitamin D may be added to commercial milk (labeled “vitamin D milk”) that the mother consumes. Commercial concentrated vitamin preparations may also be prescribed. The fluid is drawn up in the dropper to the prescribed amount (0.3 or 0.6 mL) and is placed directly in the infant’s mouth. This is done each morning at approximately the same time to prevent forgetting the vitamins.
Preventing Infection
Infections that are relatively harmless to an adult may be fatal to the newborn. The newborn’s response to inflammation and infection is slow because of the immaturity of the immune system, as follows:
• Immunoglobulin G (IgG) is an immunoglobulin that crosses the placenta and provides the newborn with passive immunity to infections to which the mother was immune. This type of immunity rarely lasts longer than 3 months.
• Immunoglobulin M (IgM) is an immunoglobulin produced by the newborn, and an elevated level suggests serious infection.
• Immunoglobulin A (IgA) is an immunoglobulin produced after the neonatal period (about age 1 month) that is contained in breast milk and provides some resistance to respiratory and gastrointestinal infections. Before age 1 month, infants are at risk for such infections.
An open wound (such as the umbilical cord) can be a portal of entry for infection. Measures to prevent infections in the newborn nursery include using standard precautions, handwashing, cleansing and replacement of equipment, and proper disposal of soiled diapers and linens. Nursery standards are developed and enforced by various professional agencies, such as the AAP, hospital accreditation boards, and local health agencies. The infection control nurse in each hospital also provides education and surveillance. Provisions governing space, control of temperature and humidity, lighting, and safety from fire and other hazards are also considered. Each newborn has an individual crib, bath equipment, and linen supply.
Handwashing is the most reliable precaution available. The nursery nurse washes his or her hands between handling different babies. The nurse stresses to parents the need for proper handwashing in the home. In many hospitals, nursery personnel wear clean scrub gowns while in the nursery for the purpose of infection control and/or security. Health care providers, technicians, and other nonnursery personnel wear cover gowns when entering the nursery and handling infants.
Health examination of personnel before employment minimizes the spread of infection by unhealthy persons. The nurse who has signs of a cold, earache, skin infection, or intestinal upset should not work in the nursery or care for ill children. Visitors are instructed not to come to the hospital or be around hospital patients if they are not feeling well.
Discharge Planning and Parent Teaching
Discharge teaching ideally begins with the admission of the woman to the hospital or birthing center. Many hospitals have flowsheets, which are helpful in ensuring that all topics have been addressed and that patients understand what has been explained to them. Areas of teaching include the following:
• Basic care of the infant, including bathing, cord care, circumcision care, feeding, and elimination
• Safety measures including position for sleep
• Support groups, such as La Leche League
• Return appointments for well-baby care
• Telephone number of nursery (note 24-hour availability)
• Proper use of car safety seats (see Figure 9-14)
• Signs and symptoms of problems and who to contact; for example, temperature greater than 38° C (100.4° F) by axilla, refusal of two feedings in a row, two green watery stools, frequent or forceful vomiting, lack of voiding or stooling
The nurse should guide the parents in assessing, bathing, and feeding the newborn so that questions can be answered early and parents can demonstrate understanding of skills and behaviors. Clinical Pathway 12-1 specifies nursing interventions for assisting the mother, the parents, or other caregivers in caring for the infant before and after discharge from the hospital.

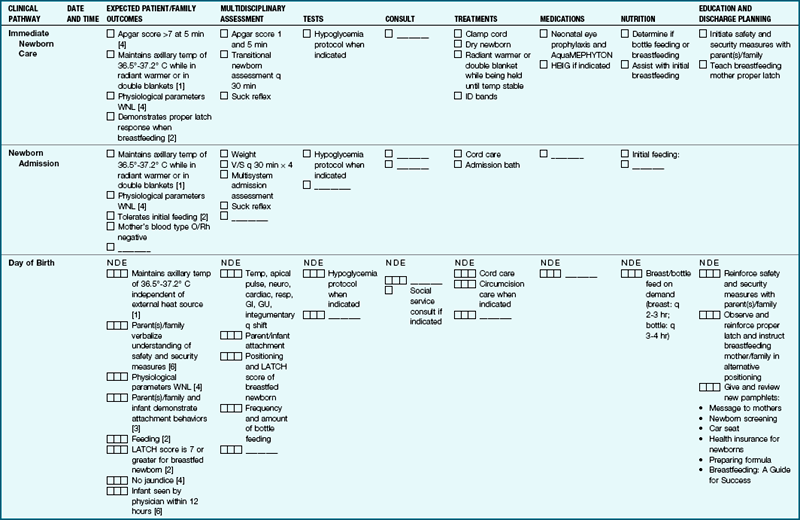
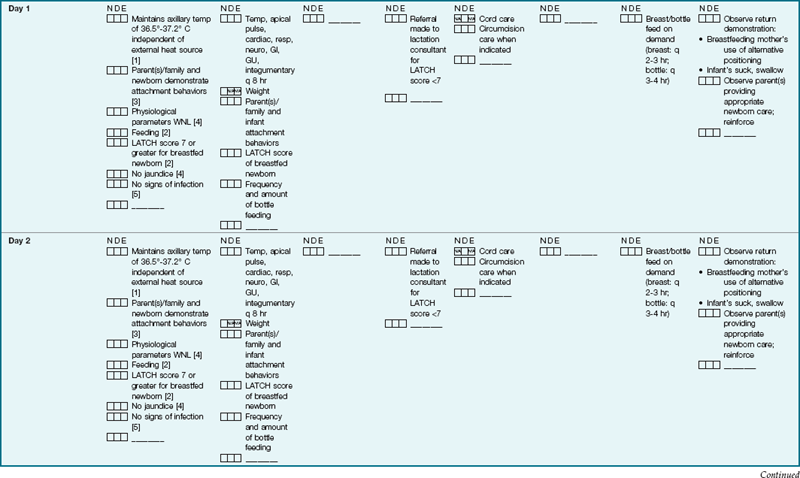
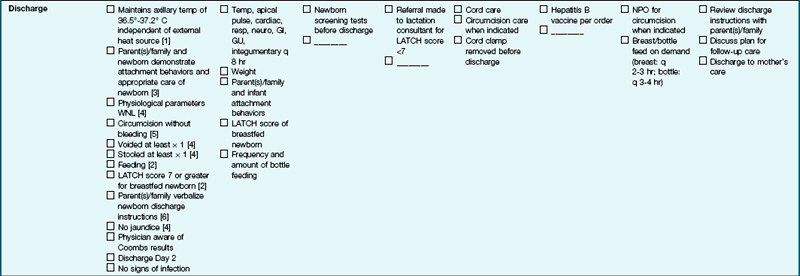
An example of a clinical pathway for a newborn from birth to discharge on the second day. This is used by all caregivers to plan and document care. (Courtesy Women’s and Children’s Services of the York Health System. York, PA. Modified with permission.)
Note: Each patient requires an individual assessment and treatment plan. This clinical pathway is a recommendation for the average patient that requires modification when necessary by the professional staff.
Home Care
Feeding: Feeding the newborn is discussed in Chapter 9.
Furnishings: It helps if the newborn has a separate room or a separate area within a room. Simple, durable, easy-to-clean furnishings are necessary. A crib with a firm mattress is a suitable place for the infant to sleep. Crib slats should adhere to safety standards. Mattress covers are usually waterproof. Fitted sheets are convenient, and blankets of lightweight cotton are warm and easy to launder. A pillow should not be placed in the crib of the newborn for safety reasons.
 Safety Alert!
Safety Alert!
Instruct parents about the danger of suffocation if the infant sleeps in the same bed with the parents.
Pictures should be attached securely to the wall with wall tape. Thumbtacks may be swallowed by the growing child. A chest of drawers for clothing, an adult chair (preferably a rocker), and a flat-topped table for changing clothes are necessary. A plastic basin may be used for the first few months to bathe the infant. A tray containing frequently used articles saves time and energy. These items might include a digital thermometer, hairbrush and comb, baby wipes, and baby lotion. A separate linen hamper for the infant’s clothes and a closed receptacle for soiled diapers are also necessary.
Clothing: Clothing must be soft, washable, of the proper size, and easy to put on and take off. Parents are instructed to launder new clothing and sheets before using them to prevent skin irritation. Use of nightgowns with drawstring necks is avoided because they may lead to strangulation. Buttons must be sewn on tightly. Snaps or Velcro fasteners are safer. If the mother does not have a clothes dryer, she needs a clothes rack to dry the infant’s garments during inclement weather.
Disposable diapers are most commonly used in hospitals and homes. They have an outer waterproof layer. Diapers made of gauze, knitted cotton, or bird’s-eye or cotton flannel are available in contoured shapes or prefolded styles. However, they take longer to dry when laundered at home and are more costly. Diaper liners are specially treated tissues placed within the cloth diaper. When diapers are soiled, the liner and stool are rinsed into the toilet. The diapers are soaked in cold water, washed with a mild laundry soap, rinsed thoroughly, and dried by a clothes dryer or outdoors in the sun. Diapers that have been improperly washed and rinsed may aggravate rashes. If a rash is present, the buttocks are kept exposed to the air as often as possible. Diapers are changed as soon as they are wet. If a rash becomes increasingly worse, the health care provider is consulted.
The quantity of items that the mother needs is determined by her washing facilities and the climate of the area in which she lives. Figure 12-16 shows how the diaper is folded so that the edge is below the umbilical cord stump in order to keep the cord clean and dry. Figure 12-17 illustrates the simplest way to dress the newborn.

FIGURE 12-16 Note that the diaper is folded so that it does not touch the umbilical cord stump. The umbilical cord stump is kept dry and usually falls off between 8 and 10 days after delivery.
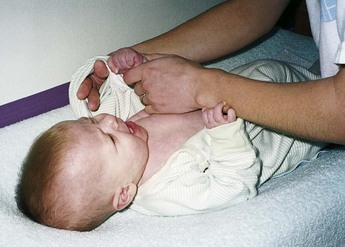
FIGURE 12-17 Dressing the newborn. The simplest technique of dressing the newborn is to place the hand through the sleeve, grasp the infant’s hand, and gently pull it through the sleeve.
The social service department may be of help in ensuring that the home environment is satisfactory and that any special needs of the infant or parent are met. The home health nurse is a key member of the interdisciplinary health care team who can help with after-discharge needs of the family.
Get Ready for the NCLEX® Examination!
Key Points
• Assessment of the newborn includes gestational age, weight and length measurements, reflexes, system assessment, and bonding with parents.
• Heat loss occurs in the newborn via conduction, convection, evaporation, and radiation.
• The newborn is born with certain reflexes. Three of these are the Moro reflex, the rooting reflex, and the tonic neck reflex.
• The Apgar score is a standardized method of evaluating the newborn’s condition at 1 and 5 minutes after delivery. Five objective signs are measured: heart rate, respirations, muscle tone, reflexes, and color.
• The most critical period for the newborn is the first hour of life, when the drastic change from life within the uterus to life outside it takes place.
• Physiological jaundice becomes evident after the second and third days of life and lasts for about 1 week.
• The newborn has an unstable heat-regulating system and must be kept warm.
• Although the kidneys function at birth, they are not fully developed. Likewise, the immune system is not fully activated.
• Vernix caseosa is a cheeselike substance that covers the skin of the newborn at birth.
• Meconium, the first stool of the newborn, is a mixture of amniotic fluid and secretions of the intestinal glands. These stools change in color from tarry greenish black, to greenish yellow (transitional stools), to yellow-gold (milk stools).
• Proper handwashing is essential for preventing infection in newborn infants.
• Nursery standards are developed and enforced by various professional agencies.
• The hydration status of newborns can be evaluated by determining the number and consistency of stools, frequency of voiding, appearance of sunken fontanelles, and status of tissue turgor.
• The normal newborn infant will lose about 10% of the birth weight in the first few days of life but will return to the birth weight by age 10 days.
• The fontanelles are spaces between the skull bones of the newborn that allow for molding and provide space for the brain to grow. They are known as “soft spots” on the infant’s head.
• Caput succedaneum is edema of the infant’s scalp that occurs during the birth process.
• Cephalhematoma is a collection of blood under the periosteum of a cranial bone. The swelling does not cross the suture lines of the skull bones.
• The goal of the infant bath is to cleanse the skin and to assess the newborn.
• Discharge teaching begins before birth and continues to discharge date. It includes infant care, follow-up visits, evaluation of support systems, and use of car safety seats.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Circumcision: www.cirp.org; www.circinfo.com/prepandcare/ccc.html
• Growth and development: www.cdc.gov/growthcharts
• Newborn care: www.parenthood.com
• Tips for parents: www.healthvideo.com/childrens-health
Review Questions for the NCLEX® Examination
1. The mother of a newborn reports to the nurse that her infant has had a black tarry stool. The nurse would tell the mother that:
1. this is most likely caused by blood the infant may have swallowed during the birth process.
2. the health care provider will be promptly notified.
3. the infant will be given nothing by mouth (remain NPO) until a stool culture is taken.
2. The soft spots on a newborn’s head are termed:
3. Infections in the newborn require prompt intervention because:
2. infections that are relatively harmless to an adult can be fatal to the newborn.
4. The mother states that her newborn has white pinpoint “pimples” on his nose and chin and she plans to squeeze them to make them disappear. The best response of the nurse would be:
1. “Be sure to wipe the area with an alcohol sponge to avoid infection.”
2. “Ask your health care provider to prescribe an antibiotic ointment for the pimples.”
3. “These pimples are called ‘Epstein’s pearls’ and are a normal occurrence.”
4. “These pimples are called ‘milia’ and will disappear on their own in a week or two.”
5. Which observation of the newborn should be reported to the health care provider as soon as possible?
Critical Thinking Question
1. A new mother brings her 5-day-old infant to the clinic and states she wants to stop breastfeeding and start formula because her infant weighs less now than he did at birth. She states that her breasts are small anyway so she probably is not providing enough milk to help him gain weight. What is the best response of the nurse?