CHAPTER 17 Occlusal Relationships for Removable Partial Dentures
The fourth phase* in the treatment of patients with removable partial dentures is the establishment of a functional and harmonious occlusion. Occlusal harmony between a removable partial denture and the remaining natural teeth is a major factor in the preservation of the health of their surrounding structures. In the treatment of patients with complete dentures, the inclination of the condyle path is the only factor not within the control of the dentist. All other factors may be altered to obtain occlusal balance and harmony in eccentric positions to conform to a particular concept and philosophy of occlusion.
Balanced occlusion is desirable with complete dentures because unbalanced occlusal stresses may cause instability of the dentures and trauma to the supporting structures. These stresses can reach a point that causes movement of the denture bases. In removable partial dentures, however, because of the attachment of the removable partial denture to the abutment teeth, occlusal stresses can be transmitted directly to the abutment teeth and other supporting structures, resulting in sustained stresses that may be more damaging than those transient stresses found in complete dentures. Failure to provide and maintain adequate occlusion on the removable partial denture is primarily a result of (1) lack of support for the denture base, (2) the fallacy of establishing occlusion to a single static jaw relation record, and (3) an unacceptable occlusal plane.
In establishing occlusion on a removable partial denture, the influence of the remaining natural teeth is usually such that the occlusal forms of the teeth on the removable partial denture must be made to conform to an already established occlusal pattern. Occlusal adjustment or restoration may have altered this pattern. However, the pattern present at the time the removable partial denture is made dictates the occlusion on the removable partial denture. The only exceptions are those in which an opposing complete denture can be made to function harmoniously with the removable partial denture, or in which only anterior teeth remain in both arches and the incisal relationship can be made so that tooth contacts do not disturb denture stability or retention. In these situations, jaw relation records and the arrangement of the teeth may proceed in the same manner as with complete dentures, and the same general principles apply.
With all other types of removable partial dentures, the remaining teeth dictate the occlusion. The dentist should strive for planned contacts in centric occlusion and no interferences in lateral excursions. Although a functional relationship of the removable partial denture to the natural dentition sometimes may be adjusted satisfactorily in the mouth, extraoral adjustment is often easier for both dentist and patient, is more accurate, and can be accomplished in a more comprehensive manner.
Establishment of a satisfactory occlusion for the removable partial denture patient should include the following: (1) analysis of the existing occlusion; (2) correction of existing occlusal disharmony; (3) recording of centric relation or an adjusted centric occlusion; (4) harmonizing of eccentric jaw movements for a functional eccentric occlusion; and (5) correction of occlusal discrepancies created by the fit of the framework and during processing of the removable partial denture.
Desirable Occlusal Contact Relationships for Removable Partial Dentures
The following occlusal arrangements are recommended to develop a harmonious occlusal relationship among removable partial dentures and to enhance stability of the removable partial dentures:

Figure 17-1 Posterior occlusion of a maxillary complete denture opposing a Class I mandibular removable partial denture. The stability of the maxillary complete denture can be promoted by developing balanced occlusion as shown.

Figure 17-2 Bilateral distal extension mandibular removable partial denture opposed by natural dentition in the maxillary arch. Working contacts are achieved, balancing contacts are purposefully avoided because they would not enhance the stability of the restoration, and protrusive balance is avoided in favor of an acceptable appearance and a favorable occlusal plane.
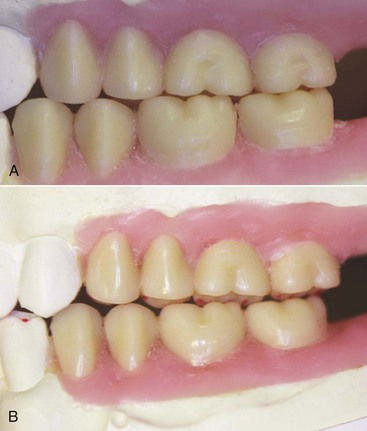
Figure 17-3 Opposing Class I partially edentulous arches arranged to allow working side contacts of opposing posterior teeth with balancing contact arranged to minimize tipping of the maxillary removable partial denture and to broadly distribute forces accruing to its supporting structures (abutments and residual ridges).

Figure 17-4 When occlusion is developed for a Class II removable partial denture (maxillary or mandibular), only working side contacts are necessary, as the cross-arch framework stability gained from tooth engagement provides resistance to movement. Balancing side contacts do not enhance stability beyond that provided by the contralateral teeth.

Figure 17-5 Mandibular posterior teeth should not be arranged distal to the upward incline (ascending ramus) of the residual ridge. The molar tooth has been placed just anterior to a mark on the cast land area designating the beginning incline.
A harmonious relationship of opposing occlusal and incisal surfaces alone is not adequate to ensure stability of distal extension removable partial dentures. In addition, the relationship of the teeth to the residual ridges must be considered. Bilateral eccentric contact of the mandibular distal extension removable partial denture need not be formulated to stabilize the denture. The buccal cusps, however, must be favorably placed to direct stress toward the buccal shelf, which is the primary support area in the mandibular arch. In such positions, the denture is not subjected to excessive tilting forces (Figure 17-6). On the other hand, the artificial teeth of the bilateral, distal extension, maxillary removable partial denture often must be placed lateral to the crest of the residual ridge (Figure 17-7). Such an unfavorable position can cause tipping of the denture, which is restrained only by direct retainer action on the balancing side. To enhance the stability of the denture, it seems logical to provide simultaneous working and balancing contacts in these situations if possible.
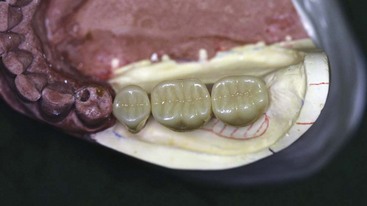
Figure 17-6 The posterior teeth in this distal extension with a narrower buccal-lingual width than the original teeth have been selected, and they are placed relative to the primary support (buccal shelf) to distribute the functional load to the most anatomically favorable location in a manner that reduces leverage effects.
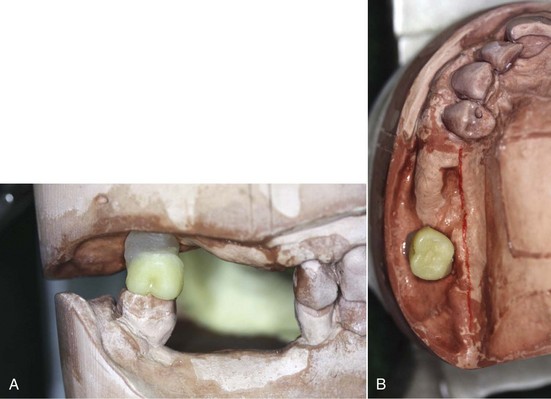
Figure 17-7 A, Maxillary molar occluded in a normal horizontal relationship to the opposing molar. B, The resultant position is lateral to the supporting crest of the residual ridge. This position is functionally unfavorable because of the potentially unstable leverage effects; however, stability can be improved by arranging simultaneous working and balancing contacts in the occlusal scheme.
Methods for Establishing Occlusal Relationships
Five methods of establishing interocclusal relations for removable partial dentures will be briefly described. Before any of these is described, it is necessary that the use of a facebow mounting of the maxillary cast and pertinent factors in removable partial denture occlusion be considered. The technique for applying the facebow has been described briefly in Chapter 12.
Although a hinge axis mounting may be desirable for complete oral rehabilitation procedures, any of the common types of facebow will facilitate mounting of the maxillary cast in relation to the condylar axis in the articulating instrument with reasonable accuracy and are acceptable for a removable partial denture. As was suggested in Chapter 12, it is still better that the plane of occlusion be related to the axis-orbital plane. Because the dominant factor in removable partial denture occlusion is the remaining natural teeth and their proprioceptive influence on occlusion, a comparable radius at the oriented plane of occlusion in an acceptable instrument will allow reasonably valid mandibular movements to be reproduced.
Semiadjustable articulators can simulate but not duplicate jaw movement. Realization of the limitations of a specific instrument and knowledge of the procedures that can overcome these limitations are necessary if an adequate occlusion is to be created.
The recording of occlusal relationships for the partially edentulous arch may vary from the simple apposition of opposing casts (by occluding sufficient remaining natural teeth) to the recording of jaw relations in the same manner as for a completely edentulous patient. As long as some natural teeth remain in contact, however, the cuspal influence that those teeth will have on functional jaw movements dictates the placement of the artificial teeth and the occlusal scheme.
The horizontal jaw relation (planned intercuspal position or centric relation) in which the restoration is to be fabricated should have been determined during diagnosis and treatment planning. Mouth preparations also should have been accomplished in keeping with this determination, including occlusal adjustment of the natural dentition, if such was indicated. Therefore one of the following conditions should exist: (1) centric relation and planned intercuspal position coincide with no evidence of occlusal pathologic conditions, therefore the decision should be to fabricate the restoration in centric relation; (2) centric relation and the planned intercuspal position do not coincide, but the planned intercuspal position is clearly defined and the decision has been made to fabricate the restoration in the planned intercuspal position; (3) centric relation and the planned intercuspal position do not coincide and the intercuspal position is not clearly defined, therefore the decision should be made to fabricate the restoration in centric relation; and (4) posterior teeth are not present in one or both arches, and the denture will be fabricated in centric relation.
Occlusal relationships may be established by using the most appropriate of the following methods to fit a particular partially edentulous situation.
Direct Apposition of Casts
The first method is used when sufficient opposing teeth remain in contact to make the existing jaw relationship obvious, or when only a few teeth are to be replaced on short denture bases and no evidence of occlusal abnormalities is found. With this method, opposing casts may be occluded by hand. The occluded casts should be held in apposition with rigid supports attached with sticky wax to the bases of the casts until they are securely mounted in the articulator.
At best, this method can only perpetuate the existing occlusal vertical dimension and any existing occlusal disharmony present between the natural dentition. Occlusal analysis and the correction of any existing occlusal disharmony should precede the acceptance of such a jaw relation record. The limitations of such a method should be obvious. Yet, such a jaw relation record is better than an inaccurate interocclusal record between the remaining natural teeth. Unless a record is made that does not influence the closing path of the mandible because of its bulk and/or the consistency of the recording medium, direct apposition of opposing casts at least eliminates the possibility that the patient may have a faulty jaw relationship.
Interocclusal Records With Posterior Teeth Remaining
A second method, which is a modification of the first, is used when sufficient natural teeth remain to support the removable partial denture (Kennedy Class III or IV) but the relation of opposing natural teeth does not permit the occluding of casts by hand. In such situations, jaw relations must be established as for fixed restorations with some type of interocclusal record.
The least accurate of these methods is the interocclusal wax record. The bulk, consistency, and accuracy of the wax will influence the successful recording of centric relation with an interocclusal wax record after chilling. Excess wax that contacts the mucosal surfaces may distort soft tissue, thereby preventing accurate seating of the wax record onto the stone casts. Distortion of wax during or after removal from the mouth may also interfere with accurate seating. Therefore a definite procedure for making interocclusal wax records is given as follows:
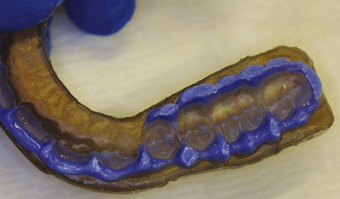
Figure 17-8 A wax wafer softened in a water bath is used to register interocclusal position. Once removed and cooled, it is corrected with a more rigid and accurate registration material. Before it is used for mounting, the registration is trimmed to allow complete seating of the cast without distortion of the material.
A wax record can be further corrected with a freely flowing occlusal registration material, such as a metallic oxide paste, which is used as the final recording medium. In making such a corrected wax record, the opposing teeth (and also the patient’s lips and the dentist’s gloves) should first be lightly coated with petroleum jelly or a silicone preparation. The occlusal registration material then is mixed and applied to both sides of the metal-reinforced wax record. It is quickly placed, and the patient is assisted with closing in the rehearsed path, which will be guided by the previous wax record. After the occlusal registration material has set, the corrected wax record is removed and inspected for accuracy. Any excess projecting beyond the wax matrix should be removed with a sharp knife until only the registration of the cusp tips remains. Such a record should seat on accurate casts without discrepancy or interference and will provide an accurate interocclusal record. When an intact opposing arch is present, use of an opposing cast may not be necessary. Instead a hard stone may be poured directly into the occlusal registration material record to serve as an opposing cast. However, although this may be an acceptable procedure in the fabrication of a unilateral fixed partial denture, the advantages of having casts properly oriented in a suitable articulator contraindicate the practice. The only exception to this occurs if the maxillary cast on which the removable partial denture is to be fabricated has been mounted previously with the aid of a facebow. In such an instance, an intact mandibular arch may be reproduced in stone by pouring a cast directly into the interocclusal record.
Some of the advantages of using a metallic oxide paste over wax as a recording medium for occlusal records include (1) uniformity of consistency; (2) ease of displacement on closure; (3) accuracy of occlusal surface reproduction; (4) dimensional stability; (5) the possibility of some modification in occlusal relationship after closure, if it is made before the material sets; and (6) reduced likelihood of distortion during mounting procedures.
Three important details to be observed when one uses such a material are as follows:
Occlusal Relations Using Occlusion Rims on Record Bases
A third method is used when one or more distal extension areas are present, when a tooth-supported edentulous space is large, or when opposing teeth do not meet. In these instances, occlusion rims on accurate jaw relation record bases must be used. Simple wax records of edentulous areas are never acceptable. Any wax, however soft, will displace soft tissue. It is impossible to accurately seat such a wax record on a stone cast of the arch.
With this method, the recording proceeds much the same as with the second method, except that occlusion rims are substituted for missing teeth (Figure 17-9). It is essential that accurate bases be used to help support the occlusal relationship. Visible light-cured (VLC) bases may be adapted to the casts through the technique described in Chapter 15 for making impression trays. Utilizing the master cast, block out undesirable undercuts. However, do not add any wax for spacing. Paint a thin layer of the model release agent on the cast and the relief wax to aid in removal of the base from the cast after the designated time of polymerization recommended by the manufacturer. Carefully, adapt the VLC base material to the cast. Do not thin the material, and do not adapt the VLC base material over the remaining teeth. Process the base in the polymerization to set the material, then separate the record base from the cast and remove any remaining blockout wax. Clean the base and apply the air barrier coating over the entire record base, and process (tissue side up) as directed.
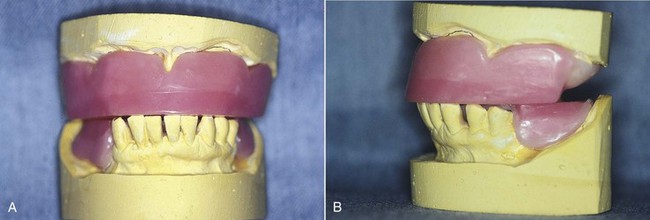
Figure 17-9 Relationship and distribution of remaining teeth for this patient requires that record bases and occlusion rims be used for accurate mounting of casts. A, Acrylic-resin record bases and hard baseplate wax occlusion rims for an edentulous maxilla and Kennedy Class I mandibular arch. These record bases are stable and were formed by sprinkling autopolymerizing acrylic-resin. B, Occlusion rims substitute for missing posterior teeth and provide an opportunity for posterior support when interocclusal records are made; this is most critical for the longer edentulous span on the mandibular right.
Record bases may also be made entirely of autopolymerizing acrylic-resin. Those materials used in dough form lack sufficient accuracy for this purpose unless they are corrected by relining. An acrylic-resin base may be formed by sprinkling monomer and polymer into a shallow matrix of wax or clay after any undercuts are blocked out. If the matrix and blockout have been formed with care, interference with removal will not occur, and little trimming will be necessary. When the sprinkling method is used and sufficient time is allowed for progressive polymerization to occur, such bases are stable and accurate. Other record bases include the use of cast metal and compression molded or processed acrylic-resin bases for jaw relation records.
Relative to the third method, some mention must be made of the ridge on which the record bases are formed. If the prosthesis is to be tooth supported or if a distal extension base is to be made on the anatomic ridge form, the bases will be made to fit that form of the residual ridge. But if a distal extension base is to be supported by the functional form of the residual ridge, it is necessary that the recording of jaw relations be deferred until the master cast has been corrected to that functional form.
Record bases must be as nearly identical as possible to the bases of the finished prosthesis. Jaw relation record bases are useless unless they are made on the same cast or a duplicate cast on which the denture will be processed, or are themselves the final denture bases. The latter may be a cast alloy or a processed acrylic-resin base.
Jaw relation records made by this method accomplish essentially the same purpose as the two previous methods. The fact that record bases are used to support edentulous areas does not alter the effect. In any method, the skill and care used by the dentist in making occlusal adjustments on the finished prosthesis will govern the accuracy of the resulting occlusion.
Methods for Recording Centric Relation on Record Bases
Centric relation may be recorded in many ways when record bases are used. The least accurate is the use of softened wax occlusion rims. Modeling plastic occlusion rims, on the other hand, may be uniformly softened by flaming and tempering, resulting in a generally acceptable occlusal record. This method is time proved, and when competently done, it is equal in accuracy to any other method.
When wax occlusion rims are used, they should be reduced in height until just out of occlusal contact at the desired vertical dimension of occlusion. A single stop is then added to maintain their terminal position as a jaw relation record is made in some uniformly soft material, which sets to a hard state. Quick-setting impression plaster, bite registration paste, or autopolymerizing resin may be used. With any of these materials, opposing teeth must be lubricated to facilitate easy separation. Whatever the recording medium, it must permit normal closure into centric relation without resistance and must be transferable with accuracy to the casts for mounting purposes.
Jaw Relation Records Made Entirely on Occlusion Rims
The fourth method is used when no occlusal contact occurs between the remaining natural teeth, such as when an opposing maxillary complete denture is to be made concurrently with a mandibular removable partial denture. It may also be used in those rare situations in which the few remaining teeth do not occlude and will not influence eccentric jaw movements. Jaw relation records are made entirely on occlusion rims when either arch has only anterior teeth present (Figure 17-10).

Figure 17-10 Opposing Kennedy Class I dental arches with remaining anterior teeth only. Recording of maxillomandibular relations was accomplished by using stable record bases and occlusion rims.
In any of these situations, jaw relation records are made entirely on occlusion rims. The occlusion rims must be supported by accurate jaw relation record bases. Here, the choice of method for recording jaw relations is much the same as that for complete dentures. Either some direct interocclusal method or a stylus tracing may be used. As with complete denture fabrication, the use of a facebow, the choice of articulator, the choice of method for recording jaw relations, and the use of eccentric positional records are optional, based on the training, ability, and desires of the individual dentist.
Establishing Occlusion by the Recording of Occlusal Pathways
The fifth method of establishing occlusion on the removable partial denture is the registration of occlusal pathways and the use of an occluding template rather than a cast of the opposing arch. When a static jaw relation record is used, with or without eccentric articulatory movements, the prosthetically supplied teeth are arranged to occlude according to a specific concept of occlusion. On the other hand, when a functional occlusal record is used, the teeth are modified to accept every recorded eccentric jaw movement.
These movements are made more complicated by the influence of the remaining natural teeth. Occlusal harmony on complete dentures and in complete mouth rehabilitation may be obtained by the use of several different instruments and techniques. Schuyler has emphasized the importance of establishing first the anterior tooth relation and incisal guidance before proceeding with any complete oral rehabilitation. Others have shown the advantages of establishing canine guidance as a key to functional occlusion before proceeding with any functional registration against an opposing prosthetically restored arch. This is done on the theory that the canine teeth serve to guide the mandible during eccentric movements when the opposing teeth come into functional contact. It also has been pointed out that the canine teeth transmit periodontal proprioceptor impulses to the muscles of mastication and thus have an influence on mandibular movement even without actual contact guidance. However, as long as the occlusal surfaces of unrestored natural teeth remain in contact, as in many a partially dentulous mouth, these teeth will always provide the primary influence on mandibular movement. The degree of occlusal harmony that can be obtained on a fixed or removable restoration will depend on the occlusal harmony that exists between these teeth.
Regarding occlusion, Thompson has written, “Observing the occlusion with the teeth in static relations and then moving the mandible into various eccentric positions is not sufficient. A dynamic concept is necessary to produce an occlusion that is in functional harmony with the facial skeleton, the musculature, and the temporomandibular joints.”* By adding “and with the remaining natural teeth,” the requirements for removable partial denture occlusion are more completely defined.
Some of the methods described previously may be applied to the fabrication of removable partial dentures in both arches simultaneously, whereas the registration of occlusal pathways necessitates that an opposing arch be intact or restored to the extent of planned treatment. A diagnostic wax-up of both maxillary and mandibular arches will facilitate visualization of the proposed mouth preparation and restorative procedures required to accommodate the planned occlusal scheme, correct orientation of the occlusal plane, correct arch form, and complete tooth modifications to accommodate the removable partial denture design—all at the desired vertical dimension of occlusion. If removable partial dentures are planned for both arches, a decision is necessary as to which denture is to be made first and which is to bear a functional occlusal relation to the opposing arch. Generally the mandibular arch is restored first and the maxillary removable partial denture is occluded to that restored arch. If the maxillary arch is to be restored with a complete denture or a fixed partial denture or crowns, a full diagnostic wax-up must be done before occlusion is established on the opposing removable partial denture. If opposing fixed partial dentures or opposing occluding crowns are to be fabricated, it may be advantageous to develop the occlusion and fabricate them simultaneously to ensure optimal positioning, cuspal relationship, and functional integrity.
Regardless of the method used for recording jaw relations, when one arch is completely restored first, that arch is treated as an intact arch even though it is wholly or partially restored by prosthetic means. The dentist must consider at the time of treatment planning the possible advantages of establishing the final occlusion to an intact arch.
Step-by-Step Procedure for Registering Occlusal Pathways
After the framework has been adjusted to fit the mouth, the technique used for the registration of occlusal pathways is as follows:
The occlusal paths, thus recorded, will represent each tooth in its three-dimensional aspect. Although the cast poured against this will resemble the opposing teeth, it will be wider than the teeth that carved it because it represents those teeth in all extremes of movement. The recording of occlusal paths in this manner eliminates entirely the need to reproduce mandibular movement on an instrument.
Instruct the patient in the removal and placement of the removable partial denture that supports the occlusion rim, and explain that by chewing in all directions, the wax will be carved by the opposing teeth. The opposing teeth must be cleaned occasionally of accumulated wax particles. It is necessary that the patient comprehend what is to be accomplished and understand that both voluntary and involuntary movements must be recorded.
Before dismissing the patient, add or remove wax where indicated to provide continuous contact throughout the chewing range. To accomplish this, repeatedly warm the wax with a hot spatula and have the patient close and chew into the warmed wax rim with the opposing dentition, each time adding to any area that is deficient. Any area left unsupported by its flow under occlusal forces must be reinforced with additional wax. It is important that the wax rim be absolutely dry and free of saliva before additional wax is applied. Each addition of wax must be made homogeneous with the larger mass to prevent separation or fracture of the occlusion rim during the time it is being worn. Leave the wax occlusion rim from 1 to 3 mm high, depending on whether the occlusal vertical dimension is to be increased.
If during this period the wax occlusion rim has not been reduced to natural tooth contact, warm it by directing air from the air syringe through a flame onto the surface of the wax. If the wax rim is held with the fingers during warming, a gradual softening process will result, rather than a melting of the surfaces already established. Repeatedly warm the occlusion rim and replace it in the mouth until the occlusal height has been reduced and lateral excursions have been recorded. At this time, use additional wax to support those areas left unsupported by the flow of wax to the buccal or lingual surfaces. Trim the areas obviously not involved, thus narrowing the occlusion rim as much as possible. Remove those areas projecting above the occlusal surface, which by their presence might limit functional movement.
When seating of the denture and changes in mandibular position have been accomplished by the previous period of wear, it is possible to complete the occlusal registration in an operatory. However, if all involuntary movements and those caused by changes in posture are to be recorded, the patient should again wear the occlusion rim for a period of time.
Natural teeth formerly in contact will not necessarily be in contact on completion of the occlusal registration. Those teeth that have been depressed over a period of years and those that have been moved to accommodate overclosure or mandibular rotation may not be in contact upon reestablishment of mandibular equilibrium. Such teeth may possibly return to occlusal contact in the future or may have to be restored to occlusal contact after initial placement of the denture. Because the mandibular position may have been changed during the process of occlusal registration, the cuspal relation of some of the natural teeth may be different from before. This fact must be recognized in determining the correct restored vertical dimension of occlusion.
Occlusion thus established on the removable partial denture will have more complete harmony with the opposing natural or artificial teeth than can be obtained by adjustments in the mouth alone, because occlusal adjustment to accommodate voluntary movement does not necessarily prevent occlusal disharmony in all postural positions or during periods of stress. Furthermore, occlusal adjustment in the mouth without occlusal analysis is limited by the dentist’s ability to correctly interpret occlusal markings made intraorally, whether by articulating ribbon or by other means.
The registration of occlusal pathways has additional advantages. It makes obtaining jaw relations possible under actual working conditions, with the denture framework in its terminal position, the opposing teeth in function, and an opposing denture, if present, fully seated. In some instances, it also makes possible the recovery of the lost vertical dimension of occlusion, unilaterally or bilaterally, when overclosure or mandibular rotation has occurred.
The completed registration is now ready for conversion to an occluding template. This is usually done by boxing the occlusal registration with modeling clay after it has been reseated and secured onto the master or processing cast. Only the wax registration and areas for vertical stops are left exposed. It is then filled with a hard die stone to form an occluding template (see Chapter 18).
It is necessary that stone stops are used to maintain the vertical relation rather than relying on some adjustable part of the articulating instrument, which might be changed accidentally. Also, if stone stops are used and both the denture cast and the template are mounted before they are separated, a simple hinge instrument may be used.
Materials for Artificial Posterior Teeth
Contemporary acrylic-resin teeth are generally preferred to porcelain teeth, because they are more readily modified and are thought to more nearly resemble enamel in their abrasion potential against opposing teeth. Acrylic-resin teeth with gold occlusal surfaces are preferably used in opposition to natural teeth restored with gold occlusal surfaces, whereas porcelain teeth are generally used in opposition to other porcelain teeth.
Acrylic-resin tooth surfaces, however, may in time become impregnated with abrasive particles, thereby becoming an abrasive substance themselves. This may explain why acrylic-resin teeth are sometimes capable of wearing opposing gold surfaces. An evaluation of occlusal contact or lack of contact, however, should be meticulously accomplished at each 6-month recall appointment, regardless of the choice of material for posterior tooth forms.
Although some controversy may continue with regard to the use of porcelain or acrylic-resin artificial teeth, there is broad agreement that narrow (reduced bucco-lingual) occlusal surfaces are desirable. Posterior teeth that will satisfy this requirement should be selected, and the use of tooth forms that have excessive bucco-lingual dimension should be avoided.
Acrylic-resin teeth are easily modified and readily lend themselves to construction of cast gold surfaces on their occlusal portions. A simple procedure for fabricating gold occlusal surfaces and attaching them to acrylic-resin teeth is described in Chapter 18 under posterior tooth forms.
Arranging Teeth to an Occluding Template
The occlusal surface of the artificial teeth, porcelain or resin, must be modified to occlude with the template. With this method, they are actually only raw materials from which an occlusal surface is developed that is in harmony with an existing occlusal pattern. Therefore the teeth must be occluded too high and then modified to fit the template at the established vertical dimension of occlusion.
Teeth arranged to an occluding template ordinarily should be placed in the center of the functional range. Whenever possible, the teeth should be arranged bucco-lingually in the center of the template. When natural teeth have registered the functional occlusion, this may be considered the normal physiologic position of the artificial dentition, regardless of its relation to the residual ridge. On the other hand, if some artificial occlusion in the opposing arch has been recorded, such as that of an opposing denture, the teeth should be arranged in a favorable relation to their foundation, even if this means arranging them slightly buccally or lingually from the center of the template.
The teeth are usually arranged for intercuspation with the opposing teeth in a normal cuspal relationship. Whenever possible, the mesiobuccal cusp of the maxillary first molar should be located in relation to the buccal groove of the mandibular first molar, and all other teeth arranged accordingly. With a functionally generated occlusion, however, it is not absolutely necessary that normal opposing tooth relationships be reestablished. In the first place, the opposing teeth in a dental arch that is not contiguous may not be in normal alignment, and intercuspation may be difficult to accomplish. In the second place, the occlusal surfaces will need to be modified so that they will function favorably regardless of their anteroposterior position. Because cusps modified to fit an occlusal template will be in harmony with the opposing dentition, it is not necessary that the teeth themselves be arranged to conform to the usual concept of what constitutes a normal anteroposterior relationship.
Establishing Jaw Relations for a Mandibular Removable Partial Denture Opposing a Maxillary Complete Denture
It is common for a mandibular removable partial denture to be made to occlude with an opposing maxillary complete denture. The maxillary denture may already be present, or it may be made concurrently with the opposing removable partial denture. In any event, the establishment of jaw relations in this situation may be accomplished by one of several previously outlined methods.
If an existing maxillary complete denture is satisfactory and the occlusal plane is oriented to an acceptable anatomic, functional, and esthetic position (which rarely occurs), then the complete denture need not be replaced and the opposing arch is treated as an intact arch as though natural teeth were present. A facebow transfer is made of that arch, and the cast is mounted on the articulator. To accomplish this, a facebow record is made with the complete denture in place. After the facebow apparatus has been removed from the patient, the complete denture is removed and an irreversible hydrocolloid impression of the denture is made. When the impression material has set, the denture is removed, cleaned, and returned to the patient. A cast is formed in the impression and then is mounted on the articulator with the facebow record. Maxillomandibular relations may be recorded on accurate record bases attached to the mandibular removable partial denture framework with the use of a suitable recording medium. Centric relation is recorded and is transferred to the articulator. Eccentric records can then be made to program the articulator.
In rare instances, when the mandibular removable partial denture replaces all posterior teeth and the anterior teeth are noninterfering, a central bearing point tracer may be mounted in the palate of the maxillary denture, and centric relation recorded by means of an intraoral stylus tracing against a stable mandibular base. If a stylus jaw relation recording method is used, the stylus must be carefully removed from the denture and attached to the same palatal location of the stone cast that was transferred to the articulator via the facebow. The mandibular cast can then be oriented by way of the horizontal jaw relation record and attached to the articulator.
When an existing complete denture is opposing the arch on which a removable partial denture is fabricated, a cast of the complete denture may be used during the fabrication procedures. However, when the occlusion is corrected after processing, and the removable partial denture is finalized during initial placement, the complete denture should be retrieved and mounted on the articulator with a centric relation record at the desired vertical dimension of occlusion. This will ensure a more accurate cuspal relationship and will prevent abrasion of the cusp contacts that would occur if a stone cast of the denture is used. This procedure is completed when the patient is in the office so as not to deprive the patient of use of the existing complete denture.
If the relationship of the posterior teeth on the maxillary denture to the mandibular ridge is favorable and the complete denture is stable, jaw relations may be established by recording occlusal pathways in the mandibular arch just as for any opposing intact arch. The success of this method depends on the stability of the denture bases, the quality of tissue support, the relation of the opposing teeth to the mandibular ridge, and the interrelation of existing artificial and natural teeth.
More often than not, the existing maxillary complete denture will not be acceptable to use because of poor tooth position. The denture will have been made to occlude with malpositioned mandibular teeth, which have since been lost, or the teeth will have been arranged without consideration for the future occlusal relation with a mandibular removable partial denture. Too often, one sees a maxillary denture with posterior teeth arranged close to the residual ridge without regard for the interarch relationship and with an occlusal plane that is too low. Usually, however, a new maxillary denture must be made concurrently with the mandibular removable partial denture, and jaw relations may be established in one of two ways.
If the mandibular removable partial denture will be tooth supported (a Kennedy Class III arch accommodating a bilateral removable prosthesis), the mandibular arch is restored first. The same applies to a mandibular arch that is restored with fixed partial dentures. In either situation, the mandibular arch is completely restored first, and jaw relations are established, as they would be to a full complement of opposing teeth. Thus the maxillary complete denture is made to occlude with an intact arch.
On the other hand, as is more often the situation, the mandibular removable partial denture may have one or more distal extension bases. The situation then necessitates that the occlusion be established on both dentures simultaneously.
All mouth preparations and restorative procedures required to correctly orient the occlusal plane, correct the arch form, accommodate the desired occlusal scheme, and accommodate the removable partial denture design must be accomplished on the remaining natural teeth. In addition, all supporting tissue must be in an acceptable state of health before the final impression is made. After final impressions, which include the alter cast impression or the corrected cast impression, are made, the maxillary occlusion rim is contoured, occlusal vertical relation with the remaining lower teeth is established, and a facebow transfer of the maxillary arch is made. The maxillomandibular relations may be recorded by any of the several methods previously outlined and the articulator mounting completed. Occlusion may be established as for complete dentures, with care taken to establish a favorable tooth-to-ridge relationship in both arches, an optimum occlusal plane, and cuspal harmony between all occluding teeth.
After try-in, several methods may be used to complete the restorations. Both dentures may be processed concurrently and remounted for occlusal correction, or the removable partial denture may be processed first. After the dentures are completed and remounted, the teeth—still in wax on the complete denture—are adjusted to any discrepancies that are occurring.
Occlusal discrepancies created during processing must be corrected before the patient is permitted to use the denture(s). Methods by which these discrepancies may be corrected are discussed in Chapter 18.