Working with Families
1 Describe the occupations and functions of families using family systems theory.
2 Appreciate the diversity of families and define methods to learn about a family’s culture and background.
3 Explore the implications of having a child with special needs with regard to the co-occupations of family members.
4 Analyze the implications of having a child with special needs with regard to family function.
5 Synthesize information about the family life cycle and transitions to identify times of potential stress for families of children with special needs.
6 Specify the roles of the occupational therapist in collaboration with families.
7 Understand how to establish and maintain partnership with a family.
8 Enact alternative methods of communication that promote family–therapist partnerships.
9 Describe ways families can be empowered to facilitate their children’s development.
10 Explain strategies for supporting the strengths of families facing multiple challenges.
This chapter introduces a range of issues related to families, particularly families of children who have special developmental or health care needs. It considers how family members fulfill the functions of a family by collectively engaging in daily or weekly activities and by sharing special events. The chapter explores factors that contribute to the variety of families with whom therapists may work in providing occupational therapy for children. Having presented this background in the occupations of families and family diversity, the chapter then turns to the ways the special needs of children bring opportunities and challenges to families. This discussion includes the ways that having a child with disabilities can influence how family members organize their time, engage in activities, and interact with one another. Throughout the chapter, the importance of a family-centered philosophy and evidence from the literature are discussed.
REASONS TO STUDY ABOUT FAMILIES
Families are complex systems. Having a child with a disability or chronic health condition, which can happen in families anywhere on the socioeconomic spectrum, of any educational, ethnic, or genetic background, adds an appreciable degree of stress into this complex system. There is a greater incidence of negative outcomes when the odds are stacked against that family because of low socioeconomic status, poor education, minority status, and difficult genetic structure. Occupational therapists encounter all varieties of families and must be prepared to work with them all. Children cannot be treated as isolated individuals; they are members of families, social units that shape behavior and life experiences. Evidence shows that child outcomes will be shaped by how well therapists communicate with families and how well the partnership between them has been established.25,52,79 Learning about family systems is important preparation for working in any practice setting.
The development of children’s occupations cannot be understood without insight into what shapes their daily activities. Young children first learn about activities, how to perform them, what activities mean, and what to expect as the outcomes of their efforts within the family context.67 Although children’s activities vary from one culture to the next, universally their families play a major role in guiding children in how to spend their time, what to do, and why the things they do are important.88,135,166 All major health-related disciplines, including but not limited to psychology, sociology, and nursing practice, use the ecological view of children and the family: that each is interconnected with the other and the environments they experience. The more fully occupational therapists understand the influences on the way families operate in their daily routines and their goals for the ways children spend their time, the better prepared they will be to support each family in helping the child engage in activities the family values.
Another reason to study families explicitly is to circumvent the inclination to reference one’s own family experiences as a template for the way families operate. Walsh points out that when people speak of “the family,” they suggest a socially constructed image of a “normal” family, giving the impression that an ideal family exists in which optimal development occurs.174 In reality, many different types of families are successfully raising children. In this chapter, two or more people who share an enduring emotional bond, a commitment to pool resources, and carry out the typical family functions can be seen as a family.39,86,166,175 This chapter focuses on families raising children. One or more parents, grandparents, and stepparents, as well as adoptive or foster parents, can successfully bring up children. The authors refer to the caregiving adult as the “parent” of the child, and focus specifically on the “parent” only when it is germane to the discussion of family diversity (Box 5-1).
A third reason to study families is that the involvement of family members is central to the best practice of occupational therapy. In addition to organizing and enabling daily activities, the family provides the child’s most enduring set of relationships throughout childhood, into early adulthood, and possibly beyond. During the course of his or her lifetime, a person with a disability may receive services from people working through health services, educational programs, and social agencies. These relationships exist because professionals bring expertise required by the special needs of the young person. As the type of services needed changes, professionals enter and leave the young person’s life. The family represents a source of continuity across this changing pattern of professional involvement. The family forms a unique emotional attachment to their child, and their continuous involvement gives them special insight into the child’s needs, abilities, and occupational interests. In light of the family’s expertise, occupational therapists strive to collaborate with family members, following their lead and supporting their efforts in promoting the well-being and development of the child with special developmental or health care needs.14,25,146Appendix 5-A, which describes the actual experiences of parents raising three children with special needs, provides additional insight into the essential nature of family relationships.
Finally, including families in the process of providing services for children is not just best practice—it is the law. In recognizing the power of families, federal legislation requires service providers and educators to seek the input and permission of a parent or guardian on any assessment, intervention plan, or placement decision. The importance of the family in the early part of the child’s life (from birth to 3 years old) is reflected by the emphasis on family-centered services in Part C of the Individuals with Disabilities Education Improvement Act 2004.69 It requires providers to talk with parents and develop a family-directed Individualized Family Service Plan (IFSP) regarding the resources the family needs to promote the child’s optimal development. Later, in the school system, parents are involved in developing the Individualized Educational Program (IEP), which guides special education and related services (see Chapters 23 and 24).
THE FAMILY: A GROUP OF OCCUPATIONAL BEINGS
Family members, individually or together, engage in a variety of activities that are part of home management, caregiving, employed work, education, play, and leisure domains that help them feel connected to each other. A father fulfills one of his family roles by picking up groceries on his way home from work, or a child studies for a test because his parents expect good grades. Family occupations occur when daily activities or special events are shared among family members, such as a parent helping her son study for a test, the whole family going to a movie, or brothers shooting baskets. By engaging in occupations together, families with children fulfill the functions of the family unit expected of them by members of their community. Societies first anticipate that families provide children with a cultural foundation for their development as occupational beings. Family members share and transmit a cultural model, a habitual framework for thinking about events, for determining which activities should be done and when, and for deciding on how to interact.43 By providing a cultural foundation, families ensure that children learn how to approach, perform, and experience activities in a manner consistent with their cultural group. This cultural learning process enables children to acquire the occupations that will make their participation in a variety of contexts possible (Box 5-2). Culture is passed from generation to generation through rituals that include celebrations, traditions, and patterned interactions that give life meaning and construct family identity.143
Occupations have meaning because they convey a sense of self, connect us to other people, and link us to place.54 Routine family occupations give life order and structure the achievement of goals.143 Routine family occupations and special events also form the basis for repeated interpersonal experiences that give family members a sense of support, identity, and emotional well-being.149 The importance of family occupations is reflected by the fact that families create special activities for the specific purpose of spending time together.139
Families are also expected to help their children develop fundamental routines and lifestyle habits that contribute to their physical health and well-being. In the context of receiving care and sharing in family activities children acquire skills that lead to their independence in activities of daily living (ADLs) and learn habits that will influence their health across their life span. For example, in the context of sharing in family dinners and leisure activities after dinner, children establish habits that can reduce or increase future problems with obesity.
A final function of a family is to prepare children for formal or informal educational activities and whatever other practices the community uses to prepare young people to become productive adults.135 Parents, in the context of their daily routines and through their encouragement, provide children participation experiences that influence how they approach learning.68 Families of children with certain disabilities have a greater challenge meeting all these expectations, as will be discussed later in this chapter.
Guided by their cultural models, special circumstances, and community opportunities for activities, families use their resources in different ways (Box 5-3). For example, one family may choose to pay (using financial resources) to have the yard work done so that time (another asset) on Saturday afternoons can be used for having a picnic together. Another family invests interpersonal energies (an emotional resource) to get everyone to help with the yard work on Saturday afternoon so that money will be available to pay for music lessons. Financial, human, and emotional resources, as well as time, are not limitless, and in healthy families, members negotiate a give and take of their assets. For example, mothers of children with developmental coordination disorder (DCD) or attention deficit–hyperactivity disorder (ADHD) may set aside extra time to help with their children’s activities and rely on hired help or assistance from other family members to get household tasks done.111,142 Typically, families with children have a hierarchical organization in which one or more family members (e.g., a parent) take major responsibility for determining how the resources are distributed, enabling the family to engage in activities that fulfill family functions. Availability of resources varies for many reasons, both within families and within their communities. Challenges for both families and therapists occur when families or the communities they live in have severely limited resources.147
SYSTEM PERSPECTIVE OF FAMILY OCCUPATIONS
A family functions as a dynamic system in which its members, comprising subsystems, engage in occupations together to fulfill the functions of a family. As with any system, the activity of one person can influence the activities of other members; this is known as interdependent influences that exist among the different parts, much as a change in one piece of a mobile causes movement in every other section. For example, a sixth grader may ask to stay after school with his friend, which means he is not available to watch his sister that afternoon while his mother shops. Consequently, the mother brings her daughter to the grocery store. Shopping with the preschool daughter takes the mother longer than shopping alone. As a result, they do not get home as quickly, and dinner is started late. The interdependent nature of family members’ activities is illustrated by the fact that the boy’s choice of what he wanted to do in the afternoon altered the activities of his mother and sister and indirectly affected the family’s mealtime routine that evening. Recognizing that a family functions as a whole, a therapist who suggests an after-school horseback riding class for a child with cerebral palsy can appreciate that the recommendation must be weighed in light of the family resources and the implications of that activity for the entire family system. As a complex social system, family members have to coordinate what they do and when they do things to share in family routines and rituals (Box 5-4). They accomplish this within subsystems, through their communications and family rules.28
With all of the activities a family does and the different members who can carry out these tasks, it would become confusing and draw on family resources if everyone had to negotiate daily who was going to do what, when, and in which way. An effective family system organizes itself into predictable patterns of daily and weekly activities and familiar ways with special events. Guided by their cultural models, and often organized through unspoken family rules, families settle into daily routines for various household activities.26,149 These daily routines include interactive rituals that take on symbolic meaning and seem so matter of course that people do not think of doing them any other way, and they resist changing them.43,143 Bedtime routines for a child, for example, can have a set sequence of taking a bath, brushing teeth, and the parent reading a book. If routines are interrupted, even by a welcomed event, such as a grandparent coming to visit, family members invest extra family resources reconfiguring their daily routines under the changed circumstances. For example, time is spent making up a bed on the sofa rather than giving the daughter a bath, and emotional energy is expended to help the daughter fall asleep in the living room so that the grandparent can sleep in her bedroom. Families may experience the disruption of their daily routines as unsettling and taxing, and it is not uncommon to hear family members sigh in relief when they can return to predictable patterns, that is, when “things get back to normal.”
In addition to routines for daily or weekly activities (Figure 5-1), families also establish predictable patterns for what they do during rituals, such as special events. Family traditions, such as cooking special food for birthday celebrations or sharing leisure activities on Sunday afternoons, help families develop a sense of group cohesion and emotional well-being for family members (Figure 5-2). Families may decide to maintain their traditions rather than address an individual member’s needs because these customary activities fulfill family functions. For example, a family that traditionally vacations with grandparents for several weeks in the summer may value the way special occupations together reinforce their sense of being a family. Conflict with the occupational therapist could arise if the therapist assumes that the family will shorten the traditional vacation to attend some therapy sessions during the summer. When the occupational therapist offers a range of options and asks the family to set priorities, family members can consider all of their routines and traditions and determine how they want occupational therapy services to fit into their lives.

FIGURE 5-1 Matthew and his brother wait for the school bus. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
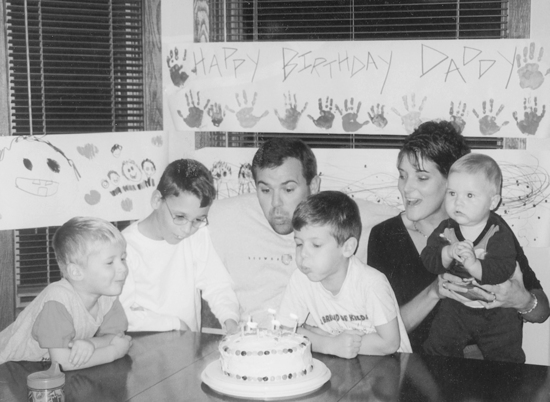
FIGURE 5-2 Matthew’s family celebrates Dad’s birthday. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
Celebrations are predictable patterns of doing activities, such as religious rituals, that are shared with members of the community. Therefore, what is done during family celebrations may be similar to what other families that share a similar background do for the same celebration. This link to others gives family members a sense of meaning associated with their special events that connects them to a community of families. Therapists may be asked for assistance so that children can participate in celebrations. For example, a parent may want positioning suggestions so that her daughter with cerebral palsy will be comfortable during Christmas Eve services. The family of a boy with sensory processing problems may need ideas for coping that they can use while attending a Fourth of July fireworks display with the neighbors. By enabling these children’s occupational engagement, the entire family participates in community celebrations and confirms their identity as a family like every other family raising children.
Among the researchers who have investigated family routines and practices, Fiese and colleagues38,99,149 have examined the meaning of routines and related ritual interactions of families’ daily activities and religious celebrations. Their studies show that families who reported finding more meaning and commitment to their routines and special activities experienced better health of family members and stronger interpersonal relationships. Occupational therapists who suggest home carryover of interventions must be sure that the activities will fit within the family’s values and their existing routines; otherwise the intervention will not be incorporated.13,144,145
FAMILY SUBSYSTEMS
Regardless of the type of family structure (e.g., birth, adoptive, partner, blended, or foster), caregiving adults sharing parental duties need to coordinate their efforts. These adults form the parent subsystem of the family, which can be a positive force and can contribute to the child’s ability to face developmental challenges. Researchers have found a number of different solutions in how parents distribute childcare, realizing that the different forms may all be adaptive if they enable the system to operate and meet family functions.64,176 Studies have found that when a child has a disability, additional time for caregiving co-occupations is required in the mother–child subsystem.29,30 The type and severity of disability the child will affect the amount of time required; for example, Crowe found that mothers of children with multiple disabilities spent at least 1 hour more per day on child-related activities compared with mothers of children with Down syndrome.29 Disabilities that seem to create more stress and caregiving effort for the family include autism, severe and multiple disabilities, behavior disorders, and medical problems that require frequent hospitalization and in-home medical care.23,54,134
Researchers have reported that mothers experience stress from the increased workload of caring for a child with disabilities.54,120,149 In addition, mothers may experience more stress than their husbands because they are typically the primary parent working with the intervention team and, as a result, face greater demands on their time and communication skills.90,93 Mothers often become the conduit for communication, responsible for transferring information and expectations between clinic and family. Therefore, because mothers find themselves caught between the perspectives of both the professionals and family members, the professional must be especially sensitive to the needs of mothers.30,93,157,170
Some researchers have found that fathers can be more at risk for stress than mothers because they may feel isolated and helpless compared with the mother, who is more involved. Young and Roopnarine found that fathers spend about one-third the time caring for their children that mothers do.179 Also, fathers may lack social supports compared with their spouses. Scholars have come to recognize the multidimensional process influencing what fathers do and why they do it.126 They have also noted that fathers are more sensitive than mothers to the influence of the ecology of the family and the attitude of others. Other studies have found that mothers and fathers report similar levels of stress related to a child with disabilities.76,115 Although stress levels were similar,76 mothers attended 80% of the child’s intervention sessions compared with fathers, who attended 33%. The problem that arises from fathers’ inability to attend therapy is that information is often conveyed via the mother. Therapists should identify and use more direct methods of communicating with the father to ensure that information is transmitted accurately and to unburden the mother of the responsibility of transmitting information (Figure 5-3).
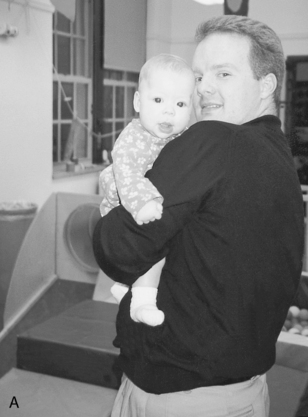
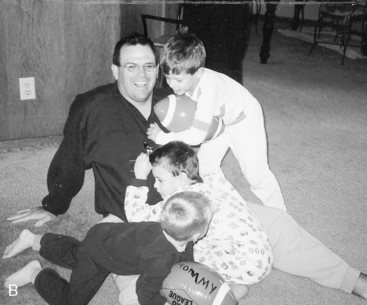
FIGURE 5-3 A, Father enjoys holding his child while attending an early intervention program in the evening with his family. B, Playtime with Dad before bed.
A child with disabilities can also affect the relationship between husband and wife. Although there is evidence that a child with disabilities can stress the marital relationship and decrease marital satisfaction, some parents have reported that their marriage was strengthened.134 Differences in marital satisfaction between families of children with disabilities and those of typically developing children tend to be minimal.20 Stress in dealing with the child may bring parents together for problem solving, and they may rely on each other for emotional support and coping. A strong relationship between husband and wife seems to buffer parenting stress. Britner et al. found that mothers who reported high levels of marital satisfaction also reported less parental distress and found their supports and interventions to be more helpful.20
Siblings
As was suggested in the discussion of the system perspective, family members reciprocally influence one another in a dynamic way. Having a brother or sister with special needs changes the experiences of other children growing up in that family (Figure 5-4). Williams et al. investigated how having a sibling with special needs influences the typically developing brother or sister.178 Using a method that allowed them to track direct and indirect effects (structural equation model), they investigated factors that might influence behavioral problems or the self-esteem of children who had a sibling with either a chronic illness (e.g., cancer, diabetes, or cystic fibrosis) or a developmental disability (e.g., autism, cerebral palsy). These workers considered factors that might influence the typical child’s experiences, such as how much the child understood about the disease, the sibling and his or her attitude, and social support. They also asked the mother about the mood and emotional closeness of the family (family cohesion). The researchers reported that the family’s socioeconomic status (SES) and cohesion and the siblings’ understanding of the disease were related to whether the typically developing sibling had behavioral problems. They also found that when the siblings felt supported, their behavior, mood, and self-esteem were more positive than when they felt unsupported.
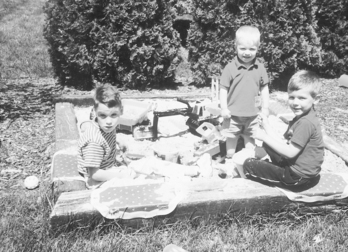
FIGURE 5-4 Matthew and his brothers enjoy backyard play. A sandbox is a fail-proof medium that provides equal opportunity for multiple levels of play. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
Siblings are an important source of support to each other throughout life. In general, the relationships between children with disabilities and their siblings are strong and positive (Figure 5-5).154 However, the research findings are varied across types of disabilities, sibling place in the family (older or younger), and sibling genders. Conflict among siblings may be more prevalent when a child has a disability such as hyperactivity or behavioral problems. Conflict tends to be less prevalent when a child has Down syndrome or mental retardation.61,81,154

FIGURE 5-5 Although Matthew is the oldest of four boys, his younger brothers already take the initiative to help him participate. A round of miniature golf requires his brothers’ assistance, which does not detract from the fun. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
Often the roles of siblings are asymmetric, with the typically developing child dominating the child with the disability. Siblings without disability generally engage the child with a disability in play activities they can participate in, such as rough-and-tumble play rather than symbolic play. Siblings may be asked to take on caregiving roles, and assuming caregiving roles can have both positive and negative effects.154 Siblings learn to relate and interact in the context of a family. Positive and solid marital systems seem to promote more positive sibling relationships, and marital stress has a deleterious effect on sibling relationships. Rivers and Stoneman studied the effects of marital stress and coping on sibling relationships when one child had autism.134 Using multiple self-report measures of siblings and parents, they found that when marital stress is greater, the sibling relationship is more negative. This study confirmed the importance of examining sibling relationships in the context of the family, recognizing that all family subsystems affect each other.
As occupational therapists promote engagement in a full range of activities as a way of helping a child participate in family life, the inclusion of siblings is an important step in occupation-centered practice. Peer support groups for the typically developing siblings can also be occupation centered. Therapists can develop a recreational program for brothers and sisters of children with whom they work so that the siblings can meet one another and realize that their family is not the only one that faces challenging behaviors. These groups generally participate in structured activities and have open-ended discussions about what it means to have siblings with disabilities. One formalized support group for siblings is Sibshops, a recreational program that addresses needs and concerns through group activities.110 Sibshops’ primary goals for brothers and sisters of children with special needs are to meet their peers, discuss common joys and concerns, learn how others handle common experiences, and learn more about their siblings with special needs. In addition, parents and professionals are given the opportunity to learn more about the experiences of these typical siblings. When possible, siblings should be involved in occupational therapy sessions. They are likely to be the best playmates and can often elicit maximum effort from their brother or sister. In addition, sibling involvement gives the therapeutic activity additional meaning (play), and siblings can act as models for teaching new skills and providing needed support in a natural context.82
Extended Family
In the extended family, the experience of having a child with special needs depends on the meaning family members bring to their relationship with the child. For some grandparents, grandchildren represent a link to the future and an opportunity for vicarious achievement. Researchers find that when children have disabilities, grandparents express both positive and negative feelings and go through a series of adjustments similar to those of the parents.98,137 Many of the negative feelings, such as anger and confusion, appear to decrease with time. However, some never completely disappear. Positive feelings, such as acceptance and a sense of usefulness, increase over time. A grandparent’s educational level and sense of closeness to the child are positively associated with greater involvement with the child. Factors such as the grandparent’s age and health and the distance the grandparent lives from the child do not appear to influence involvement (Figure 5-6). Grandparents learn information about their grandchild’s condition primarily through the child’s parents. However, some seek information from other sources, such as support groups for grandparents of special-needs children. Margetts et al. found that grandparents of children with autism spectrum disorder felt strongly about the caring and support they provided for both their children and grandchildren. These researchers suggested that for professionals to be truly family centered, they need to ask whether the parents want to include the grandparents in the initial assessment of the child.

FIGURE 5-6 Matthew’s grandparents enjoy their time with him and offer important support to his parents. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
Patterson, Garwick, Bennett, and Blum interviewed parents of children with chronic conditions about the behavior of extended family members.130 Family members, such as grandparents, uncles, and aunts of the child, were especially important to fathers and mothers for emotional and practical assistance. When extended family members were not supportive, parents expressed frustration and hurt over their lack of contact. In addition, parents recalled examples of times family members made insensitive comments about the child, ignored the child, or did not want to talk about the child’s disability. Parents of children with behavioral problems reported that extended family members tended to blame the child’s actions on the parents’ inability to discipline correctly.161 Families may be reluctant to ask relatives for assistance, wishing instead that they might volunteer.47 With the consent of the parents, occupational therapists can encourage extended family members to become more involved by offering to share information with them and inviting them to therapy sessions. In this way, therapists can help families build on important social and emotional resources.
FAMILY LIFE CYCLE
Family systems undergo metamorphosis and adapt as family members change. Some transitions can be anticipated with developing children and seem to be tied to age more than ability. For example, normative events in children that require adjustments in families include the birth of a child, starting kindergarten, transitions between schools, leaving high school, and living outside the home. Other changes in the family are not anticipated. Non-normative events may include a grandparent coming to live with the family or a parent accepting a different job in another city. Families that are cohesive and adaptable adjust interactive routines, reorganize daily activities, and return to a sense of “normal” family life. If interactive routines and role designation are too rigidly set, the family may not be able to operate effectively through periods of transition. This is especially true if the family experiences unanticipated, threatening events, such as a job loss or a medical crisis. All families use coping strategies to accommodate periods of transition.
Occupational therapists must understand that all families are unique. Although life-cycle models consist of predictable events, the individuality of each family must be acknowledged. The characteristics and issues at each life stage are highly variable, and each family moves through the stages at different rates. For example, family members may experience and resolve their feelings when they first learn about their child’s diagnosis, or they may take months to “come to grips” with the information.131 In addition, the family may experience cycles of sadness and acceptance later, within and between life stages. Issues that the family seemed to resolve when the child was an infant may occur again when the child reaches school age and an “educational diagnosis” is made or a learning problem is identified. Other life stage–related events, such as the child’s ability to develop friendships when first entering grade school, may become an issue again, such as when the child enters high school.165 Appendix 5-A provides examples of the issues that arise in each of the life stages. Finally, owing to the nature of the family structure, different members of the family may be at different stages at the same time. Therefore, characteristics of the family members and the child’s phase of development must be considered. For example, in a skipped-generation family, grandparents frequently have to deal with changes associated with old age at the same time they are parenting their grandchildren. In other families, parents may be taking care of their elderly parents in addition to caring for a child with special needs. Similarly, a young couple may have more energy and resources to cope with the birth of a child with special needs than does an older couple with four other children participating in school activities.
Early Childhood
Identifying a child as being at risk for health or developmental problems is usually a complicated process. Unless the child is born with medical problems, or with congenital problems in a body structure, or has features that suggest a syndrome, many children are not diagnosed until months, and sometimes years, later. Families that describe their experiences in raising a child with a disability frequently recall their journey by looking back to a period when “something was not right.”40 Families of children with pervasive developmental delays recall a sense that they had to search for a diagnosis with repeated testing and visits to several clinics or evaluation centers. Even parents of a child with an unusual physical complaint, such as joint pain that only occurs at night, might have to persevere in finding the cause when professionals initially determine that the child is only seeking attention. After receiving a diagnosis and ending a period of uncertainty, families hope for a period of stability, but as one educated father commented, “No amount of professional or personal preparation trains you for the reality of chronic illness” (p. 243).63
Parents’ requests for information generally include questions regarding day-to-day childcare, medication management, insurance issues, and support systems available.65
Parents whose first child has special needs do not have the same experiences to draw on as those of families with older children.47 Parents of young children may ask questions such as: “Do you think he can go into a regular classroom” and “Do you think she will be able to live on her own some day” Thoughtful responses to these questions recognize the parents’ need for optimism and hope. However, the responses must be honest and realistic. Even therapists with years of experience and extensive knowledge about disability and development cannot make definitive statements about the future. Long-range predictions about when the child will achieve a certain milestone or level of independence are always speculative. However, parents feel frustrated when they are told that the future cannot be predicted. Lawlor and Mattingly found that families want to be exposed to anticipatory planning.90 Parents want to understand that they have reason to expect their child, despite disabilities, will have a place in society and an opportunity to engage in socially valued occupations during adulthood. Therapists can help parents understand the range of possibilities by telling them about the continuum of services for older children and young adults in the community. Talking with parents of older children with a similar condition or hearing the therapist’s story of a child with the same characteristics provides some insight into the future.42,177 Even without knowing the child’s developmental course, parents start to develop an understanding that services are in place, and they begin to create new stories about their child’s future.
Given information about the system, their rights, and the resources available to them in their communities, parents can solve problems and independently access needed services. The caregiving routines of parents whose young child has a disability are not particularly different from those of all parents of young children. At this time in the child’s life, the parent’s work consists of managing the child’s play environment and introducing new, developmentally appropriate objects and materials. The parent ensures safety and may adjust or arrange the play environment so that the infant can access objects of interest. Feeding, diapering, bathing, and daily care are also natural parenting activities at this time. Only when infants and young children have serious medical conditions or behavioral problems are daily occupations significantly altered.
When children are medically unstable but still at home, a family may have home-based nursing for extended periods (i.e., months to several years). Murphy described the stress created by the constant presence of nurses and professional care providers in the home.113 Role ambiguity often results when parents feel that they must take on unpaid nursing work and nurses take on parenting roles. Parents also report stress from a lack of privacy and the continual feeling that they are “on duty.” Parents of medically fragile children must make tremendous accommodations, which should elicit high levels of sensitivity and responsiveness from professionals. For example, when parents have a medically unstable infant and around-the-clock, in-home nursing care, services such as respite become a priority.
School Age
When a child enters school, all families are excited about the new opportunities for learning and the child’s new demonstration of independence. However, school entry is not always a positive event for families of children with disabilities. Families that experienced early intervention services may be disappointed to find fewer family services and less family support offered by the school. Typically, parents are not encouraged to attend classes or school-based therapy sessions. Many parents view the transition to school as an opportunity to be less involved and a sign of their child’s maturation. To ease the transition from home to school, the parents of children with special needs should learn about the school’s programs, schedules, rules, and policies (Figure 5-7).

FIGURE 5-7 Matthew has an aide at school who supports his participation in both academic and nonacademic activities. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
For children with mild learning disabilities, entry into school may be the first time that the gap between a child’s performance and teachers’ expectations for his or her performance is identified. Therefore, this may also be the first time that parents receive information that their child has special needs. When this is the case, parents can experience surprise, disbelief, or relief. School age is a time when children with disabilities may first discover that they have differences. How they make the adjustment to this information depends on the knowledge and sensitivity of the adults and children around them.
To the school-aged child, making friends and maintaining friendships become critically important. Some parents report concern if their children appear lonely, isolated, and friendless. Turnbull and Ruef found that children with behavioral problems frequently have no friends, leaving the parents with the additional responsibility of creating and supervising play opportunities with other children.161 Teachers and therapists can use different strategies to promote friendships in inclusive environments. Typically developing peers can take turns being a child’s “special buddy,” and they can offer assistance with projects or tutoring. In situations in which social stigma is an issue, peer relations can be promoted by explaining the disability to the other children and by designing classroom activities that promote cooperation and positive interaction.
Adolescence
Adolescence is a challenging and potentially stressful time for all families, as the development of self-identity, sexuality, and expectations of emotional and economic autonomy herald the transition to adulthood. These issues may pose additional challenges in the lives of children with disabilities as they maneuver through adolescence. Parents need to prepare the young person to handle his or her growing social, financial, and sexual needs, as well as how to avoid substance abuse. (See the review of high-risk behaviors in adolescents with chronic illness by Valencia and Cromer.169) In certain cases, parents face decisions about their child’s use of birth control and protection from sexually transmitted diseases.45 With adolescence, new concerns about a son’s or daughter’s vulnerability increase as that child ventures further into the community and beyond. These decisions will vary significantly depending on the nature of the disability: cognitive, physical, social, visible, or not. They will also be mediated by financial opportunities or constraints.
Although the child usually is well accepted by family members, the social stigma incurred from peers and others may increase during adolescence. As one mother said, “The community accepts our children much more easily when they are small and cute. Babyish mannerisms are no longer acceptable … [Our son] has had real problems with his social relationships. He simply does not know how to initiate a friendship. He has difficulty maintaining a sensible conversation with his peers. He doesn’t handle teasing well, so he is teased unmercifully” (p. 90).4
The cute child with unusual behaviors may become a not-so-cute adolescent with socially unacceptable behaviors. As one parent explained why her son was not invited to a holiday party, “Everyone in the family was invited except Billy. I thought it must be an oversight, but the friend later explained apologetically, ‘I thought Billy’s presence might make the other guests uncomfortable.’ This kind of attitude is difficult to accept, particularly when he had been included very successfully in a similar party. I find myself crying at the unfairness” (p. 16).140
Other parents have reported difficulty in caring for their child’s growing physical needs. As the child reaches adulthood, parents who are reaching middle age may feel their strength and energy declining. As one parent put it,
The sapping of energy occurs gradually. The isolation it imposes does, too. As I work professionally with young mothers, I see them coping energetically with the demands of everyday life. They are good parents, caring ones, doing everything possible to help their child [with a disability] reach full potential, sometimes doing more than they have to; and if they have other children, they are doing the same for them. Most of these mothers even get out, see friends, attend meetings, volunteer in the community, and do all the things their friends and families expect them to do. All this is at least possible when one’s child is little, although it demands enormous energy. But to look at the mothers of children who have turned into teenagers is to see the beginnings of the ravages. Their lifestyle is changing. They go out less, see fewer people, do less for their children. They are stripping their living to the essentials (p. 144).112
Adolescence is the time when most parents must learn to let their children make their way in the world. For parents of children with disabilities, this time may require additional emotional support and financial resources. Magill-Evans, Wiart, Darrah, and Kratochvil conducted a small qualitative study with parents of adolescents with physical disabilities and some of the adolescents themselves that documented the multifaceted needs of each family in balancing the connection of the youth and the parent between the old way of relating and the new acceptance of the autonomy needs of the young adult.97 They found that both the young person and the parent had issues to be dealt with at this time, ranging from the need of each for emotional support during the transition to the need for financial resources to meet the physical or educational requirements of the young person for care from nonfamily members. Gender differences have also been found to have significant impact during the transition to adulthood. In one survey study of adolescents receiving special education services, the expectations and opportunities regarding work and family for males were perceived to be greater, even though the female respondents placed greater emphasis on having children and going to college. In addition, while both genders were concerned about obtaining health insurance, more of the female respondents rated this as a very important goal.133 As with all facets of the life cycle, this is a time for a sensitive, collaborative approach between families and service providers so that the right supports and resources are offered to each family.
FAMILY RESOURCES AND THE CHILD WITH SPECIAL NEEDS
Having a child with special needs does not eliminate any of the functions of a family. That is, through their activities, families continue to provide a cultural and psychosocial foundation and guide their children’s experiences in activities that will lead to optimal health and participation in the larger community. Understanding how families make choices in light of finite resources and their vision of children’s futures puts some of these decisions families make about daily activities and what they want to work on in a different light.74 For a period, especially when a problem is recently diagnosed or when medical treatment is needed, family resources (e.g., time, money, and emotional energy) may be directed primarily to the needs of the child.108 For example, a mother who has a full-time job to help pay medical and therapy bills and spends four hours a day feeding her medically fragile child has limited time and emotional energy to devote to helping another child with homework or to sharing in recreational activities. Over time, this allocation of resources can have negative implications for family members, and if the feeding problems are chronic, other choices may need to be made.
Financial Resources
Having a child with special needs has implications for family economics. Parents with children who have disabilities have many hidden and ongoing expenses. When children are hospitalized, many expenses (e.g., days out of work, childcare for siblings, transportation, meals, motel rooms) are incurred, in addition to costs not covered by insurance.123 Mothers on welfare reported that they faced multiple barriers.94 Although they wanted to become self-sufficient, they found that employment seemed like a distant dream as they struggled with transportation and finding childcare, particularly for older children.173 Jinnah and Stoneman offer an excellent review of literature and qualitative study on parents’ experiences with finding childcare for their school-age children.70 Part of their recommendations address the training needs of providers of childcare, as well as the information needs of parents regarding the accessibility requirements of childcare centers under the Americans with Disabilities Act.
Although financial problems create added stress, therapists are often reluctant to discuss finances, especially costs associated with their own services. In a sample of mothers of children with cerebral palsy, Nastro found that insurance coverage was inadequate to meet the families’ needs. As one mother reported, “Each piece of equipment has a big price tag. Even the smallest piece has a couple-hundred-dollar price tag. Most insurance companies do not cover it. Medicaid does not cover everything” (p. 52).116
Also, many insurance plans have caps on the number of therapy visits allowed per year. Therefore, parents must cut back on services or pay for sessions by finding a way to save somewhere else. Children who require extensive medical treatment can bring economic devastation to a family, especially when insurance coverage is inadequate.80,124
Another challenge to financial resources occurs when a parent decides to remain unemployed so that he or she has time to provide extra caregiving. Multiple studies have documented that a parent may need to work fewer hours, if at all, to care for the child.10,132 With one spouse unable to take on paid employment, these households are at higher risk for problems associated with low income. Financial strain is increased in single-parent homes. Case-Smith found that mothers of children with medical conditions left employment because of the frequency of their children’s illness.23 These children needed specialized medical care (i.e., nursing care) that prohibited their attending community childcare centers. The need to stay home with a child who has multiple medical needs and frequent illness coupled with lack of community childcare for such a child can become a particularly difficult situation for parents to manage. Part of the essence of family-centered care is addressing such needs in a family.71
Human Resources
The human resources important to a family in raising children are education, practical knowledge, and problem-solving ability. An understanding of the basis of the child’s problems and of possible adaptations is a powerful resource in helping families establish effective patterns of daily activities. As a parent, Marci Greene observed that a comprehensive parent–professional partnership should include ongoing sharing of information with parents.48 Initially, most parents want additional information about their children’s conditions and about accessing services.82 This is followed by needing information about potential complications, and how to care for their child’s physical and psychological needs on a daily basis.65 However, parents appreciate dialog with professionals beyond informational topics such as the development of feeding skills or behavioral management. Parents want professionals to share conceptual knowledge as well.48 The timing of parents’ ability to use this knowledge and engage in home programs varies appreciably from the time of initial diagnosis of disability through adjustment to their situation, and in qualitative studies having the need for information met is often deemed inadequate.65,131
Families who are coping with stress have reported that “the ability to build on personal experience and expertise” (p. 261) is an essential coping strategy.47 Parents can develop this knowledge through parent-to-parent groups in which families can share strategies with other families who have similar types of issues.40,177 For therapists, listening to parents and individualizing the information, as well as connecting family members to other resources, helps build the parents’ personal resources. The CanChild Centre for Childhood Disability Research has developed a formal, individualized information Keeping It Together™ (KIT) for parents, which has been shown to increase parent “perceptions of their ability and self-confidence in getting, giving and using information to assist their child with a disability” (p. 498).153 Therapists must remember that many parents are the experts on their own children and often have extensive information or stories to share about what works for them.11
Time Resources
Daily and weekly activities, by their very definition, require time investment, and every family at one time or another experiences stress because there are too many things to be done and not enough time. Children with disabilities often depend on caregivers longer than typically developing children, and the extra daily care or supervision needed can extend for many years.30,40,97 The amount of time spent in shared activities around caregiving can be wearing and frustrating and can reduce the family’s time for recreation and social gatherings. In a study of more than 200 families of children with Down syndrome, mothers spent three times as much time in childcare as mothers of typically developing children.10 The fathers of children with Down syndrome spent twice as much time in childcare as fathers of typically developing children. One commonly used coping strategy of family caregivers is to organize the day into well-established routines.47 Helitzer and colleagues found that mothers of children with disabilities reported that they used “structure, routine, and organized time management as a way to maintain a sense of control” (p. 28).57 However, their busy, structured lives often were disrupted by crises, such as trips to the hospital or urgent care department and, as a result, the mothers felt they were “living on the edge” and that every disruption in their routines was experienced as a crisis.
Crowe found that mothers of children with multiple disabilities spent significantly more time in child care activities and less time in socialization than mothers of typical children.29 In a qualitative study of parents of children with chronic medical conditions and disabilities, parents reported that they had round-the-clock responsibilities in administering medical procedures and performing caregiving tasks.23 They described the challenges of “always being there” to care for their child’s extraordinary medical needs and to engage their very dependent child in developmentally appropriate activities. These parents, whose children were often ill and even hospitalized, were always “on call” and often had to cancel activities outside the home when the child was ill.
Service providers can be a source of threat to the family’s time and emotional resources. Providers seeking to implement family-centered practice often expect parents to take on responsibility for implementing therapy.93,96 Greene described how her family “experienced the burden of home programming” as occupational therapists, physical therapists, and speech and language pathologists made separate recommendations, each requiring a chunk of the day.93 These home assignments became a source of guilt and marital difficulty as the family struggled to meet the needs both of their daughter and of her typically developing sibling. Less experienced therapists, in their enthusiasm to help, often neglect to consider the family’s time commitments when offering suggestions.
Emotional Energy Resources
Families of children with disabilities may experience special forms of stress, social isolation, and less psychological well-being than families with typically developing children.9,32,102 The idea that parents of children with disabilities experience recurrent grief is pervasive in the literature, yet disputed.41,166 Fox et al. conducted a qualitative investigation to understand how children with developmental delays and behavioral problems influenced the family’s lifestyle.40 Their parents suggested that dealing with the child’s needs required a lot of emotional energy from the different family members. One theme—“It’s a 24-hour, 7-day-a-week involvement”—was supported by stories of frustration from responding to challenging behaviors and applying parenting practices that would meet the needs of their children. Parents reported that individuals who offered “a shoulder to lean on” and professional assistance, encouragement, and information were particularly helpful.
Studies have shown that parents of children with disabilities may experience anxiety and depression.55,120 Mothers appear more vulnerable than fathers. In a large comparison study of families of children with autism, developmental disability, or without disabilities, Olsson and Hwang found that mothers of children with autism were more depressed than mothers of children with mental retardation and that both groups were more depressed than mothers of children without disabilities. The fathers in these families did not exhibit more depression than fathers of typical children. Mothers’ self-competence may be more related to the parenting role than that of fathers, and mothers may be more vulnerable when stressful difficulties arise in the parenting domain. Hastings, investigating levels of stress, depression, and anxiety in a cohort of 18 couples with children with autism, found that mothers and fathers felt similar levels of stress; however, mothers were more anxious.55 Mothers may feel more responsibility for the child55 and may take on a larger part of the extra care that a child with disabilities requires.120
When children have chronic medical problems that require round-the-clock use of technology, parents often find themselves exhausted and sleep deprived. Some of the consequences for parents whose children require routine medical procedures are anxiety and depression because of the risks inherent in the administration of the medical procedures. When parents must administer medical procedures beyond the typical parent–child activities of nurturance, caregiving, and play, they appear to experience stress and anxiety. In addition, they often do not have the time and resources to access energizing and relaxing activities, such as socializing and recreation.9,80
Stress level in families with children with chronic diseases or conditions has been found to have a strong relationship with family income and family function, with lower income associated with higher stress, especially as the children become adolescents.9 Parents with limited resources, whether financial, educational, emotional, or a combination, are at higher risk of experiencing parental stress, which may lead to abusing or neglecting children with disabilities.150 The added needs of children with chronic health issues or behavioral or intellectual limitations can push the low-resource parent over the edge of reason to a point where maltreatment of the child is the consequence.58
SOURCES OF DIVERSITY IN FAMILIES
Families with children who need occupational therapy services come from many different backgrounds and in a variety of forms, and therapists working with these children have the rewarding opportunity to learn from their families. Therapists must find a balance between focusing on the similarities and appreciating the differences among families.1 Because individuals are inclined to view the world through their own cultural model and to use personal experiences as a point of reference, it takes professional commitment to become skilled at working with a variety of different families.
Family researchers and service providers have focused on understanding how a family’s culture and traditions affect child-rearing practices and how these might be adaptive, strengthening a family or bringing about positive developmental outcomes.83 Families have patterns of different characteristics (e.g., family structure, family income, having a family member with a disability) and the ecology in which families’ function varies (e.g., religious opportunity, crime rate in the neighborhood, period in history). Therefore, generalizations of research findings about diverse family groups are rarely accurate, and sensitivity to the unique differences of each family is always needed. Three sources of family diversity discussed next are the family’s ethnic background, family structure, and socioeconomic status. A fourth section considers differences in parenting styles and practices.
Ethnic Background
Ethnicity is a term used to describe a common nationality or language shared by certain groups of families. It tends to be a broad concept, and heterogeneity among families within groups described as Latino, African American, Anglo-American, or Asian should be anticipated. Furthermore, people may identify themselves as belonging to more than one ethnic group, making it harder to use the concept to guide the way the therapist works with families. Coll and Pachter offer two reasons for retaining ethnicity as an important variable when working with families raising children.27 First, families that are not part of the dominant ethnic group experience a discontinuity between their cultural models and the majority culture that shapes the social institutions. Thus a cultural as well as a language gap may exist between health systems and educational programs and the families of minority ethnic groups.2 In addition, as the proportion of ethnic groups grows in the United States, the sons and daughters of these groups make up a larger proportion of the overall population of children in this country. Occupational therapists who serve children with special needs can anticipate working with an ever-growing, ethnically diverse group of families. The influence of ethnic background on the ways a family fulfills its functions and raises its children is a complex topic that is merely introduced here. Resources on the Evolve website provide further information.
Ethnic groups share cultural practices that can determine who has the authority to allocate family resources and a value system that sets priorities for family routines and special events. Families in an ethnic group may have similar daily activities, ways of interacting, and ways of thinking about events, and may find similar meaning in their routines, traditions, and celebrations. Differences among ethnic groups are expressed in gender role expectations, child-rearing practices, and expectations at certain ages, as well as in definitions of health and views of disability. Cultural practices are not static traits; rather, they change when members of the group adapt to new situations.53
Although every family wants their children to be successful members of the community, their vision of what this entails varies among different ethnic groups and influences how children spend their time and what is expected of them.88 Carlson and Harwood studied the structure and control Anglo-American and Puerto Rican mothers asserted over their infants during ADLs.22 The researchers observed mothers in their daily routines and found that Puerto Rican mothers controlled their infants’ behaviors more than the Anglo-American mothers, who tolerated more off-task behaviors. Carlson and Harwood pointed out that Puerto Rican parents are guided by the anticipation that their children will join a Puerto Rican community that values respectful cooperation. The Anglo-American willingness to follow the child’s lead is compatible with valuing individual autonomy. Without insight into ethnic differences, a therapist watching parent–child interaction may mistakenly interpret a Puerto Rican mother’s physical control and effort to divert a child’s attention to the needs of others as intrusive and insensitive to the toddler’s sense of identity and self-efficacy. Therapists avoid this type of error by understanding what a parent hopes to achieve before formulating an opinion about the appropriateness of a family’s interactive routines.
The influx of recent immigrants expands the diversity within ethnic groups that therapists will encounter. Within a community, one family may have members who have been in a country for generations, and the family next door may have recently relocated to the country. Migration affects the family and how it functions at multiple levels.37 First, relocation to another country frequently includes a series of separations and reunions of children and family members. Suarez-Orozco, Todorova, and Louie found that 85% of the 385 youths in their sample of recent immigrants had been separated from a parent and nearly half had lived apart from both of their parents during the process of family migration.155 Although the length of separation varied, it was not unusual for a child to have been apart from the father for 2 years or longer. In some families, the tradition of having a child live with a grandparent or other relative may buffer the initial separation and help reduce the stress. Yet when the children are brought into the United States to join their immigrant parents, they must leave behind a caregiver and familiar community. Researchers found that reunification could be protracted, because families may not have been able to pay for travel or housing for all family members, meaning that people arrived in stages, months or years apart. In addition, when both parents immigrated ahead of their children, it was not unusual for the children subsequently brought into the country to have to adjust to living not only with their parents again but also possibly with younger siblings born in the new country. Therapists working with immigrant families need to be sensitive to the possibility of family friction, depression, and a sense of uncertainty among family members.
For each immigrant family, the process of acculturation varies; this is the process of selectively blending their traditions in how things are done, what activities are important, and interactive styles with the cultural practices of the majority group.37 Parenting practices might insulate children from exposure to the language, ways, and values of the majority culture until the children go to school. For example, enrolling children in child care programs may seem the equivalent of child abandonment in some cultures, and families may bring a grandparent with them as part of the immigration process so that both parents can find paid employment. This may mean that children entering school have had few experiences beyond their home environment. In school, surrounded by new peers, the children’s acculturation process is influenced, creating conflict among family members.27 Unfortunately, feeling disconnected from home or discriminated against at school leads some youths to drop out of school as a way to ease the tension.53 When this situation includes a child with disabilities, the occupational therapist has more to consider in addition to the specific needs of the child.2
Family Structure
Family features, such as the presence of children in the household, marital status, sexual orientation, and age/generation, are factors described as the family structure.1 It is important to remember in working with families that acceptance of diversity within the family structure and family subsystems is necessary to be effective.
Family structure in combination with its cultural model influences how the family organizes itself to fulfill essential roles, such as caregiving of dependent family members or allocation of family resources. The idea that there is a best family structure in which children are raised is a myth.174 For example, single-parent families have been portrayed as dysfunctional and as leaving children more vulnerable to having problems3; yet single parents have also been found to raise competent, well-adjusted children.114 One third of the births in the United States are to unmarried women.117 The majority of single-parent households are headed by women; however, the number of fathers who are single parents has increased.168 The Fragile Families and Child Wellbeing Study is an attempt to discard myths and replace them with evidence that will guide intervention and policy making to support low-resource families.105 Some of their findings demonstrate that “Unwed parents are committed to each other and to their children at the time of birth…Most unmarried mothers are healthy and bear healthy children” (p. 3).105
Larson sampled the activities and emotions during activities of employed mothers in two-parent or single-parent homes of adolescents and found that the stereotype of the single-parent home was not necessarily the rule.87 Single mothers in his study had less stressed, more flexible routines after a day at work, and friendlier relationships with their teenagers than did their counterparts in two-parent homes. Mothers with a husband reported more hassles trying to make and serve dinner by a designated dinnertime and experienced housework as more unpleasant. Larson speculates that the negotiation of responsibilities and trying to live up to expectations of being a “wife” in a two-parent home contributed to these differences. Clearly, every family structure has advantages and risk factors.87
Gay, lesbian, and bisexual families reflect one variation of family structure that therapists encounter. Children may be the products of a parent’s previous heterosexual relationship or may be born or adopted into families headed by adults who are gay, lesbian, or bisexual.127 Because parents do not want to expose their children to the prejudice of homophobia, many are reluctant to be identified, and estimates of the number of parents who are not heterosexual range from 1% to 12% of families.151 Many of the issues and needs of all parents are expressed by gay, lesbian, and bisexual parents.125
Because sexual orientation has been the basis for judicial decisions that have denied people parenting rights, recent studies have investigated the issue of whether the sexual orientation of the parent affects the child’s behaviors or influences the child’s sexual orientation. Studies comparing the psychological adjustment and school performance of children being raised by lesbian or gay parents to those of children with heterosexual parents have generally found no differences.127
A final source of stress, divorce, the way many single-parent families are formed, can cause disruption that alters household routines, traditions, and celebrations. Sometimes the stress between the marital partners leads to impaired occupational functioning of the children and the divorce may come as a relief. Factors that contribute to positive developmental outcomes for children after couples break up include the parents’ psychological well-being, economic resources, whether the family is part of a larger kinship network, and how parents navigate the separation and dissolution process. For example, Greene, Anderson, Hetherington, Forgatch, and DeGarmo reported contradictory findings regarding how well children adjust after their parents’ divorce.49 Initially, parenting practices were erratic, and the parent–child relationship, especially between custodial mothers and young sons, could be stormy. Yet two years after a divorce, many of the problems had diminished; therefore, some of the consequences of divorce depend on where in the adjustment process researchers conduct their study. Anderson argued that the best way to strengthen single-parent families was to empower parents by recognizing their strengths and encouraging them to reestablish routines.5 The therapist can be supportive by acknowledging that these parents face considerable challenges in raising children alone and by aiding the parent in identifying resources such as friends, extended family, religious groups, and other single parents.
When birth parents are unable or unavailable to care for children, kinship care is a way to preserve family ties that might be lost if children are placed in foster homes.75 Households in which grandparents are raising their grandchildren are examples of those providing kinship care and are a growing source of differences between families. These families, primarily headed by middle-aged or older women and disproportionately by women of color, are often formed after adverse events, such as child neglect or abandonment, maternal substance abuse, or incarceration or death of the parents.72,75,85 Much of the research on grandparents raising their children’s children explores the issue of caregiver stress. Evidence from both qualitative and quantitative studies suggests that grandparents caring for their grandchildren (or great-grandchildren) find it both rewarding and challenging.8,75 Grandparents reported satisfaction in being able to “be there” for the child or children and reported that they have had to learn new parenting skills in response to the new generation. However, they also experienced parenting stress, which was exacerbated when they lacked social support, had limited financial resources, or were in poor health. When a child is reported to have behavioral or health problems, the caregiving demands increase the grandparents’ sense of emotional distress.56
During their childhood, many children experience changes in the family structure. Unwed mothers may marry, or parents in a family may divorce and later one or both may remarry. A child may transition from a two- to a three-generation family when an aging grandparent moves into the home. Therapists should talk with family members in an inclusive manner that does not suggest an assumed family structure. Asking a parent or child, “Can you tell me about your family” does not suggest any expectations about who is in a family and helps family members openly express their definition of who is in their family.
Socioeconomic Status
The influence of the family’s SES on children’s occupations and development is complex.62 SES reflects a composite of different factors, including the social prestige of family members, the educational attainment of the parents, and the family income. These factors influence each other and have various implications for how a family fulfills its functions, by influencing the degree of access families have to activities and experiences for their children. Education influences parenting practices by affecting how an adult incorporates new ideas about a healthy life style and child development into these practices. Factors that influence employment, such as a below-average education, inability to speak English, or disability of a family member, leave families more vulnerable as job opportunities come or go. When employment is found, the job may not pay enough to meet the family’s needs, leaving the family with no resources if unexpected events occur.
Researchers have demonstrated that low income or limited education is associated with differences in the quality of parents’ interaction with their children.62,135 In these circumstances, parents may not be as responsive, addressing the child less often, providing fewer learning opportunities, and not engaging in an interactive teaching process. Parish and Cloud present a compelling review of the literature on the factors that lead children with disabilities to be more likely to live in poverty.124 These factors include the increased cost of raising such a child and the decreased ability of their mothers to be employed, because of both the needs of the child and the lack of available child care. A recent study in England found the incidence of very preterm birth was much greater among mothers of lower SES, and preterm birth raises risk factors for the child.148 Suggestions for working with families with low SES are addressed later in the chapter.
Therapists need sensitivity and skill to work with families across the SES continuum. Although this factor has not yet been addressed in the professional literature, having higher SES clearly affords additional opportunities, time, and expectations of parents for those experiences they desire for their children. The concept of “helicopter parents” who hover over every aspect of their child’s life tends to extend to their children with special needs. Therapists must draw on their many skills in assisting these parents to find balance between what can be done through direct service, what they can do themselves, and how to allow a child space in which to be a “typical” child.
Parenting Style and Practices
The individual interactive style and parenting practices of an adult raising a child are additional factors that must be considered in gaining an understanding of the diversity of families. Steinberg and Silk distinguish between parenting style, the emotional climate between parent and child, and parenting practices, goal-directed activities parents do in raising their children.152 For example, two parents may believe that if they want their children to do well in school, it is their responsibility to spend time with the children reviewing their homework (a parenting practice). However, the interpersonal interactions while they engage in this shared activity (parenting style) can be distinctly different. One parent may discuss the work and help the child find solutions to problems, whereas the other parent may feel he has the emotional energy only to point out errors. There is no test or license for parenting in this country. During the time of extended families, there was mentorship and modeling for parenting practices. In today’s nuclear families, stresses run higher and skills may be lacking. When work separates the family, or as the dysfunctional practices of previous generations come to play in the current generation, there is great need to help parents learn parenting skills. Some individual professionals and disciplines, often State Extension Services, are creating programs to teach parenting skills. This is an area in which the holistic occupational therapy knowledge base and framework would prove quite beneficial.
A well-adapted child develops as a result of from complex interactions between parenting style and practice. Regardless of ethnic background, poverty status, and parenting practices, a parenting style that is warm, responsive, and positive and that provides structure and learning opportunities is associated with children who rank higher on many measures of social and cognitive development.6,152
Dialog between parents and therapists does not always go smoothly, and the collaborative nature of the relationship is sometimes lost if the parent and therapist hold different ideas about parenting style or parenting practices. This tension increases if the parent worries about the therapist’s disapproval.91 The professional cannot assume greater knowledge than the parent about what the child needs to be able to do or about the interactive style that best accompanies shared activities (Research Note 5-1). Therapists can be supportive and can empower parents by working with them so that family resources such as time and emotional energy are available when shared activities occur.
 RESEARCH NOTE 5-1
RESEARCH NOTE 5-1
This study used expert raters to examine videotapes of daily dressing and snack activities to measure qualities of engagement and directiveness in caregiver–child interactions when the children were 30 months old. Thirty-six pairs were divided into three groups (healthy children born full term, and children born prematurely and very low birth weight with and without white matter disorder) and matched on birth history, maternal education, ethnicity, and child gender.
There were no significant differences between groups for the average caregiver and child ratings, but correlations between caregiver directiveness and positive caregiver engagement ranged across the three groups: parents of full-term infants had higher engagement when they were less directive, whereas parents of children with white matter disorder had high engagement with high directiveness. The correlations between the caregiver and child qualities of positive engagement were small in both very-low-birth-weight groups, suggesting more variability in the responses.
Results suggest that patterns of caregiver interactions during daily activities may vary according to the child’s abilities, as defined here by the level of biological risk. Caregivers of children with the greatest risk were both engaging and directive of their children during the activities, whereas caregivers of full-term children were more positive when less directive, and less positive when the child’s behavior required them to be more directive. The findings suggest that caregiver–child interactions vary appreciably according to the level of the children’s abilities.
During activities of daily living (dressing and eating) caregivers appear to adjust their level of social and emotional assistance to the level needed by their young child.
Full-term children who are more capable in these tasks need appreciably less caregiver support.
Daily activities and play activities afford different interactional opportunities; more research is needed in both areas to assist clinicians in working with caregivers and their children.
Kadlec, M.B., Coster, W., Tickle-Degnen, L., & Beeghly, M. (2005). Qualities of caregiver–child interaction during daily activities of children born very low birth weight with and without white matter disorder. American Journal of Occupational Therapy, 59, 57–66.
AN ECOLOGIC PERSPECTIVE
As with any other open system, the social and physical features surrounding the family influence it. Cultural models are partly shaped by values, beliefs, and ways of thinking shared with others who have similar backgrounds.43 An ecologic and transactional perspective of development and parenting encourages therapists to consider family resources and the adult’s psychological background, personal history, and personality, which are in constant interaction with characteristics of the child being parented.21,84,136 In addition, the occupations of families do not take place just within the home. Many of the resources for family activities that enable families to function effectively are available in the neighborhood and the larger community. Proximity to places of worship, stores, high-quality child care, and friends is part of the family’s ecology and influences how family members spend their time. At a slightly more removed level, family functions are supported when social institutions make services available (e.g., a health department that runs an immunization clinic, the volunteer group that helps parents choose the best childcare centers, businesses that raise money for a school system).
The advantage of an ecologic perspective is that it raises awareness of the ways things distant from the family and beyond its control influence how the family fulfills its functions. For example, a large corporation that decides to cut its work force causes job loss in the neighborhood and forces people to leave the area to find employment. Suddenly the parents no longer have a babysitter and have to change leisure time activities. On an even more distant level, shifts in public attitudes during a particular period of time influence the environment and resources for families. For example, families can be affected by the attitudes of voters who determine public policies about the rights of people with disabilities, universal health care coverage, welfare reform, and the rights of undocumented immigrants.39
Further illustrating the importance of an ecologic perspective, Stacey and Biblarz noted that child development researchers need to examine not only a family’s structure, but also how the family fits into its community.151 When parents who are gay or lesbian reside in a community accepting of different orientations, the parents may be more likely to engage in open discussion about sexual preferences. Not being part of such a community can be considered a risk factor.122 Single mothers, especially single adolescent mothers, may be at similar risk for a sense of being disconnected from the community.92 A family living under these circumstances may be less open to social support offered by people outside the family at times of crisis and thus not as resilient as one living in a community that is accepting of a parent’s lifestyle.
For therapists working with children with special needs and their families, it is especially important to take an ecologic perspective and to investigate whether families can access a range of community activities that will enable them to fulfill their functions. For example, in a survey of family-centered services in Ontario, King et al. found that communities vary in how they support the inclusion of families raising children with disabilities.78 Limited access to recreational resources and lack of social support for parents reduced the participation of children with special needs in leisure activities. Therapists who strive to enable children’s occupations that lead to participation in community contexts are no longer focused on the occupation of individual children. Turnbull, Turbiville, and Turnbull propose a collaborative empowerment model in which families draw on their knowledge of their children’s abilities and receive support from other families and professionals to make changes at the community level.163 By joining with families in advocating for children’s rights, occupational therapists contribute to a synergistic force that increases the family’s access to resources outside their homes and helps them function as a family.
SUPPORTING PARTICIPATION IN FAMILY LIFE
Development of Independence in Self-Care and Health Maintenance Routines
Occupational therapists who understand the nature of family occupations can help parents manage and adapt daily living tasks with their children. The therapist assists the parent in establishing goals about daily routines and tasks that the parent values, and then observes how they are being done. The therapist may engage the parent in a discussion of alternative strategies, or may model techniques that help the child perform daily living activities with greater skill and independence (Figure 5-8). With knowledge of the biomechanics of lifting and moving, the therapist considers whether the task is performed in a way that conserves energy and avoids injury. This consideration is especially important when a physical impairment significantly limits mobility. Strategies to help a 5-year-old bathe, dress, and use the toilet may no longer be safe for the parent’s back when the child becomes an adolescent. A therapist’s knowledge of adaptive solutions to self-care, such as Velcro fasteners, or, if standing balance is too challenging, dressing while sitting, can be quite helpful to parents, especially first-time parents.111

FIGURE 5-8 Matthew’s bath time routine allows him to practice a range of skills, including play and social interaction. Courtesy Jill and Mark McQuaid, Dublin, Ohio.
Becoming independent in self-care occupations frequently requires repeated practice until performance becomes a habit. Occupational therapists who understand principles of behavior management can help parents reinforce a child’s efforts at independence. Continuity in frequently repeated self-care occupations, such as using the toilet and eating with utensils, is increased through communication among the occupational therapist, teacher, parents, and others. A notebook that the child carries between school and home may serve this purpose.
Routines that lead to more independence in self-care provide opportunities to enrich the child’s learning. During dressing, the child can improve strength by pulling up pants and increase vocabulary by naming colors found on the clothing. Therapists can suggest how to turn tasks into learning situations. However, as with all suggestions, the parent weighs the costs and benefits. Often the occupational therapist hears, “That just won’t work for us.” When this happens, a decision must be made regarding whether the task can serve two objectives, or whether the simple goal of independent self-care is sufficient.
Any extra time that the therapist asks the parent to spend teaching new steps in self-care should be in response to a parent’s identified need. In addition, the effort should be justified by evidence that the altered routine has a good chance of bringing an immediate change. Alternative suggestions should be made quickly when an adapted technique does not work. The goal of occupational therapy recommendations should be to benefit the entire family by increasing the child’s independence at minimal cost in time and energy to the parents. As stated by Bernheimer and Keogh, “Successful interventions are the ones that can be woven back into the daily routine; they are the threads that provide professionals with the means to reinforce, rather than fray, the fabric of everyday life” (p. 430) (Figure 5-9).12

Participation in Recreation and Leisure Activities
King, Law, Hanna, et al. and King, Law, King, et al. propose that the family’s ability to engage family members in recreational and leisure activities is the result of a multidimensional process that includes the community, the family, and the child with a disability (Figure 5-10).77,78 Their conceptual framework draws on literature in leisure studies and work with families of children with special needs. Some factors can directly influence participation, such as availability of an inclusive program, wherein peers and activity leaders support and believe in the child’s ability to participate (Figure 5-11). Other factors, such as the extent to which the parents perceive acceptance from friends and neighbors and how parents view being active, indirectly shape whether families choose to participate in recreational activities in the community. Parents of children with developmental delays and behavioral problems will sometimes stop taking their child out in response to negative reactions of other people to their child’s noises or tantrums.41 Parents of children with developmental coordination disorder may need to consider individual rather than team sports as options for their children (Figure 5-12).111 Resources, such as money to purchase equipment and time to transport children, influence the extent to which a family can participate in recreational activities. If families can afford vacations, many theme parks are now more accommodating to their needs (Figure 5-13).

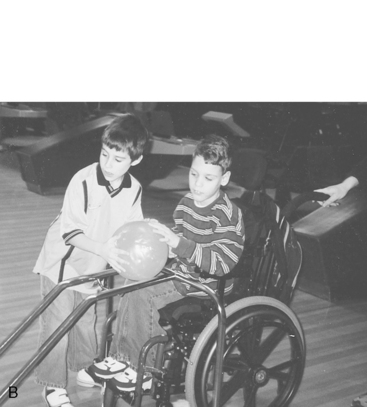
FIGURE 5-10 A, Recreational opportunities in the community provide an important family occupation. B, Matthew bowls with a friend. Courtesy Jill and Mark McQuaid, Dublin, Ohio.


FIGURE 5-11 A, Most skiing facilities have equipment for children unable to stand independently. B, Wee Can Ski provides equipment for children with a variety of disabilities.



FIGURE 5-13 A, Dad pulls his tired children through a theme park. B, Years later, Todd returns the favor.
Occupational therapists can communicate that they respect the value of recreation and leisure by including it in assessment and intervention plans. Therapists can suggest adapted equipment the child can use to make recreational activities possible. With the passage of the Americans with Disabilities Act in 1990, more recreational opportunities became available to individuals with disabilities. Information about community recreational activities is often available in local newsletters or on websites (Figure 5-14). Therapists can note which activities are accessible and appropriate for children with disabilities. They can also suggest strategies for making the family’s outings more successful, such as providing headphones for a child with auditory sensitivity. Practitioners can also help parents accomplish caregiving tasks efficiently to make more time available for recreation. Scheduling therapy and education programs to enable families to engage in recreational activities can also support family function.
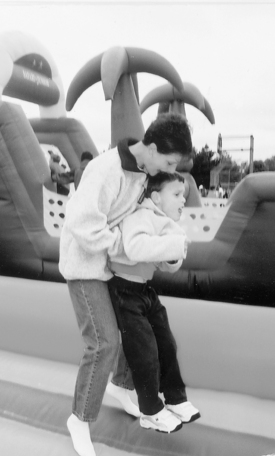
Socialization and Participation in Social Activities
Socialization is needed not only for health; it is an important mechanism for preparing family members to enter their cultural group and participate in community activities. Most families of children with disabilities, particularly those with problem behaviors, report that far too few opportunities exist for participation in the community. Families perceive that they are the only socialization agent for their children because community social activities simply do not accommodate their children.161 In addition, children with disabilities may interact more frequently with adults than with peers, particularly if they have classroom aides. Constant interaction with adults to the exclusion of peers may exacerbate feelings of incompetence in interactions with peers.
Children with disabilities, particularly those with problem behaviors, face a “glaring void of friendships” (p. 224).161 Educational and intervention programs should focus more attention on helping friendships to develop and flourish. Although professionals have created more activities and environments that include children with disabilities, they have not necessarily encouraged mutual and reciprocal friendships to develop. Turnbull and Ruef urge professionals to focus on understanding the components of friendship and the connections that form into mutual friendships.161
The presence of disability in the child may also create barriers to the parents’ opportunities to socialize. Families of children with special needs often feel that they have less time to spend participating in social activities.30 Because childcare is typically difficult to arrange and must be set up in advance, taking advantage of spontaneous social opportunities is rarely possible.129 Children who act out or demonstrate disruptive behaviors may be particularly difficult to manage in social situations.
Parents often find it helpful to develop friendships with other parents experiencing similar circumstances. A number of studies have found that increased social supports are associated with healthier family functioning and lower levels of stress.44,170 Helitzer et al. implemented a program for mothers of children with disabilities to address their concerns and difficulties in daily routines and coping.57 The mothers were encouraged to provide emotional support to one another and to assist each other in resolving specific dilemmas in daily routines. These mothers perceived that they had changed their self-image and coping strategies through participation in the group sessions. They placed great value on having “a supportive opportunity to discuss their feelings and thoughts in a setting that was nonjudgmental and comfortable” (p. 408).170 Similar programs offer parents social supports and strategies to help in coping, as well as practical ideas that make everyday life easier, help them adapt to stress, and give them a more positive attitude toward their children.177 These social supports appear to be of equal or greater importance to families than professional services.20
Fostering Readiness for Community Living
Families of children with disabilities express concerns about the future of these children, particularly once they leave school. They worry that these children will not have the life skills needed to live independently.82,97 As children become adolescents and then young adults, parents need information on possible living arrangements in the community. Often young adults are capable of leaving home but need support persons and arrangements for short- or long-term supervision and monitoring. These young adults may not have many options, and the options either may be overly restrictive (to secure funding) or may not provide sufficient supervision. Parents of young adults with disabilities emphasize the need for information on housing, particularly innovative supported living arrangements. For these young adults to succeed in living in the community with support, families need assistance in finding roommates, other support persons, funding, and arrangements for supervision and monitoring.97,161
Young adults with disabilities face many challenges in finding and maintaining employment,133,161 but there are examples of successful transitions that give hope to families and professionals alike (Appendix 5-A).97,166 Families and professionals need to work together to advocate for changes in the community to create opportunities for young adults to become employed and productive members of society (see Chapter 27).
FAMILY ADAPTATION, RESILIENCE, AND ACCOMMODATION
Despite the inclination of families to organize their activities into predictable patterns in the form of their routines, traditions, and celebrations, because dynamic systems that exist over time, change is inherent in being a family. Internal or external forces press for family adaptation or changes in what they do and how they interact. Pressures that can alter family activities include daily hassles, such as multiple demands on a parent’s time or unpredictable transportation, as well as positive life transitions, such as the birth of a baby or an older son’s leaving home to take a job, which alter household routines. Other events requiring that families adapt their routines and traditions may be unexpected, such as job loss, illness, or an event that affects the community (e.g., a natural disaster). When families experience new demands and stresses, they continue to function by creating meaning about the stressful event and by working as a system to adapt and continue their daily activities.
The process of adaptation starts when a family recognizes the state of affairs, an interruption in their activities, or a loss of emotional well-being.46,128 Families use a variety of strategies to make sense of what is happening.174 For example, they can tell stories about a similar instance or another generation that experienced a comparable event. They can redefine what seems like a catastrophic event by making a comparison with another family in which something they see as more devastating has occurred. For example, finding spiritual meaning in an adverse event is a way of changing how it is experienced. Regardless of the strategy used, by co-constructing their own definitions of events, families diminish the feeling of being out of control and, based on how they define the state of affairs, they can allocate resources to manage the situation.
Families demonstrate resilience when they draw on resources to reconstruct their routines or create new ones that enable them to continue to fulfill family functions. For example, McCubbin, Balling, Possin, Frierdich, and Bryne identified factors that contributed to families’ resilience and ability to manage when children were diagnosed with cancer.101 Based on their interviews of 42 parents, they found resiliency factors that made it easier for the family to construct new routines to deal with the situation. These families drew on their own resources, such as religious beliefs and the emotional support of each other, and then reset their definition of how they would live or operate as a family. The parents rearranged their routines so that one parent could be with the child receiving inpatient medical treatment while the other stayed at home with the siblings. Parents reported that they also drew on resources in their community. For example, when neither parent had time to cook, members from their church brought in meals so the family could share meals together. In a longitudinal study of families with a child with developmental delays, Bernheimer and Weisner refer to these changes that maintain daily routines as accommodations.13 They identified 10 accommodation domains (e.g. services, marital roles, social support) that varied in frequency of need over time. When the children were 3 years old, the highest-frequency areas of accommodation were childcare tasks, sources of information, and support. They note, as has been mentioned previously, that family daily routines were strongly influenced by cultural and family values and goals.
The family members’ ability to communicate with each other is important to co-construction of meaning and adaptation of daily routines. Families engage in affective and instrumental communication. In affective communication, family members express their care for and support of each other. In instrumental communication, members give each other role assignments, establish schedules, make decisions, and resolve conflicts. Clear, effective communication is important for establishing meaning for an event or problem and for planning resolution of the crisis. As Patterson put it, “A family’s belief in their inherent ability to discover solutions and new resources to manage challenges may be the cornerstone of building protective mechanisms and thereby being resilient” (p. 243).128
A child with exceptional health or developmental needs creates new demands on a family system. Families with sufficient resources and flexibility respond by adapting their daily routines and special events so that they can fulfill their family functions. Bernheimer and Keogh illustrated the importance of family resilience in the conclusion of their longitudinal study of families of children with special needs:
The majority of our families are doing quite well. Like the children in our study, they share common characteristics but are strikingly unique in many ways. They are adapting and adjusting within their physical and cultural environments, and are making decisions about the organization of their lives and about their children, consistent with their values and beliefs and with what they think is important (p. 429).12
Occupational therapists who recognize the power of daily routines and family traditions are sensitive to disruption of a family’s pattern of activities and can assist parents in reestablishing or creating meaningful family routines. For example, the occupational therapist may suggest strategies that enable a child with a gastrostomy tube to participate in the family mealtime (e.g., explaining to the parents what foods the child can safely “taste” at the dinner table). The therapist can also help families find ways to make important traditions possible. If a child with autism has difficulty in a new environment, the therapist can recommend ways to help the child adjust by suggesting that he carry a CD player with his favorite music as preparation for leaving home for the traditional family vacation.
The fact that most families adjust successfully to children’s disabilities should not lead occupational therapists to ignore the initial and ongoing challenges that families face. Times of coping and adaptation vary according to whether a family must adjust to an acute traumatic event leading to a disability or the family gains a gradual, unfolding understanding of the child’s developmental differences. After the diagnostic period, when the child’s problems are identified, the family goes about the process of living. During this period, the demands for adaptation and coping vary. The following sections describe how occupational therapists can offer support, intervention services, and education to families.
PARTNERING WITH FAMILIES
Parent–professional partnership grows from an appreciation that by working together, both the occupational therapist and the parent can share important expertise and knowledge that will make a difference in the child’s life. The sustained involvement and special insights families bring have been discussed earlier; this section goes into more specificity regarding the different ways occupational therapists work with families.
Family-centered services refers to a combination of beliefs and practices that define particular ways of working with families that are consumer driven and competency enhancing. Such beliefs and practices are necessary if occupational therapists are to be successful in team development and implementation.159 Definitions range from acting as service coordinators, to addressing the needs of the family for financial and social resources as part of an intervention program, to empowering family members as part of a team to make decisions relative to their child’s program.96 Three complementary models for family-centered services are (1) family support, (2) direct services, and (3) family collaborative education.
Family support is designed to bolster a network of social support to enhance the family’s natural strengths and family functions. DeGrace recommended not being so focused on the child’s issues that the therapist does not recognize how the disability impacts family occupations.32 Social support, such as being able to talk with other parents, decreases the family members’ feelings of isolation and stress.13,102,177 Promoting a family’s well-being through emotional support and practical suggestions allows families to engage in responsive interaction with their children. The occupational therapist’s role in providing family support is to help the family secure needed resources and capitalize on its existing competencies and strengths.51
Direct services are provided when the therapist engages a child in an activity with the goal of promoting the child’s skill acquisition and minimizing the consequences of a disability. This is the traditional and, for the therapist and most institutional facilities, the more reimbursable form of interaction. Family members should be present and participating in the therapeutic activity, but the occupational therapist’s attention is on promoting the child’s engagement in the activity. Unless handled with skill and sensitivity to the family, this type of service may fall outside family-centered practice.
Family collaborative education has a number of purposes and should be individualized to the families’ interests, learning styles, and knowledge levels. In parent-mediated therapy, the caregiver is taught how to engage the child in an activity designed to achieve a parent-identified goal or outcome.7 Strong evidence indicates that the more parents know about development, the more responsive and supportive they are in interacting with that child and the better prepared they are to foster optimal development.146,153,171 Parents of children with delays are not looking for developmental milestones; their efforts to engage their children in daily activities are not informed by hearing that, typically, children feed themselves with spoons between 15 and 24 months or don simple clothing between 2 and 3 years. Parents want to hear how children with special needs learn things that other typically developing children seem to teach themselves. Kaiser and Hancock reported on an effective, systematic approach to teaching parents new skills.73 First, the parents identified the outcome or skills they wanted to foster, and the interventionists then guided them in what to do and how to implement child instruction within the natural flow of everyday activities.
Often a variety of methods may be needed to engage the different family members. Ninio and Rinott recommended a number of strategies for encouraging the father’s participation.118 Programs that seem to best support the father’s involvement actively attempt to involve the father in planning meetings, offer convenient scheduling for therapy and meetings such as evenings or weekends,76 focus on providing information about the disability and community resources, and provide opportunities for the father to enjoy activities with his child. When the father is the family’s primary decision maker, it is critical that he receive complete information about the decisions that need to be made, including the purchase of assistive technology and accessing resources for the child. Margetts and colleagues focused on the potential of engaging grandparents,98 whereas Trent-Stainbrook and colleagues researched a successful program in which older siblings were taught how to interact responsively with their younger sibling with Down syndrome.158
Sharing information with families is likely to be most effective when the child demonstrates interest in doing the activities the team has targeted. At that point, the therapist becomes a “coach” who facilitates an exchange of ideas that helps the parent discover ways of helping the child learn the activity.52 This dialogue includes periods of observation and reflection. Coaches bring pragmatic understanding of the intervention strategy and serve as a resource.73 Unlike in direct therapy, the family is the focus of the therapist’s attention, and the parent/family member is the one interacting with the child. Sharing with a family in this way requires a range of skills, including an understanding of development, a well-grounded expertise in how to implement an intervention that has proved effective,73 and an ability to communicate in an egalitarian way, which the family can choose to follow or not.93
Many authors advocate expanding the definition of family education to one in which a collaborative exchange of information occurs among parents, professionals, and people in the community. The therapist wants to empower the family, not engender dependence on a professional’s expertise.7,33,96 If family education focuses on helping the parent minimize the child’s disability and optimize developmental gains, the focus is too narrow. Furthermore, if teaching is always a one-way process, it does not necessarily strengthen the family by recognizing the expertise of its members. Involving parents who are knowledgeable about community organizations and activities designed for children with special needs as educators in collaborative teams promotes their expertise. Parents can contribute information, resources, and strategies for caregiving for a child with special needs well beyond the professional’s knowledge.14,160
Establishing a Partnership
The first interactions of the therapist with a family open the door to the establishment of a partnership. In a family-centered approach, the therapist demonstrates a family orientation that establishes trust and builds rapport through the use of open communication, mutual respect, shared decision making, and parental empowerment.14 The therapist’s initial interview reflects an interest not only in the child’s behaviors but also in the family’s concerns with managing those behaviors. These first interactions demonstrate that an equal partnership is desired and encourage a give and take of information. At the same time, parents begin to understand that professionals are there to help them and provide information and resources that support the child’s development.7,51,159
Trust building is not easily defined, and it is associated with nonverbal language, words, and mutual respect. Thinking the best of families is important to the development of this partnership. This may not always be easy, particularly when the family’s lifestyle contradicts that of the professional. Being positive and maintaining a nonjudgmental position with a family can be challenging, but it is essential to establish and build a trusting relationship. Parent participants in focus groups defined respect as simple courtesies from professionals, such as being on time to meetings.15 The professionals who were interviewed linked respect to being nonjudgmental and accepting of families. When professionals are disrespectful to families, parents may become reluctant to access services or may lose their sense of empowerment. Demonstrating respect for families becomes particularly important when they are of different racial, ethnic, cultural, and socioeconomic status. Families from different cultures often have different perspectives on child rearing, health care, and disabilities. Table 5-1 lists cultural characteristics, examples, and the possible consequences for intervention programs.
TABLE 5-1
Cultural Considerations in Intervention Services
| Cultural Considerations | Examples | May Determine |
| Meaning of the disability | Disability in a family may be viewed as shameful and disgraceful or as a positive contribution to the family. | Level of acceptance of the disability and the need for services |
| Attitudes about professionals | Professionals may be viewed as persons of authority or as equals. | Level of family members’ participation; may be only minimal if the partnership is based only on respect or fear |
| Attitudes about children | Children may be highly valued. | Willingness of the family to make many sacrifices on behalf of the child |
| Attitudes about seeking and receiving help | Problems in the family may be viewed as strictly a family affair or may be shared easily with others. | Level of denial; may work against acknowledging and talking about the problem |
| Family roles | Roles may be gender-specific and traditional or flexible. Age and gender hierarchies of authority may exist. | Family preference; may exist for the family member who takes the leadership role in the family–professional partnership |
| Family interactions | Boundaries between family subsystems may be strong and inflexible or relaxed and fluid. | Level of problem sharing/solving in families; family members may keep to themselves and deal with problems in isolation or may problem solve as a unit |
| Time orientation | Family may be present or future-oriented. | Family’s willingness to consider future goals and future planning |
| Role of the extended family | Extended family members may be close or distant, physically and emotionally. | Who is involved in the family–professional partnership |
| Support networks | Family may rely solely on nuclear family members, on extended family members, or on unrelated persons. Importance of godparents. | Who can be called on in time of need |
| Attitude toward achievement | Family may have a relaxed attitude or high expectations for achievement. | Goals and expectations of the family for the member with the disability |
| Religion | Religion and the religious community may be strong or neutral factors in some aspects of family life. | Family’s values, beliefs, and traditions as sources of comfort |
| Language | Family may be non–English-speaking, bilingual, or English-speaking. | Need for translators |
| Number of generations removed from country of origin | Family may have just emigrated or may be several generations removed from the country of origin. | Strength and importance of cultural ties |
| Reasons for leaving country of origin | Family may be immigrants from countries at war. | Family’s readiness for involvement with external world |
From Turnbull, A. P., & Turnbull, H. R. (1990). Families, professions and exceptionality: A special partnership (pp. 156-157). Columbus, OH: Merrill.
Qualitative studies have revealed snapshots of actual family experiences with service providers. Blue-Banning and colleagues found families emphasized that partnerships were built on equality and reciprocity.15 A sense of equality was created when professionals acknowledged the validity of the parents’ point of view, and partnerships flourished when there were opportunities for each member to contribute. In contrast, Lea examined the perspectives of teenage mothers and their children’s providers of early intervention services and found the perception of a lack of partnering on the part of the providers.92 These mothers felt that their providers did not know or respect them, and that their concerns were ignored. This in turn led them to have little trust in the providers. Professionals must reflect on their practices and determine whether they are truly valuing the families they are working with and whether their expectations for intervention are aligned with the family’s values and goals.96
Providing Helpful Information
Parents of children with disabilities report that information is a primary need from service providers.47,65,89,153 The information that therapists provide to families about the intervention system prepares the families to work with existing systems, to use resources available, and to understand their rights as consumers. This information also enables the family members to become informed decision makers and to choose their level of participation in the intervention program.
Child-related information that may be of benefit to parents includes information about the child’s development, the disability, the child’s health, and assessment results. To provide up-to-date information, therapists must continually engage in reading and other professional development activities. Naturally, families want the most accurate and complete information, which places a responsibility on professionals to obtain current information and continually update their skills. The families in one qualitative study “admired providers who were willing to learn and keep up to date with the technology of their field…[A] competent professional is someone who is not afraid to admit when he or she does not know something, but is willing to find out” (p. 178).15
Although parents express that they want information about their child and about the diagnosis, it must be given in a supportive manner. Service providers who focused on the negative aspects of the child’s condition or compared the child to typically developing peers were viewed as not supportive.130 Once a deficit has been identified and the child qualifies for services, hearing the child’s developing abilities expressed as delays or deficits can be hurtful for the parents. Describing what the child has accomplished using a criterion-referenced instrument, such as using the Pediatric Evaluation of Disability Inventory,50 helps parents remain positive and encouraged. Using an occupation-centered approach, the therapist asks what self-care activities the child is attempting or what play skills are emerging. Articulating a therapeutic goal linked to an emerging skill that the parents have identified reduces professional jargon and helps parents understand how the intervention plan relates to their child. Typically, parents hope to receive recommendations for activities that help the child play, for toys that match the child’s abilities, and for strategies that lead to independence in self-care. They also look to the therapist for help in managing motor impairments or differences in sensory processing that limit occupational performance.
Providing Flexible, Accessible, and Responsive Services
Because each family is different and has individualized needs, services must be flexible and adaptable. The occupational therapist should continually adapt the intervention activities as the family’s interests and priorities change. Families value the commitment of professionals to their work and feel that it is important that professionals view them as “more than a case.”15,52,103 Parents expressed appreciation when professionals exhibited “above and beyond” commitment by meeting with them outside the workday, remembering their child’s birthday, or bringing them materials to use.
Although therapists are often flexible and responsive to the child’s immediate needs and the parent’s concerns, the range of possible services is sometimes limited by the structure of the system. When a parent desires additional services, a change in location (e.g., home-based vs. center-based care), or services to be provided at a different time, the therapist may or may not be able to accommodate the request because of the therapist’s schedule. Often the agency or school system enforces policies regarding the therapist’s caseloads and scope of services. Practitioners are caught in the middle, between the system’s structure and individualized family needs. A ready solution does not always exist for the therapist who is constrained by time limitations, the demands of a large caseload, or institutional policies.
Much of the time, the therapist recognizes that he or she cannot change the structure of the system and must work as efficiently as possible within it. At the same time, the therapist should inform the family of the program’s rules and policies so that family members are aware of the constraints of the system. The occupational therapist can also take the initiative to work toward changing the system to allow more flexibility in meeting family needs. There is currently a discussion being carried out among stakeholders regarding what supports and services family-centered practice should encompass, as opposed to the usual focus of how it is carried out.162 It is necessary for occupational therapists to have a voice in this discussion because it is aimed at policy issues.
Some suggestions for therapists from parents on providing flexible and responsive services include the following164:
1. Listen with empathy to understand family concerns and needs.
2. Verbally acknowledge family priorities.
3. Make adaptations to services based on parent input.
4. Explain the constraints of the system when the parents’ requests cannot be met.
5. Suggest alternative resources to parents when their requests cannot be met within the system.
6. Discuss parents’ suggestions and requests with administrators to increase the possibilities that policies and agency structure can change to benefit families.
Respecting Family Roles in Decision Making
Parents who share in decision making regarding intervention for their child are more satisfied with services.109 Although professionals tend to acknowledge readily the role of the parents as decision makers, they do not always give parents choices or explain options in ways that enable parents to make good decisions. Too often, plans that should be family-centered are written in professional jargon and do not always address family concerns.16 Parents are involved in decision making about their child in the following ways:
1. Parents can defer to the therapist in decision making. Deferring to the therapist may reflect confidence in the therapist’s judgment and may be an easy way for parents to make a decision about an issue that they do not completely understand.
2. Parents have veto power. It is important that parents know that they have the power to veto any decision made or goal chosen by the team. Awareness of the legitimacy of this role gives parents assurance that they have an important voice on the team and can make changes, should they desire them. This role appears to be quite satisfying to parents.100
3. Parents share in decision making. As described in the previous section, when parent–professional partnerships have been established, the parents fully participate in team discussions that lead to decisions about the intervention plan. Service options and alternatives are made clear, and parents have the information needed to make final decisions. Requests of parents are honored (within the limitations of the program).
Families cannot always be given a wide range of choices about who will provide services and when and where these services will be provided. However, their role in decision making should still be emphasized; otherwise, family-centered practice is not occurring.13,93,96 Families who are empowered to make decisions early in the intervention process will be better prepared for that role throughout the course of the child’s development. In most cases, assessment of choices and good decision making are skills that parents promote in their children as they approach adulthood.
COMMUNICATION STRATEGIES
Effective communication is built on trust and respect; it requires honesty and sensitivity to what the parent needs to know at the moment. Therapists have tremendous amounts of information to impart to parents. Effective helping is most likely to occur when the information given is requested or sought by the parent.
Occupational therapists communicate with parents using a variety of methods: formal and informal, written, verbal, and nonverbal. Table 5-2 describes communication strategies consistent with the principles described earlier. The strategies are based primarily on feedback from parents regarding what they have found to be effective help from occupational therapists.24,52,60
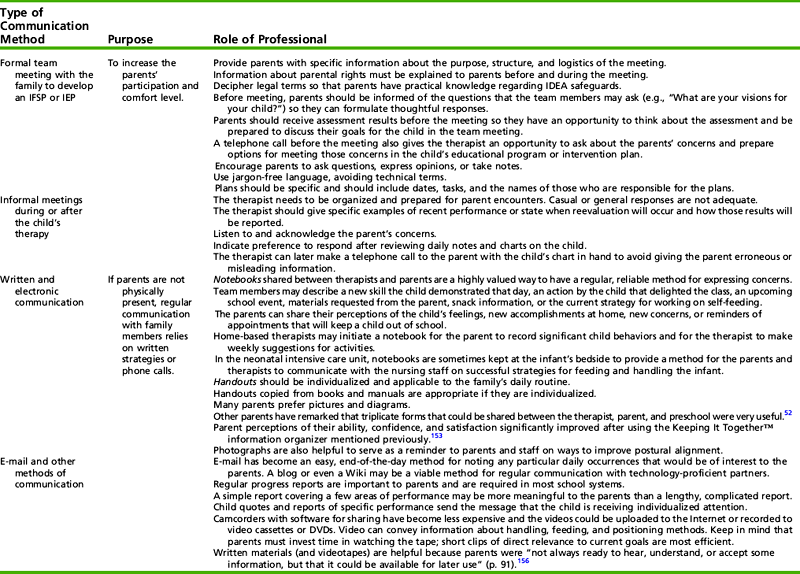
HOME PROGRAMS: BLENDING THERAPY INTO ROUTINES
Throughout this text, recommendations are given for ways to integrate therapeutic strategies into the daily occupations of children, with the clear recognition that learning occurs best in the child’s natural environment. Skills demonstrated in therapy translate into meaningful functional change only when the child can generalize the skill to other settings and demonstrate the skill in his or her daily routine. Therapists often recommend home activities for parents to implement with their child, so that he or she can apply new skills at home.
Before making recommendations, the therapist should ask the parents about daily routines and the typical flow of family activities during the week. Understanding which routines and traditions hold special meaning for the family will help therapists focus. The therapist and the parents discuss family occupations during the day and identify naturally occurring opportunities to teach the child new skills by understanding what needs to occur and deciding when it will work for them. The result of this close examination of the typical week enables the therapist and the parents to embed goals and activities in interactive routines, in which the therapeutic process does not diminish the value and pleasure.
The ways mothers use home programs and the characteristics of home programs that parents value and implement have been studied fairly extensively.24,59,144,157 Hinojosa completed a qualitative study in which eight mothers of preschool children with cerebral palsy (CP) were interviewed.59 Most of the mothers did not carry out the suggested home programs. Mothers reported that they did not have the time, energy, or confidence to follow the programs effectively. Hinojosa suggested that it is inappropriate to expect mothers to follow a strict home program. Instead, therapists should help mothers find and learn adaptive ways to meet their children’s needs with minimal disruption to their lives. Case-Smith and Nastro replicated Hinojosa’s study using a sample of mothers from Ohio who had young children with CP.24 Each had accessed private and publicly funded therapies. Initially, when their children were infants, these mothers had participated extensively in home programs. They indicated that these efforts were self-motivated and did not feel that the specific home programs were “an imposed expectation” on the part of the therapists. As the children reached preschool age, the mothers no longer implemented home programs with their children. Reasons for discontinuing home programs included lack of time and increased resistance on the part of their children. Segal and Beyer examined the use of a specific therapeutic intervention, the Wilbarger Brushing protocol.145 They found that the factors with the most influence on adherence to the program were the child’s response to the intervention, the parent’s perception of its benefit, and whether the parent could fit it into daily routines. Tetreault and colleagues found similar results in their study of home activity programs, with the addition of family size as a factor; finding more children in the home tended to led to less adherence, possibly due to the burden on the mother.157 Lyon expressed a mother’s perspective on implementing therapy at home:
I’ve come to terms with being “only human.” If I could ensure that Zak could go through the day always moving in appropriate ways, flexing when he should flex, straightening when he should straighten, and play and learn and experience and appreciate … I would; but, that is not possible. I do have a responsibility to help Zachary develop his motor skills, but I also have a responsibility to help him learn about life. So on those days when we have so much fun together or are so busy that bedtime comes before therapy time, I finally feel comfortable that I have given him something just as vital to his development, a real “mom” (p. 4).95
Although some mothers tend not to implement specific prescribed strategies, they report appreciating the therapists’ suggestions and ideas about home activities that promote child development or make caregiving easier. Case-Smith and Nastro found that the mothers in their sample frequently used the handouts with specific activities and recommendations long after they had been given to them.24
Positive relationships with families seem to develop when open and honest communication is established, and when parents are encouraged to participate in their child’s program to the extent that they desire. When asked to give advice to therapists, parents stated that they appreciated (1) specific, objective information; (2) flexibility in service delivery; (3) sensitivity and responsiveness to their concerns106; (4) positive, optimistic attitudes24; and (5) technical expertise and skills.15 One mother expressed that hope and optimism are always best. “Given a choice, I would want my therapist to be an optimist and perhaps to strive for goals that might be a bit too optimistic, keeping in mind that we might not come to that” (p. 64).116 McWilliam et al. describe this positive attitude as “a belief in parents’ abilities, a nonjudgmental mind-set and optimistic view of children’s development, and an enthusiasm for working with families” (p. 213).106
WORKING WITH FAMILIES FACING MULTIPLE CHALLENGES
Features that contribute to diversity in families are characteristics that occupational therapists welcome and accommodate in providing individualized services. For example, parents dealing with their own chronic physical illnesses may require help dealing with energy or emotional support as they experience social stigma associated with an illness such as HIV/AIDS (see Research Note 5-2 for a study of parents with physical disabilities).121 The principles presented in this text remain critically important, but they may be more difficult for therapists to implement when they are working with families facing multiple challenges. Challenges to a family’s ability to fulfill its functions (e.g., living in poverty, acute onset of a disability in the parent) increase the vulnerability of children with special needs and add unique challenges to family functions. By identifying protective factors that bolster the child’s resilience, the therapist can approach issues from a positive perspective to support strengths, capitalize on family assets, and work to make maximum use of community resources.
RESEARCH NOTE 5-2
The purpose of this study was to explore the meaning of motherhood and the mothering-related experiences of mothers with physical disabilities.
A qualitative study using two focus groups (of mothers with children under eight years old and mothers of older children) plus individualized interviews of eight of the participating mothers were conducted. Most of the mothers were wheelchair users and were well educated.
The categories that emerged were their attempts to ensure the physical and psychological well-being of their children, their child-rearing philosophies and practices that addressed the challenge of setting boundaries and managing their children’s behavior when there was a huge reliance on verbal explanations and instructions, and the overall nature of the parent-child relationship.
Mothers with disabilities who have access to formal and informal supports (assistance with hiring personal attendants) are better equipped to set boundaries, follow through, and promote cooperative behavior. Consistent parenting practices pave the way for children to be respectful of and feel supported by the parent.
This article provides another example of working with families comprising parents with special needs. The examples in this study reinforce the need of all parents (and providers) to be consistent in their expectations and communications with their children. Occupational therapists must be aware of community and state resources for their families with special needs.
Prilleltensky, O. (2005) My child is not my carer: Mothers with physical disabilities and the well-being of children. Disability & Society, 19, 209–223.
The occupational therapist grounded in family systems perspective and committed to empowering families will work effectively with a whole-family system in a family-centered manner, regardless of the type of disability of one or more family members. Understanding and valuing how the family system orchestrates members’ occupations to fulfill family function allows the occupational therapist to take a holistic view of the family’s needs and priorities. Although parents advocate a positive view, it is important to recognize when an unusual parental behavior reflects family dysfunction (e.g., child abuse, child neglect). Issues in child abuse and child neglect are discussed in Chapter 13. When family dysfunction is pervasive, most occupational therapists need input from colleagues with expertise in counseling and family systems. Services for the child with special needs continue, but the therapist considers ecologic and family systems factors in collaborating with the team to set priorities and provide services.
Families in Chronic Poverty
Beyond the diversity issues discussed under “Socioeconomic Status,” chronic poverty has a pervasive effect on family and child experiences. A majority of families receiving public assistance are children and mothers with poor educational backgrounds, an inconsistent work history, and low-wage jobs. Welfare recipients are often stereotyped as lazy and unmotivated, and as having children “just to make money off the system.”92,141 In current economic circumstances, poverty has any number of causes. The process of “qualifying” for services can be frustrating, depersonalizing, and degrading. Once a family qualifies for help, resources are not always enough to make ends meet. In interviews with hundreds of single mothers living on welfare or working in low-paying jobs, Edin and Lein found that both groups had to engage in a variety of survival strategies to access enough resources to meet their families’ needs.35 Both groups reported sharing apartments and working on the side or having a second job. In addition, both groups relied on financial assistance from their social network, such as the child’s father or family and friends.
Seccombe and colleagues conducted an ethnographic study of women receiving welfare and asked about their reasons for needing assistance.141 Although the participants realized that the U.S. culture tends to emphasize individual responsibility for rising above poverty, many of the women believed that bad luck was a primary reason their families needed assistance. Single parents are particularly vulnerable35,105; without family members to help, these mothers lack control over the events in their lives. Unexpected events, such as a car breaking down or special meetings at school about a child, can cause the parent to miss hours at a job and can increase financial strain. Some women have reported that they returned to welfare and Medicaid “for the child.”141 Poverty represents a multidimensional issue, and therapists cannot make assumptions about the reasons a family lives in poverty.
Recognizing that poverty creates a unique cultural worldview enables therapists to consider what it means to provide family-centered services.66,92 For example, a different world view of time, with the emphasis on the here and now, makes it harder to schedule or keep appointments. Families of low SES are rarely able to follow through with their plans. Therefore, planning for the future has little meaning, and participating in the setting of annual goals at IFSP or IEP meetings may not be considered important.
Further increasing the vulnerability of children with special needs who live in poverty are the multiple challenges that put their parents at greater risk for poor parenting. In one study, almost half (45%) of the mothers struggled with depression, and fewer than half of them reported that they had a family member who could help babysit.138 Even with incentives such as diapers, toys, and food, low-income mothers got their children to an early intervention program only 40% to 50% of the time, compared with 75% of the time for middle-income mothers.19 Therapists who are aware that poverty creates special conditions strive to individualize intervention plans and consider how formal support can replicate the positive effects of social support to promote better parenting.19,34
It is necessary to look beyond simple associations between poverty and parenting, because some parents do better than others despite a low SES.114 Occupational therapists need to understand how some parents living in poverty adapt and raise children successfully (Case Study 5-1). For example, single parents who have strict disciplinary standards may seem harsh. However, their parenting practices may be grounded in an anticipation that their children will grow into a world where obedience to people in authority is important for keeping a job. Other parents who restrict their children’s community activities may be effective in monitoring who they are with, minimizing the negative influences of poor neighborhoods. When a therapist is sensitive to and deeply understands a family with a low SES, she or he can make recommendations that help the child with special needs while supporting the family in their precarious position.
 CASE STUDY 5-1 Family with Multiple Challenges
CASE STUDY 5-1 Family with Multiple Challenges
Jason and his mother, Ms. Thorp, lived in a government-subsidized, one-bedroom apartment, and they received food stamps and welfare assistance. Because it was a dangerous neighborhood, Ms. Thorp tried to keep Jason inside as much as possible. At his 4-year-old annual physical, the physician noticed that Jason was not completely toilet trained and that he had limited expressive vocabulary. His mother stated that he did not use a spoon. An interdisciplinary assessment at the Developmental Evaluation Center revealed a short attention span, a below-average self-care standard score on the Pediatric Evaluation of Disabilities Inventory, and 20% delay in expressive language. The occupational therapist also noted that Jason demonstrated poor fine motor skills (i.e., he did not complete puzzles, color with a crayon, or cut along a line). Because Jason had not been exposed to a varied learning environment, the team recommended that he enroll in a childcare program with children his own age. They also recommended that the speech–language pathologist and the occupational therapist consult with his teacher.
In developing an IEP, his mother, with input from the social worker, had selected a childcare program near her home, so she could walk Jason to school. The teachers welcomed him and thought that they could work on toilet training, but they insisted that Jason needed to be able to feed himself lunch before he entered the program.
The therapist discussed Jason’s use of a spoon with Ms. Thorp, but she did not instruct her to force Jason to use utensils. The therapist recalled hearing that children living in poverty were less likely to have meals in a particular location or at regular times, and she realized that strategies at different levels would be needed to achieve spoon-feeding.
The therapist decided that she could be supportive and effective in changing mealtime routines by providing services in the home. At the beginning of the home visit, the therapist realized that the family had no kitchen table. In talking about their daily schedule, Ms. Thorp reported that they did not awaken at any specific time. However, Jason was usually up by 11:30 am to watch his favorite television show. She reported that watching television together was an activity she enjoyed with her son.
Ms. Thorp gave Jason a cheese sandwich sometime in the late morning. She selected cheese sandwiches because the nutritionist said they were good, and Jason did not make a mess when he walked around with them. Ms. Thorp reported that she was not a “morning person,” so she frequently did not have breakfast or lunch. Instead, she snacked during the day. For dinner, she frequently made chicken or hamburgers, which she and Jason ate in the living room. The plate was placed on the coffee table, and Jason stood near it and finger fed himself. If she made something like pinto beans, Ms. Thorp fed Jason so that he would not make a mess. She explained, “When we moved in, there were bugs everywhere. I fought hard to kill them because I know they are dirty. I know if he makes a mess with food, the bugs will be right back!”
The therapist brought a cup of pudding as a treat for Jason, and she asked him to spoon it himself. They sat Jason in the corner of the sofa. When he was handed the spoon, he dipped it into the pudding, inverted the spoon as he brought it to his mouth, and sucked the pudding from the spoon. Ms. Thorp became upset when pudding dropped from his spoon onto his shirt. She took the spoon away and fed him the rest of the pudding.
The therapist wanted to understand Jason’s weekly routine. She learned that Jason spent every Tuesday night with his father, who would take him out for an ice cream cone. His maternal grandmother occasionally watched Jason on weekends when Ms. Thorp supplemented their income by filling in as a cook’s assistant in a coffee shop. The therapist interpreted the family’s strengths as the following:
1. Ms. Thorp is a devoted mother who wants her son to be healthy and wants a clean apartment.
2. Ms. Thorp listens to and follows the advice of the nutritionist.
3. The Thorps share an interactive routine around a television show in the morning, which helps create temporal organization.
4. Jason’s family includes extended family who see him regularly.
Her concerns about Jason’s learning to spoon feed include the following:
1. Jason does not have a place for meals, and he rarely sees anyone using a spoon.
2. Meals are typically foods that can be eaten with the fingers.
3. Jason does not use tools well, and Ms. Thorp does not want him to be messy.
4. Ms. Thorp is easily overwhelmed by details, and she does not seem to solve problems easily.
The next time she visited, the therapist brought a stool from the therapy equipment library. They adjusted the height so that it could be pulled up to the coffee table, creating a place for Jason to sit and eat. She also purchased two place mats with his favorite cartoon hero on them. The therapist brought a container of macaroni and cheese for Jason to eat. Jason loved his “chair” and table. When given the spoon to eat macaroni from a bowl, he scooped but inverted the spoon on the way to his mouth. He looked surprised and then finger fed himself the noodles. Together the therapist and Ms. Thorp planned that Jason would have “noodles” as lunch, and they agreed that lunch would occur immediately before Jason’s favorite TV show.
On her third home visit, the therapist arranged to come in the evening when Jason’s father came to take him for ice cream. When she arrived, Ms. Thorp returned the stool because her mother had a stool Jason could use. The therapist explained to Jason’s father that his son needed more practice using a spoon. He agreed to get cups of ice cream instead of ice cream cones and to eat with Jason.
Within 4 weeks of the therapist’s third visit, Ms. Thorp reported that Jason was successfully using a spoon. The team arranged for Jason to begin preschool the next week.
Parents with Special Needs
Parents themselves may have special needs that require an emphasis on supportive services. Parents who face physical or sensory challenges may need help in solving problems, such as monitoring the activity of an active child or being alerted to the cry of an infant.107 Occupational therapists, who work from the perspective that parenting reflects a process of co-occupation, can assist the parent in the modification of tasks. For example, adapting the location of routines, such as diaper changing and infant bathing, can enable parents with physical limitations to participate in caregiving and simple routines that build affection between the parent and child. Therapists can explore the use of adaptive equipment, such as motion detectors or sound-activated alarm systems, to compensate for the parents’ sensory deficits and ensure responsiveness to their child’s cues. Most parents who have had long-term experiences with a physical limitation independently develop creative solutions for providing care for their children, and they only occasionally seek a therapist’s assistance in determining how to perform specific caregiving tasks.
Parents who struggle with drug addiction or mental health conditions may worry whether they are up to caregiving responsibilities.104 They often require counseling, mental health services, and opportunities to participate in support groups.119 When parents have special needs that strongly influence their caregiving ability, their needs often become the first emphasis of intervention.
Parents with intellectual disabilities, mental health issues, or drug addiction are at risk for having children with developmental disabilities. Professionals have questioned the competency of parents with intellectual delays, and courts have removed their children in disproportionate numbers.17 However, with support systems in place, these parents can be surprisingly successful. Parents at risk because of intellectual or mental health impairments appear to be most successful in caring for young children when they are married, have few children, have adequate financial support, and have multiple sources of support.167
In providing support to parents with intellectual disabilities, Espe-Sherwindt and Kerlin recommended that professionals focus on the parents’ internal and external control, self-esteem, social skills, and problem-solving skills.36 Therapists can help empower parents to make their own decisions, thereby increasing their sense of self-control. Often individuals with intellectual delay or drug addiction have low self-esteem and lack confidence in their ability to make decisions. Because self-esteem is important in interactions with children, this aspect of interaction should be considered.
Professionals should also focus on helping parents with intellectual or mental health impairments build problem-solving skills. Everyday care for children requires constant problem solving. Many times professionals give advice or recommendations without encouraging the parents to solve the problem independently or to try their own actions first. When others direct parents, they become more dependent. However, when parents successfully solve a problem, they become empowered to act independently in daily decision making. Problem solving can be taught and modeled. Espe-Sherwindt and Kerlin suggested that teaching problem-solving skills in daily caregiving could be critical to parents’ development of caregiving competence.36
When occupational therapists work with parents with intellectual or mental health impairments, it becomes essential to know the parents’ learning styles and abilities. Many times instructions need to be repeated and reinforced. Therapists must use good judgment in what techniques are taught to these parents, with emphasis on safe and simple methods. The occupational therapist should also recognize the need for additional support to help parents with intellectual delays access those needed services. Regular visits in the home by aides, nurses, or teaching assistants can meet the level of support needed. If the occupational therapist communicates his or her goals and strategies to the visiting aide, therapy activities are more likely to be implemented by the parents and other professionals working with the family.
Working with parents with intellectual or mental health impairments can be frustrating when appointments are missed or requests are not followed. Therefore, an understanding of the parents’ needs is essential. The development of simple, repetitive routines and systems that the parents can learn and follow enables them to become competent caregivers. With support, they can offer a child a positive and loving environment that fosters both health and development.
Professionals use a variety of strategies to deal with challenging families. When families have continual stress and problems, it is important for therapists to begin to build trust slowly, to share observations and concerns, and to accept parents’ choices.31 When parents do not seem to understand the intervention process, professionals can attempt to establish rapport by using concrete, simple terms; by providing both graphic and oral information; and by providing ideas that would immediately help the child. Professionals also report that parents can better articulate their concerns when services are home based, when lay terminology is used, and when services are presented in a slow, nonjudgmental way.31 Focusing on the child’s strengths and developing trust and responsiveness are also important when parents are coping with their own challenges.
SUMMARY
Working with families is one of the most challenging and rewarding aspects of pediatric occupational therapy. The family’s participation in intervention is of critical importance in determining how much the child can benefit. Therapy goals and activities that reflect the family’s priorities often result in meaningful outcomes.
This chapter described families as systems with unique structures and interactive patterns. The potential effects of a child with a disability on a family’s occupations were related to implications for the occupational therapist’s role. Issues that arise during different stages of the family’s life cycle were described. In the final section, principles and strategies for working with families were discussed. The strategies included communication methods to inform and involve parents in the intervention program. It is critically important that the occupational therapist show sensitivity to and respect for the family’s values and interests, maintain a positive attitude, continually update skills, obtain current information to give parents, and offer consistent, positive support of family members.
REFERENCES
1. Allen, K.R., Fine, M.A., Demo, D.H. An overview of family diversity: Controversies, questions and values. In: Demo D.H., Allen K.R., Fine M.A., eds. Handbook of family diversity. New York: Oxford University Press; 2000:1–14.
2. Alvarado, M.I. Mucho camino: The experiences of two undocumented Mexican mothers participating in their child’s early intervention program. American Journal of Occupational Therapy. 2004;58:521–530.
3. Amato, P.R. Diversity within single-parent families. In: Demo D.H., Allen K.R., Fine M.A., eds. Handbook of family diversity. New York: Oxford University Press; 2000:149–172.
4. Anderson, C. The diversity, strengths and challenges of single-parent households. In: Walsh F., ed. Normal family processes: Growing diversity and complexity. 3rd ed. New York: Guilford Press; 2003:121–152.
5. Anderson, D. He’s not “cute” anymore. In: Dougan T., Isbell L., Vyas P., eds. We have been there. Nashville, TN: Abington Press; 1983:90–91.
6. Aran, A., Shalev, R.S., Biran, G., Gross-Tsur, V. Parenting style impacts on quality of life in children with cerebral palsy. Journal of Pediatrics. 2007;151:56–60.
7. Bailey, D.B., Bruder, M.B., Hebbeler, K., Carta, J., Defosset, M., Greenwood, C., et al. Recommended outcomes for families of young children with disabilities. Journal of Early Intervention. 2006;28:227–251.
8. Baird, A., John, R., Hayslip, B. Custodial grandparenting among African Americans: A focus group perspective. In: Hayslip B., Glen R.G., eds. Grandparents raising grandchildren: Theoretical, empirical, and clinical perspectives. New York: Springer Publishing; 2000:125–144.
9. Barakat, L.P., Patterson, C.A., Tarazi, R.A., Ely, E. Disease-related parenting stress in two sickle cell disease caregiver samples: Preschool and adolescent. Families, Systems, & Health. 2007;25:147–161.
10. Barnett, S., Boyce, G.C. Effects of children with Down syndrome on parents’ activities. American Journal of Mental Retardation. 1995;100(2):115–127.
11. Bedell, G.M., Cohn, E.S., Dumas, H.M. Exploring parents’ use of strategies to promote social participation of school-age children with acquired brain injuries. American Journal of Occupational Therapy. 2005;59:273–284.
12. Bernheimer, L.P., Keogh, B.K. Weaving interventions into the fabric of everyday life: An approach to family assessment. Topics in Early Childhood Special Education. 1995;15:415–433.
13. Bernheimer, L.P., Weisner, T.S. Let me just tell you what I do all day…”: The family story at the center of intervention research and practice. Infants & Young Children. 2007;20(3):192–201.
14. Betz, C.L. Parent-professional partnerships: Bridging the disparate worlds of children, families, and professionals [Editorial]. Journal of Pediatric Nursing: Nursing Care of Children & Families. 2006;21(5):333–335.
15. Blue-Banning, M., Summers, J.A., Frankland, H.C., Nelson, L.L., Beegle, G. Dimensions of family and professional partnerships: Constructive guidelines for collaboration. Exceptional Children. 2004;70(2):167–184.
16. Boone, H.A., McBride, S.L., Swann, D., Moore, S., Drew, B.S. IFSP practices in two states: Implications for practice. Infants and Young Children. 1998;10(4):36–45.
17. Booth, T., Booth, W. Brief research report: Findings from a court study of care proceedings involving parents with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities. 2004;1:179–181.
18. Bradley, R.H., Corwyn, R.F., McAdoo, H.P., Coll, C.G. The home environments of children in the United States: Part 1. Variations by age, ethnicity, and poverty status. Child Development. 2001;72:1844–1867.
19. Brinker, R.P. Family involvement in early intervention: Accepting the unchangeable, changing the changeable, and knowing the difference. Topics in Early Childhood Special Education. 1992;12(3):307–332.
20. Britner, P.A., Morog, M.C., Pianta, R.C., Marvin, R.S. Stress and coping: A comparison of self-report measures of functioning in families of young children with cerebral palsy or no medical diagnosis. Journal of Child and Family Studies. 2003;12:335–348.
21. Bronfenbrenner, U. Discovering what families do. In: Blankenhorn D., Bayme S., Elshtain J.B., eds. Rebuilding the nest. Milwaukee: Family Service America; 1990:27–38.
22. Carlson, Harwood. Attachment, culture, and the caregiving system: The cultural patterning of everyday experiences among Anglo and Puerto Rican mother-infant pairs. Infant Mental Health Journal. 2003;24:53–73.
23. Case-Smith, J. Parenting a child with a chronic medical condition. American Journal of Occupational Therapy. 2004;58:551–560.
24. Case-Smith, J., Nastro, M. The effect of occupational therapy intervention on mothers of children with cerebral palsy. American Journal of Occupational Therapy. 1993;46:811–817.
25. Case-Smith, J., Sainato, D., McQuaid, J., Deubler, D., Gottesman, M., Taber, M. IMPACTS project: Preparing therapists to provide best practice early intervention services. Physical & Occupational Therapy in Pediatrics. 2007;27(3):73–90.
26. Christian, L.G., Understanding families: Applying family systems theory to early childhood practice. Journal of the National Association for the Education of Young Children (electronic), 2006.. Retrieved April 28, 2008, from, http://journal.naeyc.org/btj/200601/ChristianBTJ.asp..
27. Coll, C.G., Pachter, L.M., Ethnic and minority parenting. Bornstein, M.H., eds. Handbook of parenting, 2nd ed., Vol. 4. Mahwah, NJ: Lawrence Erlbaum, 2002;1–20.
28. Connard, C., Novick, R. The ecology of the family: A background paper for a family-centered approach to education and social service delivery. Retrieved January 28, 2008, from http://www.nwrel.org/cfc/publications/ecology2.html, 1996.
29. Crowe, T.K. Time use of mothers with young children: The impact of a child’s disability. Developmental Medicine and Child Neurology. 1993;35:612–630.
30. Crowe, T.K., Florez, S.I. Time use of mothers with school-age children: A continuing impact of a child’s disability. American Journal of Occupational Therapy. 2006;60:194–203.
31. DeGangi, G.A., Wietlesbach, S., Poisson, S., Stein, E., Royeen, C. The impact of culture and socioeconomic status on family-professional collaboration: Challenges and solutions. Topics in Early Childhood Special Education. 1994;14(4):503–520.
32. DeGrace, B.W. The everyday occupation of families with children with autism. American Journal of Occupational Therapy. 2004;58:543–550.
33. Dolev, R., Zeedyk, M.S. How to be a good parent in bad times: Constructing parenting advice about terrorism. Child: Care, Health & Development. 2006;32(4):467–476.
34. Dunst, C.J., Trivette, C.M., Jodry, W. Influences of social support on children with disabilities and their families. In: Guralnick M.J., ed. The effectiveness of early intervention. Baltimore: Brookes; 1997:499–522.
35. Edin, K., Lein, L. Work, welfare, and single mothers’ economic survival strategies. American Sociological Review. 1996;61:253–266.
36. Espe-Sherwindt, M., Kerlin, S.L. Early intervention with parents with mental retardation: Do we empower or impair. Infants and Young Children. 1990;2(4):21–28.
37. Falicov, C.J. Immigrant family processes. In: Walsh F., ed. Normal family processes: Growing diversity and complexity. 3rd ed. New York: Guilford Press; 2003:280–300.
38. Fiese, B.H., Tomcho, T.J. Finding meaning in religious practices: The relation between religious holiday ritual and marital satisfaction. Journal of Family Psychology. 2001;15:597–609.
39. Fine, M.A., Demo, D.H., Allen, K.R. Family diversity in the 21st century: Implications for research, theory and practice. In: Demo D.H., Allen K.R., Fine M.A., eds. Handbook of family diversity. New York: Oxford University Press; 2000:440–448.
40. Fox, L., Vaughn, B.J., Wyatte, M.I., Dunlap, G. We can’t expect other people to understand”: Family perspectives on problem behaviors. Exceptional Children. 2002;68:437–450.
41. Gallagher, P.A., Fialka, J., Rhodes, C., Arceneaux, C. Working with families: Rethinking denial. Young Exceptional Children. 2001;5(2):11–17.
42. Gallagher, P.A., Rhodes, C.A., Darling, S.M. Parents as professionals in early intervention: A parent educator model. Topics in Early Childhood Special Education. 2004;24(1):5–13.
43. Gallimore, R., Lopez, E.M. Everyday routines, human agency and ecocultural context: Construction and maintenance of individual habits. Occupational Therapy Journal of Research. 2002;22:70–77.
44. Gavidia-Payne, S., Stoneman, Z. Family predictors of maternal and paternal involvement in programs for young children with disabilities. Child Development. 1997;68:701–717.
45. Gordon, P.A., Tschopp, M.K., Feldman, D. Addressing issues of sexuality with adolescents with disabilities. Child and Adolescent Social Work Journal. 2004;21(5):513–527.
46. Grant, G., Ramcharan, P., Goward, P. Resilience, family care and people with intellectual disabilities. International Review of Research in Mental Retardation. 2003;26:135–173.
47. Grant, G., Whittell, B. Differentiated coping strategies in families with children or adults with intellectual disabilities: The relevance of gender, family composition and the life span. Journal of Applied Research in Intellectual Disabilities. 2000;13:256–275.
48. Greene, M. A parent’s perspective. Topics in Early Childhood Special Education. 1999;19:147.
49. Greene, S.M., Anderson, E.R., Hetherington, E.M., Forgatch, M.S., DeGarmo, D.S. Risk and resilience after divorce. In: Walsh F., ed. Normal family processes: Growing diversity and complexity. 3rd ed. New York: Guilford Press; 2003:96–120.
50. Haley, S.M., Coster, W.J., Ludlow, L.H., Haltiwanger, J.T., Andrellos, P.J. Pediatric Evaluation of Disability Inventory. San Antonio: Psychological Corporation, 1992.
51. Hanft, B.E., Rush, D.D., Shelden, M.L. Coaching families and colleagues in early intervention. Baltimore: Paul H. Brookes, 2004.
52. Harrison, C., Romer, T., Simon, M.C., Schulze, C. Factors influencing mothers’ learning from paediatric therapists: A qualitative study. Physical & Occupational Therapy in Pediatrics. 2007;27:77–96.
53. Harwood, R.L., Leyendecker, B., Carlson, J., Asencio, M., Miller, A.M. Parenting among Latino families in the U.S. In Bornstein M.H., ed.: Handbook of parenting: Social conditions and applied parenting, 2nd ed., Mahwah, NJ: Lawrence Erlbaum Associates, 2002.
54. Hasselkus, B.R. The meaning of everyday occupation. Thorofare, NJ: Slack, 2002.
55. Hastings, R.P. Child behavior problems and partner mental health as correlates of stress in mothers and fathers of children with autism. Journal of Intellectual Disability Research. 2003;47:231–237.
56. Hayslip, B., Emick, M.A., Henderson, C.E., Elias, K. Temporal variations in the experience of custodial grand parenting: A short-term longitudinal study. Journal of Applied Gerontology. 2002;21:139–156.
57. Helitzer, D.L., Cunningham-Sabo, L.D., VanLeit, B., Crowe, T.K. Perceived changes in self-image and coping strategies of mothers of children with disabilities. Occupational Therapy Journal of Research. 2002;22(1):25–33.
58. Hibbard, R.A., Desch, L.W., the Committee on Child Abuse and Neglect and Council on Children with Disabilities. Maltreatment of children with disabilities. Pediatrics. 2007;119(5):1018–1025.
59. Hinojosa, J. How mothers of preschool children with cerebral palsy perceive occupational and physical therapists and their influence on family life. Occupational Therapy Journal of Research. 1990;10(3):144–162.
60. Hinojosa, J., Sproat, C.T., Mankhetwit, S., Anderson, J. Shifts in parent-therapist partnerships: Twelve years of change. American Journal of Occupational Therapy. 2002;56:556–563.
61. Hodapp, R.M. Families of persons with Down Syndrome: New perspectives, findings, and research and service needs. Mental Retardation and Developmental Disabilities Research Reviews. 2007;13:279–287.
62. Hoff, E., Laursen, B., Tardif, T., Socioeconomic status and parenting. Bornstein, M.H., eds. Handbook of parenting, 2nd ed., Vol. 2. Mahwah, NJ: Lawrence Erlbaum Associates, 2002;231–252.
63. Holloway, R.L. Families and chronic illness: Introduction to the special section for. Families, Systems, and Health. Families, Systems, & Health. 2007;25:243–245.
64. Hombeck, G.N., Gorey-Ferguson, L., Hudson, T., Seefeldt, T., Shapera, W., Turner, T., et al. Maternal, paternal, and marital functioning in families of preadolescents with spina bifida. Journal of Pediatric Psychology. 1997;22:167–181.
65. Hummelinck, A., Pollock, K. Parents’ information needs about the treatment of their chronically ill child: A qualitative study. Patient Education and Counseling. 2006;62:228–234.
66. Humphry, R. Families living in poverty: Meeting the challenge of family-centered services. American Journal of Occupational Therapy. 1995;49:687–693.
67. Humphry, R. Young children’s occupations: Explicating the dynamics of developmental processes. American Journal of Occupational Therapy. 2002;56:171–179.
68. Humphry, R., Wakeford, L. Development of everyday activities: A model for occupation-centered therapy. Infants & Young Children. 2008;21(3):230–240.
69. Individuals with Disabilities Education Act of 2004 (IDEA). (P.L. 108-446.)
70. Jinnah, H.A., Stoneman, Z. Parents’ experiences in seeking child care for school age children with disabilities—where does the system break down. Children and Youth Services Review. 2008;30(8):967–977.
71. Johnson, C.P., Kastner, T.A., the Committee/Section on Children With Disabilities. Clinical report: Helping families raise children with special health care needs at home. Pediatrics. 2005;115(2):507–511.
72. Joslin, D. Emotional well-being among grandparents raising children affected and orphaned by HIV disease. In: Hayslip B., Glen R.G., eds. Grandparents raising grandchildren: theoretical, empirical, and clinical perspectives. New York: Springer Publishing; 2000:87–105.
73. Kaiser, A.P., Hancock, T.B. Teaching parents new skills to support their young children’s development. Infants and Young Children. 2003;16:9–22.
74. Kellegrew, D. Constructing daily routines: A qualitative examination of mothers with young children with disabilities. American Journal of Occupational Therapy. 2000;54:252–259.
75. Kelley, S.J., Whitley, D., Sipe, T.A., Yorker, B.C. Psychological distress in grandmother kinship care providers: The role of resources, social support and physical health. Child Abuse and Neglect. 2000;24:311–321.
76. King, G.A., King, S.M., Rosenbaum, P.L. How mothers and fathers view professional caregiving for children with disabilities. Developmental Medicine and Child Neurology. 1996;38:397–407.
77. King, G., Law, M., Hanna, S., King, S., Hurley, P., Rosenbaum, R., et al. Predictors of the leisure and recreation participation of children with physical disabilities: A structural equation modeling analysis. Children’s Health Care. 2006;35(3):209–234.
78. King, G., Law, M., King, S., Rosenbaum, P., Kertoy, M.K., Young, N.L. A conceptual model of factors affecting the recreation and leisure participation of children with disabilities. Physical and Occupational Therapy in Pediatrics. 2003;23:63–89.
79. King, G., Tucker, M.A., Baldwin, P., Lowry, K., LaPorta, J., Martens, L., et al. A life needs model of pediatric service delivery: Services to support community participation and quality of life for children and youth with disabilities. Physical & Occupational Therapy in Pediatrics. 2002;22(2):53–77.
80. Kirk, S. Families’ experiences of caring at home for a technology-dependent child: A review of the literature. Child: Care, Health and Development. 1998;24(2):101–114.
81. Knott, F., Lewis, C., Williams, T. Sibling interaction of children with autism: Development over 12 months. Journal of Autism and Developmental Disorders. 2007;37:1987–1995.
82. Knox, M., Parmenter, T.R., Atkinson, N., Yezbeck, M. Family control: The views of families who have a child with an intellectual disability. Journal of Applied Research in Intellectual Disabilities. 2000;13:17–28.
83. Koramoa, J., Lynch, M.A., Kinnair, D. A continuum of child-rearing: Responding to traditional practices. Child Abuse Review. 2002;11:415–421.
84. Kotchick, B.A., Forehand, R. Putting parenting in perspective: A discussion of the contextual factors that shape parenting practices. Journal of Child and Family Studies. 2002;11:255–269.
85. Kroll, B. A family affair Kinship care and parental substance misuse: Some dilemmas explored. Child and Family Social Work. 2007;12:84–93.
86. Laird, J. Lesbian and gay families. In Walsh F., ed.: Normal family processes: growing diversity and complexity, 3rd ed., New York: Guilford Press, 2003.
87. Larson, R., Mothers’ time in two-parent and one-parent families: The daily organization of work, time for oneself, and parenting of adolescents. Minding the time in family experiences: emerging perspectives and issues, New York, Elsevier Science, 2001;Vol. 3:85–109.
88. Larson, R.W., Verma, S. How children and adolescents spend time across the world: Work, play, and developmental opportunities. Psychological Bulletin. 1999;125:701–736.
89. Law, M., Teplicky, R., King, S., King, G., Kertoy, M., Moning, T., et al. Family-centred service: Moving ideas into practice. Child: Care, Health & Development. 2005;31:633–642.
90. Lawlor, M.C., Mattingly, C.F. The complexities embedded in family-centered care. American Journal of Occupational Therapy. 1998;52:2059–2067.
91. Lawlor, M.C., Mattingly, C.F. Beyond the unobtrusive observer: Reflections on researcher-informant relationships in urban ethnography. American Journal of Occupational Therapy. 2001;55(2):147–154.
92. Lea, D. You don’t know me like that’: Patterns of disconnect between adolescent mothers of children with disabilities and their early interventionists. Journal of Early Intervention. 2006;28(4):264–282.
93. Leiter, V. Dilemmas in sharing care: Maternal provision of professionally driven therapy for children with disabilities. Social Science & Medicine. 2004;58:837–849.
94. LeRoy, B.W. Mothering children with disabilities in the context of welfare reform. In: Escaile S.A., Olson J.A., eds. Mothering occupations: challenge, agency, and participation. Philadelphia: F.A. Davis; 2004:372–390.
95. Lyon, J. I want to be Zak’s mom, not his therapist. Developmental Disabilities Special Interest Section Newsletter. 1989;12(1):4.
96. MacKean, G.L., Thurston, W.E., Scott, C.M. Bridging the divide between families and health professionals’ perspectives on family-centred care. Health Expectations. 2005;8:74–85.
97. Magill-Evans, J., Wiart, L., Darrah, J., Kratochvil, M. Beginning the transition to adulthood: The experiences of six families with youths with cerebral palsy. Physical & Occupational Therapy in Pediatrics. 2005;25(3):19–36.
98. Margetts, J.K., Le Couteur, A., Croom, S. Families in a state of flux: The experiences of grandparents in autism spectrum disorder. Child: Care, Health and Development. 2006;32:565–574.
99. Markson, S., Fiese, B.H. Family rituals as a protective factor for children with asthma. Journal of Pediatric Psychology. 2000;25:471–479.
100. McBride, S.L., Brotherson, M.J., Joanning, H., Whiddon, D., Dermitt, A. Implementation of family-centered services: Perceptions of families and professionals. Journal of Early Intervention. 1993;17:414–430.
101. McCubbin, M., Balling, K., Possin, P., Frierdich, S., Bryne, B. Family resilience in childhood cancer. Family Relations. 51. 2002:103–111.
102. McGuire, B.K., Crowe, T.K., Law, M., VanLeit, B. Mothers of children with disabilities: Occupational concerns and solutions. OTJR: Occupation, Participation and Health. 2004;24:54–63.
103. McIntosh, J., Runciman, P. Exploring the role of partnership in the home care of children with special health needs: Qualitative findings from two service evaluations. International Journal of Nursing Studies. 2008;45:714–726.
104. McKay, E.A. Mothers with mental illness: an occupation interrupted. In: Escaile S.A., Olson J.A., eds. Mothering occupations: Challenge, agency, and participation. Philadelphia: F.A. Davis; 2004:238–258.
105. McLanahan, S., Garfinkel, I., Reichman, N., Teitler, J., Carlson, M., Audigier, C.N. The fragile families and child wellbeing study: Baseline national report, 2003. Retrieved March 18, 2008, from, http://www.fragilefamilies.princeton.edu/publications.asp.
106. McWilliam, R.A., Tocci, L., Harbin, G.L. Family-centered services: Service providers’ discourse and behavior. Topics in Early Childhood and Special Education. 1998;18(4):206–221.
107. Meadow-Orlans, K.P. Sources of stress for mothers and fathers of deaf and hard of hearing infants. American Annals of the Deaf. 1995;140(4):352–357.
108. Melamed, B.G., Parenting the ill child. Bornstein, M.H., eds. Handbook of parenting, 2nd ed., Vol. 5. Mahwah, NJ: Lawrence Erlbaum, 2002;329–348.
109. Merenstein, D., Diener-West, M., Krist, A., Pinneger, M., Cooper, L.A. An assessment of the shared-decision model in parents of children with acute otitis media. Pediatrics. 2005;116:1267–1275.
110. Meyer, D.J., Vadasy, P.F. Sibshops: workshops for siblings of children with special needs. Baltimore: Paul H. Brookes, 1994.
111. Missiuna, C., Moll, S., King, S., King, G., Law, M. A trajectory of troubles: Parents’ impressions of the impact of developmental coordination disorder. Physical & Occupational Therapy in Pediatrics. 2007;27(1):81–101.
112. Morton, K. Identifying the enemy: A parent’s complaint. In: Turnbull H.R., Turnbull A., eds. Parents speak out: Now and then. Columbus, OH: Merrill; 1985:143–148.
113. Murphy, K.E. Parenting a technology assisted infant: Coping with occupational stress. Social Work in Health Care. 1997;24(3/4):113–126.
114. Murray, M., Bynum, M.S., Brody, G.H., Willert, A., Stephens, K. African American single mothers and children in context: A review of studies on risk and resilience. Clinical Child and Family Psychology Review. 2001;4:133–155.
115. Nagy, S., Ungerer, J. The adaptation of mothers and fathers to children with cystic fibrosis: A comparison. Children’s Health Care. 1990;19(3):147–154.
116. Nastro, M. An ethnographic study of mothers of children with cerebral palsy and the effect of occupational therapy intervention on their lives. Columbus: Ohio State University, 1992. [Unpublished master’s thesis].
117. National Center for Health Statistics Unmarried Childbearing, 2000. Retrieved July 2003 from, www.cdcgov/nchs/fastats/unmarry.htm.
118. Ninio, A., Rinott, N. Fathers’ involvement in the care of their infants, and their attributions of cognitive competence to infants. Child Development. 1988;59:652–663.
119. O’Keefe, N., O’Hara, J. Mental health needs of parents with intellectual disabilities. Current Opinion in Psychiatry. 2008;21(5):463–468.
120. Olsson, M.B., Hwang, C.P. Depression in mothers and fathers of children with intellectual disability. Journal of Intellectual Disability Research. 2001;45:535–543.
121. Opacich, K., Savage, T.A. Mothers with chronic illness: reconstructing occupation. In: Escaile S.A., Olson J.A., eds. Mothering occupations: Challenge, agency, and participation. Philadelphia: F.A. Davis; 2004:217–237.
122. Oswald, R.F., Culton, L.S. Under the rainbow: Rural gay life and its relevance for family providers. Family Relations. 2003;52:72–81.
123. Parish, S.L., Cloud, J.M. Child care for low-income school-age children: Disability and family structure effects in a national sample. Children and Youth Services Review. 2006;28:927–940.
124. Parish, S.L., Cloud, J.M. Financial well-being of young children with disabilities and their families. Social Work. 2006;51(3):223–232.
125. Park, C.A. Lesbian parenthood: A review of the literature. American Journal of Orthopsychiatry. 1998;68:376–389.
126. Parke, R.D., Fathers and families. Bornstein, M.H., eds. Handbook of parenting, 2nd ed., Vol. 3. Mahwah, NJ: Lawrence Erlbaum, 2002;27–74.
127. Patterson, C.J. Lesbian and gay parenthood. In: Bornstein M.H., ed. Handbook of parenting. 2nd ed. Mahwah, NJ: Lawrence Erlbaum Associates; 2002:317–338.
128. Patterson, J.M. Integrating family resilience and family stress theory. Journal of Marriage and Family. 2002;64:349–360.
129. Patterson, J.M., Blum, R.W. Risk and resilience among children and youth with disabilities. Archives of Pediatric Adolescent Medicine. 1996;1150:692–698.
130. Patterson, J.M., Garwick, A.W., Bennett, F.C., Blum, R.W. Social support in families of children with chronic conditions: Supportive and nonsupportive behaviors. Developmental and Behavioral Pediatrics. 1997;18:383–391.
131. Piggot, J., Hocking, C., Paterson, J. Parental adjustment to having a child with cerebral palsy and participation in home therapy programs. Physical & Occupational Therapy in Pediatrics. 2003;23(4):5–29.
132. Porterfield, S.L. Work choices of mothers in families with children with disabilities. Journal of Marriage and Family. 2002;64:972–981.
133. Powers, K., Hogansen, J., Geenen, S., Powers, L.E., Gil-Kashiwabara, E. Gender matters in transition to adulthood: A survey study of adolescents with disabilities and their families. Psychology in the Schools. 2008;45(4):349–364.
134. Rivers, J.W., Stoneman, Z. Sibling relationships when a child has autism: Marital stress and support coping. Journal of Autism and Developmental Disorders. 2003;33(4):383–394.
135. Rogoff, B. The cultural nature of human development. New York: Oxford University Press, 2003.
136. Sameroff, A.J., Fiese, B.H. Transactional regulation: The developmental ecology of early intervention. In: Shonkoff J.P., Meisels S.J., eds. Handbook of early childhood intervention. 2nd ed. New York: Cambridge University Press; 2000:135–159.
137. Schimoeller, G.L., Baranowski, M.D. Intergenerational support in families with disabilities: Grandparents’ perspective. Families in Society: The Journal of Contemporary Human Services. 1998;79:465–476.
138. Schteingart, J.S., Molnar, J., Klein, T.P., Lowe, C.B., Hartmann, A.H. Homelessness and child functioning in the context of risk and protective factors moderating child outcomes. Journal of Clinical Child Psychology. 1995;24:320–331.
139. Schultz-Krohn, W. Meaningful family routines in a homeless shelter. American Journal of Occupational Therapy. 2004;58(5):531–542.
140. Schulz, J.B. The parent-professional conflict. In: Turnbull H.R., Turnbull A.P., eds. Parents speak out: Then and now. 2nd ed. Columbus, OH: Merrill; 1985:3–22.
141. Seccombe, K., James, D., Walters, K.B. They think you ain’t much of nothing”: The social construction of the welfare mother. Journal of Marriage and the Family. 1998;60:849–865.
142. Segal, R. Adaptive strategies of mothers with children with ADHD: Enfolding and unfolding occupations. American Journal of Occupational Therapy. 2000;54:300–306.
143. Segal, R. Family routines and rituals: A context for occupational therapy interventions. American Journal of Occupational Therapy. 2004;58(5):499–508.
144. Segal, R., Beyer, C. Integration and application of a home treatment program: A study of parents and occupational therapists. American Journal of Occupational Therapy. 2006;60(5):500–510.
145. Segal, R., Hinojosa, J. The activity setting of homework: An analysis of three cases and implications for occupational therapy. American Journal of Occupational Therapy. 2006;60(1):50–59.
146. Shonkoff, J.P., Phillips, D.A. From neurons to neighborhoods: The science of early childhood development. Washington, DC: National Academy Press, 2000.
147. Skogrand, L., Shirer, K., Working with low-resource and culturally diverse audiences. The Forum for Family and Consumer Issues, 2007;12(1). Retrieved March 25, 2008, from, http://ncsu.edu/ffci/publications/2007/v12-n1–2007-spring/skogrand-shirer/fa-9-skogrand-shirer.php.
148. Smith, L.K., Draper, E.S., Manktelow, B.N., Dorling, J.S., Field, D.J. Socioeconomic inequalities in very preterm birth rates. Archives of Disease in Childhood—Fetal and Neonatal Edition. 2007;92:F11–F14.
149. Spagnola, M., Fiese, B.H. Family routines and rituals: A context for development in the lives of young children. Infants & Young Children. 2007;20(4):284–299.
150. Spratt, E.G., Saylor, C.F., Macias, M.M. Assessing parenting stress in multiple samples of children with special needs (CSN). Families, Systems, & Health. 2007;25(4):435–449.
151. Stacey, J., Biblarz, T.J. How does the sexual orientation of parents matter. American Sociological Review. 2001;66:159–183.
152. Steinberg, L., Silk, J.S., Parenting adolescents. Bornstein, M.H., eds. Handbook of parenting, 2nd ed., Vol. 1. Mahwah, NJ: Lawrence Erlbaum, 2002;103–133.
153. Stewart, D., Law, M., Burke-Gaffney, J., Missiuma, C., Rosenbaum, P., King, G., et al. Keeping It Together™: An information KIT for parents of children and youth with special needs. Child: Care, Health & Development. 2006;32:493–500.
154. Stoneman, Z. Supporting positive sibling relationships during childhood. Mental Retardation and Developmental Disabilities Research Reviews. 2001;7:134–142.
155. Suarez-Orozco, C., Todorova, L.G., Louie, J. Making up for lost time: The experiences of separation and reunification among immigrant families. Family Process. 2002;41:625–643.
156. Summers, J.A., Dell’Oliver, C., Turnbull, A.P., Benson, H., Santelli, E., Campbell, M., et al. Examining the individualized family service plan process: What are family and practitioner preferences. Topics in Early Childhood Special Education. 1990;10(2):78–99.
157. Tetreault, S., Parrot, A., Trahan, J. Home activity programs in families with children presenting with global developmental delays: Evaluation and parental perceptions. International Journal of Rehabilitation Research. 2003;26:165–173.
158. Trent-Stainbrook, A., Kaiser, A.P., Frey, J.R. Older siblings’ use of responsive interaction strategies and effects on their younger siblings with Down syndrome. Journal of Early Intervention. 2007;29(4):273–286.
159. Trivette, C.M., Dunst, C.J. DEC recommended practices: Family-based practices. In: Sandall S., Hemmeter M.L., Smith B.J., McLean M.E., eds. DEC recommended practices: A comprehensive guide for practical application in early intervention/early childhood special education. Missoula, MT: Division for Early Childhood; 2005:107–126.
160. Turnbull, A.P., Blue-Banning, M., Turbiville, V., Park, J. From parent education to partnership education: A call for a transformed focus. Topics in Early Childhood Education. 1999;19:164–172.
161. Turnbull, A.P., Ruef, M. Family perspectives on inclusive lifestyle issues for people with problem behavior. Exceptional Children. 1997;63:211–227.
162. Turnbull, A.P., Summers, J.A., Turnbull, R., Brotherson, M.J., Winton, P., Roberts, et al. Family supports and services in early intervention: A bold vision. Journal of Early Intervention. 2007;29(3):187–206.
163. Turnbull, A.P., Turbiville, V., Turnbull, H.R. Evolution of family-professional partnerships: Collective empowerment as the model for the early twenty-first century. In: Shonkoff J.P., Meisels S.J., eds. Handbook of early childhood intervention. 2nd ed. New York: Cambridge University Press; 2002:630–650.
164. Turnbull, A.P., Turnbull, H.R. Families, professions and exceptionality: A special partnership. Columbus, OH: Merrill, 1990;156–157.
165. Turnbull, A.P., Turnbull, H.R. Families, professionals, and exceptionality: A special partnership, 3rd ed. Columbus, OH: Merrill, 1997.
166. Turnbull, A., Turnbull, R., Erwin, E.J., Soodak, L.C. Families, professionals, and exceptionality: Positive outcomes through partnerships and trust, 5th ed. Columbus, OH: Merrill, 2006.
167. Tymchuk, A.J., Andron, L., Unger, O. Parents with mental handicaps and adequate child care: A review. Mental Handicap. 1987;15:49–54.
168. U.S. Bureau of the Census, 169. America’s families and living arrangements: Population characteristics. U.S. Department of Commerce Economics and Statistics Administration, 2002. www.census.gov. [Retrieved August 2003 from].
169. Valencia, L.S., Cromer, B.A. Sexual activity and other high-risk behaviors in adolescents with chronic illness: A review. Journal of Pediatric and Adolescent Gynecology. 2000;13:53–64.
170. VanLeit, B., Crowe, T.K. Outcomes of an occupational therapy program for mothers of children with disabilities: Impact on satisfaction with time use and occupational performance. American Journal of Occupational Therapy. 2002;56:402–410.
171. Wacharasin, C., Barnard, K.E., Spieker, S.J. Factors affecting toddler cognitive development in low-income families: Implications for practitioners. Infants and Young Children. 2003;16:175–187.
172. Walker, S. Culturally competent protection of children’s mental health. Child Abuse. Review. 2002;11:380–393.
173. Wall, S., Kisker, E.E., Peterson, C.A., Carta, J.J., Jeon, H. Child care for low-income children with disabilities: Access, quality, and parental satisfaction. Journal of Early Intervention. 2006;28(4):283–298.
174. Walsh, F. A family resilience framework: Innovative practice applications. Family Relations. 2002;51:130–137.
175. Walsh, F. Normal family processes: Growing diversity and complexity, 3rd ed. New York: Guilford Press, 2003.
176. Weiss, K.L., Marvin, R.S., Pianta, R.C. Ethnographic detection and description of family strategies for child care: Application to the study of cerebral palsy. Journal of Pediatric Psychology. 1997;22:263–278.
177. Williams, L. The many roles of families in family-centered care—Part III. Pediatric Nursing. 2007;33(2):144–146.
178. Williams, P.D., Williams, A.R., Graff, J.C., Hanson, S., Stanton, A., Hafeman, C., et al. Interrelationships among variables affecting well siblings and mothers in families of children with chronic illness or disability. Journal of Behavioral Medicine. 2002;25:411–424.
179. Young, D.M., Roopnarine, J.L. Fathers’ childcare involvement with children with and without disabilities. Topics in Early Childhood Special Education. 1994;14(4):488–502.