Chapter 16 Nervous System
The nervous system consists of three main parts:
• The central nervous system (CNS), which includes the brain and the spinal cord
• The peripheral nervous system (PNS), which includes neurons outside the CNS and the cranial and spinal nerves that connect the brain and spinal cord with the peripheral structures
• The autonomic nervous system (ANS), which has parts in both the CNS and PNS and which consists of neurons that innervate smooth muscle, cardiac muscle, glandular epithelium, or combinations of these tissues
Origin of Nervous System
The nervous system develops from the neural plate, a thickened area of embryonic ectoderm (Fig. 16-1A and B). The notochord and paraxial mesoderm induce the overlying ectoderm to differentiate into the neural plate. Formation of the neural folds, neural tube, and neural crest from the neural plate is shown in Figure 16-1B to F. The neural tube differentiates into the CNS, consisting of the brain and spinal cord. The neural crest gives rise to the cells that form most of the PNS and ANS.
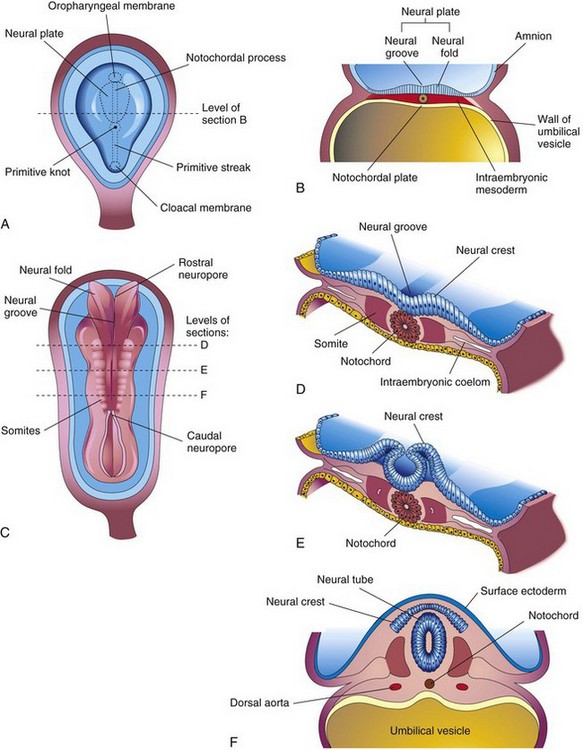
Figure 16–1 The neural plate and formation of the neural tube. A, Dorsal view of an embryo at approximately 18 days, exposed by removing the amnion. B, Transverse section of the embryo, showing the neural plate and early development of the neural groove and neural folds. C, Dorsal view of an embryo at approximately 22 days. The neural folds have fused opposite the fourth to sixth somites, but are open at both ends. D to F, Transverse sections of this embryo at the levels shown in C, showing the formation of the neural tube and its detachment from the surface ectoderm.
Formation of the neural plate and neural tube, a process known as neurulation, begins during the early part of the fourth week (22-23 days). Fusion of the neural folds proceeds in cranial and caudal directions until only small areas remain open at both ends (Fig. 16-2A and B). At these sites, the lumen of the neural tube—the neural canal—communicates freely with the amniotic cavity (Fig. 16-2C). The cranial opening—the rostral neuropore—closes on approximately the 25th day; the caudal neuropore closes 2 days later (Fig. 16-2D). Closure of the neuropores coincides with the establishment of a vascular circulation for the neural tube. The walls of the neural tube thicken to form the brain and spinal cord (Fig. 16-3). The neural canal forms the ventricular system of the brain and central canal of the spinal cord. The dorsoventral patterning of the neural tube appears to involve the sonic hedgehog (Shh) gene, Pax genes, bone morphogenetic proteins, and dorsalin, a transforming growth factor (TGF-β).
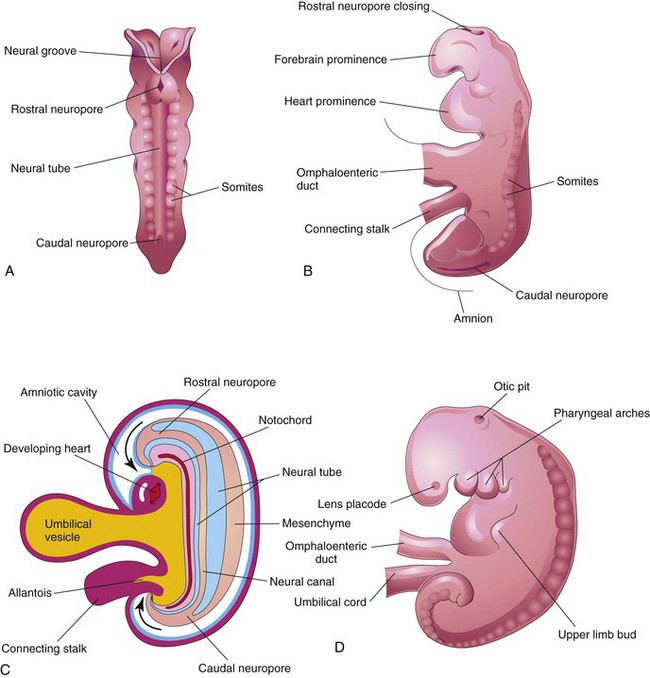
Figure 16–2 A, Dorsal view of an embryo at approximately 23 days, showing fusion of the neural folds, leading to formation of the neural tube. B, Lateral view of an embryo at approximately 24 days, showing the forebrain prominence and closing of the rostral neuropore. C, Sagittal section of the embryo, showing the transitory communication of the neural canal with the amniotic cavity (arrows). D, Lateral view of an embryo at approximately 27 days. Note that the neuropores shown in B are closed.
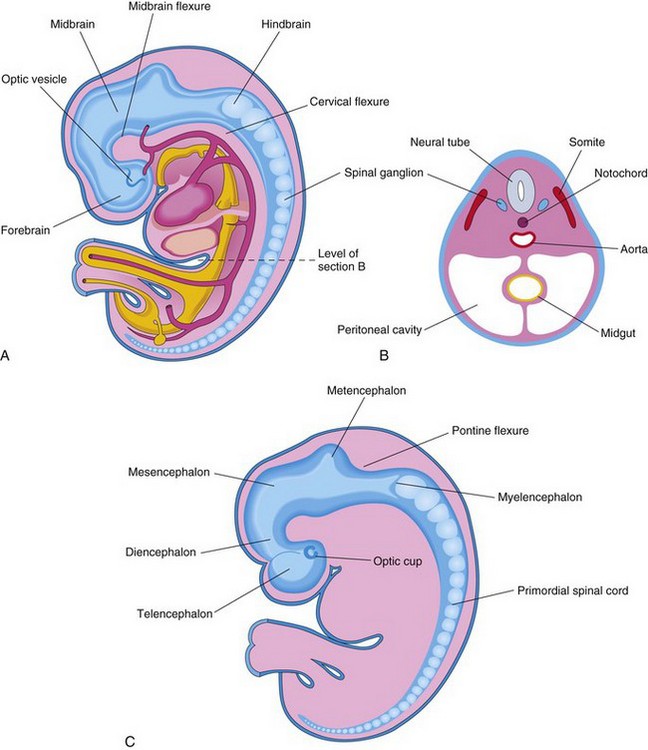
Figure 16–3 A, Lateral view of an embryo at approximately 28 days, showing the three primary brain vesicles: forebrain, midbrain, and hindbrain. Two flexures demarcate the primary divisions of the brain. B, Transverse section of the embryo, showing the neural tube that will develop into the spinal cord in this region. The spinal ganglia derived from the neural crest are also shown. C, Lateral view of the central nervous system of a 6-week embryo, showing the secondary brain vesicles and pontine flexure.
Development of Spinal Cord
The neural tube caudal to the fourth pair of somites develops into the spinal cord (Fig. 16-3). The lateral walls of the neural tube thicken and gradually reduce the size of the neural canal to a minute central canal (Fig. 16-4A to C). Initially, the wall of the neural tube is composed of a thick, pseudostratified, columnar neuroepithelium (Fig. 16-4D). These neuroepithelial cells constitute the ventricular zone (ependymal layer), which gives rise to all neurons and macroglial cells (e.g., astrocytes and oligodendrocytes) in the spinal cord (Fig. 16-5). Soon, a marginal zone composed of the outer parts of the neuroepithelial cells is recognizable (see Fig. 16-4E). This zone gradually becomes the white matter of the spinal cord as axons grow into it from nerve cell bodies in the spinal cord, spinal ganglia, and brain.
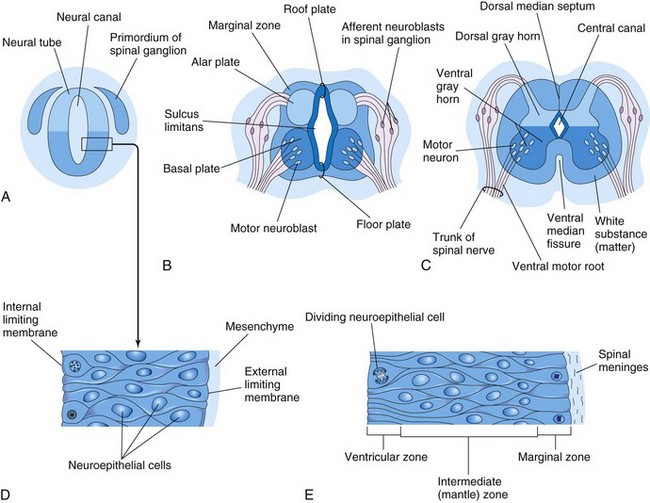
Figure 16–4 Development of the spinal cord. A, Transverse section of the neural tube of an embryo at approximately 23 days. B and C, Similar sections in 6- and 9-week embryos, respectively. D, Section of the wall of the neural tube shown in A. E, Section of the wall of the developing spinal cord, showing its three zones.
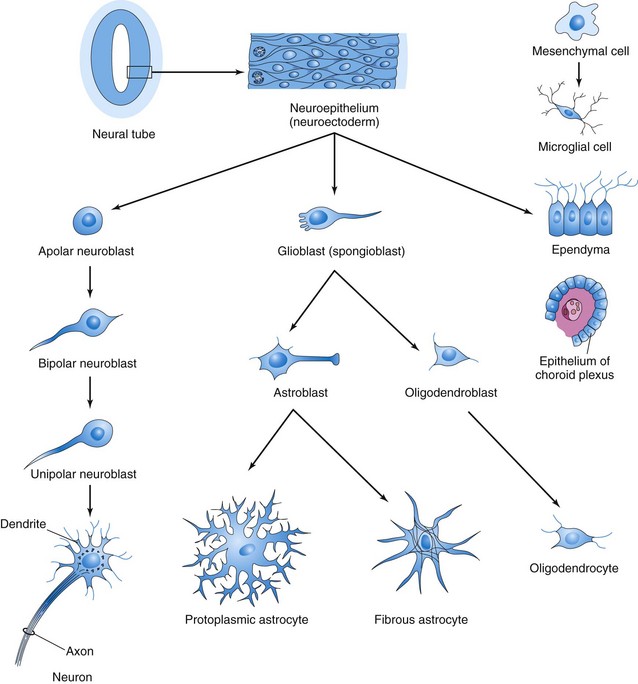
Figure 16–5 Histogenesis of cells in the central nervous system. After further development, the multipolar neuroblast (lower left) becomes a nerve cell or a neuron. Neuroepithelial cells give rise to all neurons and macroglial cells.
Some neuroepithelial cells in the ventricular zone differentiate into primordial neurons—neuroblasts. These embryonic cells form an intermediate zone (mantle layer) between the ventricular and marginal zones. Neuroblasts become neurons as they develop cytoplasmic processes (Fig. 16-5). The primordial supporting cells of the CNS—the glioblasts (spongioblasts)—differentiate from the neuroepithelial cells, mainly after neuroblast formation has ceased. The glioblasts migrate from the ventricular zone into the intermediate and marginal zones. Some glioblasts become astroblasts and later astrocytes, whereas other glioblasts become oligodendroblasts and eventually oligodendrocytes (Fig. 16-5). When neuroepithelial cells cease producing neuroblasts and glioblasts, they differentiate into ependymal cells, which form the ependyma lining the central canal of the spinal cord.
Microglial cells (microglia), which are scattered throughout the gray and white matter, are small cells that are derived from mesenchymal cells (Fig. 16-5). Microglial cells invade the CNS rather late in the fetal period, after it has been penetrated by blood vessels. Microglia originate in the bone marrow and are part of the mononuclear phagocytic cell population.
Proliferation and differentiation of neuroepithelial cells in the developing spinal cord produce thick walls and a thin roof and floor plates (Fig. 16-4B). Differential thickening of the lateral walls of the spinal cord soon produces a shallow, longitudinal groove on each side, the sulcus limitans (Figs. 16-4B and 16-6). This groove separates the dorsal part, the alar plate (lamina), from the ventral part, the basal plate (lamina). The alar and basal plates produce longitudinal bulges extending through most of the length of the developing spinal cord. This regional separation is of fundamental importance because the alar and basal plates are later associated with afferent and efferent functions, respectively.
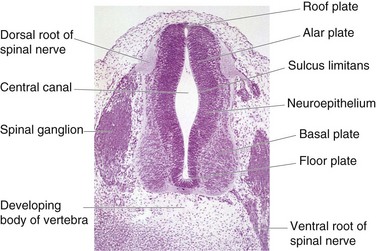
Figure 16–6 Transverse section of an embryo (×100) at 40 days. The ventral root of the spinal nerve is composed of nerve fibers arising from neuroblasts in the basal plate, whereas the dorsal root is formed by nerve processes arising from neuroblasts in the spinal ganglion.
Cell bodies in the alar plates form the dorsal gray columns that extend the length of the spinal cord. In transverse sections, these columns are the dorsal gray horns (Fig. 16-7). Neurons in these columns constitute afferent nuclei, which form the dorsal roots of the spinal nerves. As the alar plates enlarge, the dorsal median septum forms. Cell bodies in the basal plates form the ventral and lateral gray columns. In transverse sections of the spinal cord, these columns are the ventral gray horns and lateral gray horns, respectively. Axons of the ventral horn cells grow out of the cord and form the ventral roots of the spinal nerves (Fig. 16-7). As the basal plates enlarge, they bulge ventrally on each side of the median plane. As this bulging occurs, the ventral median septum forms and a deep longitudinal groove—the ventral median fissure—develops on the ventral surface of the cord.
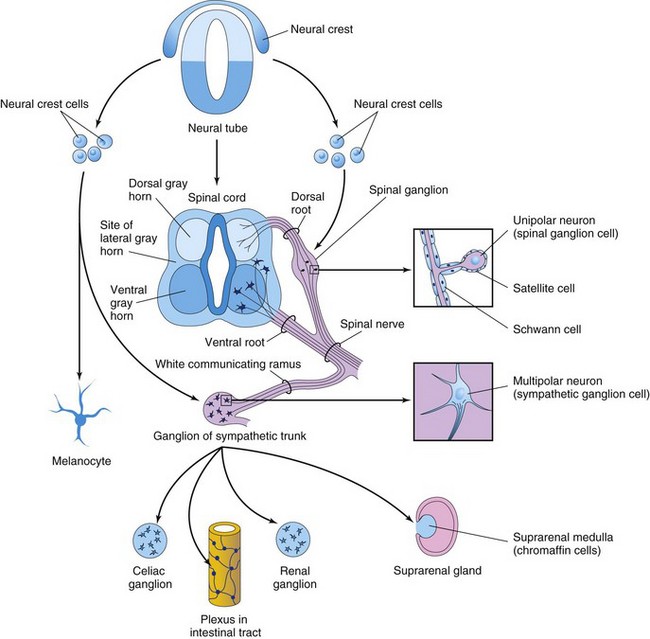
Figure 16–7 Derivatives of the neural crest. Neural crest cells also differentiate into the cells in the afferent ganglia of cranial nerves and many other structures.
Development of Spinal Ganglia
The unipolar neurons in the spinal ganglia (dorsal root ganglia) are derived from neural crest cells (Fig. 16-7). The peripheral processes of the spinal ganglion cells pass in the spinal nerves to sensory endings in somatic or visceral structures. The central processes enter the spinal cord, constituting the dorsal roots of the spinal nerves.
Development of Spinal Meninges
The mesenchyme surrounding the neural tube condenses to form the primordial meninx or meninges (Figs. 16-2C and 16-4A, D, and E). The external layer of this membrane gives rise to the dura mater (Fig. 16-8A). The internal layer—the pia mater and arachnoid mater—leptomeninges—is derived from neural crest cells. Fluid-filled spaces appear within the leptomeninges that soon coalesce to form the subarachnoid space (Fig. 16-9A). Embryonic cerebrospinal fluid (CSF) begins to form during the fifth week.
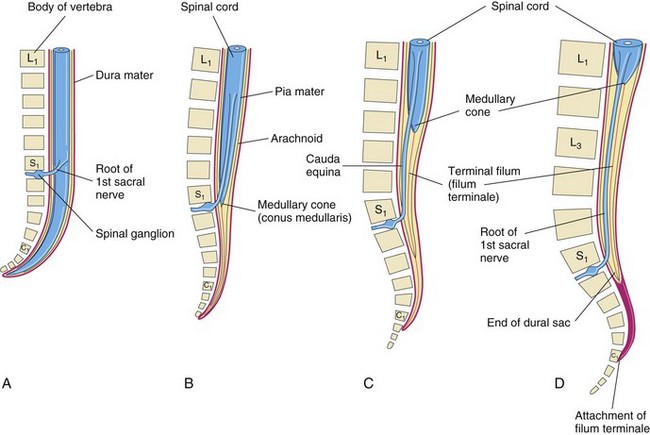
Figure 16–8 The position of the caudal end of the spinal cord in relation to the vertebral column and the meninges at various stages of development are shown. The increasing inclination of the root of the first sacral nerve is also shown. A, At 8 weeks. B, At 24 weeks. C, Newborn infant. D, Adult.
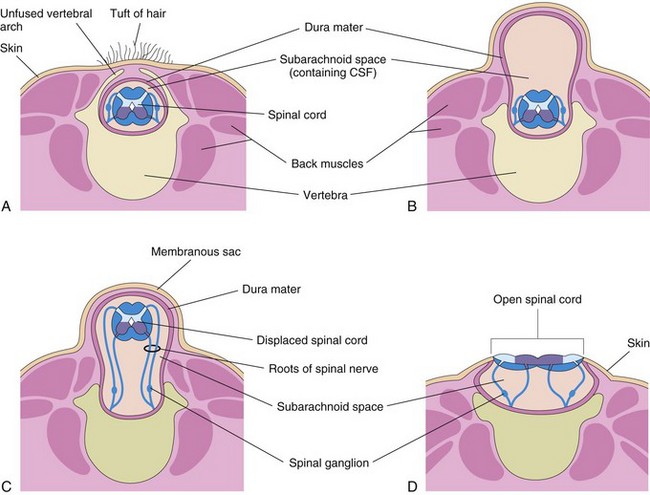
Figure 16–9 Various types of spina bifida. A, Spina bifida occulta. Observe the unfused vertebral arch. B, Spina bifida with meningocele. C, Spina bifida with meningomyelocele. D, Spina bifida with myeloschisis. The types shown in B to D are referred to collectively as spina bifida cystica because of the cystlike sac that is associated with them.
Positional Changes of Spinal Cord
The spinal cord in the embryo extends the entire length of the vertebral canal at 8 weeks (Fig. 16-8A). The spinal nerves pass through the intervertebral foramina opposite their levels of origin. Because the vertebral column and dura mater grow more rapidly than the spinal cord, the positional relationship to the spinal nerves does not persist. The caudal end of the spinal cord gradually comes to lie at relatively higher levels. At 24 weeks, it lies at the level of the first sacral vertebra (Fig. 16-8B). The spinal cord in the newborn infant terminates at the level of the second or third lumbar vertebra (Fig. 16-8C). The spinal cord in the adult usually terminates at the inferior border of the first lumbar vertebra (Fig. 16-8D). As a result, the spinal nerve roots, especially those of the lumbar and sacral segments, run obliquely from the spinal cord to the corresponding level of the vertebral column. The nerve roots inferior to the end of the cord—the medullary cone (Latin conus medullaris)—form a sheaf of nerve roots, the cauda equina (Latin horse’s tail). Although in adults the dura mater and arachnoid mater usually end at the S2 vertebra distal to the caudal end of the spinal cord, the pia mater forms a long, fibrous thread, the terminal filum (Latin filum terminale) (Fig. 16-8C and D). The filum extends from the medullary cone to the periosteum of the first coccygeal vertebra.
Myelination of Nerve Fibers
Myelin sheaths surrounding nerve fibers within the spinal cord begin to form during the late fetal period and continue to form during the first postnatal year. In general, fiber tracts become myelinated at approximately the time they become functional. Motor roots are myelinated before sensory roots. The myelin sheaths surrounding the nerve fibers within the spinal cord are formed by oligodendrocytes. The myelin sheaths surrounding the axons of peripheral nerve fibers are formed by the plasma membranes of the neurolemma cells (Schwann cells). Myelination of the nerve fibers is regulated by β-1 integrins. These neuroglial cells are derived from neural crest cells that migrate peripherally and wrap themselves around the axons of somatic motor neurons and presynaptic autonomic motor neurons as they pass out of the CNS (Fig. 16-7). These cells also wrap themselves around both the central and peripheral processes of the somatic and the visceral sensory neurons, as well as around the axons of postsynaptic autonomic motor neurons.
Birth Defects of Spinal Cord
Most congenital anomalies of the spinal cord result from defective closure of the neural tube during the fourth week. These neural tube defects (NTDs) affect the tissues overlying the spinal cord, including the meninges, neural arches, muscles, and skin (Fig. 16-9B to D). Anomalies involving the neural arches are referred to as spina bifida.
Spina Bifida Occulta
Spina bifida occulta results from failure of the embryonic halves of the neural arch to grow normally and fuse in the median plane (Fig. 16-9A). Spina bifida occulta occurs in vertebra L5 or S1 in approximately 10% of otherwise normal people. In its most minor form, the only evidence of its presence may be a small dimple with a tuft of hair arising from it (Fig. 16-10). Spina bifida occulta usually produces no clinical symptoms.
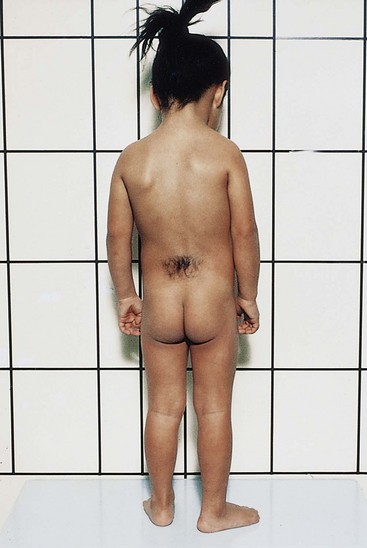
Figure 16–10 A female child with a hairy patch in the lumbosacral region, indicating the site of a spina bifida occulta.
(Courtesy of A.E. Chudley, M.D., Section of Genetics and Metabolism, Department of Pediatrics and Child Health, Children’s Hospital and University of Manitoba, Winnipeg, Manitoba, Canada.)
Spina Bifida Cystica
Severe types of spina bifida, involving protrusion of the spinal cord, meninges, or both through the defects in the vertebral arches, are referred to collectively as spina bifida cystica because of the cystlike sac that is associated with these anomalies (Figs. 16-9B to D and 16-11). Spina bifida cystica occurs in approximately 1 in 1000 births. When the sac contains meninges and CSF, the anomaly is called spina bifida with meningocele (Fig. 16-9B). The spinal cord and spinal roots are in their normal position, but spinal cord abnormalities may be present. If the spinal cord, nerve roots, or both are included in the sac, the anomaly is called spina bifida with meningomyelocele (Figs. 16-9C and 16-11). Spina bifida with meningomyelocele involving several vertebrae is often associated with partial absence of the brain—meroencephaly (anencephaly) (Fig. 16-12).

Figure 16–11 The back of a newborn infant with a large lumbar meningomyelocele. The neural tube defect is covered with a thin membrane.
(Courtesy of A.E. Chudley, M.D., Section of Genetics and Metabolism, Department of Pediatrics and Child Health, Children’s Hospital and University of Manitoba, Winnipeg, Manitoba, Canada.)
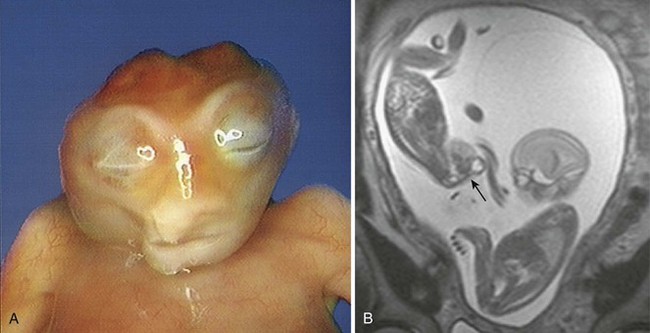
Figure 16–12 A, A fetus with meroencephaly (anencephaly). B, Magnetic resonance image (MRI) of diamniotic-monochorionic twins, one with meroencephaly. Note the absent calvarium of the abnormal twin and the amnion of the normal twin.
(A, Courtesy of Wesley Lee, M.D., Division of Fetal Imaging, Department of Obstetrics and Gynecology, William Beaumont Hospital, Royal Oak, MI. B, Courtesy of Deborah Levine, MD, Director of Obstetric and Gynecologic Ultrasound, Beth Israel Deaconess Medical Center, Boston, Massachusetts.)
Causes of Neural Tube Defects
Genetic, nutritional, and environmental factors play a role in the production of NTDs. Epidemiologic studies have shown that folic acid supplements (400 µg daily) taken at least 1 month before conception and continuing through the first trimester reduce the incidence of NTDs. Certain drugs increase the risk of NTD. For example, valproic acid, an anticonvulsant, causes NTDs in 1% to 2% of pregnant women if given during the fourth week of development, when the neural folds are fusing.
Development of Brain
The neural tube cranial to the fourth pair of somites develops into the brain. Even before the neural folds are completely fused, three distinct vesicles are recognizable in the rostral end of the developing neural tube. From rostral to caudal, these primary brain vesicles (Fig. 16-13) form the forebrain (prosencephalon), midbrain (mesencephalon), and hindbrain (rhombencephalon). During the fifth week, the forebrain partially divides into two secondary brain vesicles, the telencephalon and diencephalon; the midbrain does not divide. The hindbrain divides into the metencephalon and myelencephalon; consequently, there are five secondary brain vesicles.
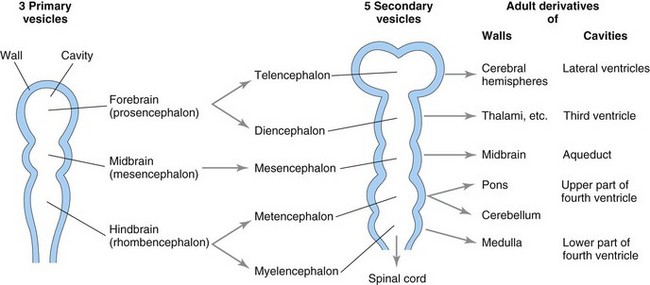
Figure 16–13 Brain vesicles, indicating the adult derivatives of their walls and cavities. The rostral part of the third ventricle forms from the cavity of the telencephalon; most of this ventricle is derived from the cavity of the diencephalon.
Brain Flexures
The embryonic brain grows rapidly during the fourth week and bends ventrally with the head fold. This bending produces the midbrain flexure in the midbrain region and the cervical flexure at the junction of the hindbrain and the spinal cord (Fig. 16-14A). Later, unequal growth of the developing brain between these flexures produces the pontine flexure in the opposite direction. This flexure results in thinning of the roof of the hindbrain. The sulcus limitans extends cranially to the junction of the midbrain and forebrain, and the alar and basal plates are recognizable only in the midbrain and the hindbrain (Figs. 16-4B and 16-14C).
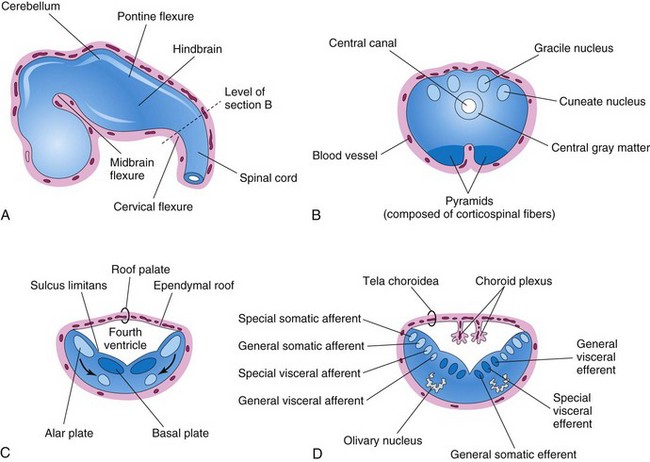
Figure 16–14 A, The developing brain at the end of the fifth week, showing the three primary divisions of the brain and the brain flexures. B, Transverse section of the caudal part of the myelencephalon. C and D, Similar sections of the rostral part of the myelencephalon, showing the position and successive stages of differentiation of the alar and basal plates. The arrows in C show the pathway taken by the neuroblasts from the alar plates to form the olivary nuclei.
Hindbrain
The cervical flexure demarcates the hindbrain from the spinal cord (Fig. 16-14A). The pontine flexure divides the hindbrain into caudal (myelencephalon) and rostral (metencephalon) parts. The myelencephalon becomes the medulla oblongata (often called the medulla), whereas the metencephalon becomes the pons and cerebellum. The cavity of the hindbrain becomes the fourth ventricle and the central canal in the caudal part of the medulla (Fig. 16-14B and C).
Myelencephalon
Neuroblasts from the alar plates in the myelencephalon migrate into the marginal zone and form isolated areas of gray matter: the gracile nuclei medially and the cuneate nuclei laterally (Fig. 16-14B). These nuclei are associated with correspondingly named nerve tracts that enter the medulla from the spinal cord. The ventral area of the medulla contains a pair of fiber bundles—pyramids—that consist of corticospinal fibers descending from the developing cerebral cortex.
The rostral part of the myelencephalon is wide and rather flat, especially opposite the pontine flexure (Fig. 16-14C and D). As the pontine flexure forms, the walls of the medulla move laterally and the alar plates come to lie lateral to the basal plates (Fig. 16-14C). As the positions of the plates change, the motor nuclei generally develop medial to the sensory nuclei.
Neuroblasts in the basal plates of the medulla, like those in the spinal cord, develop into motor neurons. In the medulla, the neuroblasts form nuclei (groups of nerve cells) and organize into three cell columns on each side (Fig. 16-14D). From medial to lateral, they are:
• The general somatic efferent, represented by neurons of the hypoglossal nerve
• The special visceral efferent, represented by neurons innervating muscles derived from the pharyngeal arches (see Chapter 10)
• The general visceral efferent, represented by some neurons of the vagus and the glossopharyngeal nerves
Neuroblasts from the alar plates of the medulla form neurons that are arranged in four columns on each side (Fig. 16-14D). From medial to lateral, they are:
• The general visceral afferent, receiving impulses from the viscera
• The special visceral afferent, receiving taste fibers
• The general somatic afferent, receiving impulses from the surface of the head
• The special somatic afferent, receiving impulses from the ear
Some neuroblasts from the alar plates migrate ventrally and form the neurons in the olivary nuclei (Fig. 16-14C and D).
Metencephalon
The walls of the metencephalon form the pons and cerebellum; its cavity forms the superior part of the fourth ventricle (Fig. 16-15). As in the rostral part of the myelencephalon, the pontine flexure causes divergence of the lateral walls of the pons, which spreads the gray matter in the floor of the fourth ventricle.
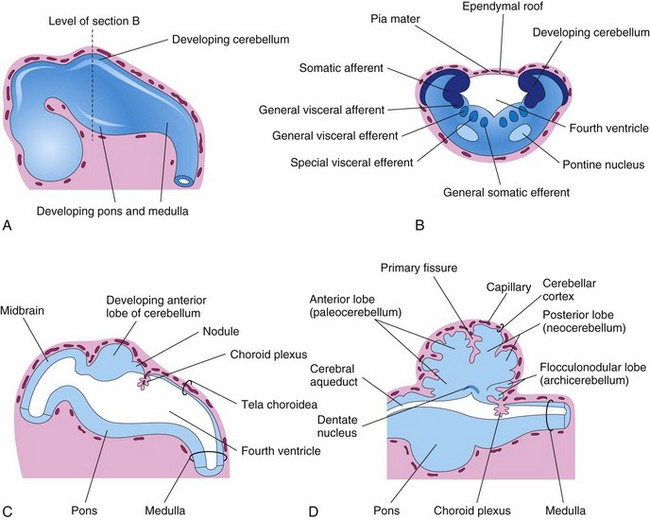
Figure 16–15 A, The developing brain at the end of the fifth week. B, Transverse section of the metencephalon (developing pons and cerebellum), showing the derivatives of the alar and basal plates. C and D, Sagittal sections of the hindbrain at 6 and 17 weeks, respectively, showing successive stages in the development of the pons and cerebellum.
The cerebellum develops from the dorsal parts of the alar plates (Fig. 16-15A and B). Initially, the cerebellar swellings project into the fourth ventricle (Fig. 16-15C). As the swellings enlarge and fuse in the median plane, they overgrow the rostral half of the fourth ventricle and overlap the pons and the medulla (Fig. 16-15D). Some neuroblasts in the intermediate zone of the alar plates migrate to the marginal zone and differentiate into the neurons of the cerebellar cortex. Other neuroblasts from these plates give rise to the central nuclei, the largest of which is the dentate nucleus (Fig 16-15D). Cells from the alar plates also give rise to the pontine nuclei, the cochlear and vestibular nuclei, and the sensory nuclei of the trigeminal nerve.
Nerve fibers connecting the cerebral and cerebellar cortices with the spinal cord pass through the marginal layer of the ventral region of the metencephalon—the pons (Fig. 16-15C and D).
Choroid Plexuses and Cerebrospinal Fluid
The thin ependymal roof of the fourth ventricle is covered externally by pia mater (Fig. 16-15C and D). This vascular membrane, together with the ependymal roof, forms the tela choroidea of the fourth ventrical. Because of the active proliferation of the pia mater, the tela choroidea invaginates the fourth ventricle, where it differentiates into the choroid plexus (infoldings of choroidial arteries of the pia mater). Similar choroid plexuses develop in the roof of the third ventricle and in the medial walls of the lateral ventricles.
The choroid plexuses secrete ventricular fluid, which becomes CSF. The thin roof of the fourth ventricle evaginates in three locations. These outpouchings rupture to form openings, the median and lateral apertures. These apertures permit CSF to enter the subarachnoid space from the fourth ventricle.
Midbrain
The midbrain (mesencephalon) undergoes very little change. The neural canal narrows and becomes the cerebral aqueduct (see Fig. 16-15D), a canal that connects the third and fourth ventricles. Neuroblasts migrate from the alar plates of the midbrain into the tectum (roof), where they aggregate to form four large groups of neurons—the paired superior and inferior colliculi (Fig. 16-16B), which are concerned with visual and auditory reflexes, respectively. Neuroblasts from the basal plates appear to give rise to groups of neurons in the tegmentum (red nuclei, nuclei of the third and fourth cranial nerves, and reticular nuclei). The substantia nigra, a broad layer of gray matter adjacent to the cerebral peduncle (Fig. 16-16D and E), may also differentiate from the basal plate, but some authorities believe that it is derived from cells in the alar plate that migrate ventrally. Fibers growing from the cerebrum form the cerebral peduncles anteriorly (Fig. 16-16B). These peduncles become progressively more prominent as additional descending fiber groups (corticopontine, corticobulbar, and corticospinal) pass through the developing midbrain on their way to the brainstem and spinal cord.
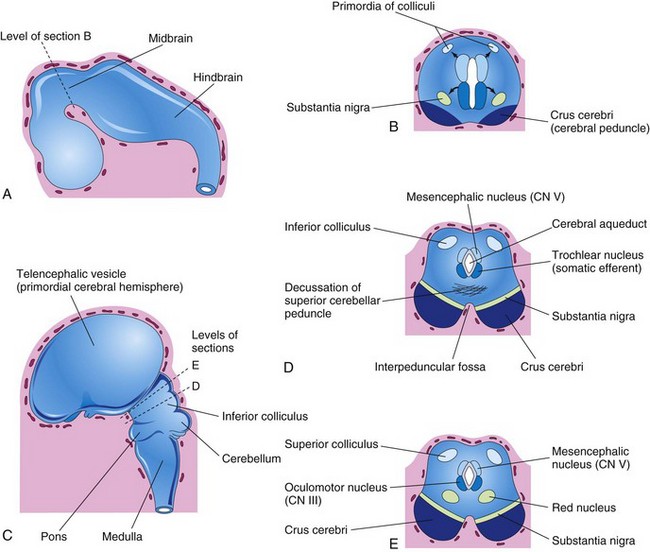
Figure 16–16 A, The developing brain at the end of the fifth week. B, Transverse section of the developing midbrain, showing the early migration of cells from the basal and alar plates. C, The developing brain at 11 weeks. D and E, Transverse sections of the developing midbrain at the level of the inferior and superior colliculi, respectively.
Forebrain
As closure of the rostral neuropore occurs, two lateral outgrowths—optic vesicles—appear (Fig. 16-3A), one on each side of the forebrain. The optic vesicles are the primordia of the retinas and optic nerves. A second pair of diverticula soon arises more dorsally and rostrally, representing the telencephalic vesicles (Fig. 16-16C). They are the primordia of the cerebral hemispheres and their cavities become the lateral ventricles. The rostral, or anterior, part of the forebrain, including the primordia of the cerebral hemispheres, is known as the telencephalon, whereas the caudal, or posterior, part of the forebrain is called the diencephalon. The cavities of the telencephalon and diencephalon contribute to the formation of the third ventricle (Fig. 16-17D and E).
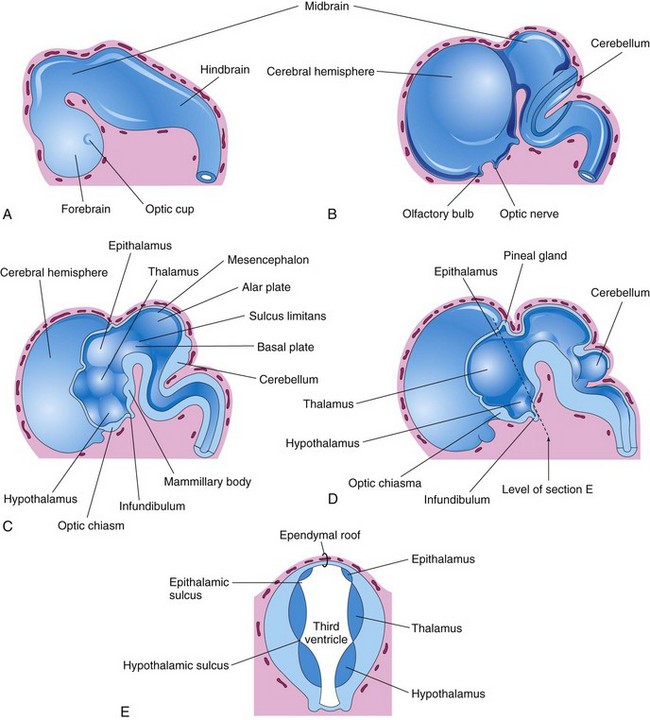
Figure 16–17 A, External view of the brain at the end of the fifth week. B, Similar view at 7 weeks. C, Median section of the brain, showing the medial surface of the forebrain and midbrain. D, Similar section at 8 weeks. E, Transverse section of the diencephalon, showing the epithalamus dorsally, the thalamus laterally, and the hypothalamus ventrally.
Diencephalon
Three swellings develop in the lateral walls of the third ventricle, which later become the thalamus, hypothalamus, and epithalamus (Fig. 16-17C to E). The thalamus develops rapidly on each side and bulges into the cavity of the third ventricle, eventually reducing it to a narrow cleft. The hypothalamus arises by the proliferation of neuroblasts in the intermediate zone of the diencephalic walls. A pair of nuclei, the mammillary bodies, form pea-sized swellings on the ventral surface of the hypothalamus (Fig. 16-17C). The epithalamus develops from the roof and dorsal part of the lateral wall of the diencephalon. Initially, the epithalamic swellings are large, but later they become relatively small.
The pineal gland (pineal body) develops as a median diverticulum of the caudal part of the roof of the diencephalon (Fig. 16-17D). Proliferation of the cells in its walls soon converts it into a solid, cone-shaped gland.
The pituitary gland (Fig. 16-18 and Table 16-1) is ectodermal in origin. It develops from two sources:
• An upgrowth from the ectodermal roof of the stomodeum—the hypophysial diverticulum (Rathke pouch)
• A downgrowth from the neuroectoderm of the diencephalon—the neurohypophysial diverticulum
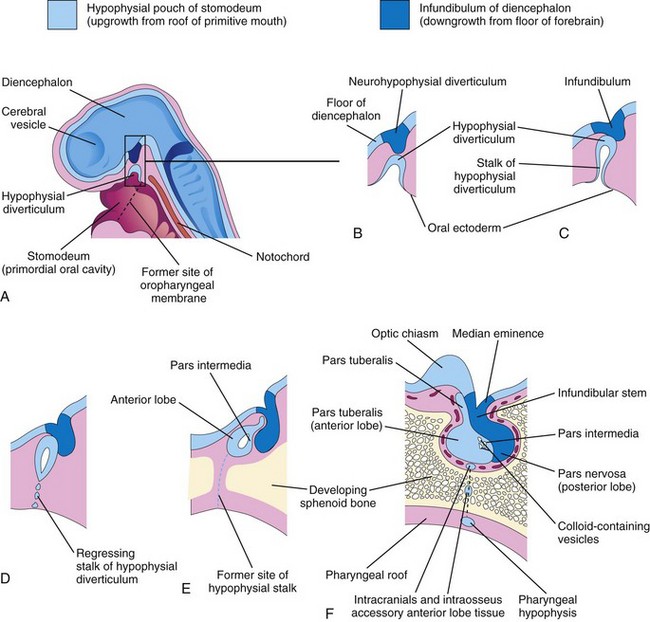
Figure 16–18 Development of the pituitary gland. A, Sagittal section of the cranial end of an embryo at approximately 36 days, showing the hypophysial diverticulum, an upgrowth from the stomodeum, and the neurohypophysial diverticulum, a downgrowth from the forebrain. B to D, Successive stages of the developing pituitary gland. By 8 weeks, the diverticulum loses its connection with the oral cavity and is in close contact with the infundibulum and posterior lobe (neurohypophysis) of the pituitary gland. E and F, Later stages, showing proliferation of the anterior wall of the hypophysial diverticulum to form the anterior lobe (adenohypophysis) of the pituitary gland.
Table 16–1 Derivation and Terminology of Pituitary Gland

This double embryonic origin of the pituitary gland explains why it is composed of two different types of tissue.
• The adenohypophysis (glandular part), or anterior lobe, arises from the oral ectoderm.
• The neurohypophysis (nervous part), or posterior lobe, originates from the neuroectoderm.
During the third week, a hypophysial diverticulum projects from the roof of the stomodeum and lies adjacent to the floor (ventral wall) of the diencephalon (Fig. 16-18A and B). By the fifth week, this diverticulum has elongated and constricted at its attachment to the oral epithelium, giving it a nipple-like appearance (Fig. 16-18C). By this stage, it has come into contact with the infundibulum (derived from the neurohypophysial diverticulum), a ventral downgrowth of the diencephalon. The stalk of the hypophysial diverticulum gradually regresses (Fig. 16-18C to E). The parts of the pituitary gland that develop from the ectoderm of the stomodeum—pars anterior, pars intermedia, and pars tuberalis—form the adenohypophysis (Table 16-1).
Cells of the anterior wall of the hypophysial diverticulum proliferate and give rise to the pars anterior of the pituitary gland. Later, an extension, the pars tuberalis, grows around the infundibular stem (Fig. 16-18F). The extensive proliferation of the anterior wall of the hypophysial diverticulum reduces its lumen to a narrow cleft (Fig. 16-18E). Cells in the posterior wall of the hypophysial diverticulum do not proliferate; they give rise to the thin, poorly defined pars intermedia (Fig. 16-18F). The part of the pituitary gland that develops from the neuroectoderm of the brain (infundibulum) is the neurohypophysis (Table 16-1). The infundibulum gives rise to the median eminence, infundibular stem, and pars nervosa.
Telencephalon
The telencephalon consists of a median part and two lateral diverticula, the cerebral vesicles (Fig. 16-18A). These vesicles are the primordial of the cerebral hemispheres, which are identifiable at 7 weeks (Fig. 16-19A). The cavity of the median part of the telencephalon forms the extreme anterior part of the third ventricle. At first, the cerebral hemispheres are in wide communication with the cavity of the third ventricle through the interventricular foramina (Fig. 16-19B). As the cerebral hemispheres expand, they cover successively the diencephalon, midbrain, and hindbrain. The hemispheres eventually meet each other in the midline, flattening their medial surfaces.
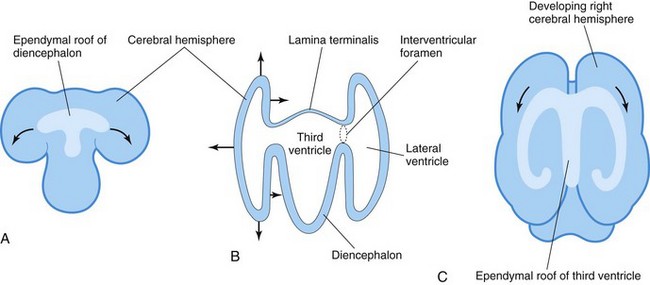
Figure 16–19 A, Dorsal surface of the forebrain, showing how the ependymal roof of the diencephalon is carried out to the dorsomedial surface of the cerebral hemispheres. B, The forebrain, showing how the developing cerebral hemispheres grow from the lateral walls of the forebrain and expand in all directions until they cover the diencephalon. The rostral wall of the forebrain, the lamina terminalis, is very thin. C, The forebrain, showing how the ependymal roof is finally carried into the temporal lobes as a result of the C-shaped growth pattern of the cerebral hemispheres. The arrows indicate some of the directions in which the hemispheres expand.
The corpus striatum appears during the sixth week as a prominent swelling in the floor of each cerebral hemisphere (Fig. 16-20B). As a result, the floor of each hemisphere expands more slowly than its thin cortical wall, and the cerebral hemispheres become C-shaped (Fig. 16-21). The growth and curvature of the hemispheres also affect the shape of the lateral ventricles. They become roughly C-shaped cavities filled with CSF. The caudal end of each cerebral hemisphere turns ventrally and then rostrally, forming the temporal lobe; in so doing, it carries with it the ventricle (forming the temporal horn) and the choroid fissure (Fig. 16-21). Here, the thin medial wall of the hemisphere is invaginated along the choroid fissure by the vascular pia mater to form the choroid plexus of the temporal horn of the lateral ventricle (Figs. 16-20B and 16-21B).
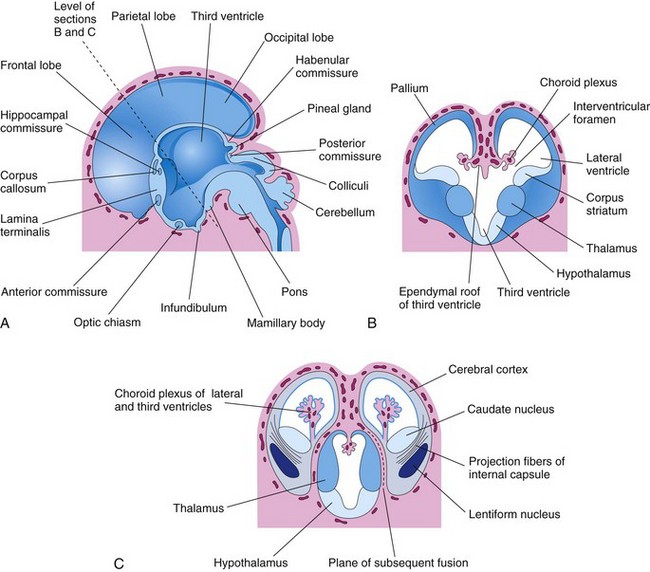
Figure 16–20 A, Medial surface of the forebrain of a 10-week embryo, showing the diencephalic derivatives, the main commissures, and expanding cerebral hemispheres. B, Transverse section of the forebrain at the level of the interventricular foramina, showing the corpus striatum and choroid plexuses of the lateral ventricles. C, Similar section at approximately 11 weeks, showing division of the corpus striatum into the caudate and lentiform nuclei by the internal capsule.
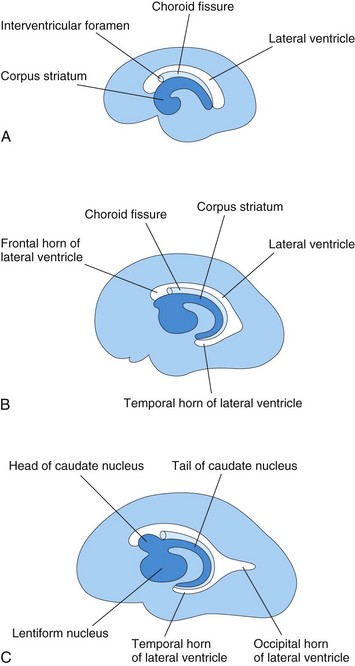
Figure 16–21 Medial surface of the developing right cerebral hemisphere, showing the development of the lateral ventricle, choroid fissure, and corpus striatum. A, At 13 weeks. B, At 21 weeks. C, At 32 weeks.
As the cerebral cortex differentiates, fibers passing to and from it pass through the corpus striatum and divide it into the caudate and lentiform nuclei. This fiber pathway—the internal capsule (Fig. 16-20C)—becomes C-shaped as the hemisphere assumes this form. The caudate nucleus becomes elongated and C-shaped, conforming to the outline of the lateral ventricle (Fig. 16-21A to C). Its pear-shaped head and elongated body lie in the floor of the frontal horn and the body of the lateral ventricle; its tail makes a U-shaped turn to gain the roof of the temporal horn.
Cerebral Commissures
As the cerebral cortex develops, groups of fibers—commissures—connect corresponding areas of the cerebral hemispheres with one another (Fig. 16-20). The most important commissures cross in the lamina terminalis, the rostral end of the forebrain. This lamina extends from the roof plate of the diencephalon to the optic chiasm. The anterior commissure connects the olfactory bulb and related brain areas of one hemisphere with those of the opposite side. The hippocampal commissure connects the hippocampal formations. The corpus callosum, the largest cerebral commissure, connects the neocortical areas (Fig. 16-20A). The rest of the lamina terminalis becomes stretched to form the septum pellucidum, a thin plate of brain tissue. By birth, the corpus callosum extends over the roof of the diencephalon.
The optic chiasm, which develops in the ventral part of the lamina terminalis (Fig. 16-20A), consists of fibers from the medial halves of the retinas that cross to join the optic tract of the opposite side.
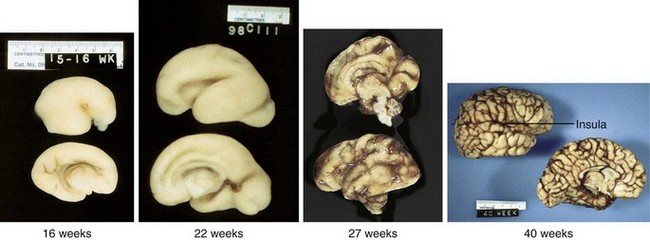
Initially, the surface of the hemispheres is smooth (Fig. 16-22); however, as growth proceeds, sulci (grooves) and gyri (convolutions) develop (Fig. 16-22). The sulci and gyri permit a considerable increase in the surface area of the cerebral cortex without requiring an extensive increase in cranial size. As each cerebral hemisphere grows, the cortex covering the external surface of the corpus striatum grows relatively slowly and is soon overgrown. This buried cortex, hidden from view in the depths of the lateral sulcus (fissure) of the cerebral hemisphere, is the insula.
Congenital Anomalies of Brain
Most major congenital anomalies of the brain result from defective closure of the rostral neuropore during the fourth week of development (Fig. 16-23A) and involve the overlying tissues (meninges and calvaria). MRI is often used for evaluation of the fetal brain in pregnancies at risk for fetal defects. The factors causing neural tube defects (NTDs) are genetic, nutritional, or environmental.
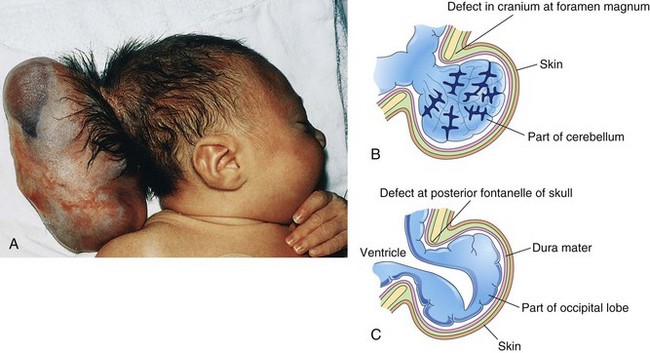
Figure 16–23 Cranium bifidum (bony defect of the cranium) and herniation of the brain and meninges. A, Infant with a large meningoencephalocele in the occipital area. B, Meningoencephalocele consisting of a protrusion of part of the cerebellum that is covered by meninges and skin. C, Meningohydroencephalocele consisting of a protrusion of part of the occipital lobe that contains part of the posterior horn of a lateral ventricle.
(A, Courtesy of A.E. Chudley, M.D., Section of Genetics and Metabolism, Department of Pediatrics and Child Health, Children’s Hospital and University of Manitoba, Winnipeg, Manitoba, Canada.)
Pharyngeal Hypophysis and Craniopharyngioma
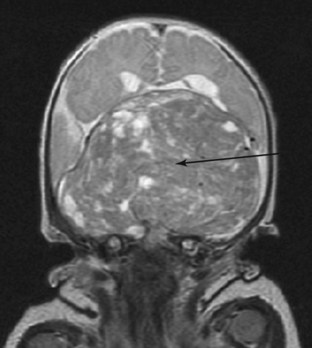
A remnant of the stalk of the hypophysial diverticulum may persist and form a pharyngeal hypophysis in the roof of the oropharynx (Fig. 16-18E and F). Occasionally, craniopharyngiomas from remnants of the stalk of the hypophysial diverticulum develop in the pharynx or in the basisphenoid (posterior part of the sphenoid bone), but most often, they form in or superior to the sella turcica of the cranium (Fig. 16-24).
Cranium Bifidum
Defects in the formation of the cranium (cranium bifidum) are often associated with congenital anomalies of the brain, meninges, or both. Defects of the cranium (skull) usually involve the median plane of the calvaria. The defect is often in the squamous part of the occipital bone and may include the posterior part of the foramen magnum. When the defect is small, usually only the meninges herniate, and the anomaly is called a cranial meningocele. Cranium bifidum associated with herniation of the brain, the meninges, or both occurs in approximately 1 in 2000 births. When the cranial defect is large, the meninges and part of the brain herniate, forming a meningoencephalocele (Fig. 16-23A and B). If the protruding brain contains part of the ventricular system, the anomaly is called a meningohydroencephalocele (Fig. 16-23).
Meroencephaly (Anencephaly)
Meroencephaly (anencephaly) is a severe anomaly of the brain that results from failure of the rostral neuropore to close during the fourth week of development (Fig. 16-12). Most of the infant’s brain extrudes from the cranium. Although this defect is often called anencephaly, a rudimentary brainstem and functioning neural tissue are present. Meroencephaly is usually associated with a multifactorial pattern of inheritance.
Microcephaly
In microcephaly, the calvaria and brain are small, but the face is of normal size. Affected infants are usually severely mentally challenged (IQ below 35-40) because the cranium and brain are underdeveloped. Some cases of microcephaly appear to be genetic (autosomal recessive); others are caused by environmental factors such as cytomegalovirus infection in utero (see Chapter 19). Exposure during the fetal period to large amounts of ionizing radiation, infectious agents, and certain drugs is a contributing factor in some cases.
Hydrocephalus
Hydrocephalus results from impaired circulation and absorption of cerebrospinal fluid (CSF) or, in unusual cases, from increased production of CSF. An excess of CSF is present in the ventricular system of the brain (Fig. 16-25). Impaired circulation of CSF often results from congenital aqueductal stenosis (narrow cerebral aqueduct). Blockage of CSF circulation results in dilation of the ventricles proximal to the obstruction and increased pressure on the cerebral hemispheres. This squeezes the brain between the ventricular fluid and the calvaria. In infants, the internal pressure results in an accelerated rate of expansion of the brain and calvaria because the fibrous sutures of the calvaria are not fused.
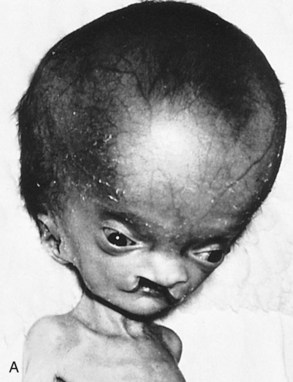

Figure 16–25 A, An infant with hydrocephalus and a bilateral cleft palate. Hydrocephalus often produces thinning of the bones of the calvaria, prominence of the forehead, and atrophy of the cerebral cortex and white substance. B, Axial magnetic resonance imaging scan (transverse section through the brain) of a fetus with X-linked hydrocephalus at approximately 29 weeks gestation, showing the massively enlarged ventricles (*) and thinned cortex (oval).
(Courtesy of Dr. E.H. Whitby, Magnetic Resonance Imaging Unit, University of Sheffield, United Kingdom.)
Arnold-Chiari Malformation
Arnold-Chiari malformation is the most common congenital anomaly involving the cerebellum (Fig. 16-26). A tongue-like projection of the medulla and inferior displacement of the vermis of the cerebellum herniate through the foramen magnum into the vertebral canal. The condition results in a type of communicating hydrocephalus in which there is interference with the absorption of CSF; as a result, the entire ventricular system is distended.
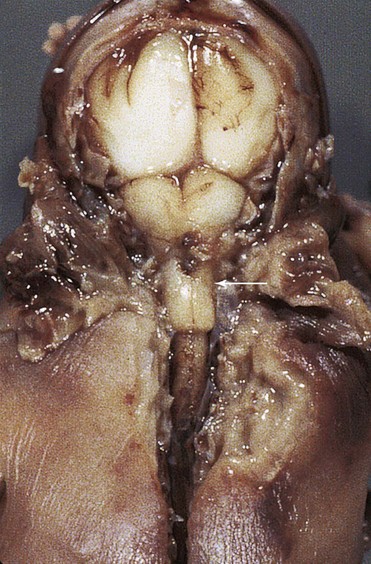
Figure 16–26 Arnold-Chiari type II malformation in a 23-week fetus. In situ exposure of the hindbrain shows cerebellar tissue well below the foramen magnum (arrow).
(Courtesy of Dr. Marc R. Del Bigio, Department of Pathology [Neuropathology], University of Manitoba and Health Sciences Centre, Winnipeg, Manitoba, Canada.)
Development of Peripheral Nervous System
The peripheral nervous system (PNS) consists of cranial, spinal, and visceral nerves and cranial, spinal, and autonomic ganglia. All sensory cells (somatic and visceral) of the PNS are derived from neural crest cells. The cell bodies of these sensory cells are located outside the CNS. The cell body of each afferent neuron is closely invested by a capsule of modified Schwann cells, known as satellite cells (Fig. 16-7), which are derived from neural crest cells. This capsule is continuous with the neurolemmal sheath of Schwann cells that surrounds the axons of afferent neurons.
Neural crest cells in the developing brain migrate to form sensory ganglia only in relation to the trigeminal (CN V), facial (CN VII), vestibulocochlear (CN VIII), glossopharyngeal (CN IX), and vagus (CN X) nerves. Neural crest cells also differentiate into multipolar neurons of the autonomic ganglia (Fig. 16-7), including ganglia of the sympathetic trunks that lie along the sides of the vertebral bodies; collateral or prevertebral, ganglia in the plexuses of the thorax and abdomen (e.g., cardiac, celiac, and mesenteric plexuses); and parasympathetic, or terminal, ganglia in or near the viscera (e.g., the submucosal, or Meissner, plexus). Paraganglia—chromaffin cells—are also derived from the neural crest. The term paraganglia includes several widely scattered groups of cells that are similar in many ways to the medullary cells of the suprarenal glands. The cell groups largely lie retroperitoneally, often in association with sympathetic ganglia. The carotid and aortic bodies also have small islands of chromaffin cells associated with them. These widely scattered groups of chromaffin cells constitute the chromaffin system.
Spinal Nerves
Motor nerve fibers arising from the spinal cord begin to appear at the end of the fourth week (Fig. 16-4). The nerve fibers arise from cells in the basal plates of the developing spinal cord and emerge as a continuous series of rootlets along its ventrolateral surface. The fibers destined for a particular developing muscle group become arranged in a bundle, forming a ventral nerve root (Figs. 16-6 and 16-7). The nerve fibers of the dorsal nerve root are formed by axons derived from neural crest cells that migrate to the dorsolateral aspect of the spinal cord, where they differentiate into the cells of the spinal ganglion (Fig. 16-7). The central processes of the neurons in the spinal ganglion form a single bundle that grows into the spinal cord, opposite the apex of the dorsal horn of gray matter (Fig. 16-4B and C). The distal processes of the spinal ganglion cells grow toward the ventral nerve root and eventually join it to form a spinal nerve (Fig. 16-7).
As the limb buds develop, the nerves from the spinal cord segments opposite to them elongate and grow into the limbs. The nerve fibers are distributed to its muscles, which differentiate from myogenic cells that originate from the somites (see Chapter 15). The skin of the developing limbs is also innervated in a segmental manner.
Cranial Nerves
Twelve pairs of cranial nerves form during the fifth and sixth weeks. They are classified into three groups according to their embryologic origins.
Somatic Efferent Cranial Nerves
The trochlear (CN IV), abducent (CN VI), hypoglossal (CN XII), and the greater part of the oculomotor (CN III) nerves, are homologous with the ventral roots of the spinal nerves (Fig. 16-27A). The cells of origin of these nerves are located in the somatic efferent column (derived from the basal plates) of the brainstem. Their axons are distributed to the muscles derived from the head myotomes (preotic and occipital) (see Fig. 15-17A).
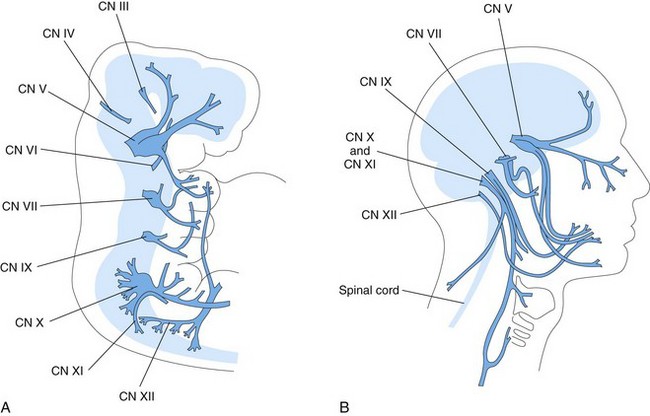
Figure 16–27 A, A 5-week embryo, showing the distribution of most of the cranial nerves, especially those supplying the pharyngeal arches. B, The head and neck of an adult, showing the general distribution of most of the cranial nerves.
The trochlear nerve (CN IV) arises from nerve cells in the somatic efferent column in the posterior part of the midbrain. Although a motor nerve, it emerges from the brainstem dorsally and passes ventrally to supply the superior oblique muscle of the eye.
The abducent nerve (CN VI) arises from nerve cells in the basal plates of the metencephalon. It passes from its ventral surface to the posterior of the three preotic myotomes from which the lateral rectus muscle of the eye is thought to originate.
The hypoglossal nerve (CN XII) develops by fusion of the ventral root fibers of three or four occipital nerves (Fig. 16-27A). Sensory roots, corresponding to the dorsal roots of the spinal nerves, are absent. The somatic motor fibers originate from the hypoglossal nucleus. These fibers leave the ventrolateral wall of the medulla in several groups—the hypoglossal nerve roots—which converge to form the common trunk of CN XII (Fig. 16-27B). They grow rostrally and eventually innervate the muscles of the tongue, which are derived from the occipital myotomes (see Fig. 15-17A).
The oculomotor nerve (CN III) supplies the superior, inferior, and medial recti and inferior oblique muscles of the eye.
Nerves of Pharyngeal Arches
Cranial nerves V, VII, IX, and X supply the embryonic pharyngeal arches; thus, the structures that develop from these arches are innervated by these cranial nerves (Fig. 16-27A and Table 10-1).
The trigeminal nerve (CN V) is the nerve of the first pharyngeal arch, but it has an ophthalmic division that is not a pharyngeal arch component. CN V is the principal sensory nerve for the head. The cells of the large trigeminal ganglion are derived from the most anterior part of the neural crest. The central processes of the cells in this ganglion form the large sensory root of CN V, which enters the lateral part of the pons. The peripheral processes of cells in this ganglion separate into three large divisions (ophthalmic, maxillary, and mandibular nerves). Their sensory fibers supply the skin of the face as well as the lining of the mouth and nose. The motor fibers of CN V arise from cells in the most anterior part of the special visceral efferent column in the metencephalon. These fibers pass to the muscles of mastication and to other muscles that develop in the mandibular prominence of the first pharyngeal arch (see Table 10-1). The mesencephalic nucleus of CN V differentiates from cells in the midbrain.
The facial nerve (CN VII) is the nerve of the second pharyngeal arch. It consists mostly of motor fibers that arise principally from a nuclear group in the special visceral efferent column in the caudal part of the pons. These fibers are distributed to the muscles of facial expression and to other muscles that develop in the mesenchyme of the second pharyngeal arch (see Table 10-1). The small general visceral efferent component of CN VII terminates in the peripheral autonomic ganglia of the head. The sensory fibers of CN VII arise from the cells of the geniculate ganglion. The central processes of these cells enter the pons, and the peripheral processes pass to the greater superficial petrosal nerve and, via the chorda tympani nerve, to the taste buds in the anterior two thirds of the tongue.
The glossopharyngeal nerve (CN IX) is the nerve of the third pharyngeal arch. Its motor fibers arise from the special and, to a lesser extent, the general visceral efferent columns of the anterior part of the myelencephalon. CN IX forms from several rootlets that arise from the medulla just caudal to the developing internal ear. All the fibers from the special visceral efferent column are distributed to the stylopharyngeus muscle, which is derived from the mesenchyme in the third pharyngeal arch (see Table 10-1). The general efferent fibers are distributed to the otic ganglion from which postsynaptic fibers pass to the parotid and posterior lingual glands. The sensory fibers of CN IX are distributed as general sensory and special visceral afferent fibers (taste fibers) to the posterior part of the tongue.
The vagus nerve (CN X) is formed by fusion of the nerves of the fourth and sixth pharyngeal arches (see Table 10-1). The nerve of the fourth pharyngeal arch becomes the superior laryngeal nerve, which supplies the cricothyroid muscle and the constrictor muscles of the pharynx. The nerve of the sixth pharyngeal arch becomes the recurrent laryngeal nerve, which supplies various laryngeal muscles.
The spinal accessory nerve (CN XI) arises from the cranial five or six cervical segments of the spinal cord (Fig. 16-26). The spinal accessory nerve supplies the sternocleidomastoid and trapezius muscles.
Special Sensory Nerves
The olfactory nerve (CN I) arises from the olfactory bulb. The olfactory cells are bipolar neurons that differentiate from cells in the epithelial lining of the primordial nasal sac. The axons of the olfactory cells are collected into 18 to 20 bundles around which the cribriform plate of the ethmoid bone develops. These unmyelinated nerve fibers end in the olfactory bulb.
The optic nerve (CN II) is formed by more than a million nerve fibers that grow into the brain from neuroblasts in the primordial retina. Because the optic nerve develops from the evaginated wall of the forebrain, it actually represents a fiber tract of the brain. Development of the optic nerve is described in Chapter 17.
The vestibulocochlear nerve (CN VIII) consists of two kinds of sensory fiber in two bundles; these fibers are known as the vestibular and cochlear nerves. The vestibular nerve originates in the semicircular ducts, whereas the cochlear nerve proceeds from the cochlear duct, in which the spiral organ (of Corti) develops (see Chapter 17). The bipolar neurons of the vestibular nerve have their cell bodies in the vestibular ganglion. The central processes of these cells terminate in the vestibular nuclei in the floor of the fourth ventricle. The bipolar neurons of the cochlear nerve have their cell bodies in the spiral ganglion. The central processes of these cells end in the ventral and dorsal cochlear nuclei in the medulla.
Development of Autonomic Nervous System
Functionally, the autonomic system can be divided into sympathetic (thoracolumbar) and parasympathetic (craniosacral) parts.
Sympathetic Nervous System
During the fifth week, neural crest cells in the thoracic region migrate along each side of the spinal cord, where they form paired cellular masses (ganglia) dorsolateral to the aorta (Fig. 16-7). All these segmentally arranged sympathetic ganglia are connected in a bilateral chain by longitudinal nerve fibers. These ganglionated cords—sympathetic trunks—are located on each side of the vertebral bodies. Some neural crest cells migrate ventral to the aorta and form neurons in the preaortic ganglia, such as the celiac and mesenteric ganglia (Fig. 16-7). Other neural crest cells migrate to the area of the heart, lungs, and gastrointestinal tract, where they form terminal ganglia in sympathetic organ plexuses, located near or within these organs.
After the sympathetic trunks have formed, axons of sympathetic neurons located in the intermediolateral cell column (lateral horn) of the thoracolumbar segments of the spinal cord, pass through the ventral root of a spinal nerve and a white communicating ramus to a paravertebral ganglion (Fig. 16-7). Here they may synapse with neurons or ascend or descend in the sympathetic trunk to synapse at other levels. Other presynaptic fibers pass through the paravertebral ganglia without synapsing, forming splanchnic nerves to the viscera. The postsynaptic fibers course through a gray communicating ramus, passing from a sympathetic ganglion into a spinal nerve; hence, the sympathetic trunks are composed of ascending and descending fibers.
Parasympathetic Nervous System
The presynaptic parasympathetic fibers arise from neurons in the nuclei of the brainstem and in the sacral region of the spinal cord. The fibers from the brainstem leave through the oculomotor (CN III), facial (CN VII), glossopharyngeal (CN IX), and vagus (CN X) nerves. The postsynaptic neurons are located in the peripheral ganglia or in plexuses near or within the structure being innervated (e.g., pupil of the eye, salivary glands).
Clinically Oriented Questions
1. Are neural tube defects hereditary? A woman had an infant with spina bifida cystica, and her daughter had an infant with meroencephaly. Is the daughter likely to have another child with a neural tube defect? Can meroencephaly and spina bifida be detected early in fetal life?
2. Some say that pregnant women who are heavy drinkers may have infants who exhibit mental and growth retardation. Is this true? There are reports of women who get drunk during pregnancy, yet have infants who seem to be normal. Is there a safe threshold for alcohol consumption during pregnancy?
3. A woman was told that cigarette smoking during pregnancy probably caused the slight mental retardation of her infant. She is not a heavy smoker. Was the woman correctly informed?
4. Do all types of spina bifida cause loss of motor function in the lower limbs? What treatments are there for infants with spina bifida cystica?