8 THE COMPLETE CAST CROWN PREPARATION
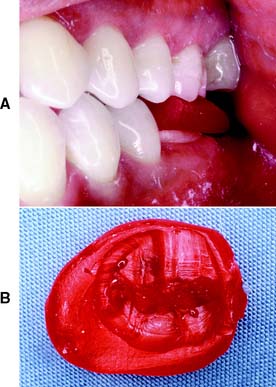
Although esthetic factors may limit its application, the all-metal complete cast crown should always be offered to patients requiring restoration for badly damaged posterior teeth. The complete cast crown has the best longevity of all fixed restorations. It can be used to rebuild a single tooth or as a retainer for a fixed dental prosthesis. It involves all axial walls, as well as the occlusal surface of the tooth being restored (Fig. 8-1).
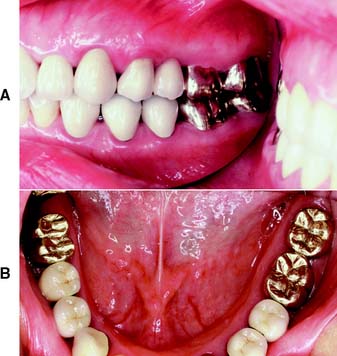
Fig. 8-1 Complete cast crowns used to restore the molar teeth. A and B, The canines and premolars, which are more visible because of their more anterior arch position, have been restored with metal-ceramic crowns.
Preparation for a complete cast crown requires that adequate tooth structure be removed to allow restoration of the tooth to its original contours. Tooth structure should be preserved when possible, but reduction should produce a crown of acceptable strength.
ADVANTAGES
Because all axial surfaces of the tooth are included in the preparation, the complete cast crown has greater retention than a more conservative restoration on the same tooth (e.g., a seven-eighths or three-quarter crown [see Fig. 7-34]).
Normally, a complete cast crown preparation also has greater resistance form than does a partial-coverage restoration on the same tooth. For a partial veneer crown to rotate off the tooth, only the tooth structure immediately lingual to the occlusal portion of the proximal groove or box need fail. However, if the axial walls of a complete cast crown have been prepared with the proper degree of taper or convergence, a significant amount of tooth structure must fail before the crown can be torqued off.
The strength of a complete cast crown is superior to that of other restorations. Its cylinder-like configuration encircles the tooth and is reinforced by a corrugated occlusal surface. Just as an O-shaped link in a chain resists deformation better than a C-shaped link, this restoration is less easily deformed than its counterparts, which are more conservative of tooth structure.
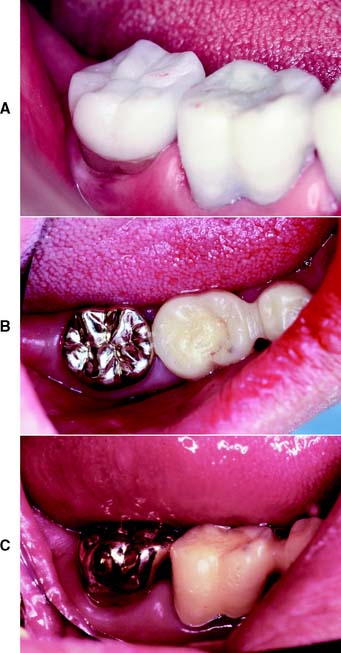
A complete cast crown allows the operator to modify axial tooth contour. This can be of special significance with malaligned teeth, although the extent of possible recontouring is limited by periodontal considerations. Similarly, it is possible to allow better access to furcations for improved patient oral hygiene through recontouring of buccal and lingual walls (Fig. 8-2). When special requirements exist for axial contours, such as when retainers are needed for partial removable dental prostheses, a complete crown is often the only restoration that allows the necessary modifications for the creation of properly shaped survey lines, guide planes, and occlusal rests (Fig. 8-3) (see Chapter 21).
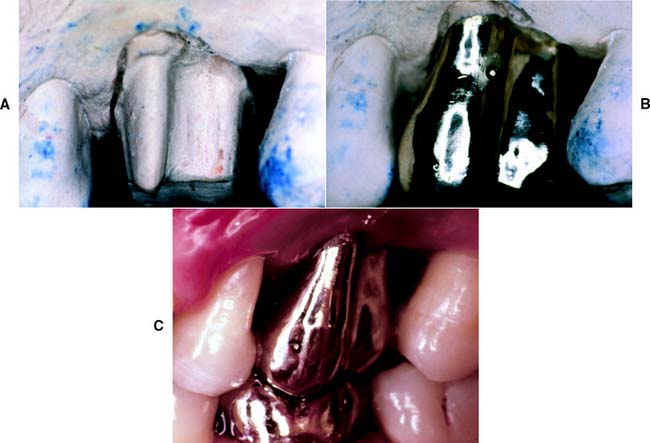
Fig. 8-2 A, B, and C, Fluting of the axial walls of a molar complete cast crown allows better access to the furcation area for oral hygiene and improves the long-term prognosis of the restoration.
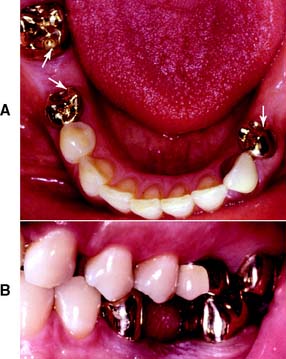
Fig. 8-3 Complete cast crowns used as retainers to accommodate a mandibular partial removable dental prosthesis. Metal-ceramic crowns have been placed on the mandibular left canine (A) and the maxillary first molar (B). Note the occlusal rests (A, arrows) and the survey contours (B), which extend to form reciprocating guide planes. (See Chapter 21.)
The restoration permits easy modification of the occlusion, which is often difficult to accomplish if a more conservative restoration is made. This is especially important when supraerupted teeth are present or when the occlusal plane needs to be reestablished.
DISADVANTAGES
Because all coronal surfaces are involved in the preparation for a complete cast crown, removal of tooth structure is extensive and can have adverse effects on the pulp and periodontium. Because of the proximity of the margin to the gingiva, it is not uncommon to see inflammation of gingival tissues (although a properly fitting complete cast crown with good axial contour should minimize this).
After cementation, it is no longer feasible to perform electric vitality testing of an abutment tooth. The conductivity of the metal interferes with the test. This can be a disadvantage if future complications occur, although thermal tests occasionally yield the necessary information.
Patients may object to the display of metal associated with complete cast crowns, and in those with a normal smile line, the restoration may be restricted to maxillary molars and mandibular molars and premolars.
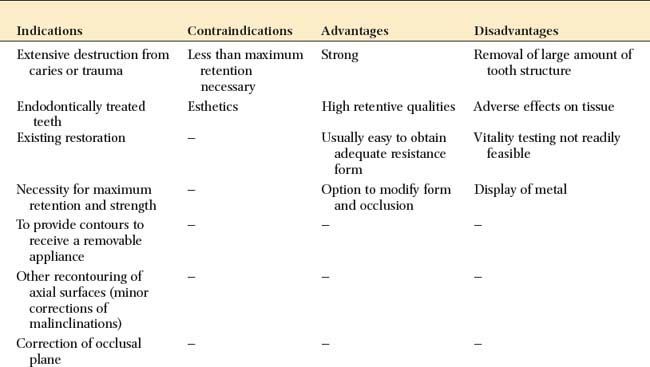
INDICATIONS
The complete cast crown is indicated on teeth that exhibit extensive coronal destruction by caries or trauma. It is the restoration of choice whenever maximum retention and resistance are needed. On short clinical crowns or when high displacement forces are anticipated, such as for the retainer of a long-span fixed dental prosthesis, grooves should be included as additional retentive features.
This restoration is fabricated when correction of axial contours is not feasible with a more conservative technique. The restoration also may be used to support a partial removable dental prosthesis, because obtaining the necessary contours with a partial-coverage restoration is more difficult. Although proximal guide planes can sometimes be prepared through simple enamel modification, arriving at properly oriented reciprocal guide planes and survey contours is often impractical. The minimum dimensions required for occlusal rests of a partial removable dental prosthetic framework necessitate removing significant amounts of enamel and, if the dentin is exposed, restoring the tooth with a cast crown.*
The complete cast crown is indicated on endodontically treated teeth. Its superior strength compensates for the loss of tooth structure that results from previous restorations, carious lesions, and endodontic access.
CONTRAINDICATIONS
The complete cast crown is contraindicated if treatment objectives can be met with a more conservative restoration. Wherever an intact buccal or lingual wall exists, use of a partial-coverage restoration should be considered. In particular, if less than maximum retention and resistance are needed (e.g., on a short-span fixed dental prosthesis), a preparation more conservative of tooth structure is called for. Similarly, if an adequate buccal contour exists or can be obtained through enamel modification (enameloplasty), a complete crown is not indicated. If a high esthetic need exists (e.g., for anterior teeth), a complete cast crown is also contraindicated.
CRITERIA
The occlusal reduction must allow adequate room for the restorative material from which the cast crown is to be fabricated: type III or IV gold casting alloy or their low–gold content equivalent. Minimum recommended clearance is 1 mm on nonfunctional (noncentric) cusps and 1.5 mm on functional (centric) cusps. The occlusal reduction should follow normal anatomic contours to remain as conservative of tooth structure as possible. Axial reduction should parallel the long axis of the tooth but allow for the recommended 6-degree taper or convergence, which is the angle measured between opposing axial surfaces.
The margin should have a chamfer configuration and is ideally located supragingivally. Sometimes crown lengthening is indicated to obtain a supragingival margin, rather than risk future periodontal disease (see Chapter 6). The chamfer should be smooth and distinct and allow for approximately 0.5 mm of metal thickness at the margin. Typically, it is an exact replica of half the rotary instrument that was used to prepare it. (The recommended dimensions for reduction are shown in Fig. 8-4.)
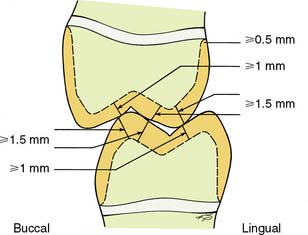
Fig. 8-4 Recommended dimensions for a complete cast crown. On functional cusps (buccal mandibular and lingual maxillary), the occlusal clearance should be equal to or greater than 1.5 mm. On nonfunctional cusps, a clearance of at least 1 mm is needed. The chamfer should allow for approximately 0.5 mm of metal thickness at the margin.
Special Considerations
Functional (centric) cusp bevel
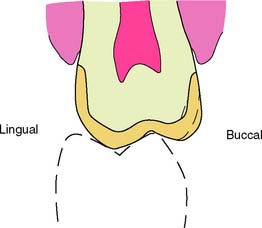
Proper tooth preparation for a complete cast crown results in the reduction’s being directly beneath the cusps of the crown (see Fig. 7-45). This is important for ensuring optimum restoration contour with maximum durability and conservation of tooth structure. Proper placement of the functional cusp bevel achieves this outcome. Because additional reduction is needed for the functional cusps (to provide 1.5 mm of occlusal clearance), the bevel must be angled flatter than the external surface (Fig. 8-5). On most teeth, the functional cusp bevel is placed at about 45 degrees to the long axis.

Nonfunctional (noncentric) cusp bevel
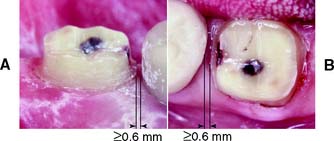
All complete crown preparations should be assessed for adequate reduction at the occlusoaxial line angles of the nonfunctional cusps. A minimum of 0.6 mm of clearance is needed here for adequate strength. Maxillary molars in particular often require an additional reduction bevel in this area (Fig. 8-6). Without it, an overcontoured restoration that does not follow normal configuration may result. Such additional reduction is often unnecessary for mandibular molars, however, because they are lingually inclined and their profile is relatively straight.
Chamfer width
Increasing the faciolingual width of a complete crown is a common error in practice and is a leading cause of periodontal disease associated with restorations. Adequate chamfer width (minimum 0.5 mm) is important for developing optimum axial contour. On small premolars, however, it may be advantageous to prepare a slightly narrower chamfer to conserve tooth structure and retention form. This requires increasingly careful manipulation of the wax pattern during fabrication of the restoration and careful assessment to ensure that the crown is not excessively contoured.
PREPARATION
The clinical procedure to prepare a tooth for a complete cast crown consists of the following steps:

| INSTRUMENT | USE |
|---|---|
| Tapered carbide bur or diamond | Occlusal guiding grooves |
| Additional retentive features | |
| Narrow, round-tipped, tapered diamond (regular grit) (0.8 mm) | Occlusal reduction |
| Axial alignment grooves | |
| Axial reduction | |
| Chamfer preparation | |
| Wide, round-tipped, tapered diamond (fine grit) (1.2 mm) | Finishing |
| Utility wax and wax caliper | Verification of occlusal clearance |
| Occlusal reduction gauge | |
| High- and low-speed friction grip contra-angles |
Step-by-Step Procedure
In this chapter, the tooth preparation steps have been illustrated for a mandibular second molar. Depending on the tooth to be prepared (e.g., a premolar versus a molar) the exact number of guiding grooves may vary. The recommended sequence remains identical, however.
Guiding grooves for occlusal reduction
A tapered carbide or a narrow, tapered diamond is recommended for placing the guiding grooves for occlusal reduction.*
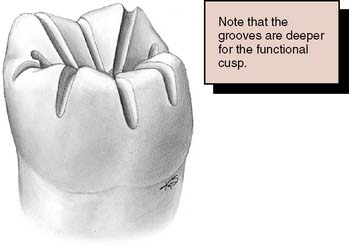
Fig. 8-8 Guiding grooves are placed on the occlusal surface. They are deeper on the functional cusp, and for the functional cusp bevel they diminish in depth from the cusp tip to the cervical margin.
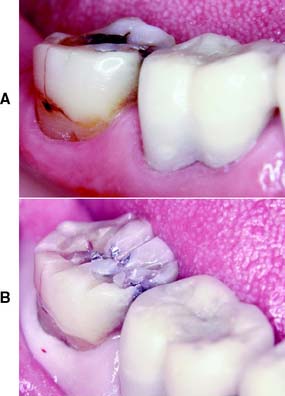
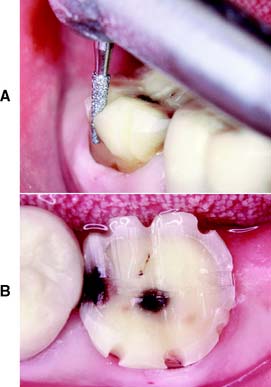
Fig. 8-9 A, A complete cast crown is indicated on this mandibular second molar with occlusal, proximal, and cervical lesions, as well as a buccal longitudinal fracture. B, Initial depth grooves placed for occlusal reduction. Note that they have not yet been extended onto the buccal surface, where the functional cusp bevel will be placed.
Occlusal reduction
Once the guiding grooves have been deemed satisfactory, the tooth structure that remains between the grooves is removed with the carbide or the narrow, round-end, tapered diamond. Proper placement of the grooves automatically results in adequate occlusal clearance.
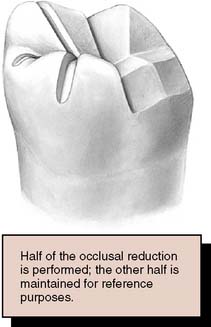
Fig. 8-10 After the guiding grooves are placed, the occlusal reduction is performed. Either the mesial or the distal half is maintained initially as a reference.

Fig. 8-11 A, Note the angulation of the bur as the functional cusp bevel is placed. B, Completed occlusal reduction. Note that it follows normal occlusal form. Three distinct planes can be seen buccolingually.
Alignment grooves for axial reduction
After the occlusal reduction is completed, three alignment grooves are placed in each buccal and lingual wall with a narrow, round-end, tapered diamond. One is placed in the center of the wall, and one in each mesial and distal transitional line angle (Fig. 8-14).
Axial reduction
The technique for axial reduction is similar to that for occlusal reduction. The remaining islands of tooth structure between the alignment grooves are removed while the chamfer margin is being placed, and the same narrow, round-tipped diamond is used for the procedure (Figs. 8-16 and 8-17).

Fig. 8-16 If axial reduction is completed first on either the distal or the mesial half of the tooth, evaluation is simplified because the remaining intact tooth can serve as a reference.
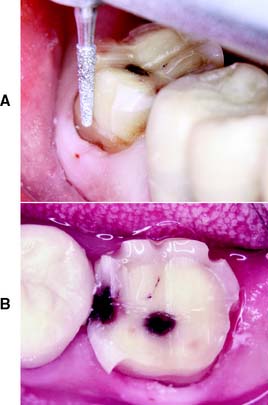
Fig. 8-17 A, Note the alignment of the diamond as tooth structure between the alignment grooves is removed. B, Axial reduction. The distobuccal axial reduction has been completed.

Fig. 8-18 A, As the mesiobuccal axial reduction is performed, a cervical chamfer is placed. B, Make the chamfer of relatively even width and maintain the somewhat angular preparation outline form to maximize resistance form.
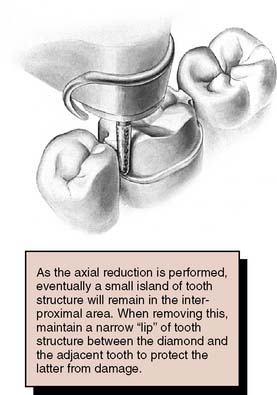
Typically, if the proper cervical placement of the margin has been selected with proper axial alignment of the instrument, a lip of tooth enamel is maintained between the diamond and the adjacent tooth that protects it from any damage (Fig. 8-19).

Finishing
A smooth surface finish and continuity of all prepared surfaces aid most phases of fabrication of the restoration. Smooth transitions from occlusal to axial surfaces facilitate impression making, waxing, investing, and casting because bubble formation is reduced (Fig. 8-22).

Fig. 8-22 A, The transition from lingual to occlusal surfaces is rounded with a fine-grit diamond. B, All sharp line angles between occlusal reduction and functional cusp bevel are similarly rounded. C, The margin is refined, and any minor irregularities are removed.
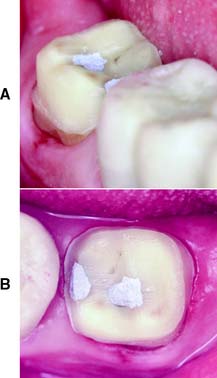
Fig. 8-23 Completed preparation. The carious lesions have been excavated and the resulting irregularities blocked out with amalgam. A, Buccal appearance. B, Occlusal appearance.
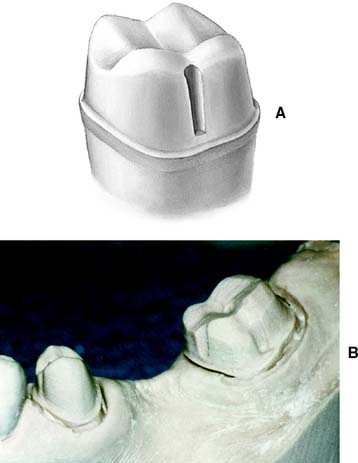
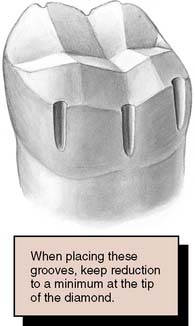
Fig. 8-24 A, When opposing axial walls are excessively tapered, internal features such as this buccal groove can be used to improve retention and resistance form. B, Mesially tipped molars and short premolars often benefit from grooves and/or boxes incorporated in the preparation design.
The criteria used to determine the need for such features to enhance retention and resistance are described in Chapter 7.
Evaluation
Upon completion, the preparation is evaluated to assess whether all the criteria have been fulfilled (Fig. 8-25).

Fig. 8-25 The completed preparation is characterized by a smooth, even chamfer; a 6-degree taper; and gradual transitions between all prepared surfaces.
One of the more common errors in complete cast crown preparations is overtapering of the opposing axial walls. This significantly reduces the retention of the completed restoration. If a tooth preparation has been inadvertently overreduced through excessive tapering of axial walls, it should be carefully evaluated to determine how it can be corrected. If a band of several millimeters of tooth structure can be prepared circumferentially with a restricted taper of approximately 6 degrees, it is probably unnecessary to modify the preparation further to compensate for areas of excessive reduction in the occlusal third. If this is not the case, an approach slightly less conservative of tooth structure may be warranted: (1) uprighting overtapered axial walls to obtain the mechanical advantage of increased retention or (2) using grooves, boxes, or pinholes as needed.
No undercuts between any opposing axial walls can be accepted. When the diamond is placed against the axial surface of the prepared tooth, parallel to the path of placement, it should be possible to move the instrument around the tooth so that the entire height of the preparation is touching the diamond at all times. The tip of the diamond should rest on the chamfer throughout this movement, and no light should be visible between the instrument and the axial surface.
Finally, occlusal and proximal clearances are assessed. They should be adjusted if inadequate provision has been made for the restorative material. Any problems must be corrected before making the interim restoration (Fig. 8-26) and the impression.
SUMMARY
The complete cast crown, an all-metal restoration often used on single posterior teeth as a retainer for a fixed dental prosthesis, provides greater retention and resistance than any other type of restoration. It is not indicated for every restorative circumstance, however. It is unnecessary if the buccal and/or lingual walls of a tooth are intact or if less than maximum retention is needed. The rather extensive removal of tooth structure required in its preparation can have adverse pulpal and periodontal effects. The high strength of the complete cast crown makes it especially suitable for restoring an endodontically treated tooth, although in patients who find visible metal a significant drawback, the metal-ceramic or a more conservative partial-coverage restoration may be preferred.
A well-organized approach to preparation for a complete cast crown should be based on the selective use of guiding grooves of predetermined depth correlated with specific properties of the restorative material. Adequate occlusal reduction is necessary, in accordance with the normal anatomic tooth contours, and the axial reduction should also conform to the normal configuration of the tooth, with minimum taper (6 degrees). Under no circumstances should undercuts remain in the proximal walls. These must be removed by additional tooth preparation or blocked out with a suitable base material. The chamfer is the margin of choice for a complete cast crown. It should be distinct and of adequate width. No unsupported enamel can be permitted. Occlusocervically, the margin should be supragingival, and it should be smooth and continuous mesiodistally. When assessing the adequacy of the chamfer, the examiner should be able to feel distinct resistance against vertical displacement by an explorer or periodontal probe.
SUMMARY CHART
COMPLETE CAST CROWN
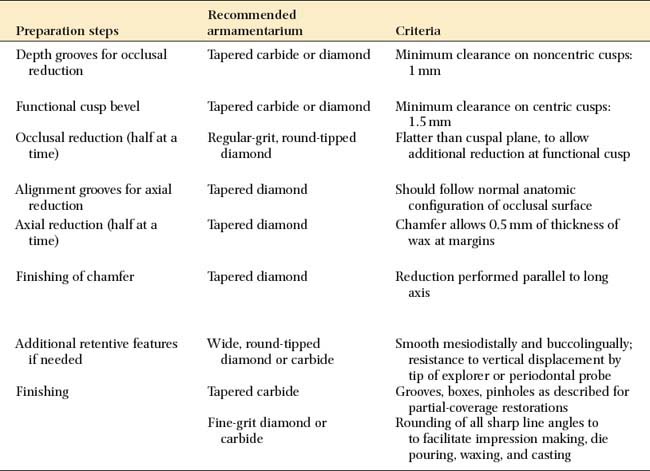
| Preparation steps | Recommended armamentarium | Criteria |
|---|---|---|
| Depth grooves for occlusal reduction | Tapered carbide or diamond | Minimum clearance on noncentric cusps: 1 mm |
| Functional cusp bevel | Tapered carbide or diamond | Minimum clearance on centric cusps: 1.5 mm |
| Occlusal reduction (half at a time) | Regular-grit, round-tipped diamond | Flatter than cuspal plane, to allow additional reduction at functional cusp |
| Alignment grooves for axial reduction | Tapered diamond | Should follow normal anatomic configuration of occlusal surface |
| Axial reduction (half at a time) | Tapered diamond | Chamfer allows 0.5 mm of thickness of wax at margins |
| Finishing of chamfer | Tapered diamond | Reduction performed parallel to long axis |
| Additional retentive features if needed | Wide, round-tipped diamond or carbide | Smooth mesiodistally and buccolingually; resistance to vertical displacement by tip of explorer or periodontal probe |
| Finishing | Tapered carbide | Grooves, boxes, pinholes as described for partial-coverage restorations |
| Fine-grit diamond or carbide | Rounding of all sharp line angles to to facilitate impression making, die pouring, waxing, and casting |