3 TREATMENT PLANNING
Treatment planning consists of formulating a logical sequence of treatment designed to restore the patient’s dentition to good health, with optimal function and appearance. The plan should be presented in written form and should be discussed in detail with the patient. Good communication with the patient is essential when the plan is formulated. Most dental disorders can be corrected with several different procedures; the patient’s preferences are paramount in establishing a suitable treatment plan. An appropriate plan informs the patient about the current conditions, the extent of dental treatment proposed, the time and cost of treatment, and the level of home care and professional follow-up needed for success. In addition, before any irreversible procedures are undertaken, the patient should understand that some details may need to be altered during the course of treatment.
This chapter outlines the decisions that are necessary in planning treatment for fixed prosthodontics. Foremost among these is the identification of patients’ needs and their preferences, which must be correlated with the range of treatments available. For long-term success, when a fixed dental prosthesis (FDP) is being considered, the abutment teeth must be carefully assessed. Finally, the treatment plan must be properly sequenced as part of an ongoing program of comprehensive dental care.
IDENTIFICATION OF PATIENT NEEDS
Successful treatment planning is based on proper identification of the patient’s needs. If an attempt is made to have the patient conform to the “ideal” treatment plan rather than have the treatment plan conform to the patient’s needs, success is unlikely. Frequently, several treatment plans are presented and discussed, each with advantages and disadvantages. Indeed, failing to explain and present alternatives may be considered legally negligent.
Treatment is necessary to accomplish one or more of the following objectives: correcting an existing disease, preventing future disease, restoring function, and improving appearance.
Correction of Existing Disease
Existing disease is revealed during the clinical examination. The disease process can usually be arrested by identification and reduction of the initiating factors, identification and improvement of the resistive factors, or both (Fig. 3-1). For example, oral hygiene instruction helps reduce the amount of residual plaque, an initiating factor, and thus helps reduce the likelihood of further dental caries. It also helps improve gingival health, and the resulting healthy tissue is more resistant to disease.

Additional fluoride intake (e.g., mouth rinses) is also recommended in a patient with a caries problem. Restorative care replaces damaged or missing tooth structure, but additional treatment is essential for controlling the disease that caused the damage.
Prevention of Future Disease
The likelihood of future disease can be predicted by evaluating the patient’s disease experience and by knowing the prevalence of the disease in the general population. Treatment should be proposed if future disease seems likely in the absence of such intervention.
Restoration of Function
Although objective measurement may be difficult, the level of function is assessed during the examination. Treatment may be proposed to correct impaired function (e.g., mastication or speech).
Improvement of Appearance
Patients often seek dental treatment because they are dissatisfied with their appearance. However, it is difficult to objectively assess dental esthetics. The dentist should develop expertise in this area and should be prepared to appraise the appearance of the patient’s dentition and listen carefully to the patient’s views. If the appearance is far outside socially accepted values, the feasibility of corrective procedures should be brought to the patient’s attention. Long-term dental health should not be compromised by unwise attempts to improve appearance. Patients should always be made aware of the possible adverse consequences of treatment.
AVAILABLE MATERIALS AND TECHNIQUES
All existing restorative materials and techniques have limitations and cannot exactly match the properties of natural tooth structure. Before the clinician selects the appropriate procedure, he or she should understand these limitations. This helps prevent an experimental approach to treatment.
Plastic Materials
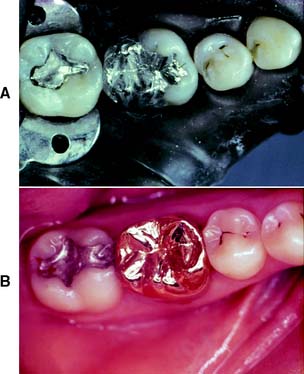
Plastic materials (e.g., silver amalgam or composite resin) are the most commonly used dental restoratives. They allow simple and conservative restoration of damaged teeth. However, their mechanical properties are inferior to those of cast metal or metal-ceramic restorations. Their continued service depends on the strength and integrity of the remaining tooth structure. When the remaining tooth substance needs reinforcement, a cast metal restoration should be fabricated, usually with amalgam as the foundation or core (see Chapter 6).
Large amalgam restorations (Fig. 3-2A) are shaped or carved directly in the mouth. The great degree of difficulty associated with this direct approach often results in defective contours and poor occlusion. The indirect procedure, used in making cast metal crowns (Fig. 3-2B), facili-tates the fabrication of more accurately shaped restorations.
Cast Metal
Cast metal crowns are fabricated outside the mouth and are cemented with a luting agent. To minimize exposure of the luting agent to oral fluids, a long-lasting restoration must have good marginal adaptation. The highly refined techniques for overcoming the problem of marginal fit also permit the manufacture of cast metal crowns with precisely shaped axial and occlusal surfaces. This ensures continued periodontal health and good occlusal function. The internal dimensions of a casting must seat without binding against the walls while remaining stable and not becoming displaced during function. Preparation design for cast metal restorations is crucial and is discussed in detail in Chapter 7, Chapter 8, Chapter 9 and Chapter 10.
Intracoronal restorations
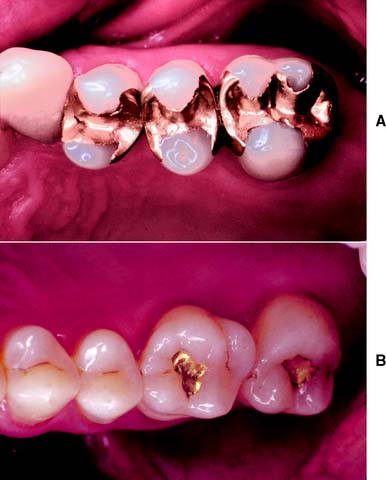
An intracoronal cast metal restoration (Fig. 3-3), or inlay, relies on the strength of the remaining tooth structure for support and retention, just as a plastic restoration does. However, greater tooth bulk is needed to resist any wedging effect on the preparation walls. Therefore, this restoration is contraindicated in a significantly weakened tooth. When fabricated correctly, it is extremely durable because of the strength and corrosion resistance of the gold casting alloy; in a tooth with a minimal proximal carious lesion, however, it usually requires greater removal of tooth structure than does an amalgam preparation. Inlays do not have sufficient resistance or retention to be used as abutment retainers for FDPs.
Extracoronal restorations
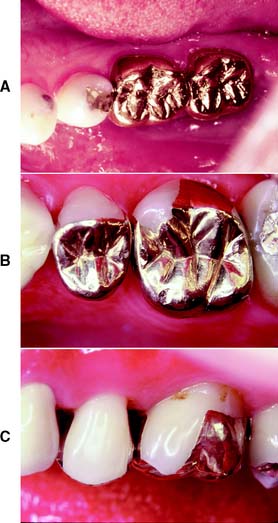
An extracoronal cast metal restoration (Fig. 3-4), or crown, encircles all or part of the remaining tooth structure. As such, it can strengthen and protect a tooth weakened by caries or trauma. To provide the necessary bulk of material for strength, considerably more tooth structure must be removed than for an intracoronal restoration. The margins of an extracoronal restoration often must be near the free gingiva, which can make maintenance of tissue health difficult. Tooth preparation for an extracoronal restoration may be combined with intracoronal features (e.g., grooves and pinholes) to gain resistance and retention.
Metal-Ceramic
Metal-ceramic restorations (Fig. 3-5) consist of a tooth-colored layer of porcelain bonded to a cast metal substructure. They are used when a complete crown is needed to restore appearance as well as function. Sufficient reduction of tooth structure is necessary to provide space for the bulk of porcelain needed for a natural appearance. Thus, the preparation design for a metal-ceramic crown is among the least conservative, although tooth structure can be conserved if only the most visible part of the restoration is veneered.
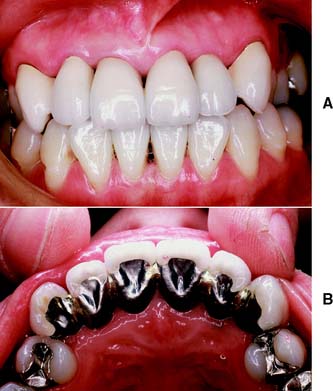
The labial margins of a metal-ceramic restoration are often discernible and may detract from its appearance. They can be hidden by subgingival placement, although they then have the potential for increasing gingival inflammation; this should be avoided when possible.1 Appearance can be improved by omitting the metal shoulder and making the labial margin in porcelain. As discussed in Chapter 24, this is a more demanding laboratory procedure.
Resin-Veneered
Resin-veneered restorations were popular before the metal-ceramic technique was fully developed, but problems with wear and discoloration of the polymethyl methacrylate veneer (Fig. 3-6) limited their use to long-term interim restorations. Current resin-veneer techniques2 incorporate bis-GMA–based materials (bisphenol-A glycidyl dimethacrylates), which have better physical properties than do the earlier acrylic resins, and adhesive techniques to improve the bond to the supporting metal.3,4

Fiber-Reinforced Resin
Advances in composite resin technology, especially the introduction of glass and polyethylene fibers,5-7 have prompted the use of indirect composite resin restorations for inlays, crowns, and FDPs. Excellent marginal adaptation and esthetic results are achievable (Fig. 3-7), but because these are newer technologies, little is known about their longer-term performance (see Chapter 27).

Complete Ceramic
Crowns, inlays, and laminate veneers made entirely of dental porcelain can be the most esthetically pleasing of all fixed restorations (Fig. 3-8). Drawbacks include a comparative lack of strength and the difficulties associated with achieving an acceptable marginal fit. The current focus in improving strength lies with either veneering a high-strength alumina, zirconia, spinel, or lithium disilicate core8-10 with a more translucent porcelain or using a leucite-reinforced translucent material11-13 (see Chapter 25). Complete ceramic restorations are fabricated by an indirect technique and generally retained with composite resin. Acid etching is used to provide retention “keys.”

Fixed Dental Prostheses
An FDP (Fig. 3-9) is often indicated when one or more teeth require removal or are missing. Such teeth are replaced by pontics that are designed to fulfill the functional and often the esthetic requirements of the missing teeth (see Chapter 20). Pontics are connected to retainers, which are the restorations on prepared abutment teeth.
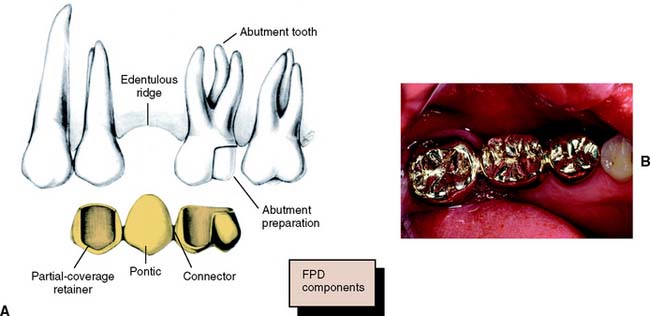
Fig. 3-9 A, A three-unit fixed dental prosthesis showing the main components. B, The pontic rigidly attached to crowns on the abutment teeth. The connectors should occupy the normal interproximal contact area and be large enough for strength but not so large as to impede plaque control.
All the components of an FDP are fabricated and assembled in the laboratory before cementation in the mouth. This requires precise alignment of tooth preparations. Because unseating forces on individual retainers can be considerable, highly retentive restorations are essential. FDPs have been demonstrated to have exceptional long-term success,14 which is ensured by controlling the magnitude and direction of forces and by making sure the patient practices appropriate oral hygiene measures.
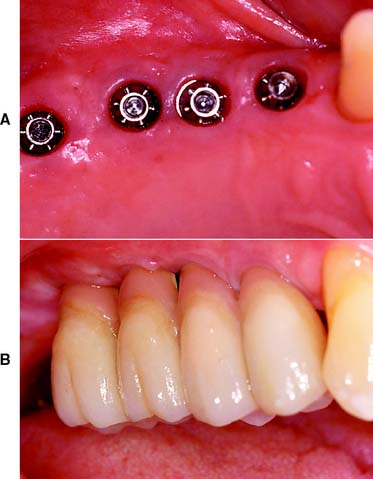
Implant-Supported Prostheses
Single or multiple missing teeth can be replaced with an implant-supported prosthesis (Fig. 3-10). For the successful “osseointegrated” technique, the bone is atraumatically drilled to receive precisely fitting titanium cylinders.15 These are left in place without loading for some months until they are invested with bone. Only then are function and esthetics restored with a prosthesis (see Chapter 13).
Partial Removable Dental Prosthesis
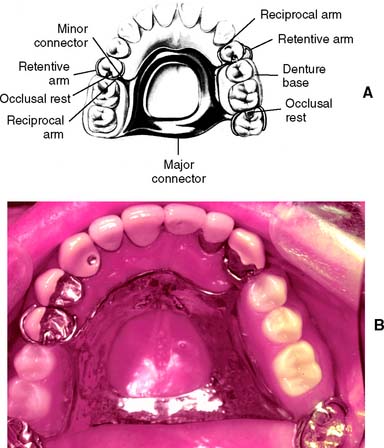
A partial removable dental prosthesis (RDP) (Fig. 3-11) is designed to replace missing teeth and their supporting structures. Forces applied to a well-designed prosthesis are distributed to the remaining teeth and the residual alveolar ridges. These forces are most accurately controlled if the abutment teeth are provided with fixed cast restorations that have carefully contoured guide planes and rest seats (see Chapter 21).
Complete Dentures
Some of the difficulties encountered with complete dentures relate to the lack of denture stability and a gradual loss of supporting bone. Stability is enhanced if the denture has a carefully designed occlusion. Problems with stability can be especially severe when the mandibular incisors are the only teeth retained, with ensuing damage to the opposing premaxilla,16 although any treatment plan that involves a complete denture opposing fixed restorations requires careful planning of the occlusion (Fig. 3-12). For selected patients, providing an overdenture that rests on endodontically treated roots may help preserve the residual ridge and enhance the stability of the complete denture.17
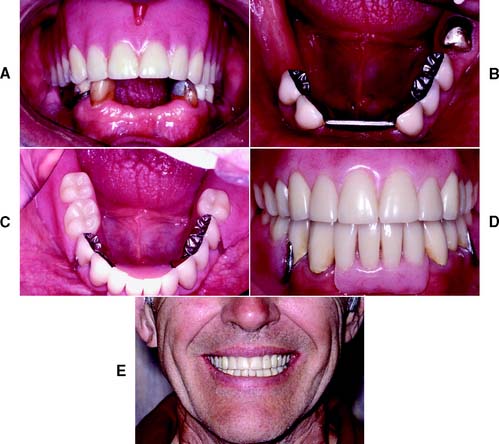
Fig. 3-12 Special planning is required when a combination of a complete maxillary denture is planned opposing a fixed mandibular prosthesis. In general, a trial maxillary denture is indicated so the fixed prosthesis can be fabricated to a well-aligned occlusal plane. A, Preoperative appearance. B to E, Completed restoration.
(Courtesy of Dr. J. A. Holloway.)
TREATMENT OF TOOTH LOSS
A treatment plan involving fixed prosthodontics generally includes the replacement of missing teeth. Most teeth are lost as a result of dental caries or periodontal disease. In rare cases, they may be congenitally absent or lost as a result of trauma or neoplastic disease.
Decision to Remove a Tooth
The decision to remove a tooth is part of the treatment-planning process and is made after assessing the advantages and disadvantages associated with retention of the tooth. Sometimes it is possible to retain a tooth with an apparently hopeless prognosis by using highly specialized and complex techniques. In other cases, removing the tooth is the treatment of choice (Fig. 3-13). A decision about replacing a missing tooth is best made at the time its removal is recommended, rather than months or years after the fact.

Consequences of Removal without Replacement
The decision to replace or not replace missing teeth requires a careful analysis of the costs and benefits of the action. The loss of posterior occlusion may lead to excessive forces on the remaining dentition with consequent damage and poor function. However, studies have demonstrated that adequate function is possible with reduced posterior occlusion.18 Deciding not to replace a tooth may lead to a situation in which the balance of the forces exerted on that tooth by the adjacent and opposing teeth and supporting tissues and by the soft tissues of the cheeks, lips, and tongue is upset (Fig. 3-14). The consequences may be supraclusion of the opposing tooth or teeth, tilting of the adjacent teeth, and loss of proximal contact (with resulting disturbances in the health of the supporting structures and the occlusion). However, the teeth adjacent to an edentulous space have not been shown to be at greater risk of damage,19 and the rate of change of teeth adjacent to an edentulous space is usually slow.20
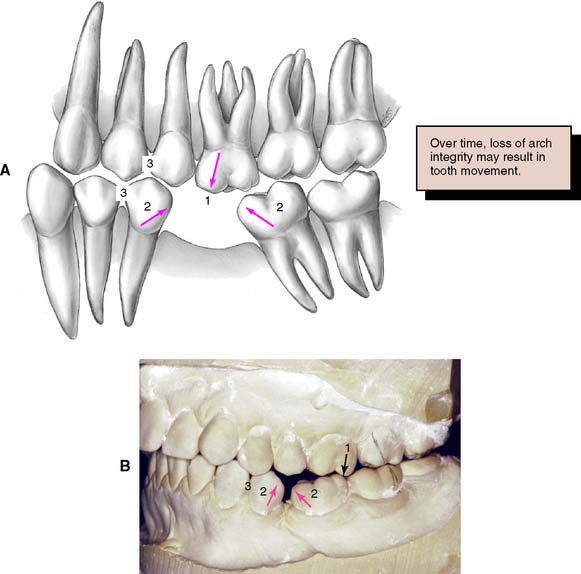
Fig. 3-14 Loss of a mandibular first molar not replaced with a fixed dental prosthesis. The typical consequences are supraclusion of opposing teeth (1), tilting of adjacent teeth (2), and loss of proximal contacts (3).
(A, Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
However, if the situation is not carefully monitored and significant movement of adjacent teeth has occurred, simple replacement of the missing tooth at this late stage may prevent further disruption, although it may be insufficient to return the dentition to full health. Extended treatment plans, including orthodontic repositioning and additional cast restorations (to correct the disturbed occlusal plane), may be needed to compensate for the lack of treatment at the time of tooth removal.
SELECTION OF ABUTMENT TEETH
Whenever possible, FDPs should be designed as simply as possible, with a single well-anchored retainer fixed rigidly at each end of the pontic. The use of multiple splinted abutment teeth, nonrigid connectors, or intermediate abutments makes the procedure much more difficult, and often the result compromises the long-term prognosis (Fig. 3-15).

Fig. 3-15 A to C, Congenitally missing lateral incisors replaced with two simple three-unit fixed dental prostheses. D to F, This patient had a missing canine as well as two congenitally missing laterals. Here, there is a much greater restorative challenge than in part A, necessitating an eight-unit prosthesis.
Replacement of a Single Missing Tooth
Unless bone support has been weakened by advanced periodontal disease, a single missing tooth can almost always be replaced by a three-unit FDP that includes one mesial and one distal abutment tooth. An exception is when the FDP is replacing a maxillary or mandibular canine. Under these circumstances, the small anterior abutment tooth needs to be splinted to the central incisor to prevent lateral drift of the FDP.
Cantilever fixed dental prostheses
FDPs in which only one side of the pontic is attached to a retainer are referred to as cantilevered. An example would be a lateral incisor pontic attached only to an extracoronal metal-ceramic retainer on a canine. Cantilevered FDPs remain popular because some of the difficulties encountered in making a three-unit FDP are lessened. Also, many clinicians are reluctant to prepare an intact central incisor, preferring instead to use a cantilever.
However, the long-term prognosis of the single-abutment cantilever is poor.21 Forces are best tolerated by the periodontal supporting structures when directed in the long axes of the teeth.22 This is the case when a simple three-unit FDP is used. A cantilever induces lateral forces on the supporting tissues, which may be harmful and lead to tipping, rotation, or drifting of the abutment (Fig. 3-16). Laboratory analysis23,24 has confirmed the potential harmful nature of such FDPs. However, clinical experience with resin-retained FDPs has suggested that cantilever designs may be preferred, especially because re-adhesion after failure is greatly facilitated25 (see Chapter 26).
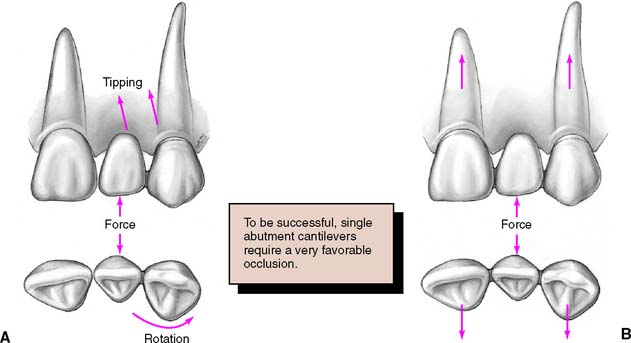
Fig. 3-16 A, Forces applied to a cantilever fixed dental prosthesis are resisted on only one side, leading to imbalance. Vertical forces can cause tipping, and horizontal forces, rotation, of abutment teeth. B, By including both adjacent teeth in the prosthesis, it is possible to resist forces much better since the teeth have to be moved bodily rather than merely rotated or tipped.
(Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
When multiple missing teeth are replaced, cantilever FDPs have considerable application (see Fig. 3-20). The harmful tipping forces are resisted by multiple abutment teeth, and movement of the abutments is unlikely. Cantilevers are also successfully used with implant-supported prostheses (see Chapter 13).
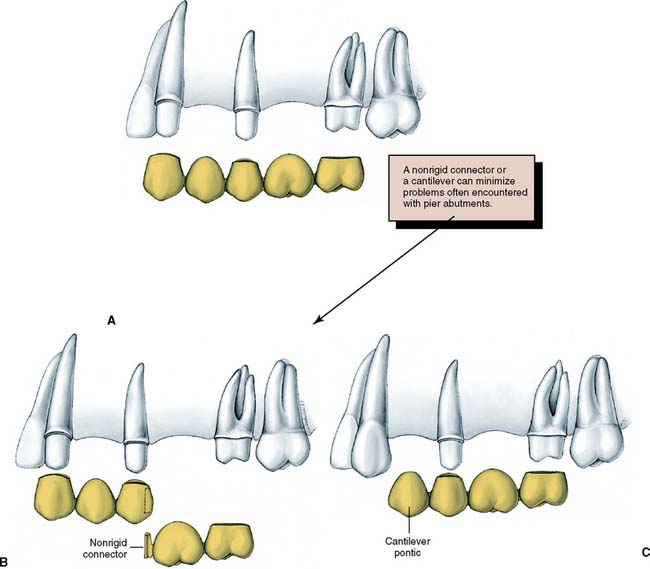
Fig. 3-20 A, A five-unit fixed dental prosthesis (FDP) replacing the maxillary first molar and first premolar. The middle abutment can act as a fulcrum during function, with possible unseating of one of the other retainers. To be successful, this type of FDP needs extremely retentive retainers. B, An alternative approach is a nonrigid dovetail connector between the molar pontic and the second premolar. C, Where periodontal support is adequate, a much simpler approach would be to cantilever the first premolar pontic.
(Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
Assessment of abutment teeth
Considerable time and expense are spared, and loss of a patient’s confidence can be avoided, by thoroughly investigating each abutment tooth before proceeding with tooth preparation. Radiographs are made, and pulpal health is assessed by evaluating the response to thermal and electrical stimulation. Existing restorations, cavity liners, and residual caries are removed26 (preferably under a rubber dam), and a careful check is made for possible pulpal exposure. Teeth in which pulpal health is doubtful should be endodontically treated before the initiation of fixed prosthodontics. Although a direct pulp cap may be an acceptable risk for a simple amalgam or composite resin, conventional endodontic treatment is normally preferred for cast restorations, especially when the later need for endodontic treatment would jeopardize the overall success of treatment.
Endodontically treated abutments
If a tooth is properly treated endodontically, it can serve well as an abutment with a post and core foundation for retention and strength (see Chapter 12). Failures occur, however, particularly on teeth with short roots or little remaining coronal tooth structure. Care is needed to obtain maximum retention for the post and core. Sometimes it is better to recommend removal of a badly damaged tooth rather than to attempt endodontic treatment.
Unrestored abutments
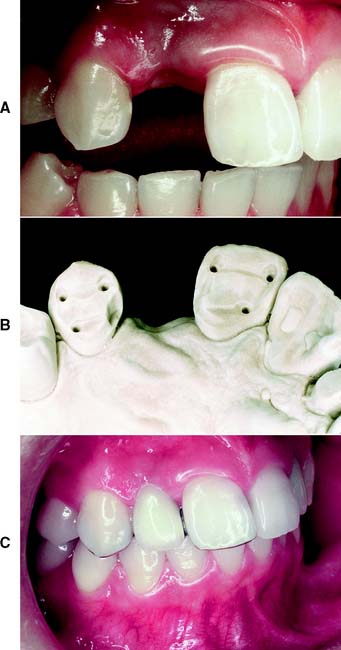
An unrestored, caries-free tooth is an ideal abutment. It can be prepared conservatively for a strong retentive restoration with optimum esthetics (Fig. 3-17). The margin of the retainer can be placed without modifications to accommodate existing restorations or caries. In an adult patient, an unrestored tooth can be safely prepared without jeopardizing the pulp as long as the design and technique of tooth preparation are wisely chosen. Certain patients are reluctant to have a perfectly sound tooth cut down to provide anchorage for an FDP. In these cases, the overall dental health of the patient, rather than the condition of each individual tooth, should be emphasized.
Mesially tilted second molar
Loss of a permanent mandibular first molar to caries early in life is still relatively common (Fig. 3-18). If the space is ignored, the second molar may tilt mesially, especially with eruption of the third molar. It then becomes difficult or impossible to make a satisfactory FDP, because the positional relationship no longer allows for parallel paths of insertion without interference from the adjacent teeth.
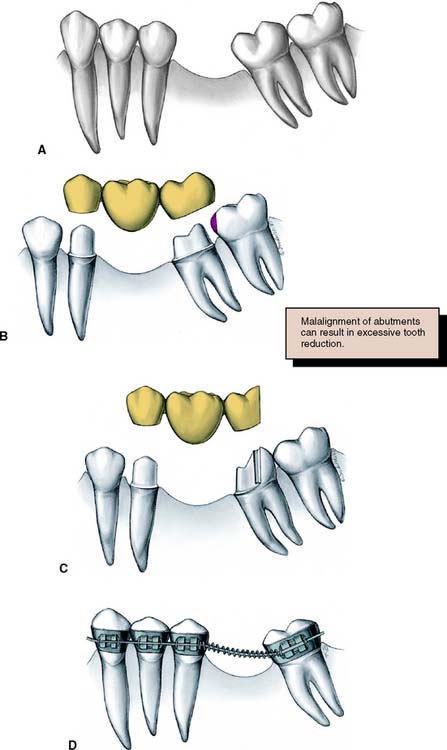
Fig. 3-18 A, Early loss of a mandibular first molar with mesial tilting and drifting of the second and third molars. B, A conventional three-unit fixed dental prosthesis will fail because its seating is prevented by the third molar. C, A modified preparation design can be used on the distal abutment. D, A better treatment plan would be to remove the third molar and upright the second molar orthodontically before fabricating a fixed dental prosthesis.
(Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
In such circumstances, an FDP is sometimes made with modified preparation designs or with a nonrigid connector, or a straightforward solution27 may be considered: uprighting the tilted abutment orthodontically with a simple fixed appliance. However, the problem can be avoided altogether if a space-maintainer appliance (Fig. 3-19) is fabricated when the first molar is removed. This device may be as simple as a square section of orthodontic wire bent to follow the edentulous ridge and anchored with small restorations in adjacent teeth.

Fig. 3-19 Square section orthodontic wire can be used as a simple stabilizing appliance to prevent drifting of abutment teeth after exodontia. The wire is retained by placing small restorations. As an alternative, orthodontic bands can be used as the retainer. Note that these simple stabilizers do not prevent supraeruption of opposing teeth; in areas where this is anticipated, a provisional fixed dental prosthesis is needed.
Replacement of Several Missing Teeth
Fixed prosthodontics becomes more difficult when several teeth must be replaced. Problems are encountered in restoring a single long, uninterrupted edentulous area or multiple edentulous areas with intermediate abutment teeth (Fig. 3-20), especially when anterior and posterior teeth are to be replaced with a single fixed prosthesis. Underestimation of the problems involved in extensive prosthodontics can lead to failure. One key to ensuring a successful result is to plan the prostheses by waxing the intended restorations on articulated diagnostic casts. This is essential for complex fixed prosthodontic treatments, particularly when an irregular occlusal plane is to be corrected, the occlusal vertical dimension is to be altered, an implant-supported prosthesis is recommended, or a combination of fixed and removable prostheses are to be used. The precise end point of such complicated treatments can be far from evident, even to an experienced prosthodontist (see Fig. 2-39).
Overloading of abutment teeth
The ability of the abutment teeth to accept applied forces without drifting or becoming mobile must be estimated and has a direct influence on the prosthodontic treatment plan. These forces can be particularly severe during parafunctional grinding and clenching (see Chapter 4), and the need to eliminate them becomes obvious during the restoration of such a damaged dentition. Although it is hoped that a well-reconstructed occlusion will reduce the duration and strength of any parafunctional activity, there is little scientific evidence to support this. It is unwise to initiate treatment on the assumption that new restorations will reduce parafunctional activity, unless this has been demonstrated with treatment appliances over a significant period.28
Direction of forces
Whereas the magnitude of any applied force is difficult to regulate, a well-fabricated FDP can distribute these forces in the most favorable way, directing them in the long axis of the abutment teeth. Potentially damaging lateral forces can be confined to the anterior teeth, where they are reduced by the longer lever arm (see Chapter 4).
Root surface area
The root surface area of potential abutment teeth must be assessed when treatment for fixed prosthodontics is planned. Ante29 suggested in 1926 that it was unwise to provide an FDP when the root surface area of the abutment was less than the root surface area of the teeth being replaced; this has been adopted and reinforced by other authors30-32 as Ante’s law. Average values for the root surface area of permanent teeth are given in Table 3-1.33 As an example of Ante’s law, consider the patient who has lost a first molar and second premolar (Fig. 3-21). In this situation, a four-unit FDP is an acceptable risk, as long as there has been no bone loss from periodontal disease, because the second molar and first premolar abutments have root surface areas approximately equal to those of the missing teeth. If the first molar and both premolars are missing, however, an FDP is not considered a good risk because the missing teeth have a greater total root surface area than the potential abutments.
Table 3-1 ROOT SURFACE AREA OF ABUTMENT
| Root Surface Area (mm2) | Percentage Root Surface Area in Quadrant | |
|---|---|---|
| MAXILLARY | ||
| Central | 204 | 10 |
| Lateral | 179 | 9 |
| Canine | 273 | 14 |
| First premolar | 234 | 12 |
| Second premolar | 220 | 11 |
| First molar | 433 | 22 |
| Second molar | 431 | 22 |
| MANDIBULAR | ||
| Central | 154 | 8 |
| Lateral | 168 | 9 |
| Canine | 268 | 15 |
| First premolar | 180 | 10 |
| Second premolar | 207 | 11 |
| First molar | 431 | 24 |
| Second molar | 426 | 23 |
Data from Jepsen A: Root surface measurement and a method for x-ray determination of root surface area. Acta Odontol Scand 21:35, 1963.
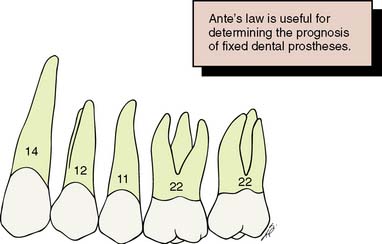
Fig. 3-21 To assess the support of a fixed dental prosthesis (FDP), Ante’s law has been invoked.
It proposes a relationship between the root surface areas of the missing teeth and those of the potential abutment teeth. (The numbers represent root surface area percentages.) If the first molar (22) and second premolar (11) are missing, the abutments for a four-unit FDP have a slightly greater total root surface area (34) than do the teeth being replaced. In that case, in the absence of other detrimental factors, an FDP’s prognosis is favorable. However, if the first premolar (12) is also missing, the loss of potential abutment root surface area comprises 45, whereas the remaining abutments have only 36, which is much less favorable.
Nyman and Ericsson,34 however, cast doubt on the validity of Ante’s law by demonstrating that teeth with considerably reduced bone support can be successfully used as FDP abutments. In the majority of the treatments discussed by these authors, the abutment root surface area was less than half that of the replaced teeth, and there was no loss of attachment after 8 to 11 years. The authors attributed this success to meticulous root planing during the active phase of treatment, proper plaque control during the observed period, and the occlusal design of the prostheses. Other authors have confirmed that abutment teeth with limited periodontal bone can successfully support fixed prostheses.35,36
Root shape and angulation
When tooth support is borderline adequate, the shape of the roots and their angulation should be considered. A molar with divergent roots provides better support than a molar with conical roots and little or no interradicular bone. A single-rooted tooth with an elliptic cross-section offers better support than a tooth with similar root surface area but a circular cross-section. Similarly, a well-aligned tooth provides better support than a tilted one. Alignment can be improved with orthodontic uprighting (Fig. 3-22).
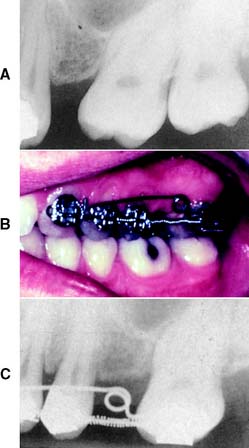
Fig. 3-22 A, A misaligned abutment tooth may be difficult or impossible to prepare for a fixed dental prosthesis abutment and provides poor support. B and C, When possible, this should be corrected with orthodontic treatment before restoration.
(Courtesy of Dr. G. Gruendeman.)
Periodontal disease
After horizontal bone loss from periodontal disease, the periodontal ligament–supported root surface area can be dramatically reduced.37 Because of the conical shape of most roots (Fig. 3-23), when one third of the root length has been exposed, half the supporting area is lost. In addition, the forces applied to the supporting bone are magnified because of the greater leverage associated with the lengthened clinical crown. Thus, potential abutment teeth need very careful assessment when significant bone loss has occurred.
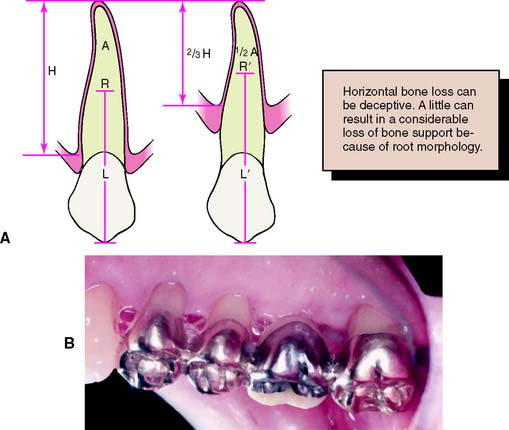
Fig. 3-23 A, Because of the conical shape of most roots, the actual area of support (A) diminishes more than might be expected from the height of the bone (H). In addition, the center of rotation (R) moves apically (R′) and the lever arm (L′) increases, magnifying the forces on the supportive structure. B, A fixed dental prosthesis (FDP) replacing a maxillary first molar. The first premolar is an abutment providing additional stabilization for this FDP on abutment teeth with compromised bone support.
(A, Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
In general, successful fixed prostheses can be fabricated on teeth with severely reduced periodontal support if the periodontal tissues have been returned to excellent health and long-term maintenance has been ensured38,39 (Fig. 3-24). When extensive reconstruction is attempted without complete control over the health of the periodontal tissues, the results can be disastrous.
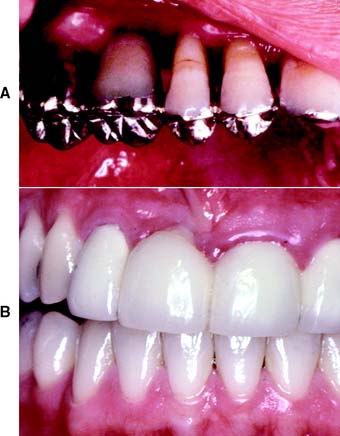
Fig. 3-24 A, Supragingival margins and large gingival embrasures facilitate plaque control in a periodontally compromised patient. B, Poor prosthetic contours and margins have contributed to this failure.
Healthy periodontal tissues are a prerequisite for all fixed restorations. If the abutment teeth have normal bone support, an occasional lapse in plaque removal by the patient is unlikely to affect the long-term prognosis. However, when teeth with severe bone loss resulting from periodontal disease are used as abutments, there is very little tolerance. It then becomes imperative that excellent plaque-removal technique be implemented and maintained at all times.
Span length
Excessive flexing under occlusal loads may cause failure of a long-span FDP (Fig. 3-25). It can lead to fracture of a porcelain veneer, breakage of a connector, loosening of a retainer, or an unfavorable soft tissue response and thus render a prosthesis useless. All FDPs flex slightly when subjected to a load; the longer the span, the greater the flexing. The relationship between deflection and length of span is not simply linear but varies with the cube of the length of the span. Thus, other factors being equal, if a span of a single pontic is deflected a certain amount, a span of two similar pontics will move 8 times as much, and three will move 27 times as much40 (Fig. 3-26).

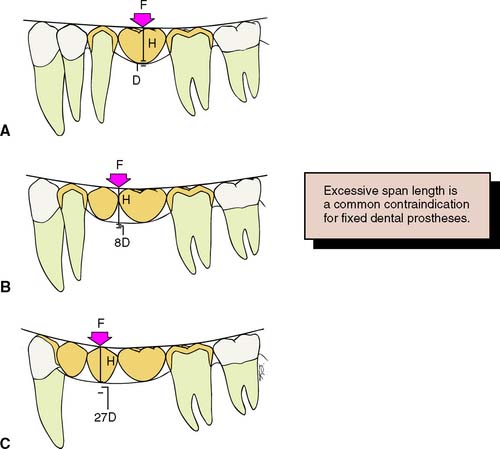
Fig. 3-26 The deflection of a fixed dental prosthesis is proportional to the cube of the length of its span. A, A single pontic deflects a small amount (D) when subjected to a certain force (F). B, Two pontics deflect 23 times as much (8D) to the same force. C, Three pontics deflect 33 times as much (27D).
Replacing three posterior teeth with an FDP rarely has a favorable prognosis, especially in the mandibular arch.41 Under such circumstances, it is usually better to recommend an implant-supported prosthesis or a partial RDP.
When a long-span FDP is fabricated, pontics and connectors should be made as bulky as possible to ensure optimum rigidity without jeopardizing gingival health. In addition, the prosthesis should be made of a material that has high strength and rigidity (see Chapter 19).
Replacing multiple anterior teeth
Special considerations in this situation include problems with appearance and the need to resist laterally directed tipping forces.
The four mandibular incisors can usually be replaced by a simple FDP with retainers on each canine. It is not usually necessary to include the first premolars. If a lone incisor remains, it should be removed because its retention unnecessarily complicates the design and fabrication of the FDP and can jeopardize the long-term result. Mandibular incisors, because of their small size, generally are poor abutment teeth. It is particularly important not to have overcontoured restorations on these teeth, because plaque control is nearly impossible. Thus, the clinician may have to make a choice between (1) compromised esthetics from too thin a ceramic veneer and (2) pulpal exposure during tooth preparation. A third alternative would be selective tooth removal.
The loss of several maxillary incisors presents a much greater problem in terms of restoring appearance and providing support. Because of the curvature of the arch, forces directed against a maxillary incisor pontic tend to tip the abutment teeth. Unlike the mandibular incisors, the maxillary incisors are not positioned in a straight line (particularly in patients with narrow or pointed dental arches). Tipping forces must be resisted by means of two abutment teeth at each end of a long span anterior FDP. Thus, when replacing the four maxillary incisors, the clinician should generally use the canines and first premolars as abutment teeth.42
There may be considerable difficulty in achieving a good appearance when several maxillary incisors are being replaced with an FDP. Obtaining the best tooth contours and position for appearance and phonetics can be a challenge. A good attempt can be made with the diagnostic waxing procedure, evaluating any esthetic problems. As treatment progresses, an interim restoration is provided (see Chapter 15). This may be used to test appearance and phonetics. It may also be readily shaped and modified to suit the patient, and the final restoration can be made as a copy of it, thereby avoiding any embarrassing misunderstandings when the finished fixed prosthesis is delivered.
If anterior bone loss has been severe, as can happen when teeth are lost as a result of trauma or periodontal disease, there may be a ridge defect (Fig. 3-27). In these patients, a partial RDP should be considered, especially when the person has a high smile line, since an FDP generally replaces only the missing tooth structure, not the supporting tissues. Again, an interim restoration may help the patient determine the most appropriate treatment. A surgical ridge augmentation procedure43 may also be an option, although the results can be unpredictable.

Indications for Partial Removable Dental Prostheses
Whenever possible, edentulous spaces should be restored with FDPs rather than partial RDPs. A well-fabricated FDP provides better health and better function than does a partial RDP44 and is preferred by most patients. Under the following circumstances, however, a partial RDP is indicated:

Fig. 3-28 A partial removable dental prosthesis replacing the mandibular right first and second molars.
(Courtesy of Dr. J. A. Holloway.)

Fig. 3-29 Where there has been considerable bone loss, a partial removable dental prosthesis has a more natural appearance than a fixed dental prosthesis.
Multiple edentulous spaces often are best restored with a combination of FDPs and partial RDPs (Fig. 3-30).
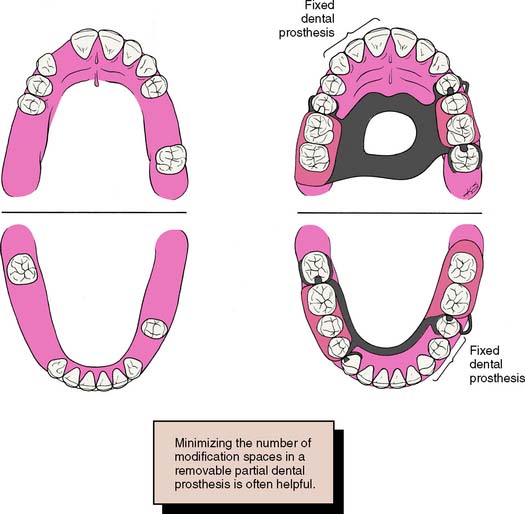
Fig. 3-30 Treatment planning for multiple edentulous spaces. A combination of fixed and removable prostheses may provide the best replacement when several teeth are missing. In the maxillary arch, the missing lateral incisor has been restored with a simple three-unit fixed dental prosthesis (FDP), which is more easily cleaned than is a partial removable dental prosthesis (RDP). In the mandibular arch, the single remaining premolar is splinted to the canine with a three-unit FDP. A partial RDP that fits around a lone-standing premolar usually does not have a good prognosis.
(Redrawn from Rosenstiel SF: Fixed bridgework—the basic principles. In Rayne J, ed: General Dental Treatment, London, Kluwer Publishing, 1983.)
TREATMENT SEQUENCE
When patient needs have been identified and the appropriate corrective measures have been determined, a logical sequence of steps must be decided on, including the treatment of symptoms, stabilization of deteriorating conditions, definitive therapy, and a program of follow-up care. The importance of proper sequencing is emphasized, because mistakes can lead to compromised effort or unnecessary and expensive remakes.
Treatment of Symptoms
The relief of discomfort accompanying an acute condition is a priority in planning treatment (Fig. 3-31). Discomfort can result from one or more of the following: a fractured tooth or teeth, acute pulpitis, acute exacerbation of chronic pulpitis, a dental abscess, acute pericoronitis or gingivitis, and myofascial pain dysfunction.

The clinician needs only sufficient diagnostic information to ascertain the nature of a particular condition and to form a diagnosis; treatment is instituted without delay. A full examination is neither desirable nor generally possible until the symptoms of the acute condition have been addressed.
Urgent treatment of nonacute problems
Fortunately, most potential candidates for fixed prosthodontics do not seek treatment for acute conditions; however, they may have a specific problem that should receive immediate attention, such as a lost anterior crown, a cracked or broken porcelain veneer, or a fractured removable prosthesis (Fig. 3-32).

Stabilization of Deteriorating Conditions
The second phase of treatment involves stabilizing conditions such as dental caries or periodontal disease by removing the etiologic factors, increasing the patient’s resistance, or doing both.
Dental caries
Treatment of carious lesions is approached in a conventional manner, and the teeth are restored with properly contoured plastic materials. These may serve as a foundation for fixed castings during a subsequent phase of treatment (see Chapter 6). However, cast restorations are best avoided in a patient with active caries, because the results of such extensive treatment would be jeopardized by recurrence of the disease. This can be prevented by a combination of dietary advice, oral hygiene measures, and fluoride treatment.
Periodontal disease
Chronic periodontitis with continuing irreversible bone loss should be treated as early as possible by effective daily plaque control. The proper removal of plaque is possible only if the teeth are smooth and their contours allow unimpeded access to the gingival sulci. Therefore, the following procedures are essential (Fig. 3-33):

Definitive Therapy
When the stabilization phase has been completed, successful elective long-term treatment aimed at promoting dental health, restoring function, and improving appearance can begin. On occasion, this takes considerable time. Several therapeutic proposals may be applicable to a single patient and may range in complexity from minimum restorative treatment with regular maintenance to full mouth prosthodontic reconstruction preceded by orthognathic surgery and orthodontic treatment. The advantages and disadvantages of each should be thoroughly explained to the patient, with diagnostic casts and waxings used as guides. When a definitive plan is established, it should attempt to minimize the possibility of having to repeat earlier treatment if problems later occur. Usually oral surgical procedures are scheduled first, followed by periodontics, endodontics, orthodontics, fixed prosthodontics, and finally, removable prosthodontics.
Oral surgery
The treatment plan should allow time for healing and ridge remodeling. Therefore, teeth with a hopeless prognosis, unerupted teeth, and residual roots and root tips should be removed early. All preprosthetic surgical procedures (e.g., ridge contouring) should be undertaken during the early phase of treatment.
Periodontics
Most periodontal procedures should (or will) have been accomplished as part of the stabilization phase of treatment. Any surgery, pocket elimination, mucogingival procedure, guided tissue regeneration, or root resection is performed at this time (see Chapter 5).
Endodontics
Some endodontic treatment may have been accomplished as part of the relief of discomfort and stabilization of conditions. Elective endodontics may be needed to provide adequate space for a cast restoration or to provide retention for a badly damaged or worn tooth.
If a tooth with doubtful pulpal health is to be used as an abutment for an FDP, it should be endodontically treated prophylactically, despite the consideration that periodic recall may be more appropriate treatment if a single restoration is planned.
Orthodontics
Minor orthodontic tooth movement is a common adjunct to fixed prosthodontics. A tooth can be uprighted, rotated, moved laterally, intruded, or extruded to improve its relationship before fixed prosthodontic treatment. Orthodontics should always be considered when a treatment plan is being proposed, especially if tooth loss has been neglected and drifting has occurred.
Fixed prosthodontics
Fixed prosthodontic treatment is initiated only after the preceding modalities have been completed. This allows modification of the original plan if unforeseen difficulties surface during treatment. For example, a tooth scheduled for endodontic treatment might prove to be untreatable, necessitating considerable modification of the restorative treatment plan.
Occlusal adjustment
Occlusal adjustments are often necessary before the initiation of fixed prosthodontics. When extensive fixed prosthodontics is to be provided, an accurate and well-tolerated occlusal relationship may be obtainable only if a discrepancy between maximal intercuspation and centric relation is eliminated first (see Chapter 4). When less extensive treatment is planned, it may be acceptable to modify the fixed prosthesis to conform to the existing occlusion, provided the patient is functioning satisfactorily. However, any supraeruption or drifting should be corrected rather than be allowed to compromise the patient’s occlusal scheme.
Anterior restorations
If both anterior and posterior teeth are to be restored, the anterior teeth are usually restored first because they influence the border movements of the mandible and thus the shape of the occlusal surfaces of the posterior teeth (see Chapter 4). If the posterior teeth are restored first, a subsequent change in the lingual contour of the anterior teeth could require considerable adjustment of the posterior restorations.
Posterior restorations
Restoring opposing posterior segments at the same time is often advantageous. This allows the development of an efficient occlusal scheme through the application of an additive wax technique (see Chapter 18). Treatment of one side of the mouth should be completed before the other side is treated; restoring all four posterior segments at the same time might lead to considerably more complications for the patient and dentist, including fracture or breaking of interim restorations, discomfort with bilateral local anesthesia, and difficulties in confirming the accuracy of jaw relationship recordings.
Complex prosthodontics
Carefully planned treatment sequencing is particularly important when complex prosthodontic treatments involving alteration of the vertical dimension or a combination of fixed and removable prostheses is required. One recommended approach is illustrated in Figure 3-34. Two sets of diagnostic casts are accurately mounted so they can be precisely interchanged on the articulator. One set is prepared and waxed to the intended end point of treatment, with denture teeth inserted where removable prostheses are to be used. The waxing is carefully evaluated on the articulator in relation to occlusion and appearance. When anterior teeth are to be replaced, they can be assessed for appearance and phonetics directly in the mouth if they are mounted on a removable record base. Definitive tooth preparation starts in one arch only, so that the occlusal surfaces of the opposing arch are preserved to act as an essential reference for mounting the definitive cast. The definitive restorations are waxed against the diagnostically waxed cast, which establishes optimal occlusion. When one arch has been completed, the opposing cast can be restored and the predicted result thus achieved.
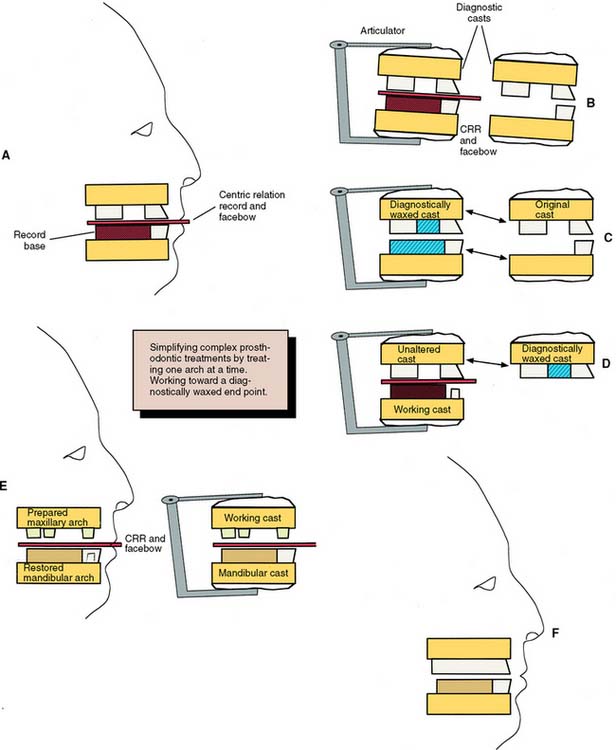
Fig. 3-34 Complex prosthodontic treatment sequence using cross-mounted diagnostic cases. A, Diagnostic impressions, facebow, and centric relation records are made for a patient requiring complex prosthodontic treatment. In this schematic, a record base is needed for mounting the mandibular cast. B, The diagnostic casts are duplicated, and each set is mounted in the identical orientation of an articulator through the use of the facebow and centric record. C, One pair of diagnostic casts is waxed to the proposed end point of treatment. If a removable prosthesis is planned, denture teeth are set for this step. The other pair of casts is left unaltered. D, One arch is treated at a time. For this patient, the mandibular arch has been prepared for crowns. The definitive cast is mounted on the articulator with a centric record made against the (unaltered) maxillary teeth. This record is used to mount the definitive cast against the (unaltered) maxillary cast. Then the maxillary cast is removed and replaced with the cross-mounted diagnostically waxed cast. The mandibular restorations are fabricated against this cast to ensure an optimal occlusal plane. E, Once the mandibular arch has been restored, the maxillary teeth are prepared and mounted against a cast of the newly restored mandibular arch. CRR, centric relation record. F, The completed restoration conforms to the diagnostic waxing.
Follow-Up
A specific program of follow-up care and regular recall is an essential part of the treatment plan. The aim is to monitor dental health, identify the signs of disease early, and initiate prompt corrective measures as necessary (see Chapter 32). Restorations do not last forever, are subject to wear, and may need replacement. Adequate follow-up will help maintain long-term health.
SUMMARY
The basis of logical treatment planning consists of identifying the patient’s needs, eliciting his or her expectations and wishes, and comparing these with the available corrective materials and techniques. It also involves evaluating whether a technique has a good prognosis. Then a rational sequence of treatment may be initiated for symptomatic relief, stabilization, definitive therapy, and follow-up care. The extent of treatment is modified throughout and is dictated by the patient’s attitude and by the objectives for that patient.
 GLOSSARY*
GLOSSARY*
ab·frac·tion \ăb frăk′shun\ n (1991): the pathologic loss of hard tooth substance caused by biomechanical loading forces. Such loss is thought to be due to flexure and chemical fatigue degradation of enamel and/or dentin at some location distant from the actual point of loading—comp ABLATION, ABRASION, ATTRITION, and EROSION
abut·ment \a-bŭt′ment\ n (1634): 1: that part of a structure that directly receives thrust or pressure; an anchorage 2: a tooth, a portion of a tooth, or that portion of a dental implant that serves to support and/or retain a prosthesis—usage see ANGULATED A., HEALING A., DENTAL IMPLANT A., INTERMEDIATE A., ONE PIECE A., PREPARATION PIECE A., STANDARD A., TWO PIECE A.
acrylic resin veneer: usually referring to fixed dental prosthesis, the veneering or lamination of the facial and/or buccal surfaces of a crown or fixed dental prosthesis using acrylic resin. The intention of such veneering is to provide a natural tooth color to the viewable portions of the restoration
acute pain: pain having a brief and relatively severe course
Ante′s Law [Irwin H: Ante, Toronto, Ontario Canada, dentist]: eponym, in fixed partial prosthodontics for the observation that the combined pericemental area of all abutment teeth supporting a fixed dental prosthesis should be equal to or greater in pericemental area than the tooth or teeth to be replaced; as formulated for removable dental prosthodontics, the combined pericemental area of the abutment teeth plus the mucosa area of the denture base should be equal to or greater than the pericemental area of the missing teeth
Ante IH. The fundamental principles, design and construction of crown and bridge prosthesis. Dent Item Int 1928;50:215–32.
artificial crown \är′ti-fish′al kroun\: a metal, plastic, or ceramic restoration that covers three or more axial surfaces and the occlusal surface or incisal edge of a tooth
bi·op·sy n, pl -sies (1895): the removal of tissue for histologic examination and diagnosis
buccolingual relationship \bŭk′o-l ng′gwal r-lā′shun-shp\: any position of reference relative to the tongue and cheeks
ng′gwal r-lā′shun-shp\: any position of reference relative to the tongue and cheeks
can·ti·lever \kăn′tl-ē′ver\ n (1667): a projecting beam or member supported on one end
cantilever fixed dental prosthesis \kăn′tl-ē′ver fkst d n′tl pr
n′tl pr s-thē′sis\: a fixed dental prosthesis in which the pontic is cantilevered, i.e., is retained and supported only on one end by one or more abutments
s-thē′sis\: a fixed dental prosthesis in which the pontic is cantilevered, i.e., is retained and supported only on one end by one or more abutments
clinical crown \kln′-kel kroun\: the portion of a tooth that extends from the occlusal table or incisal edge to the free gingival margin
complete crown \km-plēt kroun\: a restoration that covers all the coronal tooth surfaces (mesial, distal, facial, lingual, and occlusal)
complete denture \km-plēt dn′chur\: a removable dental prosthesis that replaces the entire dentition and associated structures of the maxillae or mandible; called a complete removable dental prosthesis
1crown \kroun\ n (12c): 1: the highest part, as the topmost part of the skull, head or tooth; the summit; that portion of a tooth occlusal to the dentinoenamel junction or an artificial substitute for this 2: an artificial replacement that restores missing tooth structure by surrounding part or all of the remaining structure with a material such as cast metal, porcelain, or a combination of materials such as metal and porcelain
2crown \kroun\ vt (12c): to place on the head, as to place a crown on a tooth, dental implant or tooth substitute—usage: implies fabrication of a restoration for a tooth on a natural tooth, dental implant and/or dental implant abutment
crown fracture \kroun frăk′chur\: micro or macroscopic cleavage in the coronal portion of a tooth
crown-root ratio \kroun-rōōt rā′shō, rā′shē-ō′\: the physical relationship between the portion of the tooth within alveolar bone compared with the portion not within the alveolar bone, as determined by radiograph
de·min·er·al·iza·tion \dē-mn′er-ă-lī-zā′shun\ n (ca. 1903): 1: loss of minerals (as salts of calcium) from the body 2: in dentistry, decalcification, usually related to the dental caries process
dental prosthesis \dn′tl prs-thē′sis\: an artificial replacement (prosthesis) of one or more teeth (up to the entire dentition in either arch) and associated dental/alveolar structures. Dental prostheses usually are subcatagoried as either fixed dental prostheses or removable dental prosthses—see also FIXED DENTAL PROSTHESIS, REMOVABLE DENTAL PROSTHESIS; comp to MAXILLOFACIAL PROSTHESIS, ANCILLARY PROSTHESIS
differential diagnosis \df′a-rn′shal dī′ag-nō′ss\: the process of identifying a condition by comparing the signs and symptoms of all pathologic processes that may produce similar signs and symptoms
e·ti·ol·o·gy \ē′tē-l′a-jē\ n (1555): 1: the factors implicated in the cause or origin of a disease or disorder 2: the study or theory of the factors causing disease
extracoronal retainer \k′stra-kôr′a-nal, kr′-, ka-rō′nal r-tā′ner\: that part of a fixed dental prosthesis uniting the abutment to the other elements of a prosthesis that surrounds all or part of the prepared crown
fixed partial denture \fkst pär′shal dn′chur\: see FIXED DENTAL PROSTHESIS
fixed dental prosthesis \fkst dn′tl prs-thē′ss\: any dental prosthesis that is luted, screwed or mechanically attached or otherewise securely retained to natual teeth, tooth roots, and/or dental implant abutments that furnish the primary support for the dental prosthesis. This may include replacement of one to sixteen teeth in each dental arch. If a metallic or ceramic component is included within the fixed dental prosthesis, that component is termed the framework. Ed note: Dental prostheses (fixed dental prostheses, removable dental prostheses) as well as maxillofacial prostheses can be supported and retained in part or whole by dental implants. Terminology to assist in describing the means of retention, support and dental materials should be limited to concatenation of three and no more than four adjectives to provide clarity. Descriptive terminology (modifiers) expressed as adejectives to each fixed dental prosthesis may include such items as the method of retention, composition, nature of support, design characteristics, and/or form of anchorage
Simon H, Yanase RT. Terminology for Implant Prostheses. Int J Oral Maxillofac Implants 2003; 18:539–543.
fren·u·lum \frn′ya-lem\ n, pl -la \lă\ (1706): a connecting fold of membrane serving to support or retain a part
high lip line \hī lp līn\: the greatest height to which the inferior border of the upper lip is capable of being raised by muscle function
horizontal overlap \hôr′-zn-tl, hr′- ō′ver-lăp′\: the projection of teeth beyond their antagonists in the horizontal plane
hydroxyapatite ceramic \hī-drk′sē-ăp′a-tīt sa-răm′k\: a composition of calcium and phosphate in physiologic ratios to provide a dense, non-resorbable, biocompatible ceramic used for dental implants and residual ridge augmentation
id·io·path·ic \d′ē-ō-păth′k\ adj (1669): self-originated; of unknown causation
immediate denture \-mē′dē-t dn′chur\: any removable dental prosthesis fabricated for placement immediately following the removal of a natural tooth/teeth
indirect retainer \n′d-rkt′, -dī- r-tā′ner\: the component of a removable dental prosthesis that assists the direct retainer(s) in preventing displacement of the distal extension denture base by functioning through lever action on the opposite side of the fulcrum line when the denture base moves away from the tissues in pure rotation around the fulcrum line
indirect retention \n′d-rkt′, -dī- r-tn′shun\: the effect achieved by one or more indirect retainers of a removable partial denture that reduces the tendency for a denture base to move in an occlusal direction or rotate about the fulcrum line
interim denture: see INTERIM PROSTHESIS
interim prosthesis \n′ter- prs-thē′ss\: a fixed or removable dental prosthesis, or maxillofacial prosthesis, designed to enhance esthetics, stabilization and/or function for a limited period of time, after which it is to be replaced by a definitive dental or maxillofacial prosthesis. Often such prostheses are used to assist in determination of the therapeutic effectiveness of a specific treatment plan or the form and function of the planned for definitive prosthesis—syn PROVISIONAL PROSTHESIS, PROVISIONAL RESTORATION
intermediate abutment \n′ter-mē′dē-t a-bŭt′ment\: a natural tooth located between terminal abutments that serve to support a fixed or removable dental prosthesis
interproximal contact \n′ter-prk′sa-mal kn′tăkt\: the area of a tooth that is in close association, connection, or touch with an adjacent tooth in the same arch
key·way \kē′wā′\ n: an interlock using a matrix and patrix between the units of a fixed dental prosthesis. It may serve two functions: 1) to hold the pontic in the proper relationship to the edentulous ridge and the opposing teeth during occlusal adjustment on the working cast (during application of any veneering material) and 2) to reinforce the connector after soldering
low lip line \lō lp līn\: 1: the lowest position of the inferior border of the upper lip when it is at rest 2: the lowest position of the superior border of the lower lip during smiling or voluntary retraction
lu·mi·nance \lōō′ma-nans\ n (1880): the intensity of light per unit area
masticatory force \măs′t-ka-tôr′ē fôrs, fōrs\: the force applied by the muscles of mastication during chewing
mesial drift \mē′zē-al drft\: movement of teeth toward the midline
mesioversion \mē′zē-ō-vûr′zhun, -shun\: with reference to a tooth, nearer than normal in its position toward the median line of the face, along the dental arch
nano·me·ter \năn′a-mē′tar\ n (1963): unit of length to measure the wavelength of light. It is equivalent to 1 ¥ 10−9 M or 10 angstroms. 1 nm = 1/1,000,000 mm
nonrigid connector \nn-rj′d ka-nk′tor\: any connector that permits limited movement between otherwise independent members of a fixed dental prosthesis
occlusal analysis \a-klōō′zal,-sal a-năl′-ss\: an examination of the occlusion in which the interocclusal relations of mounted casts are evaluated
occlusal equilibration \a-klōō′zal, -sal -kwl′a-brā′shun\: the modification of the occlusal form of the teeth with the intent of equalizing occlusal stress, producing simultaneous occlusal contacts or harmonizing cuspal relations
occlusal interference \a-klōō′zal, -sal n′tur-fîr′ans\: any tooth contact that inhibits the remaining occluding surfaces from achieving stable and harmonious contacts
occlusal prematurity \a-klōō′zal, -sal prē′ma-tyōōr′-tē, -tōōr′-, -chōōr′-\: any contact of opposing teeth that occurs before the planned intercuspation
occlusal reshaping \a-klōō′zal, -sal rē-shāp′ng\: the intentional alteration of the occlusal surfaces of teeth to change their form
occlusal stability \a-klōō′zal, -sal sta-bl′-tē\: the equalization of contacts that prevents tooth movement after closure
occlusion analysis \a-klōō′shun a-năl′-ss\ obs: a systematic examination of the masticatory system with special consideration to the effect of tooth occlusion on the teeth and their related structures (GPT-4)
pal·lia·tive \păl′ē-ā′tv\ adj (1543): affording relief but not a cure
pier abutment: see INTERMEDIATE ABUTMENT
plunger cusp \plŭn′jer kŭsp\: a cusp that tends to force food into interproximal areas
prog·no·sis \prg-nō′ss\ n (1655): a forecast as to the probable result of a disease or a course of therapy
pros·the·sis \prs-thē′ss\n, pl-ses (1900) 1: an artificial replacement of an absent part of the human body 2: a therapeutic device to improve or alter function 3: a device used to aid in accomplishing a desired surgical result Editorial note: The taxonomy of the word prostheses is as complex as are the varieties of items made by humans for any utilitarian purpose. While classification of botanical or zoological species can be relatively precise due to the common nature of genetic derivation (including descriptions of genetic alterations), such is not the case with respect to many things made by humans. One has only to think about the range of forms used in the course of human history classified as “items of transportation” to be convinced of the complexity and frequently transient nature of such a mode as the automobile! With respect to dentistry, the noun prosthesis generally is described first by a type adjective (dental, maxillofacial or ancillary) and frequently second by use of one or more additional adjectives (termed modifiers) to clarify such matters as anatomic location, form, materials, means of retention, support, time of usage, or other items. Using coordinate adjectives (two or more adjectives separated by a comma, instead of by coordinating conjunctions) to assist in further description of the prosthesis is helpful but should generally be limited to three or at most four for convenience in maintaining understanding of the noun prosthesis. Frequently, an adjective clause ·descriptorÒ can be used following the word prosthesis to help clarify such issues as the nature of the support [i.e. tooth number(s), dental implant number(s)] available for the prosthesis. A descriptor is something (a word, phrase or characteristic feature) that serves to identify or describe; especially a word or phrase (as an index term) used to identify an item in an information retrieval system. Use of acronyms to describe a prosthesis is to be discouraged since such descriptors do not transfer between languages and thus can be easily misunderstood.
Modifier: {anatomic location} i.e. maxillary, mandibular, inferior, superior
{form} i.e. complete, partial, splint, stent, carrier, bar, ovoid, round
{material} i.e. ceramic, metal, resin
{retention} i.e. cement, screw, friction, tissue, fixed, removable
{support} i.e. tooth, implant, tissue
{time} i.e. surgical, temporary, interim, definitive
Type: (dental, maxillofacial, ancillary)
Descriptor: <support> tissue borne, implant borne, tooth/implant borne
see also DEFINITIVE P., DENTAL P., INTERIM P., MAXILLOFACIAL P., PROVISIONAL P., SUPPLEMENTARY P., and SURGICAL P.
pulp \pŭlp\ n: the richly vascularized connective tissue of mesodermal origin with much innervation contained in the central cavity of the tooth
removable partial denture prosthesis \r-mōō′va-bal păr′shal dēn′chur\: any prosthesis that replaces some teeth in a partially dentate arch. It can be removed from the mouth and replaced at will—also called partial removable dental prosthesis
residual bone \r-zj′ōō-al bōn\: that component of maxillary or mandibular bone that remains after the teeth are lost
residual ridge \r-zj′ōō-al rj\: the portion of the residual bone and its soft tissue covering that remains after the removal of teeth
res·to·ra·tion \rs′ta-rā′shun\ n (1660): a broad term applied to any material or prosthesis that restores or replaces lost tooth structure, teeth, or oral tissues
span length \spăn lngkth\: the length of a beam between two supports
splint·ing \spln′tng\ v: 1: in dentistry, the joining of two or more teeth into a rigid unit by means of fixed or removable restorations or devices 2: in physiology, prolonged muscle spasms that inhibit or prevent movement
stress breaker: see STRESS DIRECTOR
stress director \strs d-rk′tar, dī-\: a device or system that relieves specific dental structures of part or all of the occlusal forces and redirects those forces to other bearing structures or regions
su·pra·erup·tion \sōō′pra--rŭp′shun\ n: movement of a tooth or teeth above the normal occlusal plane
su·pra·oc·clus·ion \sōō′pra-a-klōō′zhun\ n: malocclusion in which the occluding surfaces of teeth extend beyond the normal occlusal plane—called also overeruption
sympathetic nervous system \sm′pa-tht′k nûr′vas ss′tum\: the part of the autonomic nervous system that responds to dangerous or threatening situations by preparing a person physiologically for “fight or flight”—see PARASYMPATHETIC NERVOUS SYSTEM
symp·tom \sm′tum, smp-\ n (14c): subjective evidence of disease or physical disturbance; something that indicates the presence of a bodily disorder
systemic etiologic factors \s-stm′k ē′tē-ō-lj′k făk′turs\: generalized biologic factors that are implicated in the causation, modification, and/or perpetuation of a disease entity
tooth supported \tōōth sa-pôr′td\: a term used to describe a prosthesis or part of a prosthesis that depends entirely on the natural teeth for support
transitional prosthesis: see INTERIM PROSTHESIS, TRANSITIONAL DENTURE
trau·ma \trou′ma, trô′-\ n, pl trau·ma·ta \trou′ ma-ta\ or
trau·mas \trou′mas\, traumatic \trou′măt-ik\ adj- traumatically \trou′măt--kă-lē\ adv (1693): an injury or wound, whether physical or psychic
up·right \ŭp′rīt\ adj: the movement of a tooth into an erect or normal position
working articulation \wûr′kng ăr-tk′ya-lā′shun\: the occlusal contacts of teeth on the side toward which the mandible is moved
STUDY QUESTIONS
1 Palomo F, Peden J. Periodontal considerations of restorative procedures. J Prosthet Dent. 1976;36:387.
2 Jones RM, et al. A comparison of the physical properties of four prosthetic veneering materials. J Prosthet Dent. 1989;61:38.
3 Vojvodic D, et al. The bond strength of polymers and metal surfaces using the “silicoater” technique. J Oral Rehabil. 1995;22:493.
4 Rothfuss LG, et al. Resin to metal bond strengths using two commercial systems. J Prosthet Dent. 1998;79:270.
5 Karmaker AC, et al. Continuous fiber reinforced composite materials as alternatives for metal alloys used for dental appliances. J Biomater Appl. 1997;11:318.
6 Rosenthal L, et al. A new system for posterior restorations: a combination of ceramic optimized polymer and fiber-reinforced composite. Pract Periodontics Aesthet Dent. 1997;9(5 suppl):6.
7 Zanghellini G. Fiber-reinforced framework and Ceromer restorations: a technical review. Signature. 1997;4(1):1.
8 Claus H. Vita In-Ceram, a new procedure for preparation of oxide-ceramic crown and bridge framework. Quintessenz Zahntech. 1990;16:35.
9 Magne P, Belser U. Esthetic improvements and in vitro testing of In-Ceram Alumina and Spinell ceramic. Int J Prosthodont. 1997;10:459.
10 Zimmer D, et al. Survival rate of IPS-Empress 2 all-ceramic crowns and bridges: three years’ results. Schweiz Monatsschr Zahnmed. 2004;114:115.
11 Denry IL. Recent advances in ceramics for dentistry. Crit Rev Oral Biol Med. 1996;7:134.
12 Sorensen JA, et al. IPS Empress crown system: three-year clinical trial results. J Calif Dent Assoc. 1998;26:130.
13 Denry IL, et al. Effect of cubic leucite stabilization on the flexural strength of feldspathic dental porcelain. J Dent Res. 1996;75:1928.
14 Walton TR. An up to 15-year longitudinal study of 515 metal-ceramic FPDs: Part 1. Outcome. Int J Prosthodont. 2002;15:439.
15 Adell R, et al. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981;10:387.
16 Saunders TR, et al. The maxillary complete denture opposing the mandibular bilateral distal-extension partial denture: treatment considerations. J Prosthet Dent. 1979;41:124.
17 Brewer AA, Morrow RM. Overdentures, 2nd ed. St. Louis: Mosby, 1980.
18 Sarita PTN, et al. Chewing ability of subjects with shortened dental arches. Community Dent Oral Epidemiol. 2003;31:328.
19 Shugars DA, et al. Survival rates of teeth adjacent to treated and untreated posterior bounded edentulous spaces. J Am Dent Assoc. 1998;129:1089.
20 Gragg KL, et al. Movement of teeth adjacent to posterior bounded edentulous spaces. J Dent Res. 2001;80:2021.
21 Cheung GS, et al. A clinical evaluation of conventional bridgework. J Oral Rehabil. 1990;17:131.
22 Glickman I, et al. Photoelastic analysis of internal stresses in the periodontium created by occlusal forces. J Periodontol. 1970;41:30.
23 Wright KWJ, Yettram AL. Reactive force distributions for teeth when loaded singly and when used as fixed partial denture abutments. J Prosthet Dent. 1979;42:411.
24 Yang HS, et al. Stress analysis of a cantilevered fixed partial denture with normal and reduced bone support. J Prosthet Dent. 1996;76:424.
25 Briggs P, et al. The single unit, single retainer, cantilever resin-bonded bridge. Br Dent J. 1996;181:373.
26 Christensen GJ. When to use fillers, build-ups or posts and cores. J Am Dent Assoc. 1996;127:1397.
27 Miller TE. Orthodontic therapy for the restorative patient. I. The biomechanic aspects. J Prosthet Dent. 1989;61:268.
28 Holmgren K, et al. The effects of an occlusal splint on the electromyographic activities of the temporal and masseter muscles during maximal clenching in patients with a habit of nocturnal bruxism and signs and symptoms of craniomandibular disorders. J Oral Rehabil. 1990;17:447.
29 Ante IH. The fundamental principles of abutments. Mich State Dent Soc Bull. 1926;8:14.
30 Dykema RW, et al, editors. Johnston’s Modern Practice in Fixed Prosthodontics. 4th ed.. Philadelphia: WB Saunders. 1986:4.
31 Tylman SD, Malone WFP. Tylman’s Theory and Practice of Fixed Prosthodontics, 7th ed., St Louis: Mosby; 1978:15.
32 Shillingburg HT, et al. Fundamentals of Fixed Prosthodontics, 2nd ed., Chicago: Quintessence Publishing; 1981:20.
33 Jepsen A. Root surface measurement and a method for x-ray determination of root surface area. Acta Odontol Scand. 1963;21:35.
34 Nyman S, Ericsson I. The capacity of reduced periodontal tissues to support fixed bridgework. J Clin Periodontol. 1982;9:409.
35 Freilich MA, et al. Fixed partial dentures supported by periodontally compromised teeth. J Prosthet Dent. 1991;65:607.
36 Decock V, et al. 18-Year longitudinal study of cantilevered fixed restorations. Int J Prosthodont. 1996;9:331.
37 Penny RE, Kraal JH. Crown-to-root ratio: its significance in restorative dentistry. J Prosthet Dent. 1979;42:34.
38 Nyman S, et al. The role of occlusion for the stability of fixed bridges in patients with reduced periodontal tissue support. J Clin Periodontol. 1975;2(2):53.
39 Laurell L, et al. Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J Prosthet Dent. 1991;66:545.
40 Smyd ES. Dental engineering. J Dent Res. 1948;27:649.
41 Napankangas R, et al. Longevity of fixed metal ceramic bridge prostheses: a clinical follow-up study. J Oral Rehabil. 2002;29:140.
42 Dykema RW. Fixed partial prosthodontics. J Tenn Dent Assoc. 1962;42:309.
43 Olin PS, et al. Improved pontic/tissue relationships using porous coralline hydroxyapatite block. J Prosthet Dent. 1991;66:234.
44 Aquilino SA, et al. Ten-year survival rates of teeth adjacent to treated and untreated posterior bounded edentulous spaces. J Prosthet Dent. 2001;85:455.