1 HISTORY TAKING AND CLINICAL EXAMINATION
Fixed prosthodontic treatment involves the replacement and restoration of teeth by artificial substitutes that are not readily removable from the mouth. Its focus is to restore function, esthetics, and comfort. Fixed prosthodontics can offer exceptional satisfaction for both patient and dentist. It can transform an unhealthy, unattractive dentition with poor function into a comfortable, healthy occlusion capable of years of further service and greatly enhance esthetics (Fig. 1-1A and B). Treatment can range from the fairly straightforward restoration of a single tooth with a cast crown (Fig. 1-1C) or replacement of one or more missing teeth with a fixed dental prosthesis (Fig. 1-1D) or implant-supported restoration to a highly complex restoration involving all the teeth in an entire arch or the entire dentition.

Fig. 1-1 A severely damaged maxillary dentition (A) restored with metal-ceramic fixed prostheses (B). C, Complete cast crown restores mandibular molar. D, Three-unit fixed dental prosthesis replacing missing mandibular premolar.
(C, Courtesy of Dr. X Lepe. D, Courtesy of Dr. J. Nelson.)
To achieve predictable success in this technically exacting and demanding field, there must be meticulous attention to every detail: from the initial patient interview and diagnosis, through the active treatment phases, and to a planned schedule of follow-up care. Otherwise, the result is likely to be unsatisfactory and frustrating for both dentist and patient, resulting in disappointment and loss of confidence in each other.
Problems encountered during or after treatment can often be traced to errors and omissions during history taking and initial examination. An inexperienced clinician may plunge into the treatment phase before collecting sufficient diagnostic information that helps predict likely pitfalls.
Making the correct diagnosis is prerequisite for formulating an appropriate treatment plan. This requires that all pertinent information be obtained. A complete history includes a comprehensive assessment of the patient’s general and dental health, individual needs, preferences, and personal circumstances. This chapter reviews fundamentals of history taking and clinical examination, with special emphasis on obtaining the necessary information to make appropriate fixed prosthodontic treatment decisions.
HISTORY
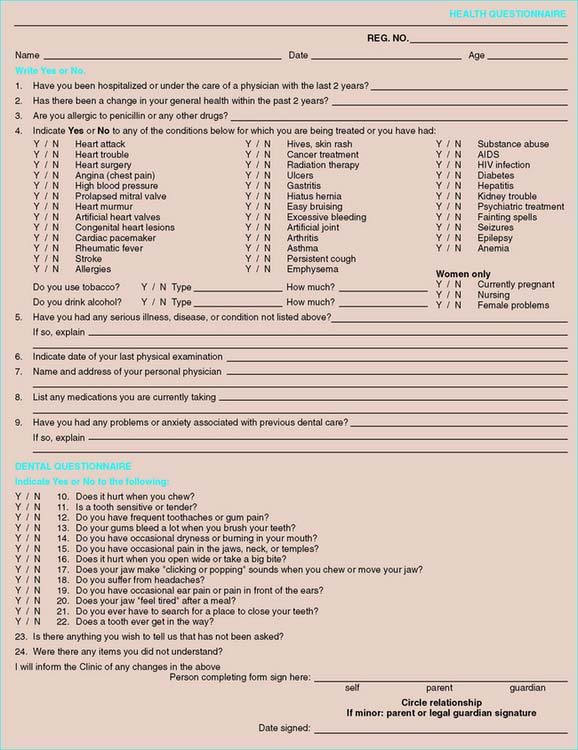
A patient’s history should include all pertinent information concerning the reasons for seeking treatment, along with any personal information, including relevant previous medical and dental experiences. The chief complaint should be recorded, preferably in the patient’s own words. A screening questionnaire (Fig. 1-2) is useful for history taking; it should be reviewed in the patient’s presence to correct any mistakes and to clarify inconclusive entries. If the patient is mentally impaired or a minor, the guardian or responsible parent must be present.
Chief Complaint
The accuracy and significance of the patient’s primary reason or reasons for seeking treatment should be analyzed first. These may be just the obvious features, and careful examination often reveals problems and disease of which the patient is unaware; nevertheless, the patient perceives the chief complaint as the major problem. Therefore, when a comprehensive treatment plan is proposed, special attention must be given to how the chief complaint can be resolved. The inexperienced clinician trying to prescribe an “ideal” treatment plan can lose sight of the patient’s wishes. The patient may then become frustrated because the dentist apparently does not understand or does not want to understand the patient’s point of view.
Chief complaints usually belong to one of the following four categories:
Comfort
If pain is present, its location, character, severity, and frequency should be noted, as well as the first time it occurred, what factors precipitate it (e.g., hot, cold, or sweet things), and any changes in its character. Is it localized or more diffuse in nature? It is often helpful to have the patient point at the area while the dentist pays close attention.
If swelling is present, the location, size, consistency, and color are noted, as well as how long it has been felt and whether it is increasing or decreasing.
Function
Difficulties in chewing may result from a local problem such as a fractured cusp or missing teeth; it may also indicate a more generalized malocclusion or dysfunction.
Social aspects
A bad taste or smell often indicates compromised oral hygiene and periodontal disease. Often social pressures prompt the patient to seek care.
Appearance
Compromised appearance is a strong motivating factor for patients to seek advice as to whether improvement is possible (Fig. 1-3). Such patients may have missing or crowded teeth, or a tooth or restoration may be fractured. Their teeth may be unattractively shaped, malpositioned, or discolored, or there may be a developmental defect.

Personal Details
The patient’s name, address, phone number, sex, occupation, work schedule, and marital and financial status are noted. Much can be learned in a 5-minute, casual conversation during the initial visit. In addition to establishing rapport and developing a basis for the patient to trust the dentist, small and seemingly unimportant personal details often have considerable influence in establishing a correct diagnosis, prognosis, and treatment plan.
Medical History
An accurate and current general medical history should include any medication the patient is taking, as well as all relevant medical conditions. If necessary, the patient’s physician or physicians can be contacted for clarification. The following classification may be helpful:

Fig. 1-4 Severe gingival hyperplasia associated with anticonvulsant drug use.
(Courtesy of Dr. P. B. Robinson.)
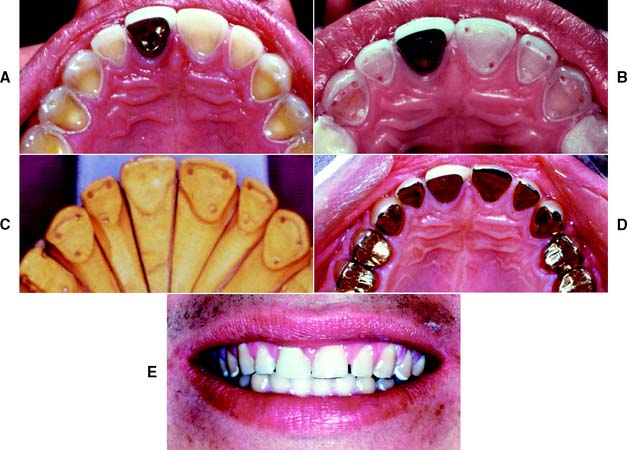
Fig. 1-5 A, Extensive damage caused by self-induced acid regurgitation. Note that the lingual surfaces are bare of enamel except for a narrow band at the gingival margin. B, Teeth prepared for partial-coverage restorations. C, Definitive cast. D and E, The completed restoration.
Dental offices practice “universal precautions” to ensure appropriate infection control. This means that full infection control is practiced for every patient; no additional measures are needed when dentists treat known disease carriers.6
Dental History
Clinicians should be cautious when commenting before a thorough examination is completed. With adequate experience, a clinician can often assess preliminary treatment needs during the initial appointment. However, fairly assessing the quality of a previously rendered treatment can be difficult, because the circumstances under which the treatment was rendered are seldom known. When such an assessment is requested for legal proceedings, the patient should be referred to a specialist familiar with the “usual and customary” standard of care.
Periodontal history
The patient’s oral hygiene is assessed, and current plaque-control measures are discussed, as are previously received oral hygiene instructions. The frequency of any previous débridement should be recorded, and the dates and nature of any previous periodontal surgery should be noted.
Restorative history
The patient’s restorative history may include only simple composite resin or dental amalgam fillings, or it may involve crowns and extensive fixed dental prostheses. The age of existing restorations can help establish the prognosis and probable longevity of any future fixed prostheses.
Endodontic history
Patients often forget which teeth have been endodontically treated. These can be readily identified with radiographs. The findings should be reviewed periodically so that periapical health can be monitored and any recurring lesions promptly detected (Fig. 1-6).

Orthodontic history
Occlusal analysis should be an integral part of the assessment of a postorthodontic dentition. If restorative treatment needs are anticipated, they should be undertaken by the restorative dentist. Occlusal adjustment (reshaping of the occlusal surfaces of the teeth) may be needed to promote long-term positional stability of the teeth and reduce or eliminate parafunctional activity. On occasion, root resorption (detected on radiographs) (Fig. 1-7) may be attributable to previous orthodontic treatment. As the crown/root ratio is affected, future prosthodontic treatment and its prognosis may also be affected. Restorative treatment can often be simplified by minor tooth movement. When a patient is contemplating orthodontic treatment, considerable time can be saved if minor tooth movement (for restorative reasons) is incorporated from the start. Thus, good communication between the restorative dentist and the orthodontist may prove very helpful.

Removable prosthodontic history
The patient’s experiences with removable prostheses must be carefully evaluated. For example, a partial removable dental prosthesis may not have been worn for a variety of reasons, and the patient may not even have mentioned its existence. Careful questioning and examination usually elicits discussion concerning any such devices. Listening to the patient’s comments about previously unsuccessful removable prostheses can be very helpful in assessing whether future treatment will be more successful.
Oral surgical history
Information about missing teeth and any complications that may have occurred during tooth removal is obtained. Special evaluation and data collection procedures are necessary for patients who require prosthodontic care after orthognathic surgery. Before any treatment is undertaken, the prosthodontic component of the proposed treatment should be fully coordinated with the surgical component.
Radiographic history
Previous radiographs may prove helpful in judging the progress of dental disease. They should be obtained if possible, because it is generally better to avoid exposing the patient to unnecessary ionizing radiation. Dental practices usually forward radiographs or acceptable duplicates promptly on request. In most instances, however, a current diagnostic radiographic series is essential and should be obtained as part of the examination.
Temporomandibular joint dysfunction history
A history of pain or clicking in the TMJs or neuromuscular symptoms, such as tenderness to palpation, may be caused by TMJ dysfunction, which should normally be treated and resolved before fixed prosthodontic treatment begins. A screening questionnaire efficiently identifies these problems. The patient should be questioned regarding any previous treatment for joint dysfunction (e.g., occlusal devices, medications, biofeedback, or physical therapy exercises).
EXAMINATION
An examination consists of the clinician’s use of sight, touch, and hearing to detect conditions outside the normal range. To avoid mistakes, it is critical to record what is actually observed rather than to make diagnostic comments about the condition. For example, “swelling,” “redness,” and “bleeding on probing of gingival tissue” should be recorded, rather than “gingival inflammation” (which implies a diagnosis).
Thorough examination and data collection are needed for the prospective fixed prosthodontic patient, and the protocol for this effort can be obtained from various textbooks of oral diagnosis.7,8
General Examination
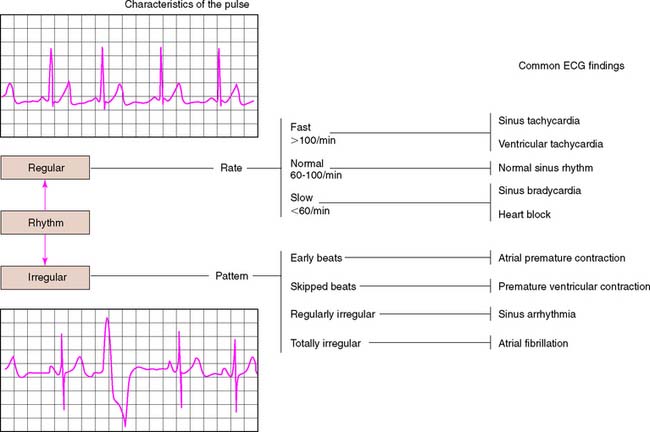
The patient’s general appearance, gait, and weight are assessed. Skin color is noted for signs of anemia or jaundice. Vital signs, such as respiration, pulse, temperature, and blood pressure, are measured and recorded. Fixed prosthodontic treatment is often indicated in middle-aged or older patients, who can be at higher risk for cardiovascular disease. Relatively inexpensive cardiac monitoring units are available for in-office use (Fig. 1-8). Patients with vital sign measurements outside normal ranges should be referred for a comprehensive medical evaluation before definitive treatment is initiated.
Extraoral Examination
Special attention is given to facial asymmetry because small deviations from normal may hint at serious underlying conditions. Cervical lymph nodes are palpated, as are the TMJs and the muscles of mastication.
Temporomandibular joints
The clinician locates the TMJs by palpating bilaterally just anterior to the auricular tragi while the patient opens and closes the mouth. This permits a comparison between the relative timing of left and right condylar movements during the opening stroke. Asynchronous movement may indicate an anterior disk displacement that prevents one of the condyles from making a normal translatory movement (see Chapter 4). Auricular palpation (Fig. 1-9) with light anterior pressure helps identify potential disorders in the posterior attachment of the disk. Tenderness or pain on movement is noted and can be indicative of inflammatory changes in the retrodiscal tissues, which are highly vascular and innervated. Clicking in the TMJ is often noticeable through auricular palpation but may be difficult to detect in palpation directly over the lateral pole of the condylar process, because the overlying tissues can muffle the click. Placement of the fingertips on the angles of the mandible helps identify even a minimal click, because very little soft tissue lies between the fingertips and the mandibular bone.

A maximum mandibular opening resulting in less than 35 mm of interincisal movement is considered restricted, because the average opening is greater than 50 mm.9,10 Such restricted movement on opening can be indicative of intracapsular changes in the joints. Similarly, any midline deviation on opening and/or closing is recorded. The maximum lateral movements of the patient can be measured (normal is about 12 mm) (Fig. 1-10).

Muscles of mastication
Next, the masseter and temporal muscles, as well as other relevant postural muscles, are palpated for signs of tenderness (Fig. 1-11). Palpation is best accomplished bilaterally and simultaneously. This allows the patient to compare and report any differences between the left and right sides. Light pressure should be used (the amount of pressure one can tolerate when gently pushing on one’s closed eyelid without feeling discomfort is a good comparative measure), and if any difference is reported between the left and right sides, the patient is asked to classify the discomfort as mild, moderate, or severe. If there is evidence of significant asynchronous movement or TMJ dysfunction, a systematic sequence for comprehensive muscle palpation should be followed as described by Solberg9 and Krogh-Poulsen and Olsson.11 Each palpation site is given a numerical score based on the patient’s response. If neuromuscular or TMJ treatment is initiated, the examiner can then repalpate the same sites periodically to assess the response to treatment (Fig. 1-12).
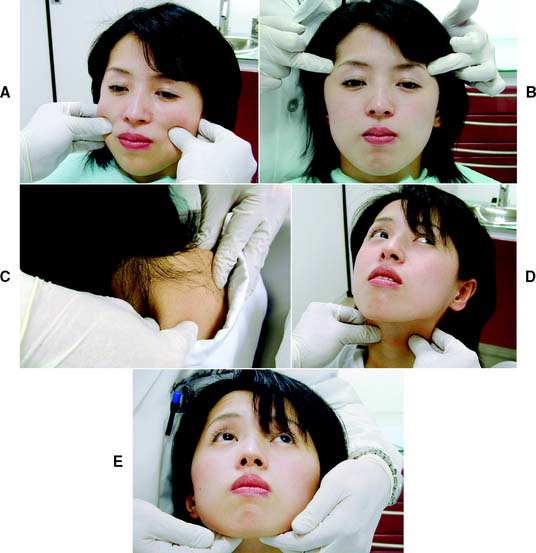
Fig. 1-11 Muscle palpation. A, The masseter. B, The temporal muscle. C, The trapezius muscle. D, The sternocleidomastoid muscle. E, The floor of the mouth.
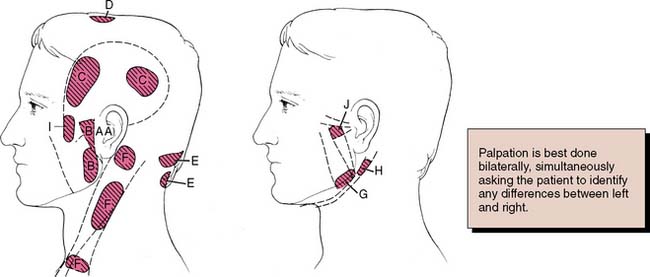
Fig. 1-12 Palpation sites for assessing muscle tenderness. A, Temporomandibular joint capsule: lateral and dorsal. B, Masseter: deep and superficial. C, Temporal muscle: anterior and posterior. D, Vertex. E, Neck: nape and base. F, Sternocleidomastoid muscle: insertion, body, and origin. G, Medial pterygoid muscle. H, Posterior digastric muscle. I, Temporal tendon. J, Lateral pterygoid muscle.
(From Krogh-Poulsen WG, Olsson A: Occlusal disharmonies and dysfunction of the stomatognathic system. Dent Clin North Am 10:627, 1966.)
Lips
The patient is observed for tooth visibility during normal and exaggerated smiling. This can be critical in fixed prosthodontic treatment planning,12 especially for margin placement of certain metal-ceramic crowns. Some patients show only their maxillary teeth during smiling. More than 25% do not show the gingival third of the maxillary central incisors during an exaggerated smile13 (Fig. 1-13). The extent of the smile depends on the length and mobility of the upper lip and the length of the alveolar process. When the patient laughs, the jaws open slightly and a dark space is often visible between the maxillary and mandibular teeth (Fig. 1-14). This has been called the negative space.14 Missing teeth, diastemas, and fractured or poorly restored teeth disrupt the harmony of the negative space and often require correction.15

Fig. 1-13 Smile analysis is an important part of the examination, particularly when anterior crowns or fixed dental prostheses are being considered. A, Some individuals show considerable gingival tissue during an exaggerated smile. B, Others may not show the gingival margins of even the central incisors.

Intraoral Examination
The intraoral examination can reveal considerable information concerning the condition of the soft tissues, teeth, and supporting structures. The tongue, floor of the mouth, vestibule, cheeks, and hard and soft palates are examined, and any abnormalities are noted. This information can be evaluated properly during treatment planning only if objective indices, rather than vague assessments, are used.
Periodontal Examination
A periodontal examination16 should provide information regarding the status of bacterial accumulation, the response of the host tissues, and the degree of reversible and irreversible damage. Because long-term periodontal health is essential for successful fixed prosthodontics (see Chapter 5), existing periodontal disease must be corrected before any definitive prosthodontic treatment is undertaken.
Gingiva
The gingiva should be lightly dried before examination so that moisture does not obscure subtle changes or detail. Color, texture, size, contour, consistency, and position are noted and recorded. The gingiva is then carefully palpated to express any exudate or pus that may be present in the sulcular area.
Healthy gingiva (Fig. 1-15A) is pink, stippled, and firmly bound to the underlying connective tissue. The free margin of the gingiva is knife-edged, and sharply pointed papillae fill the interproximal spaces. Any deviation from these findings should be noted. With the development of chronic marginal gingivitis (Fig. 1-15B), the gingiva becomes enlarged and bulbous, loss of stippling occurs, the margins and papillae are blunted, and bleeding and exudate are observed.

Fig. 1-15 A, Healthy gingiva: pink, knife-edged, and firmly attached. B, Gingivitis: Plaque and calculus have caused marginal inflammation, with changes in color, contour, and consistency of the free gingival margin. Inflammation extends into the keratinized attached gingiva.
The width of the band of attached keratinized gingiva around each tooth may be assessed by measuring the surface band of keratinized tissue in an apicocoronal dimension with a periodontal probe and subtracting the measurement of the sulcus depth. Another method of obtaining this measurement by visual examination is to gently depress the marginal gingiva with the side of a periodontal probe or explorer. At the mucogingival junction (MGJ), the effect of the instrument is seen to end abruptly, indicating the transition from tightly bound gingiva to more flexible mucosa. Injecting anesthetic solution into the nonkeratinized mucosa close to the MGJ to make the mucosa balloon slightly is a third method of visualizing the MGJ. However, this is done only if the other methods do not provide the desired information.
Periodontium
The periodontal probe (Fig. 1-16A) is one of the most reliable and useful diagnostic tools available for examining the periodontium. It provides a measurement (in millimeters) of the depth of periodontal pockets and healthy gingival sulci on all surfaces of each tooth. In this examination, the probe is inserted essentially parallel to the tooth and is “walked” circumferentially through the sulcus in firm but gentle steps; the examiner determines the measurement when the probe is in contact with the apical portion of the sulcus (Fig. 1-16B). Thus, any sudden change in the attachment level can be detected. The probe may also be angled slightly (5 to 10 degrees) in the interproximal areas to reveal the topography of an existing lesion. Probing depths (usually six per tooth) are recorded on a periodontal chart (Fig. 1-17), which also contains other data pertinent to the periodontal examination (e.g., tooth mobility or malposition, open or deficient contact areas, inconsistent marginal ridge heights, missing or impacted teeth, areas of inadequate attached keratinized gingiva, gingival recession, furcation involvements, and malpositioned frenum attachments).
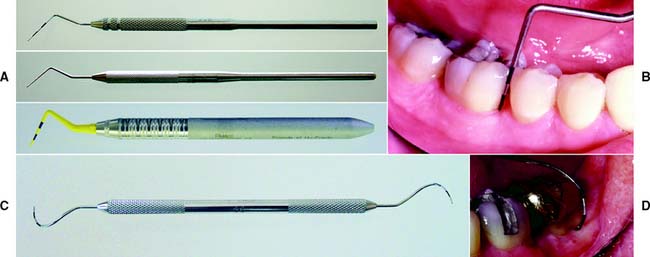
Fig. 1-16 A, Three types of sulcus/pocket-measuring probes. B, Correct position of a periodontal probe in the interproximal sulcular area, parallel to the root surface and in a vertical direction as far interproximally as possible. C and D, Graduated furcation probe.
(A and C, From Boyd: Dental Instruments, 2nd ed. St. Louis, WB Saunders, 2005.)
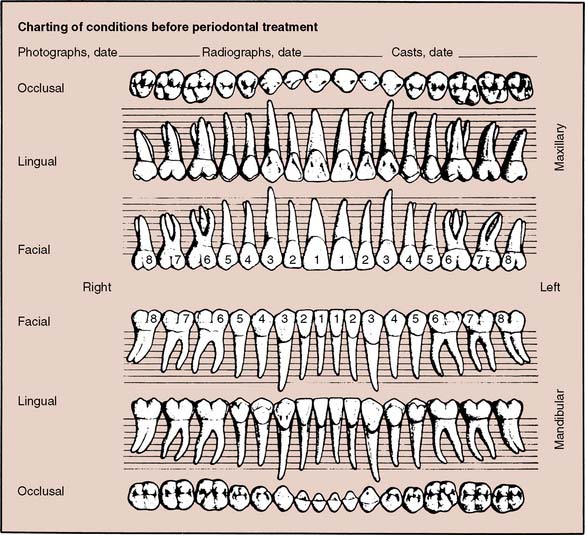
Fig. 1-17 Chart for recording pocket depths. The parallel lines are approximately 2 mm apart. The notations involved in using the chart are as follows: 1, Block out any missing teeth. 2, Draw a red X through the crown of any tooth that is to be extracted. 3, Record the gingival level with a continuous blue line. 4, Record pocket depths with a red line interrupted at the proximal surfaces of each tooth. 5, Shade the pocket form on each tooth with a red pencil (between the red and blue lines). 6, Indicate bifurcation or trifurcation involvements with a small red X at the involved area. 7, Record open contacts with vertical parallel lines (||) through the area. 8, Record improper contacts with a wavy red line through the area. 9, Record gingival overhang(s) with a red spur (^) through the area. 10, Outline cavities and faulty restorations of periodontal significance in red. 11, Indicate rotated teeth by outlining in blue to show their actual position.
(Modified from Goldman HM, Cohen DW: Periodontal Therapy, 5th ed. St. Louis, Mosby, 1973.)
Clinical Attachment Level
Documenting the level of attachment helps the clinician determine the amount of periodontal destruction that has occurred and is essential in rendering a diagnosis of periodontitis (loss of connective tissue attachment).17,18 This measurement also provides the clinician with more detailed and accurate information regarding the prognosis of an individual tooth. The clinical attachment level is determined by measuring the distance between the apical extent of the probing depth and a fixed reference point on the tooth, most commonly either the apical extent of a restoration and/or the cementoenamel junction (CEJ). This measurement can be documented on modified periodontal charts (Fig. 1-18) and incorporated with the standard periodontal documentation (see Fig. 1-17) to complete the clinical periodontal examination. When the free margin of the gingiva is located on the clinical crown and the level of the epithelial attachment is at the CEJ, there is no loss of attachment, and recession is noted as a negative number. When the level of the epithelial attachment is on root structure and the free margin of the gingiva is at the CEJ, the attachment loss equals the probing depth, and the recession is 0. In a situation in which there is increased periodontal destruction and recession, the loss of attachment measurement equals the probing depth plus the measurement of recession19 (see Fig. 1-18B and C). Clinical attachment loss is a measure of periodontal destruction at a site, rather than current disease activity, and it may be considered the diagnostic “gold standard” for periodontitis.20 It should be documented in the initial periodontal examination.21 It is an important consideration in the devel opment of the overall diagnosis, treatment plan, and prognosis of the dentition and can be an effective research tool.
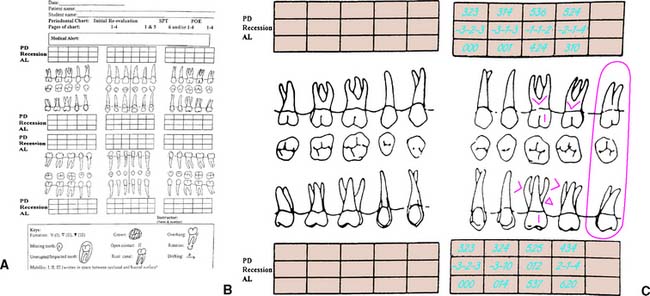
Fig. 1-18 A, Modified periodontal chart. B, Maxillary right sextant of modified periodontal chart with areas to record probing depths (PD), recession, and attachment loss (AL). C, Maxillary left sextant of modified periodontal chart exhibiting clinical documentation.
(Courtesy of the University of Detroit Mercy School of Dentistry, Department of Periodontology and Dental Hygiene, Detroit, Michigan.)
Dental Charting
An accurate charting of the state of the dentition reveals important information about the condition of the teeth and facilitates treatment planning. Adequate charting (Fig. 1-19), in addition to all periodontal information, must show the presence or absence of teeth, dental caries, restorations, wear faceting and abrasions, fractures, malformations, and erosions. Missing teeth often have an effect on the position of adjacent teeth (see also the section on arch integrity in Chapter 3). Similarly, the presence of dental caries on one interproximal surface should alert the examiner to carefully inspect the adjacent proximal wall, even if caries is not apparent radiographically. The degree and extent of caries development over time can have a considerable effect on the eventual outcome of fixed prosthodontic treatment. The condition and type of the existing restorations are noted (e.g., amalgam, cast gold, composite resin, all-ceramic). Open contacts and areas where food impaction occurs must also be identified. The presence of wear facets is indicative of sliding contact sustained over time and thus may indicate parafunctional activity (see Chapter 4). Wear facets are often easier to see on diagnostic casts, however (see Chapter 2); during the clinical examination, the location of any observed facet is recorded. Fracture lines in teeth may necessitate fixed prosthodontic intervention, although minor hairline cracks in walls that are not subject to excessive loading can often go untreated and simply be observed at recall appointments (see Chapter 32). The location of fractures should be indicated on the chart, as should any other abnormalities.
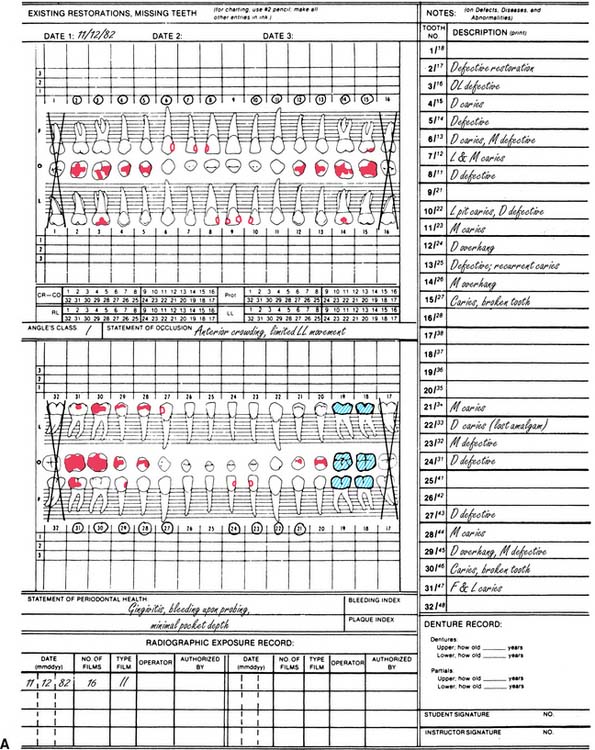
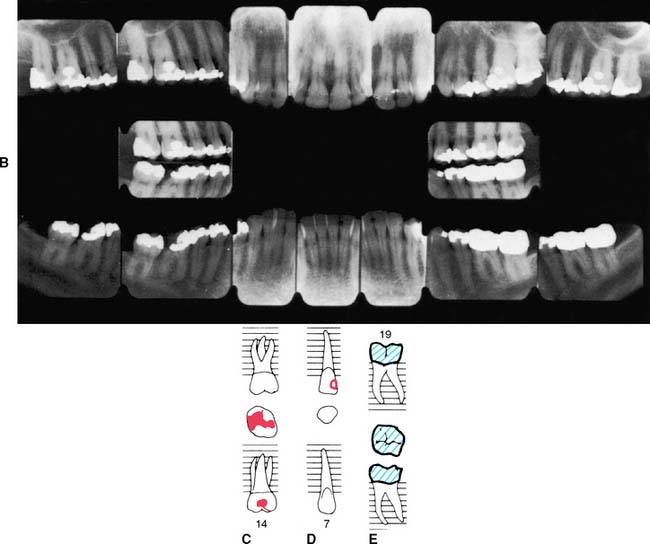
Fig. 1-19 A, An appropriate charting system designates the location, type, and extent of existing restorations and the presence of any disease condition, all of which become part of the permanent patient record. B, Radiographic findings obtained from a full-mouth series are correlated with the clinical findings and noted in the record. C to E, Charting is performed to provide a quick reference to conditions in the mouth. The following may be useful: (1) Amalgam restorations (C) are depicted by an outline drawing blocked in solidly to show the size, shape, and location of the restoration. (2) Tooth-colored restorations (D) are depicted by an outline drawing of the size, shape, and location of the restoration. (3) Gold restorations (E) are depicted by an outline drawing inscribed with diagonal lines to show the size, shape, and location of the restoration. (4) Missing teeth are denoted by a large X on the facial, lingual, and occlusal diagrams of each tooth that is not visible clinically or on radiographs. (5) Caries is recorded by circling the tooth number located at the apex of the involved tooth and noting the presence and location of the cavity in the description column corresponding to the tooth number on the right. (6) Defective restorations are recorded by circling the tooth number and noting the defect in the description column.
(Modified from Roberson T, et al: The Art and Science of Operative Dentistry, 4th ed. St. Louis, Mosby, 2002.)
Occlusal examination
The initial clinical examination starts with the clinician’s asking the patient to make a few simple opening and closing movements while the clinician carefully observes the opening and closing strokes. The objective is to determine to what extent the patient’s occlusion differs from the ideal (see Chapter 4) and how well the patient has adapted to this difference. Special attention is given to initial contact, tooth alignment, eccentric contacts, and jaw maneuverability.
Initial tooth contact
The relationship of teeth in both centric relation (see Chapter 4) and the maximum intercuspation should be assessed. If all teeth come together simultaneously at the end of terminal hinge closure, the centric relation (CR) position of the patient is said to coincide with the maximum intercuspation (MI) (see Chapters 2 and 4). The patient is guided into a terminal hinge closure to detect where initial tooth contact occurs (see the sections on bimanual manipulation and terminal hinge closure in Chapters 2 and 4). The clinician should ask the patient to “close feather-light” until any of the teeth touch and to have the patient help identify where that initial contact occurs by asking him or her to point at the location. If initial contact occurs between two posterior teeth (usually molars), the subsequent movement from the initial contact to the MI position is carefully observed and its direction noted. This is referred to as a slide from CR to MI. The presence, direction, and estimated magnitude of the slide are recorded, and the teeth on which initial contact occurs are identified. Any such discrepancy between CR and MI should be evaluated in the context of other signs and symptoms that may be present (e.g., elevated muscle tone previously observed during the extraoral examination, mobility on the teeth where initial contact occurs, wear facets on the teeth involved in the slide).
General alignment
The teeth are evaluated for crowding, rotation, supra-eruption, spacing, malocclusion, and vertical and horizontal overlap (Fig. 1-20). Teeth adjacent to edentulous spaces often have shifted position slightly. Small amounts of tooth movement can significantly affect fixed prosthodontic treatment. Tipped teeth affect tooth preparation design or, in severe cases, may result in a need for minor tooth movement before restorative treatment. Supra-erupted teeth are often overlooked clinically but frequently complicate fixed dental prosthesis design and fabrication.

Fig. 1-20 Alignment of the dentition can be assessed intraorally, although diagnostic casts allow a more detailed assessment. This patient has caries-free teeth in good alignment.
The relative relationship of adjacent teeth to teeth that require fixed prosthodontic treatment is important. A tooth may have drifted into the space previously occupied by the tooth in need of treatment because a large filling was previously lost. Such changes in alignment can seriously complicate or preclude fabrication of a cast restoration for the damaged tooth and may even necessitate its extraction.
Lateral and protrusive contacts
Excursive contacts on posterior teeth may be undesirable under certain circumstances (see Chapter 4).
The degree of vertical and horizontal overlap of the teeth is noted. When asked, most patients are capable of making an unguided protrusive movement. During this movement, the degree of posterior disclusion that results from the overlaps of the anterior teeth is observed.
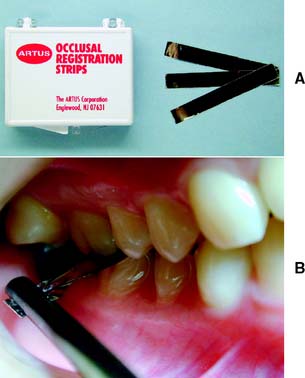
The patient is then guided into lateral excursive movements, and the presence or absence of contacts on the nonworking side and then the working side is noted. Such tooth contact in eccentric movements can be verified with a thin Mylar strip (shim stock). Any posterior cusps that hold the shim stock are evident (Fig. 1-21). Teeth that are subject to excessive loading may develop varying degrees of mobility. Tooth movement (fremitus) should be identified by palpation (Fig. 1-22). If a heavy contact is suspected, a finger placed against the buccal or labial surface while the patient lightly taps the teeth together helps locate fremitus in MI.

Jaw maneuverability
The ease with which the patient moves the jaw and the way it can be guided through hinge closure and excursive movements should be assessed, because these factors are a good guide to neuromuscular and masticatory function. If the patient has developed a pattern of protective reflexes, manipulating the jaw is difficult. The patient’s restricted maneuverability is recorded.
Radiographic Examination
Radiographs provide essential information to supplement the clinical examination. Detailed knowledge of the extent of bone support and the root structure of each standing tooth is essential for establishing a comprehensive fixed prosthodontic treatment plan. Although radiation exposure guidelines recommend limiting the number of radiographs to only those that will result in potential changes in treatment decisions, a full periapical series (Fig. 1-23) is normally required for new patients so that a comprehensive fixed prosthodontic treatment plan can be developed. Patient exposure can be minimized by using a technique that provides the most information with a minimal need for repeat films and by using appropriate protection. The use of digital radiography can further help reduce radiation exposure.
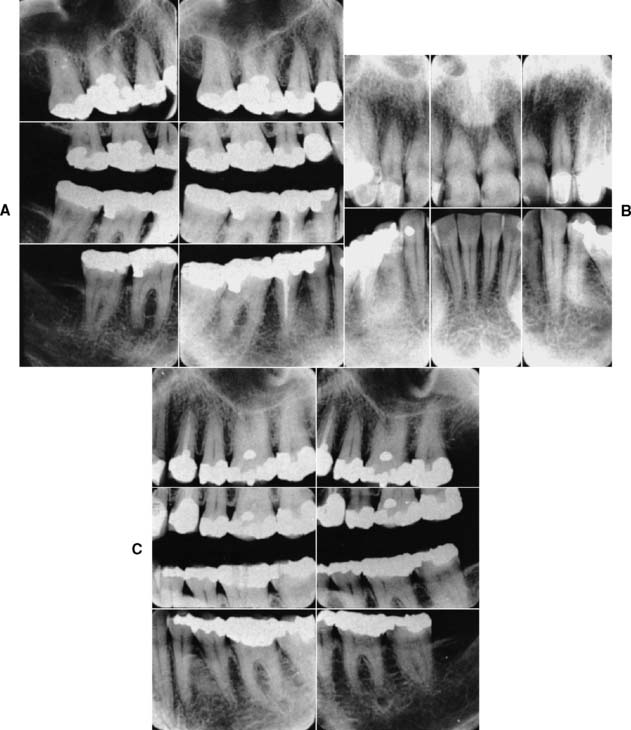
Fig. 1-23 A to C, A full-mouth radiographic survey should enable the dentist to make a detailed assessment of the structure of each tooth and its bone support.
Panoramic films (Fig. 1-24) provide useful information about the presence or absence of teeth. They are especially helpful in assessing third molars and impactions, evaluating the bone before implant placement (see Chapter 13), and screening edentulous arches for buried root tips. However, they do not provide a sufficiently detailed view for assessing bone support, root structure, caries, or periapical disease.

Fig. 1-24 A panoramic film cannot be substituted for a full-mouth series because the image is distorted. Nevertheless, it is very useful for assessing unerupted teeth, screening edentulous areas for buried root tips, and evaluating the bone before implant placement.
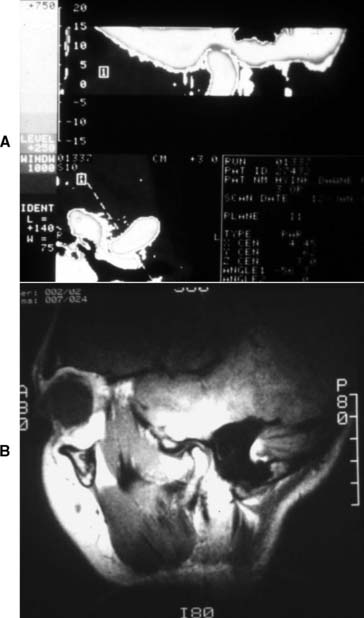
Special radiographs may be needed for the assessment of TMJ disorders and a wide variety of pathologies ranging from bone and mineral disorders to metabolic disorders, genetic abnormalities, and soft tissue calcifications such as carotid artery calcification.21 For assessment of the TMJs, a transcranial exposure (Fig. 1-25), with the help of a positioning device, reveals the lateral third of the mandibular condyle and can be used to detect structural and positional changes. However, interpretation may be difficult,22 and more information may be obtained from other images23 (Fig. 1-26).

Vitality Testing
Before any restorative treatment, pulpal health must be assessed, usually by measuring the response to gentle tapping with an instrument, or percussion, and thermal or electrical stimulation. A diagnosis of nonvitality can be confirmed by preparing a test cavity without the administration of local anesthetic. Vitality tests, however, assess only the afferent nerve supply. Misdiagnosis can occur if the nerve supply is damaged but the blood supply is intact. Careful inspection of radiographs is therefore essential in the examination of such teeth.
DIAGNOSIS AND PROGNOSIS
Not all patients seeking fixed prosthodontic treatment have diagnostic problems. Nevertheless, diagnostic errors are possible, especially when a patient complains of pain or symptoms of occlusal dysfunction. Treatment may be needed to eliminate obvious dental caries, to restore a fractured prosthesis, or to replace a missing tooth. A logical and systematic approach to diagnosis helps avoid mistakes.
Differential Diagnosis
When the history and examination are completed, a differential diagnosis is made. The practitioner should determine the most likely causes of the observed condition or conditions and record them in order of probability. A definitive diagnosis can usually be developed after such supporting evidence has been assembled.
A typical diagnosis condenses the information obtained during the clinical history taking and examination. For instance, a diagnosis could read as follows: “28-year-old male, no significant medical history; vital signs normal. Chief complaint: Mesiolingual cusp fracture on tooth #30. Teeth #1, #16, #17, #19, and #32 missing. Patient reports significant postoperative discomfort after previous molar extraction. High smile line. Caries: #6, mesial; #12, distal; #20, mesio-occlusal; and #30, mesio-occlusal-distal. Tooth #8 has received previous endodontic treatment. Generalized gingivitis four posterior quadrants, with recession noted on teeth #23, #24, and #25. 5-mm pockets on teeth #18, #30, and #31. Radiographic evidence of periapical pathology in tooth #30. Tooth #30 tests nonvital.”
This hypothetical scenario summarizes the patient’s problems, allowing subsequent prioritization as a treatment plan is developed (see Chapter 3). In this case, the patient’s chief complaint likely has a longer term history that has only recently led to symptoms that the patient could identify, causing him to seek care.
Prognosis
The prognosis is an estimation of the likely course of a disease. It can be difficult to make, but its importance to patient management and successful treatment planning must nevertheless be recognized. The prognosis of dental disorders is influenced by general factors (age of the patient, lowered resistance of the oral environment) and local factors (forces applied to a given tooth, access for oral hygiene measures). For example, a young person with periodontal disease has a more guarded prognosis than does an older person with the same disease experience. In the younger person, the disease has followed a more virulent course because of the generally less developed systemic resistance; these facts should be reflected in treatment planning.
Fixed prostheses function in a hostile environment: the moist oral environment is subject to constant changes in temperature and acidity and considerable load fluctuation. A comprehensive clinical examination helps identify the likely prognosis. All facts and observations are first considered individually and then correlated appropriately.
General factors
The overall caries rate of the patient’s dentition indicates future risk to the patient if the condition is left untreated. Important variables include the patient’s understanding and comprehension of plaque-control measures, as well as the physical ability to perform those tasks. Systemic problems analyzed in the context of the patient’s age and overall health provide important information. Diabetic patients are prone to a higher incidence of periodontal disease, and special precautionary measures may be indicated before treatment begins. Such conditions also affect the overall prognosis.
Some patients are capable of an extremely high occlusal force (see page 238), whereas others are not. If an elevated muscle tone of hypertrophied elevator muscles is identified during the extraoral examination and multiple intraoral wear facets are observed, loading of the teeth is considerably higher than in the dentition of a frail 90-year-old who tires easily when asked to close. Other important factors in determining overall prognosis are the history and success of previous dental treatments. If a patient’s previous dental care has been successful over a period of many years, a better prognosis can be anticipated than when apparently properly fabricated prostheses fail or become dislodged within a few years of initial placement.
Local factors
The observed vertical overlap of the anterior teeth has a direct effect on the load distribution in the dentition and thus can have an effect on the prognosis. In the presence of favorable loading, minor tooth mobility is less of a concern than in the presence of unfavorably directed or high load. Impactions adjacent to a molar that will be crowned may pose a serious threat in a younger individual, in whom additional growth can be anticipated, but it may be of lesser concern in an older individual.
Individual tooth mobility, root angulation, root structure, crown/root ratios, and many other variables all have an effect on the overall fixed prosthodontic prognosis. They are addressed later in this book.
Prosthodontic Diagnostic Index (PDI) for the Partially Edentulous and the Completely Dentate Patient
The American College of Prosthodontists (ACP) has developed diagnostic indices for partial edentulism24 and for the completely dentate patient25 on the basis of diagnostic findings that are summarized here with the permission and support of the ACP. These guidelines are intended to help practitioners determine appropriate treatments for their patients. For each index, four categories, Class I to Class IV, are defined; Class I represents an uncomplicated clinical situation and Class IV represents a complex clinical situation. The indices are designed for use by dental professionals involved in the diagnosis and treatment of partially edentulous and completely dentate patients. Potential benefits of the system include (1) improved intraoperator consistency, (2) improved professional communication, (3) insurance reimbursement commensurate with complexity of care, (4) improved screening tool for dental school admission clinics, (5) standardized criteria for outcomes assessment and research, (6) enhanced diagnostic consistency, and (7) simplified aid in the decision to refer a patient.
Each class is differentiated by specific diagnostic criteria (ideal or minimal, moderately compromised, substantially compromised, or severely compromised) of the following (for the partially edentulous):
For the completely dentate patient, only tooth condition and occlusal scheme are evaluated.
Location and Extent of the Edentulous Areas
In the ideal or minimally compromised edentulous area, the edentulous span is confined to a single arch and one of the following:
In the moderately compromised edentulous area, the edentulous span is in both arches, and one of the following conditions exists:
Condition of the Abutment Teeth (Tooth Condition for Completely Dentate Patients)
Ideal or minimally compromised abutment teeth condition:
Moderately compromised abutment teeth condition:
Substantially compromised abutment teeth condition:
Occlusal Scheme
Ideal or minimally compromised occlusal scheme:
Moderately compromised occlusal scheme:
Residual Ridge
The criteria published for the Classification System for Complete Edentulism26 are used to categorize any edentulous span present in the partially edentulous patient.
Classification System
The four criteria and their subclassifications are organized into an overall classification system for partial edentulism; the two criteria provide the system for completely edentulous patients.
Class I
This class (Figs. 1-27 and 1-28) is characterized by ideal or minimal compromise in the location and extent of edentulous area (which is confined to a single arch), abutment conditions, occlusal characteristics, and residual ridge conditions. All four of the diagnostic criteria are favorable.
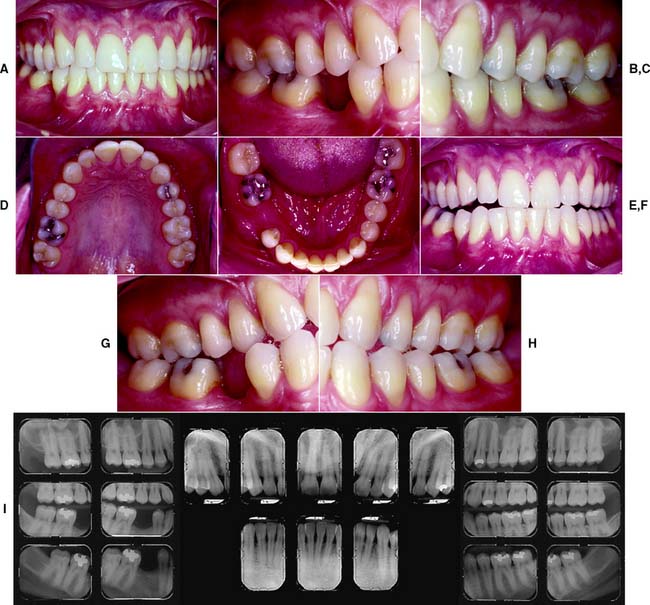
Fig. 1-27 Class I patient. This patient is categorized as Class I because of an ideal or minimally compromised edentulous area, abutment condition, and occlusion. There is a single edentulous area in one sextant. The residual ridge is considered type A. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Frontal view, protrusive relationship. G, Right lateral view, right working movements. H, Left lateral view, working movement. I, Full-mouth radiographic series.
(From McGarry TJ, et al: Classification system for partial edentulism. J Prosthodont 11:181, 2002.)

Fig. 1-28 Class I patient. The patient is categorized as Class I because an ideal or minimally compromising tooth condition, and occlusal scheme is exhibited. A single large amalgam core restoration requires a complete coverage restoration in one sextant. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Panoramic radiograph.
(From McGarry TJ, et al: Classification system for the completely dentate patient. J Prosthodont 13:73, 2004.)
The edentulous area does not compromise the physiologic support of the abutments.
The edentulous area may include any anterior maxillary span that does not exceed two incisors, any anterior mandibular span that does not exceed four missing incisors, or any posterior span that does not exceed two premolars or one premolar and one molar.
Class II
This class (Figs. 1-29 and 1-30) is characterized by moderately compromised location and extent of edentulous areas in both arches, abutment conditions necessitating localized adjunctive therapy, occlusal characteristics necessitating localized adjunctive therapy, and residual ridge conditions.

Fig. 1-29 Class II patient. This patient is categorized as Class II because he has edentulous areas in two sextants in different arches. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Frontal view, protrusive relationship. G, Right lateral view, right working movement. H, Left lateral view, left working movement. I, Full-mouth radiographic series.
(From McGarry TJ, et al: Classification system for partial edentulism. J Prosthodont 11:181, 2002.)

Fig. 1-30 Class II patient. The patient is categorized as Class II because one sextant exhibits three defective restorations with an esthetic component. Additional variables of gingival architecture and individual tooth proportions increase the complexity of diagnosis. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Panoramic radiograph.
(From McGarry TJ, et al: Classification system for the completely dentate patient. J Prosthodont 13:73, 2004.)
Class III
This class (Figs. 1-31 and 1-32) is characterized by substantially compromised location and extent of edentulous areas in both arches, abutment condition necessitating substantial localized adjunctive therapy, occlusal characteristics necessitating reestablishment of the entire occlusion without a change in the occlusal vertical dimension, and residual ridge conditions.
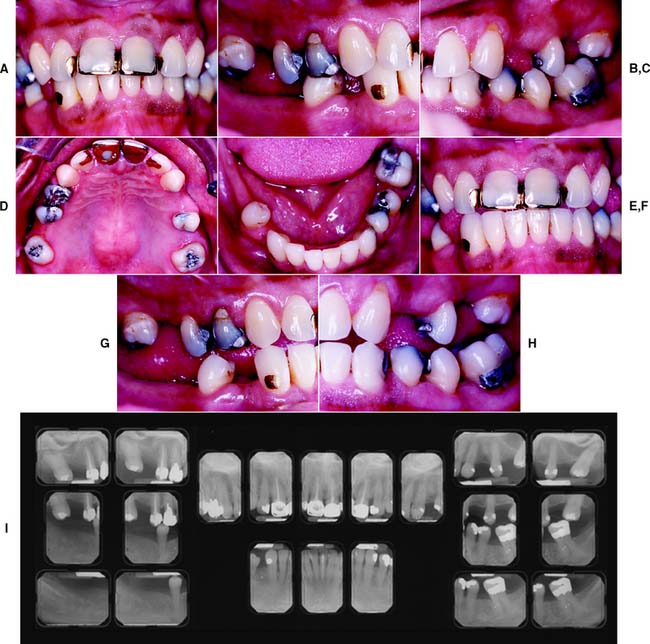
Fig. 1-31 Class III patient. This patient is categorized as Class III because the edentulous areas are located in both arches and there are multiple such locations within each arch. The abutment condition is substantially compromised as a result of the need for extracoronal restorations. There are teeth that are extruded and malpositioned. The occlusion is substantially compromised because reestablishment of the occlusal scheme is required without a change in the occlusal vertical dimension. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Frontal view, protrusive relationship. G, Right lateral view, right working movement. H, Left lateral view, left working movement. I, Full-mouth radiographic series.
(From McGarry TJ, et al: Classification system for partial edentulism. J Prosthodont 11:181, 2002.)

Fig. 1-32 Class III patient. The patient is categorized as Class III because large defective amalgam and composite restorations are present in four sextants. The remaining tooth structure is substantially compromised in most posterior teeth. The occlusion is substantially compromised, necessitating reestablishment of the occlusal scheme without a change in the occlusal vertical dimension. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Panoramic radiograph.
(From McGarry TJ, et al: Classification system for the completely dentate patient. J Prosthodont 13:73, 2004.)
Class IV
This class (Figs. 1-33 and 1-34) is characterized by severely compromised location and extent of edentulous areas with guarded prognosis, abutments requiring extensive therapy, occlusion characteristics necessitating reestablishment of the occlusion with a change in the occlusal vertical dimension, and residual ridge conditions.
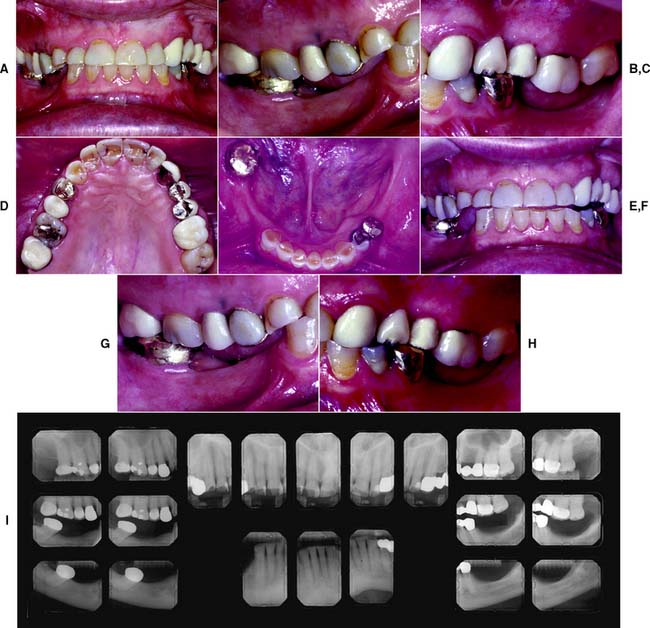
Fig. 1-33 Class IV patient. Edentulous areas are found in both arches, and the physiologic abutment support is compromised. Abutment condition is severely compromised as a result of advanced attrition and failing restorations, necessitating extracoronal restorations and adjunctive therapy. The occlusion is severely compromised, necessitating reestablishment of occlusal vertical dimension and proper occlusal scheme. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Frontal view, protrusive relationship. G, Right lateral view, right working movement. H, Left lateral view, left working movement. I, Full-mouth radiographic series.
(From McGarry TJ, et al: Classification system for partial edentulism. J Prosthodont 11:181, 2002.)

Fig. 1-34 Class IV patient. The patient is categorized as Class IV because advanced attrition of the occlusal surfaces is present in more than three sextants. The occlusion is severely compromised with the need to reestablish occlusal vertical dimension and a proper occlusal scheme. A, Frontal view, maximum intercuspation. B, Right lateral view, maximum intercuspation. C, Left lateral view, maximum intercuspation. D, Occlusal view, maxillary arch. E, Occlusal view, mandibular arch. F, Panoramic radiograph.
(From McGarry TJ, et al: Classification system for the completely dentate patient. J Prosthodont 13:73, 2004.)
Other characteristics include severe manifestations of local or systemic disease, including sequelae from oncologic treatment, maxillomandibular dyskinesia and/or ataxia, and refractoriness (a patient’s presenting with chronic complaints after appropriate therapy).
Guidelines for the Use of PDI Classification System for Partial Edentulism and the Completely Dentate Patient
The analysis of diagnostic factors is facilitated with the use of a worksheet (Tables 1-1 and 1-2). Each criterion is evaluated and a checkmark placed in the appropriate box. In instances in which a patient’s diagnostic criteria overlap two or more classes, the patient is categorized in the more complex class.
Table 1-1 WORKSHEET USED TO DETERMINE PROSTHODONTIC DIAGNOSTIC INDEX CLASSIFICATION
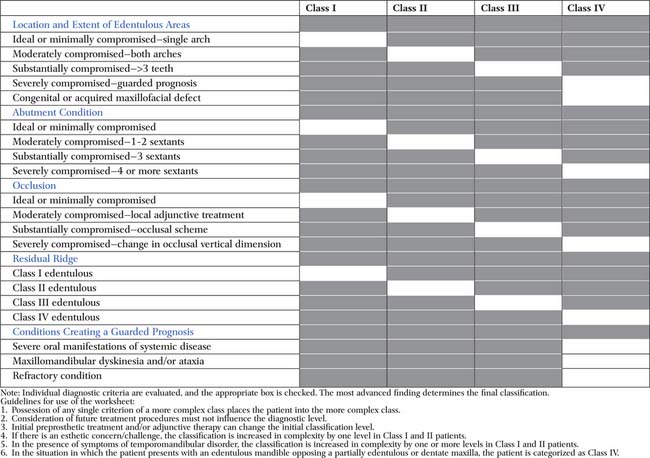 |
Table 1-2 WORKSHEET USED TO DETERMINE PROSTHODONTIC DIAGNOSTIC INDEX CLASSIFICATION OF COMPLETELY DENTATE PATIENTS
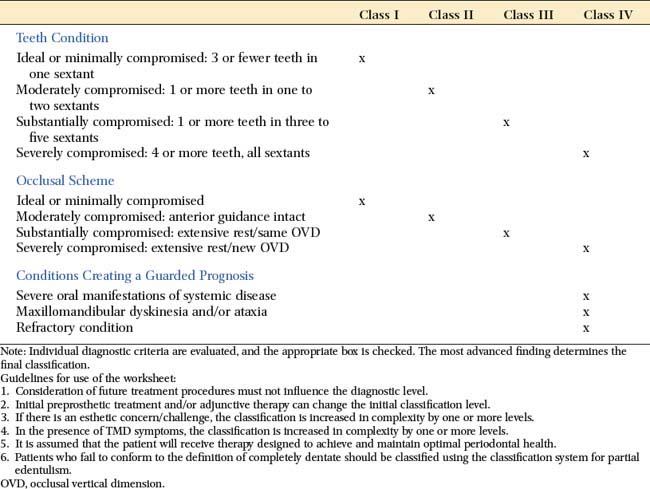
The following additional guidelines should be followed to ensure consistent application of the classification system:
The classification system for partial edentulism is based on the most objective criteria available to facilitate uniform use of the system. Such standardization may lead to improved communications among dental professionals and third parties. This classification system serves to identify patients most likely to require treatment by a specialist or by a practitioner with additional training and experience in advanced techniques. This system should also be valuable to research protocols as different treatment procedures are evaluated. With the increasing complexity of patient treatment, this partial edentulism classification system, coupled with the complete edentulism classification system, helps dental school faculty assess entering patients for the most appropriate patient assignment for better care. On the basis of use and observations by practitioners, educators, and researchers, this system is modified as needed.
SUMMARY
The history and clinical examination must provide sufficient data for the practitioner to formulate a successful treatment plan. If they are too hastily accomplished, details may be missed, which can cause significant problems during treatment, when it may be difficult or impossible to make corrections. Also, the overall outcome and prognosis may be adversely affected. In particular, it is crucial to develop a thorough understanding of special patient concerns relating to previous care and expectations about future treatment. Many problems encountered during fixed prosthodontic treatment are directly traceable to factors overlooked during the initial examination and data collection. A diagnosis is a summation of the observed problems and their underlying etiologies. The patient’s overall prognosis is influenced by general and local factors.
 GLOSSARY*
GLOSSARY*
acute closed lock \a-kyōōt′ klōzd l k\: a form of temporomandibular joint dysfunction characterized by limitation in jaw movement caused by anterior displacement of the intra-articular disc and associate with pain, limitation of jaw opening to 25 to 30 mm (as measured in the incisor area) and, with jaw opening, a deflection of the mandible toward the affected joint
k\: a form of temporomandibular joint dysfunction characterized by limitation in jaw movement caused by anterior displacement of the intra-articular disc and associate with pain, limitation of jaw opening to 25 to 30 mm (as measured in the incisor area) and, with jaw opening, a deflection of the mandible toward the affected joint
acute pain: pain having a brief and relatively severe course
al·gi·nate n (ca. 1909): see IRREVERSIBLE HYDROCOLLOID
an·am·ne·sis \ăn′ăm-nē′s s\ n, pl -ne·ses (ca. 1593): 1: a recalling to mind; a reminiscence 2: the past history of disease or injury based on the patient’s memory or recall at the time of interview and examination 3: a preliminary past medical history of a medical or psychiatric patient
s\ n, pl -ne·ses (ca. 1593): 1: a recalling to mind; a reminiscence 2: the past history of disease or injury based on the patient’s memory or recall at the time of interview and examination 3: a preliminary past medical history of a medical or psychiatric patient
anatomic crown \ăn′a-tm′k kroun\: the portion of a natural tooth that extends coronal from the cementoenamel junction—called also anatomical crown
anterior disk displacement: see DISK DISPLACEMENT
anterior guidance \ăn-tîr′ē-or gīd′ns\: 1: the influence of the contacting surfaces of anterior teeth on tooth limiting mandibular movements 2: the influence of the contacting surfaces of the guide pin and anterior guide table on articulator movements—usage see ANTERIOR GUIDE TABLE 3: the fabrication of a relationship of the anterior teeth preventing posterior tooth contact in all eccentric mandibular movements—see ANTERIOR PROTECTED ARTICULATION, GROUP FUNCTION, MUTUALLY PROTECTED ARTICULATION
anterior programming device \ăn-tîr′ē-or prō′grăm’ng d-vīs′\: an individually fabricated anterior guide table that allows mandibular motion without the influence of tooth contacts and facilitates the recording of maxillomandibular relationships; also used for deprogramming—see also deprogrammer
apex \ā′p ks′\ n, pl apex·es or api·ces \ā′p-sēz′, ăp′-\ (1601): 1: the uppermost point; the vertex 2: in dentistry, the anatomic end of a tooth root
ks′\ n, pl apex·es or api·ces \ā′p-sēz′, ăp′-\ (1601): 1: the uppermost point; the vertex 2: in dentistry, the anatomic end of a tooth root
ar·throg·ra·phy \är-thrp′a-thē\ n: 1: roentgenography of a joint after injection of an opaque contrast material 2: in dentistry, a diagnostic technique that entails filling the lower, upper, or both joint spaces of the temporomandibular joint with a contrast agent to enable radiographic evaluation of the joint and surrounding structures; used to diagnose or confirm disk displacements and perforations
1ar·tic·u·late \är-tk′ya-lāt′\ vb (1691): 1: to join together as a joint 2: the relating of contacting surfaces of the teeth or their artificial replicas in the maxillae to those in the mandible
2ar·tic·u·late \är-tk′ya-lāt′, -lt\ adj (1586): in speech, to enunciate clearly or be clearly spoken
ar·tic·u·la·tor \är-tk′ya-lā′tor\ n: a mechanical instrument that represents the temporomandibular joints and jaws, to which maxillary and mandibular casts may be attached to simulate some or all mandibular movements—usage: articulators are divisible into four classes Class I articulator: a simple holding instrument capable of accepting a single static registration. Vertical motion is possible—see NONADJUSTABLE A. Class II articulator: an instrument that permits horizontal as well as vertical motion but does not orient the motion to the temporomandibular joints. Class III articulator: an instrument that simulates condylar pathways by using averages or mechanical equivalents for all or part of the motion. These instruments allow for orientation of the casts relative to the joints and may be arcon or nonarcon instruments—see SEMI-ADJUSTABLE A. Class IV articulator: an instrument that will accept three dimensional dynamic registrations. These instruments allow for orientation of the casts to the temporomandibular joints and simulation of mandibular movements—see FULLY ADJUSTABLE A., FULLY ADJUSTABLE GNATHOLOGIC A.
aus·cul·ta·tion \ô′skal-tā′shun\ n (ca. 1828): the process of determining the condition of various parts of the body by listening to the sounds they emit
buccolingual relationship \bŭk′o-lng′gwal r-lā′shun-shp\: any position of reference relative to the tongue and cheeks
case history substand: the collected data about an individual, family, environmental factors (including medical/dental history) and any other information that may be useful in analyzing and diagnosing conditions or for instructional purposes; best termed the patient history
2cast \kăst\ n (14c): a life-size likeness of some desired form. It is formed within or is a material poured into a matrix or impression of the desired form—see DENTAL C., DIAGNOSTIC C., FINAL C., PRELIMINARY C., REFRACTORY C., REMOUNT C.
cath·ode \kăth′ōd\ n (1834): the negative pole in electrolysis
CAT : acronym for Computerized Axial Tomography
centric relation record \sn′trk r-lā′shun r-kōrd\: a registration of the relationship of the maxilla to the mandible when the mandible is in centric relation. The registration may be obtained either intraorally or extraorally
centric slide \sn′trk slīd\ obs: the movement of the mandible while in centric relation, from the initial occlusal contact into maximum intercuspation (GPT-4)
chronic pain \krn′ik pān\: pain marked by long duration or frequent recurrence
click \klk\ n (1611): a brief sharp sound; with reference to the temporomandibular joint, any bright or sharp sound emanating from the joint—see CLICKING, EARLY CLOSING C., EARLY OPENING C., LATE CLOSING C., LATE OPENING C., MID OPENING C. RECIPROCAL C.
click·ing \kl′kng\ n (611): a series of clicks, such as the snapping, cracking, or noise evident on excursions of the mandible; a distinct snapping sound or sensation, usually audible (or by stethoscope) or on palpation, which emanates from the temporomandibular joint(s) during jaw movement. It may or may not be associated with internal derangements of the temporomandibular joint
computerized tomography \kom-pyōō′ta-rīzd tō-mg′ra-fē\: (CT) the technique by which multidirectional x-ray transmission data through a body is mathematically reconstructed by a computer to form an electrical cross-sectional representation of a patient’s anatomy. CT is used as an acronym to designate any technical field associated with these techniques
condylar axis \kn′da-lar ăk′ss\: a hypothetical line through the mandibular condyles around which the mandible may rotate
condylar hinge position \kn′da-lar hnj pa-zsh′an\ obs: the position of the condyles of the mandible in the glenoid fossae at which hinge axis movement is possible (GPT-4)
crep·i·ta·tion \krp′-tā′shun\ n: a crackling or grating noise in a joint during movement, liken to the throwing of fine salt into a fire or rubbing hair between the fingers; the noise made by rubbing together the ends of a fracture
de·flec·tion \d-flk′shun\ n (1605): 1: a turning aside or off course 2: a continuing eccentric displacement of the mandibular midline incisal path symptomatic of restriction in movement
de·min·er·al·iza·tion \dē-mn′er-ă-lī-zā′shun\ n (ca. 1903): 1: loss of minerals (as salts of calcium) from the body 2: in dentistry, decalcification, usually related to the dental caries process
dental cast \dn′tl kăst\: a positive life size reproduction of a part or parts of the oral cavity
de·pro·gram·mer \dē-prō′grăm′er\ n: various types of devices or materials used to alter the proprioceptive mechanism during mandibular closure
de·vi·a·tion \dē′vē-ā′shun\ n (15c): with respect to movement of the mandible, a discursive movement that ends in the centered position and is indicative of interference during movement
diagnostic cast \dī′ag-ns′tik kăst\: a life-size reproduction of a part or parts of the oral cavity and/or facial structures for the purpose of study and treatment planning
di·a·ste·ma \dī′a-stē′ma\ n, pl -ma·ta (1854): a space between two adjacent teeth in the same dental arch
differential diagnosis \df′a-rn′shal dī′ag-nō′ss\: the process of identifying a condition by comparing the signs and symptoms of all pathologic processes that may produce similar signs and symptoms
disk derangement \dsk d-rănj′ment\: an abnormal relationship of the articular disk to the condyle, fossa, and or/and eminence
dis·tal \ds′tal\ adj (1808): remote; farther from the point of reference; away from the median sagittal plane of the face following the curvature of the dental arch
dys·func·tion \ds-fŭngk′shun\ n (ca. 1916): the presence of functional disharmony between the morphologic form (teeth, occlusion, bones, joints) and function (muscles, nerves) that may result in pathologic changes in the tissues or produce a functional disturbance
eccentric \k-sn′trk\ adj (14c): 1: not having the same center 2: deviating from a circular path 3: located elsewhere than at the geometric center 4: any position of the mandible other than that which is its normal position
en·am·el \-năm′el\ n (15c): in dentistry, the hard, thin, translucent layer of calcified substance that envelopes and protects the dentin of the coronal aspect of the tooth; it is the hardest substance in the body—called also adamantine layer
enamel projection : an apical extension of enamel, usually toward a furcation in the roots
e·ro·sion \-rō′zhun\ n (1541): 1: an eating away; a type of ulceration 2: in dentistry, the progressive loss of tooth substance by chemical processes that do not involve bacterial action producing defects that are sharply defined, wedge-shaped depressions often in facial and cervical areas—comp ABFRACTION, ABRASION, ATTRITION
etiologic factors \ē′tē-ō-lj′k făk′tors\: the elements or influences that can be assigned as the cause or reason for a disease or lesion—see LOCAL E.F., SYSTEMIC E.F.
e·ti·ol·o·gy \ē′tē-l′a-jē\ n (1555): 1: the factors implicated in the cause or origin of a disease or disorder 2: the study or theory of the factors causing disease
ex·am·in·a·tion \g-zăm′a-nā′shun\ n (14c): scrutiny or investigation for the purpose of making a diagnosis or assessment
ex·cur·sion \k-skûr′shun\ n (1577): 1: a movement outward and back or from a mean position or axis; also, the distance traversed 2: in dentistry, the movement occurring when the mandible moves away from maximum intercuspation
fac·et \făs′t\ n (1625): a small, planar surface on any hard body—see WEAR FACET—usage: the French spelling of facet, facette, has continued to confuse the profession regarding pronunciation
fixed prosthodontics \fkst prs′tha-dn′tks\: the branch of prosthodontics concerned with the replacement and/or restoration of teeth by artificial substitutes that not readily removed from the mouth
forces of mastication \fôrs-es ŭv măs′t-kā′shun\ obs: the motive force created by the dynamic action of the muscles during the physiologic act of mastication (GPT-4)
frem·i·tus \frm′-tus\ n (1879): a vibration perceptible on palpation; in dentistry, a vibration palpable when the teeth come into contact
gingival crevice \jn′ja-val krv′s\: a shallow fissure between the marginal gingiva and the enamel or cementum. It is bounded by the tooth surface on one side, the crevicular epithelium on the other, and the coronal end of the junctional epithelium at its most apical point—called also gingival sulcus
high lip line \hī lp līn\: the greatest height to which the inferior border of the upper lip is capable of being raised by muscle function
horizontal overlap \hôr′-zn-tl, hr′- ō′ver-lăp′\: the projection of teeth beyond their antagonists in the horizontal plane
id·io·path·ic \d′ē-ō-păth′k\ adj (1669): self-originated; of unknown causation
incisal guidance \n-s′zal gīd′ans\: 1: the influence of the contacting surfaces of the mandibular and maxillary anterior teeth on mandibular movements 2: the influence of the contacting surfaces of the guide pin and guide table on articulator movements
in·fra·oc·clu·sion \n′fra-a-klōō′shun\ n: malocclusion in which the occluding surfaces of teeth are below the normal plane of occlusion
initial occlusal contact \-nsh′al a-klōō′sal kn′tăkt\: during closure of the mandible, the first or initial contact of opposing teeth between the arches
in·ter·cus·pa·tion \n′ter-kŭs-pā′shun\ n, obs: the interdigitation of cusps of opposing teeth (GPT-4)
interdental papilla \n′ter-dn′tl pa-pl′a\: a projection of the gingiva filling the space between the proximal surfaces of two adjacent teeth
interocclusal distance \n′ter-a-klōō′sal ds′tans\: the distance between the occluding surfaces of the maxillary and mandibular teeth when the mandible is in a specified position
joint crepitus \joint krp′-tŭs\: the grating sensation caused by the rubbing together of the bony surfaces of joints—called also articular crepitus
lab·i·al \lā′bē-al\ adj (1594): 1: of or pertaining to the lip 2: toward the lip
la·bio·ver·sion \lā′bē-ō-vûr′shun\ n: labial position of a tooth beyond the normal arch form
leaf gauge \lēf gāj\: a set of blades or leaves of increasing thickness used to measure the distance between two points or to provide metered separation
lin·gual \lng′gwal\ adj (15c): pertaining to the tongue; next to or toward the tongue
lip line : see HIGH L.L., LOW L.L.
local etiologic factors \lō′kal ē′tē-a-lj′k făk′tarz\: the environmental influences that may be implicated in the causation, modification, and/or perpetuation of a disease entity
low lip line \lō lp līn\: 1: the lowest position of the inferior border of the upper lip when it is at rest 2: the lowest position of the superior border of the lower lip during smiling or voluntary retraction
man·di·ble \măn′da-bal\ n (15c): the lower jawbone
man·dib·u·lar \măn-db′ya-lar\ adj: of or pertaining to the mandible
mandibular hinge position \măn-db′ya-lar hnj pa-zish′an\ obs: the position of the mandible in relation to the maxilla at which opening and closing movements can be made on the hinge axis (GPT-4)
mandibular trismus \măn-db′ya-lar trz′mas\: reduced mobility of the mandible resulting from tonic contracture of the masticatory muscles
masticatory force \măs′t-ka-tôr′ē fôrs, fōrs\: the force applied by the muscles of mastication during chewing
masticatory pain \măs′t-ka-tôr′ē pān\: discomfort about the face and mouth induced by chewing or other use of the jaws but independent of local disease involving the teeth and mouth
masticatory system \măs′t-ka-tôr′ē ss′tam\: the organs and structures primarily functioning in mastication. These include the teeth with their supporting structures, craniomandibular articulations, mandible, positioning and accessory musculature, tongue, lips, cheeks, oral mucosa, and the associated neurologic complex
max·il·la \măk-sl′a\ n, pl max·il·lae \măk-sl′ē\ (15c): the irregularly shaped bone that, with its contralateral maxilla, forms the upper jaw. It assists in the formation of the orbit, the nasal cavity, and the hard palate; it contains the maxillary teeth
maxillary tuberosity \măk′sa-lr′ē tōō′ba-rs′-tē\: the most distal portion of the maxillary alveolar ridge
max·il·lo·fa·cial \măk′sa-la-fā′shul\ adj: pertaining to the dental arches, the face, head and neck structures
maxillofacial prosthesis \măk′sa-la-fā′shul prs-thē′ss\: any prosthesis used to replace part or all of any stomatognathic and/or craniofacial structure. Editorial Note: the taxonomy for maxillofacial prostheses may include modifiers (adjectives) to provide descriptive evidence of the nature of the prosthesis including anatomic location, retention, support, time, materials, and form. Frequently the means of retention is used, and may encompass descriptive adjectives such as the adjacent tissue, teeth, dental/craniofacial implants or a combination of such, thus appropriate terminology can include tissue retained MP, tooth retained MP, implant retained MP, tissue/implant retained MP. Descriptive terminology may also be included to delineate time utilization such as surgical, interim and definitive
maxillofacial prosthetics \măk′sa-la-fā′shul prs-tht′iks\: the branch of prosthodontics concerned with the restoration and/or replacement of the stomatognathic and craniofacial structures with prostheses that may or may not be removed on a regular or elective basis
me·nis·cus \ma-ns′kas\ n, pl me·nis·ci \ma-ns′ī\: see DISK
me·si·al \mē′zē-al\ adj (1803): near or toward the centerline of the dental arch; toward the median sagittal plane of the face, following the curvature of the dental arch
mo·bile \mō′bal, -bēl, -bīl\ adj (15c): capable of moving or being moved; movable
mou·lage \mōō-läzh′\ n (1902): 1: the negative impression of a body structure 2: an impression or cast made for use, especially as evidenced in a criminal investigation 3: impression or reverse likeness of a part that produces a model when converted to a positive replica, i.e., by means of plaster
MRI : acronym for Magnetic Resonance Imaging
muscle-splinting \mŭs′al-splnt′ng\ slang: involuntary contraction (rigidity) of muscles occurring as a means of avoiding the pain caused by movement of the part (resistance to passive stretch). The involved muscle(s) relaxes at rest
musculoskeletal pain \mŭs′kya-lō-skl′-tl pān\: deep, somatic pain that originates in skeletal muscles, facial sheaths, and tendons (myogenous pain), bone and periosteum (osseous pain), joint, joint capsules, and ligaments (arthralgic pain), and in soft connective tissues
myofascial trigger point \mī′a-făsh′al trg′ar point\: a hyperirritable spot, usually within a skeletal muscle or in the muscle fascia, that is painful on compression and can give rise to characteristic referred pain, tenderness (secondary hyperalgesia), and autonomic phenomena
neu·ral·gia \n
-răl′ja\ n (ca. 1822): neurogenous pain felt along the peripheral distribution of a nerve trunk
neu·ri·tis \n
-r′ts\ n (1840): inflammation of a nerve
neurogenous pain \n
-rj′a-nŭs pān\: pain that is generated within the nervous system as a result of some abnormality of neural structures
NMR : acronym for Nuclear Magnetic Resonance; a radiologic procedure that gives images in any plane without radiation or any biologic after effect by picking up signals from resonating hydrogen nuclei
nonworking side interference \nn-wûr′kng sīd n′tar-fîr′ans\: undesirable contacts of the opposing occlusal surfaces on the nonworking side
oc·clude \a-klōōd′\ vb oc·clud·ed; oc·clud·ing vt (1597): 1: to bring together; to shut 2: to bring or close the mandibular teeth into contact with the maxillary teeth
oc·clu·sal \a-klōō′zal, -sal\ adj (1897): pertaining to the masticatory surfaces of the posterior teeth, prostheses, or occlusion rims
occlusal force \a-klōō′zal, -sal fôrs, fōrs\: the result of muscular force applied on opposing teeth; the force created by the dynamic action of the muscles during the physiologic act of mastication; the result of muscular activity applied to opposing teeth
oral mucosa \ôr′al, ōr′- myōō-kō′sa\: the lining of the oral cavity
oro·phar·ynx \ôr′a-făr′ngks\ n (1887): the part of the pharynx lying between the soft palate and the upper edge of the epiglottis—called also oral pharynx, pars oralis pharyngis, pharyngooral cavity, and vestibule of the pharynx
os·te·i·tis \s′tē-ī′ts\ n (ca. 1839): inflammation of bone
os·te·o·ar·thri·tis \s′tē-ō-är-thrī′ts\ n (1878): chronic degeneration and destruction of the articular cartilage and/or fibrous connective tissue linings of the joint components and disks, leading to bony spurs, pain, stiffness, limitation of movement, and changes in bone morphology. Advanced conditions may involve erosions and disk degeneration with crepitus—syn DEGENERATIVE JOINT DISEASE
o·ver·hang \ō′var-hăng\ n (1864): excess restorative material projecting beyond a cavity or preparation margin
pal·ate \păl′t\ n (14c): see HARD P., SOFT P.
pal·pate \păl′pāt′\ vt pal·pat·ed \păl-pā′td\; pal·pat·ing \păl-pā′tng\ (1849): to examine by touch—pal·pa·tion n
panoramic radiograph \păn′a-răm′k rā′dē-ō-grăf′\: a tomogram of the maxilla and mandible taken with a specialized machine designed to present a panoramic view of the full circumferential lengths of the maxilla and mandible on a single film—called also orthopantograph
per·cus·sion \pur-kŭsh′an\ n (1544): 1: the act of striking a part with sharp blows as an aid in diagnosing the condition of the underlying parts by means of the sound obtained 2: in dentistry, striking a part with short, sharp blows as a diagnostic aid in evaluation of a tooth or dental implant by the sound obtained
per·i·ap·i·cal \pr′-ăp′-kal, ā′p-\ adj: relating to tissues surrounding the apex of a tooth, including the alveolar bone and periodontal ligament
per·i·ra·dic·u·lar \pr′-răd′-kyōō-lar\ adj: around or surrounding a tooth root
physical elasticity of muscle \fz′-kal -lă-sts′-tē, ē′lă-ŭv mŭs′al\ obs: the physical quality of muscle of being elastic; that is, yielding to active or passive physical stretch (GPT-4)
preoperative record \prē-p′ar-a-tv, -p′ra-, -p′a-rā- rk′ard\ obs: any record made for the purpose of study or treatment planning (GPT-4)
pretreatment records \prē-trēt′mant rk′ardz\: any records made for the purpose of diagnosis, recording of the patient history, or treatment planning in advance of therapy
prog·na·thism \prg-na-thz′um\ n (ca. 1864): an overgrowth of the mandible in an anteroposterior direction; a protrusion of the mandible in relation to the maxillae
prosthetic restoration \prs-tht′k\ obs: an artificial replacement for an absent part of the human body (GPT-4)
pros·tho·don·tics \prs′tha-dn′tks\ n, pl but sing or pl in constr (1947): prosthodontics is the dental specialty pertaining to the diagnosis, treatment planning, rehabilitation and maintenance of the oral function, comfort, appearance and health of patients with clinical conditions associated with missing or deficient teeth and/or maxillofacial tissues using biocompatible substitutes—see FIXED PROSTHODONTICS, IMPLANT PROSTHODONTICS, MAXILLOFACIAL PROSTHETICS, REMOVABLE PROSTHODONTICS
pros·tho·don·tist \prs′tha-dn-tst\ n (1917): 1: a specialist in prosthodontics 2: a dentist who has successfully completed an advanced education program in prosthodontics that is accredited by the appropriate accrediting body. In the United States, that body is the Commission on Dental Accreditation of the American Dental Association—see BOARD-CERTIFIED P., BOARD-ELIGIBLE P., EDUCATIONALLY QUALIFIED P.
prox·i·mal \prk′sa-mal\ adj (1727): 1: situated close to 2: next to or nearest the point of attachment or origin, a central point especially, located toward the center of a body—comp DISTAL—prox·i·mal·ly adj
pulpitis \pŭl′p-ts\ n: inflammation of the dental pulp
1ra·di·o·graph \rā′dē-ō-grăf′\ n (1880): an image produced on any sensitive surface by means of electromagnetic radiation other than light; a x-ray photograph
ra·di·o·lu·cent \rā′dē-ō-lōō′sant\: permitting the passage of radiant energy with relatively little attenuation by absorption
ra·di·o·paque \rā′dē-ō-pāk′\ (1917): a structure that strongly inhibits the passage of radiant energy
range of motion \rănj ŭv mō′shun\: the range, measured in degrees of a circle, through which a joint can be extended or flexed. The range of the opening, lateral, and protrusive excursions of the temporomandibular joint
reciprocal click \r-sp′ra-kal klk\: clicks emanating from the temporomandibular joint, one of which occurs during opening movement and the other during closing movement
reduced interarch distance \r-dōōsd′ n′tar-ärch\: an occluding vertical dimension that results in an excessive interocclusal distance when the mandible is in rest position and in a reduced interridge distance when the teeth are in contact—called also overclosure
res·to·ra·tion \rs′ta-rā′shun\ n (1660): a broad term applied to any material or prosthesis that restores or replaces lost tooth structure, teeth, or oral tissues
retruded contact position \r-trōō′dd kn′tăkt pa-zsh′an\: that guided occlusal relationship occurring at the most retruded position of the condyles in the joint cavities. A position that may be more retruded than the centric relation position
reverse articulation \r-vûrs′ är-tk′ya-lā′shun\: an occlusal relationship in which the mandibular teeth are located facial to the opposing maxillary teeth; the max illary buccal cusps are positioned in the central fossae of the mandibular teeth
root fracture \rōōt frăk′chur\: a microscopic or macroscopic cleavage of the root in any direction
sub·lin·gual \sŭb′lng′gwal\ adj (1661): pertaining to the region or structures located beneath the tongue
symp·tom \sm′tum, smp-\ n (14c): subjective evidence of disease or physical disturbance; something that indicates the presence of a bodily disorder
systemic etiologic factors \s-stm′k ē′tē-ō-lj′k făk′turs\: generalized biologic factors that are implicated in the causation, modification, and/or perpetuation of a disease entity
temporomandibular disorders \tm′pa-rō′măn-db′ya-lar ds-ôr′derz\: 1: conditions producing abnormal, incomplete, or impaired function of the temporomandibular joint(s) 2:(obs) a collection of symptoms frequently observed in various combinations first described by Costen (1934, 1937), which he claimed to be reflexes due to irritation of the auriculotemporal and/or chorda tympanic nerves as they emerged from the tympanic plate caused by altered anatomic relations and derangements of the temporomandibular joint associated with loss of occlusal vertical dimension, loss of posterior tooth support, and/or other malocclusions. The symptoms can include headache about the vertex and occiput, tinnitus, pain about the ear, impaired hearing and pain about the tongue—acronym TMD
tin·ni·tus \tn′tus\ n (1843): a noise in the ears, often described as ringing or roaring
TMD : acronym for TemporoMandibular Disorders—see TEMPOROMANDIBULAR DISORDERS
1to·mo·graph \tm′a-grăf\ n: a device for moving an x-ray source in one direction as the film moves in the opposite direction
2to·mo·graph \tm′a-grăf\ n: a radiograph produced from a machine that has the source of radiation moving in one direction and the film moving in the opposite direction
to·mo·gra·phy \tō-mg′ra-fē\ n: a general term for a technique that provides a distinct image of any selected plane through the body, while the images of structures that lie above and below that plane are blurred. Also, the term body-section radiography has been applied to the procedure, although the several ways of accomplishing it have been given distinguishing names
tor·us \tôr′us\ n, pl tori (1563): 1: a smooth rounded anatomical protuberance 2. in dentistry, prominence (s) sometimes seen on the lingual surface of the mandible and the midline of the hard palate
transcranial oblique radiograph \trăns-krā′nē-al ō-blēk′, a-blēk′ rā′dē-ō-grăf′\: a flat radiographic projection in which the central beam travels across the cranium and through the temporomandibular joint on the opposite side showing an oblique lateral view of the condyle
trau·ma \trou′ma, trô′-\ n, pl trau·ma·ta \trou′ma-ta\ or trau·mas
\trou′mas\, trau·mat·ic \trou′măt-k\ adj—trau·mat·i·cal·ly \trou′măt--kă-lē\ adv (1693): an injury or wound, whether physical or psychic
trigger point \trg′ur point\: a focus of hyperirritability in tissue which when palpated, is locally tender and gives rise to heterotopic pain
unstrained jaw relation \ŭn′r-strānd′ jô r-lā′shun\ obs: 1: the relation of the mandible to the skull when a state of balanced tonus exists among all the muscles involved 2: any jaw relation that is attained without undue or unnatural force and that causes no undue distortion of the tissues of the temporomandibular joints (GPT-4)
working side contacts \wûr′kng sīd kn′tăkts\: contacts of teeth made on the side of the articulation toward which the mandible is moved during working movements
1X-ray \ks′rā\ vt (1896): the process of exposing objects to roentgen rays and projecting their shadow on sensitized surfaces
xer·o·stomia \zîr′a-stō′mē-a\ n: dryness of the mouth from lack of normal secretions
STUDY QUESTIONS
1 Moazzez R, et al. Dental erosion, gastro-oesophageal reflux disease and saliva: how are they related? J Dent. 2004;32:489.
2 Milosevic A. Eating disorders and the dentist. Br Dent J. 1999;186:109.
3 Cope MR. Metoclopramide-induced masticatory muscle spasm. Br Dent J. 1983;154:335.
4 Pajukoski H, et al. Salivary flow and composition in elderly patients referred to an acute care geriatric ward. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:265.
5 Hunter KD, Wilson WS. The effects of antidepressant drugs on salivary flow and content of sodium and potassium ions in human parotid saliva. Arch Oral Biol. 1995;40:983.
6 . Infection control recommendations for the dental office and laboratory. J Am Dent Assoc. Suppl. 1992:1.
7 Epstein O, et al. Clinical Examination, 3rd ed. St. Louis: Mosby, 2003.
8 Little JW, et al. Dental Management of the Medically Compromised Patient, 6th ed. St. Louis: Mosby, 2002.
9 Solberg WK. Occlusion-related pathosis and its clinical evaluation. Clark JW, editor. Clinical Dentistry, vol 2. Hagerstown, Md: Harper & Row, 1976. chap 35
10 Pullinger AG, et al. Differences between sexes in maximum jaw opening when corrected to body size. J Oral Rehabil. 1987;14:291.
11 Krogh-Poulsen WG, Olsson A. Occlusal disharmonies and dysfunction of the stomatognathic system. Dent Clin North Am. 1966;10:627.
12 Moskowitz ME, Nayyar A. Determinants of dental esthetics: a rational for smile analysis and treatment. Compend Contin Educ Dent. 1995;16:1164.
13 Crispin BJ, Watson JF. Margin placement of esthetic veneer crowns. I. Anterior tooth visibility. J Prosthet Dent. 1981;45:278.
14 Lombardi RE. The principles of visual perception and their clinical application to denture esthetics. J Prosthet Dent. 1973;29:358.
15 Rosenstiel SF, Rashid RG. Public preferences for anterior tooth variations: a web-based study. J Esthet Restor Dent. 2002;14:97.
16 Parameter on comprehensive periodontal examination. American Academy of Periodontology. J Periodontol. 2000;71:847.
17 Guidelines for periodontal therapy. American Academy of Periodontology. J Periodontol. 1998;69:405.
18 Carranza FAJr, Newman MG. Clinical Periodontology, 8th ed. Philadelphia: WB Saunders, 1996.
19 Goodson JM. Selection of suitable indicators of periodontitis. In: Bader JD, editor. Risk Assessment in Dentistry. Chapel Hill, N.C.: University of North Carolina Dental Ecology, 1989.
20 American Academy of Periodontology. Parameters of Care. Chicago: American Academy of Periodontology, 1998.
21 Carter L. Clinical indications as a basis for ordering extraoral imaging studies. Compend Contin Educ Dent. 2004;25:351.
22 Van Sickels JE, et al. Transcranial radiographs in the evaluation of craniomandibular (TMJ) disorders. J Prosthet Dent. 1983;49:244.
23 Brooks SL, et al. Imaging of the temporoman-dibular joint: a position paper of the American Academy of Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:609.
24 McGarry TJ, et al. Classification system for partial edentulism. J Prosthodont. 2002;11:181.
25 McGarry TJ, et al. Classification system for the completely dentate patient. J Prosthodont. 2004;13:73.
26 McGarry TJ, et al. Classification system for complete edentulism. The American College of Prosthodontics. J Prosthodont. 1999;8:27.