20 PONTIC DESIGN
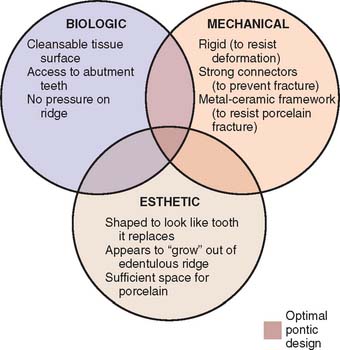
Pontics are the artificial teeth of a partial fixed dental prosthesis (FDP) that replace missing natural teeth, restoring function and appearance (Fig. 20-1). They must be compatible with continued oral health and comfort. The edentulous areas where a fixed prosthesis is to be provided may be overlooked during the treatment planning phase. Unfortunately, any deficiency or potential problem that may arise during the fabrication of a pontic is often identified only after the teeth have been prepared or even when the definitive cast is ready to be sent to the laboratory. Proper preparation includes a careful analysis of the definitive dimensions of the edentulous areas: mesiodistal width, occlusocervical distance, buccolingual dimension and location of the residual ridge. To design a pontic that meets hygienic requirements and prevents irritation of the residual ridge, particular attention must be given to the form and shape of the gingival surface. Merely replicating the form of the missing tooth or teeth is not enough. The pontic must be carefully designed and fabricated not only to facilitate plaque control of the tissue surface and around the adjacent abutment teeth but also to adjust to the existing occlusal conditions. In addition to these biologic considerations, pontic design must incorporate mechanical principles for strength and longevity, as well as esthetic principles for satisfactory appearance of the replacement teeth (Fig. 20-2).
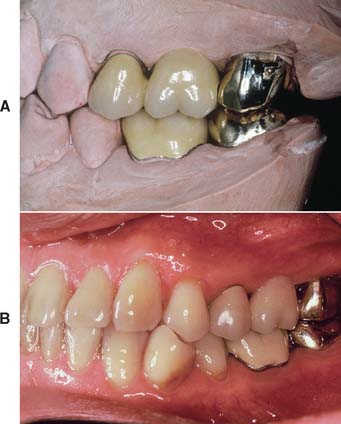
Fig. 20-1 A and B, A metal ceramic pontic in this three-unit partial fixed dental prosthesis replaces the maxillary first molar.
The pontic, as it mechanically unifies the abutment teeth and covers a portion of the residual ridge, assumes a dynamic role as a component of the prosthesis and cannot be considered a lifeless insert of gold, porcelain, or acrylic.1
PRETREATMENT ASSESSMENT
Certain procedures enhance the success of an FDP. In the treatment-planning phase, diagnostic casts and waxing procedures may prove especially valuable for determining optimal pontic design (see Chapters 2 and 3).
Pontic Space
One function of an FDP is to prevent tilting or drifting of the adjacent teeth into the edentulous space. If such movement has already occurred, the space available for the pontic may be reduced and its fabrication complicated. At this point, creating an acceptable appearance without orthodontic repositioning of the abutment teeth is often impossible, particularly if esthetic appearance is important. (Modification of abutments with complete-coverage retainers is sometimes feasible.) Careful diagnostic waxing procedures help determine the most appropriate treatment (see Chapters 2 and 3). Even with a lesser esthetic requirement, as for posterior teeth, overly small pontics are unacceptable because they trap food and are difficult to clean. When orthodontic repositioning is not possible, increasing the proximal contours of adjacent teeth may be better than making an FDP with undersized pontics (Fig. 20-3). If there is no functional or esthetic deficit, the space can be maintained without prosthodontic intervention.
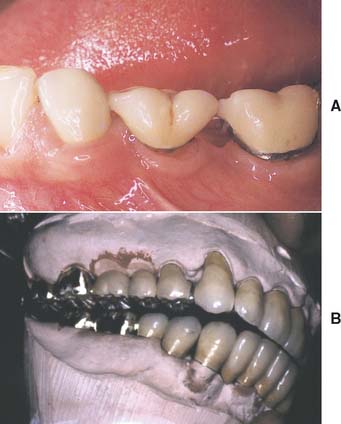
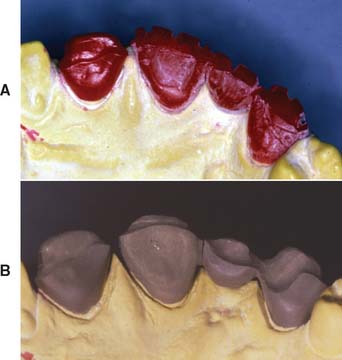
Fig. 20-3 Careful planning is always necessary in deciding how to restore an undersized pontic space where orthodontic treatment is not practical. A, In this patient, individual crowns of increased proximal contours were preferred to a partial fixed dental prosthesis with undersized pontics. Excellent plaque control had been demonstrated, and the design provided the optimum occlusal relationship. B, Here two small pontics were used to replace the missing maxillary teeth.
Residual Ridge Contour
The edentulous ridge’s contour and topography should be carefully evaluated during the treatment planning phase. An ideally shaped ridge has a smooth, regular surface of attached gingiva, which facilitates maintenance of a plaque-free environment. Its height and width should allow placement of a pontic that appears to emerge from the ridge and mimics the appearance of the neighboring teeth. Facially, it must be free of frenum attachment and be of adequate facial height to sustain the appearance of interdental papillae.
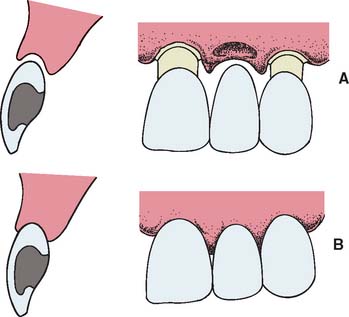
Loss of residual ridge contour may lead to unesthetic open gingival embrasures (“black triangles”) (Fig. 20-4A), food impaction (Fig. 20-4B), and percolation of saliva during speech. Siebert2 classified residual ridge deformities into three categories (Table 20-1 and Fig. 20-5):
There is a high incidence (91%) of residual ridge deformity after anterior tooth loss3; the majority of these are Class III defects. Because patients with Class II and III defects are frequently dissatisfied with the esthetics of their FDPs,4 preprosthetic surgery to augment such residual ridges should be carefully considered.

Fig. 20-4 Loss of residual ridge contour, leading to unesthetic open gingival embrasures (A) and food entrapment (arrow) (B).
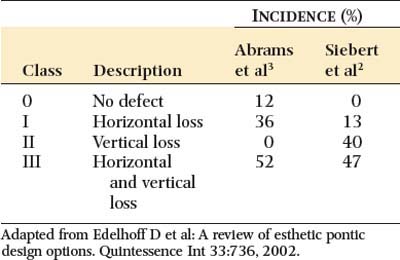
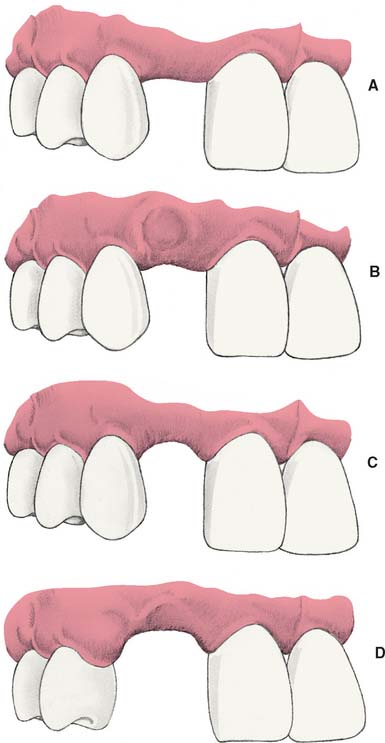
Fig. 20-5 Residual ridge deformities as classified by Siebert.2 A, Class O, no defect. B, Class I defect. C, Class II defect. D, Class III defect.
Surgical Modification
Although residual ridge width may be augmented with hard tissue grafts, this is usually not indicated unless the edentulous site is to receive an implant (see Chapter 13).
Class I defects
Soft tissue procedures have been advocated for improving the width of a Class I defect; however, because Class I defects are infrequent and are not esthetically challenging, surgical augmentation of ridge width is uncommon. Paying careful attention to interim pontic contour helps the operator identify patients who would benefit from surgery. In the roll5 technique, soft tissue from the lingual side of the edentulous site is used. The epithelium is removed, and the tissue is thinned and rolled back upon itself, thereby thickening the facial aspect of the residual ridge (Fig. 20-6). Pouches may also be prepared in the facial aspect of the residual ridge6 into which subepithelial7,8 or submucosal9 grafts harvested from the palate or tuberosity may be inserted (Fig. 20-7).
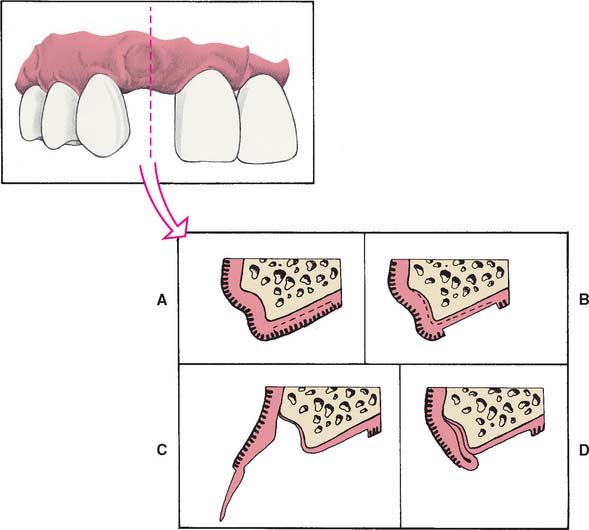
Fig. 20-6 The roll technique for soft tissue ridge augmentation. A, Cross-section of Class I residual ridge defect before augmentation. B, Epithelium removed from palatal surface. C, Elevation of flap, creating a pouch on the vestibular surface. D, The flap is rolled into the pouch, enhancing ridge width.
Class II and III defects
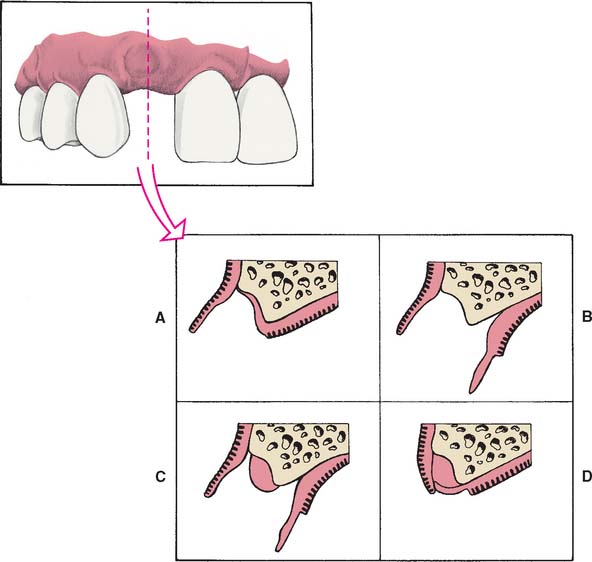
Unfortunately, few soft tissue surgical techniques can increase the height of a residual ridge with predictability. The interpositional graft2,10 is a variation of the pouch technique, in which a wedge-shaped connective tissue graft is inserted into a pouch preparation on the facial aspect of the residual ridge. The epithelial portion of the wedge may be positioned coronally to the surrounding epithelium if an increase of ridge height is desired (Fig. 20-8A and B). The onlay graft is designed to gain ridge height2,11 but also contributes to ridge width, which makes it useful for treating Class III ridge defects (Fig. 20-9). It is a thick “free gingival graft” harvested from partial- or full-thickness palatal donor sites. Because the amount of height augmentation can be only as thick as the graft, the procedure may have to be repeated several times to reestablish normal residual ridge height. Although the onlay graft has greater potential for increasing ridge height than does the interpositional graft, its survival is greatly dependent on revascularization, which requires meticulous preparation of the recipient site. Therefore, it is more technique sensitive than the interpositional graft. In fact, connective tissue grafts have been demonstrated to achieve approximately 50% more ridge volume gain 3.5 months after surgery than do free gingival grafts in single-tooth residual ridge defects.12
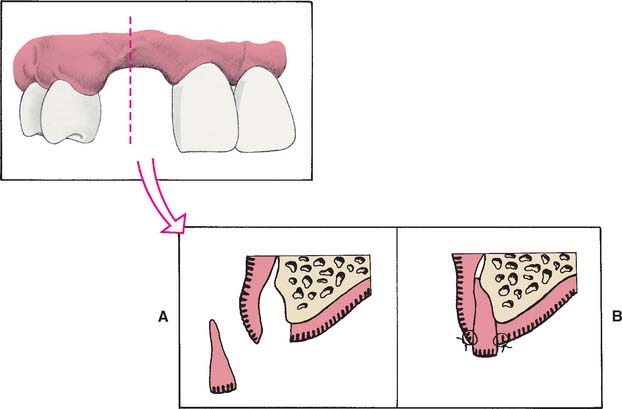
Fig. 20-8 An interpositional graft for augmentation of ridge width and height. A, Tissue reflected. B, Graft positioned and sutured in place.
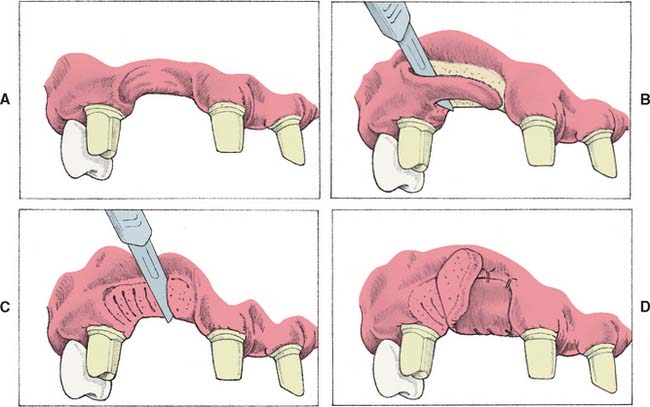
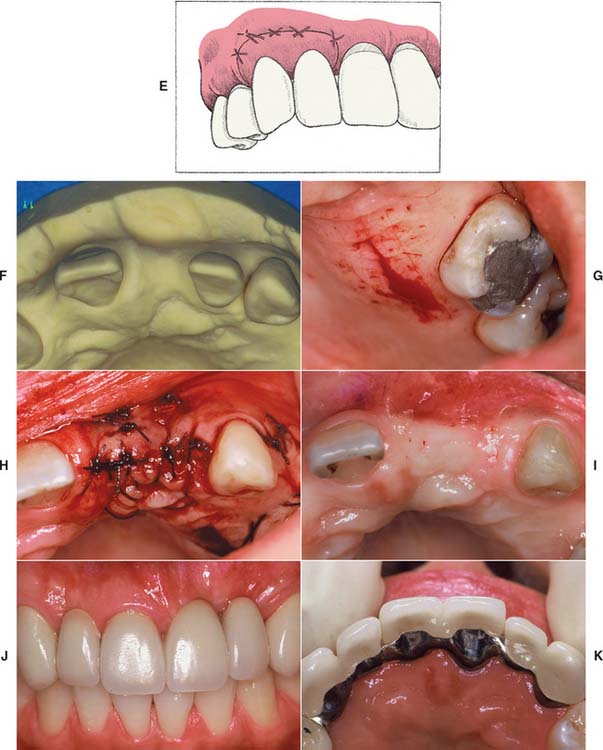
Fig. 20-9 An onlay graft for augmentation of ridge width and height. A, Presurgical view of Class III residual ridge defect with abutment teeth prepared. B, Recipient bed prepared by removing epithelium. C, Striation cuts are made in connective tissue to encourage revascularization. D, Onlay graft is sutured in place., E, An interim partial fixed dental prosthesis with open embrasures is placed immediately to allow adaptation of tissue during healing. F, Cast with Class III residual ridge defect; the lateral incisor was unrestorable. G, Donor site for graft. H, Graft sutured in place. I, Augmented ridge. J and K, Final restoration with improved contours.
Gingival Architecture Preservation
Although the degree of residual ridge resorption after tooth extraction is unpredictable, resulting deformities are not an inevitable occurrence. Preservation of the alveolar process can be achieved through immediate restorative and periodontal intervention at the time of tooth removal. By conditioning the extraction site and providing a matrix for healing, the pre-extraction gingival architecture, or “socket,” can be preserved.
Preparing the abutment teeth before the extraction is the preferred technique. An interim FDP can be fabricated indirectly, ready for immediate insertion. Because socket preservation is dependent on underlying bone contour, the extraction of the tooth to be replaced should be atraumatic and aimed at preserving the facial plate of bone. The scalloped architecture of interproximal bone forming the extraction site is essential for proper papilla form, as are facial bone levels in the prevention of alveolar collapse. If bone levels are compromised before or during extraction, the sockets can be grafted with an allograft material (hydroxyapatite, tricalcium phosphate, or freeze-dried bone).13-15
Immediately after preparation of the extraction site, a carefully shaped interim FDP is placed (Fig. 20-10A and B). The tissue side of the pontic should be an ovate form, and, according to Spear,16 it should extend approximately 2.5 mm apical to the facial free gingival margin of the extraction socket (Fig. 20-10C and D). Because the soft tissues of the socket begin to collapse immediately after the tooth extraction, the pontic causes tissue blanching as it supports the papillae and facial/palatal gingiva. The contour of the ovate tissue side of the pontic is critical and must conform to within 1 mm of the interproximal and facial bone contour to act as a template for healing. Oral hygiene in this area is difficult during the initial healing period, and so the interim restoration should be highly polished to minimize plaque retention. After approximately 1 month of healing, oral hygiene access is improved by recontouring the pontic to provide 1 to 1.5 mm of relief from the tissue. When the gingival levels are stable (approximately 6 to 12 months), the final restoration can be fabricated (Fig. 20-10E).

Fig. 20-10 Alveolar architecture preservation technique. A, Atraumatic tooth extraction. B, Cross-section view of the immediate interim partial fixed dental prosthesis, demonstrating ovate pontic form. C, Interim restoration. Note the 2.5-mm apical extension of the ovate pontic. D, The seated interim restoration should cause slight blanching of interdental papilla. E, Interim restoration 12 months after extraction. Note the preservation of interdental papilla.
(Courtesy of Dr. F.M. Spear and Montage Media, Mahwah, New Jersey.)
Techniques involving orthodontic extrusions have also been employed to preserve ridge form before extraction. In these proactive methods, light forces are used to extrude the teeth destined to be extracted. As the teeth are extruded, apposition of bone occurs at the root apex, thereby filling the socket with bone as the tooth is slowly extracted orthodontically. First employed to avoid ridge augmentation and gain vertical ridge height before immediate implant placement,17 the orthodontic extrusion technique has been used successfully to maintain ridge contour before treatment with conventional FDPs (Fig. 20-11). In addition to the additional time and expense of orthodontic treatment, because the teeth to be extracted must continuously be adjusted as they are extruded, previous endodontic treatment is necessary.
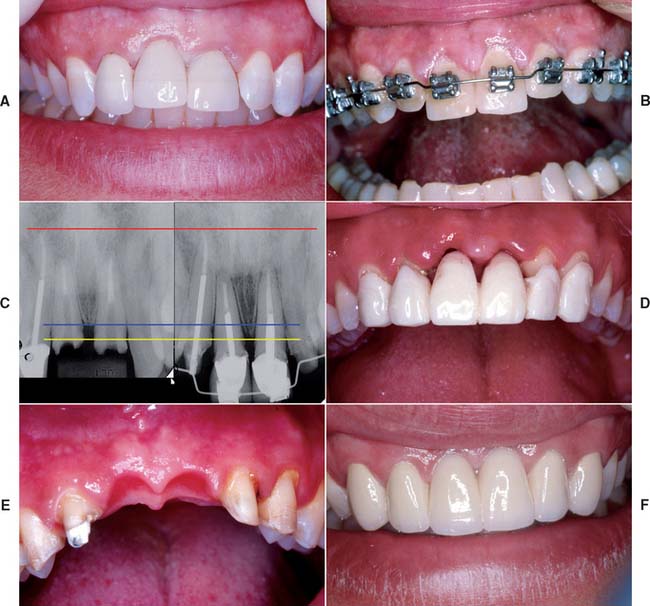
Fig. 20-11 Orthodontic extrusion to preserve alveolar architecture. A, Pretreatment (note gingival crest height discrepancy between the maxillary central incisors). B, Orthodontic extrusion. C, Pre-extrusion and post-extrusion radiographs. Red line denotes reference point; blue and yellow lines denote change in gingival crest height. D, Post-extraction evaluation of interim restoration with ovate pontics. E, Gingival architecture immediately prior to pression. F, Final restoration.
Although maintenance of the residual ridge after extraction is admirable, socket-preservation techniques are technically challenging and require frequent patient monitoring and conscientious hygiene on the part of the patient. Even when the procedure is performed meticulously, success is unpredictable because of the variability in patients’ healing response. Additional surgical augmentation of the ridge may still be necessary for some patients.
PONTIC CLASSIFICATION
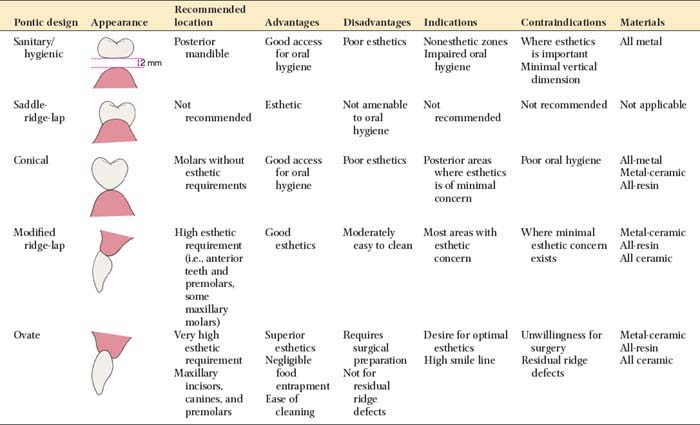
Pontic designs are classified into two general groups: those that contact the oral mucosa and those that do not (Box 20-1). There are several classifications within these groups, based on the shape of the gingival side of the pontic. Pontic selection depends primarily on esthetics and oral hygiene. In the anterior region, where esthetic appearance is a concern, the pontic should be well adapted to the tissue to make it appear as if it emerges from the gingiva. Conversely, in the posterior regions (mandibular premolar and molar areas), contours can be modified in the interest of designs that are less esthetic but amenable to oral hygiene. The advantages and disadvantages of the various pontic designs are summarized in Table 20-2.
Sanitary or Hygienic Pontic
As its name implies, the primary design feature of the sanitary pontic allows easy cleaning, because its tissue surface remains clear of the residual ridge (Fig. 20-12A). This hygienic design permits easier plaque control by allowing gauze strips and other cleaning devices to be passed under the pontic and seesawed in a shoeshine manner. Disadvantages include entrapment of food particles, which may lead to tongue habits that annoy the patient. The hygienic pontic is the least “toothlike” design and is therefore reserved for teeth seldom displayed during function (i.e., the mandibular molars).
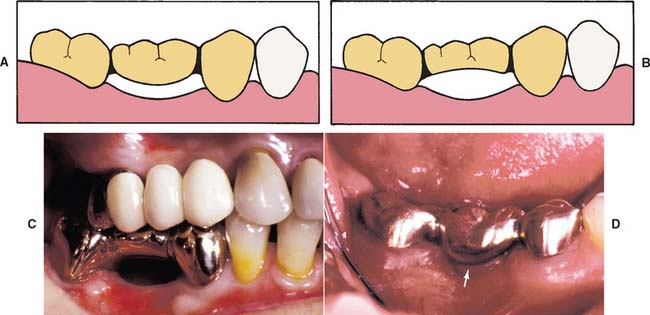
Fig. 20-12 A, Sanitary pontic. B and C, Modified sanitary pontic. D, Placement of the pontic, close to the ridge, has resulted in tissue proliferation (arrow).
A modified version of the sanitary pontic has been developed18 (Fig. 20-12B and C). Its gingival portion is shaped like an archway between the retainers. This geometry allows increased connector size while decreasing the stress concentrated in the pontic and connectors.19 It is also less susceptible to tissue proliferation that can occur when a pontic is too close to the residual ridge (Fig. 20-12D).
Saddle or Ridge Lap Pontic
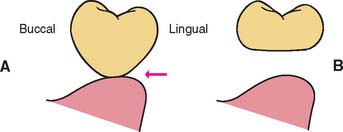
The saddle pontic has a concave fitting surface that overlaps the residual ridge buccolingually, simulating the contours and emergence profile of the missing tooth on both sides of the residual ridge. However, saddle or ridge lap designs should be avoided because the concave gingival surface of the pontic is not accessible to cleaning with dental floss, which leads to plaque accumulation (Fig. 20-13). This design deficiency has been shown to result in tissue inflammation1 (Fig. 20-14).
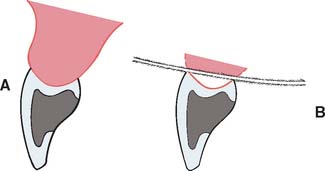
Fig. 20-13 A, Cross-section view of ridge lap pontic. B, The tissue surface is inaccessible to cleaning devices.

Fig. 20-14 A and B, Partial fixed dental prosthesis (FDP) with a ridge-lap (concave) gingival surface. C, When it was removed, the tissue was found to be ulcerated. D, The defective FDP was recontoured and used as an interim restoration while the definitive restoration was being fabricated. Within 2 weeks the ulceration had resolved.
Modified Ridge Lap Pontic
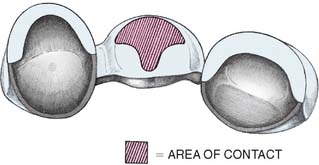
The modified ridge lap pontic combines the best features of the hygienic and saddle pontic designs, combining esthetics with easy cleaning. Figures 20-15 and 20-16 demonstrate how the modified ridge lap design overlaps the residual ridge on the facial side (to achieve the appearance of a tooth emerging from the gingiva) but remains clear of the ridge on the lingual side. To enable optimal plaque control, the gingival surface must have no depression or hollow. Rather, it should be as convex as possible from mesial to distal aspects (the greater the convexity, the easier the oral hygiene). Tissue contact should resemble a letter T (Fig. 20-17) whose vertical arm ends at the crest of the ridge. Facial ridge adaptation is essential for a natural appearance. Although this design was historically referred to as ridge-lap,20,21 the term ridge-lap is now used synonymously with the saddle design. The modified ridge lap design is the most common pontic form used in areas of the mouth that are visible during function (maxillary and mandibular anterior teeth and maxillary premolars and first molars).
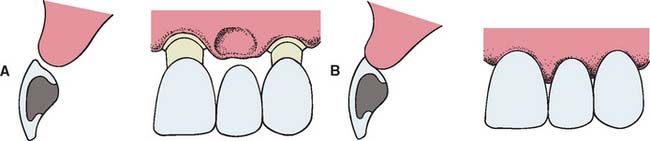
Fig. 20-15 Modified ridge lap pontic. A, Partial fixed dental prosthesis (FDP) partially seated. B, FDP seated.

Conical Pontic
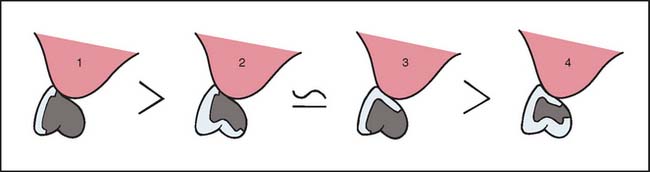
Often called egg-shaped, bullet-shaped, or heart-shaped, the conical pontic (Fig. 20-18) is easy for the patient to keep clean. It should be made as convex as possible, with only one point of contact at the center of the residual ridge. This design is recommended for the replacement of mandibular posterior teeth, where esthetic appearance is a lesser concern. The facial and lingual contours are dependent on the width of the residual ridge; a knife-edged residual ridge necessitates flatter contours with a narrow tissue contact area. This type of design may be unsuitable for broad residual ridges, because the emergence profile associated with the small tissue contact point may create areas of food entrapment (Fig. 20-19). The sanitary or hygienic pontic is the design of choice in these clinical situations.
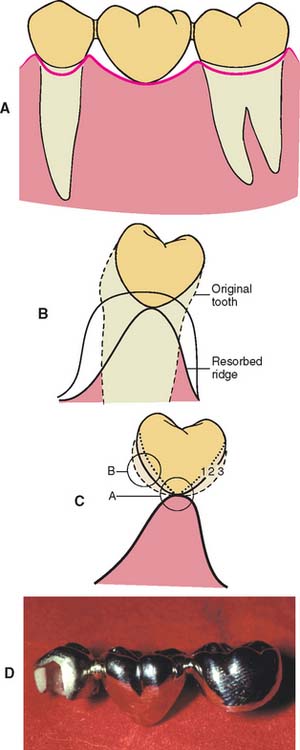
Fig. 20-18 A and B, A pontic with maximum convexity and a single point of contact with the tissue surface is the design easiest to keep clean. C, Evaluating the contour of three possible pontic shapes (1, 2, and 3). Contour 3 is the most convex in area B but is too flat in area A. Contour 1 is convex in area A but is too flat in area B. Contour 2 is the best. D, An all-metal partial fixed dental prosthesis with a conical pontic, suitable for replacement of a mandibular molar.
Ovate Pontic
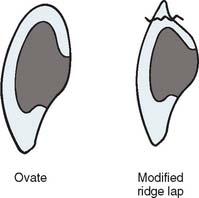
The ovate pontic is the most esthetically appealing pontic design. Its convex tissue surface resides in a soft tissue depression or hollow in the residual ridge, which makes it appear that a tooth is literally emerging from the gingiva (Fig. 20-20). Careful treatment planning is necessary for successful results. Socket-preservation techniques should be performed at the time of extraction to create the tissue recess from which the ovate pontic form will emerge. For a preexisting residual ridge, soft tissue surgical augmentation is typically required. When an adequate volume of ridge tissue is established, a socket depression is sculpted into the ridge with surgical diamonds or electrosurgery. In either case, meticulous attention to the contour of the pontic of the interim restoration is essential when the residual ridge that will receive the definitive prosthesis is conditioned and shaped.
The ovate pontic’s advantages include its pleasing appearance and its strength. When used successfully with ridge augmentation, its emergence from the ridge appears identical to that of a natural tooth. In addition, its recessed form is not susceptible to food impaction. The broad convex geometry is stronger than that of the modified ridge lap pontic, because the unsupported, thin porcelain that often exists at the gingivofacial extent of the pontic is eliminated (Fig. 20-21). Because the tissue surface of the pontic is convex in all dimensions, it is accessible to dental floss; however, meticulous oral hygiene is necessary to prevent tissue inflammation resulting from the large area of tissue contact. Other disadvantages include the need for surgical tissue management and the associated cost. Furthermore, an additional evaluation appointment is typically necessary to achieve an esthetic result. The socket depression, with its pseudopapillae, requires the support of the interim ovate pontic and will collapse when the interim restoration is removed before an impression is made. To compensate for this three-dimensional change in the socket that occurs during the impression, it is necessary to scrape the cast in this area to ensure positive contact and support of the pseudopapillae with the definitive pontic. Because these adjustment are made somewhat arbitrarily, it may also be necessary to make revisions to the tissue surface of the pontic (reshaping or porcelain additions) at the evaluation phase.
BIOLOGIC CONSIDERATIONS
The biologic principles of pontic design pertain to the maintenance and preservation of the residual ridge, abutment and opposing teeth, and supporting tissues. Factors of specific influence are pontic-ridge contact, amenability to oral hygiene, and the direction of occlusal forces.
Ridge Contact
Pressure-free contact between the pontic and the underlying tissues is indicated to prevent ulceration and inflammation of the soft tissues.1,22 If any blanching of the soft tissues is observed at evaluation, the pressure area should be identified with a disclosing medium (e.g., pressure-indicating paste) and the pontic recontoured until tissue contact is entirely passive. This passive contact should occur exclusively on keratinized attached tissue. When a pontic rests on mucosa, some ulcerations may appear as a result of the normal movement of the mucosa in contact with the pontic (Fig. 20-22). Positive ridge pressure (hyperpressure) may be caused by excessive scraping of the ridge area on the definitive cast (Fig. 20-23). This was once promoted as a way to improve the appearance of the pontic-ridge relationship. However, because of the ulceration that inevitably results when flossing is not meticulously performed, the concept is not recommended1,23,24 unless followed as previously described for an ovate pontic.22,25 Although ovate pontics maintain positive tissue contact to support the pseudopapillae, healthy mucosa can be maintained, provided that the contact to the mucosa is tight but noncompressive and the gingival portion of the pontic is regularly cleaned.26


Oral Hygiene Considerations
The chief cause of ridge irritation is the toxins released from microbial plaque, which accumulate between the gingival surface of the pontic and the residual ridge, causing tissue inflammation and calculus formation.
Unlike removable partial dental prostheses, FDPs cannot be taken out of the mouth for daily cleaning. Patients must be taught efficient oral hygiene techniques, with particular emphasis on cleaning the gingival surface of the pontic. The shape of the gingival surface, its relation to the ridge, and the materials used in its fabrication influence ultimate success.
Normally, where tissue contact occurs, the gingival surface of a pontic is inaccessible to the bristles of a toothbrush. Therefore, excellent hygiene habits must be developed by the patient. Devices such as proxy brushes, pipe cleaners, Oral-B Super Floss,* and dental floss with a threader are highly recommended (Fig. 20-24). Gingival embrasures around the pontic should be wide enough to permit oral hygiene aids. However, to prevent food entrapment, they should not be opened excessively. To enable passage of floss over its entire tissue surface, tissue contact between the residual ridge and pontic must be passive.

Fig. 20-24 The patient must be instructed in how to clean the gingival surface of a pontic with floss.
If the pontic has a depression or concavity in its gingival surface, plaque accumulates, because the floss cannot clean this area, and tissue irritation27 follows. This is usually reversible; when the surface is subsequently modified to eliminate the concavity, inflammation disappears (see Fig. 20-14). Therefore, an accurate description of pontic design should be submitted to the laboratory, and the prosthesis should be checked and corrected if necessary before cementation. Prevention is the best solution for controlling tissue irritation.
Pontic Material
Any material chosen to fabricate the pontic should provide good esthetic results where needed: biocompatibility, rigidity, and strength to withstand occlusal forces; and longevity. FDPs should be made as rigid as possible, because any flexure during mastication or parafunction may cause pressure on the gingiva and cause fractures of the veneering material. Occlusal contacts should not fall on the junction between metal and porcelain during centric or eccentric tooth contacts, nor should a metal-ceramic junction occur in contact with the residual ridge on the gingival surface of the pontic.
Investigations into the biocompatibility of materials used to fabricate pontics have centered on two factors: (1) the effect of the materials and (2) the effects of surface adherence. Glazed porcelain is generally considered the most biocompatible of the available pontic materials,28-30 and clinical data23,31 tend to support this opinion, although the crucial factor seems to be the material’s ability to resist plaque accumulation32 (rather than the material itself). Well-polished gold is smoother, less prone to corrosion, and less retentive of plaque than an unpolished or porous casting.33 However, even highly polished surfaces accumulate plaque if oral hygiene measures are ignored.34,35
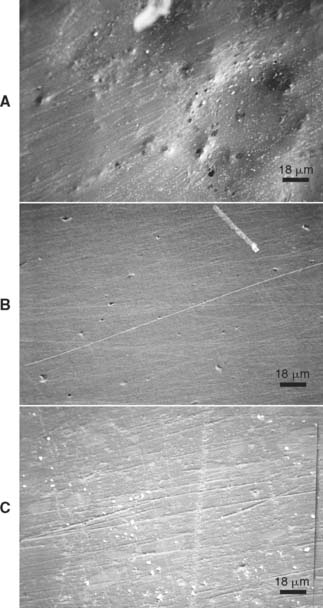
Glazed porcelain looks very smooth, but when viewed under a microscope, its surface shows many voids and is rougher than that of either polished gold or acrylic resin36 (Fig. 20-25). Nevertheless, highly glazed porcelain is easier to clean than other materials. For easier plaque removal and biocompatibility, the tissue surface of the pontic should be made in glazed porcelain. However, ceramic tissue contact may be contraindicated in edentulous areas where there is minimal distance between the residual ridge and the occlusal table. In these instances, placing ceramic on the tissue side of the pontic may weaken the design of the metal substructure, particularly with porcelain occlusal surface (Fig. 20-26). If gold is placed in tissue contact, it should be highly polished. Regardless of the choice of pontic material, patients can prevent inflammation around the pontic with meticulous oral hygiene.37
Occlusal Forces
Reducing the buccolingual width of the pontic by as much as 30% has been suggested38,39 as a way to lessen occlusal forces on, and thus the loading of, abutment teeth. This practice continues today, although it has little scientific basis. Critical analysis40 has revealed that forces are lessened only when food of uniform consistency is chewed and that a mere 12% increase in chewing efficiency can be expected from a one-third reduction of pontic width. Potentially harmful forces are more likely to be encountered if an FDP is loaded by the accidental biting on a hard object or by parafunctional activities such as bruxism, rather than by chewing of foods of uniform consistency. These forces are not reduced by narrowing the occlusal table.
In fact, narrowing the occlusal table may actually impede or even preclude the development of a harmonious and stable occlusal relationship. Like a malposed tooth, it may cause difficulties in plaque control and may not provide proper cheek support. For these reasons, pontics with normal occlusal widths (at least in the occlusal third) are generally recommended. One exception is if the residual alveolar ridge has collapsed buccolingually. Reducing pontic width may then be desired and would thereby lessen the lingual contour and facilitate plaque-control measures.
MECHANICAL CONSIDERATIONS
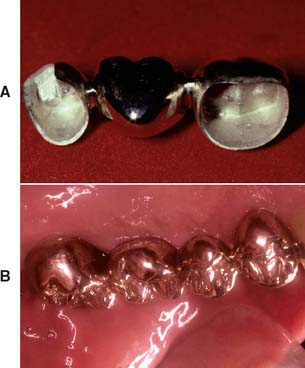
The prognosis of FDP pontics is compromised if mechanical principles are not followed closely. Mechanical problems may be caused by improper choice of materials, poor framework design, poor tooth preparation, or poor occlusion. These factors can lead to fracture of the prosthesis or displacement of the retainers. Long-span posterior FDPs are particularly susceptible to mechanical problems. Inevitably, there is significant flexing from high occlusal forces and because the displacement effects increase with the cube of the span length (see p. 98). Therefore, evaluating the likely forces on a pontic and designing accordingly are important. For example, a strong all-metal pontic may be needed in high-stress situations, rather than a metal-ceramic pontic (Fig. 20-27), which would be more susceptible to fracture. When metal-ceramic pontics are chosen, extending porcelain onto the occlusal surfaces to achieve better esthetics should also be carefully evaluated. In addition to its potential for fracture, porcelain may abrade the opposing dentition if the occlusal contacts are on enamel or metal.

Fig. 20-27 Failure of a long span metal-ceramic partial fixed dental prosthesis subjected to high stress.
Available Pontic Materials
Some FDPs are fabricated entirely of metal, porcelain, or acrylic resin, but most consist of a combination of metal and porcelain. Acrylic resin-veneered pontics have had limited acceptance because of their reduced durability (wear and discoloration). The newer indirect composites, based on high inorganic-filled resins and the fiber-reinforced materials (see Chapter 27), have revived interest in composite resin and resin-veneered pontics.
Metal-ceramic pontics
Most pontics are fabricated by the metal-ceramic technique. If properly used, this technique is helpful for solving commonly encountered clinical problems. A well-fabricated metal-ceramic pontic is strong, is easy to keep clean, and looks natural. However, mechanical failure (Fig. 20-28) can occur and often is attributable to inadequate framework design. The principles of framework design are discussed in Chapter 19, but the following points are emphasized in this chapter:



Resin-veneered pontics
Historically, acrylic resin-veneered restorations had deficiencies that made them acceptable only as longer term interim restorations. Their resistance to abrasion was lower than that of enamel or porcelain, and noticeable wear occurred with normal toothbrushing (Fig. 20-32). Furthermore, the relatively high surface area/volume ratio of a thin resin veneer made dimensional change from water absorption and thermal fluctuations (thermocycling) a problem. Because no chemical bond existed between the resin and the metal framework, the resin was retained by mechanical means (i.e., undercuts). Continuous dimensional change of the veneers often caused leakage at the metal-resin interface, with subsequent discoloration of the restoration.

Nevertheless, there are certain advantages to using polymeric materials instead of ceramics: They are easy to manipulate and repair and do not require the high–melting range alloys needed for metal-ceramic techniques. Indirect composite resin systems introduced since the 1990s have resolved some of the problems inherent in previous indirect resin veneers. These new-generation indirect resins have a higher density of inorganic ceramic filler than do traditional direct and indirect composite resins. Most are subjected to a post-curing process that results in high flexural strength, minimal polymerization shrinkage, and wear rates comparable with those of tooth enamel.41 In addition, improvements in the bond between the composite resin and metal42 may lead to a reappraisal of resin veneers.
Fiber-reinforced composite resin pontics
Composite resins can be used in partial FDPs without a metal substructure (see Chapter 27). A substructure matrix of impregnated glass or polymer fiber provides structural strength. The physical properties of this system, combined with its excellent marginal adaptation and esthetics, make it a possible metal-free alternative for FDPs, although long-term clinical performance is not yet known.
ESTHETIC CONSIDERATIONS
No matter how well biologic and mechanical principles have been followed during fabrication, the patient evaluates the result by how it looks, especially when anterior teeth have been replaced. Many esthetic considerations that pertain to single crowns also apply to the pontic (see Chapter 23). Several problems unique to the pontic may be encountered when achieving a natural appearance is attempted.
The Gingival Interface
An esthetically successful pontic replicates the form, contours, incisal edge, gingival and incisal embrasures, and color of adjacent teeth. The pontic’s simulation of a natural tooth is most often betrayed at the tissue-pontic interface. The greatest challenge here is to compensate for anatomic changes that occur after extraction. Special attention should be paid to the contour of the labial surface as it approaches the pontic-tissue junction, to achieve a “natural” appearance. This cannot be accomplished by merely duplicating the facial contour of the missing tooth, because after a tooth is removed, the alveolar bone undergoes resorption and/or remodeling. If the original tooth contour were followed, the pontic would look unnaturally long incisogingivally (Fig. 20-33). To achieve the illusion of a natural tooth, an esthetic pontic must deceive observers into believing they are seeing a natural tooth.

Fig. 20-33 Correct incisogingival height is critical to esthetic pontic design. A, Esthetic failure of a four-unit partial fixed dental prosthesis (FDP) replacing the right central and lateral incisors. The pontics have been shaped to follow the facial contour of the missing teeth, but because of bone loss they look too long. B, The replacement FDP. Note that the gingival half of each pontic has been reduced. Esthetic appearance is much improved. C, This esthetic failure is the result of excessive reduction. The central incisor pontics look too short.
The modified ridge-lap pontic is recommended for most anterior situations; it compensates for lost buccolingual width in the residual ridge by overlapping what remains. Rather than emerging from the crest of the ridge as a natural tooth would, the cervical aspect of the pontic sits in front of the ridge, covering any abnormal ridge structure resulting from tooth loss. Fortunately, because most teeth are viewed from only two dimensions, this relationship remains undetected. A properly designed, modified ridge-lap provides the required convexity on the tissue side, with smooth and open embrasures on the lingual side for ease of cleaning. This is difficult to accomplish. Clinically, many pontics are seen with less-than-optimal contour, which results in an unnatural appearance. This can be avoided with careful preparation at the diagnostic waxing stage (see Chapter 3). Sometimes the ridge tissue must be surgically reshaped to enhance the result.
In normal situations, light falls from above, and an object’s shadow is below it. Unexpected lighting or unexpectedly placed shadows (Fig. 20-34) can be confusing to the brain. Because of past experience, the brain “knows” that a tooth grows out of the gingiva, and it therefore “sees” a pontic as a tooth unless telltale shadows suggest otherwise. Special care must be taken in studying where shadows fall around natural teeth, particularly around the gingival margin. If a pontic is poorly adapted to the residual ridge, there is an unnatural shadow in the cervical area that looks odd and spoils the illusion of a natural tooth (Fig. 20-35). In addition, recesses at the gingival interface collect food debris, further betraying the illusion of a natural tooth.
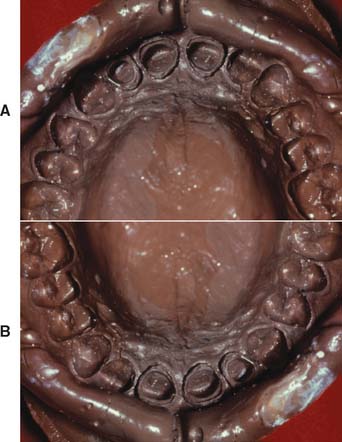
Fig. 20-34 Optical illusion. A and B are identical except that one image is upside down. Most people make different three-dimensional interpretations of each photograph, interpreting one as a negative impression and the other as a positive cast. (Verify the illusion by turning the book.) The interpretation is based on how shadows fall; in normal situations, objects are seen illuminated from above.
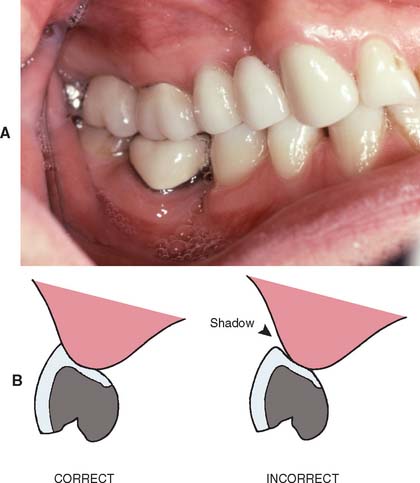
Fig. 20-35 A pontic should be interpreted as “growing” out of the gingival tissue. The second premolar pontic in the four-unit partial fixed dental prosthesis (A) is successful because it is well adapted to the ridge; however, the pontic for the first premolar is evident because of its poor adaptation to the ridge, which creates a shadow. B, Shadows around the gingival surface (arrow) spoil the esthetic illusion.
When appearance is of utmost concern, the ovate pontic, used in conjunction with alveolar preservation or soft tissue ridge augmentation, can provide an appearance at the gingival interface that is virtually indistinguishable from that of a natural tooth. Because it emerges from a soft tissue recess, this pontic is not susceptible to many of the esthetic pitfalls applicable to the modified ridge lap pontic. However, in most cases, the patient must be willing to undergo the additional surgical procedures that an ovate pontic requires.
Incisogingival Length
Obtaining a correctly sized pontic simply by duplicating the original tooth is not possible. Ridge resorption makes such a pontic look too long in the cervical region. The height of a tooth is immediately obvious when the patient smiles and shows the gingival margin (Fig. 20-36). An abnormal labiolingual position or cervical contour, however, is not immediately obvious. This fact can be used to produce a pontic of good appearance by recontouring the gingival half of the labial surface (see Fig. 20-36). The observer sees a normal tooth length but is unaware of the abnormal labial contour. The illusion is successful.
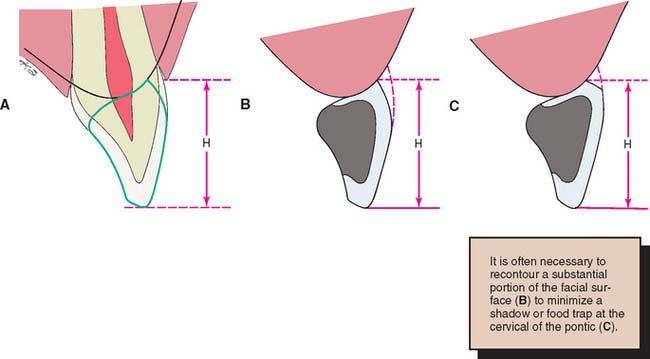
Fig. 20-36 A, A pontic should have the same incisogingival height (H) as the original tooth. B, Correctly contoured pontic. C, Incorrectly contoured pontic. (The dotted lines in B and C show the original tooth contour.) The shelf at the gingival margin may trap food and create an esthetically unacceptable shadow.
Even with moderately severe bone resorption, obtaining a natural appearance by exaggerated contouring of the pontics may still be possible. In areas where tooth loss is accompanied by excessive loss of alveolar bone, however, a pontic of normal length would not touch the ridge at all.
One solution is to shape the pontic to simulate a normal crown and root with emphasis on the cementoenamel junction. The root can be stained to simulate exposed dentin (Fig. 20-37). Another approach is to use pink porcelain to simulate the gingival tissues (Fig. 20-38). However, such pontics then have considerably increased tissue contact and require scrupulous plaque control for long-term success. Ridge augmentation procedures have been successful in correcting areas of limited resorption. When bone loss is severe, the esthetic result obtained with a partial removable dental prosthesis is often better than with an FDP.
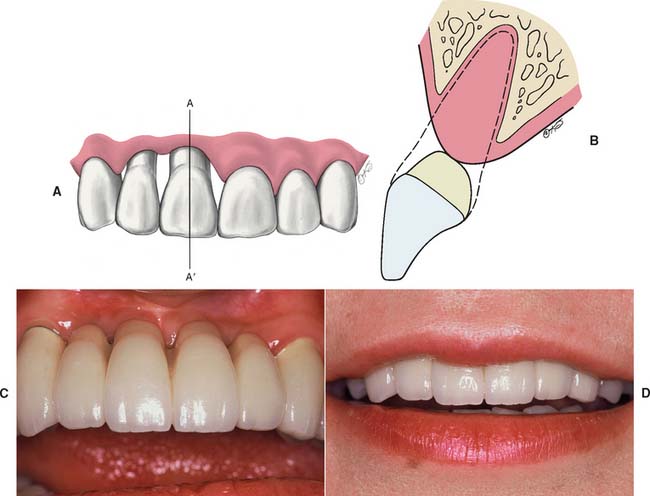
Fig. 20-37 It is difficult without surgical augmentation to fabricate an esthetic fixed prosthesis for a patient with extensive alveolar bone loss. A to D, One approach is to contour the crowns normally and shape and stain the apical extension to simulate exposed root surface.
(A and B, Redrawn from Blancheri RL: Optical illusions and cosmetic grinding. Rev Asoc Dent Mex 8:103, 1950.)

Fig. 20-38 Partial fixed dental prosthesis replacing maxillary left central and lateral incisors. This patient had lost significant bone from the edentulous ridge. A and B, Appearance of the prosthesis was enhanced with the use of pink porcelain between the pontics to simulate gingival tissue. The patient has been able to maintain excellent tissue health through the daily use of Oral-B Super Floss.
Mesiodistal Width
Frequently, the space available for a pontic is greater or smaller than the width of the contralateral tooth. This is usually because of uncontrolled tooth movement that occurred when a tooth was removed and not replaced.
If possible, such a discrepancy should be corrected by orthodontic treatment. If this is not possible, an acceptable appearance may be obtained by incorporating visual perception principles into the pontic design. In the same way that the brain can be confused into misinterpreting the relative sizes of shapes or lines because of an erroneous interpretation of perspective (Fig. 20-39), a pontic of abnormal size may be designed to give the illusion of being a more natural size. The width of an anterior tooth is usually identified by the relative positions of the mesiofacial and distofacial line angles, and the overall shape by the detailed pattern of surface contour and light reflection between these line angles. The features of the contralateral tooth (Fig. 20-40) should be duplicated as precisely as possible in the pontic, and the space discrepancy can be compensated by altering the shape of the proximal areas. The retainers and the pontics can be proportioned to minimize the discrepancy. (This is another situation in which a diagnostic waxing procedure helps solve a challenging restorative problem.)
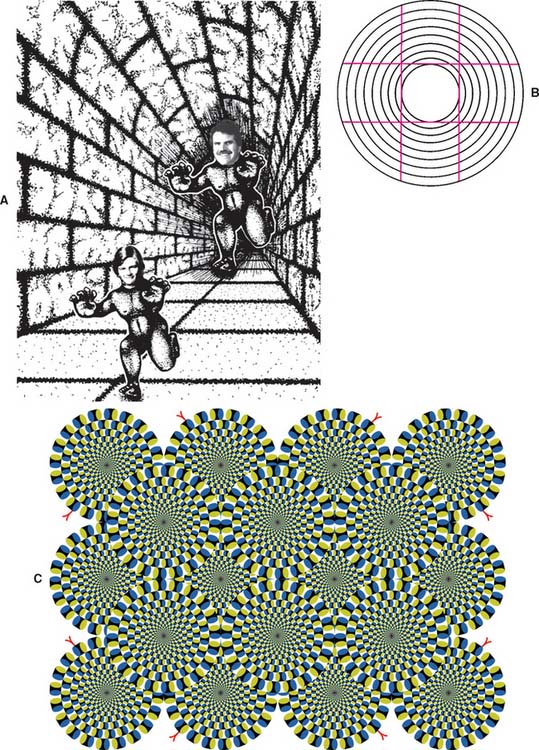
Fig. 20-39 Optical illusions. A, The authors are the same size. B, The lines are straight. (Tilt the book to verify this.) C, Kitaoka’s “Rotating Snake” Illusion. Look at this one close up. Rotation of the “wheels” occurs in relation to eye movements. On steady fixation the effect vanishes.44
(A, Modified from Shepard RN: MindSights. New York, WH Freeman, 1990; C, © Akiyoshi Kitaoka 2003, reproduced by permission.)
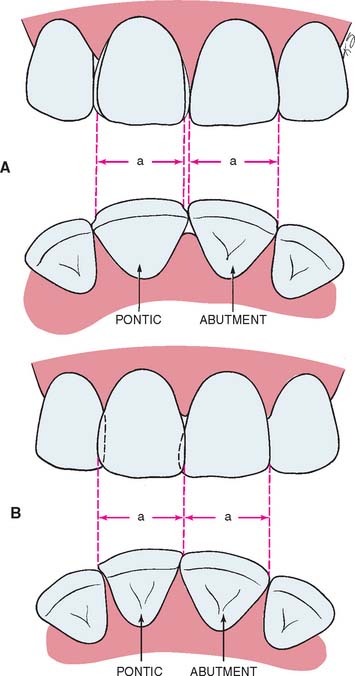
Fig. 20-40 An abnormally sized anterior pontic space can be restored esthetically by matching the location of the line angles and adjusting the interproximal areas. Large (A) and small (B) pontic spaces. Dimension a should be matched in the replacement.
(Redrawn from Blancheri RL: Optical illusions and cosmetic grinding. Rev Asoc Dent Mex 8:103, 1950.)
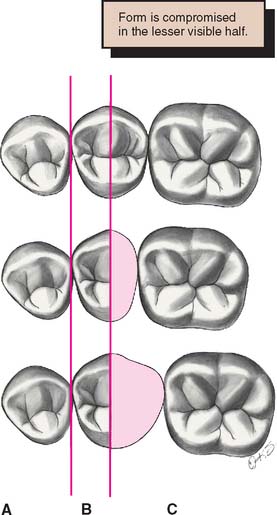
Space discrepancy presents less of a problem when posterior teeth are being replaced (Fig. 20-41) because their distal halves are not normally visible from the front. A discrepancy here can be managed by duplicating the visible mesial half of the tooth and adjusting the size of the distal half.
PONTIC FABRICATION
Available Materials
Over time, several techniques for pontic fabrication have evolved. Prefabricated porcelain facings were very popular for use with conventional gold alloys. As use of the metal-ceramic technique increased during the 1970s, prefabricated facings lost their popularity and essentially disappeared. Although an acceptable substitute, custom-made metal-ceramic facings never gained widespread acceptance. Table 20-3 summarizes the various techniques (Fig. 20-42).
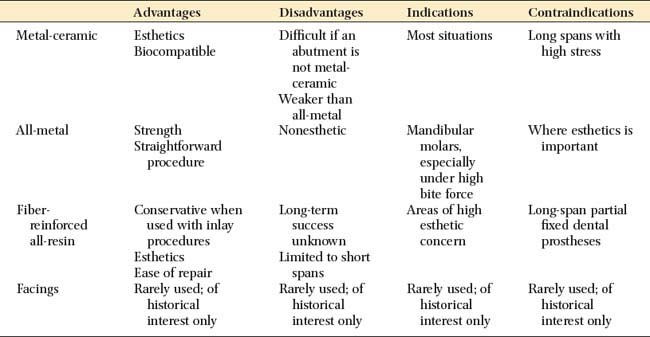

Fig. 20-42 A, Eight-unit partial fixed dental prosthesis (FDP) with porcelain facings. B and C, This three-unit posterior FDP has been fabricated by post-ceramic soldering of a metal-ceramic facing to conventional gold. D, Metal-ceramic FDP with a modified ridge lap pontic (canine) that appears to emerge from the gingiva.
Most pontics are now made with the metal-ceramic technique, which provides the best solution to the biologic, mechanical, and esthetic challenges encountered in pontic design. Their fabrication, however, differs slightly from the fabrication of individual crowns. These differences are emphasized in the ensuing paragraphs.
Metal-Ceramic Pontics
A well-designed metal-ceramic pontic allows for easy plaque removal, strength, wear resistance, and good esthetics (see Fig. 20-42D). Its fabrication is relatively simple if at least one retainer is also metal-ceramic. The metal framework for the pontic and one or both of its retainers is then cast in one piece. This facilitates pontic manipulation during the successive laboratory and clinical phases. In the following discussion, it is assumed that either one or both of the retainers are metal-ceramic complete crowns. When this is not the case, an alternative approach is necessary.
Anatomic contour waxing
For strength and esthetics, an accurately controlled thickness of porcelain is needed in the finished restoration. To ensure this, a wax pattern is made to the final anatomic contour. This also enables an assessment of connector design adequacy and the relationship between the connectors and the proposed configuration of the ceramic veneer (see Chapter 28).
Armamentarium (Fig. 20-43)

Step-by-step procedure


Evaluation
The form of the wax pattern is evaluated (Fig. 20-46), and any deficiencies are corrected. Particular attention is given to the connectors, which should have the correct shape and size. The connectors provide firm attachment for the pontic so that it does not separate from the retainers during the subsequent cut-back procedure.

Cut-back
Step-by-step procedure
When one connector of a three-unit FDP is to be cast and the other soldered, the cast connector should be sectioned first when the foregoing procedure is followed. The gingival surface of the pontic should be cut back in the metal rather than in the wax, because the tissue contact helps stabilize the pontic. Access is difficult, and it is easy to break the fragile wax connector.

Metal preparation
Step-by-step procedure

Evaluation
Less than 1 mm of porcelain thickness is needed on the gingival surface, because once it is cemented, the restoration is seen from the facial rather than from the gingival side. Excessive gingival porcelain is a common fault in pontic framework design and may lead to fracture and poor appearance (see Fig. 20-29).
To facilitate plaque control, the metal-ceramic junction should be located lingually. Then tissue contact is on the porcelain and not on metal, which retains plaque more tenaciously.43
Porcelain application
Many of the steps for porcelain application are identical to those in individual crown fabrication (see Chapter 24). There are some features peculiar to pontic fabrication, however, and these are emphasized.
Armamentarium (Fig. 20-49)

Step-by-step procedure

Evaluation
The porcelain on the tissue surface of the pontic should be as smooth as possible (Fig. 20-51). Pits and defects make plaque control difficult and promote calculus formation. The metal framework must be highly polished, with special care directed to the gingival embrasures (where access for plaque removal is more difficult).

All-Metal Pontics
Pontics made from metal (Fig. 20-52) require fewer laboratory steps and are therefore sometimes used for posterior FDPs. However, they have some disadvantages (e.g., their appearance). In addition, investing and casting must be done carefully because the mass of metal in the pontic is prone to porosity as the bulk increases. A porous pontic retains plaque and tarnishes and corrodes rapidly.
SUMMARY
Designs that allow easy plaque control are especially important to a pontic’s long-term success. Minimizing tissue contact by maximizing the convexity of the pontic’s gingival surface is essential. Special consideration is also needed to create a design that combines easy maintenance with natural appearance and adequate mechanical strength. When the appropriate design has been selected, it must be accurately conveyed to the dental technician.
There are subtle differences between metal-ceramic pontic fabrication and the fabrication of other types of pontics. Under most circumstances, the metal-ceramic technique is used because it is straightforward and practical. However, it requires careful execution for maximum strength, appearance, and effective plaque control. Alternative procedures are sometimes helpful, particularly when gold alloys are used for the retainers. Resin-veneered pontics should be restricted to use as longer-term interim restorations, and all-metal pontics may be the restoration of choice in nonesthetic situations, particularly those in which forces are high.
 GLOSSARY*
GLOSSARY*
aug·men·ta·tion \ôg′m n-tā′shun\ n (14c): to increase in size beyond the existing size. In alveolar ridge augmentation, bone grafts or alloplastic materials are used to increase the size of an atrophic alveolar ridge
n-tā′shun\ n (14c): to increase in size beyond the existing size. In alveolar ridge augmentation, bone grafts or alloplastic materials are used to increase the size of an atrophic alveolar ridge
back·ing \băk′ ng\ n (1793): a metal support that attaches a facing to a prosthesis
ng\ n (1793): a metal support that attaches a facing to a prosthesis
center of the ridge \sn′ter ŭv thē rj\: the faciolingual or buccolingual mid-line of the residual ridge
clinical crown \kln′-kel kroun\: the portion of a tooth that extends from the occlusal table or incisal edge to the free gingival margin
connective tissue \ka-nk′tv tsh′ōō\: a tissue of mesodermal origin rich in interlacing processes that supports or binds together other tissues
crest \krst\ n (14c): a ridge or prominence on a part of a body; in dentistry, the most coronal portion of the alveolar process
crest of the ridge \krst ŭv tha rj\: the highest continuous surface of the residual ridge—not necessarily coincident with the center of the ridge
emergence profile \-mûr′jens prō′fīl\: the contour of a tooth or restoration, such as a crown on a natural tooth or dental implant abutment, as it relates to the adjacent tissues
hygienic pontic \hī′jē-n′k, hī-jn′-pōn′tk\: a pontic that is easier to clean because it has a domed or bullet shaped cervical form and does not overlap the edentulous ridge
modified ridge lap \m d′a-fīd′ rj lăp\: a ridge lap surface of a pontic that is adapted to only the facial or buccal aspect of the residual ridge
d′a-fīd′ rj lăp\: a ridge lap surface of a pontic that is adapted to only the facial or buccal aspect of the residual ridge
ovate pontic : a pontic that is shaped on its tissue surface like an egg in two dimensions, typically partially submerged in a surgically-prepared soft-tissue depression to enhance the illusion that a natural tooth is emerging from the gingival tissues
pon·tic \pn′tk\ n: an artificial tooth on a fixed dental prosthesis that replaces a missing natural tooth, restores its function, and usually fills the space previously occupied by the clinical crown
residual ridge \r-zj′ōō-al rj\: the portion of the residual bone and its soft tissue covering that remains after the removal of teeth
residual ridge crest \r-zj′ōō-al rj krst\: the most coronal portion of the residual ridge
residual ridge resorption \r-zj′ōō-al rj rē-sôrb′ shun, -zôrb′-\: a term used for the diminishing quantity and quality of the residual ridge after teeth are removed (Ortman HR. Factors of bone resorption of the residual ridge. J PROSTHET DENT 1962;12:429–40.
Atwood DA. Some clinical factors related to rate of resorption of residual ridges. J PROSTHET DENT 1962;12:441–50.)
ridge augmentation \rj ôg′mn-tā′shun\: any procedure designed to enlarge or increase the size, extent, or quality of deformed residual ridge
ridge crest \rj krst\: the highest continuous surface of the residual ridge not necessarily coincident with the center of the ridge
ridge lap \rj lăp\: the surface of an artificial tooth that has been shaped to accommodate the residual ridge. The tissue surface of a ridge lap design is concave and envelops both the buccal and lingual surfaces of the residual ridge
sanitary pontic obs: a trade name originally designed as a manufactured convex blank with a slotted back. The name was used occasionaly as a synonym for a hygienic pontic, wherein the pontic does not contact the residual ridge
STUDY QUESTIONS
1 Stein RS. Pontic-residual ridge relationship: a research report. J Prosthet Dent. 1966;16:251.
2 Siebert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. I. Technique and wound healing. Compend Contin Educ Dent. 1983;4:437.
3 Abrams H, et al. Incidence of anterior ridge deformities in partially edentulous patients. J Prosthet Dent. 1987;57:191.
4 Hawkins CH, et al. Ridge contour related to esthetics and function. J Prosthet Dent. 1991;66:165.
5 Abrams L. Augmentation of the deformed residual edentulous ridge for fixed prosthesis. Compend Contin Educ Dent. 1980;1:205.
6 Garber DA, Rosenberg ES. The edentulous ridge in fixed prosthodontics. Compend Contin Educ Dent. 1981;2:212.
7 Langer B, Calagna L. The subepithelial connective tissue graft. J Prosthet Dent. 1980;44:363.
8 Smidt A, Goldstein M. Augmentation of a deformed residual ridge for the replacement of a missing maxillary central incisor. Pract Periodont Aesthet Dent. 1999;11:229.
9 Kaldahl WB, et al. Achieving an esthetic appearance with a fixed prosthesis by submucosal grafts. J Am Dent Assoc. 1982;104:449.
10 Meltzer JA. Edentulous area tissue graft correction of an esthetic defect: a case report. J Periodontol. 1979;50:320.
11 McHenry K, et al. Reconstructing the topography of the mandibular ridge with gingival autografts. J Am Dent Assoc. 1982;104:478.
12 Studer SP, et al. Soft tissue correction of a single-tooth pontic space: a comparative quantitative volume assessment. J Prosthet Dent. 2000;83:402.
13 Nemcovsky CE, Vidal S. Alveolar ridge preservation following extraction of maxillary anterior teeth. Report on 23 consecutive cases. J Periodontol. 1996;67:390.
14 Bahat O, et al. Preservation of ridges utilizing hydroxylapatite. Int J Periodontol Res Dent. 1987;6:35.
15 Lekovic V, et al. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J Periodontol. 1997;68:563.
16 Spear FM. Maintenance of the interdental papilla following anterior tooth removal. Pract Periodont Aesthet Dent. 1999;11:21.
17 Ingber JS. Forced eruption. II. A method of treating nonrestorable teeth—periodontal and restorative considerations. J Periodontol. 1976;47:203.
18 Perel ML. A modified sanitary pontic. J Prosthet Dent. 1972;28:589.
19 Hood JA, et al. Stress and deflection of three different pontic designs. J Prosthet Dent. 1975;33:54.
20 Shillingburg HT, et al. Fundamentals of Fixed Prosthodontics, 2nd ed., Chicago: Quintessence Publishing; 1981:387.
21 Eissmann HF, et al. Physiologic design criteria for fixed dental restorations. Dent Clin North Am. 1971;15:543.
22 Tripodakis AR, Constandinides A. Tissue response under hyperpressure from convex pontics. Int J Periodont Restorative Dent. 1990;10:409.
23 Cavazos E. Tissue response to fixed partial denture pontics. J Prosthet Dent. 1968;20:143.
24 Henry PJ, et al. Tissue changes beneath fixed partial dentures. J Prosthet Dent. 1966;16:937.
25 Jacques LB, et al. Tissue sculpturing: an alternative method for improving esthetics of anterior fixed prosthodontics. J Prosthet Dent. 1999;81:630.
26 Zitzmann NU, et al. The ovate pontic design: a histologic observation in humans. J Prosthet Dent. 2002;88:375.
27 Hirshberg SM. The relationship of oral hygiene to embrasure and pontic design: a preliminary study. J Prosthet Dent. 1972;27:26.
28 McLean JW. The Science and Art of Dental Ceramics, vol 2. Chicago: Quintessence Publishing. 1980:339.
29 Harmon CB. Pontic design. J Prosthet Dent. 1958;8:496.
30 Henry PJ. Pontic form in fixed partial dentures. Aust Dent J. 1971;16:1.
31 Allison JR, Bhatia HL. Tissue changes under acrylic and porcelain pontics [Abstract No. 168]. J Dent Res. 1958;37:66.
32 Silness J, et al. The relationship between pontic hygiene and mucosal inflammation in fixed bridge recipients. J Periodont Res. 1982;17:434.
33 Gildenhuys RR, Stallard RE. Comparison of plaque accumulation on metal restorative surfaces. Dent Surv. 1975;51(1):56.
34 Keenan MP, et al. Effects of cast gold surface finishing on plaque retention. J Prosthet Dent. 1980;43:168.
35 Ørstavik D, et al. Bacterial growth on dental restorative materials in mucosal contact. Acta Odontol Scand. 1981;39:267.
36 Clayton JA, Green E. Roughness of pontic materials and dental plaque. J Prosthet Dent. 1970;23:407.
37 Tolboe H, et al. Influence of pontic material on alveolar mucosal conditions. Scand J Dent Res. 1988;96:442.
38 Smith DE. The pontic in fixed bridgework. Pacific Dent Gaz. 1928;36:741.
39 Ante IH. Construction of pontics. J Can Dent Assoc. 1936;2:482.
40 Beke AL. The biomechanics of pontic width reduction for fixed partial dentures. J Acad Gen Dent. 1974;22(6):28.
41 Ferracane JL, Condon JR. Post-cure heat treatments for composites: properties and fractography. Dent Mater. 1992;8:290.
42 Rothfuss LG, et al. Resin to metal bond strengths using two commercial systems. J Prosthet Dent. 1998;79:270.
43 Wise MD, Dykema RW. The plaque-retaining capacity of four dental materials. J Prosthet Dent. 1975;33:178.
44 Kitaoka A, Ashida H. Phenomenal characteristics of peripheral drift illusion. Vision. 2003;15:261.
45 Ortman HR. Factors of bone resorption of the residual ridge. J Prosthet Dent. 1962;12:429.
46 Atwood DA. Some clinical factors related to rate of resorption of residual ridges. J Prosthet Dent. 1962;12:441.