Benign tumours
Skin tumours are common, and their incidence is rising in western countries (p. 24). The treatment of skin tumours makes up a large part of current dermatological practice (p. 24). Many skin tumours are benign, and these are described in this section. Viral warts, actinic keratoses and naevi are mentioned elsewhere.
Benign epidermal tumours
Seborrhoeic wart (basal cell papilloma)
A seborrhoeic wart (seborrhoeic keratosis) is a common, usually pigmented, benign tumour consisting of a proliferation of basal keratinocytes (Fig. 1). The cause is unknown, although they may be ‘naevoid’. Seborrhoea is not a feature.
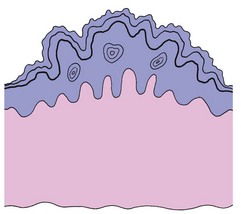
Fig. 1 Histopathology of seborrhoeic wart.
The illustration shows a hyperkeratotic epidermis, thickened by basal cell proliferation, with keratin cysts.
Clinical presentation
Seborrhoeic warts have the following features:
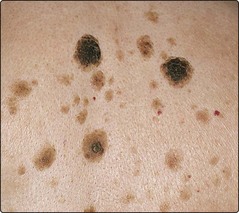
 often multiple (Fig. 2), sometimes solitary
often multiple (Fig. 2), sometimes solitary
affect the elderly or middle-aged
mostly found on the trunk and face
generally round or oval in shape
start as small papules, often lightly pigmented or yellow
become darkly pigmented warty nodules, 1–6 cm in diameter
have a ‘stuck-on’ appearance, with keratin plugs and well-defined edges.
Skin tags
Skin tags are pedunculated benign fibroepithelial polyps, a few millimetres in length. They are common, mainly seen in the elderly or middle-aged, and show a predilection for the neck, axillae, groin and eyelids (Fig. 3). The cause is unknown, but they are often found in obese individuals. Occasionally, skin tags are confused with small melanocytic naevi or seborrhoeic warts. The treatment, usually for cosmetic reasons, is by snipping the stalk with scissors or cutting through it with a hyfrecator (under local anaesthetic if necessary), or using cryotherapy.

Epidermal (epidermoid) cyst
Epidermal cysts, usually seen on the scalp, face or trunk, are sometimes incorrectly called sebaceous cysts. They are keratin filled and derived from the epidermis or, in the case of the related pilar cyst, the outer root sheath of the hair follicle. The cysts are firm, skin coloured, mobile and normally 1–3 cm in diameter. Bacterial infection is a complication. Excision is curative.
Milium
Milia are mostly seen on the face, where they typically appear as small white keratin cysts (1–2 mm in size) around the eyelids and on the upper cheeks. They are often seen in children, but may appear at any age. Occasionally, milia may develop as part of healing after a subepidermal blister, e.g. with porphyria cutanea tarda. Milial cysts can normally be extracted using a sterile needle.
Benign dermal tumours
Dermatofibroma (fibrous histiocytoma)
Dermatofibromas are common dermal nodules, and are usually asymptomatic. Histologically, they show a proliferation of histiocytes and fibroblasts, with dermal fibrosis and sometimes epidermal hyperplasia. They possibly represent a reaction pattern to an insect bite or other trauma, although often no such history is obtained.
Clinical presentation
Dermatofibromas are usually seen in young adults, most commonly women, and mainly occur on the lower legs. They are firm, dermal nodules 5–10 mm in diameter and may be pigmented (Fig. 4). They enlarge slowly, if at all.

Pyogenic granuloma
A pyogenic granuloma is a rapidly developing bright red or blood-crusted nodule that may be confused with a malignant melanoma. It is neither pyogenic nor granulomatous, but is an acquired haemangioma.
Clinical presentation
A pyogenic granuloma typically:
develops at a site of trauma, e.g. a prick from a thorn
presents as a bright red, sometimes pedunculated, nodule 5–10 mm in diameter that bleeds easily (Fig. 5)
enlarges rapidly over 2–3 weeks

Keloid
A keloid is an excessive proliferation of connective tissue in response to skin trauma and differs from a hypertrophic scar because it extends beyond the limit of the original injury. Keloids show the following characteristics:
Present as protuberant and firm smooth nodules or plaques (Fig. 6).
Occur mainly over the upper back, neck, chest and ear lobes.
Develop more commonly in black Africans.
Have their highest incidence in the second to fourth decades.

Treatment is with a topical silicone sheet or gel, or steroid injection (p. 21).
Campbell-de-Morgan spot (cherry angioma)
Campbell-de-Morgan spots are benign capillary proliferations, commonly seen as small bright-red papules on the trunk in elderly or middle-aged patients (see Fig. 2). If necessary, they can be removed by hyfrecation or cautery.
Tumours of the skin appendages
Tumours of the skin appendages, i.e. of the eccrine and apocrine sweat ducts, hair follicles and sebaceous glands, are relatively rare. Clinically, they often present as rather non-specific cutaneous nodules, and they are difficult to diagnose without histology following excision. Occasionally, these tumours are malignant.
Lipoma
Lipomas are benign tumours of fat, and present as soft masses in the subcutaneous tissue. They are often multiple and are mostly found on the trunk, neck and upper extremities. Sometimes they are painful. Removal is rarely needed.
Chondrodermatitis nodularis
Chondrodermatitis nodularis is not a neoplasm, but presents as a painful small nodule on the upper rim of the helix of the pinna, usually in elderly men (p. 118). It is due to inflammation in the cartilage that may be a response to degenerate dermal collagen induced by pressure or chronic sun exposure. They are often confused with basal cell carcinomas. Excision is curative.
Benign tumours
| Lesion | Age at onset | Main features |
|---|---|---|
| Epidermal | ||
| Viral wart | Childhood mainly | Usually on hands or feet (p. 52) |
| Actinic keratosis | Old age | Sun-exposed areas (p. 106) |
| Seborrhoeic wart | Old/middle age | Keratosis, often on trunk or face |
| Milia | Childhood | White cysts, often on face |
| Epidermal cyst | After childhood | Mostly on face or scalp |
| Skin tags | Middle/old age | Seen on neck, axillae and groin |
| Dermal | ||
| Dermatofibroma | Young adult, F > M | Nodule, often on leg |
| Melanocytic naevus | Teens/young adult | Brown macule or papule (p. 96) |
| Cherry angioma | Old/middle age | Small red papule on trunk |
| Pyogenic granuloma | Child/young adult | Red nodule, often on finger |
| Keloid | Second–fourth decades | Chest/neck, affects black Africans |
| Lipoma | Any age | Soft tumour on trunk or limbs |
| Chondrodermatitis nodularis | Old/middle age | Nodule on upper pinna, M > F |