Chapter 11 Developing healthy public policy
Overview
Healthy public policy (HPP) was identified in the Ottawa Charter (World Health Organization (WHO) 1986) as one of the five key strategies for promoting health. HPP focuses on changing the environment in order to make the healthy choice easier. Health is affected by many different policy areas:
Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control (Universal Declaration of Human Rights Article 25(1)).
HPP therefore includes all the major areas of policy that are the responsibility of democratic governments – employment, welfare, education, transport, food and health and social services. Relevant policies may also be instigated by private commercial organizations or devolved government agencies. Promoting HPP across this range of agencies and issues appears to be a daunting task. How to make inroads into this aspect of health promotion is the subject of this chapter, which examines the infrastructure required to facilitate HPP, the role of the practitioner and the potential of this approach to promote health. Readers are referred to Chapter 4 of our companion volume (Naidoo & Wills 2005) for a more detailed discussion of the policy process.
Defining HPP
Policy is a contested term, with meanings ranging from intentions to decisions and strategies. Milio (2001, p. 622) in a glossary of definitions describes it as ‘a guide to action to change what would otherwise occur, a decision about amounts and allocations of resources: the overall amount is a statement of commitment to certain areas of concern; the distribution of the amount shows the priorities of decision makers. Policy sets priorities and guides resource allocation’. We shall adopt a broad definition of policy as a plan of action to guide decisions and actions. Policy can be developed and implemented at many different levels, from organizational to national to international. Whilst policy may be allocated to a specific sphere, such as health, education or transport, in practice its effects are often wide-ranging and extend beyond the sphere originally targeted. Figure 8.3 in Chapter 8 illustrates the many agencies and organizations that promote health in some way. At government level the Treasury, for example, tries to influence individual behaviour through taxation of unhealthy products whilst the Department of Children, Schools and Families tries to do this through school-based health education. Joined-up policy-making is the term used to refer to integrated policy-making across different spheres. The determinants of health are multiple and interconnected, so in order to be effective, policy also needs to be holistic. It is often assumed that policy, once made and adopted by the relevant agency, translates smoothly into the intended action and anticipated outcomes. However this is the exception rather than the rule. Policy is (re)interpreted at all levels and its practical application may diverge from the original intention. It is therefore not enough to make policy; it must be followed through, monitored and supported by appropriate training and resources.
WHO has defined HPP as: ‘placing health on the agenda of policy makers in all sectors and at all levels, directing them to be aware of the health consequences of their decisions and to accept their responsibilities for health’ (WHO 1986, p. 2). This is a very broad definition, as is the Ottawa Charter’s (WHO 1986) definition of HPP as a central plank for health promotion. The Ottawa Charter cited the following fundamental resources for health: peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice and equity. This embraces all governmental activities, except, ironically enough, the provision of health services, although they might be counted as part of the social justice and equity resources. The Second International Conference on Health Promotion in Adelaide, Australia in 1988 (WHO 1988) explored HPP. It called for a political commitment to health by all sectors and an explicit accountability for health impacts.
Further international conferences focused on the globalization of health and the need for international cooperation to tackle the determinants of health. The Sundsvall Conference concentrated on the global, interlinked nature of environmental change to promote health (WHO 1991). The Jakarta Declaration (WHO 1997) and the Mexico conference (WHO 2000a) focused on the interlinked nature of social, economic and political development for health. The Bangkok Charter (WHO 2005) sought to make health promotion central to the global development agenda, and called for commitments from governments, communities and the private corporate sector to address health determinants and reduce inequalities.
 BOX 11.1
BOX 11.1Some core values underpinning HPP may be inferred from the conferences and charters outlined above and are also discussed in Chapter 4. These include:
What is clear from the above definitions resulting from the WHO international conferences is the broad scope of HPP, encompassing as it does all levels of government from international to national to local.
No policy would claim to have adverse health effects and most would claim to increase well-being in some way, albeit indirectly. Yet many policies may have apparently contradictory effects. For example, it has been argued that the overall economic effect of a reduction in smoking would be negative, due to the loss of tobacco tax revenue to the exchequer, and the extra demand on services due to people living longer. Economic policies that increase the income of the wealthiest have been defended on the grounds that there would be a ‘trickle-down’ effect, despite evidence that increases in relative inequality are detrimental to health (Wilkinson 1996). The application of stringent animal and environmental welfare regulations in the UK has resulted in an increase in meat imports from other countries where the same regulations do not apply. The consequences of policy programmes therefore need to be thought through in some detail. Health impact assessment (HIA) is an approach that does just this. HIA enables the identification, prediction and evaluation of likely changes to health, both now and in the future, as a consequence of a policy programme or plan. HIA recognizes that health is affected by a broad range of determinants linked in various pathways. For example, a HIA of a policy to extend licensing hours would weigh up the benefits and disadvantages of the proposal’s impact on individuals, the local community, the environment and the economy. Whilst the proposal may benefit the local economy, disadvantages to health, law and safety, and community cohesion are likely.
HIA as an approach is likely to become more widespread as various international agreements require an assessment be made of the likely impact of policy. For example, the European Union requires the establishment of mechanisms to ensure a high level of human health protection in the definition and implementation of all Community policies and activities (article 152 of the Treaty of Rome).
 BOX 11.2
BOX 11.2Health impact assessments in London
Congestion charges
Prior to the introduction of congestion charging in London, an HIA concluded that the scheme had the potential to improve health by:
Hosting the Olympic Games
Hosting the 2012 Olympic Games in London is anticipated to bring economic benefits to local communities. It might be assumed that the construction of additional sporting facilities will improve the opportunities for physical activity amongst the local population. However this is not necessarily the case. The extent to which members of a community will use facilities and opportunities is almost impossible to quantify in advance. There may also be an adverse health impact (e.g. air and noise pollution) on the community during the construction phase. A rapid HIA concluded that the overall impact will be positive: ‘there will be greater benefits to the local communities arising from increased employment and income opportunities, greater physical activity and enhanced community cohesion’ (http://www.londonshealth.gov.uk/PDF/Olympic_HIA.pdf).
The history of HPP
HPP has a long and illustrious history. Many would date its origins in the UK to the 19th century and the rise of the Sanitary Reform Movement, prompted by concerns about the spread of disease in overcrowded industrial slums. Edwin Chadwick’s Report from the Poor Law Commissioners on an Inquiry into the Sanitary Conditions of the Labouring Population of Great Britain (1842) made it clear that the poor did not have the power to change their conditions, and that protecting and promoting their health were tasks of local government. The 19th century saw a plethora of legislation and regulations to protect and promote health – a trend that was carried on into the 20th and 21st centuries (see Example 11.3).
Landmarks in healthy public policy in the UK during the 19th, 20th and 21st centuries
1842 Edwin Chadwick’s Report from the Poor Law Commissioners on an Inquiry into the Sanitary Conditions of the Labouring Population of Great Britain is published
1843 The Royal Commission on the Health of Towns is established
1844 The Health of Towns Association is founded
1845 Final report from the Royal Commission on the Health of Towns is published
1848 Public Health Act for England and Wales requires local authorities to provide clean water supplies and hygienic sewage disposal systems, and introduces the appointment of medical officers of health for towns
1854 John Snow controls a cholera outbreak in London by removing a contaminated local water supply
1866 Sanitary Act – local authorities had to inspect their district
1868 Housing Act – local authorities could ensure owners kept their properties in good repair
1871 Local Government Board (which became the Ministry of Health in 1919) was established
1872 Public Health Act makes medical officers of health mandatory for each district
1875 Public Health Act consolidates earlier legislation and the tone changes from allowing to requiring local authorities to take public health measures
1906 Education Act establishes the provision of school dinners
1907 Education Act establishes the school medical service. Notification of Births Act and the development of health visiting is encouraged
1967 Road Safety Act set a legal limit of 80 mg of alcohol per 100 ml of blood and imposed a 70 miles per hour speed limit
1968 Clean Air Act to reduce air pollution and respiratory diseases
1974 National Health Service (NHS) reorganization – community and public health services transferred from local authorities to the NHS
1974 Heath and Safety at Work Act requires all employers to secure the health, safety and welfare at work of all employees
1977 Housing (Homeless Persons) Act places a duty on local authorities to house homeless persons
1983 Seat belt legislation. Wearing of seat belts in rear seats becomes law in 1991. Children to be restrained in car seats becomes law in 2006
1988 Water Bill requires privatized water suppliers to conform to health standards
1989 Tax subsidy on unleaded petrol
2000 The Food Standards Agency, an independent body, is established to protect the public’s health and consumer interests in relation to food
2004 Smoking ban in all public places introduced in the Republic of Ireland
2005 Pubs and clubs able to apply for unlimited extension to opening hours
2005 Civil Partnership Act (2005) allows same-sex couples to enter a civil partnership, giving them the same next-of-kin rights in relation to health care as married couples
2006 Smoking ban introduced in all public places in Scotland
2006 Work and Families Act extends maternity and adoption leave from 6 to 9 months’ paid leave, to be taken by the father or the mother
2007 Smoking ban in all public places introduced in England, Northern Ireland and Wales
2007 Junk food advertising banned from television programmes aimed at young children (4–9-year-olds)
The 19th-century view of public health was dominated by the effects of the physical environment on health. The 21st-century view of public health is ecological, whereby economic, environmental and social factors interconnect and have an impact on health. Current health concerns include ensuring that everyone has access to green space, a safe environment, mobility and transport, as well as clean, safe land and water. Everyone should be able to use renewable energy, reduce waste products to a minimum and use efficient recycling methods.
Regulation is just one way in which policy can support health. Governments may also use fiscal or monetary means such as taxing unhealthy products or hypothecation (a dedicated tax to support a specific purpose, e.g. funding cycling routes through a congestion charge on motor vehicles). Policy can support health through the provision of services, e.g. recycling facilities.
There is clearly a role for individual champions of public health. The story of John Snow, who stopped the cholera epidemic in Soho in 1854 by removing the handle of the Broad Street water pump, illustrates the importance of the epidemiological (studying the incidence and prevalence of disease) approach in public health (Figure 11.1). Previously, people had believed that bad air (miasma) from the rubbish and waste in the slums was responsible for the spread of disease. Snow’s successful action demonstrated that cholera was a waterborne disease which could be prevented by the provision of clean water supplies.
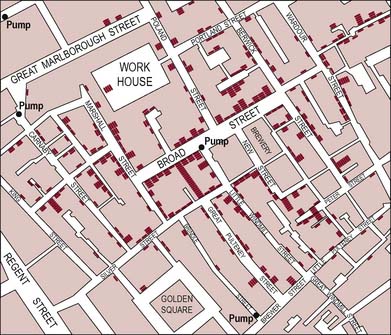
Figure 11.1 A portion of Snow’s map of the spread of cholera in London. Purple bars represent the number of fatal cases in each house. The position of the Broad Street pump from which all the victims had obtained water is also marked.
Single-issue pressure groups or non-governmental organizations (e.g. Help the Aged; Friends of the Earth) may also act as champions lobbying and advocating for specific policies. An example is Oxfam’s lobbying to change trade-related aspects of intellectual property rights (TRIPS) regulations in relation to patented medicines. Publicity showing how human immunodeficiency virus (HIV)-positive patients in South Africa and Zimbabwe could not afford patented drug therapies set the scene. Oxfam then launched a sustained campaign to ensure that low-income countries have access to medicines at minimal cost, including the right to access non-patented medicines. At the time of writing (2008) th e campaign is ongoing.
There is also a role for research to establish the links between determinants and health. Credible research needs to document the severity of the problem and the effectiveness of the proposed solutions. The British Medical Association (2003), for example, has called for more evidence to show that improved housing can improve health. Lobbying to translate research findings into plain English and spell out their implications for health is also important. The gathering of robust evidence for the effectiveness of HPP, given the long timescales and complexity of interrelated factors, has proved to be problematic. The lack of a robust evidence base for HPP has been commented on by policy-makers and researchers (Petticrew et al 2004).
Many factors impacting on health operate on a global scale that transcends national boundaries, e.g. infectious diseases, poverty and food shortages, war and civil conflict and climate change. At the global level, international organizations such as the United Nations (UN), WHO, the World Trade Organization, the World Bank and the International Monetary Fund (IMF) are all hugely influential in affecting the socioeconomic determinants of health. An example of global health-promoting policy-making is the WHO’s establishment of a Commission on Social Determinants of Health in 2005 and the UN Millennium Development Goals, which include targets to reduce poverty, hunger, child and maternal mortality, and infectious diseases; and to promote universal primary education, gender equality and environmental sustainability (United Nations Development Programme 2006).
The impact of global players is not always beneficial. For example, financial bodies such as the World Trade Organization support free-trade policies which often benefit middle- and high-income countries rather than low-income countries. The IMF has imposed structural adjustment programmes in low-income countries, which has had the effect of reducing their public spending, including spending on health. There is a ‘brain drain’ of skilled health professionals from low-income countries to middle- and high-income countries, which leads to a spiral of reduced service delivery and further migration of professionals (Sanders et al 2003).
The role of states is usually emphasized in HPP but policy is also made at other levels. In Part 3 we discuss how settings such as schools and hospitals can be supportive environments for health. Organizational policies, such as those relating to cultural competence for example, may have an impact on working practices.
Key characteristics of HPP: advantages and barriers
 BOX 11.4
BOX 11.4Take a topic, e.g. obesity, sexual health or drug use. Identify a range of health promotion interventions including educational, behavioural and policy-making. What might be the advantages of an HPP approach to health promotion? And what might be the disadvantages?
HPP as an approach to health promotion has many strengths. Perhaps most important is its recognition of the multiple socioeconomic environmental determinants of health, and the necessity to change these determinants in order to promote health. Alongside this recognition and ‘upstream’ focus goes a commitment to reducing inequalities in health and promoting equity. An upstream approach also has economic benefits. A positive impact on determinants of health will prevent much ill health and disease, thus averting the need to spend money on services and treatment. Prevention is typically far more cost-effective than treatment.
HPP has the potential to make clear inroads into the state of the health of the public. McPherson (2001) states that 30% of coronary heart disease and 25% of all cancers are preventable through appropriate public health action. If achieved, this reduction would have economic as well as health benefits. The potential of HPP to achieve dramatic shifts in behaviour and attitudes is another reason for its popularity.
Smoke-free workplaces in the Republic of Ireland
An evaluation of the legislation introducing smoke-free workplaces in the Republic of Ireland in 2004 reported very positive results. There were dramatic declines in reported smoking in all venues, including restaurants (from 85% to 3%), bars and pubs (from 98% to 5%). Support for the ban from smokers increased, with 83% of smokers reporting that they thought the smoke-free law was a good or very good thing. Nearly half (46%) of smokers said the law made them consider quitting, and of smokers who had quit following the ban, 80% reported the law had helped them quit and 88% that the law helped them to stay quit (Fong et al 2006).
There are many barriers to achieving HPP. Hunter (2003) identifies several barriers, including the tendency of both the government and the public to focus on health services instead of public health, and the silo mentality of government departments that means cross-departmental working to promote public health remains an aspiration rather than a reality. Public health issues tend to be ‘wicked issues’ (Rittel & Webber 1973). Wicked issues are complex issues that are not well understood and not amenable to easy manipulation or solution. Public health issues, such as sustainability or reducing health inequalities, are multidisciplinary in nature, and effective action is likely to require a long timescale, well beyond political parties’ terms of office. As Hunter (2003, p. 17) puts it: ‘Almost by definition public health issues are wicked issues.’
Opponents of an HPP approach might argue that it removes personal responsibility, and supports a ‘nanny state’ that dictates to its citizens their opportunities and behaviours. Indeed, Beattie (1993) described legislative action in his model of approaches to health promotion as authoritative and ‘top-down’. Those who subscribe to conservative and individualistic political beliefs and ideology might be particularly likely to hold this view. This criticism has been met by the proposal that governments should act as stewards, guiding and protecting the health of the public, but not replacing the need for individual responsibility. Stewardship is about collective responsibility, which requires agreement about what needs to be done. The WHO ranks stewardship as more important than health service delivery or funding, because ‘the ultimate responsibility for the overall performance of a country’s health system must always lie with government’ (WHO 2000b).
Joffe & Mindell (2004) argue that the focus should shift from telling people what to do to making healthy choices easier; that the state should shift from being a ‘nanny state’ to a ‘canny state’ – one ‘that is clever, prudent, capable, and shrewd’ (Joffe & Mindell 2004, p. 967). There are therefore several roles that governments may adopt in order to pursue healthy public policies. Some, such as the ‘nanny state’, appear old-fashioned and deeply unpopular. Others, such as stewardship or the ‘canny state’, appear more contemporary and in tune with a range of current values and ideologies in which the people in a civic society determine direction and government ‘steers’ but does not ‘row’ (Giddens 1998). Any form of legislative action requires agreement by the public. Tones has argued that, without health education, HPP would not be possible. Health education can not only set an agenda, e.g. environmental concern, but can also help ‘to create a climate of opinion that will enable government, for example, to institute and claim the credit for change without risking electoral unpopularity’ (Tones 2001, p. 14).
Identify a health issue of concern to you, e.g. obesity, alcohol, smoking, mental health.
Go ‘upstream’ and try to identify the socioeconomic factors implicated in this health issue. Then try to define what policies might make an impact upstream on this issue. What agency or organization is responsible for this policy? What steps could you take to lobby for such a policy?
Resources and skills required for HPP
Identify an example of HPP, e.g. smoking ban, food labelling regulations, transport policy to promote walking and cycling, neighbourhood regeneration. What kind of skills and resources are necessary to formulate and implement HPP?
Influencing, planning for, and operationalizing, HPP calls for a variety of skills. The required skills include health education, partnership working, lobbying, advocacy, managing, leadership and public relations. The Ottawa Charter (WHO 1986) described three key skills that would be necessary to act on the five action areas – mediation, advocacy and enablement. The competences for public health practice (www.skillsforhealth.org.uk) currently include a key area in policy and strategy development and implementation which calls for an understanding of the policy-making process, different methods of HIA and interagency working.
The policy-making process is complex and has been described elsewhere (Naidoo & Wills 2005,) Chapter 4. The four key stages are (Walt 1994):
An understanding of the policy-making process is crucial. A variety of different skills are needed at each stage. For example, stage 1, problem identification and issue recognition, may require research, lobbying and advocacy in order to prompt awareness of a particular issue. HIA can raise awareness of health impacts.
Partnership working is an important element within the policy process. The benefits and statutory requirements for collaboration are outlined in Chapter 5 of our companion volume (Naidoo & Wills 2005). Identifying key stakeholders, clarifying their interests in the proposed policy and making links with others to present a united agenda for change is all part of the wider policy process. Chapter 8 outlines the roles of some agencies. An awareness of different organizational cultures and their interests is vital for partnership working. Key skills are how to influence, negotiate, facilitate and manage in a multiagency environment to bring about change.
Public health advocacy has been described as the process of overcoming structural barriers to public health work (Chapman & Lupton 1994). It means influencing and then expressing public opinion to influence policy-makers’ judgements about what is politically desirable and acceptable (Kemm 2001). Presenting the case for a policy might mean finding areas of overlap or congruence between the interests of the people you are representing and the key people with influence. Advocacy may also be used to present the case against a policy. The use of the mass media in advocacy is discussed further in Chapter 12.
Think of a recent policy change in your workplace. How was the policy implemented? Was there resistance to the policy? Was implementation successful?
It cannot be assumed that once a policy has been approved the implementation stage is straightforward. This stage may be particularly problematic for policies that affect organizational working. Implementation involves getting the agreement of those who are affected by it, and their commitment to its operationalization. There is often resistance to the imposition of change from above. Frontline workers or ‘street-level bureaucrats’ (Lipsky 1979) have been identified as playing a key role in the implementation and delivery of policy changes, with the capacity to progress or impede the policy process.
Although in an ideal world HPP would be a rational process, in reality policy-making is not rational but incremental, or what has been labelled ‘muddling through’ (Lindblom 1959, Tones & Green 2004). Ideally policy-making would be driven by clarity about the problem, desired goals and outcomes and the best means of achieving these. This in turn would require an objective assessment of all alternatives at each stage of the policy process. The outcome would be the best possible choice, and there would be consensus about this. In reality, policy-making is incremental and typically considers a restricted range of options, blurs the distinction between goals and implementation, and achieves consensus about small changes rather than radical overhauls.
The Framework Convention on Tobacco Control (WHO 2003)
The Framework Convention on Tobacco Control (FCTC) is an attempt to challenge the powerful economic interests of the tobacco industry and tobacco growers, and protect individual nations and populations from their power. The FCTC was agreed by the member states of the WHO in 2003, following almost 4 years of negotiation. Lobbying from antitobacco pressure groups and the tobacco lobby’s persistent manoeuvring from the inside had made the creation of the FCTC a difficult task. By 2004, 131 countries had signed the treaty and 21 had ratified it. The USA was a notable omission to those ratifying the Convention. The FCTC is the first global health treaty and came into force in 2005 (Beaumont et al 2007).
The practitioner’s role in HPP
Although many practitioners might not think of HPP as being part of their work remit, there are a number of ways in which practitioners might become involved. Depending on job role and employing organization or service, practitioners may take on a range of roles in relation to HPP. These roles range from leading the process, sharing the vision and promoting the benefits of the HPP approach, to active involvement in the process of lobbying, advocacy and partnership working.
Your local council is proposing a new transport plan to encourage cycling and walking. The plan includes congestion charging, the introduction of cycling lanes and dedicated lanes for cars carrying more than one person. Proponents argue that this will encourage people to integrate exercise into their personal travel plans. Opponents argue the scheme will lead to more congestion and longer travel times due to reduced road space and more speed restrictions. The council is inviting consultation with all interested parties. What, if anything, would you see as your role as a practitioner? How, if at all, would this differ from your role as a member of the public?
As a practitioner faced with a proposed new policy affecting your clients, you would probably consider it your duty to assess the plan in terms of its likely impact on the health of your clients. This might include initiating discussions and forums with clients to gauge their reaction to the proposal, or a more ad hoc process of sounding things out with individuals as and when you deem it appropriate. Perhaps you would take it upon yourself to translate research findings into plain English, or to spell out the likely effects of the proposed policy. You might propose that a rapid HIA is undertaken which would ensure the views of community groups are heard. You might also take the issue up with your professional association, and get them involved in the issues.
As a member of the public, you might be involved in the same spectrum of activities (apart from working with professional associations). However your role and expertise would be different, and you would engage as an interested member of the public rather than as a practitioner with a duty of care. This might give you more freedom to voice your opinions and make your principles and values known.
How, if at all, has the policy process been covered in your professional training?
Has your training included skills helpful for those engaging with the policy context and process?
The policy context, process and implementation, as well as specific skills helpful for those engaging with policy, tend to be neglected areas within professional training. This is the current situation despite the fact that practitioners are often crucial in determining whether or not a policy achieves its goals. Policies need to be implemented in order to have an impact. This will usually involve a change in working practices, and there is a tendency to resist change within organizations. Change is often stressful and time-consuming, and unless people are convinced of its merits, there may well be resistance. Inertia or misinterpretation of what is required may also mean policies get no further than the paper they are written on. In order to be effective, practitioners need to be ‘on board’ and committed partners in implementing policies. This in turn depends on whether and how their organization has engaged them in the policy-making process.
Within the health services there is a long history of continual change and reorganization. This can lead to a degree of cynicism and lack of engagement with the policy-making process. For many, policy implementation in the past has been experienced as increased levels of micromanagement, leading to a negative stance towards policy. However policy-making is a powerful professional tool, and the skills for effective engagement in the policy process need to be embedded in professional training.
Evaluating an HPP approach
How would you evaluate the impact of the ban on advertising ‘junk food’ during television programmes targeted at children?
Evaluating the impact of policies is often difficult, due to the long timescale involved, the lack of controlled comparisons and the complexity of factors and relationships affected by policy changes. Areas that are commonly researched in order to assess the impact of policy changes are:
More details of the evaluation process are given in Chapter 20.
Conclusion
HPP is a vital cornerstone of health promotion. Policy is a complex phenomenon that exists at many different levels. HPP has a sound rationale and some notable successes, but remains rather underused as a strategy. This is probably due to its complexity and the fact that responsibility for HPP often falls between agencies and practitioners. HPP is inevitably affected by politics, values and ideologies, all of which are constantly shifting. This provides another reason for the relatively low profile of HPP. The potential of HPP to be an effective and efficient means of promoting health and preventing ill health suggests that it should be embedded in professional training. The ability to understand and engage effectively in the policy process should be part of every practitioner’s professional skills base.