Chapter 4 Defining health promotion
Overview
The process of attempting to promote health may include a whole range of interventions including:
Until the 1980s most of these interventions were referred to as ‘health education’ and the practice was almost exclusively located within preventive medicine or, to a lesser extent, education. In recent years, the term health promotion has become widely used. There is no agreed consensus on what health promotion is or what health promoters do when they try to promote health, nor what a successful outcome might be. Many professions, including nursing, have found health promotion to be part of an expanding job description. This development reflects the arguments presented in this book, that it is health and not illness or disease which should underpin health care work. Yet what practitioners do in the name of health promotion varies enormously. This chapter outlines the historical development of health promotion and considers different views on the purpose, the nature and the scope of health promotion practice.
Foundations of health promotion
The term health promotion is a recent one used for the first time in the mid-1970s (Lalonde 1974) and the Alma Ata conference (World Health Organization 1978) is cited as setting the agenda for health promotion. Its foundations are complex and differ between countries and regions but in general arose from:
The term health promotion is used in a number of different ways, often without any clarification of meaning. In 1985 when the term was becoming widely adopted, Tannahill (1985) described it as a meaningless concept because it was used so differently. Over a decade later, Seedhouse (1997) describes the field of health promotion as muddled, poorly articulated and devoid of a clear philosophy. These early understandings reflect the origins of health promotion and range from:
More recently, health promotion is defined by building on the Ottawa Charter (World Health Organization 1986) definition, as Nutbeam (1988, pp. 1–2) explains:
Health promotion represents a comprehensive social and political process. It not only embraces actions directed at strengthening the skills and capabilities of individuals, but also actions directed towards changing social, environmental and economic conditions so as to alleviate their impact on public and individual health. Health promotion is the process of enabling people to take control over the determinants of their health and thereby improve their health.
 BOX 4.1
BOX 4.1A shared understanding of the meaning and purpose of health promotion is elusive. A diversity of disciplinary and ideological perspectives and policy changes has resulted in apparently conflicting conceptualizations. Health promotion as a concept can thus be understood as:
Origins of health promotion in the UK
The first phase of health promotion development is known as the ‘social hygiene period’ with roots in both public health and health education. Its origins of health promotion lie in the 19th century when epidemic disease eventually led to pressure for sanitary reform for the overcrowded industrial towns. Alongside the public health movement emerged the idea of educating the public for the good of its health. The Medical Officers of Health appointed to each town under the Public Health legislation of 1848 frequently disseminated everyday health advice on safeguards against ‘contagion’. Voluntary associations were also formed, including the London Statistical Society (1839), the Health of Towns Association (1842) and the Sanitary Institute (1876). The temperance movement held Band of Hope mass meetings, and through schools and churches lectured to young people on the virtue of abstinence. By the 1920s health education had become associated with diarrhoea, dirt, spitting and venereal disease! The evidence that between 10% and 20% of soldiers in the First World War had contracted venereal disease led to propaganda, one-off lectures and the first of ‘shock-horror’ techniques in which soldiers were shown lurid pictures of diseased genitals to dissuade them from having sex (Blythe 1986; Welshman 1997).
The second phase of health promotion development is known as the ‘personal services’ period. Changing patterns of morbidity and mortality shifted attention away from disease to personal behaviour. The Central Council for Health Education was established in 1927, paid for by local authority public health departments, and public health doctors formed the majority of its membership. An extract from some of the tasks listed as important reflects an emphasis on information, and education to bring about change in personal habits and behaviour:
The Central Council was principally concerned with propaganda and instruction. During the Second World War it delivered 3799 lectures on sex education and venereal disease which were attended by 340 000 people (Amos 1993). A database of health education film synopses is held by the British Film Institute (at http://www.ftvdb.bfi.org.uk/sift/organization/9345http://ftvdb.bfi.org.uk/sift/organization/9345) and confirms the emphasis on propaganda and instruction.
 BOX 4.2
BOX 4.2The Health Education Council (HEC), which was set up in 1968 as a quango – a quasi-autonomous non-governmental organization – reflected the Department of Health and Social Security’s, as it then was, medical model of health. The members were drawn from public health, and the medical and dental professions, with the inclusion of advertising and consumer affairs representatives. Its brief was to create a ‘climate of opinion generally favourable to health education, develop blanket programmes of education and selected priority subjects’ (Cohen Committee 1964). Similar health education agencies were set up in Wales, Scotland and Northern Ireland.
The HEC came to be associated with mass publicity campaigns such as Look After Yourself (LAY) which was launched in 1978. LAY reflected the view that people could be encouraged to adopt lifestyles which would lead to better health. The lead agency for health education in England consistently emphasized such mass campaigns and short-term initiatives. Sutherland, the first director of education and training at the HEC, has vividly described the pressures and lobbying which led the HEC away from confrontation with vested interests, such as agriculture or tobacco, and kept it confined to mass-media campaigns despite evidence of their limited effect (Sutherland 1987).
By the 1970s there was an increasing recognition that health policy could not continue to be confined to clinical and medical services, which were both proving expensive and not improving the health status of the population. Health education and the prevention of disease represented a means of cutting costs and an ideology which could place the onus of responsibility on the individual.
Health as an individual responsibility
The government document Prevention and Health: Everybody’s Business (Department of Health and Social Security 1976) was published in 1976 and encapsulated a behavioural approach which saw health problems as the result of individual lifestyles.
To a large extent though, it is clear that the weight of responsibility for his own health lies on the shoulders of the individual himself. The smoking-related diseases, alcoholism and other drug dependencies, obesity and its consequences, and the sexually transmitted diseases are among the preventable problems of our time and, in relation to all of these, the individual must decide for himself (Department of Health and Social Security 1976).
The message of the document is that improving health depends on individuals changing the way they live in order to avoid ‘lifestyle’ diseases. A decade later, in 1987, a similar message was put forward by the White Paper Promoting Better Health which suggested that the major killer diseases could be avoided if people took greater responsibility for their own health (Department of Health 1987). The Health of the Nation strategy was also permeated by a philosophy of individualism despite the acknowledgement in the strategy that ‘responsibilities for action are widely spread from individuals to government’ (Department of Health 1992). Later White Papers in England, Saving Lives: Our Healthier Nation (Department of Health 1999) and Choosing Health: Making Healthier Choices Easier (Department of Health 2004) similarly look to individuals to make informed decisions about their health. The latter document highlighted the following behavioural priorities:
Alongside this government response, however, was the awareness that poor health was linked to poverty. In 1980 the Black report, commissioned by the government, showed how those in lower social classes had a far higher risk of dying prematurely than more advantaged groups (Townsend & Davidson 1982). The HEC commissioned a further study on inequality, Inequalities in Health: The Black Report and the Health Divide (Townsend et al 1992). The report was published on a national holiday in August, ostensibly to avoid publicity, so damning was its evidence on the extent of poverty and deprivation. The last three decades have seen a re-emergence of public health measures and a recognition of the need to address the social, economic and environmental determinants of health. The Acheson report (HM Government 1998), commissioned by an incoming Labour government, recommended that as part of health impact assessment, all policies likely to have an impact on health should be formulated in such a way to favour the less well-off. In all countries, making the connection between the social determinants of health and health promotion policy and action is a major task, as discussed by the international Commission on the Social Determinants of Health (http://www.who.int/social_determinants/en/).Developing healthy public policy is the subject of Chapter 11. In many countries however, much of health promotion remains ‘downstream’, focusing on the behavioural determinants of ill health such as smoking rather than the material factors and sociostructural conditions outlined in Chapter 2.
Public health
In 1920, Winslow Professor of Public Health at Yale University described public health as:
The Science and Art of preventing disease, prolonging life, and promoting health and efficiency through organized community effort for:
In the UK health promotion and public health are terms that are often used interchangeably. Health promotion is sometimes distinguished as one of the processes in securing public health. In many countries there is understood to be a clear distinction: public health is the practice of public health medicine with an emphasis on the prevention and control of disease. This distinction is explored in greater detail in our companion volume, Public Health and Health Promotion: Developing Practice (Naidoo & Wills 2005).
Historically, public health has been driven by social policy as much as by medicine. The early public health movement in the 19th century in the UK used a medical scientific model to explain the disease process. The gathering of information and interpretation of quantitative data (epidemiology) was employed to underpin decisions. Social policy interventions were deployed to protect the public and prevent disease (see Chapter 11).
 BOX 4.4
BOX 4.4Many practitioners now have public health included in their job remit, e.g. specialist community nurses, occupational health nurses. How is your role in public health defined?
The UK Faculty of Public Health identifies three domains of public health practice: health improvement, service improvement and health protection. The term health promotion is not included. Instead, the term multidisciplinary public health has become widely adopted, signalling environmental, social and individual health dimensions. Our companion volume (Naidoo & Wills 2005) discusses the similarities and differences between public health and health promotion in more detail.
The World Health Organization and health promotion
The World Health Organization has played a key part in proposing a broader agenda for health promotion. In 1977 the World Health Assembly at Alma Ata committed all member countries to the principles of Health for All 2000 (HFA 2000: World Health Organization 1977) that there ‘should be the attainment by all the people of the world by the year 2000 of a level of health that will per-mit them to lead a socially and economically productive life’. The World Health Organization made explicit five key principles for health promotion in a discussion paper commonly referred to as the Copenhagen document:
The context for the development of broad-based health strategies thus needed to be based on equity, community participation and intersectoral collaboration, The World Health Organization also identified that improvement in lifestyles, environmental conditions and health care will have little effect if certain fundamental conditions are not met. These include:
The World Health Organization launched a programme for health promotion in 1984, and conferences at Ottawa (1986), Adelaide (1988), Sundsvall (1991), Jakarta (1997), Mexico (2000) and Bangkok (2003) have further outlined areas for action. The practice and principles of health promotion developed in the Ottawa Charter (World Health Organization 1986) are still widely used to provide a framework for practice:
Each of these health promotion actions is the subject of a chapter in Part 2 of this book.
The processes of mediation, advocacy and enablement were identified as ways in which health could be promoted. These processes are discussed further below.
Defining health promotion
Disease prevention
In Chapter 1 we saw that there are many different meanings attached to the concept of health but the notion that health is the ‘absence of disease’ is a dominant one. Different perceptions about the nature of health and the factors contributing to it underpin interpretations of health promotion. The shift from infectious and communicable disease to chronic diseases in the 20th century highlighted the role of people’s lifestyles in disease causation. Prevention therefore became much more important, often through targeting high-risk groups who have an increased likelihood of developing a specific disease.
Health promotion is often categorized as concerned with primary, secondary or tertiary prevention.
Medical support and symptom control are important to those living with life-threatening illness but so too is enhancing their quality of life.For those working in a clinical setting, this is the usual interpretation of health promotion. It can differ little from the education of patients about the condition that brought them to the health service. Its aim is for patients to avoid a recurrence by following a treatment regime or some change in their lifestyle and to enhance quality of life when living with a chronic condition. Disease prevention does not, however, look beyond the risk factors or groups to the origins of ill health.
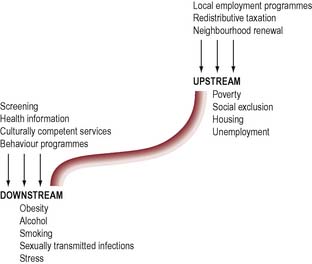
McKinlay (1979), in persuading us of the need to refocus upstream, tells a story:
There I am standing by the shore of a swiftly flowing river and I hear the cry of a drowning man. So I jump into the river, put my arms around him, pull him to shore and apply artificial respiration. Just when he begins to breathe, there is another cry for help. So I jump into the river, reach him, pull him to shore, apply artificial respiration, and then just as he begins to breathe, another cry for help. So back in the river again, without end, goes the sequence. You know I am so busy jumping in, pulling them to shore, applying artificial respiration, that I have no time to see who the hell is upstream pushing them all in.
The concept of refocusing upstream is a powerful and persuasive argument for health promotion. It can help us to reorient our thinking from a belief that medical care can, or will, solve most health problems towards prevention.
Figure 4.1 illustrates some specific examples of downstream interventions tackling health behaviours that give rise to problems and upstream interventions tackling the causes of such behaviours.
You might have included the fostering of hope and support, prevention of depression, home help, death education (Kellehear & O’Connor 2008).
Health education
Educating people about their health is commonplace but ‘health education’ as a formalized activity only emerged in the 1980s. The recognition of the need to diffuse information about the physical and moral ‘evils’ of squalor and drink can however be dated to the mid 19th century. An awareness that individuals make health choices which can contribute to the development of disease led to the view that it was possible to inform people about the prevention of disease, to motivate them to change their behaviour, through persuasion and mass communication techniques, and to equip them through education with the skills for a healthy lifestyle.
‘Traditional’ health education was often criticized for its narrow focus on information provision based on the assumption of a simple causation relationship between knowledge and behaviour. The emphasis on individual responsibility for health led to accusations of victim-blaming. Victim-blaming makes individuals feel guilty, although it may be factors beyond their control (poverty, social and environmental factors) that prevent them from making health changes.
Health education may be defined as planned opportunities for people to learn about health and make changes in their behaviour. It includes:
This might be seen as a limited interpretation of a health promotion role confining activity to information, education and communication, as discussed in Chapter 9.
One of the paradoxes of health education and a prevailing professional dilemma is the degree of voluntarism or free choice. Health education is based on an expert authority model derived from both medicine and education. It is the health educator or doctor who decides if there is a health need and the adequacy of an individual’s lifestyle, who decides the nature of the intervention and the most effective means of communication, who tries to ensure compliance, and who will decide if the intervention has ‘worked’. When we look at the practice of health education, we might be led to believe that health education is the giving of information and success in promoting health is when the client follows the advice. For other health educators education is a means of drawing out. Clients are not ‘empty vessels’ who will rationally change their behaviour once provided with the relevant information, advice or guidance. After all, information about the risks to health from smoking has been known since 1963 and information about human immunodeficiency virus (HIV) transmission since 1986, yet people continue to smoke and not use condoms. These health educators seek neither to coerce nor to persuade, both because this is unlikely to be effective but also because it is unethical. The health educator is a facilitator and enabler rather than an expert. Rather than telling clients what to do, the health educator works with them to identify their needs and work towards an informed choice, even when this may lead to health-damaging behaviour. The goal is to empower individuals to take health-related decisions by developing health literacy, self-efficacy, self-esteem and coping skills (Nutbeam 2000; Kickbusch 2001).
Health literacy may be defined as the capacity of an individual to obtain, interpret and understand basic health information and services in ways that are health enhancing (US Department of Health and Health Services 2000).
Who might be disadvantaged by efforts to improve health literacy?
The concept of health literacy is not new or radical and can be identified in many of the definitions of empowerment. However, it contains a central message that, although knowledge alone is insufficient to achieve change, not understanding the conditions that determine health or knowing how to change them is also de-powering (Abel 2007). We are faced with a society in which there is more choice of foods and other products, more health information from many sources, more choice in patient treatments, more choice of providers. In such a consumer society, Kickbusch (2006) argues active health citizenship is a critical empowerment strategy that enables people to make sense of and discriminate between such choices.
John is a labourer on the roads. He is 47 and single and his social life revolves around the pub. He drinks a few pints at lunchtime with his sandwiches and usually four pints on the way home. He visits his GP with backache. The GP takes his blood pressure and finds it dangerously high. Do you:
This scenario illustrates some of the key tensions in health education:
These issues are discussed further in Chapter 6 on ethical issues and Chapter 11 on developing healthy public policy.
The two strands of voluntarism and authoritarianism reflect the historical development of health education, as educationists and social scientists challenged the mainstream of preventive medicine by contesting the assumption that health education could, or indeed should, seek to bring about behaviour change through information or persuasion. Thus emerged the principle of self-empowerment which many argue is central to the practice of health education (Tones & Tilford 2001). Empowerment is an approach which enables people to take charge of their lives, including changing their behaviour if they so wish. Tones (1986) argues that an essential element of health education is ‘critical consciousness-raising’ to raise people’s awareness of the fundamental causes of ill health, a notion first espoused by the Brazilian priest Paolo Freire. Only through this process can the structural influence on health be addressed (see Chapter 5 for a discussion of Tones’ model of health promotion) and policy change be pursued and accepted.
The underlying principle of health education is to facilitate people to make their own choices about health behaviour. For those who believe the roots of ill health lie in social structures, this emphasis on choice is merely illusory. In Chapter 6 we shall explore further the limits to freedom of choice and how far an ethical principle such as the promotion of autonomy can govern our practice as health educators.
The range of approaches to health education are outlined and discussed in the following chapter. They range from the medical model, focusing on health surveillance and achieving behaviour change, to the educational model, which relies on the exploration of attitudes and values. Alongside these are the approaches more closely aligned to health promotion, such as community development, which emphasizes the need to take collective action for health, and a social model which focuses on the need to influence decision-makers at local and national level.
Health promotion
The World Health Organization has moved the definition of health promotion away from prevention of specific diseases or the detection of risk groups towards the health and well-being of whole populations. Instead of experts and professionals diagnosing problems, the people themselves define health issues of relevance to them in their local community. Teachers, primary health care workers, workplace managers, social and welfare workers can all be involved in promoting health. Instead of health being seen as the responsibility of individuals alone, the social factors determining health are taken into account, and health is viewed as a collective responsibility of society which needs to be prioritized by organizations and government in their decision-making.
Consider these descriptions of the work of a nurse on an acute medical ward and a health promotion adviser working with young people. Would you consider them to be practising health education or health promotion? What criteria do you use to make your judgement?
A key difference between these two interventions is their aims. In the coronary care unit, the nurse is actively engaged in disease prevention – to prevent a further heart attack. In the school, the health promotion adviser aims to equip young people with the information and skills for a healthy lifestyle. In both cases, the health promoter aims for behaviour change, more obviously so in the coronary care unit. Both use similar educational methods of providing information, encouraging clients to reflect on their attitudes and experience, and providing opportunities to practise skills.
The terms health education and health promotion are often used interchangeably but, whilst health promotion can be seen as an umbrella term incorporating aspects of health education, it is much broader in concept.
Health promotion incorporates all measures deliberately designed to promote health and handle disease … A major feature of health promotion is undoubtedly the importance of ‘healthy public policy’ with its potential for achieving social change via legislation, fiscal, economic and other forms of ‘environmental engineering’ (Tones 1990).
There are, as we saw in Chapter 2, a range of factors which influence people’s health. Some are material–structural and some are behavioural. These need to be addressed other than by education alone. Health promotion thus involves public policy change and community action to enable people to make changes in their lives. A phrase first coined by Milio (1986) has come to encapsulate health promotion – ‘making the healthy choice the easier choice’ – and was adopted as the strapline for the Public Health Strategy for England (Department of Health 2004). As we have seen, it is easy for practitioners to confine their health promotion role to offering information and advice on how to adopt a healthier lifestyle. However, for people to make such changes, the factors and situations which led them to adopt ‘unhealthy’ behaviours need to be addressed. People may smoke because of stress, even though they know it is bad for their health. Others may use an illegal drug because it is widely used by their peer group and is part of their social life. Equally, it is easier for some people to make healthy choices than it is for others. It is easy to eat a diet with fresh fruit and vegetables for people with reasonable incomes who have easy access to supermarkets or high-street shopping. Some factors affecting individual health are outside individual control: inadequate housing, busy roads, lack of child care.
School nurses were concerned that a high proportion of children’s packed lunches contained fizzy drinks, jam sandwiches, crisps and a chocolate bar. How can the healthy choice be made an easier choice?
Schools are cautious about giving advice to parents as they don’t want to be seen as interfering. Advice can be given in leaflets and children encouraged to prepare food in cook–eat sessions. Personal social and health education (PSHE) sessions could include discussions of what makes a healthy lunch and why it is important.
Nutritional standards for school meals were introduced in 2006 in all UK countries and ‘junk food’ was removed from vending machines. The ‘healthy choice’ thus became a necessary one. The dilemma of whether policy measures such as this are coercive is discussed in Chapter 6.
The new methods of health promotion are introducing new forms of social regulation which are not ostensibly oppressive or obviously controlling. In these, often innocuous-looking forms, they nevertheless enter and regulate our lives in new ways and bring with them new concerns for our civil liberties and rights (Bunton 1992).
An integrated definition of health promotion
Although health promotion is part of national efforts to improve health, its rejection of a disease-oriented pathogenic model of health differentiates it from medical approaches. Its goals derive from a positive, salutogenic concept of health and well-being (as discussed in Chapter 1). Its methods are empowering, ‘enabling individuals and groups to have a say in how their health is promoted and valuing their perspective; supporting people to acquire the skills and confidence to take greater control over their health’ (Naidoo & Wills 2005, p. 14).
In practice, health promotion encompasses different political orientations which can be characterized as the individual versus structural approaches. For some, health promotion is a narrow field of activity which seems to explain health status by reference to individual lifestyles and is a process largely determined by an expert who advises on beneficial changes. In its emphasis on personal responsibility it sees a minimal role for the state and, thus, has come to be associated with a conservative viewpoint. For others, including the World Health Organization, health promotion recognizes that health and wealth are inextricably linked, and seeks to address the root causes of ill health and problems of inequity using radical and challenging approaches (www.who.int/social_determinants/en/).
It is not helpful to debate whether one form of activity is better or worse than the other: both are necessary. Health promotion may involve lobbying and political advocacy, but it may just as easily involve working with individuals and groups to enhance their knowledge and understanding of the factors affecting their health.
Health education has become equated with persuasive attempts to manipulate behaviour but this is a narrow interpretation and ignores its importance as a core element of health promotion. Tones & Green (2004) propose the term new health education to refocus understanding and activity to education that enables individuals and communities to achieve greater control over their health.
Many practitioners believe that their role is limited in achieving the social changes necessary to eliminate health inequalities or the community change necessary to provide social support. Yet there are ways in which individual practitioners can promote health over and beyond merely informing, advising or listening. The World Health Organization identifies three ways in which practitioners can promote health through their work: advocacy, enablement and mediation.
Advocacy
Advocacy in health promotion is the process of defending or promoting a cause. It may mean representing the interests of disadvantaged groups and may mean speaking on their behalf or lobbying to influence policy. It may also mean action to gain political commitment, policy support, social acceptance and systems support for a particular goal or cause. For example, health promotion networks in Australia, New Zealand, the USA and Canada have long advocated for a focus on the health of indigenous peoples.
Enablement
Enabling means that health promotion practitioners take action in partnership with others to promote health by identifying needs and developing networks and resources in the community; assisting people to develop knowledge and skills; and helping people identify and address the determinants of their own health. Enablement is an essential core skill for health promoters since it requires them to act as a catalyst and then stand aside, giving control to the community (see Chapter 10 for further discussion of working with communities).
Mediation
Health promoters mediate between different interests by providing evidence and advice to local groups and by influencing local and national policy through lobbying, media campaigns and participation in working groups.
In the definitions of health promotion so far, health promotion has been interpreted as a process of improving the health of individuals or community. It can also be seen as a set of values or principles. The World Health Organization identifies these as empowerment, equity, collaboration and participation. These values should be incorporated in all health and welfare work for it to be health-promoting (Naidoo & Wills 2005).
To what extent do you encourage participation and enable your clients to take more control over their health?
Health promotion is thus an integrating approach to identifying and doing health work. Cribb & Dines (1993) argue that ‘the central question is not what is the domain of health promotion but is this being done in a health-promoting way? And this is a question that can be asked about any and every example of practice, not merely those which are clearly aimed at disease prevention or health education.’
To accept such a definition means there can be no boundaries to health promotion since any situation or event between client and practitioner has the potential to be health-promoting.
Conclusion
Many health workers are strongly committed to health education and the promotion of health. However, this has often been manifested in one-to-one programmes limited to providing information. Many may be daunted by the broad definition of health promotion and feel that this broad approach is beyond their professional remit. Indeed, it would not be possible for any one worker or group to bring about the changes needed for a health-promoting society. It is important that we remind ourselves of the World Health Organization view which describes the process of promoting health as not only involving political change and interagency collaboration, but also enabling people to take more control over their own health and equipping them with the means for well-being. Health promotion thus includes increasing individual knowledge about the functions of the body and ways of preventing illness, raising competence in using the health care system, and raising awareness and strengthening community action about the political and environmental factors that influence health.
Britain has one of the highest rates of teenage pregnancy in Europe. The under-18 conception rate dropped by 11.8% between 1998 and 2005 and now is at its lowest for 20 years.
The conception rate for under-16s in 2005 was 7.8 per 1000 which means 7462 girls under 16 getting pregnant each year: 57% of these led to legal termination (Teenage Pregnancy Unit 2007).
Which of the following aims for a health promotion intervention around teenage pregnancy would come closest to your own?
Which of the following activities would you consider a priority for a health promotion intervention? Why?