Chapter 5 Models and approaches to health promotion
Overview
The diversity in concepts of health, influences on health and ways of measuring health lead, not surprisingly, to a number of different approaches to health promotion. Chapter 4 began to explore the concepts of health education and health promotion. In this chapter, five different approaches will be discussed:
These approaches will be examined in terms of their different aims, methods and means of evaluation. These approaches have different objectives:
All of the approaches reflect different ways of working. Identifying the different approaches is primarily a descriptive process. The framework is descriptive – it does not indicate which approach is best, nor why a practitioner might adopt one approach rather than another. A number of theoretical frameworks or models of health promotion are outlined, discussed and assessed in relation to practice in the latter part of the chapter.
It is common for a practitioner to think that theory has no place in health promotion and that action is determined by work role and organizational objectives rather than values or ideology. We have argued elsewhere that practitioners should be aware of the values implicit in the approach they adopt: ‘Values thus determine the way in which the world is seen and the selection of activities and priorities and how strategies are implemented’ (Naidoo & Wills 2005, p. 13).
Models of health promotion are not guides to action but attempts to delineate a contested field of activity and to show how different priorities and strategies reflect different underlying values. They are useful in helping practitioners think through:
The medical approach
Aims
This approach focuses on activity which aims to reduce morbidity and premature mortality. Activity is targeted towards whole populations or high-risk groups. This kind of health promotion seeks to increase medical interventions which will prevent ill health and premature death. This approach is frequently portrayed as having three levels of intervention:
The medical approach to health promotion is popular because:
As we have seen in Chapter 1, the medical approach is conceptualized around the absence of disease. It does not seek to promote positive health and can be criticized for ignoring the social and environmental dimensions of health. In addition, the medical approach encourages dependence on medical knowledge and removes health decisions from lay people. Thus, health care workers are encouraged to persuade patients to cooperate and comply with treatment.
Public health medicine is the branch of medicine which specializes in prevention, and most day-to-day preventive work is carried out by the community health services which include specialist community public health nurses and district nurses.
Methods
The principle of preventive services such as immunization and screening is that they are targeted to groups at risk from a particular condition. Whilst immunization requires a certain level of take-up for it to be effective, screening is offered to specific groups. For example, in the UK cervical screening every 3–5 years is offered to all women aged 25–64.
For screening to be effective for the condition or disease:
The UK National Screening Committee oversees screening policies and gives advice based on available evidence. For more details visit www.nsc.nhs.uk/uk_nsc.
Preventive procedures need to be based on a sound rationale derived from epidemiological evidence. The medical approach also relies on having an infrastructure capable of delivering screening or an immunization programme. This includes trained personnel, equipment and laboratory facilities, information systems which determine who is eligible for the procedure and record uptake rates, and, in the case of immunization, a vaccine which is effective and safe. It can be seen then that the medical approach to health promotion can be a complex process, and may depend on the establishment of national programmes or guidelines.
 BOX 5.1
BOX 5.1Consider the example of amniocentesis – the testing of the amniotic fluid around a fetus to detect chromosomal abnormalities. Does this test meet the criteria for effective screening outlined above?
In most districts, amniocentesis is only offered to women over the age of 35 and those with a family history of chromosomal abnormality. Yet 80% of children with Down’s syndrome are born to mothers under 35 simply because more women in this age group have babies. Amniocentesis is not a simple test. It carries a risk of miscarriage. It can also only be performed after 14–16 weeks of pregnancy when a possible termination is more difficult. It is less than 100% sensitive and therefore some women may go away falsely reassured. A termination and/or counselling is the only intervention available.
Having screening or immunization facilities available is only effective if people can be persuaded to use them.
What methods can you think of that are used to increase the uptake of preventive screening services?
Mass media campaigns can raise awareness but an additional personalized trigger is often needed for people to access screening services. Personal invitations and appointments, telephone calls, telephone counselling and reminders from health care professionals have all been identified as helpful in increasing screening uptake. Removing economic barriers, such as transport or postage costs, can increase uptake in lower-income groups (Jepson et al 2000).
Evaluation
Evaluation of preventive procedures is based ultimately on a reduction in disease rates and associated mortality. This is a long-term process and a more popular measure capable of short-term evaluation is, for example, the increase in the percentage of the target population being screened or immunized.
Although there appears to be a close correlation between immunization uptake and a decline in disease rates, the example of whooping cough suggests some caution is needed. In 1974 80% of children were vaccinated against whooping cough. Following media publicity about the safety of the vaccine, immunization rates fell and did not reach 80% population coverage again until 1987. There were major whooping cough epidemics in 1977–1979 and 1981–1983, suggesting that immunization had contributed to the decline in notifications. However, the overall decline in mortality from whooping cough was occurring before the vaccine was introduced in 1957, suggesting that better nutrition, living conditions and medical care may also be significant.
The medical approach is not always successful. Recently, whooping cough has re-emerged in countries with high vaccination coverage and low mortality rates (British Medical Journal 2002). What could account for this?
Behaviour change
Aims
This approach aims to encourage individuals to adopt healthy behaviours, which are seen as the key to improved health. Chapter 9 shows how making health-related decisions is a complex process and, unless a person is ready to take action, it is unlikely to be effective. As we saw in Chapter 4, seeking to influence or change health behaviour has long been part of health education.
This approach is popular because it views health as a property of individuals. It is then possible to assume that people can make real improvements to their health by choosing to change their lifestyle. It also assumes that if people do not take responsible action to look after themselves then they are to blame for the consequences.
Consider the reasons why people may not be able to put a healthy diet into practice. Reasons include:
Evidence supports some factors, e.g. lack of money (Morris et al 2000). Other factors, e.g. ‘food deserts’, are more speculative (Cummins & Macintyre 2002).
It is clear that there is a complex relationship between individual behaviour and social and environmental factors. Behaviour may be a response to the conditions in which people live and the causes of these conditions (e.g. unemployment, poverty) are outside individual control.
Methods
The behaviour change approach has been the bedrock of activity undertaken by the lead agencies for health promotion. Campaigns persuade people to desist from smoking, adopt a healthy diet and undertake regular exercise. This approach is targeted towards individuals, although mass means of communication may be used to reach them. It is most commonly an expert-led, top-down approach, which reinforces the divide between the expert, who knows how to improve health, and the general public who need education and advice. However, this is not inevitable. Interventions may be directed according to a client’s stated needs when these have been identified. For example, social marketing techniques (see Chapter 12) focus on finding out what consumers want and need, and then providing it.
Many health care workers educate their clients about health through the provision of information and one-to-one counselling. Patient education about a condition or medication may seek to ensure compliance, in other words, a behaviour change, or it may be more client-directed and employ an educational approach.
Evaluation
Evaluating a health promotion intervention designed to change behaviour would appear to be a simple exercise. Has the health behaviour changed after the intervention? But there are two main problems: change may only become apparent over a long period, and it may be difficult to isolate any change as attributable to a health promotion intervention.
 BOX 5.5
BOX 5.5A recent systematic review of interventions using behaviour change methods to prevent weight gain found mixed results. Only one randomized controlled trial, that included various methods including a correspondence programme, goal setting, self-monitoring and being prepared for contingencies, reported significant positive results. The review concluded that progress in this field would be facilitated by:
The educational approach
Aims
The purpose of this approach is to provide knowledge and information, and to develop the necessary skills so that people can make an informed choice about their health behaviour. The educational approach should be distinguished from a behaviour change approach in that it does not set out to persuade or motivate change in a particular direction. However, education is intended to have an outcome. This will be the client’s voluntary choice and it may not be the one the health promoter would prefer.
The educational approach is based on a set of assumptions about the relationship between knowledge and behaviour: that by increasing knowledge, there will be a change in attitudes which may lead to changed behaviour. The goal of a client being able to make an informed choice may seem unambiguous and agreed upon. However this ignores not only the very real constraints that social and economic factors place on voluntary behaviour change, but also the complexities of health-related decision-making (see Chapter 9).
Methods
Psychological theories state that learning involves three aspects:
An educational approach to health promotion will provide information to help clients to make an informed choice about their health behaviour. This may be through the provision of leaflets and booklets, visual displays or one-to-one advice. It may also provide opportunities for clients to share and explore their attitudes to their own health. This may be through group discussion or one-to-one counselling. Educational programmes may also develop clients’ decision-making skills through role plays or activities designed to explore options. Clients may take on roles or practise responses in ‘real-life’ situations. For example, clients taking part in an alcohol programme may role-play situations where they are offered a drink. Educational programmes are usually led by a teacher or facilitator, although the issues for discussion may be decided by the clients. Educational interventions require the practitioner to understand the principles of adult learning and the factors which help or hinder learning (Ewles & Simnett 2003).
Evaluation
Increases in knowledge are relatively easy to measure. Health education through mass-media campaigns, one-to-one education and classroom-based work have all shown success in increasing information about health issues, or the awareness of risk factors for a disease. Information alone is, however, insufficient to change behaviour and, as we shall see in Chapter 9, even the desire and ability to change behaviour are no guarantee that the individual will do so.
Empowerment
Aims
The World Health Organization (1986) defined health promotion as enabling people to gain control over their lives. This approach helps people to identify their own concerns and gain the skills and confidence to act upon them. It is unique in being based on a ‘bottom-up’ strategy and calls for different skills from the health promoter. The health promoter needs to become a facilitator whose role is to act as a catalyst, getting things going and freeing up resources, and then to withdraw from the situation.
 BOX 5.6
BOX 5.6When we talk of empowerment, we need to distinguish between self-empowerment and community empowerment. Self-empowerment is used in some cases to describe those approaches to promoting health which are based on counselling and which use non-directive, client-centred approaches aimed at increasing people’s control over their own lives. For people to be empowered they need to:
Empowerment is also used to describe a way of working which increases people’s power to change their ‘social reality’. Chapter 10 includes a discussion of community development as a way of working which seeks to create active participating communities who are empowered, and able to challenge and change the world about them. This may or may not include political consciousness-raising such as that advocated by the radical educationist Paulo Freire (1972).
Methods
Many health, education and social care practitioners use empowerment strategies, which may be referred to as client-centred approaches, advocacy or self-care. Laverack (2005) states that the challenge for practitioners is to use their own power (power-over) to help clients to gain power (power-from-within).
Empowering though reminiscence
Reminiscence is an example of a communication strategy which encourages older people to tell their story and recall past events. This provides opportunities for them to say what kind of care they want. It shifts the balance of the relationship to the client or patient and helps build trust and understanding. In dementia care, older people can be encouraged to retrieve their past experience and maintain their personhood. Some ethnic groups with strong oral traditions use reminiscence to preserve their cultural identity (Coleman & O’Hanlon 2004).
Community development is a similar way of working to empower groups of people by identifying their concerns and working with them to plan a programme of action to address these concerns. Some health promoters have a specific remit to undertake community development work; most do not. Community development work is time-consuming and most health promoters have clearly defined priorities which take up all their time. Funding for this kind of work is invariably insecure and short-term. The communication, planning and organizational skills necessary for this approach may not be included in professional training. For many health promoters, relinquishing the expert role may be difficult and uncomfortable. Ways of working with communities are discussed more fully in Chapter 10.
Evaluation
Evaluation of such activity is problematic, partly because the process of empowerment and networking is typically long-term. This makes it difficult to be certain that any changes detected are due to the intervention and not some other factor. In addition, positive results of such an approach may appear to be vague and hard to specify, especially when compared to outcomes used by other approaches, such as targets or changes in behaviour which are capable of being quantified. Evaluation includes the extent to which specific aims have been met (outcome evaluation) and the degree to which the group has gelled, or been empowered as a result of the intervention (process evaluation). Evaluation therefore needs to include qualitative methods that reveal people’s perceptions and beliefs as well as quantitative methods that demonstrate outcomes such as behaviour change.
Social change
Aims
This approach, which is sometimes referred to as radical health promotion, acknowledges the importance of the socioeconomic environment in determining health. Its focus is at the policy or environmental level, and the aim is to bring about changes in the physical, social and economic environment which will have the effect of promoting health. This may be summed up in the phrase ‘to make the healthy choice the easier choice’. A healthy choice is available, but to make it a realistic option for most people requires changes in its cost, availability or accessibility. Chapter 11 discusses the processes involved in creating healthy public policies.
Several studies have shown that a healthy diet which includes fruit and vegetables costs more than the typical diet of a low-income family (Cade et al 1999). What should be the focus of health promotion interventions on healthy eating?
You may have included some of the following:
Methods
The social change or radical approach is targeted towards groups and populations, and involves a top-down method of working. Although there may be widespread consultation, the changes being sought are generally within organizations, and require commitment from the highest levels. Chapter 11 discusses developing healthy public policy and how legislation has had an enormous impact on the nation’s health. The successful implementation of policy and legislation requires the support of the public which is achieved through education, lobbying and social marketing. Chapter 12 discusses social marketing in greater detail.
For most health promotion workers, the scope for this type of activity will be more limited than for the traditional medical or behaviour change approaches. The necessary skills for working in this way, such as lobbying, policy planning, negotiating and implementation, may not be included in professional training. Working in such a way may be interpreted as beyond the brief of the job, too political or someone else’s remit. There is however scope for professional organizations to become involved as stakeholders in social change processes. For example, health practitioners’ professional bodies were involved in lobbying for a total smoking ban in public places, alongside pressure groups such as Action on Smoking and Health (ASH) (Ford 2005).
Evaluation
Evaluation of the social change approach includes outcomes such as legislative, organizational or regulatory changes which promote health, e.g. regulations governing food labelling, a ban on tobacco sponsorship and advertising or a ban on smoking in public places.
The extent of partnership working and the profile of health issues on common agendas may also be used to demonstrate a greater degree of commitment to social change for health. These outcomes are typically long-term, complex processes where it would be difficult to prove a link to particular health promotion interventions.
Are there parts of your work which are aimed at social change? Have you sought to influence policies and practices which affect health?
Organizational development, environmental health measures, economic or legislative activities and public policies on housing, education or the provision of services may all be examples of health promotion aimed at social change.
Partnership working with other agencies enables the socioeconomic and environmental determinants of health to be targeted, e.g. health, education and environment practitioners may work together to lobby for the provision of safe outdoor recreation areas.
Practitioners may seek to address the root causes of ill health by developing health profiles, conducting health equity audits, working in partnerships with other agencies, social commentary and research.
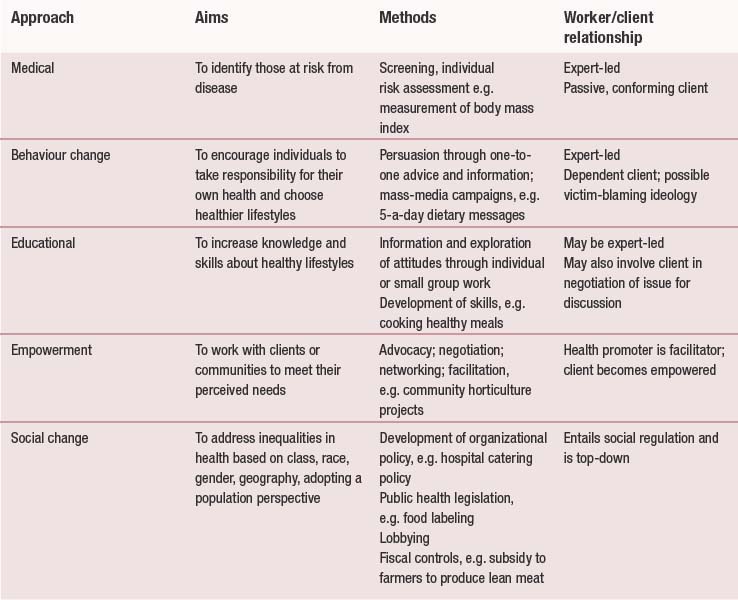
Table 5.1 uses the example of healthy eating to show how different approaches to health promotion will have different aims and use different methods, The public health White Paper Choosing Health: Making Healthier Choices Easier Choices has the following priorities: reducing smoking, reducing obesity and improving diet,encouraging sensible drinking, improving sexual health and improving mental health (Department of Health 2004). Consider how health promotion interventions in one of these areas will be affected by working with the five identified approaches to health promotion: medical, behaviour change, educational, empowerment and social change.
Models of health promotion
The above schema of different approaches to health promotion is primarily descriptive. It is what health promoters do, and it is possible to move in and out of different approaches depending on the situation. A more analytical means of identifying types of health promotion is to develop models of practice. All models, be they building models, diagrammatic maps or theoretical models, seek to represent reality in some way and try to show in a simplified form how different things connect. Implicit in the use of models is a theoretical framework that explains how and why the elements in the model are connected. Theory is defined as ‘systematically organized knowledge applicable in a relatively wide variety of circumstances devised to analyze, predict or otherwise explain the nature or behaviour of a specified set of phenomena that could be used as the basis for action’ (Van Ryn & Heany 1992). Models of health promotion may help to:
Using a model can be helpful because it encourages you to think theoretically, and come up with new strategies and ways of working. It can also help you to prioritize and locate more or less desirable types of interventions.
There has been a proliferation of models in health promotion literature, with large areas of overlap but little consensus on terminology or underlying criteria. Thus we find that Beattie (1991) uses criteria of ‘mode of intervention’ (authoritative-negotiated) and ‘focus of intervention’ (individual–collective) to generate four models (see Figure 5.2 below). Caplan & Holland (1990) use ‘theories of knowledge’ and ‘theories of society’ (see Figure 5.1 below). The terminology for models also varies. For example, French (1990) calls a social change approach ‘politics of health’, whilst Caplan & Holland (1990) distinguish between a radical model and a Marxist model. This can be extremely confusing for the reader.
The following two models derive from sociological and social policy frameworks. They adopt a structural analysis which draws attention to the material and social influences on health and the social structures which contribute to inequalities in health. They show how health promotion approaches are influenced by political ideology and different value positions about power, responsibility and autonomy.
Caplan & Holland (1990)
This model suggests that there are essentially four paradigms or ways of looking at health promotion. These paradigms can be generated from two dimensions (Figure 5.1). The first dimension is concerned with the nature of knowledge. Knowledge is seen as based along a continuum which ranges from subjective approaches to understanding through to objective approaches. Objective explanations deriving from science (e.g. health is the absence of disease) are only part of the picture. Emphasis may also be given to lay accounts and people’s own unique interpretations of what their health means to them.
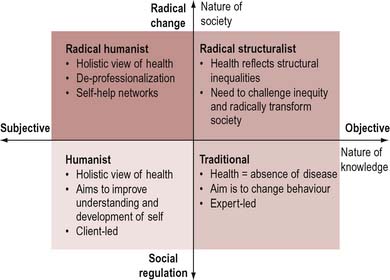
Figure 5.1 Four paradigms or perspectives of health promotion. Adapted from Caplan & Holland (1990).
The second dimension relates to assumptions concerning the nature of society. These range from theories of radical change to theories of social regulation. When these two dimensions are put together it suggests four paradigms or perspectives of health promotion, as illustrated in Figure 5.1.
Each quadrant represents a major approach to the understanding of health and the practice of health promotion. They are not necessarily exclusive but there will be situations when to hold one position or approach precludes the adoption of other approaches. Each quadrant incorporates different theoretical and philosophical assumptions about society, concepts of health and the principal sources of health problems.
The model is useful in showing that practice is the outcome of deeper social conflicts and values.
Beattie (1991)
Beattie offers a structural analysis of the health promotion repertoire of approaches. He suggests that there are four paradigms for health promotion (Figure 5.2). These are generated from the dimensions of mode of intervention, which ranges from authoritative (top-down and expert-led) to negotiated (bottom-up and valuing individual autonomy). Much health promotion work involving advice and information is determined and led by practitioners. Equally, policy work may also be expert-led, the priorities determined by epidemiological data. The other dimension relates to the focus of the intervention which ranges from a focus on the individual who is responsible for his or her own health to a focus on the collective and the roots of ill health.
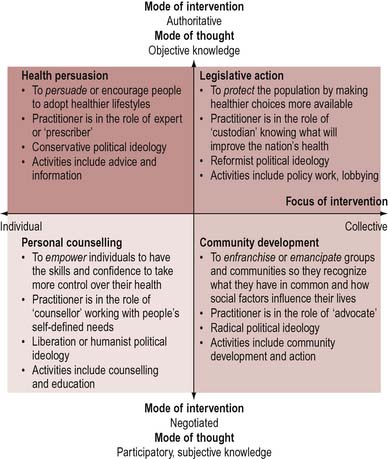
Beattie’s typology generates four strategies for health promotion.
Figure 5.2 shows how Beattie’s model can point up the following aspects:
Each of the four strategies corresponds to a different political perspective. Thus conservative reformist perspectives see health promotion as attempting to correct or repair what is seen as a deficit in the conservative perspective (e.g. lack of information) or an aspect of deprivation in the reformist perspective (e.g. difficulties of access). These perspectives give rise to authoritative and prescriptive approaches. Libertarian and radical perspectives both see health promotion as seeking to empower or enfranchise individuals. The radical perspective, in addition, seeks to mobilize and emancipate communities. Each of these perspectives also casts the practitioner in a different role in relation to clients.
Beattie’s model is a useful one for health promoters because it identifies a clear framework for deciding a strategy, and yet reminds them that the choice of these interventions is influenced by social and political perspectives.
Tannahill (Downie et al 1996)
This model of health promotion is widely accepted by health care workers. Tannahill talks of three overlapping spheres of activity: health education; prevention; and health protection.
Tannahill’s diagrammatic representation (Figure 5.3) shows how these different approaches relate to each other in an all-inclusive process termed health promotion.The model is primarily descriptive of what goes on in practice. It is useful for the health promoter to see the potential in other areas of activity, and to see the scope of health promotion. It does not, however, give any insight into why a practitioner may choose one approach over another. It suggests that all approaches are interrelated but, as we have seen, they reflect distinctive ways of looking at health issues.
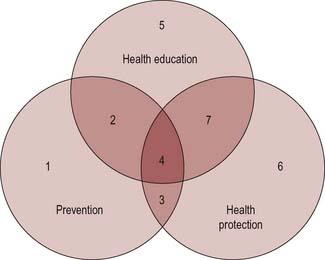
Figure 5.3 Tannahill’s model of health promotion. From Downie et al (1996).
Tones (Tones & Tilford 2001)
The following model claims to be an empowerment model which has as its cardinal principle the goal of enabling people to gain control over their own health. It prioritizes empowerment, which is seen as both the core value and the core strategy underpinning and defining the practice of health promotion.
Tones makes a simple equation that health promotion is an overall process of healthy public policy × health education (Figure 5.4).
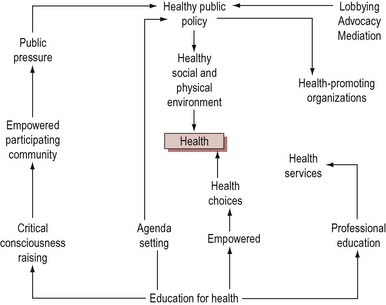
Tones considers education to be the key to empowering both lay and professional people by raising consciousness of health issues. People are then more able to make choices and to create pressure for healthy public policies. We have seen how there is a distinction between self-empowerment and community empowerment. Tones argues that there is a reciprocal relationship between the two. Changes in the social environment achieved through healthy public policies will facilitate the development of self-empowered individuals. People who have the skills to participate effectively in decision-making are better able to access resources and shape policy to meet their needs. The support of individuals is also necessary for implementing change. Empowerment, as opposed to prevention or a radical political approach, is the main aim of health promotion in Tones’ model. Working for empowerment enhances individual autonomy and enables individuals, groups and communities to take more control over their lives.
Conclusion
A number of quite different activities are subsumed under the label ‘health promotion’. Attempts to organize these activities into different categories have generated a plethora of models and typologies. The most obvious starting point is to describe the variety of current practice and this is the approach taken at the beginning of this chapter.
However, there are limitations to this method and it may be criticized as being insufficiently analytical. Theorists who have taken this one step further have identified key criteria which serve to locate different forms of practice, both existing and potential. Adopting a more analytical approach enables judgements to be made about more and less desirable forms of practice, and opens up these judgements for debate. If health promotion is to progress as a discipline and an activity in its own right, a strong theoretical framework is necessary.
The search to clarify models and typologies of practice may appear to be academic and unrelated to the ‘here and now’ of your activities to promote health. However, we would argue that for practice to grow beyond a reactive response to demands made by others, practitioners need to have an idea of all available options and reflect on which approaches are most congruent with their own beliefs and values. It is only when we can contemplate different ways of promoting health that we can make judgements as to what is possible and what is preferable. Recognizing that the two are not always synonymous may be frustrating in the short term, but must in the long term contribute towards the effectiveness and efficiency of health promotion.