Chapter 27 Infections of the genitourinary tract
Normal flora and the natural defences of the genitourinary tract
The predominant vaginal flora in adult women consists of lactobacilli. They keep the vaginal pH low and appear to prevent the growth of potential pathogens. For instance, their suppression by antibiotics may lead to overgrowth of the yeast Candida albicans found in relatively low numbers in the healthy vagina. Other common groups of vaginal organisms include diphtheroids, streptococci, anaerobes and coliforms. Most of these organisms may behave as opportunistic pathogens when appropriate conditions supervene. Approximately 20% of women of child-bearing age carry group B β-haemolytic streptococci in the vagina. These may be acquired by a baby during its passage through the birth canal, resulting in serious infections such as meningitis and sepsis.
The urine in the bladder is normally sterile, but the voided urine often becomes contaminated by flora from the distal portions of the urethra, such as Staphylococcus epidermidis, coliforms, diphtheroids and streptococci. Additionally, in females, the organisms present in the distal part of the urethra may include contaminants from the gut flora such as enterobacteria and lactobacilli. The flushing action of the urine is arguably the most important defence factor of the urethra in both males and females. Bactericidal mechanisms in the bladder mucosa, including local antibody response and lysozyme, play an important role in preventing ascending infection of the urinary tract.
Important pathogens
Important pathogens are listed in Figure 27.1 and Table 27.1.
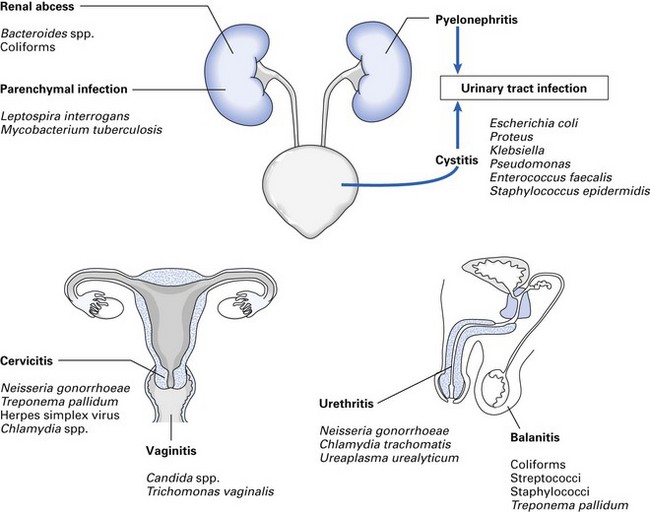
Table 27.1 Sexually transmitted diseases
| Disease | Agent |
|---|---|
| Bacterial infections | |
| Gonorrhoea | Neisseria gonorrhoeae (the gonococcus) |
| Syphilis | Treponema pallidum |
| Vaginitis | Gardnerella vaginalis, anaerobes |
| Chancroid | Haemophilus ducreyi |
| Viral infections | |
| Genital herpes | Herpes simplex virus (type 2 mainly) |
| Genital warts | Papillomavirus |
| Hepatitis Ba | Hepatitis B virus |
| AIDSa | Human immunodeficiency virus (HIV) |
| Others | |
| Lymphogranuloma venereum | Chlamydia trachomatis types L1–L3 |
| Granuloma inguinale (donovanosis) | Calymmatobacterium granulomatis (a Klebsiella-like microorganism) |
| Pubic lice (crabs) | Phthirus pubis |
| Genital scabies | Sarcoptes scabiei |
| Non-specific urethritis | Chlamydia trachomatis types D–K |
| Trichomoniasis | Trichomonas vaginalis |
| Vaginal thrush | Candida albicans |
AIDS, acquired immune deficiency syndrome.
Sexually transmitted diseases
A large group of infections are essentially transmitted by sexual intercourse; they may affect both heterosexual and homosexual partners. Varying patterns of sexual behaviour can result in such infections manifesting in the oral cavity, oropharynx and the rectum; sexually transmitted diseases frequently – but not invariably – produce genital lesions; several produce severe systemic disease that may even lead to death, such as human immunodeficiency virus (HIV) infection and hepatitis B.
Gonorrhoea
Gonorrhoea is caused by Neisseria gonorrhoeae (the gonococcus).
Clinical features
In women: acute urethritis, increased vaginal secretions with purulent discharge. In men: acute gonococcal urethritis with severe dysuria and purulent discharge. The disease may involve the rectum and oropharynx. Pharyngitis, sore throat, tonsillitis and gingivitis may occur as a result of gonococcal infection, especially from orogenital contact in homosexual men. Asymptomatic infection is common in both men and women. Complications include prostatitis, salpingitis and occasionally haematogenous spread, causing arthritis, septicaemia and meningitis.
Pathogenesis and epidemiology
Gonococcal infection has been reported only in humans. The infection is limited to the mucosa of the anterior urethra in men and the cervix of women. In the newborn, gonococcal conjunctivitis may occur due to cross infection from the mother’s birth canal.
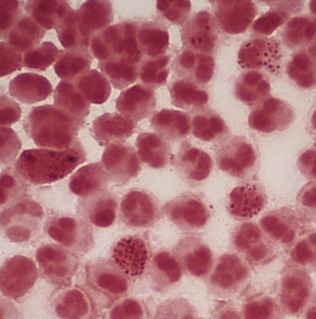
Diagnosis
Gram smears show Gram-negative pairs of the typical kidney-shaped gonococci inside neutrophils (Fig. 27.2). Swabs from the urethra cultured on lysed blood or chocolate agar yield oxidase-positive, translucent colonies, and rapid carbohydrate utilization tests are also diagnostic (see Chapter 14).
Non-specific urethritis
One of the most common sexually transmitted diseases, non-specific urethritis is seen more in men than in women. It is caused by more than one agent, but Chlamydia trachomatis is the most common cause. A mycoplasmal organism (‘bacteria’ without a cell wall), Ureaplasma urealyticum, may also cause significant morbidity.
Clinical features
Acute purulent urethral discharge resembles that of gonorrhoea; cervicitis occurs in women.
Diagnosis
Smears and swabs of urethral or cervical discharge are diagnostic. Culture is now rarely done. Smears are examined for intracytoplasmic inclusions by immunofluorescence. Serology for chlamydial antigens by indirect immunofluorescence with monoclonal antibody or by enzyme-linked immunosorbent assay (ELISA).
Syphilis
The incidence of syphilis worldwide has increased in recent years, and in 2006, the figure was estimated to be 12 million worldwide and 70 000 new cases were reported in the USA.
Syphilis is one of the classic diseases with protean manifestations (i.e. affecting virtually all organ systems of the body), and has re-emerged as an important disease associated with HIV infection and sexual promiscuity. The disease, important due to its late and severe sequelae, is preventable, and treatable with effective and inexpensive antibiotics.
The disease is caused by Treponema pallidum, the syphilis spirochaete.
Clinical features
Syphilis has an incubation period of 10–90 days (average 3 weeks) and is characterized by four main clinical stages: primary, secondary, tertiary and late or quaternary (Fig. 27.3).
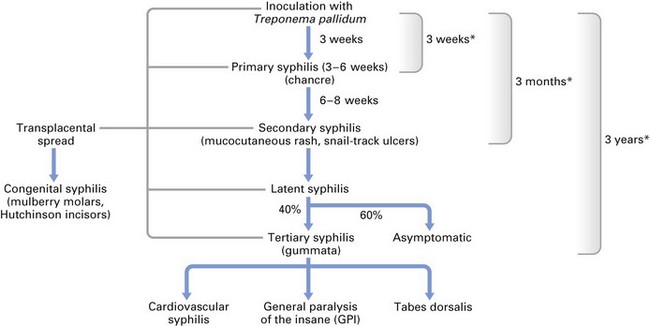
Primary syphilis
A painless red papule develops at the inoculation site of the spirochaete, some 3 weeks (range 9–90 days) after the contact; this may be in the labia, vagina, cervix, penis or the oral mucosa. The papule then produces the chancre of primary syphilis: a flat, red, indurated, highly infectious ulcer with a serous exudate. Enlarged, painless regional lymphadenopathy is common. The chancre disappears spontaneously within 3–8 weeks.
Secondary syphilis
This stage is reached 6–8 weeks later and lasts for 1–3 months. A generalized mucocutaneous spread of the spirochaetes ensues at this stage and the lesions appear as papules on the skin and oral ulcers (see Chapter 35). The ulcers may coalesce to give the characteristic ‘snail tracks’ and mucous patches in about a third of those affected (Fig. 27.4). These lesions, like the primary chancre, are highly infectious. Other manifestations are generalized lymphadenopathy and condylomata (warts) of the anus and vulva; rarely, periostitis, arthritis and glomerulonephritis may be seen.

Tertiary syphilis
The most destructive phase of the disease occurs 3–10 years after primary syphilis. Lesions appear as characteristic gummata or granulomatous nodules of the skin, mucosa, bone and other internal organs. Gummata commonly break down to produce shallow, punched-out ulcers. In the oral cavity, gumma may rarely break down to produce palatal perforations, leading to oronasal fistulae. These lesions are not infective as the tissue damage is due to a delayed type of hypersensitivity reaction.
Late or quaternary syphilis
Occurs 10–20 years after primary syphilis. The two main clinical forms of late syphilis are cardiovascular syphilis and neurosyphilis, with resultant pathology of the aorta and the nervous system, respectively.
Latent syphilis
This may be seen in some after many years without any symptoms. The disease lies dormant without any clinical signs (except for positive serology) and may manifest as cardiovascular or neurosyphilis.
Congenital syphilis
Treponema pallidum is one of the few microorganisms that has the ability to cross the placental barrier; thus, the foetus may be infected during the second or third trimester from a syphilitic mother (either in the primary or secondary stage of syphilis). The disease will manifest in the infant as:
Diagnosis
Direct microscopy
Spirochaetes in exudate from primary or secondary lesions are identified by dark-ground microscopy; now rarely done. Care should be taken to differentiate T. pallidum from oral spirochaetes when oral lesions are examined. Note: T. pallidum cannot be grown in laboratory media but can be propagated in the testes of rabbits.
Serology
Antigens used for syphilis serology are of two types:
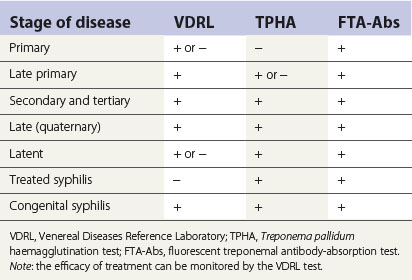
The interpretation of syphilis serology is complex (because of the many medical conditions that yield false-positive reactions) and is not discussed here.
Recently, it has been shown that real-time polymerase chain reaction (PCR) is a fast, efficient and reliable test for the diagnosis of primary syphilis, but no added value for the diagnosis of secondary syphilis.
Notes on some common sexually transmitted diseases
HIV infection
This is a pandemic infection commonly transmitted by sexual intercourse and is also a disease of enormous importance for health care personnel (see Chapter 30).
Trichomoniasis
A common protozoal infection in women is caused by Trichomonas vaginalis. It is transmitted mainly by sexual intercourse: in men, the infection is often symptomless; in women, it manifests as a chronic vaginal infection ranging from a yellow, offensive discharge with vaginitis to symptomless or low-grade infection.
Candidiasis
Candidiasis is a yeast infection commonly transmitted by sexual intercourse; it is frequently seen in women but rare in men. Candida albicans is the most frequent causative yeast; the disease is characterized by white false membranes in the vulva and the vagina, which may be accompanied by a watery discharge; many cases are symptomless.
Diagnosis and treatment are as described in Chapter 22.
Herpes genitalis
Mainly due to herpes simplex type 2 virus, but as a result of sexual promiscuity, type 1 viruses (which are more or less confined to oral regions) are frequently implicated. The lesions are vesicular and painful, and seen in anogenital regions. The primary lesion, associated with fever and inguinal lymphadenopathy, is more protracted and painful than the secondary recurrences. Asymptomatic infection is common in both men and women; hence, sexual spread of the disease is common.
Diagnosis and treatment are as described in Chapter 21.
Control of sexually transmitted diseases
Although control is difficult, tracing of sexual partners of infected individuals is essential to prevent spread of disease in the community. Patients are requested to name consorts and the latter should submit themselves to examination and treatment. In the long term, prevention of sexually transmitted diseases, including HIV infection, is far more important in reducing health care costs of the community.
Urinary tract infections
Urinary tract infections are common, especially in women, despite the availability of a spectrum of antibiotics. They are defined as follows:
Cystitis, pyelonephritis or urethritis may occur either singly or in combination.
Important pathogens
Causative agents are many and varied (see Fig. 27.1) but Escherichia coli is the most common, accounting for 60–80% of infections. Some E. coli strains are more invasive than others, possibly as a result of the possession of capsular or K antigens, which inhibit phagocytosis, and their superior ability to adhere to the uroepithelium with the aid of the pili on cell surfaces.
Other organisms that commonly cause infection include:
Note: acute urinary tract infection is mostly monomicrobial in origin, while polymicrobial infection with more than one organism is common in chronic infections.
Clinical features
Urinary tract infection is mainly a disease of women, with a male to female ratio of 1 : 10. Clinical features of cystitis include dysuria, urgency, suprapubic pain, increased frequency and haematuria. Fever, loin pain and tenderness are signs of pyelonephritis.
Dentistry and genitourinary infections
It is important that the dentist is aware of sexually transmitted diseases as many of them manifest in the oral cavity as a result of deviant sexual habits and the escalating sex industry in both developed and developing countries. Indeed, some would consider the oral cavity as a sexual organ. Furthermore, organisms that may cause sexually transmitted diseases (e.g. herpes, HIV infection) may have the propensity to be transmitted in the clinical setting, from the patient to the dentist, by direct contact or indirectly via contaminated instruments if appropriate infection control measures are not implemented.
Urinary tract infections are of no direct relevance to dentistry except insofar as patients are taking antibiotics, which may either affect the oral flora or, rarely, interact with drugs prescribed by the dentist. Indeed, the potential of metronidazole to kill anaerobic bacteria was first detected by an astute dentist who noted the resolution of acute ulcerative gingivitis in a patient under his care who was undergoing treatment for vaginal trichomonal infection with this drug (at that time prescribed solely as an antiprotozoal agent).
Key facts
Doherty L., Fenton K.A., Jones J., et al. Syphilis: Old problem, new strategy. British Medical Journal. 2002;325:153-156.
Greenwood D., Slack R., Peutherer J., editors. Medical microbiology, 16th ed., Edinburgh: Churchill Livingstone, 2002.
Shanson D.C. Infections of the urinary tract; sexually transmitted diseases, Ch. 20. Microbiology in clinical practice, 3rd ed. Oxford: Butterworth-Heinemann. 1999.
Siegel M.A. Syphilis and gonorrhea. Dental Clinics of North America. 1996;40:369-383.
Review questions (answers on p. 354)
Please indicate which answers are true, and which are false.