Chapter 30 Human immunodeficiency virus infection, AIDS and infections in compromised patients
Human immunodeficiency virus infection and acquired immune deficiency syndrome
By the end of 2008, an estimated 33.4 million people worldwide were living with human immunodeficiency virus (HIV) infection. That same year, some 2 million people died of acquired immune deficiency syndrome (AIDS)-related illnesses, and in total, 20 million globally have died of AIDS and related illnesses thus far. Globally, less than one person in five at risk of HIV has access to basic HIV prevention services. Only 36% of people who needed HIV treatment had access to it by the end of 2009.
Although HIV infection is now a global pandemic, AIDS was only described in 1981, in young homosexual men in the USA. However, the disease appears to have originated in Africa, where cases have been revealed from as long ago as 1959. The virus causes depletion of CD4+ T-helper lymphocytes over many years; as a consequence of which, patients succumb to opportunistic infections, particularly Pneumocystis carinii pneumonia (PCP) and oral candidiasis, and neoplasms, especially Kaposi’s sarcoma.
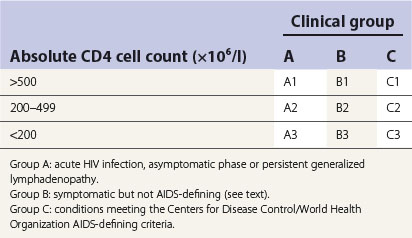
After infection with HIV, there is a prolonged asymptomatic period that may last up to 10 years, but the risk of developing severe immunodeficiency and AIDS increases with time. Thus, the clinical spectrum of HIV infection is broad, ranging from asymptomatic or mild infection to severe clinical illness and profound immunodeficiency. The variety of clinical manifestations seen in AIDS has spawned a number of definitions of the disease. However, the US Centers for Disease Control and Prevention has rationalized and revised these to include all patients with CD4+ cell counts of less than 200 per microlitre.
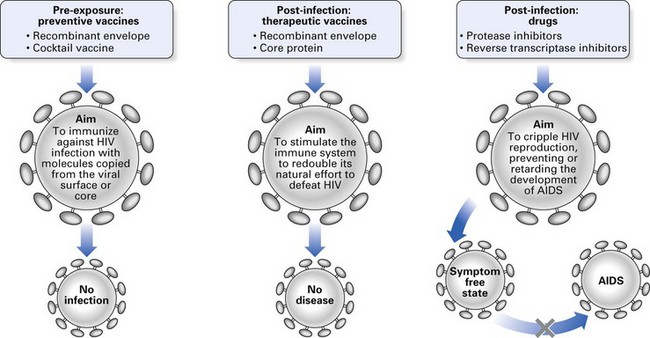
The battle to conquer HIV infection and AIDS is fought on many fronts, consuming millions of dollars, and thus far all efforts at producing a preventive vaccine have failed. However, the introduction of new antiviral regimens such as highly active antiretroviral therapy (HAART) has increased life expectancy in HIV infection and dramatically reduced complications, suppressing viral replication to undetectable levels.
The impact of HIV and AIDS on the practice of clinical dentistry has been enormous; first, because of the regimentation in infection control it has spawned throughout the profession, and second, because of the many oral manifestations and their management, of which the practising dentist has to be aware.
Definitions
Retroviridae
HIV is a lymphotrophic virus that belongs to the family Retroviridae. The latter RNA viruses comprise a single taxonomic group made up of three subfamilies:
Human immunodeficiency virus
The virus has a diameter of 100 nm, and its structure is described below. There are two types: HIV-1 is the most prevalent; HIV-2 is a variant that originated in West Africa and has spread to Central Africa, Europe and South America. Type 1 is classified into two major groups: M, containing 10 genetically distinct subtypes (A–J), and O, containing a heterogeneous collection of viruses. Type 2 HIV, except for its antigenic and nucleic acid profile, has similar biological properties to HIV-1.
The structure of HIV is shown in Figure 30.1. It consists of:
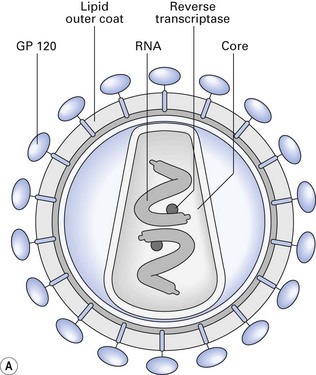
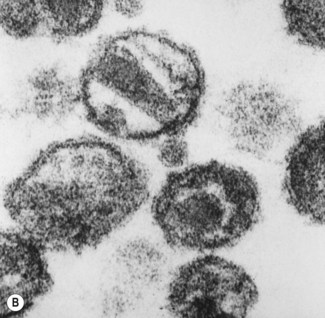
Fig. 30.1 Human immunodeficiency virus. (A) Structure; (B) scanning electron micrograph of virions showing the pyramid-shaped central core.
Stability of HIV
The survival of HIV under varying conditions has been investigated.
Important: the above figures indicate the limits of survival at very high starting concentrations of HIV (up to 1000 times more than the levels found in the blood of patients) under experimental conditions. Also, the efficacy of the mentioned disinfectants is affected by a variety of factors such as the associated organic bioburden. Hence, care and strict adherence to protocols are essential when dealing with HIV.
Transmission of HIV
The virus is most commonly acquired by having sex with an infected partner. The virus can enter the body through the lining of the vagina, vulva, penis, rectum or mouth during sex. The infection can also be transmitted by exchange of infected blood, or other body fluids such as breast milk, and is not transmitted by social or casual, non-sexual contact. Currently, heterosexual sex is the major mode of transmission worldwide. Other notable transmission modes include sharing of needles, vertical transmission in utero, breast-feeding and transfusion of infected blood or blood products (factor VIII concentrate). Occasional cases of HIV infection result from needlestick injuries in health care settings. The question of HIV transmission among health care workers, including dentists, is addressed at the end of this chapter.
Saliva and HIV transmission
There is only a very slim possibility that HIV may be transmitted by saliva, for the following reasons.
Epidemiology
The main groups of individuals affected are:
The global pandemic
As mentioned above, by the end of 2008, an estimated 33.4 million people worldwide were living with HIV, and some 20 million have died of HIV infection or related illnesses since the beginning of the epidemic: one person is infected with HIV every 6.4 s. Of those succumbing to AIDS, 90% are living in developing countries, especially in Asia and Africa. The estimated annual increase worldwide is about 20%, but this varies widely in different geographic locales. For instance, the annual increase is about 11% in the Americas, 26% in Africa and 167% in Asia, indicating the staggering explosion of the disease in the latter region. India is the new epicentre of the disease, and it is estimated that by 2010, some 20 million Indians will be infected with HIV. This reflects to a great extent the close link between the disease and the economic, social and cultural issues and taboos in each region.
Currently, HIV infection is the leading cause of death in US men aged 25–44 year. In some countries, such as the Ivory Coast, HIV/AIDS is the leading cause of death; and in Uganda, it causes 80% of deaths in adults aged 20–39 years.
Acquired immune deficiency syndrome
Natural history of the disease
AIDS is an insidious disease, characterized by opportunistic infections (fungal, viral and mycobacterial), malignancies (especially Kaposi’s sarcoma and lymphomas that may be virally induced) and autoimmune disorders (Fig. 30.2).
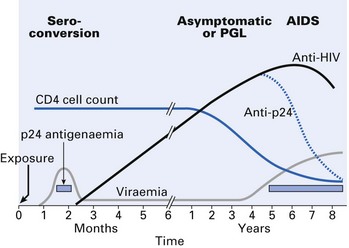
The average time to development of AIDS is 8–11 years in most adults in the developed world, and much less in the developing world due to aggravating cofactors such as malnutrition and intercurrent infection (e.g. malaria). A few individuals (some 2%) have not developed AIDS despite antibody positivity. Overall, almost half of those diagnosed with AIDS will die. Untreated, the median survival is about 1 year from the time of diagnosis, and 95% will die within 5 years.
Mean time for seroconversion after exposure to HIV is 3–4 weeks, with the onset of an acute seroconversion illness similar to glandular fever. Most will have antibodies within 6–12 weeks after infection and virtually all will be positive within 6 months. Symptoms of such seroconversion include fever, malaise, rash, oral ulceration and, occasionally, encephalitis and meningitis. In some, the disease may then become quiescent and asymptomatic for several years (range 1–15 years or more) for reasons yet unknown. Some of them may have persistent generalized lymphadenopathy (PGL), where the enlarged lymph nodes are painless and asymmetrical in distribution and involve submandibular and neck nodes. In the HIV disease classification, patients with these symptoms are categorized as group A (Table 30.1).
Progressive disease leads to other features, including fatigue, fever, weight loss, candidiasis, diarrhoea, hairy leukoplakia, herpes zoster and perianal herpes, and these illnesses are sometimes referred to as the AIDS-defining complex. Patients with these symptoms and signs of progressive illness are categorized as group B.
Finally, a percentage of HIV-infected individuals develop full-blown AIDS (50–70% depending on drug therapy and other associated cofactors; median life expectancy is 18 months). These individuals are in group C. The AIDS-defining conditions are subdivided into opportunistic infections and secondary neoplasms, and include Kaposi’s sarcoma, PCP and many other exotic infections (Table 30.2).
Table 30.2 Opportunistic infections, neoplasms and miscellaneous complications of HIV disease
| Opportunistic infections | |
| Mucocutaneous | Human herpesviruses |
| 1, 2, 3, 4, 5, 8 | |
| Human papillomaviruses | |
| Molluscum contagiosum | |
| Non-tuberculous mycobacteria | |
| Candida albicans | |
| Staphylococcus aureus | |
| Histoplasmosis | |
| Gastrointestinal | Cryptosporidiosis |
| Microsporidiosis | |
| Isosporiasis | |
| Giardiasis | |
| Respiratory | Pneumocystis carinii |
| Aspergillosis | |
| Candidosis | |
| Cryptococcosis | |
| Histoplasmosis | |
| Zygomycosis (mucormycosis) | |
| Strongyloidosis | |
| Mycobacteria, including tuberculosis | |
| Staphylococcus aureus | |
| Streptococcus pneumoniae | |
| Haemophilus influenzae | |
| Toxoplasmosis | |
| Cytomegalovirus (CMV) | |
| Meningitis | Creutzfeldt–Jakob agent |
| Encephalitis | Papovaviruses |
| Cryptococcus neoformans | |
| Toxoplasma gondii | |
| Neoplasms | |
| Kaposi’s sarcoma | |
| Lymphoma | |
| Squamous cell carcinoma | |
| Leukaemia | |
| Miscellaneous | |
| Encephalopathy | |
| Thrombocytopenic purpura | |
| Lupus erythematosus | |
| Seborrhoeic dermatitis |
The Centers for Disease Control disease classification also incorporates blood CD4 lymphocyte count, as a decrease in the latter is associated with adverse prognosis (Table 30.1).
Opportunistic infections and neoplasms in AIDS
The opportunistic infections, neoplasms and other features of AIDS and its prodrome are listed in Table 30.2.
Pneumocystis carinii pneumonia
This pneumonia is caused by an extracellular protozoan, P. carinii, which grows slowly in its trophozoite and cyst forms within the lung alveoli. Seen in 80% of patients, it is the immediate cause of death in 20% of those dying with AIDS. It is treated with aerosolized pentamidine.
Toxoplasmosis
Protozoal infection with Toxoplasma gondii is seen in 15% of AIDS patients, affecting especially the central nervous system.
Atypical mycobacteriosis
Atypical mycobacteriosis is present in about 40% of patients in the West; caused by Mycobacterium avium complex (MAC) infections due to mycobacteria such as Mycobacterium avium and Mycobacterium intracellulare. In some countries, up to a quarter of HIV-positive people are infected with Mycobacterium tuberculosis, which may be increasingly drug-resistant (multidrug-resistant tuberculosis (MDR-TB): see Chapter 19).
Orofacial manifestations of HIV infection
The earliest indicators of HIV infection may manifest in the oral cavity, and some 50 disease entities that may affect the orofacial region of HIV-infected patients have been described. However, with advent of HAART therapy (see below), the prevalence of oral manifestations has dramatically reduced. The more common orofacial manifestations of HIV infection are (Table 30.3):
Table 30.3 Oral manifestations of HIV disease
| Strongly associated | Less common associates | Sometimes seen |
|---|---|---|
| Candidiasis | Herpes simplex or zoster infection | Exotic fungal infections (ulcers) |
| Erythematous | Human papillomavirus infections | Cryptococcosis |
| Pseudomembranous | Mycobacterial infections | Histoplasmosis |
| Linear gingival erythema | Penicilliosis | |
| Hairy leukoplakia | ||
| Kaposi’s sarcoma (not in Asia) | Unilateral/bilateral swelling of salivary glands | Drug reactions |
| Necrotizing (ulcerative) gingivitis | Dry mouth | Cranial neuropathies |
| Necrotizing (ulcerative) periodontitis | Ulceration (non-specific) | Facial palsies |
| Melanotic hyperpigmentation | Trigeminal neuralgia | |
| Non-Hodgkin’s lymphoma | Recurrent aphthous stomatitis |
Oral candidiasis
Oral candidiasis (usually erythematous or pseudomembranous candidiasis) is very common in HIV infection, especially at the early stage of the disease; it is a reliable and ominous prognostic indicator of the disease progression to AIDS (the earlier the appearance of oral candidiasis, the worse the prognosis). Oesophageal candidiasis frequently accompanies oral candidiasis and is usually managed by azole drugs, commonly fluconazole. However, azole resistance is increasingly common.
Linear gingival erythema and angular cheilitis are possibly due to mixed fungal and bacterial infections (see Chapter 35).
Viral infections
Viral infections include herpetic stomatitis, herpes zoster, Kaposi’s sarcoma and others such as hairy leukoplakia and papillomas of viral origin.
Herpetic stomatitis
A 10% prevalence of herpetic stomatitis in HIV-infected persons has been reported. Herpes simplex infections are mainly intraoral, sometimes extensive and persistent, but rarely disseminate. A minority suffer from herpes zoster and papillomavirus infections. The latter manifest as oral papillomas, warts or condylomata.
Kaposi’s sarcoma
Caused by human herpesvirus 8, this is a multifocal systemic tumour due to proliferating microvascular and fibroblastic processes, seen mostly in sexually transmitted HIV infection.
Hairy leukoplakia
This classically appears as an asymptomatic, greyish-white to white, corrugated lesion on the tongue, either unilaterally or bilaterally (Fig. 30.3). The aetiological agent is the Epstein–Barr virus. (Note: it is also seen in patients belonging to other risk groups, and uncommonly in healthy individuals.) As more than three-quarters of HIV-infected patients with hairy leukoplakia develop AIDS within 3 years, it is considered to indicate a poor prognosis.

Necrotizing (ulcerative) gingivitis and necrotizing (ulcerative) periodontitis
An unusual type of recalcitrant, aggressive periodontal disease has been identified in those who are infected with HIV. The disease begins as a form of gingivitis, which mimics acute ulcerative gingivitis. However, it differs from the latter as the disease progresses unceasingly despite routine management protocols such as metronidazole therapy, debridement and scrupulous oral hygiene. The anterior gingiva is most commonly affected. In some patients, HIV gingivitis has a very destructive course, leading to periodontitis with loss of soft tissue and bone, sequestrum formation and, in extreme cases, tooth exfoliation.
Diagnosis
History and clinical criteria are of the essence in the provisional diagnosis of HIV infection but laboratory investigations, after appropriate professional counselling, are required for confirmation of the disease.
The first step in serodiagnosis is the enzyme-linked immunosorbent assay (ELISA) or agglutination screening tests for serum antibodies. Up to about 2% of the ELISA tests are either false positive or false negative: hence, a positive ELISA must be retested in duplicate samples. If two or more of the latter three ELISA results are positive, confirmatory testing has to be done by a Western blot assay. Thus, the principles and ethics of diagnosis are:
Other laboratory diagnostic methods include:
Management
A number of antimicrobial agents are used in the management of HIV and its related infections. The two main groups of drugs used to suppress HIV proliferation are:

Combination therapy with nucleoside analogues and protease inhibitors is far more effective than monotherapy with individual drugs. However, the side effects and the cost of treatment are both barriers to such ‘cocktail’ therapy. HAART consists of two nucleoside inhibitors and one protease inhibitor. There is significant clinical improvement in HAART therapy, yet the virus persists intracellularly as a provirus, only to re-emerge if or when therapy is abated.
A large number of antimicrobial drugs are also used prophylactically to prevent emergence of fungal, bacterial and viral infections, and as therapeutic supportive measures to prolong the quality of life in these patients.
Prevention of HIV infection
HIV transmission and dental health care workers
The risk to dental professionals
A number of prospective surveillance studies indicate that there is no risk of HIV transmission by either saliva or blood in routine dental care. However, accidental injuries via contaminated needles are associated with a very low risk of infection (0.3%). In view of the thousands of infected patients treated since the advent of the AIDS pandemic, it is highly unlikely that the occupational hazard of dentists contracting HIV infection is greater than that for other health care workers. Additionally, the susceptibility of HIV to many disinfectants, the hygienic environment in most dental surgeries and the use of disposable instruments reduce the risk still further. After close scrutiny of the small number of alleged HIV transmission episodes in dentistry, the US Centers for Disease Control have stated that there has been no such transmission in dental settings thus far.
The HIV-infected dental health care worker
The disclosure of possible HIV transmission to five patients by an infected dentist (in Florida, USA) has raised important ethical, moral and legal issues pertaining to continued delivery of dental care by infected dental personnel. (However, the dental transmission route has now been ruled out as it is believed that the patients acquired the infection from high-risk activities.)
The consensus of professional opinion is that it is the ethical and moral responsibility of dentists who believe that they may be infected with HIV to obtain medical advice and, if found to be infected, to act upon the medical advice, if necessary by modifying the practice of dentistry in some way or by ceasing practice altogether.
Infections in compromised patients
A compromised patient is a person whose normal defence mechanisms are impaired, making the individual more susceptible to infection (e.g. individuals with damaged heart valves, diabetes and immunodeficiency states, including AIDS).
Although the majority of compromised patients are hospitalized, a significant proportion are ambulant community dwellers and likely to seek routine dental care. It is important to note that the drugs and dental treatment provided may interfere with the compromised state and the medications prescribed.
Mechanisms leading to immunocompromised states
Immunodeficiency disease can be either primary (developmental or genetically determined), which is rare, or secondary, due to procedures such as irradiation and cytotoxic drug therapy.
Primary immunodeficiency
Rarely children are born with congenital deficiency of the immune system. These include deficiencies in B cells, with depressed immunoglobulin production, T cell deficiency (e.g. thymic aplasia), combined B cell and T cell deficiency, and neutrophil dysfunction.
Secondary immunodeficiency
Secondary immunodeficiency can be due to disease or therapy (Table 30.4).
Table 30.4 Main causes of secondary immunodeficiency
Disease
Diseases include neoplasms of the lymphoid system leading to lymphomas (Hodgkin’s disease), leukaemia and multiple myeloma, and – of special interest – AIDS due to HIV infection (see above). Other diseases such as diabetes, renal failure, rheumatoid arthritis and autoimmune disease (e.g. systemic lupus erythematosus) diminish immunity by often complex and incompletely understood mechanisms.
Therapy
Modern medical treatment, especially drugs, radiotherapy and surgical removal of the spleen, may diminish or abolish immune function:
Oral infections in compromised patients
Due to the poor immune functionality associated with the specific underlying condition or the management procedure, the oral cavity is perhaps the first site where focal infection may be noted in compromised individuals. Such infections may be caused by endogenous commensal flora of low pathogenicity (e.g. oral candidiasis) or exogenous organisms acquired from the environment (e.g. drug-resistant hospital staphylococci, methicillin-resistant Staphylococcus aureus, coliforms). Both virulent organisms and even the most harmless commensals may cause life-threatening disease (Table 30.5).
Table 30.5 Examples of organisms that cause infection in compromised patients
| Agent | Infection |
|---|---|
| Bacteria | |
| Enterobacteriaceae | Urinary tract infection, pneumonia, septicaemia, meningitis, oral mucositis, osteoradionecrosis |
| Mycobacterium tuberculosis and other mycobacteria | Tuberculosis, disseminated disease, IRIS |
| Staphylococcus aureus | Septicaemia, pneumonia, mucositis, osteoradionecrosis |
| Streptococcus pneumoniae | Septicaemia |
| Fungi | |
| Candida spp. | Thrush, systemic candidiasis, chronic mucocutaneous disease |
| Cryptococcus neoformans | Meningoencephalitis |
| Aspergillus and Mucor spp. | Disseminated disease |
| Viruses | |
| Herpes simplex virus | Severe cold sores |
| Cytomegalovirus | Pneumonia, IRIS |
| Protozoa | |
| Pneumocystis carinii | Interstitial pneumonia (in AIDS) |
| Toxoplasma gondii | Severe toxoplasmosis |
IRIS, immune reconstitution inflammatory syndrome.
Some examples of specific orofacial infections in compromised patients are given below:
Management: antibiotic or antiviral drugs against the infectious organism sometimes with corticosteroids to suppress inflammation.
Important cofactors for oral infection in immunocompromised patients
Clinical presentation
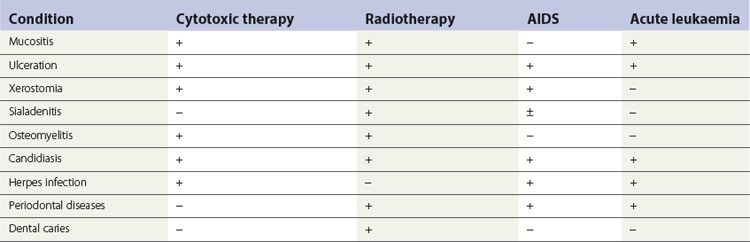
The presentation of oral infections varies widely, depending on the cofactors mentioned above. Some conditions are more commonly associated with a particular category of compromised patient than others. For instance, in acute leukaemia, the response to dental plaque is exaggerated, leading to gross gingival swelling, but periodontal disease is not a significant problem during cytotoxic therapy. Oral problems encountered in immunocompromised patients are listed in Table 30.6.
Prevention of infection
General guidelines
Surveillance
Careful monitoring of the susceptible individual for signs of infection is required; if these occur, treatment should be instituted without delay.
Specific guidelines
Pretreatment management
Pretreatment management includes:
Xerostomia and infection
Xerostomia or dry mouth may be the result of:
The resulting chronic dryness of the mucosa and the inadequate salivary cleansing mechanism increase the susceptibility of oral tissues to incidence of:
Other non-infective sequelae are difficulty in eating and swallowing dry food, and in wearing complete dentures; burning sensation of the oral mucosa; and changes in the sense of taste (dysgeusia).
A reduction or absence of salivary secretion has a profound effect on the composition of the normal oral flora. Reduced moisture levels tend to favour growth of bacteria resistant to drying, such as Staphylococcus aureus, and inhibit oral commensals adapted to high moisture levels. In addition, the pH of salivary secretions in these patients is low and the oxygen tension (Eh) is high, which may be unfavourable to the growth of bacteria such as Veillonella, commensal Neisseria and Micrococcus spp. Moreover, this environment favours the growth of Candida spp.
Sequelae of chronic xerostomia
Extensive dental caries
Dental caries may occur, especially in the cervical and incisal surfaces of the teeth and at the margins of dental restorations, sometimes subgingivally.
Periodontal disease
Periodontal disease, especially gingivitis, is common because of the lack of moisture.
Candidal infections
Candida-associated denture stomatitis, angular cheilitis and papillary atrophy of the tongue are frequent.
Ascending parotitis
Ascending parotitis is the result of the absence or reduced natural flushing action of the salivary flow in Stensen’s duct.
Prevention
Treat with antibiotics: empirical therapy with penicillinase-resistant penicillins. Pus should be sent for culture and antibiotic sensitivities. Stimulate salivary secretion with sialagogues; if adequate amounts of saliva cannot be stimulated, use a proprietary saliva substitute.
Key facts
Davies A.N., Epstein J.B. Oral complications of cancer and its management. Oxford: OUP; 2010.
Dalgleish A.G., Weiss R.A. Human retroviruses. In Zuckerman A.J., Banatvala J.E., Pattison J.R., editors: Principles and practice of clinical virology, 3rd ed., Chichester: John Wiley, 1994. Ch. 24
EC Clearinghouse on Oral Problems Related to HIV Infection and WHO Collaborating Centre on Oral Manifestations of Immunodeficiency Virus. Classification and diagnostic criteria for oral lesions in HIV infection. Journal of Oral Pathology and Medicine. 1993;22:289-291.
Friedman-Kien A.E., Cockerell C.J. Color atlas of AIDS, 2nd ed. Philadelphia: W.B. Saunders; 1996.
Lewis M.A.O., Jordan R.C.K. A colour handbook of oral medicine. London: Manson Publishing; 2004.
Lucht E., Nord C.E. Opportunistic oral infections in patients infected with HIV-1. Reviews in Medical Microbiology. 1996;7:151-163.
Samaranayake L.P. Oral mycoses in human immunodeficiency virus infection: A review. Oral Surgery, Oral Medicine, Oral Pathology. 1992;73:171-180.
Samaranayake L.P., Pindborg J.J. Hairy leukoplakia. British Medical Journal. 1989;298:270-271.
Samaranayake L.P., Scully C. Oral candidosis in HIV infection. Lancet. 1989;ii:1491-1492.
Scully C., Cawson R.A. Medical problems in dentistry, 6th ed. London: Churchill Livingstone; 2010.
Sepkowitz K.A. AIDS – The first twenty years. New England Journal of Medicine. 2001;344:1764-1768.
Tsang C., Samaranayake L.P. Immune reconstitution inflammatory syndrome (IRIS) after highly active antiretroviral therapy: A review. Oral Diseases. 2010;16:248-256.
Review questions (answers on p. 354)
Please indicate which answers are true, and which are false.