5 Treating facet joint generated pain
Facet joints are the posterior articulating joints in the spine. They carry most of the compressive load when the spine is in extension and guide motion during flexion, extension and rotation. High and low threshold mechanoreceptors and mechanically sensitive pain receptor nerves fire as the joint capsule is stretched and the cartilaginous joint surface compressed during joint movement. Proprioceptive nerve endings in the joint capsule fire during normal range of motion of the joint. Abundant free and encapsulated nerve endings and small nerve fibers capable of secreting substance P and calcitonin gene-related peptide (CGRP) enervate the capsule and joint surfaces. During trauma the joint approaches end range extension stretching the joint capsule and compressing the cartilage to the point of injury. Injury and inflammation of the facet joint and surrounding muscles excite and sensitize the nerves at the joint (Cavanaugh 1996). Excessive capsule stretch, seen in whiplash and hyperextension injuries, activates nociceptors in the joint capsule, leads to prolonged neural after-discharges and can cause damage to the capsule and to the axons in the capsule and is a probable cause of persistent neck and back pain. Facet joints have been implicated as a major source of low back and neck pain (Cavanaugh 2006).
Facet joints become painful as the joint tissues degenerate and become inflamed (Beaman 1993). The cartilage surface becomes irregular, frayed and calcified. The periosteum and subchondral bone becomes inflamed and calcified. Nerve fibers infiltrate the inflamed and degenerated tissues and secrete substance P in the eroded areas sending pain signals to the brain via the nerves and spinal cord. The nerves at the facet joint capsule transmit proprioceptive information in normal joints and pain information in inflamed or injured joints. Chen found more c-fiber receptors on the dorsolateral aspect of the facet joint where muscles and tendons were attached (Chen 2006). Inflammation leads to decreased firing thresholds and elevated baseline discharge rates of nerve endings in facet capsules (Cavanaugh 2006). Chronic inflammation leads to fibrosis between the nerves and soft tissues such as the capsule, the muscles and the fascia (Lewis 2004). These adhesions can make even normal motion painful as the nerves are stretched by the movement of the soft tissues to which they are adhered.
The reduced firing threshold, increased baseline neural discharge and perineural fibrosis in the injured and degenerated facet joint tissues feeds constant neural input into the spinal cord which feeds back to the muscles around the joint contributing to the formation of taut bands and myofascial trigger points in the paraspinal and postural muscles (Gerwin 2004). The myofascial trigger points compound the pain (Travell 1983, 1992) and the taut bands complicate joint function when the shortened sensitized muscle fibers contribute to joint compression and sensitized neural input and help perpetuate joint inflammation. This interaction between the nerve, joint and muscle forms a feed-back–feed-forward neuro-mechanical cycle that is very difficult to break once it becomes established and is the reason that chronic low back and neck pain is so pervasive and difficult to treat. To interrupt it effectively, all three aspects of dysfunction should be addressed at once. FSM makes this possible in most cases.
Identifying which pathologies in which tissues are creating the pain becomes important when treating with FSM because the frequency choices are specific to the tissue and pathology. FSM has been shown to decrease COX and LOX mediated inflammation, inflammatory cytokines and CGRP (McMakin 2005, 2007, Phillips 2000). FSM has been shown to decrease scar tissue and to reduce the pain associated with myofascial trigger points (McMakin 1998, 2004, Huckfeldt et al 2003). FSM has frequencies for calcium deposits and calcium influx into soft tissues, for nerve pain and for myofascial trigger points in the involved muscles.
By using adjunctive modalities such as appropriate exercise and stretching, posture re-education, oral or topical anti-inflammatory medications and oral anti-inflammatory nutrients such as fish oils (EPA/DHA) even the most chronic facet joint pain can improve. Complete resolution of acute or chronic facet pain may require more invasive interventions such as steroid and lidocaine injections into the joint under fluoroscopy to “get on top of” the inflammation so the more conservative modalities can be effective. Studies show that facet injections as a sole treatment modality aren’t effective for long term facet joint pain relief but clinical experience has shown that when combined with other therapies such as FSM, appropriate exercise, nutritional supplementation and postural reeducation they can be a very successful adjunct.
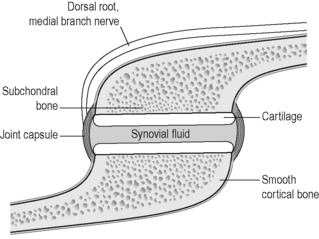
Figure 5.1 • A healthy facet joint has intact cortical bone, periosteum and cancellous bone. The joint capsule and ligaments are not thickened; the cartilage is hydrated and smooth and the synovial fluid is uniformly lubricating.
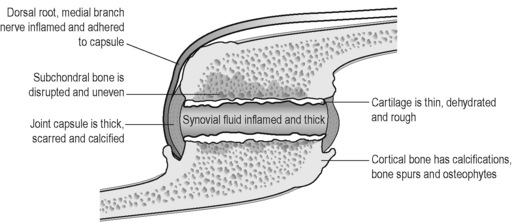
Figure 5.2 • Inflammation and chronic inflammation of the facet joint causes thickening of the joint capsule and ligaments and calcium deposits at the periosteum, the ligaments and the joint capsule. The cartilage is thinned and uneven and the synovial fluid is thick.
Diagnosing facet joint pain
When the patient complains of neck, thoracic or lumbar spine pain, or “backache” the facet joints should be considered and examined for involvement. In general, the pain from the inflamed joint will be at the spine and radiating in a scleratomal pattern into the area just adjacent to the joint. Facet joint referred pain rarely goes below the knee in the lumbar spine and is most commonly seen in the upper back and shoulder in cervical spine facets.
The pain level may be rated from mild, 3–4/10 on a 0 to 10 visual analog scale (VAS) to severe, 7–8/10 VAS depending on the severity of recent injury, previous facet joint damage, degeneration, inflammation and scarring.
The pain will be worse with extension and sitting which compress the posterior joints and better with flexion which gaps the joints and relieves the pressure. The patient will state that they cannot lay prone at all and if laying supine must have the knees and hips flexed at 90 degrees. The pain will be worse with rotary motions that compress the joint on one side and move soft tissues that are adhered to nerves and the joint capsule. Movements that use trigger point laden muscles will create both local and referred pain from the myofascial trigger points. Inflammation in the facet joints can trigger neural pain and create dermatomal nerve pain although this is less common. The same injuries that traumatize and damage the facet joints can also damage the discs and the patient may have pain with flexion or rotation caused by disc inflammation (see Chapter 4).
The saying “The patient is entitled to more than one diagnosis” is especially true of patients with facet generated pain. The patient may have overlapping facet joint, neuropathic, discogenic and myofascial trigger point pain.
History of causation consistent with facet Injury
Any trauma that creates sudden spinal extension or compression can injure a facet joint. The most common traumatic mechanisms are automobile accidents and falls.
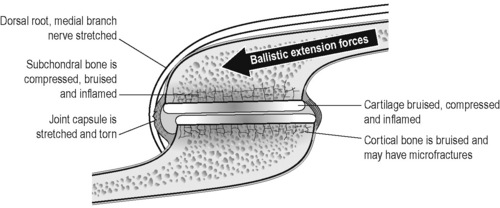
Figure 5.3 • During trauma ballistic extension forces stretch the facet joint capsule beyond its normal limits, compress and bruise the cartilage and subcortical bone, may cause micro-fractures in the cortical bone and traction injuries to the dorsal root medial branch. The damage causes inflammation; post-traumatic fibrosis impairs circulation and often leads to chronic inflammation and progressive joint degeneration. The capsule and ligaments are further stretched during the rebound flexion in a whiplash injury.
Prolonged static posture in extension while sitting or chronic poor muscle balance can lead to chronic segmental joint extension; compressing the facet joint and leading to local joint damage – most commonly seen in the lumbar or cervical spine.
The psoas muscle is the ultimate culprit in most chronic low back facet generated pain. The psoas and iliacus form the iliopsoas and attach to the anterior vertebral bodies and discs of the lumbar spine and the lesser trochanter of the femur. The psoas is a trunk flexor. When the psoas is tight it should pull the trunk into flexion but the posterior lumbar and thoracic paraspinal muscles tighten to keep the torso upright. These opposing mechanical forces compress both the facet joints and the discs but the facet joints seem to take the brunt of the insult.
A similar muscular imbalance exists in the cervical spine with the scalenes as neck flexors and the posterior neck muscles opposing to keep the neck upright. The lower cervical discs and the upper cervical facet joints are compromised in this case. Chronic forward head posture while seated reading or typing at a computer is responsible for muscle pain and fatigue and facet joint compression and degeneration.
Physical examination
Most practitioners reading this text have been trained to perform a physical examination to evaluate spine and facet joint pain. This brief description is meant to be a reminder rather than a comprehensive or definitive instruction. The reader who desires more complete instruction is referred to Hoppenfeld (1976) or Souza (2009) or a similar resource.
This examination procedure may seem incredibly simply but it has been completely foolproof in the authors, experience when combined with a probable history and mechanism of injury. To examine the lumbar and thoracic spine facet joints, lay the patient prone and briefly and gently apply pressure to the suspect facet joints with the thumb placed perpendicular to the spine and parallel to the direction of the facet joint. If the patient says “ouch” then that facet joint is a pain generator. As the joint is compressed and patient reports pain, the paraspinal muscles will usually splint. If the examination is too forceful it will increase the patient’s pain and in the worst case may contribute to further facet joint damage.
To examine the cervical spine facet joints have the patient lay supine or seated and gently and briefly use the finger pads to compress the joints. If the patient is supine gently lift up into the joints with the finger pads following the joint line and feel for the muscle splinting and guarding that accompanies the patient’s report of pain. The joint capsule and surrounding muscles will feel like a tight firm ball just lateral to the midline. If the patient is seated support the head with one hand and gently and briefly use the pads of the fingers to compress the joints. If the patient says “ouch” then that joint is a pain generator. The postural muscles will be activated while the patient is seated and may camouflage the local muscle splinting that occurs when the joint is compressed.
If it is necessary for forensic or medical legal purposes to confirm that the joint identified by the physical examination is indeed a pain generator, the practitioner may order a facet block to be done to the joint in question. Facet blocks should be done, with some pain medication or light sedation, under fluoroscopy by physicians trained and certified by ISIS (International Spinal Injection Society) or some similar body. The block may be done with local anesthetic for diagnosis only but it is more common to do a block that is both diagnostic and therapeutic which combines an anti inflammatory steroid with a local anesthetic. If the block reduces or eliminates the joint pain it confirms that the joint was a pain generator.
Treating chronic facet joint pain

• The patient must be hydrated to benefit from microcurrent treatment.
• Hydrated means 1 to 2 quarts of water consumed in the 2 to 4 hours preceding treatment
• Athletes and patients with more muscle mass seem to need more water than the average patient.
• The elderly tend to be chronically dehydrated and may need to hydrate for several days prior to treatment in addition to the water consumed on the day of treatment
• DO NOT accept the statement, “I drink lots of water”
• ASK “How much water, and in what form, did you drink today before you came in?”
• Coffee, caffeinated tea, carbonated cola beverages do not count as water.
Channel A: condition frequencies
The frequencies listed alphabetically are thought to remove or neutralize the condition for which they are listed except for 81, 49 / which are thought to increase secretions and vitality respectively
| 91 / | |
| 284 / | |
| 18 / | |
| 40 / | |
| 13 / | |
| 3 / | |
| 81 / | |
| 49 / |
3 Channel B: facet joint tissue frequencies
 Both frequencies are used when treating bone. It is presumed that one frequency is for cortical bone and one is for cancellous bone but it is not known what portion is addressed by which frequency. The periosteum lines the outside of the bone, interweaves with tendinous and ligamentous attachments and is very well innervated and pain sensitive. Cartilage lines the facet joint and becomes damaged, degenerated, calcified and inflamed when traumatized by acute or chronic compression of the joint surface. The joint capsule attaches to the periosteum, surrounds the joint and becomes fibrosed, calcified, scarred and inflamed when over stretched by trauma. The recurrent nerves innervating the joint capsule transmit proprioceptive information in the normal facet joint and pain information in the degenerated joint. They infiltrate the joint in response to chronic inflammation becoming fibrosed and scarred to the capsule and fascia as degeneration progresses. Dermatomal nerve roots may become painful as inflammatory peptides diffuse out from the inflamed facet joint tissues.
Both frequencies are used when treating bone. It is presumed that one frequency is for cortical bone and one is for cancellous bone but it is not known what portion is addressed by which frequency. The periosteum lines the outside of the bone, interweaves with tendinous and ligamentous attachments and is very well innervated and pain sensitive. Cartilage lines the facet joint and becomes damaged, degenerated, calcified and inflamed when traumatized by acute or chronic compression of the joint surface. The joint capsule attaches to the periosteum, surrounds the joint and becomes fibrosed, calcified, scarred and inflamed when over stretched by trauma. The recurrent nerves innervating the joint capsule transmit proprioceptive information in the normal facet joint and pain information in the degenerated joint. They infiltrate the joint in response to chronic inflammation becoming fibrosed and scarred to the capsule and fascia as degeneration progresses. Dermatomal nerve roots may become painful as inflammatory peptides diffuse out from the inflamed facet joint tissues.A/B pairs for scar tissue
These frequencies were discovered in a list of frequencies published by Albert Abram’s in Electromedical Digest in 1931. 58 / 00 was the frequency combination to remove “abnormal cellular stroma”, whatever that might have been. 58 / 01 was used for scar in bony tissue. 58 / 02 was used for scar in soft tissue and 58 / 32 was used for scar tissue adhesions.
In treating chronic complaints the 58/’s are used in order as listed above for approximately 1 to 2 minutes each at the beginning of the treatment to soften the tissues. If there is no bone involved in the complaint it is customary to leave out 58 / 01. For those practitioners who can feel the softening produced by the frequency, it is often helpful to run the frequency until the softening is reduced and the tissue becomes relatively more firm. There may be some patients in whom one or more of these frequencies will produce softening for up to 3 to 4 minutes.
The 58/’s will increase range of motion but do not change pain.

Caution: 58 / 00, 01, 02, 32
• Do not use these frequencies on injuries newer than 5 to 6 weeks old.
• Newly injured tissue must form scar tissue in order to repair itself.
• Removing the scar tissue seems to undo the healing by weeks in a new injury.
• The 58/’s can be used very briefly (15 seconds) to modify scar tissue as it is forming after the first four weeks.
• Never use this combination before the injury is 4 weeks old
This precaution is the result of trial and uncomfortable error. A patient was being treated for facet and soft tissue injuries caused by an auto accident that had occurred 3 weeks previously. She was pain free after four treatments in 21 days and was treated on a Tuesday. She returned on Thursday complaining that whatever had been done on Tuesday had “undone” 2 weeks of healing and she felt as much pain as she had 2 weeks previously. Review of the Tuesday treatment revealed that the 58/’s had been used in addition to the protocols that had been reducing the pain for the preceding 3 weeks. She was so pain free that it seemed as if the injury was much older and the date of injury was not checked before treatment. The presumption was made that the 58/’s had removed repair tissue necessary to keep the joint and soft tissues pain free and stable. Two more errors in the first year of treating with FSM in similar situations helped to determine that the 58/’s should not be used within five to six weeks of a new injury. They can be used briefly four weeks after the date of injury – for 5 to 10 seconds each – to thin out scar tissue as it is forming, especially in athletes who seem to heal faster.
This reaction is predictable and reproducible. Take this precaution seriously. The wise practitioner will only make this mistake once; it is better not to make it at all.
Treatment protocol chronic facet pain
Channel A condition / Channel B tissue
58 / 00, 01, 02, 32
• A/B pair for Removing scar tissue and adhesions
• Treatment time: When used to treat chronic complaints the 58/’s are used in order as listed above for approximately 1 to 2 minutes each at the beginning of the treatment to soften the tissues and remove scar tissue. Facet joints have bone as a tissue so 58 / 01 is usually included in the protocol. For those practitioners who can feel the softening produced by the frequency, it is often helpful to run the frequency until the softening is reduced and the tissue becomes relatively more firm. There may be some patients in whom one or more of these frequencies will produce softening for up to 3 to 4 minutes.
40 / 396, 59, 39, 783, 157, 480, 191, 100
• Inflammation / Nerve, bone, periosteum, cartilage, capsule, tendon, ligament.
• Treatment time: Use these combinations for 2 to 4 minutes each. Research has shown 40Hz to have a time dependent response in a mouse model of inflammation. 50% of the reduction in inflammation was present at 2 minutes. The full response was present at 4 minutes. Treat the nerve first as it seems to relax the muscles and allow better palpation of the facet tissues. The periosteum is the most pain sensitive part of the bone and the nerve and the joint capsule are the most sensitive to inflammation and should respond best to this frequency. This protocol should reduce the joint pain but will not change range of motion.
91, 13 / 142, 396, 480, 783, 157, 191
• Calcium ions, scar tissue / fascia, nerve, joint capsule, periosteum, cartilage, and tendons.
• 91 / 783, 480, 157, 396 seems to reduce joint pain most effectively and softens the joint capsule dramatically.
• 13 / 142, 396, 480 usually increase range of motion most effectively. Scarring between the capsule and the nerve appear to create sharp pain with palpation and respond well to treatment. See manual technique below.
• Treat all the tissues if time allows.
• Treatment time: Use these combinations for 1 to 2 minutes each or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens.
If response is slow: narcotics
Experience has shown that patients who are on high levels of narcotics or who have had multiple injections with anesthetics respond slowly to treatment. This effect is reversed by the frequencies to “remove” narcotics and anesthetics. It is not thought that these frequencies actually remove the narcotic or anesthetic since they do not increase pain. It is much more likely that they somehow influence the membrane in such a way as to make it more receptive to treatment.
Use 43, 46, 19 / 396 first if the patient is on narcotics. The current application and lead placement are the same as for the joint treatment.
If there is dense scar tissue or bony stenosis of the nerve root or spinal cord or if a disc fragment is compressing the nerve root or cord at the involved level the patient’s pain may increase when polarized positive current is applied. If the patient is positioned comfortably, it is the only time the pain will increase during polarized positive treatment for nerve inflammation. It may increase in the dermatome or at the spine or both. Assess patient position to determine whether it is contributing to the pain increase.
Stop treating immediately if pain goes up during treatment. Move the patient to a seated position if possible. Move the contacts slightly up the spine superior to the nerve root being treated, reduce current levels and change the current from polarized positive to alternating. If this is going to reduce the reaction it will do so in 5 to 10 minutes. If the pain continues to increase, stop treating with current. The pain should go back down in a few hours although it may take up to 24 hours to reduce to base line.
This reaction is diagnostic. If physical examination findings of reduced sensation and deep tendon reflexes at the involved level or hyperactive deep tendon reflexes below the involved level are present this reaction suggests the need to x-ray or perform an MRI to confirm the presence of compression.
Treat the muscles
When treating the facet joint remember to treat the muscles and trigger points. The taut muscles act as confounding pain generators and at the same time compress the facet joint increasing the degenerative forces on both the facet joint and the disc (see Chapter 7).
Treat the psoas and lumbar paraspinals muscles in the low back.
Treat the scalenes and the cervical paraspinals in the neck.
Treat the thoracic paraspinals and the rectus abdominus in the trunk.
See the chapter on treating muscles and myofascial pain for details.
Treatment application
• Current level: 100–300μamps. Use lower current levels for very small or debilitated patients. Use higher current levels for larger or very muscular patients. In general higher current levels reduce pain more quickly. Do not use more than 500μamps as animal studies suggest that current levels above 500μamps reduce ATP formation while current levels below 500μamps increase ATP.
• ± Polarization or Polarized Positive +: Current is used in alternating mode. Alternating DC current is actually pulsed DC (direct) current that alternates its polarity from positive to negative. Some patients respond better to polarized positive current for reasons that are not understood. It is best to try both on each patient at each session.
• Waveslope: Moderate to sharp for chronic facet pain. Use a gentle wave slope for acute facet pain.
The waveslope refers to the rate of increase of current flow on the leading edge of the square wave. A sharp waveslope has a very steep current up ramp; a gentle waveslope has a gradual current up ramp.• Contact placement for spinal facet joints
FSM typically uses graphite gloves to conduct the current. The graphite gloves need to be kept moist so they conduct the current comfortably. The graphite gloves can be placed in or leads attached with alligator clips can be attached to a small warm wet towel or fabric sleeve. Care should be taken to see that the wet fabric contacts do not touch each other. Current will follow the path of least resistance and the wet contacts are presumed to be less resistant than the patient therefore the current will flow in the wet contacts and avoid the tissue that needs treating.• Wrap the positive leads contact around the spine or lay the contact over the spine to treat the facet joints.
• Wrap the negative leads around the adjacent limb at the end of the referred pain area if myofascial trigger points are being treated at the same time.
• The positive leads graphite glove can be placed directly on the skin under the spinal area to be treated after being wet thoroughly with water.
• The negative leads graphite glove can be placed directly on the skin on the body surface anterior to the spinal area to be treated after being wet thoroughly with water.

Figure 5.4 • To treat the cervical facet joints, place the positive leads glove in a warm wet fabric contact (hand towel) at the posterior cervical spine. Place the negative leads glove in a warm wet fabric contact (face cloth) at the anterior cervical spine or on the upper chest. Place the hands under the towels to palpate the tissue changes, mobilize the joints and work the muscles paying close attention to the periosteum at the joint line and the capsule over the joint while running 91 / 783, 480.


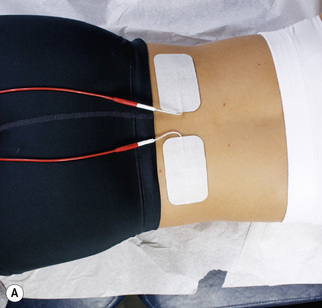
Figure 5.5 • To treat the thoracic facet joints wrap the positive leads glove in a warm wet fabric contact (hand towel) or attach the leads to the contact with alligator clips and place it lengthwise down the posterior spine with the patient supine with knee bent and back flat. Wrap the negative leads glove in a warm wet fabric contact (hand towel) and place it lengthwise down the trunk so the current flows through the tissue in three dimensions. The practitioner’s hands can be placed under the contacts to work the soft tissues and mobilize the joints.
• Adhesive Electrode Pads may be used for convenience although the gloves seem to be more effective for reasons not understood. The adhesive electrode pads are especially useful for home treatment because they allow the patient to be active while being treated.
When applying treatment with adhesive electrode pads, the current and the frequencies must pass through the area to be treated in an interferential pattern, forming an “X” in three dimensions. The positive electrodes are placed at the spine at the level of the facet to be treated. The negative electrodes may be placed directly anterior or anterior and slightly inferior to the spinal contacts for the facet being treated.
A diagram for the placement would look like this:
Figure 5.6 • Place the positive leads contact under the spine with the patient positioned supine with knees bent and back flat. Place the negative leads contact on the abdomen. Place the hands under the towels to palpate the tissue changes, mobilize the joints and work the muscles, especially the psoas and quadratus lumborum and lumbar paraspinals.

Figure 5.7 • Place the positive leads glove or attach the negative leads by alligator clips to the warm wet cloth contact (hand towel) and place it behind the neck with the patient supine. Place the negative leads glove or attach the negative leads by alligator clips to a warm wet towel draped across the scapula, under the axilla and wrapped around the upper arm to treat the facet joints and the nerves and muscles of the neck, upper back, and shoulder. Use the hands under the towels to palpate the changes, work the muscles, and mobilize the facet joints.
| Positive Electrode Channel A | Positive Electrode Channel B |
| Area to be Treated | |
| Negative Electrode Channel B | Negative Electrode Channel A |

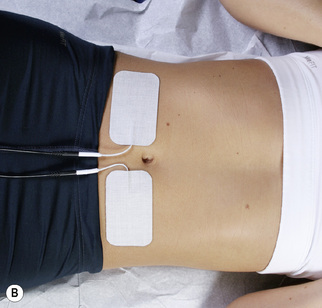
Figure 5.8 • Place the positive leads glove or attach the negative leads by alligator clips to the warm wet cloth contact (hand towel) and place it under the low back with the patient supine. Place the negative leads glove or attach the negative leads by alligator clips to a warm wet towel draped across the abdomen and upper thigh to treat the facet joints and the nerves and muscles of the low back, hip and thigh. Use the hands under the towels to palpate the changes, work the muscles, and mobilize the facet joints.

Figure 5.9 • To treat the thoracic facet joints, nerves and muscles with the patient prone wrap the positive leads glove in a warm wet fabric contact (hand towel) or attach the leads to the contact using alligator clips and place it lengthwise down the posterior spine. Wrap the negative leads glove in a warm wet fabric contact (hand towel) or attach the negative leads to the contact using alligator clips and place it lengthwise down the trunk under the prone patient so the current flows through the tissue in three dimensions. The practitioner’s hands can be placed under the contacts to palpate the changes, work the soft tissues and mobilize the joints.
Facet joint pain with no referral
• Place the positive electrode from channel A on the skin just lateral to the spinal segment at the level of the facet joint.
• Place the negative electrode from channel A so the current flows down an imaginary line diagonally through the body from the channel A positive electrode to the abdomen just anterior to the involved facet joint.

Figure 5.10 • The graphite glove can be placed directly on the skin after being wet thoroughly by spraying with water. The glove must be wet or the current will sting and prickle. There is not enough current to create a burn but it can be very uncomfortable.

Figure 5.11 • The graphite glove can be placed directly on the skin if that is most convenient. Once the glove is moistened with water it usually stays moist for the duration of the treatment. The galvanic skin response to current flow usually creates slight sweating under the contact. This placement is for cervical facet joint pain. Place the positive leads contact at the back of the neck and the negative leads contact on the chest or on the front of the neck. This placement puts the contacts in the correct position for polarizing the current should that become necessary.
• For example, to treat a lumbar facet, place the positive lead from channel A on the right side of the low back. Place the negative leads from channel A on the left side of the abdomen at or below the level of the facet being treated.

Figure 5.12 • The graphite glove can be placed directly on the skin if that is most convenient. Once the glove is moistened with water it usually stays moist for the duration of the treatment. The galvanic skin response to current flow usually creates slight sweating under the contact. This placement is for lumbar facet joint pain. Place the positive leads contact at the low back and the negative leads contact on the abdomen. This placement puts the contacts in the correct position for polarizing the current should that become necessary.
• Place the positive lead from Channel B on the left side of the low back and the negative leads from channel B on the right side of the abdomen.
Patient position
Patient supine
• In the lumbar spine, the knees and hips should be bent so that the low back is flat. This is the comfort position for the lumbar facet joints unless the patient has accompanying disc pain generators. If there is accompanying discogenic pain find whatever neutral comfortable position is possible. The patient may be treated side lying.
• In the cervical spine, the chin should be tucked so the neck is flat. This is the comfort position for cervical spine facets.
• If a patient continually moves the neck while lying supine they may have both facet and disc pain generators. The most common pattern seen after whiplash injuries is a C5–6 or C6–7 disc injury combined with an upper cervical facet joint injury usually at C2–3. The disc injury produces neck and shoulder pain and the C2–3 facet joint injury produces a headache and peri-orbital pain. As the patient flattens the cervical curve to relieve the upper facets the disc annulus compresses and the patient begins to experience discogenic midscapular pain and neck and shoulder pain. The patient will arch the neck to relieve the disc pain until the facet compression in the upper cervical spine becomes intolerable. This is more pronounced while the patient is supine but can be seen while they are seated as well. Placing a small one inch diameter roll under the C5–6 disc area to keep it in extension will allow the patient to flex and flatten the upper cervical spine and relieve the facet joint compression.

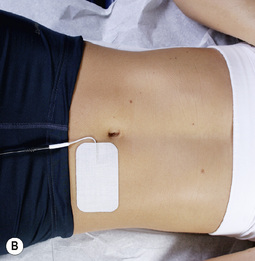
Figure 5.13 • To treat lumbar facet joint pain with adhesive electrode pads place the positive lead from channel A on the right side of the low back. Place the negative lead from channel A on the left side of the abdomen at or below the same level as the facet joint being treated. Then place the positive lead from channel B on the left side of the low back and the negative leads from channel B on the right side of the abdomen.
Patient prone
If the facet patient must lay prone for treatment access to the posterior lumbar or cervical muscles place a pillow or bolster under the abdomen to create lumbar flexion. Tip the head rest or face rest down to create cervical flexion. Do not treat a cervical facet patient prone with the head turned to the side. It is not possible to treat a patient successfully to reduce pain while their position increases pain.

Figure 5.15 • Place the positive leads from channel A on the right side of the neck and the negative lead from channel A on the left upper chest just below the clavicle. Place the positive leads from channel B on the left side of the neck and the negative leads from channel B on the right upper chest just below the clavicle. The current and frequencies form an interferential pattern, crossing in three dimensions through the area to be treated.
• Treatment interval: Facet joint patients can and should be treated twice a week for 4 to 6 weeks with at least one day separating the treatments.
• Manual technique: For those trained in manual therapies using the hands while using FSM requires some adjustment of technique. The key is to let the frequency do the work and to use the hands with very gentle pressure and complete relaxation. The hands should be almost limp with just enough tone in the distal finger muscles to allow the fingers to gently assess the state of the tissue. The therapist should use the shoulder muscles and serratus anterior to advance the arm and increase the pressure of the hand on the tissue being treated. The hands are sensing change and softening in the muscles not forcing it. The patient’s muscles will relax and allow deeper palpation if the practitioner’s hands are relaxed and will defensively tense if the contact is too firm or if the palpating fingers are too tense.
• When using 91, 13 / 480, 396 on the cervical spine place the pads of the fingers under the joint line and gently lift the facet joint on one side of the spine about 2mm. Release this side back to neutral and gently lift the joint on the other side about 2mm. This creates a small amount of segmental rotation at the joint capsule. The nerve becomes adhered to the inflamed and hardened joint capsule and the goal is to gently tease the nerve off of the capsule to allow increased range of motion. The manual technique here is unlike anything most physical medicine practitioners do. It is a gentle slow segmental rocking movement intended to move the joint through its range while allowing the frequency to release the scar tissue and hardening. It is best experienced by relaxing the fingers and using them to sense and follow the frequency effect.
• Let the frequency do the work. If possible, move the fingers to the tissue being treated when the frequency for that tissue is running. When the frequencies are softening scar tissue or mineral deposits use gentle but firm finger pressure to assist the process.
What tissue is it? What is wrong with it?
As proficiency with FSM increases the practitioner using a manual microcurrent device can become more specific with the choice of frequencies for tissues to be treated and pathologies to be removed from them. This process usually occurs gradually as the skilled practitioner becomes more familiar with palpating the local anatomy and more sensitive to the effects of the frequencies on the structures being treated.
With an illustrated anatomy text such as Netter’s Atlas of Illustrated Anatomy (Netter 1991) as a visual guide, palpation can become very specific as to tissue. Following the recommended “relaxed hand” palpation technique allows the sensing fingers to become quite sensitive. When the finger tips encounter a painful tissue it can be identified by the tension in the muscles surrounding the area, by the patient’s verbal response or by the subtle sense that the tissue is simply “different” from the less painful tissue in the area. If the practitioner will attend to the subtle awareness that the tissue is simply “different” this distinction alone is sufficient to create a very skilled palpation sense. This level of skill is within the grasp of every practitioner given time, motivation, practice and patience.
When palpation identifies a taut or tender area the practitioner can pause and ask internally, “What tissue is it?” Make a guess as to what tissue it is-based on the texture and the visual landmarks provided by the illustrated anatomy text. Then ask internally, “What is wrong with this tissue?” For example, the fingers may palpate what feels like the surface of the periosteum where a tendon attaches that feels as if it is both inflamed and calcified.
This awareness actually forms a hypothesis. Test the hypothesis by treating with 40, 91 / 783, 191 (remove inflammation and calcified hardening from the periosteum and tendon). If the tissue softens and the local palpatory pain is reduced, then the hypothesis was very likely correct. If nothing changes then reconsider the anatomy and/or the pathology.
Perhaps the problem tissue is indeed the periosteum and the tendon but perhaps they are scarred down, tethering and stretching the nerve fibers rather than being inflamed and calcified. This assessment forms a new hypothesis which can be tested by running the frequencies 13, 3 / 783, 191, 396 (remove scar and sclerosis from the periosteum, tendon and the nerve).
Repeat this process as needed to complete the treatment and achieve maximum improvement in the tissue. This process may be overwhelming to the novice FSM practitioner because there are so many new tasks and details to master but it actually simplifies and optimizes treatment as soon as it can be accomplished.
Adjunctive instructions for the facet pain patient
The patient should be instructed to avoid activities or movements that create spinal extension such as improper sitting postures or leaning backwards. Sitting posture that protects the cervical spine facet joints involves lumbar extension and erect spinal posture to bring the head and ears directly over the shoulders. Forward head posture causes strain on the neck muscles and the discs and increases compressive load on the facet joints.
The patient should consult with a therapist who can instruct them in proper posture and exercises to strengthen the core abdominal muscles and the muscles around the facet joints and to mobilize the joints in a pain free range to increase circulation and facilitate tissue repair.
Chiropractors, osteopaths and physical therapists should avoid lumbar side posture or rotary adjustments which by their nature gap one joint and jam the joint on the opposite side unless the facet pain is strictly one sided. It is possible to adjust bilateral facets by positioning the patient supine on a drop table and performing a gentle drop table adjustment with a light thrust from the front. The same adjustment can be performed as a mobilization with the patient flexed to 90 degrees at the hips and knees.
Nutritional support
Professional grade nutritional supplements can be helpful in reducing inflammation and relaxing muscles. Essential fatty acids (EPA/DHA) reduce inflammation. Magnesium malate and magnesium glycinate are well absorbed and help relax muscle tissue. Glucosamine and chondroitin sulfate and MSM (methylsulfonylmethane) are said to be effective in reducing pain in degenerative joints. SAMe (s-adenosyl methionine) is becoming more widely used for reducing joint inflammation and pain. A complete listing of nutritional adjunctive therapies is beyond the scope of this text but the reader is encouraged to become knowledgeable in this area and to customize treatment to the patient’s needs.
Narcotics
If patients are on high levels of narcotics or have had multiple injections with anesthetics it is sometimes necessary to run the frequencies to “remove” narcotics and anesthetics. It is not thought that these frequencies actually remove the narcotic or anesthetic. It is much more likely that they somehow influence the membrane in such a way as to make it more receptive to treatment.
Treating acute facet joint pain
• The patient must be hydrated to benefit from microcurrent treatment.
• Hydrated means 1 to 2 quarts of water consumed in the 2 to 4 hours preceding treatment
• Athletes and patients with more muscle mass seem to need more water than the average patient.
• The elderly tend to be chronically dehydrated and may need to hydrate for several days prior to treatment in addition to the water consumed on the day of treatment
• DO NOT accept the statement, “I drink lots of water”
• ASK “How much water, and in what form, did you drink today before you came in?”
• Coffee, caffeinated tea, carbonated cola beverages do not count as water.
Channel A: condition frequencies
The frequencies listed are thought to remove or neutralize the condition for which they are listed except for 81, 49 / which are thought to increase secretions and vitality respectively
| 18 / | |
| 124 / | |
| 40 / | |
| 81 / | |
| 49 / | |
| 294 / | |
| 321 / | |
| 9 / |
Channel B: facet joint tissue frequencies
It is presumed that one is for cortical bone and one is for cancellous bone but it is not known which is for what tissue. When treating bone both frequencies are used. The periosteum lines the bone and is very pain sensitive. Tendons, ligaments and the joint capsule attach to the periosteum by interweaving with the fibers that cover it. Cartilage lines the facet joint and becomes damaged, degenerated, calcified and inflamed when traumatized by acute or chronic compression of the joint surface. The joint capsule surrounds the joint and becomes scarred and inflamed when over stretched by trauma. This refers to the dermatomal nerves that may be irritated by the facet joint inflammation and the recurrent nerves that innervate the joint capsule and infiltrate the joint in response to chronic inflammation. The fascia is the thin connective tissue covering surrounding the muscles and virtually all visceral tissue.• Artery and Elastic Tissue in the Muscle Belly: __/ 62
62Hz is the frequency used for the artery and the elastic tissue in the arterial walls. The muscle belly responds to this frequency either because it is full of small arteries or because the elastic tissue in the muscle belly is somehow related to the artery wall. Animal research in mice demonstrated a 62% reduction in swelling as a measure of LOX mediated inflammation when the frequency 40 / 116 (reduce inflammation in the immune system) was used. This was a 4-minute time-dependent response with half the effect being present at 2 minutes and the full effect present at 4 minutes.Treatment protocol acute facet pain
Use in the first week following an injury to the facet joint
When a patient presents within 12 hours of a fall, auto accident or any trauma in which the joint has been hyperextended pain can be much reduced and recovery much accelerated by using FSM for the acute injury. The channel A condition frequencies are different than for the chronic conditions. It is important to remember that the body needs fibrosis to repair the newly injured tissue and no frequency thought to remove fibrosis should be used in the 6 weeks following the injury.
The 4-hour window
If a patient can be treated within 4 hours of the time of a new injury, as long as the tissue is intact, the healing is tremendously accelerated. Every effort should be made to encourage patients to be treated within this critical time period.
18 / 62
• 18Hz has been used clinically to stop bleeding post-operatively, in the menses and to prevent bruising. 62Hz is the frequency for the arteries. Use this only in the first 48 hours after an injury.
• Treatment time: Use for 4 to 10 minutes or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens.
124 / 59, 39, 783, 157, 480, 191, 62, 100
• Something torn or broken / bone, periosteum, cartilage, capsule, tendon, artery or muscle belly, ligament.
• 124Hz is thought to remove the “fact of being torn or broken” from the injured tissue. This is a conceptual shift to the medically trained mind. In an energetic model, conditions have a physical consequence in the tissue – the periosteum or joint capsule is “torn or broken” – and at the same time there is also an energetic or vibrational pattern that impresses itself on the semiconductor field that is the injured tissue. It is as if the pattern of being “torn or broken” has impressed itself on the field representing the tissue, interferes with the normal healing processes and prevents tissue repair. In an energetic model it is thought that removing this pattern of being “torn or broken” enables the normal repair processes to become effective. This frequency rarely if ever changes symptoms but it seems to enhance tissue repair of “torn or broken” tissues.
• Treatment time: Use for 1 minute with each tissue or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens. Use this frequency only on the first two to three treatments.
294, 321, 9, 49 / 480, 157, 783
• Trauma, Paralysis, Allergy Reaction, vitality / joint capsule, cartilage, periosteum.
• These four frequencies – the basics – do not tend to change symptoms but they appear to be important in restoring normal function to injured tissue. If you think of a time when you have suffered a physical injury you may notice that it is possible to distinguish between the symptoms from the injury and the effect of the “fact” of the trauma, the shock of it to your system. 294 / is thought to address the “fact of the trauma” or the shock to the system created by the trauma.
• When a tissue is traumatized it sometimes behaves as if it has “lost” a line of instructions not unlike a computer when it freezes for the same reason. 321 / is thought to “reboot” the tissue and is described as being used to neutralize “paralysis” moving it past the lost instruction and on to the next step to facilitate return to function.
• When any tissue is traumatized the first response is the secretion of histamine to initiate the inflammatory response. When treating to arrest the immediate effects of a new injury removing the histamine from the injured area seems to stop the inflammatory progression.
• Any tissue that has been traumatized returns to full function more efficiently if “vitality”, 49Hz, is restored. These frequencies don’t necessarily change symptoms but they seem to help speed recovery.
• Treatment time: Use for 1 to 2 minutes or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens. Use these frequencies only on the first two to three treatments. In the interests of time only three tissues have been included. If time allows and there is information that suggests a particular tissue has been particularly traumatized any tissue may be added to the channel B sequence.
40 / 59, 39, 783, 396, 157, 480, 191 142, 62, 100
• Inflammation / bone, periosteum, nerve, cartilage, capsule, tendon, fascia, artery, muscle belly, ligament.
• Treatment time: Use these combinations for 2 to 4 minutes each. The key to reducing acute facet joint pain is to reduce inflammation as rapidly and dramatically as possible. Research has shown 40Hz to have a consistent positive effect in reducing inflammation in both humans and animals. Animal research showed a 4-minute time-dependent response but human research showed up to 90 minutes was required to reduce cytokines when treating the spinal cord (see Chapters 1 & 8). If the practitioner is sensitive to the sensation of softening and time allows, use 40Hz for as long as the tissue is softening.
A/B Pair
40 / 116
• Reduce inflammation in any tissue.
• Animal research in mice demonstrated a 62% reduction in swelling as a measure of LOX mediated inflammation when the frequency 40 / 116 (reduce inflammation in the immune system) was used. This was a 4-minute time-dependent response with half the effect being present at 2 minutes and the full effect present at 4 minutes. 40 / 116 reduced inflammation generally regardless of the tissue that had been inflamed by the chemical agents. It is used here to reduce any inflammation not addressed by 40 / and the tissues.
81, 49 / 142
• 81Hz is used for increasing secretions. / 142Hz is used for the fascia. The fascia secretes the ground substance necessary for repair of the fascia, ligaments and tendons.
• Treatment time: Use for 1–2 minutes or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens.
Treatment application
• Contact Placement and Treatment Application are the same as for Chronic Facet Joint treatment except for the waveslope.
• Use a gentle waveslope for acute injury treatment. All other microcurrent and treatment parameters are the same.
• Patient Position: Use the recommended facet treatment positioning or any position that is comfortable for the injured patient.
• Manual Technique: The manual technique in acute facet joint injuries requires an even softer touch. Use very light contact and minimal pressure because the newly injured tissues are acutely inflamed. The patient can be treated with no manual contact at all for the first one or two treatments.
Treating facet joint pain week 1 to week 5 after injury
The conditions affecting the tissues in week one to week five after a facet joint injury are different than those used acutely and different than those used in week six and in chronic facet joint injuries.
• The patient must be hydrated to benefit from microcurrent treatment.
• Hydrated means 1 to 2 quarts of water consumed in the 2 to 4 hours preceding treatment
• Athletes and patients with more muscle mass seem to need more water than the average patient.
• The elderly tend to be chronically dehydrated and may need to hydrate for several days prior to treatment in addition to the water consumed on the day of treatment
• DO NOT accept the statement, “I drink lots of water”
• ASK “How much water, and in what form, did you drink today before you came in?”
• Coffee, caffeinated tea, carbonated cola beverages do not count as water.
Channel A: condition frequencies
The frequencies listed are thought to remove or neutralize the condition for which they are listed except for 81, 49 / which are thought to increase secretions and vitality respectively
| 40 / | |
| 91/ | |
| 284 / | |
| 81 / | |
| 49 / |
Channel B: facet joint tissue frequencies
Cartilage lines the facet joint and becomes damaged, degenerated, calcified and inflamed when traumatized by acute or chronic compression of the joint surface. The joint capsule surrounds the joint and becomes scarred and inflamed when over stretched by trauma. This refers to the dermatomal nerves that may be irritated by the facet joint inflammation and the recurrent nerves that innervate the joint capsule and infiltrate the joint in response to chronic inflammation. The fascia is the thin connective tissue covering surrounding the muscles and virtually all visceral tissue.Treatment protocol for facet joint pain week 1 to week 5 after injury
When a patient presents within the first to the sixth week after a fall, auto accident or any trauma in which the joint has been hyperextended, pain can be much reduced and recovery much accelerated by using FSM for the subacute injury. The channel A condition frequencies are different than for the chronic or acute conditions. It is important to remember that the body needs fibrosis to repair the newly injured tissue and no frequency thought to remove fibrosis should be used in the six weeks immediately following an injury.
40 / 59, 39, 783, 396, 157, 480, 191 142, 62, 100
• Inflammation, / bone, periosteum, nerve, cartilage, capsule, tendon, fascia, artery, muscle belly, ligament.
• Treatment time: Use these combinations for 2 to 4 minutes each. 40Hz is used for reducing inflammation. Research has shown 40Hz to have a time-dependent response in a mouse model of inflammation. 50% of the reduction in inflammation was present at 2 minutes. The full response was present at 4 minutes.
284 / 59, 39, 783, 396, 157, 480, 191 142, 62, 100
• Chronic inflammation / bone, periosteum, nerve, cartilage, capsule, tendon, fascia, artery, muscle belly, ligament.
• 284Hz was called “deep old bruise” in Dr. Van Gelder’s original list. It has been known to reduce or eliminate bruising in a very short period of time. “Chronic inflammation” is a more accurate description of the condition alleviated by this frequency. Inflammation and chronic inflammation can coexist. Chronic inflammation is present within 48 hours of the onset of acute inflammation.
91 / 142, 480, 783, 157
• Calcium ions and hardening / fascia, joint capsule, periosteum, and cartilage.
• Within 2 weeks of a new injury, especially if it is an acute exacerbation of the chronic injury 91/ seems to reduce joint pain and soften the tissues very effectively. It is a safe transition between the subacute and chronic treatments that can be used from the second week up through the chronic treatment phase.
81, 49 / 142
• 81Hz is used for increasing secretions. /142Hz is used for the fascia. The fascia secretes the ground substance necessary for repair of the fascia, ligaments and tendons.
• Treatment time: Use for 1–2 minutes or if you are sensitive to the feel of tissue softening and time allows, use the frequency as long as the softening happens.
NOTE: In acute exacerbations of a chronic facet problem do NOT use the 58/’s or 13/ or any frequency to remove or soften scar tissue. Scar tissue is needed to repair the recent injury. The 58/’s may be used after the injury is 6 weeks old to soften the repair tissue and make the joint and soft tissues more flexible and help prevent future re-injury.
Treatment application
• Contact Placement and Treatment Application are the same as for Chronic Facet Joint treatment except for the waveslope.
• Use a gentle waveslope for acute injury treatment. All other microcurrent and treatment parameters are the same.
• Patient Position: Use the recommended facet treatment positioning or any position that is comfortable for the injured patient.
• Manual Technique: The manual technique in facet joint injuries from the second week through the six week allows more soft tissue mobilization than the acute phase but a little less than the chronic condition. The myofascial tissues may be addressed as discussed in the chronic facet patient.
Chronic facet joint patient case report
The patient was a 47-year-old man who worked as a security driver for an armored car company. His job included driving and lifting boxes that weighed up to 40 pounds. When he arrived at the clinic he was scheduled for disc surgery in 4 weeks. The surgeon had proposed doing a three level disc replacement and fusion and told the patient that he would be back to work in 6 weeks. His symptoms were 8 years chronic low back pain and leg pain only down to the knee. He could not lay prone; extension and sitting made his pain worse. His sensory examination was normal.
He had had physical therapy, massage and chiropractic treatments. He rated his pain as varying from a 5–7/10 on a 0–10 VAS. He was treated in the clinic 5 days a week with FSM, supine manipulation on a drop table specific for facet joint mobilization. He was pain free at the end of each visit and his pain at each subsequent visit declined consistently over a 2-week period. He was sent to physical therapy specifically for a home exercise program for core strengthening and spinal stabilization. He purchased an FSM unit to treat himself at home as needed. He remains pain free after 2 years with home FSM treatment and exercises.
Beaman D.N., Graziano G.P., Woitys E.M., Chang V. Substance P innervation of lumbar spine facet joints. Spine. 1993;18:1044-1049.
Cavanaugh J.M., Ozaktay A.C., Yamashita H.T., King A.I. Lumbar facet pain; biomechanics, neuroanatomy and neurophysiology. J. Biomech.. 1996;29:1117-1129.
Cavanaugh J.M., Lu Y., Chen C., Kallakuri S. Pain generation in lumbar and cervical facet joints. J. Bone Joint Surg. Am.. 2006;88(Suppl. 2):63-67.
Chen C., Lu Y., Kallakuri S., Patwardhan A., Cavanaugh J.M. Distribution of A-delta and C-fiber receptors in the cervical facet joint capsule and their response to stretch. J. Bone Joint Surg. Am.. 2006;88:1807-1816.
Gerwin R.D., Dommerholt J., Shah J. An expansion of Simons’ integrated hypothesis of trigger point formation. Current Pain and Headache Reports. 2004;8:468-475.
Hoppenfeld S. Physical examination of the spine and extremities. New York: Appleton-Century Crofts, Division of Prentice Hall, 1976.
Huckfeldt R., Mikkelson D., Larson K., Hammond L., Flick B., McMakin C. The use of micro current and autocatalytic silver plated nylon dressings in human burn patients: a feasibility study. Pacific Rim Burn Conference. 2003.
Lewis C. Physiotherapy and spinal nerve root adhesion: a caution. Physiother. Res. Int.. 2004;9:164-173.
McMakin C. Microcurrent treatment of myofascial pain in the head, neck and face. Topics in Clinical Chiropractic. 1998;5(1):29-35.
McMakin C. Microcurrent therapy: a novel treatment method for chronic low back myofascial pain. Journal of Bodywork and Movement Therapies. 2004;8:143-153.
McMakin C. Cytokine changes with microcurrent treatment of fibromyalgia associated with cervical spine trauma. Journal of Body Work and Movement Therapies. 2005;9:169-176.
McMakin C. Private communication. 2007.
Netter F. Atlas of human anatomy. New York: Ciba-Geigy, 1991. Plate 159
Phillips T. Unpublished data, private communication. 2000.
Souza T. Differential diagnosis and management for the chiropractor: protocols and algorithms, fourth ed. Sudbury, MA: Jones & Bartlett Publishers, 2009.
Travell J.G., Simons D.G. Myofascial pain and dysfunction: the trigger point manual. Baltimore: Williams & Wilkins, 1983.
Travell J.G., Simons D.G. Myofascial pain and dysfunction: the trigger point manual. Baltimore: Williams & Wilkins; 1992;2.