CHAPTER 79 Pelvic girdle and lower limb: overview and surface anatomy
This chapter is made up of two sections. The first is an overview of the general organization of the lower limb, with particular emphasis on the fascial skeleton, distribution of the major blood vessels and lymphatic channels, and the branches of the lumbar and sacral plexuses: it is intended to complement the detailed regional anatomy described in Chapters 80 to 84 Chapter 81 Chapter 82 Chapter 83 Chapter 84. The second section describes the surface anatomy of the lower limb.
The structure of the lower limb is determined by its adaptations for weightbearing, locomotion and the maintenance of equilibrium (stability). Indeed, the adaptations for weightbearing and for stability, and the differing developmental histories of the limbs account for the major structural and functional differences between the upper and lower limbs. The inguinal (pelvicrural) and gluteal (buttock) regions are important anatomical junctional zones between the trunk and the lower limb through which longitudinally running nerves and vessels may pass in either direction. The inguinal region includes the junctional zones between the limb and abdominal cavity via the myopectineal orifice (the gap between the inguinal ligament and hip bone), and between the limb and pelvic cavity via the obturator foramen. The gluteal region includes the junctional zones between the limb and the abdominopelvic cavity via the greater sciatic foramen, and between the limb and the perineum via the lesser sciatic foramen (Fig. 79.1).
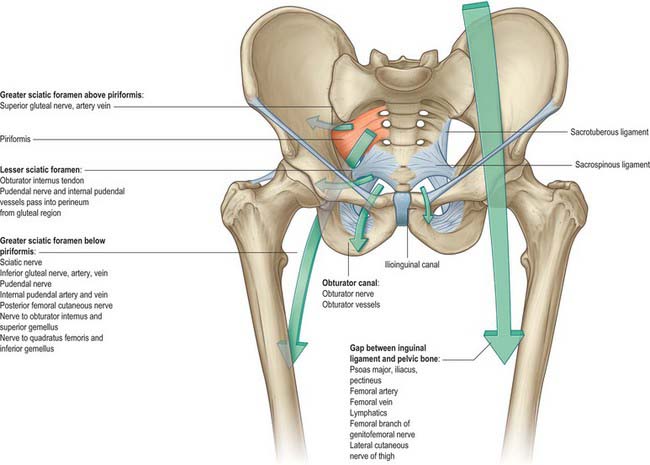
Fig. 79.1 Gateways from the abdomen, pelvis and perineum to the lower limb.
(From Drake, Vogl and Mitchell 2005.)
SKIN, FASCIA AND SOFT TISSUES
In the young adult the skin of the lower limb is generally stronger and thicker than that of the upper limb: weightbearing skin, e.g. of the sole of the foot, is particularly thickened. The skin of the buttocks and posterior thigh bears weight in the sitting position, and consequently is relatively thick. The skin over the anteromedial aspect of the lower leg is particularly fragile and vulnerable in the elderly. Body hair is usually well developed in all areas except the sole and posterior ankle.
Fascial skeleton
The ‘fascial skeleton’ (deep fascia) of the lower limb is well-defined and forms a tough circumferential ‘stocking-like’ structure that constrains the musculature (Fig. 79.2). Septa pass from the deep surface of this fascial sheath to the bones within, confining the functional muscle groups within osteofascial compartments. The tough fascia gives additional areas of attachment to the muscles and ensures that they work to maximal effect. Thickenings in the ensheathing layer may act as additional tendons (e.g. iliotibial tract). Elsewhere, thickenings in the fascial skeleton form fibrous retinacula where tendons cross joints. Although they are particularly prominent in the embalmed cadaver, these fascial layers are also readily demonstrable in the living, and are of considerable functional significance. The pattern of soft-tissue organization has a bearing on the physiological effects of the muscles and is crucial for efficient venous return from the limb. The fascial planes also control and direct the spread of pathological fluids (blood, pus) within the limb and play an important part in determining the degree and direction of displacement seen in long bone fractures.
Osteofascial compartments in the lower limb
The muscles of the thigh may be grouped into three compartments according to their function, namely anterior (extensor), posterior (flexor) and medial (adductor): only the anterior and posterior compartments possess distinct fascial boundaries. A very definite fascial separation into anterior (extensor), posterior (flexor) and lateral (evertor) compartments exists in the leg, and compartment syndrome is most common in this region (see below). Osteofascial compartments in the foot are described in Chapter 84.
Vessels and nerves run through all the osteofascial compartments and supply the muscles contained within them. The muscles acting within these closed compartments assist in maintaining the anti-gravity flow of venous blood.
The fascial boundaries that limit the osteofascial compartments are largely inelastic, which means that any condition that leads to an increase in the volume of the compartmental contents, e.g. muscle swelling caused by trauma or unaccustomed overuse, haemorrhage and local infection, is likely to cause an increase in intracompartmental pressure. If unrelieved, this increased pressure will lead to compressive occlusion of the vessels in the compartment and consequent ischaemic damage to the nerves and muscles of the compartment, a phenomenon known as compartment syndrome.
BONES AND JOINTS
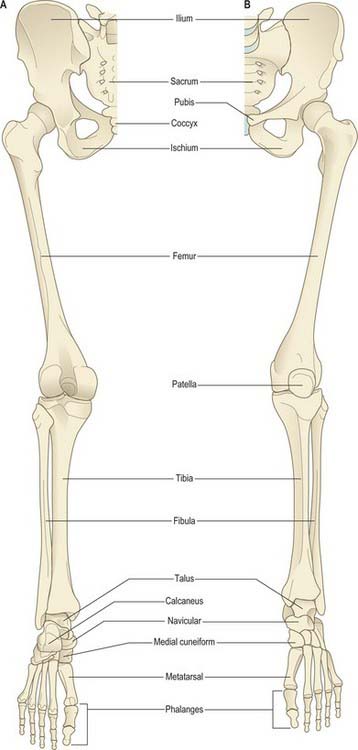
The bones of the lower limb are the three fused components of the pelvic girdle; the femur and patella (thigh); the tibia and fibula (leg); the tarsus, metatarsus and phalanges (foot) (Fig. 79.3). The hip bones (especially the ilium and ischium), femur, tibia and bones of the hindfoot are strong and their external (cortical) and internal (trabecular) structure is adapted for weightbearing.
The pelvic girdle connects the lower limb to the axial skeleton via the sacroiliac joint, a synovial joint in which mobility has been sacrificed for stability and strength, to allow for effective weight transmission from the trunk to the lower limb. Anteriorly, the pelvic girdle articulates with the contralateral girdle at the pubic symphysis, a secondary cartilaginous joint that may display a slight degree of mobility during hip and sacroiliac movement and during childbirth. The hip joint, a synovial ball-and-socket joint, exhibits a very effective compromise between mobility and stability that allows movement in all three orthogonal planes. The more distal joints have gained mobility at the expense of stability. The knee joint includes the patellofemoral articulation, which allows the patella to glide over the distal femur. However, the main component of the knee joint is a bicompartmental synovial articulation between the femur and the tibia that allows flexion, extension and some medial and lateral rotation of the leg. It is not a true hinge joint because its axes of flexion and extension are variable and there is coupled rotation. The tibia and fibula articulate with each other at the superior and inferior tibiofibular joints. The superior joint, a plane synovial joint, allows slight gliding movement only. The inferior joint, a fibrous joint, lies just above the ankle and allows a degree of fibular rotation linked to ankle motion. The ankle (talocrural) joint is formed by the distal ends of the tibia and fibula ‘gripping’ the talus, and allows dorsiflexion and plantarflexion. There are multiple joints in the foot that may be classified topographically on the basis of whether they are in the hindfoot, midfoot or forefoot. Collectively, these joints allow the complex movements required as the foot fulfils its functional roles as a platform for standing and for shock absorption and propulsion in gait.
Both knee and ankle are commonly subject to closed injuries, and the relatively superficial location of the knee renders it susceptible to open injury and infection. Although the ankle is frequently injured and is a major loadbearing joint, the incidence of clinically significant degenerative arthritis is surprisingly low when compared with that found in the hip and knee.
MUSCLES
The effects of extension and medial rotation of the limb that occur during fetal development are manifest in the relative positions of the muscle groups in the thigh and the leg, and in the adult pattern of segmental innervation (dermatomes). In broad outline, the anterior aspect of the adult limb is the extensor aspect, while the flexors lie posteriorly; the reverse is true at the hip.
The role of the muscles of the lower limb in the maintenance of equilibrium during locomotion and in stance is rarely emphasized sufficiently. Many of the muscles act frequently or predominantly from their distal attachments. During both stance and locomotion, the distal attachment is often fixed and the proximal attachment is mobile, e.g. the predominant action of gluteus medius is as a pelvic stabilizer rather than as a hip abductor. (In contrast, in the upper limb the proximal muscle attachments are usually fixed and the distal attachments are mobile, an arrangement that is consistent with the prehensile function of the hand.) The lower limb contains many muscles that act upon more than one joint, and it is unusual for any joint of the lower limb to move in isolation.
Muscles of the lower limb may be subdivided into muscles of the iliac and gluteal regions, and of the thigh, leg and foot. (Note that in anatomical nomenclature, ‘leg’ refers to that part of the lower limb between the knee and ankle.) The main muscles of the iliac region are psoas major and iliacus, the major flexors of the hip that run from the lumbar spine and inner surface of the ilium respectively to the lesser trochanter of the femur. The much less important psoas minor (when present) runs from the lumbar spine to the pubis. The muscles of the gluteal region include the three named gluteal muscles and the deeper short lateral rotators of the hip joint. Gluteus maximus lies most superficially, running from the posterior pelvis to the proximal femur and fascia lata. It is a powerful extensor of the hip joint, acting more often to extend the trunk on the femur than to extend the limb on the trunk. Gluteus medius and minimus, attaching proximally to the outer iliac surface and distally to the greater trochanter of the femur, are abductors of the hip; their most important action is to stabilize the pelvis on the femur during locomotion, and they are helped in this function by tensor fasciae latae, a more anteriorly placed muscle that arises from the anterolateral ilium and inserts into the fascia lata. Two of the short lateral rotators of the hip, piriformis and obturator internus, arise from within the pelvic walls, while the others, obturator externus, the gemelli and quadratus femoris, are attached externally: all of these muscles are attached distally to the proximal femur.
The muscles of the thigh lie in three functional compartments. The anterior or extensor compartment includes sartorius and the quadriceps group. Sartorius and rectus femoris are attached proximally to the pelvis and can thus act on the hip joint as well as on the knee, whereas the vasti are attached proximally to the femoral shaft, and, acting as a unit, are powerful knee extensors. The medial or adductor compartment contains the named adductor muscles and gracilis; pectineus may also be included. These muscles are attached proximally to the anterior aspect of the pelvis, and distally to the femur; gracilis has no femoral attachment, being attached distally to the proximal tibia, while a part of adductor magnus has a proximal attachment to the ischial tuberosity. The posterior (‘hamstring’) compartment includes semitendinosus, semimembranosus and biceps femoris. These muscles are attached proximally to the ischial tuberosity and act both to extend the trunk on the femur and to flex and rotate the knee. Adductor magnus, as may be inferred from the extent of its proximal attachment and its dual innervation, shares the first of these functions with the hamstrings. Biceps femoris is the only muscle of the thigh that is attached distally to the fibula, and has no tibial attachment.
In the leg the anterior or extensor compartment includes the extensors (dorsiflexors) of the ankle and the long extensors of the toes. Tibialis anterior, the main ankle dorsiflexor, also inverts the foot at the subtalar joint, while the smallest muscle of the compartment, fibularis (peroneus) tertius, is a dorsiflexor that everts the foot. The posterior or flexor (plantarflexor) compartment has superficial and deep components. The superficial component contains gastrocnemius and soleus, powerful plantar flexors of the ankle, and the slender plantaris. Gastrocnemius and soleus are attached distally via the calcaneal (Achilles) tendon. The deep component of the flexor compartment contains popliteus, a rotator of the knee, the long flexors of the toes and tibialis posterior, the main invertor of the foot. The lateral compartment contains the main evertors of the foot, fibularis (peroneus) longus and brevis; both muscles are also plantar flexors at the ankle.
Gastrocnemius, plantaris and popliteus are the only muscles of the leg that are attached proximally to the femur and they can therefore act on the knee as well as at the ankle. The remaining leg muscles are attached proximally to the tibia, fibula or both, and to the interosseous membrane. The intrinsic muscles of the sole of the foot are arranged in layers. They facilitate the actions of the long flexors of the toes, and by effecting subtle changes in the shape of the foot they help control foot posture in stance and locomotion.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
ARTERIAL SUPPLY
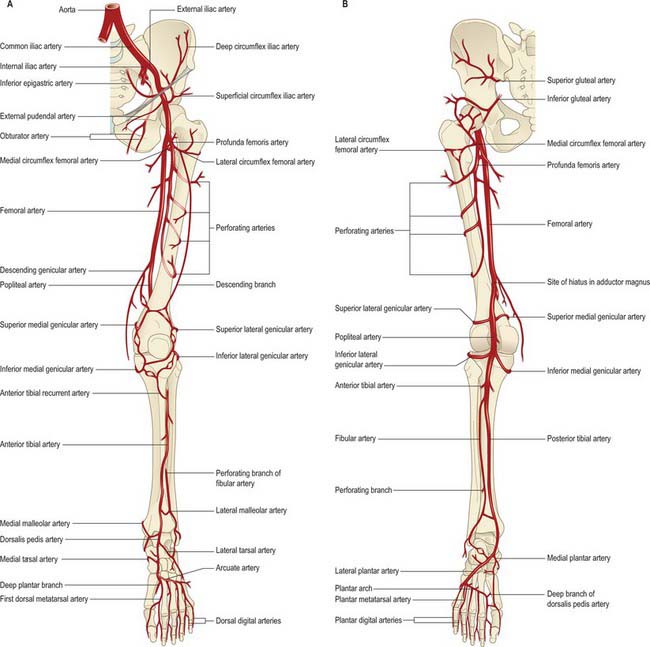
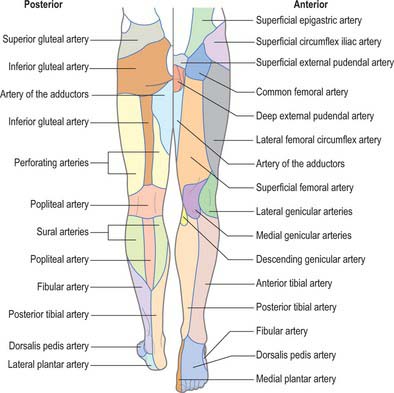
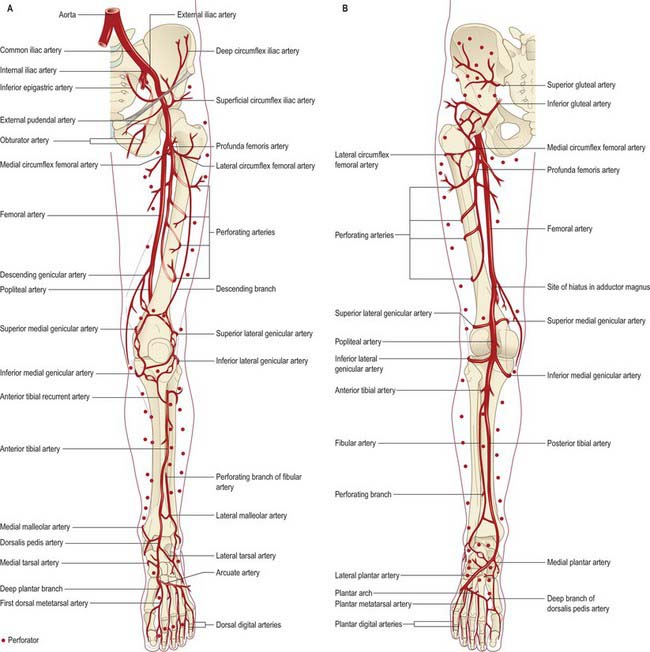
The femoral artery (the continuation of the external iliac artery) provides the principal arterial supply to the lower limb distal to the inguinal ligament and the gluteal fold (Figs 79.4, 79.5). The femoral artery courses within the anteromedial aspect of the thigh, becoming the popliteal artery on entering the posterior compartment of the thigh and dividing into its terminal branches in the posterior compartment of the leg. The obturator and inferior gluteal vessels also contribute to the supply of the proximal part of the limb. In the embryo the inferior gluteal artery supplied the main axial artery of the limb, which is represented in the adult by the arteria comitans nervi ischiadici (artery to the sciatic nerve).
The bones of the lower limb receive their arterial supply from nutrient vessels, metaphysial arterial branches of the peri-articular anastomoses, and the arteries supplying the muscles that attach to their periosteum. The pattern of arterial supply is particularly relevant to fracture healing, the spread of infection and malignancy, and to the planning of reconstructive surgical procedures. For further details consult Cormack & Lamberty (1994), Taylor & Razaboni (1994) and Crock (1996).
Arterial perforators of the lower limb
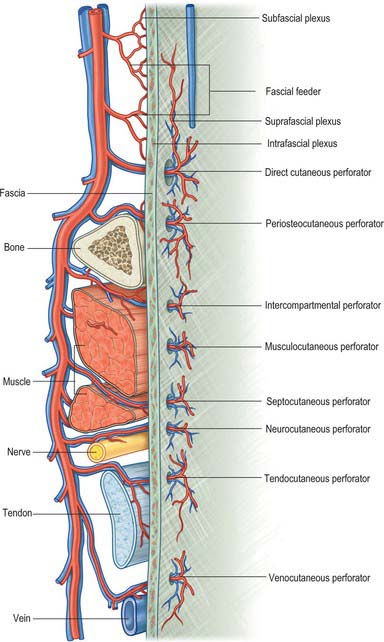
Achieving adequate and aesthetically satisfactory skin and soft tissue cover for large, superficial tissue defects is a perennial challenge in the field of plastic and reconstructive surgery, and accounts for a substantial part of the plastic surgeon’s workload. Generally, split-thickness and full-thickness skin grafts are suitable only for very superficial defects. To achieve tissue cover for deeper and larger tissue defects, the plastic surgeon employs one of a variety of autologous tissue flaps. The viability of a flap transplanted from one part of the body to another is crucially dependent on the blood supply of the flap. An appreciation of the angiosome concept (see Ch. 6), coupled with technological advances in reconstructive microsurgery, has stimulated the development and use of perforator (or perforator-based) flaps. These are flaps of skin or subcutaneous tissue supplied by one or more fascial ‘perforators’, i.e. arteries which reach the suprafascial plexus either directly from a source vessel, or indirectly from some other neighbouring tissue (Fig. 79.6). Perforator-based flaps are typically harvested with sparing of underlying muscle tissue and minimal trauma: their use is said to reduce postoperative pain, donor site morbidity and functional loss.
The lower limb is the largest donor site in the body for perforator-based flaps. Commonly used flaps are antero-lateral thigh flaps which provide a large amount of skin; superior and inferior gluteal artery perforator flaps used in breast reconstruction; vascularized fibula flaps for reconstruction of deficient bone; vascularized tensor fasciae latae flaps for tendon reconstruction; vascularized sural nerve flaps for nerve reconstruction; and the gracilis muscle flap, used in reanimation of paralysed muscle.
In the context of perforator flap surgery, the lower limb may be considered in terms of four anatomic regions: gluteal; anterior hip and thigh; knee and leg; ankle and foot. Each lower limb accounts for approximately 23% of the total body surface area (thigh 10.5%, leg 6.5%, buttock 2.5% and foot 3.5%) and contains an average of 90 arterial perforators (Fig. 79.7).
VENOUS DRAINAGE
The veins of the lower limb can be subdivided, like those of the upper limb, into superficial and deep groups (Figs 79.8, 79.9). The superficial veins are subcutaneous and lie in the superficial fascia; the deep veins (beneath the deep fascia) accompany the major arteries. Valves are present in both groups, but are more numerous in the deep veins. (Valves are more numerous in the veins of the lower limb than in the veins of the upper limb.) Venous plexuses occur within and between some of the lower limb muscles. The principal named superficial veins are the long and short saphenous veins; their numerous tributaries are mostly unnamed. For details and variations consult Kosinski (1926).
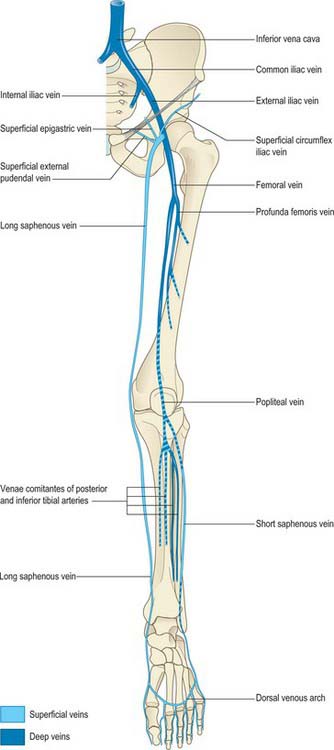
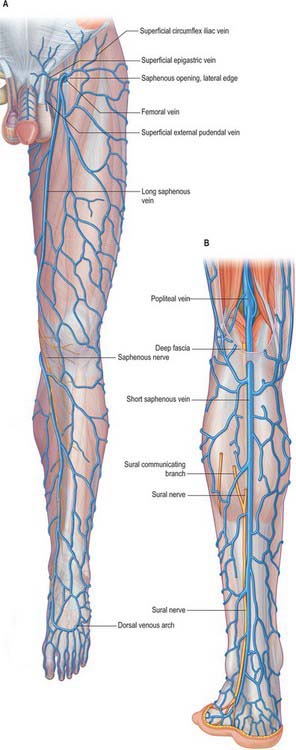
Fig. 79.9 A, The long saphenous vein and its tributaries. B, The short saphenous vein and its tributaries.
Deep veins of the lower limbs accompany the arteries and their branches. Plantar digital veins arise from plexuses in the plantar regions of the toes, connect with dorsal digital veins and unite to form four plantar metatarsal veins. These run in the intermetatarsal spaces and connect with dorsal veins by means of perforating veins. They then connect with each other to constitute a deep plantar venous arch adjacent to the plantar arterial arch. From this arch, medial and lateral plantar veins run near the corresponding arteries: they communicate with the long and short saphenous veins before forming the posterior tibial veins behind the medial malleolus. The posterior tibial veins accompany the posterior tibial artery. They receive veins from the calf muscles, especially the venous plexus in soleus, and connect with superficial veins and with the fibular veins. The latter, running with their artery, receive tributaries from soleus and from superficial veins.
The anterior tibial veins are continuations of the venae comitantes of the dorsalis pedis artery. They leave the extensor region between the tibia and fibula, pass through the proximal end of the interosseous membrane, and unite with the posterior tibial veins, at the distal border of popliteus, to form the popliteal vein.
Venous (muscle) pumps
In a standing position, venous return from the lower limb depends largely on muscular activity, especially contraction of the calf and foot muscles, known as the ‘muscle pump’, whose efficiency is aided by the tight sleeve of deep fascia. ‘Perforating’ veins connect the long saphenous vein with the deep veins, particularly near the ankle, distal calf and knee. Their valves are arranged so as to prevent flow of blood from the deep to the superficial veins. At rest, pressure in a superficial vein is equal to the height of the column of blood extending from that vein to the heart. When calf muscles contract, blood is pumped proximally in the deep veins and is normally prevented from flowing into the superficial veins by the valves in the perforating veins. During muscular relaxation, blood is drawn into the deep veins from the superficial veins. If the valves in the perforating veins become incompetent, these veins become sites of ‘high pressure leaks’ during muscular contraction, and the superficial veins become dilated and varicose. Similar perforating connections occur in the anterolateral region, where varicosities may also occur. Valvar incompetence in the connecting veins between the long saphenous vein and femoral vein in the adductor canal may predispose to superficial varicosities in the medial aspect of the thigh (Dodd & Cockett 1976).
LYMPHATIC DRAINAGE
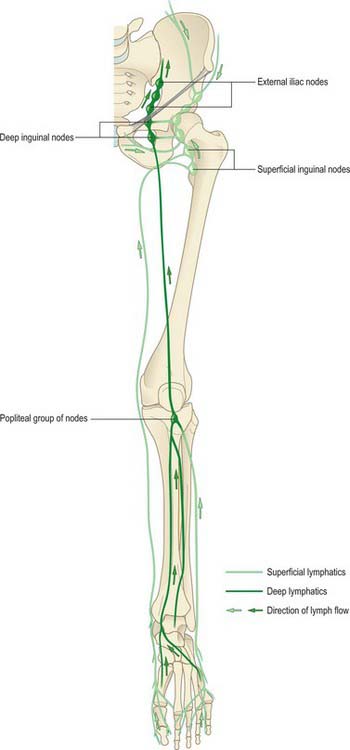
Most lymph from the lower limb traverses a large intermediary inguinal group of nodes (Fig. 79.10). Peripheral nodes are few and all are deeply sited. Except for an inconsistent node lying proximally on the interosseous membrane near the anterior tibial vessels, they occur only in the popliteal fossa. Enlarged popliteal nodes may be palpated along the line of the popliteal vessels while the passively supported knee is gradually moved from extension to semi-flexion. Inguinal nodes are found superficial and deep to the deep fascia. The deep nodes are few and lie alongside the medial aspect of the femoral vein. The superficial nodes may be divided into a lower vertical group that clothe the proximal part of the long saphenous vein, and an upper group that lie parallel to, but below, the inguinal ligament and which are related to the superficial circumflex iliac and superficial external pudendal vessels. Lymph from the lower limb passes from the inguinal nodes to the external and common iliac nodes, and ultimately drains to the lateral aortic group. Deep gluteal lymph reaches the same group through the internal and common iliac chains.
Superficial tissues
The superficial lymph vessels begin in subcutaneous plexuses. Collecting vessels leave the foot medially, along the long saphenous vein, or laterally with the short saphenous vein. Medial vessels are larger and more numerous; they start on the tibial side of the dorsum of the foot, ascend anterior or posterior to the medial malleolus and accompany the long saphenous vein. They drain to the distal superficial inguinal nodes. Lateral vessels begin on the fibular side of the dorsum of the foot; some cross anteriomedially in the leg to join the medial vessels and so pass to the distal superficial inguinal lymph nodes, others accompany the short saphenous vein and drain to the popliteal nodes. Superficial lymph vessels from the gluteal region run anteriorly to the proximal superficial inguinal nodes.
Deeper tissues
The deep lymph vessels accompany the anterior and posterior tibial, fibular, popliteal and femoral vessels. The deep vessels from the foot and leg are interrupted by popliteal nodes; those from the thigh pass to the deep inguinal nodes. The deep vessels of the gluteal and ischial regions follow their corresponding blood vessels. Those accompanying the superior gluteal vessels end in a node near the intrapelvic part of the superior gluteal artery, adjacent to the superior border of the greater sciatic foramen, while those which follow the inferior gluteal vessels traverse one or two of the small nodes below piriformis and pass to the internal iliac nodes.
INNERVATION
OVERVIEW OF THE LUMBAR AND SACRAL PLEXUSES
Nerves derived from the lumbar and sacral plexuses innervate the lower limb (Figs 79.11). The lumbar plexus lies deep within psoas major, anterior to the transverse processes of the first three lumbar vertebrae. The sacral plexus lies in the pelvis on the anterior surface of piriformis, external to the pelvic fascia, which separates it from the inferior gluteal and pudendal vessels. The lumbosacral trunk (L4 and L5) emerges medial to psoas major on the posterior abdominal wall and lies on the ala of the sacrum before crossing the pelvic brim to join the ventral ramus of S1.
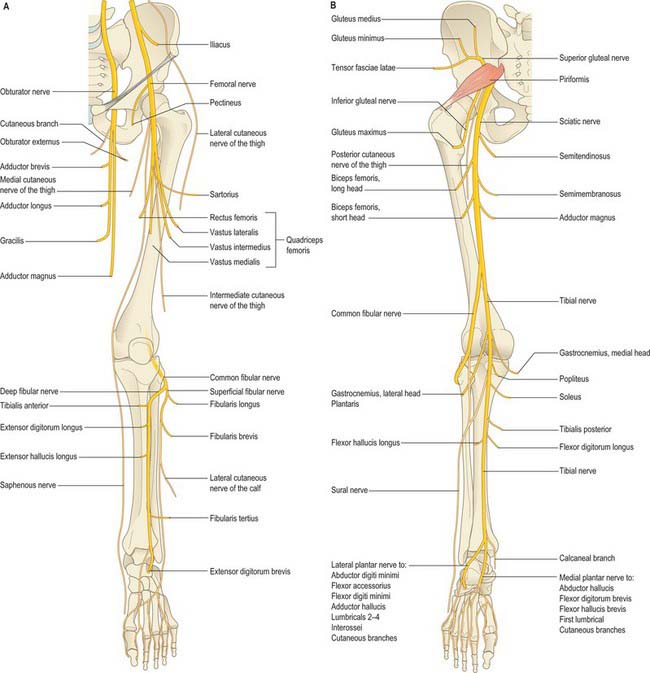
Fig. 79.11 Nerves of the lower limb, their cutaneous branches and muscular branches. A, anterior aspect. B, Posterior aspect. Adductor magnus has dual innervation.
Lesions of the lumbar and sacral plexuses
The deep and protected situation of the plexuses means that lesions are not common. The lumbar plexus may be involved in retroperitoneal pathology, and the sacral plexus may be invaded by spreading pelvic malignancy. Both may be involved in the reticuloses, affected by plexiform neuromas, or damaged in fractures of the lumbar spine and pelvis or in other conditions that cause severe retroperitoneal and pelvic haemorrhage. Temporary lesions may occur after pregnancy and childbirth, e.g. after difficult forceps delivery of a large baby. Pain, which may be diffuse, is the most common feature, and there is often clinical involvement of several roots.
OVERVIEW OF THE PRINCIPAL NERVES OF THE LOWER LIMB
Femoral nerve (L2–4)
The femoral nerve is the nerve of the anterior compartment of the thigh. It arises from the posterior divisions of the second to fourth lumbar ventral rami, descends through psoas major and emerges on its lateral border to pass between psoas and iliacus. It enters the thigh behind the inguinal ligament and lateral to the femoral sheath. Its terminal branches form in the femoral triangle about 2 cm distal to the inguinal ligament. In the abdomen the nerve supplies small branches to iliacus and a branch to the proximal part of the femoral artery. It subsequently supplies a large cutaneous area on the anterior and medial thigh, medial leg and foot, and gives articular branches to the hip and knee. The femoral nerve is described in detail on page 1383.
Obturator nerve (L2–4)
The obturator nerve is the nerve of the medial compartment of the thigh. It arises from the anterior divisions of the second to fourth lumbar ventral rami, descends through psoas major and emerges from its medial border at the pelvic brim. It crosses the sacroiliac joint behind the common iliac artery and lateral to the internal iliac vessels, runs along the lateral pelvic wall medial to obturator internus, and enters the thigh through the upper part of the obturator foramen. Near the foramen it divides into anterior and posterior branches which are separated at first by part of obturator externus and more distally by adductor brevis. It gives articular branches to the hip and knee, and may supply skin on the medial thigh and leg. The obturator nerve is described in detail on page 1383.
Sciatic nerve (L4, L5, S1–3)
The sciatic nerve is the nerve of the posterior compartment of the thigh and, via its major branches, of all the compartments of the leg and foot. Formed in the pelvis from the ventral rami of the fourth lumbar to third sacral spinal nerves, it is typically 2 cm wide at its origin and is the thickest nerve in the body. It enters the lower limb via the greater sciatic foramen below piriformis and descends between the greater trochanter and ischial tuberosity. The nerve passes along the back of the thigh, where it is crossed by the long head of biceps femoris, and divides into the tibial and common fibular (peroneal) nerves proximal to the knee: the level of bifurcation is variable. The tibial and common fibular nerves are structurally separate and only loosely held together within the sciatic nerve. The tibial nerve is derived from the anterior divisions of the sacral plexus and the common fibular nerve is made up of the posterior divisions of the plexus. The sciatic nerve gives off articular branches that supply the hip joint through its posterior capsule (these are sometimes derived directly from the sacral plexus) and the knee joint. All the hamstring muscles, including the ischial part of adductor magnus, but not the short head of biceps femoris, are supplied by the medial (tibial) component of the sciatic nerve. The short head of biceps is supplied by the lateral (common fibular) component. The sciatic nerve is described in detail on page 1384.
Tibial nerve (L4, L5, S1–3)
The tibial nerve is derived from the anterior divisions of the sacral plexus. It descends along the back of the thigh and popliteal fossa to the distal border of popliteus, then passes anterior to the arch of soleus with the popliteal artery and continues into the leg. In the popliteal fossa it lies lateral to the popliteal vessels, becomes superficial to them at the knee and crosses to the medial side of the artery. In the leg it is the nerve of the posterior compartment and descends with the posterior tibial vessels to lie between the heel and the medial malleolus. It ends beneath the flexor retinaculum by dividing into the medial and lateral plantar nerves. The tibial nerve supplies articular branches to the knee and ankle. Its cutaneous area of supply, including its terminal branches, includes the back of the calf, the whole of the sole, the lateral border of the foot and the medial and lateral sides of the heel. The tibial nerve is described in detail on page 1427.
Common fibular nerve (L4, L5, S1, S2)
The common fibular nerve (common peroneal nerve) is derived from the posterior divisions of the sacral plexus. In the leg it is the nerve of the anterior and lateral compartments. It descends obliquely along the lateral side of the popliteal fossa to the fibular head, lying between the tendon of biceps femoris and the lateral head of gastrocnemius, then curves lateral to the neck of the fibula lying on the bone deep to fibularis longus and divides into superficial and deep fibular (peroneal) nerves. Before it divides, it gives off articular branches to the knee and the superior tibiofibular joints, and cutaneous branches. The cutaneous area supplied by the common fibular nerve and its terminal branches includes the anterolateral and lateral surfaces of the leg and most of the dorsum of the foot. The common fibular nerve is described in detail on page 1427.
Gluteal nerves
The gluteal nerves arise from the posterior divisions of the sacral plexus. The superior gluteal nerve (L4, L5, S1) leaves the pelvis through the greater sciatic notch above piriformis and supplies gluteus medius, gluteus minimus, tensor fasciae latae and the hip joint. The inferior gluteal nerve (L5, S1, S2) passes through the greater sciatic notch below piriformis and supplies gluteus maximus. The gluteal nerves are described in detail on page 1384.
AUTONOMIC INNERVATION
The autonomic supply to the limbs is exclusively sympathetic. The preganglionic sympathetic inflow to the lower limb is derived from neurones in the lateral horn of the lower thoracic (T10, T11 and T12) and upper lumbar (L1, L2) spinal cord segments. Fibres pass in white rami communicantes to the sympathetic chain and synapse in the lumbar and sacral ganglia. Postganglionic fibres pass in grey rami communicantes to enter the lumbar and sacral plexuses, and many are distributed via the cutaneous branches of the nerves derived from these plexuses. The blood vessels to the lower limb receive their sympathetic supply via adjacent peripheral nerves. Postganglionic fibres accompanying the iliac arteries are destined mainly for the pelvis but may supply vessels in the upper thigh.
Surgical or chemical lumbar sympathectomy may be indicated in arterial disease and in the management of plantar hyperhidrosis, and may be used to treat rest pain or other troublesome sensory symptoms in arterial disease or in causalgia. The segment of the chain including the second and third lumbar ganglia is removed: preservation of the first lumbar ganglion is said to lessen the risk of ejaculatory problems.
MOVEMENTS, MUSCLES AND SEGMENTAL INNERVATION
Most limb muscles are innervated by neurones which are derived from more than one segment of the spinal cord. The predominant segmental origin of the nerve supply for each of the muscles of the lower limb and for the movements which take place at the joints of the lower limb is summarized in Tables 79.1-79.4. Red has been used in Table 79.3 to highlight those muscles or movements which have diagnostic value (see below): damage to these segments or to their motor roots results in maximum paralysis. Data are based chiefly on clinical evidence (Sharrad 1995). The following caveats should be borne in mind when consulting these tables.
Table 79.1 Segmental innervation of the muscles of the lower limb
| L1 | Psoas major, psoas minor |
| L2 | Psoas major, iliacus, sartorius, gracilis, pectineus, adductor longus, adductor brevis |
| L3 | Quadriceps, adductors (magnus, longus, brevis) |
| L4 | Quadriceps, tensor fasciae latae, adductor magnus, obturator externus, tibialis anterior, tibialis posterior |
| L5 | Gluteus medius, gluteus minimus, obturator internus, semimembranosus, semitendinosus, extensor hallucis longus, extensor digitorum longus, finularis tertius, popliteus |
| S1 | Gluteus maximus, obturator internus, piriformis, biceps femoris, semitendinosus, popliteus, gastrocnemius, soleus, fibularis longus and fibularis brevis, extensor digitorum brevis |
| S2 | Piriformis, biceps femoris, gastrocnemius, soleus, flexor digitorum longus, flexor hallucis longus, some intrinsic foot muscles |
| S3 | Some intrinsic foot muscles (except abductor hallucis, flexor hallucis brevis, flexor digitorum brevis, extensor digitorum brevis) |
Table 79.2 Segmental innervation of joint movements of the lower limb
| Hip | Flexors, adductors, medial rotators | L1–3 |
| Extensors, abductors, lateral rotators | L5, S1 | |
| Knee | Extensors | L3,4 |
| Flexors | L5, S1 | |
| Ankle | Dorsiflexors | L4, 5 |
| Plantarflexors | S1, 2 | |
| Foot | Invertors | L4, 5 |
| Evertors | L5, S1 | |
| Intrinsic muscles | S2, 3 |
Table 79.3 Movements, muscles and segmental innervation in the lower limb. Muscles and movements that have diagnostic value are marked in red
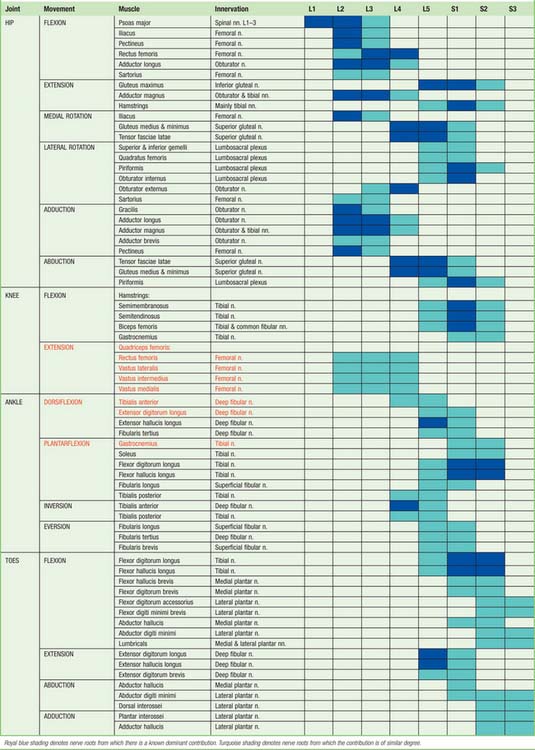 |
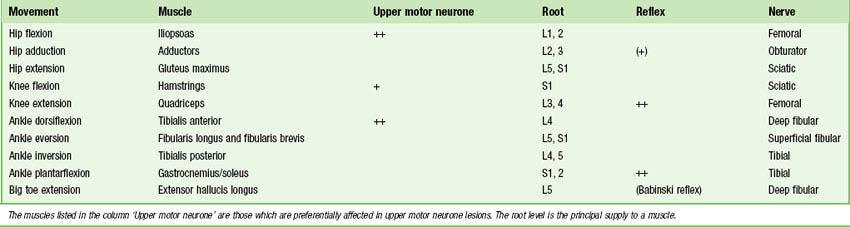
At the central nervous level of control, muscles are not recognized as individual actuators but as components of movement, and may therefore contribute to several types of movement, acting variously as prime movers, antagonists, fixators or synergists. Some muscles have been included in more than one place in Table 79.3, on the basis that a muscle which acts across one joint can produce a combination of movements (e.g. flexion with medial rotation, or extension with adduction) and a muscle which crosses two joints can produce more than one movement. It must also be remembered that these listings are not exhaustive.
There is no universal consensus concerning the contribution that individual spinal roots make to the innervation of individual muscles: the most positive identifications, which are limited, have been obtained by electrically stimulating spinal roots and recording the evoked electromyographic activity in the muscles. Much of the information in Tables 79.1-79.4 is therefore based on neurological experience gained in examining the effects of lesions, and some of it is far from new. Spinal roots have been given turquoise shading when they innervate a muscle to a similar extent, or when differences in their contribution have not been described. Royal blue has been used to indicate roots from which there is known to be a dominant contribution. Minor contributions have been retained in the table in order to increase its utility in other contexts, such as electromyography and comparative anatomy.
Neurological localization of a lesion
In clinical practice it is only necessary to test a relatively small number of muscles in order to determine the location of a lesion. Any muscle to be tested must satisfy a number of criteria. It should be visible, so that wasting or fasciculation can be observed, and the muscle consistency with contraction can be felt. It should have an isolated action, so that its function can be tested separately. It should help to differentiate between lesions at different levels in the neuraxis and in the peripheral nerve, or between peripheral nerves. It should be tested in such a way that normal can be differentiated from abnormal, so that slight weakness can be detected early with reliability. Some preference should be given to muscles with an easily elicited reflex. Table 79.4 gives a list of movements and muscles chosen according to these criteria: in practice, these tests would be combined with tests of sensory function. Knowledge of the sequence in which motor branches leave a peripheral nerve to innervate specific muscles is very helpful in localizing the level of a lesion.
SURFACE ANATOMY
SKELETAL LANDMARKS
Pelvis
An oblique skin crease, the fold of the groin, marks the junction of the front of the thigh with the anterior abdominal wall, and lies distal to the inguinal ligament (Fig. 79.12). The anterior superior iliac spine lies above the lateral end of the fold and can always be palpated. At its medial end, the fold reaches the pubic tubercle. From the anterior superior iliac spine, the iliac crest is easily palpable along its entire length. It terminates posteriorly as the posterior superior iliac spine, which may be felt in the depression seen just above the buttock. This depression lies at the level of the second sacral segment, at the level of the middle of the sacroiliac joint and the termination of the spinal dural sac. The ischial tuberosity may be palpated in the lower part of the buttock. It is covered by gluteus maximus when the hip joint is extended, but can be identified without difficulty when the hip is flexed, e.g. in the sitting position, when the tuberosity emerges from under cover of the lower border of gluteus maximus and becomes subcutaneous, separated from the skin only by a pad of fat and the ischial bursa. In this position, the weight of the body is supported by the ischial tuberosities.
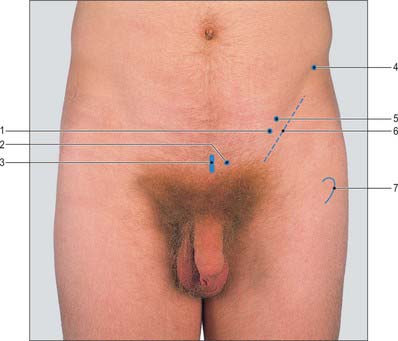
Fig. 79.12 Inguinal region. 1. Mid-inguinal point. 2. Pubic tubercle. 3. Pubic symphysis. 4. Anterior superior iliac spine. 5. Midpoint of inguinal ligament. 6. Groin crease. 7. Greater trochanter.
(With permission from Lumley JSP, 2002, Surface Anatomy, The Anatomical Basis of Clinical Examination, 3rd edn. Edinburgh: Churchill Livingstone.)
Femur
The greater trochanter of the femur, which is the only palpable part of the proximal portion of the femur, lies the breadth of the subject’s hand below the midpoint of the iliac crest. It can be both seen and felt as a prominence in front of the hollow on the side of the gluteal region. The lower end of the femur is less deeply placed. When the knee is flexed passively, the medial surface of the medial condyle and the lateral surface of the lateral condyle of the femur may both be palpated, and portions of the femoral articular surface can be examined on each side of the lower part of the patella.
Patella
The patella can be readily identified. When the quadriceps is relaxed in the fully extended knee, the patella can be tilted and moved on the lower end of the femur. The lower limit of the patella lies more than 1–2 cm above the line of the knee joint (Figs 73.13 and 73.14).
Knee
The patella and the medial and lateral condyles of the femur have been described above. The tibial condyles form visible and palpable landmarks at the medial and lateral sides of the patellar tendon (Fig. 79.13). The latter may be traced downwards from the apex of the patella to the tibial tubercle, which is easily seen as well as felt. When the knee is flexed, the anterior margins of the tibial condyles can be felt: each forms the lower boundary of a depression at the side of the patellar tendon. The lateral condyle is the more prominent of the two. The joint line of the tibiofemoral joint corresponds to the upper margins of the tibial condyles and can be represented by a line drawn round the limb at this level. The anterior horns of the menisci lie in the angles between this line and the edges of the patellar tendon. The iliotibial tract is attached to a prominence, Gerdy’s tubercle, on the anterior aspect of the lateral condyle that is usually 1 cm below the joint line and 2 cm lateral to the tibial tubercle.
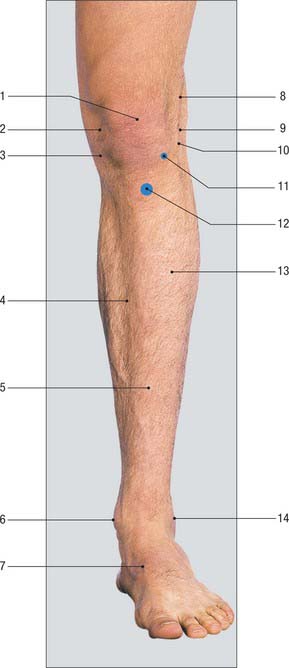
Fig. 79.13 Anterior aspect of the knee and leg. 1. Patella. 2. Medial femoral condyle. 3. Medial tibial condyle. 4. Medial surface of tibial shaft. 5. Anterior border of tibia. 6. Medial malleolus. 7. Tibialis anterior tendon. 8. Iliotibial tract. 9. Lateral femoral condyle. 10. Joint line of knee. 11. Gerdy’s tubercle on anterior aspect of lateral tibial condyle. 12. Tibial tubercle. 13. Anterior compartment of leg. 14. Lateral malleolus.
(With permission from Lumley JSP, 2002, Surface Anatomy, The Anatomical Basis of Clinical Examination, 3rd edn. Edinburgh: Churchill Livingstone.)
The head of the fibula forms a slight surface elevation on the upper part of the posterolateral aspect of the leg. It lies vertically below the posterior part of the lateral condyle of the femur, not less than 1 cm below the level of the knee joint.
Leg and ankle
The subcutaneous medial surface of the tibia corresponds to the flat anteromedial aspect of the leg. Above, this surface merges with the medial condyle of the tibia, and below it is continuous with the visible prominence of the medial malleolus of the tibia (Fig. 79.14A). The sinuous anterior border of the tibia can be felt distinctly throughout most of its extent, but inferiorly it is somewhat masked by the tendon of tibialis anterior, which lies to its lateral side. The lateral malleolus of the fibula forms a conspicuous projection on the lateral side of the ankle: it descends to a more distal level than the medial malleolus and is placed on a more posterior plane (Fig. 79.14B). The lateral aspect of the lateral malleolus is continuous above with an elongated, subcutaneous, triangular area of the lower shaft of the fibula. The lateral part of the anterior margin of the lower end of the tibia can be detected immediately in front of the base of the lateral malleolus; the line of the ankle joint can be gauged from it.

Fig. 79.14 A, Medial aspect of the knee, leg and foot. 1. Knee joint line. 2. Tibialis posterior tendon. 3. Navicular tuberosity. 4. Medial cuneiform. 5. Patellar tendon. 6. Medial surface of tibia. 7. Anterior border of tibia. 8. Medial malleolus. 9. Tibialis anterior tendon. B, Lateral aspect of the knee. 1. Patella. 2. Iliotibial tract. 3. Patellar tendon. 4. Lateral malleolus. 5. Tendon of fibularis tertius. 6. Tendon of biceps femoris. 7. Head of fibula. 8. Tendons of fibularis longus and brevis. 9. Styloid process of 5th metatarsal.
(A and B with permission from Lumley JSP, 2002, Surface Anatomy, The Anatomical Basis of Clinical Examination, 3rd edn. Edinburgh: Churchill Livingstone.)
Foot
The anterior part of the upper surface of the calcaneus can be identified a little in front of the lateral malleolus on the dorsum of the foot. When the foot is passively inverted, the upper and lateral part of the head of the talus can be both seen and felt 3 cm anterior to the distal end of the tibia; it is obscured by the extensor tendons when the toes are dorsiflexed.
The dorsal aspects of the bodies of the metatarsal bones can be felt more or less distinctly, although they tend to be obscured by the extensor tendons of the toes. The tuberosity on the base of the fifth metatarsal bone forms a distinct projection, which can be both seen and felt, half-way along the lateral border of the foot.
The flat lateral surface of the calcaneus can be palpated on the lateral aspect of the heel and can be traced forwards below the lateral malleolus, where it is hidden by the tendons of fibularis longus and brevis. The peroneal tubercle (fibular tubercle), when sufficiently large, can be felt 2 cm below the tip of the lateral malleolus. A palpable depression just anterior to the lateral malleolus leads to the lateral end of the sinus tarsi.
On the medial side of the foot, the sustentaculum tali of the calcaneus can be felt 2 cm vertically below the medial malleolus. The medial aspect of the calcaneus can be felt (indistinctly) below and behind the sustentaculum tali. The most conspicuous bony landmark on the medial side of the foot is the tuberosity of the navicular bone, which is usually visible and can always be felt 2.5 cm anterior to the sustentaculum tali. Anterior to this, the medial cuneiform bone can be identified by tracing the tendon of tibialis anterior into it. The upper and medial parts of the joint between the medial cuneiform and the first metatarsal can be felt as a narrow groove.
When the foot is placed on the ground, it rests on the posterior part of the inferior surface of the calcaneus, the heads of the metatarsal bones and, to a lesser extent, on its lateral border. The instep, which corresponds to the medial longitudinal arch of the foot, is elevated from the ground. The medial and lateral tubercles of the calcaneus can be identified on the posterior part of the inferior surface of the calcaneus, but they are obscured by the tough fibro-fatty pad that covers them. The heads of the metatarsal bones are similarly covered by a thick pad, which forms the ball of the foot. The foot is at its widest at this level, reflecting the slight splay of the metatarsal bones as they pass anteriorly.
The calcaneocuboid joint lies 2 cm behind the tubercle on the base of the fifth metatarsal bone and is practically in line with the talonavicular joint, whose position may be gauged from the position of the head of the talus. The tarsometatarsal joints lie on a line joining the tubercle of the fifth metatarsal bone to the tarsometatarsal joint of the great toe. When the latter joint cannot be felt on the medial border of the foot, its position may be indicated 2.5 cm in front of the tuberosity of the navicular bone. The joint between the second metatarsal and the intermediate cuneiform lies some 2–3 mm behind the line of the other tarsometatarsal joints. The metatarsophalangeal joints lie 2.5 cm behind the webs of the toes.
MUSCULOTENDINOUS AND LIGAMENTOUS LANDMARKS
Buttock and hip
The bulky prominence of the buttock is caused by the forward tilt of the pelvis (which throws the ischium backwards), the size of gluteus maximus, and the large amount of subcutaneous fat.
The horizontal gluteal fold marks the upper limit of the posterior aspect of the thigh. It does not correspond to the lower border of gluteus maximus but is caused by fibrous connections between the skin and the deep fascia. The natal cleft, which separates the buttocks inferiorly, starts above at the third or fourth sacral spine. The upper border of gluteus maximus begins on the iliac crest some 3 cm lateral to the posterior superior iliac spine and runs downwards and laterally to the apex of the greater trochanter. Its lower border corresponds to a line drawn from the ischial tuberosity, through the midpoint of the gluteal fold, to a point about 9 cm below the greater trochanter (Fig. 79.15). Although gluteus maximus overlaps the ischial tuberosity in the standing position, on sitting it slides superiorly posterior to the tuberosity, leaving it free to bear weight. The muscle can be felt to contract when the hip is extended against resistance.
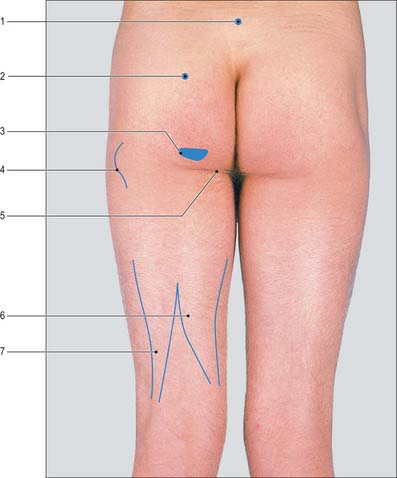
Fig. 79.15 Gluteal region and posterior aspect of the thigh. 1. 4th lumbar spinous process. 2. Posterior superior iliac spine. 3. Ischial tuberosity. 4. Greater trochanter. 5. Gluteal crease. 6. Semitendinosus and semimembranosus. 7. Biceps femoris.
(With permission from Lumley JSP, 2002, Surface Anatomy, The Anatomical Basis of Clinical Examination, 3rd edn. Edinburgh: Churchill Livingstone.)
Gluteus medius completely covers the underlying gluteus minimus. Both muscles lie in a slight depression superolateral to gluteus maximus and inferior to the anterior portion of the iliac crest. They constitute the major abductors of the hip and are demonstrated by asking the subject to stand on one limb. The ipsilateral muscles contract and tilt the pelvis in order to stabilize the centre of gravity, and the contralateral gluteal fold will rise. If the hip abductors are paralysed, e.g. in congenital dislocation of the hip or in a long-standing fracture of the neck of the femur, this mechanism is disturbed and the normal tilting of the pelvis does not occur. Indeed, when the patient stands on the affected hip, the pelvis tilts downwards on the contralateral side (Trendelenburg’s sign).
Thigh
The inguinal ligament can be felt running between the anterior superior iliac spine and the pubic tubercle when the thigh is abducted and externally rotated. Just distal to the inguinal ligament, but running horizontally, is the hip flexure line (Holden’s line), where the deep layer of superficial fascia of the abdominal wall meets the fascia lata of the thigh.
The shallow depression lying immediately below the fold of the groin corresponds to the femoral triangle. It is bounded on its lateral side by the strap-like sartorius which can be both seen and felt in a reasonably thin and muscular subject when the hip is flexed in the sitting position, while keeping the knee extended, especially when the thigh is slightly abducted and rotated laterally. Sartorius can be traced downwards and medially from the anterior superior iliac spine to approximately half-way down the medial side of the thigh; distally, it may be identified as a soft longitudinal ridge passing towards the posterior part of the medial femoral condyle. The adductor group of muscles forms the bulky, fleshy mass at the upper part of the medial side of the thigh. The medial border of adductor longus forms the medial boundary of the femoral triangle and can be felt as a distinct ridge when the thigh is adducted against resistance. At its upper end, its tendon of origin immediately below the pubic tubercle can be identified and felt between the finger and thumb, which is a useful guide to this bony landmark.
The forward convexity of the front of the thigh is caused by the curvature of the femur covered by the fleshy mass of quadriceps femoris. Rectus femoris appears as a ridge passing down the anterior aspect of the thigh when the sitting subject flexes the hip with the knee extended. Vastus medialis constitutes the bulge above and medial to the patella. Vastus lateralis forms the elevation above and lateral to the patella, more proximal and less pronounced than that of vastus medialis. Vastus intermedius is hidden by the other three muscles.
The flattened appearance of the lateral aspect of the thigh is produced by the iliotibial tract, which is a thickened portion of the deep fascia of the thigh (fascia lata). It stands out as a strong, visible ridge on the lateral aspect of the knee when the knee is either extended against gravity or when the opposite limb is lifted from the floor while standing.
Knee
The large depression that can be seen at the back of the knee when the joint is actively flexed against resistance corresponds to the popliteal fossa (Fig. 79.16). The transverse skin crease of the popliteal fossa is 2–3 cm above the tibiofemoral joint line. The fossa is bounded on the lateral side by the prominent tendon of biceps femoris, which can be felt between the finger and thumb and can be traced downwards to the head of the fibula. Three tendons can be felt on the medial side of the fossa. Semitendinosus is the most lateral and posterior, and gracilis is the most medial and anterior. These two tendons stand out sharply and can be seen when the knee is flexed against resistance and the limb actively adducted. The third tendon is that of semimembranosus: it is more deeply situated and can be felt in the interval between the tendons of semitendinosus and gracilis. It is much thicker than the other two tendons and broadens rapidly as it is traced upwards. Distally, in thin individuals, the upper border of the pes anserinus can be palpated. The upper borders of the two heads of gastrocnemius form the medial and lateral inferior boundaries of the popliteal fossa.
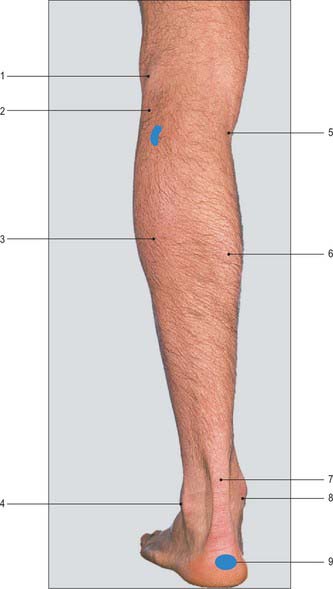
Fig. 79.16 Posterior aspect of the leg and heel. 1. Tendon of biceps femoris. 2. Head of fibula. 3. Lateral head of gastrocnemius. 4. Lateral malleolus. 5. Semitendinosus. 6. Medial head of gastrocnemius. 7. Calcaneal tendon. 8. Medial malleolus. 9. Calcaneus.
(With permission from Lumley JSP, 2002, Surface Anatomy, The Anatomical Basis of Clinical Examination, 3rd edn. Edinburgh: Churchill Livingstone.)
The lateral collateral ligament may be felt passing from the tip of the fibular head to the lateral epicondyle of the femur when the knee is flexed and laterally directed pressure is applied to the medial side of the knee. The medial patellofemoral ligament may be felt overlying the medial femoral condyle in the flexed knee, running between the midpoint of the medial patella and medial femoral epicondyle.
Leg
The muscles in the anterior osteofascial compartment of the leg form a gentle prominence over the upper two-thirds of its anterolateral aspect: this prominence is accentuated when the foot is actively dorsiflexed. In the lower third of the leg these muscles are replaced by their tendons. The tendon of tibialis anterior can be seen just lateral to the anterior border of the tibia and traced downwards and medially across the front of the ankle (Fig. 79.14A). The other tendons cannot be examined satisfactorily above the ankle. Immediately above the medial malleolus and close to the medial border of the tibia, the tendons of tibialis posterior and flexor digitorum longus can be felt (rather indistinctly) when the foot is actively inverted and plantar flexed.
On the lateral aspect of the leg, fibularis longus can be seen as a narrow ridge during active eversion and plantarflexion of the foot. It covers and hides fibularis brevis. Both muscles cover the lateral aspect of the fibula, which means that the shaft of the fibula can only be palpated indistinctly between its neck and its lower subcutaneous triangular area.
The bulky prominence of the calf of the leg is formed by gastrocnemius and soleus, both of which can be identified either when the foot is plantar flexed against resistance, or when the heel is raised from the ground by standing on tiptoes. The two heads of gastrocnemius unite to form the inferior angle of the popliteal fossa. The medial head of gastrocnemius descends to a lower level than the lateral head. Soleus lies deep to gastrocnemius; when tensed, it bulges from under gastrocnemius, particularly on the lateral side, and its fleshy belly extends to a more distal level. Both muscles end below in the conspicuous calcaneal tendon which can be gripped between the finger and thumb and followed downwards to its insertion into the posterior aspect of the calcaneus (Fig. 79.16).
Foot
When the toes are actively dorsiflexed, the belly of extensor digitorum brevis forms a small elevation on the dorsum of the foot, a little in front of the lateral malleolus. It is the only intrinsic muscle of the foot to arise from the dorsum of the foot. The tendon of tibialis anterior stands out conspicuously on the medial side when active dorsiflexion of the toes is combined with inversion: it can be traced downwards and medially to the medial cuneiform bone. Also in dorsiflexion, the tendon of extensor hallucis longus can be identified lateral to tibialis anterior. Still more laterally, and immediately in front of the lateral part of the inferior end of the tibia, the tendons of extensor digitorum longus and fibularis tertius are crowded together as they pass through the fibrous loop of the inferior extensor retinaculum. More distally, these tendons diverge to their insertions.
The tendon of tibialis posterior winds posterior to the medial malleolus and then curves forwards in the interval between this bony landmark and the sustentaculum tali to reach the tuberosity of the navicular bone. The tendon is thrown into relief when the foot is forcibly plantar flexed and inverted. The tendon of flexor digitorum longus lies midway between the medial margin of the calcaneal tendon and the margin of the medial malleolus. It curves forwards below tibialis posterior and lies on the medial aspect of the sustentaculum tali. From there, it passes forwards and laterally to the centre of the sole of the foot, where it breaks up into tendons for the lateral four toes. The tendon of flexor hallucis longus lies inferior to, and grooves, the sustentaculum tali. As it passes forward to the great toe, it crosses the line of the flexor digitorum longus opposite the interval between the sustentaculum tali and the tuberosity of the navicular bone. Abductor hallucis may be seen in some subjects as a fleshy mass across the instep of the foot, passing from the medial calcaneal tubercle to the ball of the great toe.
The plantar fascia is most easily palpated along its medial border, in the sole of the foot when the toes are maximally dorsiflexed. Its precise origin is difficult to palpate because of the thickness of the heel pad, but it is easily palpated just distal to the heel pad as far as the ball of the foot.
VESSELS, PULSES AND NERVES
Arteries
The femoral artery enters the thigh at a point midway between the anterior superior iliac spine and the pubic symphysis, directly anterior to the hip joint. Its course can be represented by the upper two-thirds of a line joining that point to the adductor tubercle when the flexed thigh is abducted slightly and rotated laterally.
The popliteal artery may be represented approximately by a line extending from the junction of the middle and lower thirds of the thigh, 2.5 cm medial to its posterior midline, to the midpoint between the femoral condyles, and continuing inferolaterally to the level of the tibial tuberosity, medial to the fibular neck. The artery bifurcates into the anterior and posterior tibial arteries at the lower border of popliteus.
The anterior tibial artery may be represented by a line extending from a point half-way between the tibial tuberosity and fibular head to a point midway between the anterior borders of the two malleoli.
The posterior tibial artery corresponds to a line drawn from a mid-axial point on the calf at the level of the neck of the fibula to a point a third of the way between the posterior border of the medial malleolus and the calcaneal tendon. The same line represents the course of the tibial nerve. At first the nerve lies lateral to the popliteal artery, then gradually crosses the vessel to gain its medial side. The trunk of the medial plantar artery begins midway between the medial malleolus and heel (medial calcaneal tubercle) and extends towards the first interdigital cleft as far as the navicular bone.
Pulses
The pulsations of the femoral artery can be felt at its origin, where the vessel can be compressed against the superior ramus of the pubis or the head of the femur. Like the carotid pulse, the femoral pulse is of value in assessing whether there is any significant cardiac output in cases of circulatory collapse. It is a common site for radiological catheter insertion and for arterial puncture for blood gas analysis.
The pulse of the popliteal artery is the most difficult of the peripheral pulses to feel because the artery lies deep in the popliteal fossa. It is best examined with the subject lying supine or prone, with the knee flexed, in order to relax the tense popliteal fascia that roofs the popliteal fossa. The popliteal pulse is then felt by deep pressure over the midline of the fossa against the popliteal surface of the femur.
Veins
The surface marking for the femoral vein is immediately medial to the femoral pulse. The long saphenous vein usually terminates 2 cm inferior to the femoral pulse. Its course may be marked out in the thigh by a line passing from this point downwards and backwards to a point the breadth of the subject’s hand behind the medial border of the patella.
The long saphenous vein can often be seen as it runs upwards and backwards across the medial surface of the tibia a little above and in front of the medial malleolus: this is a useful site for obtaining surgical venous access or for harvesting vein for cardiac bypass surgery. The vein is accompanied in this region by the saphenous nerve, which is usually anterolateral, but may be posterior, to the vein. The vein and nerve then run proximally and posteriorly along the medial border of the tibia to reach a point the breadth of the subject’s hand posterior to the medial border of the patella. The short saphenous vein may be represented by a line that runs from the posterior surface of the lateral malleolus up the midline of the calf to the popliteal fossa; together with the sural nerve, it is the key anatomical guide to surgical dissection of the popliteal fossa.
The dorsal venous arch is often a conspicuous feature on the dorsum of the foot and curves, convex forwards, across the metatarsus. The long saphenous vein arises from its medial end and runs upwards and backwards immediately in front of the medial malleolus. The short saphenous vein arises from the lateral end of the arch and passes backwards and inferior to, and then upwards and posterior to, the lateral malleolus.
Femoral venous cannulation
While femoral venous puncture is relatively easy and supplies ready access to the right atrium, the use of this approach is relatively unpopular for long-term cannulation because of a higher incidence of thrombosis and sepsis. However, it is a useful site for venous sampling in a patient with collapsed veins. For femoral venous cannulation the skin puncture site is approximately 1 cm medial to the femoral artery and just below the inguinal ligament. After skin puncture the needle is advanced with the syringe at an angle of 30° to the skin, aiming cephalad.
Nerves
The areas of distribution and spinal segments of origin of the cutaneous nerves of the lower limb are shown in Figure 79.17.
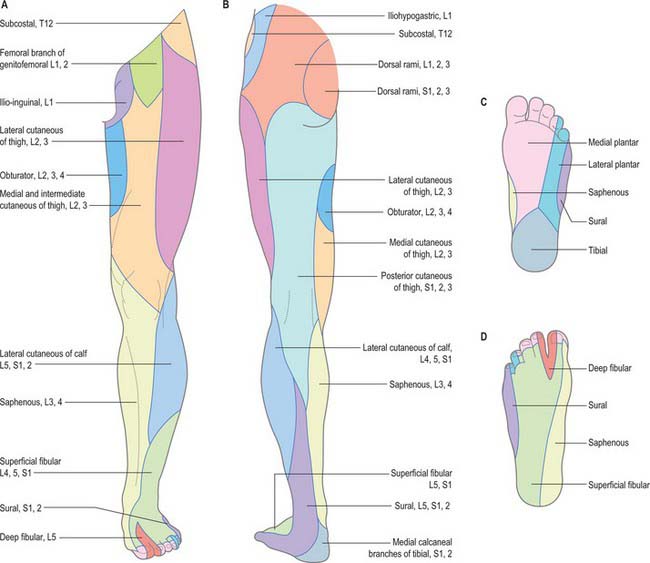
Fig. 79.17 The cutaneous nerves of the lower limb: areas of distribution and spinal segments of origin. A, Anterior aspect; B, posterior aspect; C, sole of foot; D, dorsum of foot.
The surface marking for the femoral nerve in the inguinal region is immediately lateral to the femoral pulse. The surface marking for the course of the saphenous nerve is described with the course of the long saphenous vein (see above).
The course of the sciatic nerve can be represented by a line that starts at a point midway between the posterior superior iliac spine and ischial tuberosity, curves outwards and downwards through a point midway between the greater trochanter and the ischial tuberosity (Fig. 79.18), and then continues vertically downwards in the midline of the posterior aspect of the thigh to the upper angle of the popliteal fossa, where it divides into the tibial and common fibular nerves (if it has not already done so at a higher level).
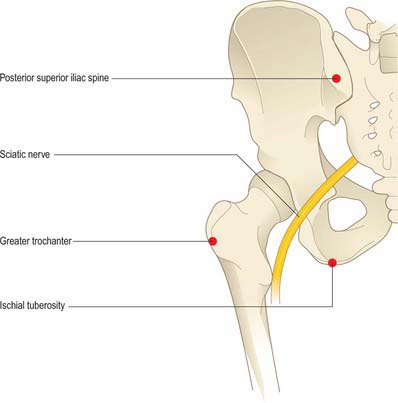
Fig. 79.18 Surface marking of the sciatic nerve. The line of the nerve joins the midpoint between the ischial tuberosity and the posterior superior iliac spine with the midpoint between the ischial tuberosity and the greater trochanter and then continues vertically down the back of the thigh.
The course of the common fibular nerve can be indicated by a line that runs from the upper angle of the popliteal fossa, along the medial side of the tendon of biceps femoris and then curves downwards and forwards around the neck of the fibula. The nerve is palpable medial and, more distally to the tendon of biceps and over the neck of the fibula, although here it is less distinct as it passes deep to the origin of fibularis longus. At the neck of the fibula the nerve is at particular risk of damage either from a tightly applied plaster cast or from a fracture.
The deep fibular nerve starts on the lateral aspect of the neck of the fibula, passes downwards and medially, and rapidly becomes associated with the anterior tibial artery, which it accompanies to the ankle. The superficial fibular nerve also begins on the lateral aspect of the neck of the fibula. It descends to a point on the anterior border of fibularis longus, at the junction of the middle and lower thirds of the leg, where it pierces the deep fascia and divides into medial and lateral branches. The latter gradually diverge as they descend to reach the dorsum of the foot and may be seen if the foot is pulled into maximal plantarflexion and adduction.
With one exception, the cutaneous nerves of the foot are not normally visible. The superficial fibular nerve is frequently seen and palpated over the dorsolateral aspect of the ankle and midfoot when the ankle is plantar flexed and the fourth toe passively flexed. This is particularly true in individuals with little subcutaneous fat. While the lateral branch is often seen, the medial branch is rarely visible. These superficial nerves are at risk from surgery in the anterior ankle region (especially during arthroscopy): they can be identified reliably by passive plantarflexion and inversion of the foot whilst running the blunt end of a ballpoint pen across the anterior ankle. An easily palpable click will localize the nerves, even in patients who are not thin.
Dermatomes
Our knowledge of the extent of individual dermatomes, especially in the limbs, is largely based on clinical evidence. The dermatomes of the lower limb arise from spinal nerves T12 to S3 (Fig 79.19 and 79.20).
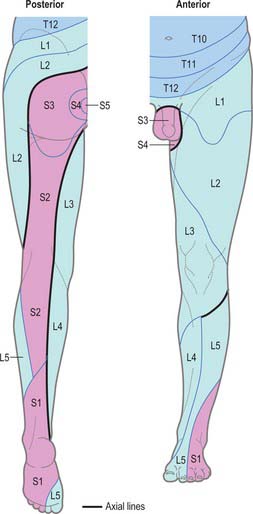
Fig. 79.19 Dermatomes of the lower limb. There is considerable variation and overlap between dermatomes, but the overlap across axial lines (heavy black) is minimal.
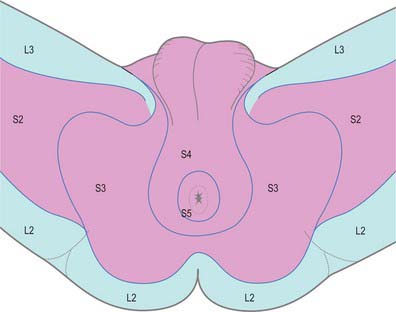
The preaxial border starts near the midpoint of the thigh and descends to the knee. It then curves medially, descending to the medial malleolus and the medial side of the foot and hallux. The postaxial border starts in the gluteal region and descends to the centre of the popliteal fossa, then deviates laterally to the lateral malleolus and the lateral side of the foot. The ventral and dorsal axial lines exhibit corresponding obliquity. The ventral starts proximally at the medial end of the inguinal ligament and descends along the posteromedial aspect of the thigh and leg to end proximal to the heel. The dorsal axial line begins in the lateral gluteal region and descends posterolaterally in the thigh to the knee; it inclines medially and ends proximal to the ankle. Considerable overlap exists between adjacent dermatomes innervated by nerves derived from consecutive spinal cord segments.
Myotomes
The predominant segmental origin of the nerve supply for each of the muscles of the lower limb and for the movements which take place at the joints of the lower limb are summarized in Tables 79.1-79.4.
Reflexes
With the patient supine and the knee supported and partially flexed, the patellar tendon is struck at its midpoint: this should elicit contraction of the quadriceps, which extends the knee.
With the patient supine and the lower limb externally rotated and partially flexed at hip and knee, the foot is passively dorsiflexed to stretch the calcaneal tendon, which is then struck with a percussion hammer. Contraction of the calf muscles plantar flexes the ankle. The reflex can also be examined with the patient kneeling on a chair.
The plantar reflex is a superficial reflex whose elicitation forms an important part of the clinical examination of the central nervous system. With the foot relaxed and warm, the outer edge of the sole is stroked longitudinally with a hard object (traditionally the examiner’s nail or a key). This should elicit flexion of the toes, although the normal adult response varies with the strength of the stimulus. In adults with upper motor neurone lesions, the response includes extension of the great toe (Babinski’s sign).
Nerve blocks
Nerves can be effectively blocked with local anaesthetic injection for surgical or post-injury pain relief. The useful blocks in the lower limb are around the hip, for thigh and knee pain, and around the ankle, for foot surgery. For the deeper nerves around the hip, the use of a nerve stimulator needle is very helpful to localize the nerve precisely before infiltration of local anaesthetic. For example, blockade of the sciatic nerve in the buttock, femoral nerve in the anterior groin, and obturator nerve in the medial groin may be undertaken to provide pain relief for total knee replacement; the tibial nerve at the posteromedial ankle, the sural nerve at the posterolateral ankle and the superficial fibular nerves at the anterior ankle may all be blocked at the ankle to allow ‘awake foot surgery’.
CLINICAL PROCEDURES
Intramuscular injection
Intramuscular injections into the buttock should be avoided to prevent iatrogenic damage to the sciatic nerve. If the buttock is to be used, the safe area is the true upper and outer quadrant, which is identified with the whole buttock exposed. The injection is then given mainly into gluteus medius rather than into gluteus maximus, provided a sufficiently long needle is used: most so-called ‘intramuscular’ injections given into the buttock are actually given into the fat. A safe alternative is to inject into the lateral aspect of the thigh (vastus lateralis).
Joint injection and aspiration
Careful aseptic technique is essential for all joint aspirations and injections.
With the patient lying supine, and after the positions of the femoral artery and the anterior superior iliac spine have been marked out, the needle is introduced anteriorly approximately 5 cm distal to the anterior superior iliac spine and 4 cm lateral to the femoral pulse, and passed posteriorly, a little proximally (cephalad), and medially.
Arthroscopy portals
The placement of portals for arthroscopy is critical, partly to maximize surgical access for visualization and for surgical instruments, but to also avoid damage to structures such as nerves and blood vessels.
Hip arthroscopy is not yet a common procedure but is increasingly being used. A variety of entry portals have been described. The anterolateral portal is sited on the skin approximately 4 cm lateral to the femoral pulse and 4 cm inferior to the inguinal ligament. A needle traversing the skin 30–45° cephalad is passed under X-ray control into the joint. Once the synovial cavity is entered the ‘vacuum’ is lost and the joint can be distracted. Other more lateral portals can be used: the lateral cutaneous nerve of the thigh and the sciatic nerve are potentially at risk.
The knee is the joint most frequently examined in this way. The standard portals are anterior. When the knee is flexed at a right angle, ‘soft triangles’ bordered by the patellar tendon, the femoral condyles and the tibia and anterior horns of the menisci are palpable on either side of the superior third of the patellar tendon. Small ‘stab’ incisions can be made in the apices of these triangular areas at about the level of the inferior pole of the patella for the anterolateral portal, and slightly lower for the anteromedial portal. These portals will allow passage of an arthroscope and instruments, with good access to most of the joint. The fat pad is close by and passage through it will hamper the view and subsequent surgery. The patellar tendon and the infrapatellar branch of the saphenous nerve are at risk from the incisions. The nerve is less vulnerable than the tendon: its position is variable but it usually lies below the appropriate portal sites. However, in the days of open meniscal surgery, the nerve was usually divided and painful neuroma formation was not uncommon.
Posteromedial and posterolateral portals are useful when better access to the posterior knee is required. The saphenous and common fibular nerves respectively are at risk with these approaches, and anatomical knowledge is vital to safe portal placement. Laterally the incision should be anterior to the tendon of biceps, which can easily be palpated. Medially the situation is more difficult because the saphenous nerve and vein run over the medial epicondylar region of the knee, a hand’s breadth posterior to the medial border of the patella. It is essential that sharp incision includes the skin only, and that dissection down to the joint capsule is undertaken bluntly. If the medial meniscus is sutured, the capsule must be exposed before tying off sutures to avoid ensnaring the nerve. In lateral meniscal repair a useful guide to avoid injury to the common fibular nerve is never to allow needles or sutures to pass medial to the tendon of popliteus whilst viewing arthroscopically.
The use of ankle arthroscopy is well established, especially in treating sports-related injuries. Anterior portals are standard. The anteromedial portal can be placed to pass just medial to the tendon of tibialis anterior, in the palpable soft spot. However, this comes close to the long saphenous vein and nerve, and limiting the sharp incision to the skin, followed by blunt deeper dissection, reduces the risk. Alternatively the anteromedial portal can be chosen to pass between the lateral edge of tibialis anterior and extensor hallucis longus. The anterolateral portal is placed with the help of the arthroscope in the joint to check the position of a preliminary needle passed into the joint. The portal should pass lateral to fibularis tertius and extensor digitorum longus. The intermediate dorsal cutaneous branch of the superficial fibular nerve is at risk as it crosses the ankle anterior to the lateral malleolus, and therefore it is wise to ink in the nerves and blood vessels before making any incision. The nerves can be felt at the front of the ankle even in obese patients. They are often seen if the ankle is maximally pulled into plantarflexion and are seen to flick as the barrel of a pen is pulled across the front of the ankle. Posterior ankle arthroscopy is controversial: there is a view that the proximity of the neurovascular bundle (medially) and the sural nerve (laterally) renders it too hazardous. Keeping lateral to the tendon of flexor hallucis will safeguard the medial neurovascular bundle.
Surgical incisions
Hip joint surgery is usually undertaken for paediatric problems, trauma, or arthroplasty in arthritis. Anterior and anterolateral approaches, often used in children, put the lateral cutaneous nerve of the thigh at considerable risk. Even in more lateral approaches, the lateral cutaneous nerve of the thigh and the femoral and sciatic nerves are all at risk through traction. A popular anterolateral approach to the hip joint involves splitting and separating forwards the anterior part of gluteus medius and vastus lateralis as a single sheet of tissue for subsequent reattachment to the greater trochanter. This technique relies on the anatomical continuity of the tissue. If the splitting of gluteus medius is more than a few centimetres superior to the tip of the greater trochanter then the superior gluteal nerve and vessels are at risk, and weakness of hip abduction and a limp may result. In the posterior approach to the hip joint, gluteus maximus is incised in the line of its fibres. This is followed by division of the tendons of the short lateral rotators (piriformis, obturator internus and gemelli) near their trochanteric attachments to reveal the joint capsule. The sciatic nerve is protected by reflecting medially the cut ends of the divided short lateral rotators.
Most open knee surgery can be undertaken through an anterior midline longitudinal incision, which gives good access and means that any future surgery can usually be undertaken via the same wound. New incisions run the risk of skin necrosis and poor wound healing as a consequence of interfering with the cutaneous blood supply. Inevitable interruption of the cutaneous nerves, including the infrapatellar branch of the saphenous nerve, means that there is always numbness lateral to a longitudinal incision.
The extensile approach to the posterior knee is extensive. The key is to expose the sural nerve and short saphenous vein and to trace them proximally. This will lead the surgeon into the popliteal fossa and, after opening the deep fascia, safely to the neurovascular bundle. The wound crosses a flexure crease. A scar perpendicular to the crease might induce a fixed flexion contracture of the joint and therefore, as at the anterior elbow, an S-shaped incision is employed where the transverse segment runs in the line of the flexure crease.
Incisions around the foot and ankle frequently put cutaneous nerves at risk and such an injury can cause a distressing painful neuroma. The sural nerve at the ankle has a notorious tendency to form neuromas, often after repair of a ruptured calcaneal tendon. Bunion surgery is also problematic and can be undertaken through an internervous plane with a dorsomedial incision over the first metatarsophalangeal joint, rather than the traditional dorsal approach.
Cormack GC, Lamberty BGH 1994, see Bibliography.
Crock HV. Atlas of Vascular Anatomy of the Skeleton and Spinal Cord. London: Martin Dunitz, 1996.
Dodd H, Cockett FB. The Pathology and Surgery of the Veins of the Lower Limb, 2nd edn. Edinburgh: Churchill Livingstone, 1976.
Kosinski C. Observations on the superficial venous system of the lower extremity. J Anat. 1926;60:131-142.
Sharrard WJW. The distribution of the permanent paralysis in the lower limb in poliomyelitis; a clinical and pathological study. J Bone Joint Surg Br. 1955;37-B(4):540-558.
Michel Salmon: Anatomic Studies, Book 1. In: Taylor GI, Razaboni RM. Arteries of the Muscles of the Extremities and Trunk. St. Louis: Quality Medical Publishing, 1994.