2 Perspectives on learning
Adult learning; see also andragogy Describes a set of principles, originally described by Knowles in 1984, that differentiate how adult learners differ from children. They include the experience the adult has accumulated, motivation and self-direction, and the interest in solving problems that are relevant to their everyday lives.
Approaches to learning; see also deep learning and surface learning These describe how students approach learning tasks. Surface and deep learning represent two different approaches. A surface approach is characterised by accepting new facts and ideas uncritically and attempting to store them as isolated, unconnected, items (rote learning). Deep learning is characterised by examining new facts and ideas critically, tying them into existing cognitive structures and making numerous links between ideas.
Cognitivism A cognitivist orientation focuses on perception, memory, and meaning. The various cognitive perspectives share two important assumptions: (a) the memory system is an active processor of information and (b) knowledge plays an important role in learning. Learning is seen as reorganizing experience to increase meaning.
Epistemology The theory or science of the method or grounds of knowledge.
Humanist orientation to learning Focuses on human potential for growth and the freedom of individuals to become “what they are capable of becoming.” Theories of self-direction, transformative learning, and adult learning fall within the humanist category.
Lifelong learning An ongoing process through which individuals acquire the knowledge, skills, and values they will need through their life.
Practical theories of learning and teaching These are based on individuals’ experiences, the combination of their formal and informal knowledge, and their values and beliefs. Practical theories strongly determine educational practice.
Self-directed learning Self-directed learning refers to an ongoing process through which individuals identify their learning needs, identify means to meet them, engage in relevant learning activities, and evaluate their progress and achievement in meeting their needs.
Socio-cultural theory Current conceptualisations of socio-cultural theory draw heavily on the work of Vygotsky (1978). A key feature of this emergent view of human development is that higher-order functions develop out of social interaction. Social relationships and culturally constructed artefacts – including language and tools – mediate learning and there is a two-way relationship between culture and individual learning. People learn meanings through activities that take place within individual, social, and institutional relationships.
Tacit learning; see also implicit learning The acquisition of knowledge independently of conscious attempts to learn, and without knowing exactly what has been learnt.
Outline
This chapter presents perspectives on learning selected for their ability to inform practice and research. We use ‘perspectives’ more or less interchangeably with ‘theories’ but prefer the term perspectives because it emphasises that any situation can be viewed from more than one angle; one perspective might be more informative for one purpose while a different perspective might be more informative for another purpose. After a brief overview of how perspectives might be grouped, we present them in the form of a map – far from any definitive ‘truth’, the map is intended to provoke discussion about why a perspective might more appropriately be positioned in one place in the map than another and how it relates to other perspectives. The following perspectives are then presented: Cognitive psychological theory, Experiential learning, Reflective learning, Tacit learning, Adult learning, Self-directed learning (SDL), and Lifelong learning. Social perspectives including Social cognitive theory (SCT) and Socio-cultural theory are introduced, ending the overview with the two main ‘neo-Vygotskian’ socio-cultural perspectives: Activity theory, and Communities of Practice theory. We conclude the chapter by suggesting some implications for both educational practice and research.
Introduction
Medical education is located at the crossroads between medicine and education. Practitioners and scientists from both the biomedical and social science domains contribute to it in the joint pursuit of two goals: to develop and provide an education that effectively prepares medical professionals for their current and future tasks, and to develop an evidence base that can inform and be informed by practice. Understanding learning plays an important role in meeting both of those goals. If we have insight into how medical students, residents, and practising physicians develop the knowledge, skills, and behaviours that allow them to work as professionals, the development of programmes and assessments and the evaluation of their effects will benefit.
In ways that are both explicit and tacit, our understandings of and perspectives on learning inform our practice as educators. They inform the decisions we make about curricula and teaching, the ways we interpret the outcomes of teaching, the candidates we admit to educational programmes, and the questions we ask in research projects. Our perspectives on teaching also affect our views of learning. These perspectives arise from our experience as teachers as well as from formal study. Educators’ deeply held values about teaching and learning translate into “practical theories” (Handal and Lauvas, 1987) that influence how they see their own roles and responsibilities and the roles and responsibilities of their learners.
An understanding of what learning entails contributes significantly to education research as well as practice. It informs the framing of research questions, design of interventions and experiments, and choice of outcome measures. To advance the field of medical education, researchers are encouraged to reflect on their practical theories and place them within a conceptual framework that can build a coherent body of evidence and, eventually, a better understanding of learning itself (Eva and Lingard, 2008; Prideaux and Bligh, 2002). Importantly, given that those involved in medical education range from busy clinicians to phenomenological researchers, there is a rich variety of perspectives on teaching and views on learning from which to choose.
The field of learning is complex and evolving. Beyond the personal and practical understandings discussed earlier, scholars have provided theoretical perspectives that illuminate learning more broadly, and reach far wider than the confines of medical education. Among these are behaviourist, cognitive, and social perspectives, as well as developmental and socio-cultural ones. Perspectives have arisen from the disciplines of psychology, education, sociology, and anthropology. Some overlap with others, which can be confusing but can also provide opportunities for deeper understanding. In this chapter, we discuss some key perspectives on learning. We also explore how such theories illuminate educational practice, and how they can complement each other in guiding understanding. Our two overarching goals are that, in reading and considering the subject matter of this chapter, you will
Orientations to learning
People who come to education from a medical background may at first be perplexed by this emphasis on underpinning theory and even people who come from theory-rich disciplines may be surprised by the variety of theoretical perspectives they encounter in the world of medical education. Psychology is a rich source of educational theory so developments in education have been very closely linked to developments in psychology. Over the last century, psychology has moved first from a dominant behaviourist stance to a cognitive one and then to focus more on situated views of cognition, which accounts for some of the breadth of perspectives. However, psychology is not the only social science that provides perspectives on learning. Wertsch (1991) wrote of the need for other perspectives – notably socio-cultural ones – because psychology has had ‘very little to say about what it means to be human in the modern world (or any other world for that matter)’. No one perspective is inherently ‘better’ than any other, and certainly not just because it is newer, which is why this chapter discusses such a range of them. We do not by any means provide an exhaustive list of perspectives in use within (medical) education but aim to give the reader a broad overview of informative ones.
Behaviourist, cognivitist, social, and humanist orientations
We begin the chapter by outlining some very broad perspectives on learning, which we term ‘orientations’. We have followed the categorisation of Merriam et al (2007), except that we regard constructivism as a broad philosophical position that underpins most contemporary ideas about learning; we devote the section following this one to it in preference to treating it as just one of five orientations to learning.
Constructivism
To understand constructivism, it is necessary to go deeper into the philosophies of knowledge and learning. In the language of philosophy, perspectives on learning differ in their ‘ontologies’ and ‘epistemologies’. As explained by Guba and Lincoln (2005), the study of ontology is concerned with the question ‘What is the form and nature of reality?’ According to them, ‘If a “real” world is assumed, then what can be known about it is “how things really are” and “how things really work”’. ‘Questions, such as those concerning matters of aesthetic or moral significance, fall outside the realm of legitimate scientific enquiry’. That would be described as a ‘positivist’ system of beliefs, which contrasts with a constructivist one. Epistemological questions concern ‘What the nature of the relationship between the knower … and what can be known is’. Guba and Lincoln (2005) go on to show how a positivist ontology leads logically to a positivist epistemology when they argue that ‘If a real reality is assumed, then the posture of the knower must be one of objective detachment or value freedom in order to… discover “how things really are” and “how things really work”’.
Since this book concerns education, we can confine ourselves to epistemology and consider how the different perspectives we discuss view the relationship between the knower and the known. The positivist epistemological perspective in the aforementioned quotations of a “real” reality that can be apprehended through an ‘objective detachment’ is characterised by Guba and Lincoln (2005) as ‘naive realism’. From a positivist standpoint, knowledge is outside the learner; it is value and context-free. In contrast, a constructivist system of beliefs does not see such a distinction between ‘real’ and ‘experienced’ realities because its epistemology is, according to Guba and Lincoln, ‘transactional/subjectivist’. So, the focus is not on knowledge as an absolute external reality, but on its construction by the knower: ‘Realities are apprehensible in the form of multiple, intangible mental constructions, socially and experimentally based, local and specific in nature (although elements are often shared among many individuals and even across cultures), and dependent … on the individual persons or groups holding the constructions’ (Guba and Lincoln, 2005). The knower and the object of their knowing are ‘assumed to be interactively linked’ so their knowledge is ‘literally created’. In an educational context, constructivism can be seen as a process whereby learners actively construct their understandings based on previous experience, knowledge, and their perceptions of the world. Constructivism also contrasts with positivism in attaching more importance to ‘matters of moral and aesthetic significance’; in other words, values and beliefs. A progressive shift towards a more constructivist view of (medical) education explains many of the recent changes in the field and much of the subject matter of this chapter reflects the dominance of a constructivist epistemology of learning.
Two axes for mapping constructivist perspectives
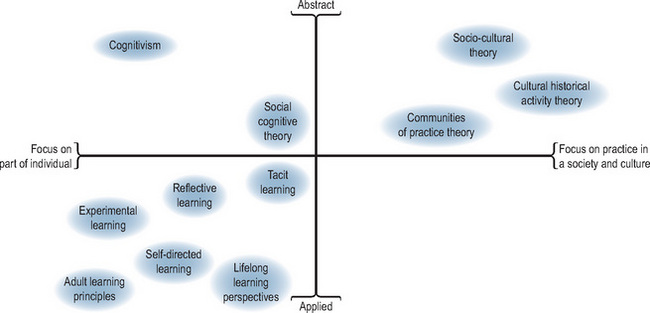
Because it can be difficult to see how different perspectives relate to or differ from each other, we offer two organizing principles to group them. First, the extent to which they focus on individual versus societal/cultural processes; second, the extent to which they provide abstract conceptualisations (AC) versus principles that can be applied directly to practice.
Individual-social axis
Learning can be viewed more as an individual or a collaborative process. Within cognitive psychology, studies of perception, meaning, and memory have focused on the processes developed and used by individual learners. Early cognitivist thinkers focused on individuals’ mental processes in order to understand learning and behaviour. Later thinking stressed the importance of embodiment, according to which cognition depends not just on the brain but also on the body. Metaphors that are in common use reinforce the view of learning as an individual process, notably the acquisition metaphor, from which perspective learning involves the acquisition and accumulation of goods by individuals. In the case of medical education, those ‘goods’ include knowledge, skills, attitudes, values and (more recently) competence. We talk about a person attaining, developing, accruing, and ‘getting a grasp’ of an idea or skill. Once someone has accumulated one of those entities, they can transfer or apply it to a different context and share it with others. As Sfard (1998) pointed out, this metaphor has been so much a part of our thinking that we scarcely noticed it until another metaphor began to emerge. This was the participation metaphor, which represents the other end of the individual-collaborative spectrum. Participation centres on activities and doing. While the acquisition metaphor implies that we can reach the point where we have ‘achieved’ learning, participation is ongoing and continuous. Learning through participation can never be separated from the context in which it occurs. Learning theories from fields such as sociology and anthropology have helped us understand how participation is shaped by societies and cultures. The participation metaphor (also known as the embedding thesis) highlights how important it is that we understand learning and development as situated in a social and physical environment. This perspective opened up the possibility of “cognition extending beyond the boundaries of individual organisms” (Robbins and Aydede, 2009). Research into team functioning and learning, for instance, often incorporates this extension thesis.
Abstract-applied axis
The second organizing principle centres on the extent to which a theory is abstract or applied. Cognitivist or socio-cultural perspectives present quite abstract notions of how people behave, interact, or learn. Based on observation and study, theorists try deductively to identify principles that underlie learning. Other theoretical perspectives are less abstract and more readily applicable; for example, adult learning principles. Some perspectives seem to be so ‘applied’ that they bear hardly any relationship to developed bodies of knowledge and are open to the criticism that they lack a solid theoretical basis (Norman, 1999).
Mapping individual perspectives
Figure 2.1 maps the theoretical perspectives discussed in this chapter to where they sit on the continuum between learning being situated primarily within (parts of) individuals or situated within a society and culture, and on the abstract-applied continuum. Of course, those positions are not fixed. Different people will conceptualise the same perspective in different ways and argue for different positions on the map. Theoretical perspectives are ‘alive’ in the sense that they are continuously being researched, applied, further developed, and extended. The purpose of the map is to indicate that perspectives differ along at least two dimensions and each perspective can be characterised by the two organizing principles we discussed. We hope this insight will help readers understand differences between theoretical perspectives and stimulate them to reflect on their own practical theories of learning.
Individual perspectives on learning and development
Cognitive psychology
Cognitive psychology is the basis for many aspects of (medical) education and this perspective underlies much of the current emphasis on active learning, reflective practice, problem-solving, diagnosis, clinical reasoning, and expertise. The relationship has been a reciprocal one because education research has also refined cognitive theory. As explained earlier, cognitive psychology is concerned with what goes on in learners’ minds and views learning as an active constructive process. To illustrate how cognitive principles apply in practice, we now explain some underlying principles of problem-based learning (PBL), an educational method that has been widely adopted in recent years.
The importance of prior knowledge
Prior knowledge, which provides meaning, context, and a connection for new knowledge, is an important determinant of the new knowledge a learner can master at any moment.
Activation of prior knowledge
For prior knowledge to be used effectively to connect and integrate new knowledge, it must be activated. This activation is brought about by considering relevant aspects of the problem (case); importantly, prior knowledge is activated by the social process of discussion (see Chapter 9 for an explanation of PBL as a small-group learning process) which elicits what each student can draw on to help explain the problem. For example, students may have family members who have experienced a health problem similar to the one under discussion. Discussion draws in their individual experiences and analyses their relevance to the problem under consideration. Similarly, summarizing what has been learnt to date about the problem can activate knowledge.
Elaboration of knowledge
To be effective and available for use, rich knowledge structures need to be developed. Those structures contain knowledge that is connected to many other bits of knowledge. Having a richer network of interconnections creates alternative pathways to stored information such that knowledge is adaptable and flexible. Elaboration can happen in several ways including discussion of the case, sharing past experience, sharing what learners have learned, peer teaching, taking notes, and gaining additional real or simulated experience with patients.
Learning in context
Learning something in a meaningful context enhances a learner’s ability to retrieve it for the solution of future problems. The closer the situation in which it is learnt is to the one in which it will be used, the more readily usable the information will be. So, the meaningful context of PBL problems and their relevance to the real problems of future practice are intended to enhance learning and memory.
Transfer of knowledge
To develop a usable, durable, flexible, and adaptable knowledge base, one must be able to transfer what is learnt in one problem or setting to another problem or setting. While it was once thought that transfer occurred quite readily, it is now clear that both teachers and learners have to encourage transfer actively. Two kinds of transfer have been described: low-road transfer, the product of exposure to and opportunities to practice on multiple examples of a problem, which can happen without explicit awareness; and high road transfer, a more deliberate process in which principles are extracted that can be applied to other relevant situations. Transfer can occur by looking backward, to see what from our previous experience and learning is helpful, or looking forwards, to identify which aspects of a problem may be useful in the future. Learners might need help to develop the habit of identifying salient aspects of problems, rather than just those that are on the surface. Transfer of a concept can be improved by embedding it in a problem, as is the case in PBL, though conventional curricula can also accomplish transfer. The process of looking for underlying concepts and principles can be strengthened by effective tutoring; for example, by encouraging students to compare the current case with others in their experience or think of other examples that reveal similar concepts. Actively rehearsing concepts in the context of a case promotes transfer (Norman, 2009a).
Developing generic problem-solving skills?
While PBL was hailed initially as a means to develop generalised problem-solving skills, subsequent research showed convincingly that a person’s ability to solve a problem is closely related to their knowledge in that specific area. So PBL may only enhance problem-solving skills in so far as it develops learners’ knowledge and critical thinking skills, and their ability to work as part of a social group to accomplish a shared goal.
To round off this review of cognitive perspectives on learning, Box 2.1 lists what Simons et al (2000)label ‘new learning outcomes’, a set of desirable features of learning outcomes, which relate very well to the preceding description of cognitive processes.
Durable: Learning endures over a period of time and is not just for today or tomorrow.
Flexible: Learning can be approached from different perspectives and angles – not tied to just one perspective. Learning should be adaptable to new contexts and changes in contexts. This requires deep learning and internal relational networks (elaborated knowledge).
Functional: Learning (knowledge and skills) should be available when needed (right time, right place)
Meaningful: Deep understanding of a few basic principles with far reaching significance is more important than superficial understanding of many facts that may become obsolete.
Generalisable: Learning is not restricted to one situation but reaches out to other situations.
Application-oriented: people should know the possible applications and conditions of their knowledge and skills.
Experiential learning
From a constructivist standpoint, experiences are pivotal in the development of undergraduate medical students, postgraduate learners, practicing physicians, and other health care professionals. Experiences lie at the heart of participation, and participation, as discussed in relation to Figure 2.1, is central to social and collaborative perspectives on learning. Experiential learning encompasses a range of concepts and has been influenced by educational theorists like Piaget, Lewin, Dewey, and Kolb. Experiential learning starts from the generally accepted notion that an individual’s concepts and behaviours arise from and are adjusted through their life experiences. The work of Kolb offers a way of understanding the cognitive processes that underlie such learning. In his influential 1984 book entitled ‘Experiential Learning: experience as the source of learning and development’, he defines learning as “the process whereby knowledge is created through the transformation of experience” (Kolb, 1984, p. 41). He proposes a four-stage cyclical model of knowledge development that combines the grasping and transformation of experience by individuals. According to Kolb, the first stage of learning starts with a concrete experience (CE), followed by reflection on that experience, leading to the formation of abstract concepts and generalisations regarding the experience, and finally the testing of new or adjusted concepts through new experience. This leads again to CE, which closes the learning cycle. Honey and Mumford (1986) slightly adapted this learning cycle. According to them, learners move from having an experience to reviewing the experience, to drawing conclusions based on the experience, and to planning the next steps. Kolb acknowledged that learning does not necessarily start with an experience and that the cycle may be entered at other stages as well (Kolb, 1984). Subsequent developments of experiential learning theory have paid less attention to the cyclical aspect.
Meanwhile, Kolb and others focused more on the two opposed modes of grasping and transforming experience (Kolb et al, 2001). CE and AC were the two modes of grasping experience whilst reflective observation (RO) and active experimentation (AE) were the two modes of transforming experience. According to Kolb, learners have a preference for a certain approach to acquiring experience and transforming it, which he called their learning style. This underlies the Learning Style Inventory (LSI) (Kolb, 2005). The LSI identifies four types of learners: convergers (AE-AC), accommodators (AE-CE), assimilators (RO-AC), and divergers (RO-CE). The LSI was designed to determine an individual’s learning preference. It was one of the first learning style questionnaires developed, and is used widely, including in the medical domain (Curry, 1999). There is, however, considerable criticism of its use and value (Norman, 2009b). According to Coffield and colleagues, the reliability of the LSI has not been established and it has low validity as a predictive test. The implications for teaching have been drawn logically from the theory rather than from research findings and there is no evidence that ‘matching’ education with preferred learning styles improves performance (Coffield et al, 2004, https://crm.lsnlearning.org.uk/user/order.aspx?code=041543). Moreover, Kolb’s underlying theory of the four-stage experiential learning model has received much criticism on very diverse grounds (see Greenaway, 2009, http://reviewing.co.uk/research/experiential.learning.htm#styles). The idea that learning takes the form of a neat four-stage cycle is challenged. For instance, Schlesinger argues that the separate elements of the cycle may be relevant, but that in practice learning is much more fragmented and chaotic (Cheetham and Chivers, 2005; Schlesinger, 1996). Bleakley pointed to the paradox of a model of ‘experience’ that neglects the social context of that experience and its influence on what is learnt from the experience (Bleakley, 2006). Nonetheless, researchers have found Kolb’s experiential learning theory useful to explain a number of phenomena related to learning in medical workplaces (Chung et al, 2003; Smith et al, 2004; White and Anderson, 1995).
Reflective learning
Reflective learning is also based in and on experience. Reflection as a means of learning has been discussed by educators as early as 1933 (Dewey, 1991), when Dewey described learning as “active, persistent and careful consideration of any belief or supposed form of knowledge in the light of the grounds that support it and the further conclusion to which it tends” (p. 9). Reflection and reflective practice have moved into a more visible and central position in definitions of competence (Epstein and Hundert, 2002), and are clearly stated to be elements of learning in the activities of such bodies as the Royal College of Physicians and Surgeons of Canada and the General Medical Council of the United Kingdom, among others. Undergraduate pre-licensure medical education programmes require learners to keep portfolios to serve not only as evidence of their experiences but also as a basis for demonstrating the ability to reflect on and synthesise experience.
While reflective practice cannot strictly be said to be a discrete perspective, it incorporates a number of cognitive theoretical constructs and its potential effectiveness as a way of learning can be highlighted through exploration of these. Reflection, as defined by Boud et al (1985), is the process by which we examine our experiences in order to learn from them. This examination involves returning to experience in order to re-evaluate it and glean learning that may affect our predispositions and action in the future. Others describe it as the process of turning something over in our minds to frame a problem or shape a solution in an unstructured situation (Moon, 1999). Finally, reflection has been conceptualised as a process whereby new learning is assimilated into our cognitive structures through becoming part of our existing knowledge and skills, attitudes, beliefs, and values (Moon, 1999). Each of these definitions emphasises different aspects of reflection, which include critical thinking as well as personal reflection and integration of learning.
Generally, reflection as a method of learning is conceptualised as an interactive set of activities, whereby we are prompted, either deliberately or unexpectedly, to return to our experience to re-examine it and learn from it. Kolb (1984) described reflection as an integral part of a cycle of learning from experience. Following a study of several professions, Schön too described an interactive process, which he depicted as follows (Schön, 1987). He described professionals’ ‘knowing-in-action’ as their accumulated body of knowledge and skills are gained through formal and informal learning and through experience, which they apply to framing, identifying, and addressing the problems of authentic practice. When professionals encounter a ‘surprise’ a process of ‘reflection-in-action’ ensues. In this period of ‘thinking on one’s feet’, solutions may be considered and rejected which may lead to a slightly altered or new course of action. The final stage in the iterative process involves ‘reflection-on-action’ or returning to the experience to evaluate its outcomes and learn from it. New learning can then be incorporated into professional ‘knowing in action’ so that it is altered by each learning experience.
Theoretically, reflection has been proposed as an active approach to learning which can (a) add to one’s knowing-in-action, (b) surface assumptions and biases that may influence one’s perceptions, (c) promote deep learning of new concepts, (d) help in the framing of difficult complex problems, (e) assist in integration of effective experiences, (f) facilitate the acceptance of feedback, and (g) help connect one’s work and learning to a broader context. Above all, it seems to hold potential for practitioners to become more self-aware, in order to better develop as balanced professionals, and to be able to think critically about both the scientific nature of their work and the nature and meaning of their experience. Such self-awareness can assist in self-regulation, and holds potential for professionals to uncover the tacit knowledge and understanding that applies in their practice and can be shared with others.
Although the evidence for its existence and any effects on learning is dispersed in the health professions education literature, a recent systematic review of the literature for the years 1994–2005 (Mann et al, 2009) confirmed its existence as a strategy employed by physicians, nurses, and other health professionals as well as students. Analyses of the structure of this activity (Mamede and Schmidt, 2004, 2005) revealed a five-factor structure consisting of openness to reflection, deliberate induction, and deliberate deduction, testing, and meta-reasoning. Reflection appears to be linked to learning and positively associated with deep learning across several studies. While it appears that some individuals are more naturally inclined to reflect than others, there is also evidence that the skills of reflection can be developed through practice, feedback, and supervision (Mann et al, 2009). It also seems that reflection can be encouraged in some contexts but discouraged in others. More recently, the literature has suggested that, at least in resident learners, a reflective approach may reduce diagnostic errors in complex problems (Mamede et al, 2008). Lastly, reflection seems to be an integral aspect of practice in high-performing physicians, and a critical process to enable acceptance and use of feedback on performance (Sargeant et al, 2006, 2009b).
The aspect of reflection to which Schön paid most attention was ‘reflection on experience’. More recently, however, scholars have tried to theorise ‘reflection-in-action’, which represents the ongoing minute-to-minute monitoring of our performance; they have posited that it is a critical element of self-assessment and self-monitoring (Eva and Regehr, 2007; Moulton et al, 2007).
Attempts to assess the presence of reflective capability and reflective practice have been reported in the literature. These reports have taken two directions: (a) the development of quantitative, self-report questionnaires completed by learners and practitioners and (b) the development of methods to assess the products of reflection, such as journals and reflections on experience. Although several have been reported, two scales have emerged in medical education, for which information about development and psychometric properties are available. These are the Reflection in Learning Scale (RLS) (Sobral, 2005), and the Groningen Reflection Assessment Scale (GRAS) (Aukes et al, 2007).
The RLS is a 14-item scale, requiring responses on a Likert-type scale, designed to measure students’ self-reported use of reflection in their learning. It has high internal consistency (α = 0.84) and test–retest stability (α = 0.86); it has also shown positive statistically significant relationships with measures of deep learning (Sobral, 2001). The GRAS is a 23-item scale, also using Likert Scale responses, developed to measure personal reflection ability in medical students. Developed from a theoretical and empirical base, the scale had satisfactory psychometric properties (α = 0.76), and content validity. A factor analysis led the authors to conclude that the scale measures a single underlying construct, with three related aspects: self-reflection; empathetic reflection; and reflective communication. Both of these scales appear to be easy to administer and score and offer potential means of assessing students’ level of and growth in reflective ability.
Measurement of reflective ability from writing, such as in journals or narrative accounts of experience, seems also to be possible. Reports of such assessments have generally come from the nursing and health professions literature; generally, they are based on criteria drawn from models of reflection, such as those by Boud et al (1985) or Mezirow (1991). These models categorise reflection in terms of both the processes involved and the depth of reflection achieved. Difficulties with inter-rater agreement and coding have been reported; nevertheless, it appears that acceptable consistency can be achieved.
Despite challenges in teaching and modelling reflection in the professional context, there is increasing support for its use to promote professional development, deepen learning, and encourage development of habits of mind for future practice. Reflective learning is not, however, without its critics, nor is it without its challenges within the professional context (Boud and Walker, 2002). Indeed, concerns have been raised about the potential for creating a ‘ritualised’ form of reflection. Coulehan and Williams (2001) described a non-reflective professionalism in which individuals were unable to see gaps that existed between their espoused ways of behaving and their professional behaviour in action. Further, as the tendency to be reflective varies across individuals, there are some who find reflection an artificial and unhelpful process (Sargeant et al, 2009a,b). Others express concern about the burden of keeping reflective journals, some seeing reflective writing as redundant (Grant et al, 2006). Concerns are expressed about the assessment of reflection, particularly the validity of written reflective material submitted for assessment.
Tacit learning
In contrast to the ‘formal learning’ that is emphasised by official curricula, much important learning results from everyday activities. This ‘informal learning’ contributes ‘tacit knowledge’, which accumulates without awareness and tends to be regarded as things a practitioner “just knows” (Eraut, 2000). As practitioners develop expertise, tacit knowledge of how to do things and which actions to apply in which situations frees their cognitive resources to frame and solve problems. Their tacit knowledge, however, is difficult to articulate, which means that they are more likely to pass on explicit aspects of their knowledge when they ‘teach’. That emphasis on the explicit rather than the tacit is strongly reinforced by outcome-based curricula, particularly ones that codify professional expertise as competencies (Chapter 6).
Constructivism’s acknowledgement that we learn experientially from daily activities, in contrast to positivism’s preoccupation with the codified knowledge that learners acquire as a result of teaching, has made it possible to give more prominence to tacit learning.
Tacit as it may be, this type of knowledge affects our expectations and the way we frame and perceive events, which has very important implications. Many would agree that professional education is in large part a process of socialisation, which means internalising the knowledge structures, routines, norms, expectations, attitudes, and values of the profession. Those matters may be explicitly taught, but much of what is learnt about them is tacit. Moreover, tacit learning may actually be in opposition to explicit teaching. Hafferty and Frank (1994) described how the “hidden curriculum” could directly oppose explicitly espoused values such as patient-centredness and ethical practice. Coulehan and Williams (2001), describing a conflict between tacit learning and stated values, elicited three types of response: detachment, in which affective aspects of activity become distanced and competence comes to be viewed as objective and technical; entitlement, in which students come to believe that, in return for their hard work, they are entitled to prestige, money, and power as well as respect for the value of their work; and finally, a non-reflective professionalism, where professionals become unaware of the gap between those values they espouse and those they enact in their practice. Coulehan and Williams went on to describe ways that learners might resolve the conflict experienced. The first is a conflating of values, in which individuals come to believe that the detachment and objectivity, which protects them, is actually best for their patients; deflating values, in which they may become cynical and lower their expectations of themselves and of others; and a positive one in which some people seem to have a natural immunity to these responses and hold on to their values. The latter response has been associated with being female, being older or more mature, and holding traditional religious or spiritual values.
Adult learning, self-directed learning, and lifelong learning
Perhaps the most strongly espoused perspectives on professional development and practice at the present time are (1) adult learning principles; (2) SDL; and (3) lifelong learning. In contrast to most perspectives discussed so far, these are ‘principles’ in that they are couched more in terms of how learning and teaching should be than how they actually are. So, adult learning principles, SDL, and lifelong learning are prescriptive rather than descriptive. We now examine how they relate to the perspectives discussed earlier.
Adult learning principles
At every level of the medical education continuum, the term “adult learners” is used to justify the design of educational experiences, expectations of learners, and the way learners are expected to approach their education. In fact, the term is so embedded in our conversation that our tacit understandings of what we mean by it are rarely shared or examined.
Adult learning principles were first discussed in the educational literature by Knowles (1984), who elucidated them as a means of explaining why andragogy, or the science of teaching adults, was different from pedagogy, or teaching children. Knowles outlined the following principles to describe adult learners, which he saw as fundamental to programme design.
Other writers have studied adult learners and described similar principles (Merriam, 2001), which have guided the design of curricula in many fields, including the education of health professionals other than doctors. The principles imply that adults come to learning experiences with a rich array of experiences and learning skills and can use those experiences to help them navigate new situations. Despite their widespread and continued incorporation into medical education curricula, adult learning principles have not proved as useful in explaining and predicting behaviour as was hoped. They apply, moreover, to teaching and learning in childhood as well as adulthood: an observation that Knowles ultimately acknowledged. The validity of individual tenets of this approach has been questioned both theoretically and empirically. Critics have noted that the model assumes education to be value-neutral and all learners to look the same. Although the relevance of learning related to individuals’ daily lives and roles is included in the model, the relationships between individuals and the societal context of their learning is ignored. Lastly, critics have asserted that the model reproduces society’s inequities. In the medical education literature, Norman (1999) described the adult learner as a “mythical species” and the assumptions as largely untested. Norman suggested the assumptions may be more a product of the environment in which adults find themselves than any fundamental difference in how adults and children learn. Relatively little empirical work has been conducted on the model and its assumptions, which therefore remain to be directly validated.
Criticisms notwithstanding, the principles of adult learning can be useful when planning learning, particularly because they focus on strengthening learners’ agency in teacher–learner relationships. They align with a cognitive perspective, which sees learners’ prior experiences as giving meaning to new information, and emphasises that prior learning becomes a powerful resource for new learning when it is activated. The adults who constitute, for example, a PBL group will collectively have accumulated very significant prior experience, both in the domain they are learning about and their learning skills. Relevance to authentic problems is another commonality between adult learning principles and a cognitive perspective. Practitioners participating in a continuing education programme, for example, will have an understanding of the problems of practice that helps them see some experiences as more relevant than others. Regarding learners as intrinsically motivated is also important, though learners respond to a mixture of intrinsic and extrinsic influences (Misch, 2002). Bandura describes extrinsic motivation as most powerful early in learning; intrinsic motivation increases once learners reach a level of knowledge and that makes an activity rewarding in its own right (Bandura, 1986).
In addition to the cognitive perspective, adult learning principles are grounded in the humanist perspective in that adults are seen as actively seeking out experiences that contribute to and reflect their ongoing development. Adult learning principles are underpinned by constructivism, in that they see experience as both a resource for and stimulus for learning, and imply that an adult’s work is to understand the important meanings of their society.
Self-directed learning
Becoming a self-directed learner is widely regarded as fundamental to self-regulation, in turn a sine qua non of professional practice. So, SDL forms the basis for some widespread approaches to designing medical education. PBL as a teaching–learning method explicitly incorporates the goals of self-direction in encouraging learners to determine both ‘what’ and ‘how’ to learn. Those who classify SDL as a theoretical orientation (Merriam et al, 2007) classify it as one of the humanist group; so it is a perspective that views learning as a process of human growth and development. Learning, therefore, is progression toward a fully developed ‘self-actualised’ self (Maslow, 1970). Transformational learning is central to SDL, requiring a capacity for critical reflection and knowing oneself as a prerequisite for autonomy (Mezirow, 1991).
Published literature has viewed SDL from two quite distinct points of view. The first sees self-directedness as a personal attribute, an attitudinal disposition that is reflected in observable behaviours. We describe as self-directed those individuals who recognise learning needs or interests, pursue them, access the requisite resources, and evaluate their progress. Those individuals strive for personal growth and autonomy. From that viewpoint, many different traits contribute to self-directedness. The second view is of self-direction as a set of skills that can be developed through experience and practice. These skills include the ability to identify one’s learning needs, set goals for learning, undertake learning, and evaluate the outcomes. Notwithstanding the motivation to be self-directed, the skills are separate, not necessarily inherent, and needing to be learned and practiced. The two viewpoints imply somewhat different educational approaches, and have stimulated different research questions. The two approaches have been brought together in a model of ‘self-direction in learning’, according to which self-direction comprises both instructional processes and learner attributes, and is undergirded by personal responsibility for learning (Brockett and Hiemstra, 1991).
As a guiding principle for curriculum design and a perspective in its own right, SDL has not had an easy path. Many learning approaches of the past have employed a transmission approach to learning, which relies on two main means of teaching: the first is a formal, didactic approach, where the content of the discipline is transmitted to upcoming generations, and the second is an apprenticeship approach, where the learner is placed in an authentic clinical setting, to work with an experienced practitioner or ‘master’ and where learning has both formal and large informal components. Opportunities to be self-directed are limited by the sheer volume of knowledge and skill that are required, which drives learners and focuses their attention on what they must master. In addition to these constraints, we have also learnt that self-direction and the demonstration of requisite skills do not generalise consistently across fields. One may be very self-directed in a field where one has experience, yet require considerable guidance and support when encountering new learning challenges. This has been attributed both to misunderstanding what is actually meant by self-direction and to a lack of clarity about the processes and goals of teaching and learning, a difficulty described extremely well by Miflin et al (1999) in relation to pre-licensure medical students entering a PBL self-directed curriculum.
Measuring self-direction has proved difficult; however, two widely used scales with known psychometric properties have been developed: The Self-Directed Learning Readiness Scale (SDLRS) (Guglielmino, 1997) and the Oddi Continuing Learning Inventory (OCLI) (Oddi et al, 1990). The 54-item SDLRS was developed to assess the degree to which people perceived themselves as possessing skills and attitudes conventionally associated with SDL. The scale has several factors: self-concept as an effective learner; initiative and independence in learning; acceptance of responsibility for learning; love of learning; creativity; future orientation; and ability to use basic study and problem-solving skills. The OCLI is a 26-item scale, developed to identify clusters of personality characteristics that relate to initiative and persistence in learning over time. The four main clusters include self-confidence; the ability to work independently and through involvement with others; avid reading; and the ability to be self-regulating. It is of note that both scales include both predispositions to self-direction and the skills to put it into practice. Also, in measuring individuals’ ability to be self-directing, these approaches tend to ignore the impact of social environments on self-directedness. As Norman suggested with respect to adult learning principles, a person’s self-directedness may be a product of the environment in which people find themselves rather than any fundamental difference between individuals. Research in this area has been complicated by the co-existence of different perspectives and challenges in reaching common operational definitions. Yet self-direction remains a deeply valued goal and tenet of the profession and a critically important attribute to identify educational needs and keep up to date over a lifetime of practice.
Viewing SDL as a set of skills that must be learnt has several implications for learning: As with other skills, those that constitute effective SDL can be improved through repeated practice with feedback; the feedback must target not only content but also the SDL process the learner has employed; learners will exhibit less self-direction and need more direction and support when they engage in new educational experiences. It is also important to remember that SDL does not mean behaving completely independently; an important part of self-direction may be choosing a mix of learning methods including formal didactic sessions. In 1989, a landmark study in continuing education was published, entitled ‘Change and Learning in the Lives of Physicians’ (Fox et al, 1989). The ‘Change Study’ as it came to be known involved interviews with 336 physicians, who identified more than 770 changes they had made in their professional practice over the previous year. These changes and in-depth analysis of them generated a model of learning and change that has stimulated much subsequent research. At the core of the model is the physician’s self-direction, a trigger that identifies the learning needs and the processes the individual uses to specify the need. The model also identified the processes of undertaking new learning and incorporating it into practice. SDL, however, is much more than a set of behaviours. To be effective, self-directed learners must have a well-developed reflective capacity and ability to assess or monitor themselves (Eva and Regehr, 2007).
Lifelong learning
Entering a profession where knowledge and skills expand and change at lightning speed impels a commitment to learning across one’s entire professional lifetime. Not so many years ago, the belief was still held that medical education could impart to graduating physicians all there was to know about medicine, a store of knowledge and skills that would last them from their launch into professional practice until their retirement, at which time their fund of knowledge might also be no longer very useful. Who could have foreseen the gains that have revolutionised medicine and science and therefore required huge ongoing learning and change on the part of the physicians?
Many examples of lifelong learning exist both inside and outside medical education. A particular example of lifelong, self-directed medical learning may be found in the Canadian Practice-Based Small Group Learning (PBSGL) programme (Premi et al, 1994), which began under the leadership of John Premi. PBSGL was first developed to mirror PBL but adapted to consider authentic practice situations rather than hypothetical scenarios. Members of a PBSGL group meet regularly, often for well over a decade, to work on cases and learning resources relating to a problem-oriented curriculum developed by The Foundation for Medical Practice. Each group selects modules that its members believe best meet their learning needs and learn around both those cases and patients under their individual care, sharing information and understanding through discussion. This group learning, which has been shown to improve patient outcomes (Herbert et al, 2004), is an exemplar of how a community of practice can incorporate both self-directed and lifelong learning.
While self-direction and lifelong learning are separate constructs, they often come together in such activities as noted above (Candy, 1991). Lifelong learning is a broader concept, of which self-direction is an important part. Longworth and Davies (1996) have defined it as follows: the development of human potential through a continuously supportive process which stimulates and empowers individuals to acquire the knowledge, values, and skills and understanding they will require throughout their lifetimes and apply them with confidence, creativity, and enjoyment in all roles, circumstances, and environments (p. 22). These authors have also described the skills required for lifelong learning; these skills, while not outlined with medicine in mind, describe well the skills required by practicing professionals (Box 2.2).
Researchers have reported the psychometric properties of a scale to measure lifelong learning (Hojat et al, 2009), which they define as: “A set of self initiated activities and information-seeking skills with sustained motivation to learn and the ability to recognise one’s own learning needs” (p. 1066). In a recent study to validate this Jefferson Scale of Physician Lifelong Learning, the authors found empirical support for lifelong learning as a multi-factorial trait. Three factors were identified in practicing physicians’ and academic clinicians’ responses: learning beliefs and motivation; attention to learning opportunities; and technical skills in seeking information. These three factors are conceptually congruent with those described by others. The scale itself was highly reliable and correlated positively with indicators of learning motivation. Ratings correlated positively with medical school rank and indicators of professional achievement.
Social perspectives
One of the strongest recent forces in learning theory has been the rise of social perspectives on learning. These include SCT and socio-cultural theory, including two ‘neo-Vygotskian’ socio-cultural perspectives: Activity theory and Communities of Practice theory.
Social cognitive theory
SCT, as described by Bandura (1986), was based on his earlier social learning theory. It unites two important theoretical perspectives: one that can be traced back to behaviourism and that emphasises the influence of the external environment on our learning and change; and cognitivism, which focuses on the processes of information gathering, processing, cognition and memory, and how they guide learning and function. Bandura labelled the theory as social, acknowledging the social origins of thought and action; the cognitive element acknowledges that thought processes mediate motivation, affect, and action.
SCT describes human behaviour and function as resulting from a dynamic, triadic, reciprocal determinism, a continuous relationship between and among the individual, the individual’s actions, and the environment. Individuals bring their background, beliefs, skills, knowledge, and personal attributes to every interaction with the environment, and their behaviour is affected by factors in the environment, which influence and interact with their individual goals. The individual also acts on the environment, and thus both affects the environment and receives feedback from it. According to Bandura (1986, 2001) individuals have basic capabilities, which have implications for both teaching and learning. These include
These six basic capabilities are profoundly important in guiding teaching and learning. They validate and align with the powerful assumptions that professionals have an ability to remain competent; learn from experience; and understand the context of their work, and the limits of their knowledge and skills. The ability to set goals for themselves and plan, implement, and evaluate progress towards those goals provides a basis for self-directed lifelong learning.
A central concept in SCT is self-efficacy. Perceived self-efficacy is people’s belief in their abilities to arrive at certain attainments (Bandura, 1997). Self-efficacy is not a global trait; it is linked to distinct areas of function. For example, a surgeon might have a high sense of efficacy in relation to surgical abilities, but a low sense of efficacy with regard to sports ability. Efficacy beliefs have been shown to impact not only on behaviour but also on goals and aspirations, and the opportunities and barriers individuals see in their environments (Bandura, 2001). They influence (a) The courses and actions people choose to pursue; (b) the challenges and goals they see for themselves and their levels of commitment to them; (c) how much effort they put forth; (d) how long they persevere in the face of barriers; (e) their resilience to adversity; (f) the quality of their emotional life, particularly in response to challenging environment; (g) the life choices they make; and (h) what they can achieve.
Perceived self-efficacy arises from four major sources. They are (a) interactive mastery experiences that give strong indicators of capability; (b) vicarious experiences that are gained from observing others and making comparisons with oneself; (c) verbal persuasion and other social influences on how individuals see themselves; and (d) physiological and affective states that provide feedback on how vulnerable or capable individuals are. For these sources of information to affect efficacy perceptions, they must be integrated, interpreted, and influenced by many personal, social, and situational factors. Generally, the most powerful efficacy information comes from interactive experiences; the other sources of information tend to exert influence in descending order. With respect to vicarious learning, role-modelling is a powerful influence on efficacy beliefs.
Feedback is also central to Bandura’s understanding of learning. According to Bandura, the provision of feedback both speeds up learning and increases accuracy. It also increases the level of goal that individuals set for themselves and their level of goal achievement. The provision of feedback has been a much discussed element of medical education’s teaching and learning repertoire for a very long time. Originally it was understood through the behaviourist lens and was understood to affect behaviour through the rewards, reinforcements, or punishments, which followed learners’ responses. Learners were understood to respond by improving or increasing certain behaviours and decreasing or stopping others. The same techniques were involved in shaping behaviour.
Not only does feedback as described by Bandura have a behaviourist element, but it is also mediated cognitively by learners who receive it under the influence of their prior experience, goals, attitudes, values, and perceptions. It is also affected by learners’ contexts and interactions with those contexts. A recent definition follows: “Feedback is conceptualised as information provided by an agent (e.g. teacher, parent, book, parent, self, experience) regarding aspects of one’s performance” (Hattie and Timperley, 2007). As noted, SCT views individuals as able to set goals and monitor their progress toward those goals. Key to being able to judge progress is receiving feedback about performance on a particular task – feedback that can help an individual reduce the gap between their current level of performance and their desired goal. Learners can benefit from feedback not only on their performance of a task but also on the processes they used in executing the task and they can develop improved strategies for self-monitoring and for error detection and error correction. Feedback is also integrally related to development of self-efficacy, which in turn improves learners’ ability to seek out feedback and improve performance further. Clear goals and expectations are essential to guide learners in achieving desired levels of performance and achieving their own goals. Maximally effective feedback is related to the goals; in fact feedback that is unrelated to goals can readily be dismissed (Hattie and Timperly, 2007).
Socio-cultural theory
Socio-cultural theory had its origins in the first half of the twentieth century in the work of the Russian scholar Vygotsky, though it was considerably later that his work was translated into English and became more widely known (Wells, 1999). There are other terms to describe this theoretical orientation, which emphasise its historical dimension as well as its social and cultural ones. Wertsch (1991) characterised socio-cultural theory as concerning the diversity of different people’s processes of learning and development, in contrast to the preoccupation of other theories of learning with ‘universalism’. So, subject matter and educational processes are not uniform but as diverse as the people who learn. Social relationships and culturally constructed artefacts – including language and tools – mediate learning and there is a two-way relationship between culture and individual learning. People learn meanings through activities that take place within individual, social, and institutional relationships. People’s understandings, their actions, and the artefacts they use are both shaped by, and shape, the contexts and cultures in which they learn (Lantolf and Thorne, 2006). Learning, from a socio-cultural perspective, is transactional. So, socio-cultural theory makes it possible to consider the development and functioning of the mind without divorcing it from its social context. Vygotsky’s claim that higher mental functioning is rooted in social life is rooted in Marxist theory – so, both the origins of socio-cultural theory and the long delay in it impacting on western thinking can be attributed to Russian communism (Wertsch, 1991).
Wertsch (1991) distinguished a socio-cultural perspective, which puts learners’ actions at the heart of learning, from a positivist/behaviourist system of beliefs, which treats individuals as passive recipients of information provided by their learning environments. In contrast to the latter perspective, socio-cultural theory treats knowledge as dependent on the knower and the cultural conditions under which it is developed and used. It is also to be distinguished from cognitive learning perspectives, linked to the metaphor of ‘the mind as computer’, which focus on the individual and treat the environment as a relatively inert source of material for the mind to work on. Socio-cultural theory differs from SCT (both, confusingly, can be abbreviated to SCT) in the extent to which it locates learning outside the individual mind in language usage, interpersonal interactions, institutions, cultures, and the legacy of history. Socio-cultural theory can be best understood by considering: mind, knowledge and meaning; mediation of learning; action; context; culture; and the dynamics of learning.
Mind, knowledge, and learning
From a socio-cultural perspective, the development and higher mental functioning of individuals is inseparable from the social milieu in which they take place and the activities that take place there. Relationships and culturally constructed artefacts (including language) play a central role in organising learning. Knowledge is not something fixed or autonomous, and it is not contained wholly within the minds of individual people; it is ‘emergently constructed and reconstructed between participants in specific situated activities using the cultural activities at their disposal as they work towards the collaborative achievement of a goal’ (Wells, 1999).
Mediation of learning
Vygotsky proposed that sign systems (notably language) and material artefacts (including works of art, legal codes, models, and theories that are created with the use of the primary artefacts) ‘mediate’ learning. Language and those artefacts both constitute, and are constituted by, culture.
Action
The actions of learners and other people in their social milieu, which are mediated by language and the artefacts mentioned above as well as culturally determined practices, have a central place in socio-cultural theory. Action can be conceived of as goal-directed, joint activity – which fits closely the participation metaphor introduced earlier (Sfard, 1998). Action is both moderated by, and moderates, the cultural, institutional, and historical context in which it is situated.
Context
Learning, from a socio-cultural perspective, is inseparably linked to the specific context in which it takes place. This attribute, called the ‘situatedness’ of learning, predicts that the way tasks are performed in any context determines what is learnt there.
Culture
This has been described as ‘an objective force that infuses social relationships and the historically developed use of artefacts’ (Lantolf and Thorne, 2006). Within a culture, values that are displayed in social practice are rooted in the history of that culture, and language usage is the most tangible characteristic of any particular culture.
The dynamics of learning
The preceding paragraphs illustrate the dynamic, interactional nature of learning according to socio-cultural theory. Each component of the theory is dynamically linked to each of the other components in a way that has been described as interdependent and mutually constitutive. Wells goes on to write of the ‘triple transformation’; of the object or situation towards which an activity is directed; of the ability to participate and thus of the knowledgeable skills of those involved; and of the cultural artefacts and practices that are drawn upon to mediate the activity (Wells, 1999). For the learner, mastering ways of speaking, thinking, and acting in a particular practice are fundamental to cognitive development. Medical schools, postgraduate medical education institutions, and individual workplaces can be seen as places where interactions among people and between people and cultural artefacts must be systematically structured to promote learning.
Neo-Vygotskian perspectives
An individual in dynamic interaction with their social milieu is clearly seen in two socio-cultural perspectives that are influential in twenty-first century education theory. The first is cultural historical activity theory; the second is communities of practice theory.
Activity theory
Vygotsky’s collaborator Leontiev developed socio-cultural theory’s central focus on human action into activity theory. Now, activity theory is most closely associated with the name of Yrjö Engeström, a contemporary Finnish scholar, who expounds ‘third generation’ activity theory. This broadens and deepens the scope of previous writing to consider more complex activity systems and highly subjective issues such as emotion, embodiment, identity, and moral commitment (Engeström, 2009).
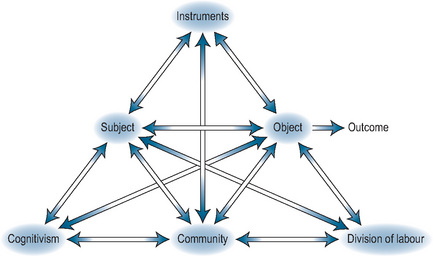
Activity theory locates the agency and learning of individuals or groups of individuals within social systems, operating within social contexts. Activity systems are collective and social in nature. Figure 2.2 shows the conventional representation of such a system and this description follows the account of Tsui et al (2009). Actions within activity systems are directed towards some specific object or goal. Those actions are performed by one or more subjects and mediated by cultural tools, language, behaviours, and physical artefacts. Activity systems are embedded within communities, whose rules and division of labour influence their outcomes. From a learning perspective, the human mind develops as a result of interactions between individual people and cultural tools. Activity is transformational because it mediates between individuals and their social worlds. Collective and individual learning are bound together by activity. ‘Expansive learning’, an important concept in activity theory, results from interactions and ‘contradictions’ between activity systems. According to this perspective, learning is open-ended, transformative, and innovative. Activity theory’s strength is the way it locates individual agency within whole social systems, with a reciprocal dynamic between individual people and the systems of which they are part.
Communities of practice (situated learning) theory
If similarities between the various strands of socio-cultural theory reside in their common perspectives on mind, mediation, action, context, culture, and the dynamics of learning (p. 33), differences between them reside in their different ‘units of analysis’, which can range from individual peoples’ utterances – as in discourse analysis – to the functioning of whole social communities. Much early socio-cultural scholarship, such as Vygotsky’s interest in how social interaction could draw a learner into their ‘zone of proximal development’, took interactions at the level of teacher and pupil as the unit of analysis. More recent work has been at a more communal level, examining the relationship between cultural institutions, social practices, language, interpersonal relationships, and individual development (Tsui et al, 2009). The previous section described how Engeström’s unit of analysis is activity systems, as characterised in Figure 2.2. Lave and Wenger’s unit of analysis is the interaction between individual learners and ‘communities of practice’ in whose activities they participate. Their work was published in two books (Lave and Wenger, 1991; Wenger, 1998) and is concisely summarised by Tsui et al (2009). It has been enthusiastically adopted by the medical education community worldwide because it so well applies to medical work-based learning in ways we now describe. In his foreword to their first book, Hanks (p. 13) described how Lave and Wenger’s writing excited him ‘because it located learning squarely in the processes of co-participation, not in the heads of individuals’. According to them, ‘Learning is distributed among co-participants not a one-person act’. Lave and Wenger originally set out to reconceptualise apprenticeship, an age-old tradition that is still strongly represented in the discourse of medical education. Their work moved the notion of apprenticeship from a dyadic relationship between teacher and learner centred on the performance of tasks, to a social relationship between learners and communities of practice, centred on the co-construction of meaning and identity. In Hanks’ words (p. 15), ‘while the apprentice may be the one transformed most dramatically by increased participation in a productive process, it is the wider process that is the crucial locus and precondition for this transformation’. Learning, from this new perspective, became ‘a way of being in the social world, not a way of coming to know about it’ (p. 24).
Chapter 11 revisits communities of practice theory in relation to acquiring team working skills and learning skills in the context of functioning clinical teams, while Chapter 12 views workplace learning from a communities of practice perspective, particularly in relationship to the growth of medical learners from novices to established physicians, and then to ‘old-timers’. This description sets out to familiarise readers with some of the terminology and concepts of this perspective. The suffix to the title of Lave and Wenger’s 1991 book was ‘legitimate peripheral participation’, a phrase that encapsulates important elements of their perspective. Learning is through participation in the activities of authentic workgroups, or communities of practice. For participation to be possible, the learner must be legitimate in the eyes of the community. Novices – such as medical students – enter such a community at its periphery because they are not yet equipped to be full participants. Through participation, for example as a senior medical student or foundation trainee, they move centripetally to become full members of the community. There is a reciprocal dynamic between their development and the development of the community such that, at the end of the lifelong learning continuum, ‘old-timers’ may be transformed by more junior participants or may come into conflict with them. Lave and Wenger see no distinction between work and learning – according to them, ‘learning is an integral and inseparable aspect of social practice’. Through participation, members of a community of practice construct meaning and develop identity. The place of language in learning, meaning, and identity is nicely captured by their notion that learners learn both from talk and to talk. Importantly, Lave and Wenger decouple learning and instruction, because learning can take place without instruction, even when activities are conducted with no educational intent. So, learning is an inevitable part of everyday life.
For present purposes, the term ‘community’ can be taken more or less at face value but the term ‘practice’ is characterised by Wenger (1998) as having several important components: ‘mutual engagement’ between members of the community; relationships of mutual accountability; and ‘shared repertoires’ of routines, words, tools, ways of doing things, stories, gestures, symbols, genres, actions, and concepts. A communities of practice perspective places great weight on identity, which is neither individual nor abstractly social. Identity exists in the mutual engagement of person and community. Identity ‘exists in the constant work of negotiating the self’. Medical learners, from this perspective, are in a constant process of defining and redefining their identities throughout the lifelong learning continuum.
Summary and conclusions
We have presented a range of perspectives on learning, selected because they are relevant to medical educators in their educational practice and scholarship, and researchers in their explorations of the field. We have framed them along two dimensions: the extent to which they are abstract or applied and the extent to which they emphasise learning as an individual or a collaborative process. We recognise that such distinctions cannot be absolute, as many perspectives encompass aspects of both ends of these dimensions; however, we hope this ‘mapping’ will help readers conceptualise them in ways that can support their practice. We have also introduced the idea of metaphors for learning, to highlight how they influence discourse and practice. We agree with others that the two metaphors of acquisition and participation are both necessary to develop maximally effective learning. In addition to presenting more abstract theoretical perspectives such as SCT and socio-cultural theory, we have presented more applied perspectives, such as adult learning, SDL, and lifelong learning. We have included them because we regard it as important to understand the origins and assumptions of perspectives that, whilst questionable in terms of their theoretical ‘purity’, are pervasive in the contemporary discourse of learning and teaching. Above all, our goal has been to provide perspectives that can guide practice and research and encourage educators to examine their own perspectives on teaching and learning.
Implications for practice
Kurt Lewin famously said ‘there is nothing as practical as a good theory’. Educators wishing to do more than unquestioningly replicate previous practice will find that keeping the following questions at the forefront of their minds will lead to better practice:
Which theoretical perspectives guide my practice?
Does my practice actually reflect the perspectives I espouse?
How can I use these perspectives to:
Adopting a constructivist view of learning makes it logical to place the learner at the centre of teaching and learning activity and see the teacher’s role as facilitating learning. Shifting the emphasis from individual learning towards social and collaborative learning makes it logical to consider clinical learning environments as communities of practice where learners develop their professional identities through both explicit and implicit processes. A socio-cultural perspective leads teachers to encourage both individual and collective learning; take advantage of cultural tools and other mediators available; use other learners, both peers and more senior learners, to facilitate learning; and consider learning and teaching as a joint enterprise, for which teachers and learners together assume responsibility.
Aukes L.C., Geertsma J., Cohen-Schotanus J., et al. The development of a scale to measure personal reflection in medical practice and education. Med Teach. 2007;29:177-182.
Ausubel D. The psychology of meaningful verbal learning. New York: Grune & Stratton, 1963.
Bandura A. Self-efficacy: the exercise of control. New York, NY: Freeman, 1997.
Bandura A. Social foundations of thought and action. A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall, 1986.
Bandura A. Social Cognitive Theory: an agentic perspective. Ann Rev Psychol. 2001;52:1-26.
Bleakley A. Broadening conceptions of learning in medical education: the message from teamworking. Med Educ. 2006;40:150-157.
Boud D., Walker D. Promoting reflection in professional courses: the challenge of context. Harrison R., Reeve F., Hanson A., Clarke J., editors. Supporting lifelong learning, vol 1. London, UK: Routledge Farmer. 2002:91-110.
Boud D., Keogh R., Walker D., editors. Reflection:turning experience into learning. London: Kogan Page, 1985.
Brockett P.G., Hiemstra R. Self-direction in adult learning: perspectives on theory, research and practice. New York, NY: Routledge, 1991.
Candy P. Self-direction for lifelong learning. San Francisco, CA: Jossey Bass, 1991.
Cheetham G., Chivers G. Professions, competence and informal learning. Cheltenham, UK: Edward Elgar, 2005.
Chung P.J., Chung J., Shah M.N., et al. How do residents learn? The development of practice styles in a residency program. Ambul Pediat. 2003;3:166-172.
Coffield F., Mosely D., Hall E., et al. Learning styles and pedagogy in post-16 learning: a systematic and critical review. London: Learning and Skills Research Centre, 2004.
Coulehan J. Today’s professionalism: engaging the mind but not the heart. Acad Med. 2005;80:892-898.
Coulehan J., Williams P.C. Vanquishing virtue: the Impact of Medical Education. Acad Med. 2001;76:598-605.
Curry L. Cognitive and learning styles in medical education. Acad Med. 1999;74:409-413.
Dewey J. How we think. Amherst, NY: Prometheus Books, 1991.
Engeström Y. The future of activity theory: a rough draft. In: Sannino A., Daniels H., Gutierrez K.D., editors. Learning and expanding with activity theory. Cambridge: Cambridge University Press, 2009.
Epstein R.M., Hundert E.M. Defining and assessing professional competence. JAMA. 2002;287:226-235.
Eraut M. Non-formal learning and tacit knowledge in professional work. Brit J Educ Psychol. 2000;70:113-136.
Eva K., Lingard L. What’s next? A guiding question for educators engaged in educational research. Med Educ. 2008;42(8):752-754.
Eva K.N., Regehr G. Knowing when to look it up: a new concept of self assessment ability. Acad Med. 2007;82:581-584.
Fox R.D., Mazmanian P.E., Putnam R.W., editors. Change and learning in the lives of physicians. New York: Praeger, 1989.
Gagné R.M. The conditions of learning and the theory of instruction. New York: Holt, Rinehart and Winston, 1985.
Grant A., Kinnersley P., Metcalf E., et al. Students’ views of reflective learning techniques: an efficacy study at a UK medical school. Med Educ. 2006;40:379-388.
Greenaway R. Critiques of David Kolb’s theory of experiential learning. 2009. [internet] Available at: http://reviewing.co.uk/research/experiential.learning.htm#styles Accessed November 23
Guba E.G., Lincoln Y.S. Paradigmatic controversies, contradictions, and emerging confluences. In: Denzin N.K., Lincoln Y.C., editors. The Sage handbook of qualitative research. ed 3. Thousand Oaks, CA: Sage; 2005:191-215.
Guglielmino L.M. Contributions of the self-directed learning readiness scale (SDLRS) and the learning preference assessment (LPA) to the definition and assessment of self-direction in learning. Paper presented at the First World Conference on Self-Directed Learning. Canada: Montreal. 1997.
Hafferty F., Frank R. The hidden curriculum, ethics teaching and the structure of medical education. Acad Med. 1994;69:861-871.
Handal G., Lauvas P. Promoting reflective teaching: supervision in action. Milton Keynes, UK: The Society for Research into Higher Education and Open University Press, 1987.
Hattie J., Timperley H. The power of feedback. Rev Educ Res. 2007;77:81-112.
Herbert C.P., Wright J.M., Maclure M., et al. Better Prescribing Project: a randomized controlled trial of the impact of case-based educational modules and personal prescribing feedback on prescribing for hypertension in primary care. Fam Pract. 2004;21(Oct):575-581.
Hojat M., Veloski J.J., Gonnella J.S. Measurement and correlates of physicians’ lifelong learning. Acad Med. 2009;84(8):1066-1074.
Honey P., Mumford A. Manual of learning styles. London, UK: Peter Honey Publications, 1986.
Knowles M.S., et al. Andragogy in action: applying modem principles of adult learning. San Francisco: Jossey-Bass, 1984.
Kolb D.A. Experiential learning: experience as the source of learning and development. Englewood Cliffs, NJ: Prentice Hall, 1984.
Kolb D.A. Learning Style Inventory. Version 3.1. Boston, MA: Hay Group, Hay Resources Direct, 2005.
Kolb D.A., Boyatzis R.E., Mainemelis C. Experiential Learning Theory: previous research and new directions. In: Sternberg R.J., Zhang L.F., editors. Perspectives on thinking, learning and cognitive styles. New Jersey: Erlbaum, 2001.
Lantolf J.P., Thorne S.L. Sociocultural theory and the genesis of second language development. Oxford: Oxford University Press, 2006.
Lave J., Wenger E. Situated learning. Legitimate peripheral participation. Cambridge: Cambridge University Press, 1991.
Longworth N., Davies W.K. Lifelong learning. London: Kogan Page, 1996.
Mamede S., Schmidt H. The structure of reflective practice in medicine. Med Educ. 2004;38:1302-1306.
Mamede S., Schmidt H. Correlates of reflective practice in medicine. Adv Health Sci Educ Theory Pract. 2005;10:327-337.
Mamede S., Schmidt H., Penaforte J. Effects of reflective practice on the accuracy of medical diagnoses. Med Educ. 2008;42:468-475.
Mann K.V., Gordon J.J., MacLeod A.M. Reflection and reflective practice in health professions education a systematic review of the literature in the health professions. Adv Health Sci Educ Theory Pract. 2009;14:595-621. DOI 10.1007/s10459-007-9090-2
Maslow A.H. Motivation and personality, ed 2. New York, NY: Harper Collins, 1970.
Merriam S.B. Andragogy and self-directed learning: pillars of adult learning theory. Merriam S.B., editor. The new update on adult learning theory: New directions for adult and continuing education, vol 89. 2001:3-14.
Merriam S.B., Caffarella R.S., Baumgartner L.M. Learning in adulthood. A comprehensive guide, ed 3. San Francisco, CA: Jossey-Bass, 2007.
Mezirow J. Transformative dimensions of adult learning. San Francisco: Jossey-Bass, 1991.
Miflin B., Campbell C.B., Price D.A. A lesson from the introduction of a problem-based, graduate entry course: the effects of different views of self-direction. Med Educ. 1999;33:801-807.
Misch D.A. Andragogy and medical education: are medical students internally motivated to learn? Adv Health Sci Educ Theory Pract. 2002;7:153-160.
Moon J. Reflection in learning and professional development. London, UK: Kogan Page, 1999.
Moulton C.A., Regehr G., Mylopoulos M., et al. Slowing down when you should: a new model of expert judgement. Acad Med. 2007;82:S109-S116.
Norman G. Teaching basic science to optimize transfer. Med Teacher. 2009;31:807-811.
Norman G.R. The adult learner: a mythical species. Acad Med. 1999;74:886-889.
Norman G.R. When will learning style go out of style? Adv Health Sci Educ Theory Pract. 2009;14:1-4.
Oddi L.F., Ellis A.J., Robertson J.E.A. Construct validation of the Oddi continuing learning inventory. Adult Ed Quar. 1990;40(3):139-145.
Premi J., Shannon S., Hartwick K., et al. Practice-based small-group CME. Acad Med. 1994;69(Oct):800-802.
Prideaux D., Bligh J. Research in medical education: asking the right questions. Med Educ. 2002;36:1114-1115.
Robbins P., Aydede M. A short primer on situated cognition. In: Robbins P., Aydede M., editors. The Cambridge handbook of situated cognition. New York: Cambridge University Press; 2009:3-10.
Sargeant J., Mann K., Sinclair D., et al. Learning in practice: experiences and perceptions of high-scoring physicians. Acad Med. 2006;81:655-670.
Sargeant J., Armson H., Chesluk B., et al. The processes and dimensions of self-assessment. Malaga, Spain: AMEE, 2009. Research presentation
Sargeant J., Mann K., van der Vleuten C., et al. Reflection: a link between receiving and using assessment feedback. Adv Health Sci Educ Theory Pract. 2009;14(3):399-410.
Schlesinger E. Why learning is not a cycle. Ind Commer Training. 1996;28:30-35.
Schön D. Educating the reflective practitioner: toward a new design for teaching and learning in the professions. San Francisco, CA: Jossey-Bass, 1987.
Sfard A. On two metaphors for learning and the dangers of choosing just one. Educ Res. 1998;27:4-13.
Simons R.-J., Vander Linden J., Duffy T. New learning. Dordecht, NL: Kluwer, 2000.
Smith C.S., Morris M., Francovich C., et al. A qualitative study of resident learning in ambulatory clinic. The importance of exposure to ‘breakdown’ in settings that support effective response. Adv Health Sci Educ Theory Pract. 2004;9:93-105.
Sobral D.T. Medical students’ mindset for reflective learning: a revalidation study and the reflection in learning scale. Adv Health Sci Educ Theory Pract. 2005;10:303-314.
Sobral D.T. Medical students’ reflection-in-learning in relation to approaches to study and academic achievement. Med Teach. 2001;23:508-513.
Tsui A.B.M., Lopez-Real F., Edwards G. Sociocultural perspectives of learning. In: Tsui A.B.M., Edwards G., Lopez-Real F., editors. Learning in school-university partnership. Sociocultural perspectives. New York: Routledge, 2009.
Vygotsky L.S. Mind in society: the development of higher psychological processes. Cambridge, MA: Cambridge University Press, 1978.
Wells G. Language and education: reconceptualising education as dialogue. Annu Rev Appl Linguist. 1999;19:135-155.
Wenger E. Communities of practice: learning, meaning and identity. Cambridge, UK: Cambridge University Press, 1998.
Wertsch J.V. Voices of the mind: a sociocultural approach to mediated action. Cambridge, MA: Harvard University Press, 1991.
White J.A., Anderson P. Learning by internal medicine residents: differences and similarities of perceptions by residents and faculty. J Gen Intern Med. 1995;10:126-131.
Bandura A. Social Cognitive Theory: an agentic perspective. Ann Rev Psych. 2001;52:1-26.
Guba E.G., Lincoln Y.S. Paradigmatic controversies, contradictions, and emerging influences. In: Denzin N.K., Lincoln Y.S., editors. The Sage handbook of qualitative research. ed 3. Thousand Oaks, CA: Sage; 2005:191-215. ISBN 0-7619-2757-3
Kaufman D.M., Mann K.V. Teaching and learning in medical education: how theory can inform practice. Edinburgh, UK: Association for the Study of Medical Education, 2007.
Lave J., Wenger E. Situated learning. Legitimate peripheral participation. Cambridge: Cambridge University Press, 1991.
Sfard A. On two metaphors for learning and the dangers of choosing just one. Educational Researcher. 1998;27:4-13.