12 Learning and teaching in workplaces
Codified knowledge See main Glossary, p 339.
Context See main Glossary, p 340.
Community of practice (CoP) See main Glossary, p 340.
Cultural knowledge Knowledge about social relationships, norms, and values that impacts on interactions within a group of people.
Curriculum in action See main Glossary, p 340.
Curriculum, intended See main Glossary, p 340.
Experienced curriculum See main Glossary, p 340.
Implicit learning See main Glossary, p 341.
Informal education/learning See main Glossary, p 341.
Intersubjectivity When members of a team understand each others’ preferences and idiosyncrasies, they can work together without the need for constant interpersonal negotiation.
Learning See main Glossary, p 341.
Medical (education) workplace See main Glossary, p 341.
Personal knowledge What individuals bring to situations that enables them to think, interact, and perform.
Self-efficacy See main Glossary, p 342.
Tacit knowledge See main Glossary, p 343.
Outline
Whether we like it or not, the main purpose of workplaces is getting a job done rather than learning. Yet, workplaces are rich learning environments and getting jobs done entails a lot of learning, a tension that creates both opportunities and challenges. Workplace learning and teaching is pivotal throughout the medical continuum, from medical student clerkship placements to trained practitioners’ continuing professional development. Sometimes learning is serendipitous and messy; at other times it is planned and systematic. Learning on the job is increasingly being complemented by learning at the job, which includes formal teaching sessions, meetings with supervisors, personal reading, and personal reflection that have always been part of medical workplaces. This chapter considers what we really mean by learning on the job and what can be done to enhance it. It is complementary to Chapter 7, which discusses learning environments. Because workplace learning is so pivotal, learning at the job is spread over many other chapters: Chapters 9, 10, and 11 consider small and large group and skills learning. Chapters 8, 13, and 18 consider individual tuition at the job, including the identification of learning needs, reflective learning and appraisal, and guiding career progression. Chapter 19 considers how to develop learners and teachers for their respective roles in clinical education. This chapter first considers, from an educational viewpoint, what a workplace is. It then separates out, from both practical and theoretical standpoints, the components and processes of workplace learning. Finally, it puts them back together into a complete system and considers how the workings of that system can be enhanced.
Features of learning in medical workplaces
Learning in context
A medical education workplace has been defined as ‘any place where patients, learners, and practitioners come together for the conjoint purpose of providing medical care and learning’ (Dornan et al, 2009). This broad definition helps make explicit that when we use the term learner we are not just referring to medical students – in continuous professional development, for example, the practitioner is the learner. What is common to all learning, however, is that workplaces where learning occurs are similar to the complex environments in which learners must apply the skills, knowledge, and attitudes that they develop. For trainees, it is similar to the context in which they will work later. For practitioners, it is identical to the context where they must apply their learning. Therefore, workplaces present learners with both learning opportunities and possible learning outcomes. This is an important feature of workplace learning. There is good evidence showing that we are better able to recall and apply knowledge and skills in places that are similar to those where they were learnt; learning is also most effective when it meets immediate needs and is directly applicable (Rogoff, 1990; Slotnick, 1999). However, the advantages of immediacy and context can be offset by workplaces providing limited time to prepare, brief, reflect, and debrief – features that are important to make the most of learning experiences. Another disadvantage is that busy workplaces can disjoin practice from theory. The dominance of ‘this is how we do it around here’ over ‘let’s make our practice evidence based and theoretically underpinned’ has brought workplace and apprenticeship learning into some disrepute, though recent advances in our understanding of how learning occurs in workplaces and how it can be enhanced have started something of a renaissance in apprenticeship models (Rogoff, 1995; Sheehan et al, 2005; Teunissen et al, 2007).
Triadic relationship
The primary focus of health care workplaces is on patient care, whereas the primary focus of traditional classroom contexts is on the learner and teacher. Learning in health care workplaces therefore changes these two-way relationships to three-way teacher–learner–patient relationships (Dornan et al, 2007). Attention to patients’ needs is of foremost importance, a value that is shared between teacher and learner but which imposes on the teacher the dual obligation of attending to the patient’s needs and to the learner’s needs. This triadic relationship is self-evident when a patient is physically present but the immediacy of a patient’s needs very easily dominates even when just a teacher and learner are in the same room. Patients’ unpredictable needs can turn the best-prepared teaching session to chaos but can, equally, present powerful learning opportunities at the most unexpected moments. While this triadic relationship can cause tensions, it can also be used to advantage by all parties. For example, many valuable learning opportunities arise when a teacher and learner are both puzzled over a patient’s problem. Arriving at a solution to this problem can help the learning of both the teacher and learner and help the health of the patient. While classroom learning is often planned and explicit, workplace learning is more opportunistic and covert. Understanding how this triadic learning relationship occurs can help all parties recognise opportunities and make the most of them when they arise.
Processes and outcomes are hard to control
Another characteristic of workplace learning and teaching is that the education actually being offered (the curriculum in action) does not fully coincide with the curriculum on paper, or intended curriculum, of a formal education programme. And the curriculum that is experienced – what trainees actually learn – is different again and will even differ between two individuals who share the same experiences (Lempp and Seale, 2004; Remmen, 1999). Furthermore, access to role models is a feature of workplaces that has a powerful influence on what people actually learn, particularly their acquisition of ‘tacit’ knowledge (knowledge that is learnt and applied almost unconsciously) and covert knowledge (Eraut et al, 2000; Polanyi, 1974). Daily interaction with other co-workers also contributes important knowledge despite both parties remaining unaware that learning and teaching are going on (Lave and Wenger, 1991). So, workplaces have very powerful effects on learning, much of which is positive, but only some of which is overt. Workplaces support a type of learning that simply cannot take place in other contexts and much of what is learnt will be remembered and applied. However, there are factors that may inhibit learning of good habits and/or promote good learning of bad habits. While some of it seems to happen effortlessly under our noses, aspects of workplace education can be improved by making it more explicit.
Table 12.1 outlines some advantages and disadvantages of workplace learning. The next section analyses in finer detail some theories of workplace learning followed by the constituent parts of workplace learning and the ways in which they interact.
Table 12.1 Advantages and disadvantages of workplace learning
| Features of workplace learning | Advantages | Disadvantages |
|---|---|---|
| Learning occurs in context | Learning is more easily applied and recalled | Workplace demands may limit available time |
| Learning has immediate relevance | Learning can be applied directly | Time spent preparing and reflecting can be limited |
| Learning can be unpredictable | Learning can occur at any time | Hard to prepare |
| Learning content can be unstructured | Learning can be directly related to needs | Hard to be systematic so gaps may be left or there may be duplication |
| Learning is from experience | Learning is powerful | Not all experiences are good experiences; some learning is from mistakes |
| Learning from patients | Results and feedback can be immediate and direct | Learning may impinge on patient safety issues |
| Learning is determined by case mix | The case mix forms a de facto curriculum that covers common problems | Important but uncommon problems may be omitted |
| Learning depends on relationships with work colleagues | Learning can be individualised and motivating when relationships are positive | Learning can be inhibited or threatening when relationships are negative |
| Learning from role models | Helps professional identity and role development | Not all role models are good role models |
| Learning from colleagues | Applicability is immediate; experience of others offers additional perspectives | Practice can dominate over theory; underpinning theory and evidence base may be lost; bad habits are perpetuated |
| Learning may be covert and outcomes tacit | Consciousness is reserved for more strenuous tasks; helps to develop fluidity in performance | Some influences may be unfavourable; tacit knowledge is hard to teach to others; learners are not aware of learning processes and outcomes |
Theoretical perspectives on workplace learning
Just as doctors need to understand the pathophysiology of diseases to care for patients, an understanding of the concepts of participation and cognition helps understand workplace learning. There are many theoretical perspectives (Cheetham and Chivers, 2005), ranging from cognitivist views of how experts transfer their knowledge and skills to learners, to sociocultural perspectives on how learning arises from interactions among members of workplace ‘communities of practice’ (CoP) (Bleakley, 2006; Slotnick, 2001; Swanwick, 2005; Wenger, 1998). Theoretical underpinnings of medical education are considered more fully in Chapter 2 but three of them – concepts around informal learning, social cognitive theory, and communities of practice theory – provide useful perspectives on workplace learning and deserve a brief overview at this point. Subsequently, workplace learning is broken down into three constituent parts: ‘tasks’, ‘contexts’, and ‘learners’. Those three interrelated parts are common to different theoretical perspectives on workplace learning and teaching.
Concepts around informal learning
Much learning at work, even in an educational context, occurs outside the formally organised and delivered curriculum. Informal learning has been described by Eraut as taking place ‘in the spaces surrounding activities and events with a more formal educational purpose’ (Eraut, 2004). From an educational viewpoint, informal learning appears to be unstructured, unintended, and opportunistic. Informal learning is closely linked to implicit or tacit learning. Reber describes implicit learning as ‘the acquisition of knowledge, independent of conscious attempts to learn and in the absence of explicit knowledge about what was learned’ (Reber, 1993). According to Eraut, it is hard to understand learning at work because of several factors. First, informal learning is largely invisible because much of it is taken for granted and not recognised as learning. Second, the resulting knowledge is either tacit or regarded as part of a person’s general capability rather than something that has been learnt. Lastly, discourse about learning is predominantly about propositional, codified knowledge, and people have difficulty describing the more complex aspects of their work and the nature of their expertise. So, although informal learning and the use of tacit knowledge are probably the largest part of the learning process in workplaces, the characteristics of informal learning make its identification difficult. To study and understand learning in workplaces, Eraut asks three questions about this type of learning: What is learnt? How is it learnt? And what are the factors that influence learning? (Eraut, 2004).
What is learnt?
Eraut distinguishes three types of knowledge outcomes. Codified knowledge is the kind of academic knowledge that can be found in nearly all workplaces in the form of textbooks, organisation-specific or specialty-specific protocols, records, correspondence, manuals, etc. Secondly, cultural knowledge plays a key role in workplace activities, which is knowledge about social relationships, norms, and values that impact on interactions within a group of people. According to Eraut, much uncodified cultural knowledge is ‘acquired informally through participation in social activities; and so much is often taken for granted that people are unaware of its influence on their behavior’. As a counterpart to these two types of socially shared knowledge, Eraut identifies ‘personal knowledge’ as ‘what individuals bring to situations that enable them to think, interact and perform’. This includes personalised versions of codified knowledge, but also knowledge of self, people, situations, attitudes, and emotions. In his terms, skills require a combination of personal and cultural knowledge. Competence is then defined as meeting other people’s (often implicit) expectations, making it a much more problematic concept in terms of defining competence as an educational outcome and in its assessment.
How is it learnt?
Given the fact that so many learning outcomes go unnoticed, studying how people learn in workplaces is challenging. Eraut’s approach to this problem is to describe four types of activity through which learning occurs: participation in group activities, working alongside others, tackling challenging tasks, and working with clients. In all of these activities the quality of relationships is essential. Billett also takes participation in workplace activities to be central to understanding workplaces as learning environments (Billett, 2004a). Moreover, he stresses the importance of how and what activities and interactions workplaces afford learners. Additionally, he acknowledges the active role learners play in choosing how they participate and in what activities they participate. Billett stresses that an individual’s participation is ‘not ad hoc, unstructured or informal’ (Billett, 2004b). He introduces the concept of the ‘workplace curriculum’ to indicate that learners’ participation is highly structured, albeit usually not on educational grounds. The organisation of tasks is usually directed towards the goals of particular workplaces, for instance the efficient provision of health care. Billett argues that ‘workplaces will invite workers to engage and learn, insofar as that participation serves its goals and/or the interests of those within it, that is the continuity and/or development of the workplace or affiliates or individuals within it’ (Billett, 2006). The opportunities for engagement afforded to learners and the way in which they choose to participate will influence the quality of a workplace as a learning environment. In taking this view, Billett explicitly introduces power and control as important regulators of opportunities. Fuller and Unwin (2003) have pursued a line of research in which they have looked at the opportunities and challenges learners experience in a workplace. Based on several case studies in vocational training programmes in the United Kingdom, they identified differences in participatory practices that could be located on a continuum from a ‘restrictive’ to an ‘expansive’ working environment (Fuller and Unwin, 2003). ‘Expansive’ workplaces offer a broad range of possible learning activities, provide gradual transition from peripheral participation to more full participation, provide support and guidance to learners, and recognise learners’ status within a community among others. ‘Restrictive’ workplaces lack these characteristics. Such restriction can arise from a number of influences, such as the attitudes of co-workers, the ‘queue’ of other learners that may take precedence, the value the workplace puts on the personal development of others, or physical constraints that limit informal interactions among co-workers. They argue that an ‘expansive’ approach leads to ‘a stronger and richer learning environment’ (Fuller and Unwin, 2003).
What factors influence workplace learning?
Eraut’s third question concerns factors that influence learning in workplaces. There are many factors that impact on learning in one way or the other. Most of them influence how learners decide on which activities to participate in and factors that influence how learners interpret their experiences. Such factors can be grouped into three broad categories: factors associated with the activity itself, factors related to an individual learner’s characteristics, and contextual factors. These three categories are discussed in detail later in this chapter. At this point we limit ourselves to an illustration of how factors that impact on learning are interrelated. Eraut highlighted the importance of confidence that arises from meeting the challenges in one’s work (Eraut, 2004). Confidence in this situation seems integrally related to Bandura’s concept of self-efficacy (Bandura, 1994); it is a context-specific perception and relates to the ability to execute a specific task or to fulfil a particular role. Confidence relates strongly to the perceived quality of relationships in the workplace; tackling challenging tasks will be easier when learners feel appropriately supported in doing so. Support and confidence lead to social inclusion in teams and engenders commitment. To develop confidence in tackling new tasks, feedback and appreciation of the value of the work are also critical. Again, workplace learning reveals a complex interrelatedness among concepts such as confidence, commitment, context, challenge, and value of work, and feedback and support in performing tasks.
Social cognitive theory
Another theoretical perspective relevant to understanding workplace teaching and learning is social cognitive theory. This perspective sheds light on how interactions between people and their environments lead to behaviour and behavioural change. Therefore, it places greater emphasis on cognitive aspects of learning than socio-cultural perspectives do. The main proponent of social cognitive theory has been the psychologist Albert Bandura. Drawing on research on learning and self-efficacy, social cognitive theory has gradually developed over the past 50 years. Central to social cognitive theory is personal agency. People are the producers and products of the social systems in which they operate (Bandura, 2001). They try to ‘make good judgments about their capabilities, anticipate the probable effects of different events and courses of action, size up sociostructural opportunities and constraints, and regulate their behaviour accordingly’ (Bandura, 2001). Bandura identified intentionality, forethought, self-reactiveness, and self-reflectiveness as core features of personal agency (Bandura, 2001). Intentions are cognitive representations of future courses of action to be performed. Individuals can motivate themselves and choose between courses of action because they anticipate certain consequences of their own behaviour. The surgeon who plans to add a new surgical technique to the range of procedures he is qualified in can intentionally look for courses and opportunities to develop the necessary new skills. Forethought is another hallmark of personal agency. For example, when attending to a woman in labour who previously suffered from postpartum haemorrhage, a resident in obstetrics will actively lead the third stage of labour (when the placenta is delivered) because he or she will have confidence in being able to influence the outcome. Intentions and forethought are influenced by an individual’s beliefs, values, goals, and personal knowledge structures. According to Bandura, the relative stability of one’s intentions explains why individuals can display considerable self-directness and do not necessarily change a course of action even if it leads to unrewarding outcomes (Bandura, 2001). Some learners will continue to be proactive in seeking learning opportunities if they believe that these experiences will help them obtain their goals, even in a situation where their initiative is not reciprocated.
Self-regulatory behaviour
In guiding learners to develop appropriate action possibilities, the concepts of self-reactiveness and self-reflectiveness are personal qualities that have received considerable attention in medical education. They stem from the realisation that the outcome of events, especially if other people are involved, is only partly the result of one individual’s agentic actions. Therefore, when engaged in tasks, individuals ‘cannot simply sit back and wait for the appropriate performances to appear’ (Bandura, 2001). To make sure that you perform appropriately, you need to regulate your thoughts and actions in the ongoing flow of events. Based on personal standards of appropriate behaviour, individuals use self-monitoring and self-guidance to react and respond to events (Bandura, 2001). Such self-regulatory aspects of behaviour are receiving increased attention within medical education as an alternative way of conceptualising self-assessment (Eva and Regehr, 2007). The concept of self-assessment is discussed in Chapter 8. Gradually, through practice, proficient modes of action are developed that are suited to similar situations and the execution of these actions becomes automated. Self-reflectiveness will then help learners continue to learn from the outcomes of events by judging ‘the correctness of their predictive and operative thinking against the outcomes of their actions, the effects that other people’s actions produce, what others believe, deductions from established knowledge and what necessarily follows from it’ (Bandura, 2001). From a teacher or supervisor perspective, this means that a trainee’s lifelong learning may be enhanced by taking time to understand the learner’s motivations and aspirations.
Self-efficacy
A central premise underlying Bandura’s work is that the factors involved in the motivation and guidance of behaviour are all ‘rooted in the core belief that one has the power to produce effects by one’s actions’ (Bandura, 2001). This belief, if related to a specific task, is called perceived self-efficacy (Bandura, 1997). Perceived self-efficacy judgements influence the tasks trainees choose to participate in, how they self-regulate, and how they self-evaluate their performance (Bandura, 2005). It thereby influences trainees’ experiences and shapes their future participation in the clinical workplace. Four distinct sources contribute to self-efficacy beliefs. First, mastery experience is the most influential source of self-efficacy beliefs (Pajares, 1997). Outcomes interpreted as successful raise self-efficacy, those interpreted as failures lower it (Bandura, 1997; Pajares, 1997). If you have done ten venepunctures successfully, you will believe that you can do the eleventh one successfully too. If you learnt something from a particular interaction or activity, you will be more confident in making future attempts. The second source is vicarious experience of the outcomes produced by the actions of others. Role models and peers are particularly relevant to judgements about the self (Bandura, 2005). If your peers are all able to do venepunctures, you are more likely to believe that you can do them as well. However, when your peers all fail to perform a procedure only senior staff members can perform, your self-efficacy beliefs will probably drop. A third source of self-efficacy, whose effects are not as strong as mastery or vicarious experiences, is verbal persuasion by others. It is usually easier to weaken self-efficacy beliefs through negative appraisals than to strengthen such beliefs through positive encouragement (Bandura, 1997). We are more motivated when told what we did right, not just what we did wrong, and we are more likely to be successful if a supervisor has confidence in us. Fourth, physiological states such as anxiety, stress, and arousal can influence self-efficacy beliefs.
Communities of practice theory
As a third theoretical perspective on workplace learning and teaching, we discuss Lave and Wenger’s work on CoP and legitimate peripheral participation. It is a prime example of the sociocultural theorising that is finding its way into medical education (Lave and Wenger, 1991; Swanwick, 2005; Wenger, 1998). In essence, Lave and Wenger conceptualised learning as ‘an integral and inseparable aspect of social practice’ (Lave and Wenger, 1991). It is valuable for understanding learning and teaching in the workplace because it offers a lens through which the development of relative newcomers (e.g. medical students and interns) within an existing group of practitioners (e.g. medical wards or departments) can be analysed. Central to this socio-cultural view on learning is the concept of ‘participation’. According to Lave and Wenger, participation is the key to understanding how learners develop within a community. Questions such as what opportunities do learners get or create to participate, with whom do they participate and on what tasks, and what do they take out of their participation are crucial in this view on learning. Lave and Wenger’s work specifically focused on the relation between novices and experts in CoP. A CoP is a ‘set of relations among persons, activity, and world, over time’ that is the result of collective learning in the ‘pursuit of a shared enterprise’ (Lave and Wenger, 1991; Wenger, 1998). Because newcomers participate alongside more experienced community members, this stimulates an exchange of knowledge and a negotiation of meaning between members, resulting in the ongoing reproduction of a CoP. After studying a number of apprenticeship situations, from tailors in West Africa to the US. Navy quartermasters, Lave and Wenger proposed legitimate peripheral participation as a descriptor of how practices are made accessible to newcomers (Lave and Wenger, 1991). Initially, newcomers are introduced into a CoP by allowing them to observe, for example, in an operating theatre or outpatient clinic. This is followed by allowing them to participate in low-risk tasks (such as a physical examination) or by letting them perform tasks under close supervision. What counts as a low-risk or simple task will depend on the expertise of the newcomer and supervisor. This type of introduction into a CoP can be described as peripheral participation. It has to be accompanied by enough legitimacy to really engage newcomers. The newcomer has to feel that he or she is allowed to be there. If, for whatever reason, a CoP does not open up, then ‘inevitable stumblings and violations’ become a ‘cause for dismissal, neglect, or exclusion’ rather than opportunities to learn (Wenger, 1998). Through their participation in a CoP, newcomers will develop along personal trajectories towards the kind of full participation that is characteristic of experts. Research on learning in the operating theatre and on trainees’ participation in internships suggests that situated learning theories, and the specific focus of legitimate peripheral participation on the development of newcomers, can be valuable for understanding medical workplace learning (Deketelaere et al, 2006; Lyon, 2004; Sheehan et al, 2005).
We have discussed three theoretical perspectives particularly relevant to workplace learning. However, as stated before, there are many educational perspectives that can be applied to workplace learning and teaching in medical education. Moreover, theories from the social sciences, ranging from social psychology to transition psychology and medical sociology, may also help us to understand aspects of learning and teaching in the workplace as well. We now provide a framework to break down workplace learning into three constituent parts: ‘tasks’, ‘contexts’, and ‘learners’. These three interrelated parts are common, in varying compositions, to different perspectives on workplace learning and can help identify differences between them. The next section analyses the constituent parts of workplace learning and the ways they interact in finer detail.
Constituent parts of workplace learning
Tasks
Workplace learning can be analysed by understanding three components and their interactions. The first of these parts is ‘tasks’. Medical students, residents, specialists, general practitioners, and other health care workers have different but complementary responsibilities whilst sharing the common purposes of providing a high standard of care, being cost-effective, and educating themselves and others. The participation of learners in a medical workplace is mainly dictated by the demands of patient care. Understanding the importance of what tasks people participate in and how the sequencing of tasks affects different individuals and groups is crucial to workplace learning. It then becomes possible to look at the way in which teams share tasks and different individuals within them interpret tasks, as this will eventually influence their learning (Eraut, 2004; Teunissen et al, 2009). Consider, for example, the endoscopic removal of a gallbladder. The surgeon-in-training is concerned about the anatomy of the abdomen and the steps needed to remove the gallbladder. The operating nurse focuses on the same steps but with a different aim than the surgeon. The anaesthetist has different concerns again. As each of them repeats different tasks with different colleagues and different patients over time, they follow paths that are both different from and linked with that of others. A practical implication of this is that a teacher may expect a certain task to lead to a particular set of learning outcomes, but it should not be assumed that everyone will learn, or would even wish to learn the same things from the same activities.
Contexts
The second component of workplace learning is context. The circumstances in which a task is undertaken are divided here into a physical and a social context.
Physical context
The term physical context refers to the physical setting in which a task occurs as well as the artefacts used to perform the task. Outpatient clinics, operating theatres, wards, and general practitioners’ surgeries are just some settings whose differences influence learning in important ways. Research on expertise has shown that people incorporate contextual information in the concepts and mental models they develop (Hatala et al, 1999). This kind of information can help them recognise the symptoms and signs of certain diseases. The differential diagnosis for a patient in Western Europe with a high fever will be different if he or she has been to a region where malaria and dengue are endemic. Physical context can hinder learning as well. Irrelevant contextual information can lead to wrong judgements (Teunissen et al, 2009) and differences in physical context can act as barriers to the transfer of learning between contexts (Hamstra et al, 2006). For example, it is most likely that what are learnt in an operating theatre are psychomotor skills and decision making, whereas what are learnt in an outpatient clinic are most likely to be diagnostic and management skills. General practice will most likely provide opportunities to learn about interventions that have longer-term outcomes or that affect people other than the patient. While any of these types of learning can occur in any context, it is important to recognise that some contexts are more likely to provide some types of learning opportunities than others.
Physical context can also influence the dynamics of learning environments. Consider, for example, the arrangement of chairs during morning rounds. Do doctors and medical students sit around the same table or are the doctors on the front row and medical students at the back? Another example is the availability of suitable medical equipment. A monitor on which students can see what the specialist is seeing makes a crucial difference to what they can learn from the laryngoscopic examination of the vocal cords and glottis. Such differences in the physical context give strong messages about the roles and value learners have in a group: whether they are to participate in discussions or just to watch and listen (Tan, 2009). So, physical context shapes learning (Lave and Wenger, 1991).
Social context
Just as physical factors shape learning, so do the people involved in a task and the social meaning system of which they are part. Doctors, nurses, secretaries, and cleaners, each with their own responsibilities and expertise, share the common goal of providing high-quality patient care. As stated earlier, such a group is called a ‘community of practice’ (Wenger, 1998). As gatekeepers of a practice, these co-workers determine the tasks learners can learn from. Everyone involved in a task is a potential learner and anyone can be a gatekeeper. The ways in which co-workers interact can facilitate or inhibit the learning of all parties. Whilst a medical student is the person who is present explicitly as a learner, a clinical supervisor or others who are present may learn vicariously from the same encounter. Significant learning opportunities are lost when senior staff monopolise interesting tasks and relegate juniors to menial ones. Simple, inclusive actions can have profound impacts on the learning opportunities tasks offer: for example, ‘You see this patient first and I’ll see her with you later’ versus ‘Come watch me see this patient’; or even ‘I’ve seen this patient, can you please arrange the following tests (but I’m not telling you why they need to be done)’. Moreover, giving learners an opportunity to engage with different tasks and different members of a community of practice will stimulate their engagement and motivation. Furthermore, a ‘queue of learners’ can also influence opportunities – a senior doctor may give higher priority to the learning needs of the senior trainee than to a medical student or nurse.
A second feature of the social context is the way people working with (or around) each other recognise each other’s role and input, develop customs and traditions, and share a common meaning system. Workers function better when they understand how others like to function and vice versa. For instance, newcomers learn how their seniors use jargon and abbreviations. By reciprocating the same jargon and abbreviations a trainee may strengthen the relationship with the senior colleague but alienate and worsen their relationship with more junior colleagues. This can also apply to role modelling – if a trainee imitates the behaviours of a senior colleague, the opportunities to learn from that colleague may be strengthened. If the behaviours being imitated, however, are negative or harmful, this strengthening of opportunities may be at the cost of good patient care. From those examples, it is easy to see how the social context can perpetuate desirable, or undesirable, behaviours through feedback loops; such influences may often not be made explicit. Likewise, a supervisor needs to be aware that seeing junior staff imitate their behaviour is not necessarily an endorsement that the behaviours are appropriate. Such positive or negative role modelling is a powerful influence on learning. We are well attuned to picking up subtle cues from others around us – hearing or reading how something should be achieved can easily be overpowered by seeing someone in authority, or who is perceived as expert, do something else. This may lead to tensions, but also powerful learning opportunities, that can often be capitalised on by good debriefing – either formally with a mentor or, not uncommonly, with co-workers in informal settings.
Thirdly, co-workers can directly affect the learning outcomes of tasks (Teunissen et al, 2007). In a setting where a clinical teacher tries to educate a resident or medical student, he or she does this by highlighting specific aspects of a task at hand, giving instructions, and feeding back on a learner’s performance (Irby, 1994). In doing so, the teacher shapes which aspects of the task and the learner’s behaviour are subjected to reflection and lead to permanent changes in the way the learner will think or act (Hattie and Timperley, 2007).
Learners
The third and final component of workplace learning is the actual learner. Within a community of practice, every member of the community is a potential learner. Conceptually, individual learners are part of the social system of a workplace, but they deserve to be discussed as individuals with unique characteristics and ways of doing things that shape their contribution to patient care and their role in a community of practice. Understanding some of the ways individuals differ is necessary if we are to understand workplace learning. Furthermore, the outcomes of learning and the decisions they inform apply to individuals, as much as they apply to the social systems in which they operate.
The outcomes of workplace learning depend not just on the experiences and prior knowledge learners bring, but importantly on how they use their experiences and knowledge to interpret tasks. Main influences on the interpretation of tasks are a learner’s:
Frame of reference
There is a wide range of learners in workplace settings: from medical students to trained professionals engaging in continuous professional development. In what way do those individuals differ? The literature on clinical reasoning provides part of the answer. Clinical reasoning focuses on ‘the processes doctors use to arrive at an initial diagnosis based on history and physical examination’ (Norman, 2005). Clinical reasoning is usually researched by conducting experiments that incorporate individuals with different amounts of experience. As Mylopoulos and Woods state, ‘the underlying assumption is that experts and novices differ in terms of the cognitive mechanisms that organise their knowledge and affect their decisions’ (Mylopoulos and Woods, 2009). The notion that each learner brings a unique set of capabilities to a situation that allows him or her to think, interact, and perform is called personal knowledge by Eraut (1994). To optimise workplace learning, understanding a person’s past experiences and current frames of reference help set attainable educational goals (Sandars, 2005).
Social psychology research conducted in the medical domain has shown that individuals’ personal knowledge is used selectively to interpret tasks. Depending on the situation, certain categories of personal knowledge or certain concepts are more salient than others and can potentially influence interpretations, learning, and subsequent behaviours. Teunissen et al (2009) investigated this by using a research technique from social psychology called ‘priming’. A priming effect occurs when a mental concept activated in one situation is preferentially applied in another, unrelated, situation, because its accessibility has been enhanced through that activation. Teunissen et al asked obstetric gynaecologic residents to participate in a number of ostensibly unrelated tasks. One of the experiments concerned residents’ patient management decisions. A total of 50 residents with different levels of experience were randomised to two groups and asked to participate in word tasks. This consisted of several items, each presenting a set of words. Participants were instructed to underline the words that would make a correct sentence. In one experimental condition, these ‘priming’ sentences conveyed action (e.g. ‘we deal with it’), and in the other they conveyed holding off (e.g. ‘it won’t be removed’). Subsequently, all residents were presented a paper case of a 37-year-old woman with menorrhagia (heavy menstrual bleeding) and asked to decide between a strategy of watchful waiting or hysterectomy. Being primed to act or hold off yielded significantly different responses in the decisions of year one and year two residents. The decisions of year three and year four residents showed a similar but less marked tendency. In neither experiment was an effect of priming found on residents in the final years of specialist training. Teunissen et al concluded from their experiments that, without residents being aware, context (such as an immediate prior experience unrelated to the case now at hand) influenced residents’ constructions of a work-related situation by activating mental concepts, which in turn affected how residents experienced situations. The strength of the effect in their specific example varied with residents’ levels of experience, indicating the importance of a person’s prior experience. The results show how aspects of an individual’s frame of reference can, even unconsciously, influence interpretations, learning, and behaviour. It again highlights the interplay between tasks, individuals’ frame of reference, and the physical and social context in which the task takes place.
Learners as active participants
Individuals are not just interpreters of tasks; they are also active participants who contribute to the way tasks evolve (Sheehan et al, 2005). Learners come to workplaces with certain goals and intentions in mind, which may or may not be in line with formal learning goals laid down in a curriculum. Understanding the behaviour of learners and seeing how their behaviour creates or inhibits learning opportunities and leads to learning outcomes allows teachers to guide their development by discussing and attuning goals and organising tasks in such a way that learners actually meet those goals. The work of Bandura on social cognitive theory provides a helpful perspective in understanding learners’ personal agency where notions of intentionality and forethought explain learners’ motivations to pursue hard-to-reach learning goals. For instance, medical students have to complete a range of clinical rotations in areas they will never practise in. They nevertheless know that, to reach their goal (i.e. graduate as a medical doctor), they will have to pass all rotations. Motivating students is a challenge that requires at least some knowledge of the goals and intentions individuals bring with them to a workplace. It means that clinical teachers need to know what tasks their practice offers and how those tasks can serve individuals with different learning goals. Understanding that a learner’s behaviour is partly the result of intentions and anticipated outcomes can also serve as a basis for reflection.
Emotions and physical states
Emotions pervade our lives and are therefore always part of learners’ interpretations (Illeris, 2002). They can stem from a good (or bad) working relationship within a health care team or from the emotions inherently coupled to life events such as birth, sickness, and death. According to Illeris, besides being a social and cognitive process, ‘all learning is simultaneously an emotional process […], that is, a process involving psychological energy, transmitted by feelings, emotions, attitudes, and motivations which mobilise and, at the same time, are conditions that may be influenced and developed through learning’ (Illeris, 2002). A supervisor who always makes a learner feel nervous or rushed will not encourage learning as well as one who creates an environment where questions are encouraged and positively reinforced. Moreover, there is strong evidence from laboratory studies that sleep deprivation impairs mood, cognitive, and motor performance (Pilcher and Huffcutt, 1996). The impact that learners’ physical states might have on their performance and learning is also demonstrated in research on self-efficacy. All these notions illustrate the importance of creating safe learning climates in order to encourage learning (Boor et al, 2008).
Going back to the range of learners within workplace settings, it is clear that the learning outcomes for a medical student in an outpatient clinic are very different from the medical specialist whom he or she is shadowing. The medical student has a different frame of reference with regard to clinical conditions compared to the specialist. Moreover, when working up a patient, students may be more concerned with how their performance will be assessed, guiding their (proactive) behaviours accordingly, whereas the specialist is concerned with treating the patient. And the fact that students are assessed by the specialist creates a power difference leading to emotions that can influence behaviour and learning.
Tying the three factors together; optimising learning in the workplace
We have discussed tasks, the physical and social contexts in which tasks are performed, and characteristics of the learner to explain the dynamic interplay that gives rise to workplace learning outcomes. Those factors are distinct but also highly interdependent. As a consequence, efforts to promote workplace learning can be directed to a variety of starting points, any of which may act to encourage active participation of the learner.
Intersubjectivity
Participation has beneficial consequences for individuals in that it facilitates effective learning, positive working relationships, and effective work performance. A key outcome of individuals working and communicating together effectively is the development of intersubjectivity. This means all members of a health care team understand each other’s preferences and idiosyncrasies so that they can work together without the need for constant interpersonal negotiations, which can be reserved for dealing with novel tasks or problems. Intersubjectivity doesn’t just happen and the behaviours that promote it are learnable. A person joining a team for the first time will not automatically know the preferences of other team members and misinterpretation of these preferences can alienate that person from the learning environment. This alienation can occur for experienced practitioners joining a new team but is even more probable for novice practitioners – not only does the novice have more to learn in general but also he or she must learn the skills required to detect the preferences of other team members. Add to this high levels of anxiety and it can be seen that there can be a potent mix of factors to inhibit good learning (Sheehan et al, 2005). One of the defining characteristics, or markers, of ineffective workplace learning is lack of participation. This is where a learner seems passive, unwilling to learn or just does what he or she is told (Wilkinson and Harris, 2002). One could be tempted to conclude that the problem lies solely with the learner but the previous sections have highlighted the importance of the context and task. Some contexts invite more participation than others. Research into this area has highlighted the crucial importance of the supervisor–learner relationship in enabling the acceptance of a learner and allowing the learner to participate fully in a team. This is an example of the impact of social context on individual learners; the clinical supervisor or a mentor can help a learner navigate his or her way through the initiation stages of joining a functioning team.
Promoting participation
Health care teams are naturally motivated to have as their highest priority the provision of high-quality care to their patients. Sometimes this can be at the expense of paying attention to relationships within the team. Intersubjectivity can arise in teams that have been working together for some time – but even for such teams, tensions can remain whereby some members work around others, avoid each other or undermine each other’s decisions. Intersubjectivity requires those tensions and differences to be made explicit. A new team member will experience them to an even greater degree and any lack of resolution can impact adversely on learning, particularly if that new team member is a novice. One solution to this is to pay attention not only to patient care but also to team tasks; sports teams do not just focus on the task (playing the game), but also on team functioning (practice). Similarly, in clinical settings, learning does not just arise from the task, but also from the team’s effective functioning.
Learners in health settings are active peripheral participants needing to integrate into a social learning environment. This integration requires actions on the part of both the learner and supervisor because neither alone can effect the transition. A reticent or unconfident learner, however, may not attract enough attention from a busy supervisor. Likewise, a supervisor who is busy or who seems aloof may make a learner feel that he or she is not allowed to seek attention. In such cases, bringing the learner into the social learning environment is more challenging and requires actions on the part of both learner and supervisor. Often this occurs in an iterative fashion – if either the learner or supervisor makes a move to show interest, the other party is more likely to reciprocate. For example, if the learner shows interest and asks pertinent questions, the supervisor will start to engage with the learner. Once the learner sees this engagement, he or she will be more likely to make more enquiries. Alternatively, it could be the supervisor who makes the first move and, provided the learner reciprocates, the supervisor will be more likely to engage further. These tentative initial steps can then build on each other in a self-reinforcing cycle. Before long, conversations begin and dialogues ensue. It is through conversing, and ‘thinking aloud’, that learners come to understand the supervisor’s idiosyncrasies and improve their clinical reasoning. It is the dialogue, the language, and the behaviours that give the experience meaning for the learner. Discussion and joint problem-solving, debate over decisions, and consideration of options are all important activities that promote participation and learning. The place of conversations around patient care, such as over morning coffee, and between all members of a team should not be underestimated as a medium for their engagement in the reciprocal process of workplace participation.
Sheehan, Wilkinson, and Billett used individual interviews and a focus group to gather data about interns’ experiences in clinical rotations within a New Zealand hospital setting. Based on their data, they drafted a model (Figure 12.1) for participation in clinical settings that identifies two critical components: the tasks of patient care and engagement with the clinical team. Those two components are further divided into two aspects: initiation and maintenance. A reinforcing cycle of activities that promote and encourage effective participation and learning results from all four factors working well.
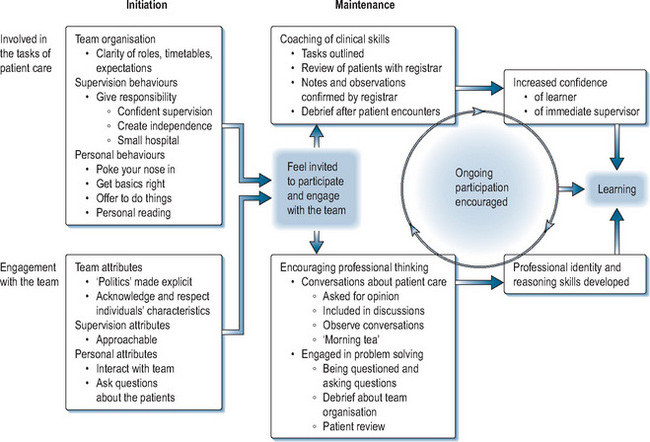
Initiation
As the Sheehan et al model also shows, one of the first steps to promote a positive learning environment is to get off to a good start by providing an effective initiation or orientation. A workplace is so familiar to supervisors that it is easy to forget it is new and foreign to most learners. Furthermore, each supervisor will have idiosyncrasies – these can be discovered by trial and error or, preferably, by discussions soon after a learner arrives into a new context. Sometimes orientation relates only to the physical environment, or to employment matters; however, to foster effective learning, it also needs to promote an early, effective supervisor–learner relationship. In practical terms, newly arrived trainees need to be provided with practical information on timetables, specific aspects of patient care related to the setting, clarification of the roles of the trainees, and a clear description of others’ expectations of their performance on the attachment. The idiosyncrasies of other team members should be made explicit. In turn, trainees are expected to be enquiring but also to show initiative by reading around problems. Once this initiation phase has been satisfactorily completed, the maintenance phase can then occur, where ongoing review and feedback relating to patient care take place alongside activities to promote and encourage interactions within the team. Attention should be paid not only to the performance of trainees in relation to patient care but also to making time for interaction between team members, thus highlighting the significance of co-participation in workplace learning.
Team interactions
The importance of interactions between team members in promoting learning is well recognised. Richards, when discussing learning from physician colleagues, observed that self-directed, workplace learning involved more interactions with colleagues than did formal learning (Richards, 1986). Jennett et al (1988) tested the effectiveness of a range of teaching methods in continuing medical education and found that those involved in small group discussions with peers learnt significantly better. Modelling by a respected peer has a positive effect (Stross et al, 1983). Studies in occupational therapy show that debriefing with peers in fieldwork practice helps learners appraise themselves and discuss confusing issues (Mackenzie, 2002). Studies in nursing reveal that similar practices boost confidence to apply knowledge and skills (Davies, 1995). These studies all provide evidence that interactions with peers or more experienced counterparts combine with everyday practice to promote learning on the job.
A communication hierarchy, which can arise if there are too many people in a team, can be a barrier to engagement; for example, when a medical student’s learning needs have to take lower priority than the learning needs of more senior staff. Despite this, a learner’s passive observation still has a place. Observing the practice of others or listening to other team members puzzling over a problem can be a valuable learning experience, provided the learners still feel entitled to be present as Lave and Wenger’s ‘legitimate peripheral participants’ (Lave and Wenger, 1991). This learning opportunity can be capitalised on further by discussing the role of the novice student in advance and agreeing a limited set of topics for debriefing afterwards. For students, this turns a passive meeting into an active learning opportunity (Irby and Wilkerson, 2008).
Effective feedback
Drawing upon apprenticeship learning, Collins and Newman devised a model of learning for reading, writing, and mathematics that they termed cognitive apprenticeship (Collins et al, 1989). According to their model, the expert (a teacher) modelled, coached, and scaffolded the learner before withdrawing support incrementally until the learner could achieve independent performance. This approach is clearly analogous to practices proven to be successful in medicine and gives a central role to effective feedback in guiding learners’ development. Ende stresses that formative feedback is a tool to keep learners on course and involved and suggests that, without it, ‘the sense of being adrift in a strange environment is amplified’ (Ende, 1983). Irby emphasises that such feedback requires interactive thinking and improvisation by supervisors because they must simultaneously identify a patient’s problems and their learners’ levels of understanding. He notes that excellent teachers ‘incorporate the whole team in discussion’ (Irby, 1992). Able clinicians and teachers can also include the patient as part of this whole team.
Several reviews and meta-analyses show that providing learners with effective feedback is difficult. Up to 38% of studies of the effect of feedback show negative effects on performance (Kluger and DeNisi, 1996). Hattie and Timperley (2007) published a synthesis of 12 meta-analyses (consisting of 196 studies and 6972 effect sizes) on the effectiveness of feedback. Their synthesis shows that feedback can only build on previous experience. So if a task is new to a learner, instructions will be more important than letting them try and then giving feedback on what went right and wrong. When giving feedback, both learners and teachers should bear in mind that the verbal and non-verbal information contained within feedback can be targeted at different levels with different results. In general, effective feedback is directed at tasks or parts of tasks and not at the person performing the task. For example, giving feedback to a resident who has just finished doing rounds should focus on concrete examples of what the resident did. Such feedback can often be preceded by asking the resident to explain to the supervisor the considerations that were weighed up before deciding on a plan of action. Understanding the reasoning behind decisions helps with the coaching of clinical reasoning. When there seems to be a recurrent problem with running late on rounds, the teacher can also focus on what it takes to strike a balance between paying attention to individual patients and being fair to the whole group of patients. Such comments give the resident insight in what went well and what can be improved. On the other hand, either positive or negative general comments such as ‘You’re good in doing rounds’ or ‘You’re too slow, you should speed up your rounds’ is ineffective as feedback (Hattie and Timperley, 2007). Such comments do not provide any clues as to what to keep doing or what actions should be changed. So, effective feedback provides timely, concrete suggestions on what to keep doing and on what to change. It helps learners to see where they are going, how they are getting on, and where they want to aim for next.
Formative feedback paired with reflection is even more powerful as this allows the assimilation and reordering of concepts and a consideration of meaning. The exploration of the meaning and implications of experiences and action in the hands of the skilled facilitator keeps discussions on higher levels, avoiding the repetition of mundane facts and more importantly growing team understanding and cohesion (Branch and Paranjape, 2002). The skills involved in these tasks should not be underestimated and have important implications for faculty development. A good doctor is not automatically a good teacher or provider of feedback. Likewise, reflection may not occur automatically for new practitioners. While reflection can be a self-directed, private activity, it is also a cognitive process that can be modelled and promoted by supervisors and mentors.
Conclusion
This chapter has discussed clinical workplaces as learning and teaching environments. Essentially, all workplaces present those working in them, from seasoned professionals to those who have just entered them, with an overwhelming range of learning opportunities. The nature of a particular workplace will influence learning objectives, processes, and outcomes; large parts of what workers learn will be overt and not marked as learning. Because of workplaces’ unique abilities to offer learners opportunities to learn in a context very similar to the one in which they will ultimately function, medical training will always be partly situated in the clinical workplace. There are some specific features of clinical workplaces that set them apart from in-school medical education; learning in health care workplaces requires the negotiation of a three-way teacher–learner–patient relationship and, because the clinical workplace’s main purpose is patient care, educational processes and outcomes are harder to control.
The features of learning and teaching in clinical workplaces make this a research area that can be analysed through many different theoretical lenses. This book offers numerous perspectives relevant to workplace learning and this chapter has discussed in more detail ‘concepts around informal learning’, ‘social cognitive theory’ including self-efficacy as a driver of learners’ proactive behaviour in workplaces and ultimately their learning, and ‘communities of practice theory’, including legitimate peripheral participation as a descriptor of learners’ participation. To put different theoretical angles into perspectives and allow readers to analyse any workplace, workplace learning has been broken down into three constituent parts: ‘tasks’, ‘contexts’, and ‘learners’. Understanding the importance of what tasks people participate in is crucial to workplace learning. After doing so, it becomes possible to look at the way in which teams share tasks and different individuals within them interpret tasks. The social and physical context in which tasks are performed is an often overlooked but crucial component of understanding workplace learning and teaching. Finally, there are individual influences on the interpretation of tasks, such as a learner’s frame of reference, his role as an active participant in a community, and his emotions and physical states.
Implications for practice
First and foremost, in letting learners participate in health care teams it is crucial that patients’ needs are attended to. Understanding some of the workings of workplaces allows for an attempt to optimise workplaces as educational environments. This chapter discussed the importance of creating intersubjectivity, where learners are part of a team whose members understand each other’s preferences and idiosyncrasies so that working together can occur without the need for constant interpersonal negotiations. If done properly, this will stimulate meaningful learning, some of which will be overt. Aspects of workplace learning and teaching may benefit from making more explicit what is being done and why. In doing so, understanding a person’s past experiences and current frame of reference will help in optimising workplace learning. Overall, the opportunities for engagement afforded to learners and the way in which they choose to participate will influence the quality of a workplace as a learning environment. In the current landscape of medical education where teaching hospitals need to balance the training of a large number of future health professionals with providing cost-effective health care, more research on what opportunities lead to what kind of learning outcomes would be particularly valuable.
High-quality workplace education can be achieved through meaningful participation, which in turn requires learners to be initiated with care within a workplace and its community of practitioners. In practical terms, newly arrived trainees should be provided with practical information, clarification of their roles as trainees, and a clear description of what is expected of them. When the initiation phase is over, ongoing learning opportunities and engagement with different members of a community of practice will stimulate ongoing engagement, commitment, and motivation. These processes relate strongly to the confidence trainees need to develop in their capabilities; tackling challenging tasks will be easier when learners feel appropriately supported in doing so. Making space for informal dialogues, including learners within the team, and promoting effective (not simply positive) feedback, will stimulate team interaction and add to the learning potential of workplaces. Ultimately, workplace learning boils down to people showing a genuine interest in each other, their development as practitioners, and their patients.
Bandura A. Self-efficacy. Ramachaudran V.S., editor. Encyclopedia of human behavior, vol 4. New York: Academic Press. 1994:71-81.
Bandura A. Self-efficacy. The exercise of control. New York: W.H. Freeman and Company, 1997.
Bandura A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. 2001;52:1-26.
Bandura A. Guide for constructing self-efficacy scales. In: Urdan T., Pajares F., editors. Self-efficacy beliefs of adolescents. Greenwich, CT: Information Age Publishing; 2005:307-337.
Billett S. Learning in the workplace: reappraisals and reconceptions. In: Hayward G., James S., editors. Skills, knowledge and organisational performance. Bristol: Policy Press; 2004:149-170.
Billett S. Workplace participatory practices: conceptualising workplaces as learning environments. J Workplace Learn. 2004;16(6):312-324.
Billett S. Constituting the workplace curriculum. J Curricul Stud. 2006;38:31-48.
Bleakley A. Broadening conceptions of learning in medical education: the message from teamworking. Med Educ. 2006;40(2):150-157.
Boor K., Scheele F., van der Vleuten C.P., et al. How undergraduate clinical learning climates differ: a multi-method case study. Med Educ. 2008;42(10):1029-1036.
Branch W.T.Jr., Paranjape A. Feedback and reflection: teaching methods for clinical settings. Acad Med. 2002;77(12):1185-1188.
Cheetham G., Chivers G. Professions, competence and informal learning. Cheltenham, UK: Edward Elgar, 2005.
Collins A., Brown J.S., Newman S.E. Cognitive apprenticeship: teaching the crafts of reading, writing and mathematics. In: Resnick L.B., editor. Knowledge, learning and instruction, essays in honor of Robert Glaser. Hillsdale, NJ: Erlbaum & Associates; 1989:453-494.
Davies E. Reflective practice: a focus for caring. J Nurs Educ. 1995;34(4):167-174.
Deketelaere A., Kelchtermans G., Struyf E., et al. Disentangling clinical learning experiences: an exploratory study on the dynamic tensions in internship. Med Educ. 2006;40(9):908-915.
Dornan T.L., Boshuizen H.P., King N., et al. Experience-based learning: a model linking the processes and outcomes of medical students’ workplace learning. Med Educ. 2007;41(1):84-91.
Dornan T.L., Boshuizen H.P., Gick R., et al. A review of the evidence linking conditions, processes and outcomes of clinical workplace learning. BEME Collaboration. 2009. Available at: http://www.bemecollaboration.org/beme/files/reviews%20in%20progress%20docs/Dornan%20Protocol.pdf Accessed September 2009
Ende J. Feedback in clinical medical education. JAMA. 1983;250(6):777-781.
Eraut M. Developing professional knowledge and competence. London: RoutledgeFalmer, 1994.
Eraut M. Informal learning in the workplace. Stud Conti Educ. 2004;26(2):247-273.
Eraut M., Alderton J., Cole G., et al. The development of knowledge and skills at work. Coffield F., editor. Differing visions of a learning society, vol I. Bristol: Policy Press. 2000:231-262.
Eva K.W., Regehr G. Knowing when to look it up: a new conception of self-assessment ability. Acad Med. 2007;82(10):S81-S84.
Fuller A., Unwin L. Learning as apprentices: creating and managing expansive learning environments. J Educ Work. 2003;16(4):407-426.
Hamstra S.J., Dubrowski A., Backstein D. Teaching technical skills to surgical residents: a survey of empirical research. Clin Orthop Relat Res. 2006;449:108-115.
Hatala R.A., Norman G.R., Brooks L.R. Influence of a single example on subsequent electrocardiogram interpretation. Teach Learn Med. 1999;11(2):110-117.
Hattie J., Timperley H. The power of feedback. Rev Educ Res. 2007;77(1):81-112.
Illeris K. The three dimensions of learning. Contemporary learning theory in the tension field between the cognitive, the emotional and the social. Roskilde, Denmark: Roskilde University Press, 2002.
Irby D.M. How attending physicians make instructional decisions when conducting teaching rounds. Acad Med. 1992;67(10):630-638.
Irby D.M. What clinical teachers in medicine need to know. Acad Med. 1994;69(5):333-342.
Irby D.M., Wilkerson L. Teaching when time is limited. BMJ. 2008;336(7640):384-387.
Jennett P.A., Laxdal O.E., Hayton R.C., et al. The effects of continuing medical education on family doctor performance in office practice: a randomized control study. Med Educ. 1988;22(2):139-145.
Kluger A.N., DeNisi A. The effects of feedback interventions on performance: historical review, a meta-analysis and a preliminary feedback intervention theory. Psychol Bull. 1996;119:254-284.
Lave J., Wenger E. Situated learning: legitimate peripheral participation. Cambridge: Cambridge University Press, 1991.
Lempp H., Seale C. The hidden curriculum in undergraduate medical education: qualitative study of medical students’ perceptions of teaching. BMJ. 2004;329(7469):770-773.
Lyon P.M. A model of teaching and learning in the operating theatre. Med Educ. 2004;38(12):1278-1287.
Mackenzie L. Briefing and debriefing of student fieldwork experiences: exploring concerns and reflecting on practice. Aust Occup Ther J. 2002;49(2):82-92.
Mylopoulos M., Woods N.N. Having our cake and eating it too: seeking the best of both worlds in expertise research. Med Educ. 2009;43(5):406-413.
Norman G.R. Research in clinical reasoning: past history and current trends. Med Educ. 2005;39(4):418-427.
Pajares F. Current directions in self-efficacy research. Maehr M.L., Pintrich P.R., editors. Advances in motivation and achievement, vol 10. Greenwich, CT: JAI Press. 1997:1-49.
Pilcher J.J., Huffcutt A.I. Effects of sleep deprivation on performance: a meta-analysis. Sleep. 1996;19(4):318-326.
Polanyi M. Personal knowledge: towards a post-critical philosophy. Chicago: University Of Chicago Press, 1974.
Reber A.S. Implicit learning and tacit knowledge: an essay in the cognitive unconscious. Oxford: Oxford University Press, 1993.
Remmen R. An evaluation of clinical skills training at the medical school of the University of Antwerp. Belgium: University of Antwerp, 1999.
Richards R.K. Physicians’ self-directed learning: a new perspective for continuing medical education III. Phys Self-Dir Learn Proj Mobius. 1986;6(4):1-14.
Rogoff B. Apprenticeship in thinking. Cognitive development in social context. New York: Oxford University Press, 1990.
Rogoff B. Observing sociocultural activities on three planes: participatory appropriation, guided appropriation, and apprenticeship. In: Wertsch J.V., Del Rio P., Alvarez A., editors. Sociocultural studies of mind. Cambridge: Cambridge University Press; 1995:139-164.
Sandars J. An activity theory perspective. Work Based Learn Prim Care. 2005;3(3):191-201.
Sheehan D., Wilkinson T.J., Billett S. Interns’ participation and learning in clinical environments in a New Zealand hospital. Acad Med. 2005;80(3):302-308.
Slotnick H.B. How doctors learn: physicians’ self-directed learning episodes. Acad Med. 1999;74(10):1106-1117.
Slotnick H.B. How doctors learn: education and learning across the medical-school-to-practice trajectory. Acad Med. 2001;76(10):1013-1026.
Stross J.K., Hiss R.G., Watts C.M., et al. Continuing education in pulmonary disease for primary-care physicians. Am Rev Respir Dis. 1983;127(6):739-746.
Swanwick T. Informal learning in postgraduate medical education: from cognitivism to ‘culturism’. Med Educ. 2005;39(8):859-865.
Tan N. Learning in surgery: practice meets theory. Clin Teacher. 2009;6(1):34-37.
Teunissen P.W., Scheele F., Scherpbier A.J.J.A., et al. How residents learn: qualitative evidence for the pivotal role of clinical activities. Med Educ. 2007;41(8):763-770.
Teunissen P.W., Stapel D.A., Scheele F., et al. The influence of context on residents’ evaluations: effects of priming on clinical judgment and affect. Adv Health Sci Educ Theory Pract. 2009;14(1):23-41.
Wenger E. Communities of practice: learning, meaning, and identity. Cambridge: Cambridge University Press, 1998.
Wilkinson T.J., Harris P. The transition out of medical school – a qualitative study of descriptions of borderline trainee interns. Med Educ. 2002;36(5):466-771.