6 Curriculum development in learning medicine
Assessment; formal That which occurs intentionally when someone comes to a view about someone’s (possibly that person’s own) learning, irrespective of what use (formative or summative) is to be made of that assessment.
Assessment; formative Assessment designed to help individuals develop by giving them information on their performance, usually in a non-judgemental and low-stakes environment (has no consequences in terms of the learner’s progress). Often termed ‘assessment for learning’ or simply feedback.
Assessment; informal That which occurs naturally and often unrecognised when someone, somehow, comes to a view about someone’s (possibly that person’s own) learning, irrespective of what use (formative or summative) is to be made of that assessment.
Curriculum (without a pronoun) That which underpins any learning and may be seen in the actions of teachers and learners in situ.
Curriculum development The commonly used term to convey the work of people (curriculum developers) engaged in creating a curriculum plan. Together, often informally, and perhaps unrecognised by them, they determine learners’ emergent educational needs.
Curriculum implementation The translation of a curriculum proposal into practice, involving people locally appreciating the contextual nature of the particular location of the curriculum.
Curriculum initiators A preferred term to ‘curriculum developers’ (see curriculum development above) which is used here to refer to people who initiate the formal development of a curriculum. Understood as such, their role is to enable curriculum development to occur locally (see curriculum development above).
Curriculum: the (or a) curriculum (i.e. with a pronoun) A plan or set of intentions, usually presented in a written form, often prepared as a document in order to guide teachers’ and learners’ actions.
Formal education That which occurs intentionally when some formal (and probably also some informal) learning happens.
Formal learning Learning that occurs within an organisation and context (formal education) that is designed for learning. Formal learning is intentional from the learner’s perspective.
Formal teaching Teaching that occurs intentionally when someone (a ‘teacher’) seeks to help another person learn something.
Informal education/learning Learning resulting from unplanned activities within an educational programme and/or daily life activities related to work, family, or leisure. It is not structured in terms of learning objectives or teaching. Informal learning may be intentional but in most cases it occurs incidentally.
Informal teaching That which occurs naturally and often unrecognised when someone (a ‘teacher’) helps another person learn something worthwhile.
Professional practice The actions and underpinning thoughts of someone intentionally engaged in helping another in some morally determined capacity, involving making judgements in that person’s best interests.
Summative assessment Coming to a view of someone’s learning for the purpose of regulating the progression of that person and/or for some form of certification.
Outline
The hundred years since the publication of Flexner’s (1910) report, particularly the last 50 years, have seen an explosion of curriculum development in medical education. In this chapter, I look critically at those changes, make some observations of my own, and end with a vision for the future. In the course of those critical observations, I offer what I see as some essential educational principles on which curriculum development should be based. The chapter is not, however, entirely theoretical. I give examples at key points in the argument. Nevertheless, I hold that medical education generally, and curriculum development in particular, needs to be based on educationally supportable principles. Quite fundamentally, any curriculum for professional practice (since this applies not just to medicine) must begin with a clear understanding of the nature of that practice. This means looking rigorously at the practice in question – researching it in ways that I describe here – from the perspective of the people most closely associated with it: practitioners themselves. Generally, this has not happened in medical education, which is the greatest weakness of many of the curricula that have emerged in recent years.
Background
A curriculum is usually thought of as an educational policy, which is often (though not necessarily) presented as a document, in
… an attempt to communicate the essential principles and features of an educational proposal in such a form that it is open to critical scrutiny and capable of effective translation into practice.
Thus, a curriculum is more than a syllabus – which is merely a list of ‘content’. A curriculum exists, whether people know it or not, in any educational event or activity. In this sense, everyday teaching, learning, and assessment are founded on there being ‘curriculum’ present.
The term ‘curriculum’… refers to all the activities, all the experiences and all the learning opportunities for which an institution, or a teacher, or a learner, takes responsibility – either deliberately or by default. This includes: the formal and the informal, the overt and the covert, the recognised and the overlooked, the intentional and the unintentional.
This leads to the notion that, in any educational enterprise, there will be various forms of a curriculum. These can include
And these ‘incarnations’ of a curriculum may look very different, not just to outside observers but also to those engaged in and with it. In other words, people perceive a curriculum from different viewpoints, and their viewpoint is greatly influenced by how they see education more generally. Put another way, people’s ‘mindset’ – their assumptions, expectations, beliefs and values about education – determines how they see, and then how they act in relation to, any curriculum. Generally, most people consider ‘the curriculum’ to be what is written down – the intentions. However, it is almost always more educationally useful to consider ‘curriculum’ as people’s reactions and responses to those intentions in their educational practice, that is through the teaching, learning, and assessing that actually happen.
These are some of the challenges that curriculum developers face. Curricula are complex – nothing about them is straightforward – which has huge implications for learning medicine. The notion that there is a simple, one-way relationship between designing a curriculum and its educational effects is, to say the least, naïve, and, at worst, dangerous. One implication is this: the traditional view of the curriculum developer (or more usually a group of people) is ‘a man with a mission’ (Stenhouse, 1975, p 120); someone who offers ‘a solution’, with a stake (often their reputation) in having found ‘the right answer’. That might not be helpful. On the hundredth anniversary of the Flexner report, have his ideas achieved fruition? Or was he simply ‘a man with a mission’?
What is the curriculum problem?
So what is the problem? In this section I offer a broad critique of both undergraduate and postgraduate medical education, particularly in the United Kingdom (UK) and North America, to establish some key implications regarding curriculum development generally.
Undergraduate medical education
Factual overload
In the UK, by the time Flexner was writing his report, a regulatory body – the General Council for Medicine (later renamed The General Medical Council or GMC for short) – had been in existence for over 50 years, and was addressing what it saw as the educational concerns of the day. In 1863 it noted:
… an overcrowding of the curriculum of education, whether as to the number of courses, or of lectures in particular courses … followed by results injurious to the student.
Thomas Huxley made the point even more forcibly in 1876:
The burden we place on the medical student is far too heavy, and it takes some doing to keep from breaking his intellectual back. A system of medical education that is actually calculated to obstruct the acquisition of sound knowledge and to heavily favour the crammer and the grinder is a disgrace.
Yet little changed, and by 1918 Newman commented that, in the United Kingdom:
The medical course [is] seriously overburdened … and too fully occupied to permit a healthy assimilation of much which the student is taught.
By the mid-1940s, a UK government report recommended ‘a ruthless pruning’ of the content, suggesting that the GMC review the curriculum. In 1947, the GMC wryly commented that they ‘could not fail to share [this] anxiety’ but regretted that they had very limited powers to effect any change, merely urging medical schools not to retain in their curricula ‘anything which it is unnecessary or premature for students to learn’ (GMC, 1947). By 1957, the GMC was becoming more assertive, challenging medical schools ‘to teach less and to educate more’, warning that
… students have tended to concentrate their attention unduly on memorising factual data. The Council feel no doubt that an effort should be made to reduce the congestion.
Yet, by the 1980s it was still saying:
We … reiterate … that the student’s factual load should be reduced as far as possible, to ensure that the memorising and reproduction of factual data should not be allowed to interfere with the primary need for fostering the critical study of principles and the development of independent thought.
Notwithstanding these repeated exhortations, there remains gross overcrowding of most undergraduate curricula, acknowledged by teachers as deplored by students. The scarcely tolerable burden of information that is imposed taxes the memory but not the intellect. The emphasis is on the passive acquisition of knowledge, much of it to become outdated or forgotten, rather than on its discovery through curiosity and experiment. The result is a regrettable tendency to under-provide those components of the course that are truly educational, that pertain to the proper function of a university and that are the hallmark of scholarship.
Inappropriate educational processes
The same observations were being made of undergraduate medical education in North America. Becker (Becker et al, 1961), in what is now recognised as a classic study, noted increasing cynicism amongst students, who responded to the amount they had to learn by ‘playing the system’; that is, finding what was immediately required of them and focusing their learning on just that. Flexner (1910, pp 60/1), though, had seen the problem not so much as overload to be reduced but as an inappropriate teaching process:
Out and out didactic treatment is hopelessly antiquated; it belongs to an age of accepted dogma … when the professor “knew” and the students “learnt.”
From the standpoint of the young student, the [medical] school … seeks to evoke the attitude, and to carry him through the processes, of the thinker and not of the parrot.
Lack of structure
Flexner saw the medical curriculum as requiring two closely related phases, which shared the same educational goal. During the first, students would learn ‘science’, though not necessarily through lectures or from books but in what Flexner (1910, p 92) referred to as ‘the laboratory’.
… a place constructed for the express purpose of facilitating the collection of data bearing on definite problems and the initiation of practical measures looking to their solution.
The second period was to be spent in the clinic – which he also saw as a kind of laboratory:
Certain conclusions as to clinical teaching follow. The student is to collect and evaluate facts. The facts are locked up in the patient. To the patient, therefore, he must go … That method of clinical teaching will be excellent which brings the student into close and active relation with the patient: close, by removing all hindrance to immediate investigation; active, in the sense, not merely of offering opportunities, but of imposing responsibilities.
Lack of integration
In the United Kingdom, however, the GMC became more and more critical of what it called ‘the pre-clinical/clinical divide’, with:
… each part of the course proliferating without the moderating influence of the other and without a co-ordinated examination of the overall aims of the course.
Indeed, the second half of the century saw two broad attempts in both the United Kingdom and North America to solve what was now being seen as the relevance problem. Both involved a form of integration – horizontal and vertical. Horizontal integration focused on the study of bodily systems rather than separate ‘pre-clinical’ disciplines; for example at Case Western Reserve medical school in the United States of America. This initiative ‘shook the world of medical education for some years to come’ (Williams, 1980):
In the struggle for faculty receptivity. there were times when brave men of goodwill and high hope felt like sitting down and crying … Experience in the pursuit of integrated systems teaching … would appear to be less a confirmation of the practicability of using the total human organism as a unifying concept of a system of education than of its value as a means of stimulating a faculty to raise its sights from the service of professional self interest to the service of students in their education.
Indeed, integrating the content in this way had little effect on how students approached their learning:
The first two years of the curriculum remain a largely passive learning experience, keyed to the lecture method of instruction. The advent of the ‘new’ curriculum … with its apparent increase in ‘free time’ concomitant with a 50% reduction in planned exercises, in fact largely resulted in the elimination of the laboratory … leaving the absolute number of hours devoted to lectures unchanged.
Similar problems were experienced at a horizontally integrated medical school in the United Kingdom (Coles, 1985) – the content was changed but not the educational process.
Lack of relevance; the advent of PBL
The second innovation, again an attempt to address the relevance problem, started in the mid 1960s at McMaster Medical School in Canada by relating theoretical teaching more closely to clinical experience, through an educational process called ‘problem-based learning’ (PBL):
[The doctor] is never told … ”there is a patient out there with liver disease. You had better read up on it before the patient comes in.” He must deal with the problem always initially as an unknown, as a stimulus for developing his problem solving skills and as a focus to determine what is the relevant learning in the basic sciences and the clinical sciences in medicine.
PBL typically presents learners, particularly in the pre-clinical years, with a paper-based clinical problem, and provides opportunities for them to explore what they need to learn in order to understand the problem. Students generally work in small groups (with or without a faculty member acting as a facilitator to help their discussions), supported in their learning by resource materials and other educational facilities such as libraries and laboratories. Where PBL has been introduced, there are few lectures or time-tabled large-group activities.
Perhaps ironically, the educational processes introduced through PBL reflect many of the views of Flexner and his contemporaries in the early part of the twentieth century such as Dewey in North America and Whitehead in the United Kingdom (see Doll, 1993, Chapter 6), with their emphasis on problem-solving, reflection, small group teaching, and the use of teachers as facilitators of learning (rather than transmitters of information), and encouraging in learners, as Flexner put it, ‘the attitude…of the thinker and not of the parrot’. Was PBL, then, a reincarnation of Flexner’s notion of the patient – what he called ‘the case’ – being the ‘laboratory’ for medical student learning? He had, after all, noted in 1910 that:
Some ingenious Harvard men, profiting by the experience of the Harvard law school, have evolved an effective discipline in the art of inference … ”Let us assume such and such a data: what do they mean? What would you do?” This is the essence of the case method, a method … calculated there to develop the friction, competition, and interest which are powerful pedagogical stimulants.
(pp 98/9)
Criticisms of PBL
PBL has shown many gains, for example, in how students approach their studying (Coles, 1985), but it has not been without its critics in its 50-year history. A study of graduates entering clinical practice questioned whether they had sufficient ‘basic knowledge’, recommending that this should be given ‘more attention in the curriculum’ (Woodward and Ferrier, 1983). Another found that students in a problem-based curriculum covered up their inadequacies in an attempt to deceive others that they were competent, as at conventional medical schools (Haas and Shaffir, 1982). Gale (1980) noted that problem-based learning:
… leaves the question of structure open. The organising agents … are not identified, thus no conclusions may be drawn about the structural properties of knowledge acquired through such learning.
A similar criticism saw little fundamental difference between what was called ‘traditional’ PBL and conventional programmes, which:
In short, traditional PBL fails to address the relevance problem because it retains the conventional curricular separation of the pre-clinical and clinical phases – a discredited view of learning as ‘preparation’ for later practice, in that it isolates ‘understanding’ from ‘action’ (Fish and Coles, 2005, p 155). Margetson (1999, pp 362 and 363) added that the ‘problems’ – the ‘cases’ in PBL – that form the basis for students’ learning are no more than what he called ‘convenient pegs on which to hang the coat of basic science knowledge which students [are deemed to] need to acquire’. This, he argued, perpetuates an atomistic view of medical education in three ways:
For Margetson, the weakness of problem-based learning curricula of this ‘traditional’ kind is that it fails to recognise that:
Human action … makes no sense apart from understanding: rather, action raises questions of the extent of understanding and its soundness.
As Schön put it, effective education requires:
Others make the same criticism that solving paper-based cases involves ‘a significantly different process from that involved in diagnosing and managing real patients’ (Rikers et al, 2004, p 1041). Margetson’s solution – what he called a ‘rigorously problem based’ curriculum – requires a ‘thorough integration of understanding (in the widest sense), knowledge and skill’ (Margetson, 1999, pp 363 and 364), which he argued could occur only in clinical practice. PBL has some merits that are sufficiently appealing to contemporary curriculum developers to make it an attractive option for undergraduate medical education. However, it may ‘work’ for other reasons – for example, ‘integration’ has been shown to occur under those curricular circumstances where learners see more clearly why they need to know what they are being taught – that is, when their ‘understanding’ and their ‘action’ are brought together (Coles, 1985). In short, PBL may not be the only way to achieve integration (Coles, 1990).
Postgraduate medical education
Preparedness for practice
In one sense, the ‘curriculum problem’ in undergraduate medical education was, by the end of the century following the publication of the Flexner report, appearing not to be the consequence of content overload, nor of relevance, nor resolved by making the educational processes more ‘learner centred’, nor by students learning the basic sciences through a ‘case study’ approach. The question curriculum developers were now being posed was more pragmatic: does the undergraduate curriculum prepare students well enough for clinical practice? In the United Kingdom these concerns, still the subject of the GMC’s current review of the medical school curriculum (GMC, 2009), were being voiced over 40 years ago:
The undergraduate medical course does not provide sufficient training for the immediate practice of medicine.
Todd Report (1968) in GMC (1993, p 5)
A 100 years ago, Flexner reported that graduating doctors in North America generally had poor levels of understanding, which required:
… an effort to mend a machine that was pre-destined to break down…to do what the medical school had failed to accomplish.
(p 174)
… the young physician already involved in responsibility should acquire the practical technique which the medical school had failed to impart … aimed pre-eminently to teach the young doctor what to “do.”
(p 174)
In the United Kingdom, the tradition was that medicine was learnt chiefly through what was called ‘an apprenticeship’:
… learning to be the professional by practising the profession under conditions of supervision and careful selection of appropriate levels of independent responsibility to meet them.
Dangers were seen in this, however, and by the middle of the twentieth century, it was noted in the United Kingdom that:
Some [newly qualified doctors] undertook posts as resident house officers where they carried out surgical operations and gave anaesthetics without supervision. Although many made it their business to acquire a sound training in the specialty of their choice, postgraduate education was unstructured and … there was no certification of its satisfactory completion.
Structuring postgraduate education
A first step towards structuring postgraduate education came in 1953 with the introduction in the United Kingdom of the ‘pre-registration year’ following graduation from medical school (see GMC, 1993, p 5). Even so, 20 years later a Royal Commission reported:
… all too often the graduate is treated as a much needed extra pair of hands rather than a probationer doctor still requiring supervision and training at a significant point in his career. Some young doctors find themselves burdened with responsibilities they are not yet in a position to assume; others are given duties not necessarily relevant to their training needs.
It was then established that, following the pre-registration year …
Competency-based education
Recently, a further reorganisation was introduced under the title Modernising Medical Careers (Department of Health, 2004) or MMC for short. This marked a highly significant shift in postgraduate medical education in the United Kingdom:
Reform had been long overdue … The apprenticeship model … now needs to be set within efficiently managed, quality assured training Programmes.
Progress [as a doctor in training] will be achieved through the acquisition of competencies and the knowledge underpinning them’.
(2004, p 8)
What was being promoted, however, was (perhaps unwittingly) a particular form of education:
Modernising Medical Careers [has] signalled a move to competency-based training throughout the medical continuum.
(2004, p 12)
We will support and encourage … the Royal Colleges to develop competency-based training and assessment.
(2004, p 7)
What, then, is ‘competency-based training’? It is an educational movement that was strong in the United States of America in the 1970s and 1980s, though it never caught on in the United Kingdom at that time. Its major claim was (and still is) in relation to vocational (i.e. sub-degree) programmes that lead to technical qualifications. Educationists argue, however, that the competency-based approach is reductionist and instrumental, an attempt:
… to reduce educational practice to a kind of ‘making action’ through which some raw material can be moulded into a pre-specifiable shape.
Whereas, educationists agree that:
… the sum of what professionals do is far greater than any parts that can be described in competen[cy] terms.
A list of competencies cannot do justice to the quality and depth of thinking associated with the ‘educated person’, namely, the serious engagement with ideas, the struggle to make sense, the entry into a tradition of thinking and criticism.
Flexner held the same view, arguing that the technician:
… deals mainly with measurable factors … Uncertainty is within fairly narrow limits. [Whereas] the reasoning of the [doctor] is much more complex. He handles at one and the same time elements belonging to vastly different categories: physical, biological, psychological elements are involved in each other … Between the young graduate in medicine and his ultimate responsibility – human life – nothing interposes … The training of the doctor is therefore more complex and more directly momentous than that of the technician.
More seriously, by pursuing a competency-based approach MMC may be changing contemporary medical education into a form of technical training:
[This] new way of thinking about the relation of teacher and learner … employs different metaphors, different ways of describing and evaluating educational activities. In doing so, it changes those activities into something else … Once the teacher ‘delivers’ someone else’s curriculum with its precisely defined ‘product’, there is little room for that transaction in which the teacher … responds to the needs of the learner. When the learner becomes a ‘client’ or ‘customer’, there is no room for the traditional apprenticeship into the community of learners. When the ‘product’ is measurable ‘targets’ on which ‘performance’ is ‘audited’, then little significance is attached to the ‘struggle to make sense’.
What is the purpose of a medical curriculum?
This shift towards seeing medicine as a technical matter has been counterbalanced by others who suggest it is:
… esoteric, complex and discretionary in character: It requires theoretical knowledge, skill, and judgement that ordinary people do not possess, may not wholly comprehend and cannot readily evaluate. Furthermore, the kind of work they do is believed to be especially important for the well-being of individuals or of society at large … It is the capacity to perform that special kind of work which distinguishes those who are professional from most other workers.
Wilfred Carr (1995, pp 68/9), an educationist, captures the same point:
To ‘practise’ … is always to act within a tradition, and it is only by submitting to its authority that practitioners can begin to acquire the practical knowledge and standards of excellence by means of which their own practical competence can be judged.
Though he adds, hinting at a fundamental principle in professional education:
… the authoritative nature of a tradition does not make it immune to criticism. The practical knowledge made available through tradition is not mechanically or passively reproduced: it is constantly being reinterpreted and revised through dialogue and discussion about how to pursue … the tradition. It is precisely because it embodies this process of critical reconstruction that a tradition evolves and changes rather than remains static or fixed.
Golby and Parrott (1999, pp 3 and 9) similarly comment:
A practice exists whenever a more or less settled body of activities is carried out to some distinctive end … What people do within a practice, the activities they engage upon, are … intelligible only by reference to … the tradition of conduct of which they are part.
Adding that a ‘tradition of conduct’ is …
… made up of contemporary practitioners who are in turn related to predecessors who have bequeathed their practice. When we engage in the characteristic activities of a practice, therefore, we are disciplined by its standards as represented by our peers and our predecessors. These standards are both technical and moral; they concern both the ‘how to’ and the ‘why’ of practice.
Gawande (2002, p 4) says this:
Medicine is … a strange and in many ways disturbing business … What you find … is how messy, uncertain and surprising [it] turns out to be … These are the moments in which medicine actually happens.
Medicine (like education) is a complex professional practice. Doctors (and teachers) must deal appropriately not just with routine situations but more particularly with the situations of uncertainty that occur unpredictably. In short, they must learn to exercise judgement:
… that form of wise and prudent judgement which takes account of what would be morally appropriate and fitting in a particular situation … not ‘right’ action in the sense that it has been proved to be correct [but] ‘right’ action justified as morally appropriate to the particular circumstances in which it was taken.
Professionals, then, must learn to decide what is ‘best’ for individuals in the circumstances in which they are found, rather than what is ‘right’ in some absolute sense (Tyreman, 2000). What knowledge does this require? Looked at from an educational perspective, the knowledge base is highly diverse:
Medical decision making … is often presented only as the conscious application to the patient’s problem of explicitly defined rules and objectively verifiable data … Seasoned practitioners also apply to their practice a large body of knowledge, skills, values and experiences that are not explicitly stated by or known to them. This knowledge may constitute a different kind of evidence, which also has a strong influence on medical decisions.
As Gawande (2002, pp 4 and 7) puts it:
We look for medicine to be an orderly field of knowledge and procedure. But it is not. It is an imperfect science, an enterprise of constantly changing knowledge, uncertain information, fallible individuals, and at the same time lives on the line. There is science in what we do, yes, but also habit, intuition and sometimes plain old guessing.
Fish and de Cossart (2005, 2007) argue that the doctor first determines what is the right thing to do generally – such as arriving at a differential diagnosis – largely based on bio-medical knowledge, which can be relatively easily taught, learnt, and assessed. The doctor then moves (often imperceptibly and very quickly) towards deciding what the best thing to do is in the particular instance:
Good [practice] is entirely dependent on what Aristotle calls phronesis, which we would translate as ‘practical wisdom’. Phronesis is the virtue of knowing which general ethical principle to apply in a particular circumstance. For Aristotle, phronesis is the supreme intellectual virtue and an indispensible feature of practice. The phronimos – the man of practical wisdom – is the man who sees the particularities of his practical situation in the light of their ethical significance and acts consistently on this basis. Without practical wisdom … ‘good practice’ becomes indistinguishable from instrumental cleverness.
A 100 years ago Flexner argued that the practice of medicine – its ‘doing’ – was underpinned by two quite different kinds of knowledge:
The practitioner deals with facts in two categories. [The sciences] enable him to apprehend one set; [but] he needs a different apperceptive and appreciative apparatus to deal with the other, more subtle elements … The physician’s function is fast becoming social and preventative, rather than individual and curative. Upon him society relies to ascertain, and through measures essentially educational to enforce, the conditions that prevent disease and make positively for physical and moral well-being.
(p 26)
Flexner’s ideas were based, then, not on the ‘facts’ of science but its approaches:
What educational models cultivate the educated practitioner?
How then might this ‘type of doctor’ become ‘educated’? Stenhouse described three possible educational models, which he termed ‘product’, ‘process’, and ‘research’ (Table 6.1).
Table 6.1 Three educational models after Stenhouse (1975)
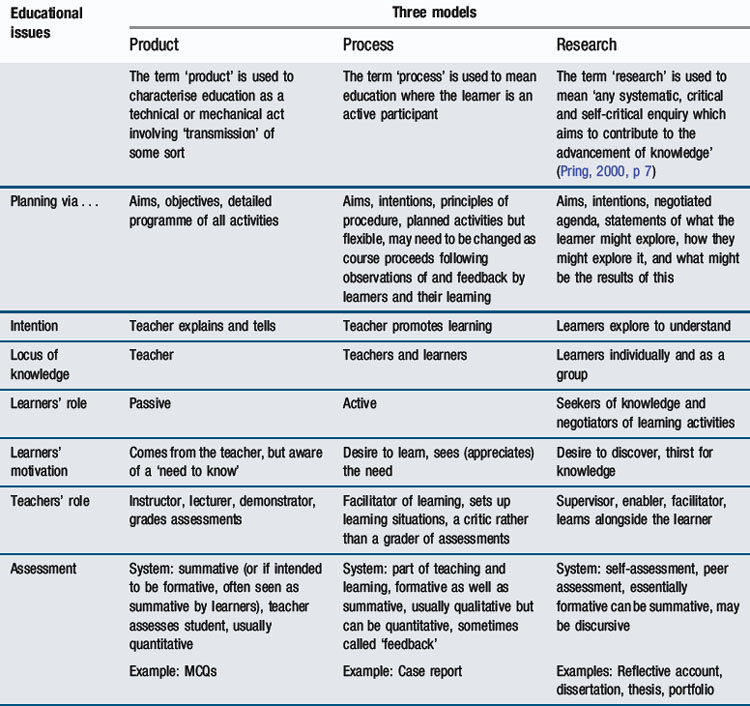
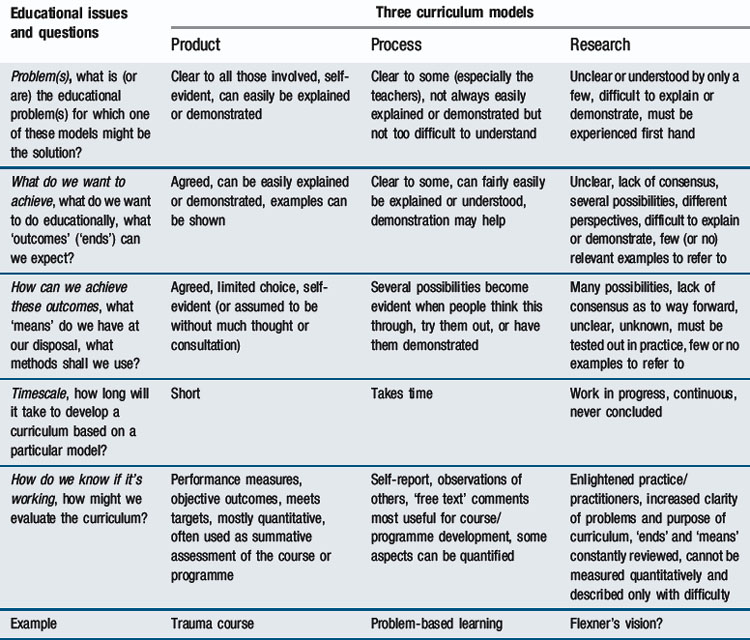
Experienced medical teachers at all levels will be familiar with these approaches. On occasions, the ‘product’ approach seems appropriate – when one needs to instruct someone about something. On another occasion, directly ‘telling’ people things would be inappropriate (and probably ineffectual). Then teachers help learners to work things out themselves. This is Stenhouse’s notion of ‘process’. In yet another setting, the teacher’s role would be to supervise a learner’s enquiry. This is the essence of the ‘research’ approach. Similarities will be apparent between the product versus process/research distinction and the contrast drawn between acquisition versus participation metaphors for learning in Chapter 2. The significance of Table 6.1, however, goes beyond this. It represents not simply ‘teaching approaches’ but ‘educational models’ – coherent views of education that are not just practically but logically distinct from one another. As the Table shows, the three models indicate not only what teachers do but define their relationship with learners and indicate the nature of other elements of the educational process such as how planning and assessment differ depending on the model chosen. The wise teacher works imperceptibly in all three models, drawing on each for particular educational purposes. The concepts contained within a particular model reflect a way of looking at education, an educational ‘mindset’. Indeed, they can be thought of as the basis of curriculum models, as shown in Table 6.2.
An example of where a ‘product’ model could be appropriate as a basis for a curriculum is in ‘trauma’ courses, where it is vital that all those involved in patient care know precisely what is expected of them and of everyone else. The ‘product’ model is appropriate for ‘training’ – in situations where, if something happens, there is the ‘right’ (i.e. an agreed) thing to do. However, such forms of practice are rare in medicine. Even ‘trauma’ requires ‘triage’, which involves ‘judgement’. Indeed, a curriculum based on the ‘product’ model was the kind of teaching and assessing that Flexner found abhorrent, and probably led to the problems of ‘overload’ and lack of ‘relevance’. Current approaches to postgraduate medical education in the United Kingdom, namely those based on a ‘competency-based’ formulation, also reflect a ‘product’ curriculum. A process model would be appropriate where the curricular intention is to help people understand what is being taught. That is the educational basis of ‘learner-centred’ and problem-solving approaches. What Margetson characterised as ‘traditional PBL’ reflects this model, as does an ‘apprenticeship’ approach to postgraduate medical education, where, although in both cases the teacher acts as a facilitator of the learner’s learning, the teacher can remain the primary focus (and often the determiner) of what is taught, learnt, and assessed. Whilst this may appear ‘learner centred’, it might constrain learners and their learning.
The research approach is harder to depict, yet is probably the most appropriate curriculum model for learning medicine at any level. It does not mean that learners undertake research projects. What Stenhouse had in mind was, as Pring (2000, p 7) more recently put it:
… any systematic, critical and self-critical enquiry which aims to contribute to the advancement of knowledge.
In a curricular context, it is the learner’s knowledge that is to advance. A medical curriculum based on a research model, then, is one that engages learners in ‘researching’ their clinical practice. The ‘knowledge’ bound up in that practice is unearthed by the learners, not ‘taught’ prior to engaging in practice. Some of this ‘unearthed knowledge’ will be bio/psycho/social ‘facts’. More will be ‘discovered’ through the action of practising and reflecting on that action. This will include ‘professional judgement’, ‘practical wisdom’, and ‘the traditions of practice’ – those higher-order forms of knowledge noted earlier to underpin professional practice. Indeed, ‘practice’ has its own inherent curriculum (Fleming, 2010), lying dormant (its nature and potential often under-recognised) in every practice encounter yet capable of being rendered ‘known’ in some form through appropriate forms of deliberation (Fish and de Cossart, 2007).
A research view of a medical curriculum is entirely consistent with Flexner’s vision:
We may fairly describe modern medicine as characterised by a severely critical handling of experience … [It] deals … not only with certainties, but also with probabilities, surmises, theory … It knows … where certainties stop and risks begin. Now it acts confidently, because it has facts; again cautiously because it merely surmises; then tentatively, because it hardly more than hopes … Scientific medicine, therefore, has its eyes open; it takes risks consciously.
(p 53)
He added, very significantly for the discussion here:
The main intellectual tool of the [scientific] investigator is the working hypothesis, or theory, as it is more commonly called … Upon this he acts, and the practical outcome of his procedure refutes, confirms or modifies his theory … This is essentially the technique of research: wherein is it irrelevant to beside practice? … The progress of science and the … intelligent practice of medicine employ, therefore, exactly the same technique. To use it … the student must be trained to the positive exercise of his faculties; and if so trained, the medical school begins rather than completes his medical education.
(p 54)
Flexner, then, likened the thinking processes underpinning effective medical practice to ‘research’, meaning not ‘the findings’ of enquiries but ‘the ways of finding’ that researchers employ – professional practice as a form of thinking action. Carr (1995, p 71), following Aristotle, called this kind of action ‘deliberation’ or ‘deliberative reasoning’:
… in deliberative reasoning, it is always conceded that there may be more than one ethical principle … and that there is no formula for methodically determining which one should be involved in a particular practical situation … It is for this reason … that deliberation is entirely dependent on the possession of what Aristotle calls phronesis … ‘Practical wisdom’ is manifest in a knowledge of what is required in a particular moral situation, and a willingness to act so that this knowledge can take a concrete form.
He added, perhaps as a muted criticism of the current obsession with accountability:
The man who lacks phronesis may be technically accountable, but can never be morally answerable.
(1995, p 71)
Perhaps that is what Flexner had in mind when he urged medical schools:
The implementation problem
Any review of medical education over the past 100 years must inevitably conclude that a lot has been said, countless exhortations made, many recommendations formulated, innovations attempted, and radical change made; if there was ‘an answer’ – a ‘solution’ to the curriculum ‘problem’ – it would surely have been found. It is clear, however, that problems identified have not been satisfactorily resolved. Either there has been strong resistance to change or the changes introduced have not addressed the problems effectively. In short, implementation has not happened. The aspirations have not been fulfilled. Why not?
Problems with the implementation of medical curricula occur partly because developers fail to consider implementation as their task. The Flexner report, for example, says a lot about ‘what might happen’ but very little about ‘how it might happen’. Curriculum proposals largely deal with educational ‘ends’ but often omit the ‘means’ for achieving those ends. The implementation problem is also bound up, in part, with our understanding of change – and in particular, how practices change. Schön, writing in 1971, characterised the most common approach to change as what he called ‘centre-periphery’ (popularly known as ‘top-down’). This approach sees ‘implementation’ as a process of ‘diffusion’:
… depends first upon the level of resources and energy at the centre, then upon the number of points at the periphery, the length of the radii or spokes through which the diffusion takes place, and the energy required to gain a new adoption.
This fundamentally depends on:
… the level of technology governing the flow of men, materials, money and information … [and the centre’s] capacity for generating and managing feedback. Because the process of diffusion is originally regulated by the centre, the effectiveness of the process depends upon the ways in which information moves from periphery back to the centre.
(1971, p 82)
When the … system exceeds the resources or the energy at the centre, overloads the capacity of the radii, or mishandles feedback from the periphery, it fails. Failure takes the form of simple ineffectiveness in diffusion, distortion of the message, or disintegration of the system as a whole … Once new centres [at the periphery] are established, for better or worse, they pursue their disparate paths.
Examples of such failures abound in attempts to develop curricula in medical education.
More particularly, the implementation problem is a consequence of the very conceptualisation of the problem itself – as one of implementation. The word means ‘to put a plan into action’. It invites a ‘centre-periphery’ approach. Looking again at Stenhouse’s definition of curriculum with which I began this chapter, however, gives a clue to a different way forward. He speaks of the need for a curriculum proposal to be presented:
The first implication is that Stenhouse clearly puts the ‘means’ for change, not just the ‘ends’ of change, firmly on the curriculum development agenda. But also, and very significantly, he uses the term ‘translation’ – a term that carries a very different meaning from ‘implementation’. It signals a particular way of going about this, and suggests two considerations:
The message is this: because something works in one situation does not mean that it will work in another. A medical analogy might help. Transplantation of an otherwise healthy organ can result in ‘rejection’ because of the effects of the recipient’s ‘immune response’. Curriculum change that is approached as ‘a plan to be implemented’, to be ‘diffused’ in a ‘centre-periphery manner’ (Schön, 1971), is like the use of immunosuppressant drugs in organ transplantation – medication is used to ‘knock out’ (suppress) the recipient’s immune defence system. Rather, curriculum planners need to understand ‘the immune system’ of the people who they hope will take up their curriculum. Instead of ‘suppressing’ the recipient’s immune system, they must understand it.
Pinar et al (1995) recommended not seeing the problem of curriculum change as deciding ‘what’ to do but an attempt to understand ‘why’ the problem exists:
‘… problems do not just require knee-jerk, commonsensical responses, but careful, thoughtful, disciplined understanding’.
It is for this reason that Stenhouse recommends that curriculum development should be seen as a form of educational research. Any curriculum proposal, he said, should be transformed:
… into a hypothesis testable in practice. It [should invite] critical testing rather than acceptance.
(p 142)
These views are well supported by recent observations that both education and medical practice are examples of ‘complex systems’ (Plsek and Greenhalgh, 2001, pp 635–638), where approaches that see them as ‘machines’ that simply need ‘oiling’ are liable to fail. Such mechanistic thinking:
… is built largely on the assumption that plans for progress must provide ‘the best’ way, completely specified in great detail, and consistently implemented in that same level of detail across the board.
Detailed specifications fail in complex systems because they do not:
… take advantage of the natural creativity embedded in the organisation, [or] allow for the inevitable unpredictability of events.
In the context of ‘curriculum’, Stenhouse (1975, p 143) argued that:
… all well-founded curriculum … development … rests on the work of teachers. It is not enough that teachers’ work should be studied: they need to study it themselves.
In other words, the teacher should be the focus of curriculum development. Seen in this way, curriculum development begins with an appreciation of what teachers and learners actually do, when they do it, how they do it, and why they do it that way. It is undoubtedly true that medical teachers (at all levels) teach well and highly appropriately, when they are committed to this work and adequately resourced to undertake it. Similarly, learners learn well where the curriculum allows them to (Coles, 1985). None of this requires ‘detailed specification’, and is more likely to occur naturally without it.
What then is curriculum development?
So where does this leave curriculum development? It is clear that:
The fundamental relationship between a trainee … and the supervising consultant is critical for professional development … There is no better way of realising the full potential of the trainee and passing on the wisdom of clinical experience.
‘Curriculum’, then, is best seen not as a plan for action but rather as what underpins education (Fleming, 2010). It is the unseen (and often unrecognised) foundation of effective teaching and learning. Learning occurs in and through this relationship – the interactions and transactions – between a teacher and a learner. In that sense, teachers and learners together ‘develop’ what is to be learnt, how it is to be learnt, and how the effects of that learning are to be recognised, that is how it is best assessed and for what purpose that assessment is undertaken (AMRC, 2009). Curriculum development, then, actually (and naturally) occurs in and through that relationship between teachers and learners – a relationship that reflects that of researcher and supervisor – in the setting of authentic practice. The true curriculum developers are the teachers and the learners. They are the people who make education ‘work’, if the conditions are conducive to that happening. In the past, people have seen ‘a curriculum’ as a ‘proposal’ – usually a document that sets out educational intentions for many contexts. This contrasts with a second view of curriculum as an educational concept which defines the essential educational relationship between teacher and learner in a particular context.
Where does this leave those who up to now have been called ‘curriculum developers’? If the role of curriculum developer is now to be given to (perhaps even given back to) teachers and learners, what is the function of people, frequently at national level, who are often the initiators of educational change? Quite fundamentally, the role of these ‘curriculum initiators’ is to help teachers and learners develop an appropriate curriculum for learning in situ – in their own setting – and certainly not to include anything in their curriculum plans that might constrain that development.
Some conclusions
A vision of learning medicine
What, then, ought a curriculum plan to entail that aspires to create the conditions for ‘learning medicine’? What might a medical curriculum proposal look like from the perspective of my general conclusions about curriculum and curriculum development? My vision is speculative. It challenges some entrenched shibboleths. It is iconoclastic. It is (inevitably) a sketch, an outline, an overview. But it is not ‘sketchy’; it is based on sound educational principles. Above all, it reflects the uneven history of curriculum development over the past 150 years. It rests on the concept of curriculum that I have drawn from my discussion in this chapter: moving from seeing curriculum as ‘an educational plan’, to curriculum in terms of the ‘educational action’ itself, that is in situ. The concept of curriculum I believe we now need to adopt is of something which underpins what teachers and learners do in practice. It is the basis for their educational actions. Strangely enough, Flexner might approve. His writing showed that he understood education, and he understood medical practice. He knew what teachers and learners did and why they did it, and then what they needed to do for their teaching and learning to be as appropriate as possible. Many curriculum developers since, for the reasons I have given, have lost that vision.
A vision for curriculum initiators
Those who initiate a curriculum plan must recognise that ‘curriculum development’ actually happens in and through the interactions of teachers and learners when they grapple, together, with their teaching and learning. Any curriculum plan must make this explicit – and make it possible for that ‘grappling’ to happen (Pring, 2000).
Any curriculum plan must show how:
A vision for teachers and learners
Teachers and learners are central to the effectiveness of any curriculum proposal. Their role needs to be fully recognised. Without them, there is no curriculum.
Coda
I began this chapter by exploring thoughts that Flexner published a 100 years ago. Throughout, I have used his writings to critique what has happened in medical education since then. In sketching out my educational vision, I suggest that he might have approved of it. Flexner was a man both of his time and before his time. He saw the need for radical reform of medical education in North America. In doing so, he raised challenges that are as true today as they were then. However, despite considerable ‘curriculum development’ (a term I now use with some caution), little educational development has occurred. Indeed, some of it has been palpably ‘counter-educational’. I have offered in this chapter some educational perspectives to account for that failure. The challenge now is to question models and structures of the past and to start afresh, though now equipped with an appreciation of sound educational principles. Medical educators can learn much from Flexner and from the curriculum failures of the 100 years since the publication of his report. Perhaps doing so brings us ‘full circle’, and helps us recognise the true contribution of his thinking. TS Eliot (1965) summed this up well:
Implications for practice
What conclusions can we draw from this account of curriculum development? The main educational principles emerging from this chapter are as follows:
Paradoxically, perhaps, I return to what has been the situation for millennia in pursuing the curriculum problem – reinstating that educative relationship between the teacher and the learner as the locus for its solution. Maybe now, through a greater understanding of what is involved, those concerned with the curriculum problem can more confidently defend the central need for some form of ‘professional apprenticeship’ for learning medicine against a tide appearing to sweep them towards technical training.
AMRC. Improving assessment. London: Academy of Medical Royal Colleges, 2009.
Baldwin P., Dodd M. Higher specialist training – early experience in Scotland. Edinburgh: Scottish Council for Postgraduate Medical and Dental Education, 1999.
Barrows H.S. Problem-based learning in medicine. In: Clarke J., Leedham J., editors. Aspects of educational technology 10: individual learning. London: Kogan Page, 1976.
Becker H.S., Geer B., Hughes E.C., et al. Boys in white. Chicago: University of Chicago Press, 1961.
Carr W. For education: towards critical educational inquiry. Buckingham: Open University Press, 1995.
Coles C. A study of the relationships between curriculum and learning in undergraduate medical education. University of Southampton, 1985. PhD thesis (unpublished) Faculty of Educational Studies
Coles C. Is problem based learning the only way? In: Boud D., Feletti G., editors. The challenge of problem based learning. London: Kogan Page, 1990.
de Cossart L., Fish D. Cultivating the thinking surgeon: new perspectives on clinical teaching, learning and assessment. Harley, UK: TFM Publishing Ltd, 2005.
Department of Health. Modernising medical careers; the next steps. Leeds: UK Health Departments, 2004.
Doll W.E. A post-modern perspective on curriculum. London: Teachers College Press, 1993.
Eliot T.S. Collected poems. London: Faber & Faber, 1965.
Epstein R.M. Mindful practice. J Am Med Assoc. 1999;282(9):833-839.
Fish D., Coles C. Medical education developing a curriculum for practice. Maidenhead: Open University Press, 2005.
Fish D., de Cossart L. Developing the wise doctor: a resource for trainers and trainees in MMC. London: The Royal Society of Medicine Press Ltd, 2007.
Fleming W.F. The curricular nature of practice. United Kingdom: University of Winchester, 2010. PhD Thesis
Flexner A. Medical education in the United States and Canada: a report to the Carnegie Foundation for the Advancement of Teaching. New York: Carnegie Foundation, 1910.
Freidson E. Professionalism reborn: theory, prophecy and policy. Oxford: Polity Press, 1994.
Gale J. The diagnostic thinking process in medical education and clinical practice: a study of medical students, House Officers and Registrars with special reference to endocrinology and neurology. London, UK: University of London, 1980. PhD thesis
Gawande A. Complications; A surgeon’s notes on an imperfect science. London: Profile Books Ltd, 2002.
GMC. Recommendations as to the Medical Curriculum. London: General Medical Council, 1947.
GMC. Recommendations as to the Medical Curriculum. London: General Medical Council, 1957.
GMC. Recommendations on basic medical education. London: General Medical Council, 1980.
GMC. Tomorrow’s doctors: recommendations on undergraduate medical education. London: General Medical Council, 1993.
GMC. Tomorrow’s doctors 2009: a draft for consultation. 2009. Available at: http://www.gmcuk.org/education/undergraduate/news_and_projects Accessed November
Golby M., Parrott A. Educational research and educational practice. Exeter: Fair Way Publications, 1999.
Haas J., Shaffir W. Ritual evaluation of competence: the hidden curriculum of professionalization in an innovative medical school program. Work Occup. 1982;9(2):131-154.
Haines A., Jones R. Implementing findings of research. Br Med J. 1994;308:1488-1492.
Lave J., Wenger E. Situated learning: legitimate peripheral participation. Cambridge: Cambridge University Press, 1991.
Margetson D.B. The relation between understanding and practice in problem-based medical education. Med Educ. 1999;33:359-364.
Merrison A.W. Report of the inquiry into the regulation of the medical profession. Br Med J. 1973. 25th June 1975
MMC. Modernising medical careers: the next steps. The future shape of foundation, specialist and general practice training programmes. London: Department of Health, 2004.
Newman G. Some notes on Medical Education in England. London: HMSO, 1918.
Open University. Evaluation of the reforms to higher specialist training 1996–1999: executive summary. Milton Keynes: The Open University Centre for Education in Medicine, 2001.
Pinar W.R., Reynolds W.M., Slattery P., et al. Understanding curriculum: an introduction to historical and contemporary curriculum discourses. New York: Peter Lang, 1995.
Plsek P.E., Greenhalgh T. The challenge of complexity in health care. Br Med J. 2001;323:625-628.
Plsek P.R., Wilson T. Complexity, leadership and management in healthcare organisations. Br Med J. 2001;323:746-749.
Pring R. Philosophy of educational research. London: Continuum Books, 2000.
Rikers R.M., Loyens S.M., Schmidt H.G. The role of encapsulated knowledge in clinical case representations of medical students and family doctors. Med Educ. 2004;38:1044-1052.
Schön D. Beyond the Stable State: public and private learning in a changing society. London: Temple Smith, 1971.
Schön D. Educating the reflective practitioner. London: Jossey-Bass, 1987.
Snyder B.R. The hidden curriculum. New York: Knopf, 1971.
Stenhouse L. An introduction to curriculum research and development. London: Heinemann, 1975.
ten Cate O. Trust, competence, and the supervisor’s role in postgraduate training. Br Med J. 2006;333:748-751.
Tooke J. Aspiring to excellence: final report of the independent inquiry into modernising medical careers. London: Department of Health, 2008.
Tyreman S. Promoting critical thinking in health care: phronesis and criticality. Med Health Care Philos. 2000;3:117-124.
Wenger E. Communities of practice: learning, meaning and identity. Cambridge: Cambridge University Press, 1999.
Williams G. Western reserve’s experiment in medical education and its outcome. New York: Oxford University Press, 1999.
Woodward C.A., Ferrier B.M. The content of the Medical Curriculum at McMaster University: graduates’ evaluation of their preparation for postgraduate training. Med Educ. 1983;17:54-60.