19 Developing teachers and developing learners
Association of American Medical Colleges (AAMC) The organisation represents all 131 accredited US and 17 accredited Canadian medical schools; approximately 400 major teaching hospitals and health systems; and nearly 90 academic and scientific societies. Through its many programmes and services, the AAMC supports the entire spectrum of education, research, and patient care activities conducted by our member institutions.
Aboriginal Term related to indigenous peoples, used here in relations with people in Australia and Canada.
Academy of educators A new organisational structure in medical schools directly tied to the support of the educational mission of the institution.
Attention-deficit/hyperactive disorder (ADHD) Chronic condition often associated with inattention and impulsive behaviour. Treatment is usually associated with counselling and/or medications.
Association for the Study of Medical Education (ASME) A UK-based organisation with international membership, which ‘seeks to improve the quality of medical education by bringing together individuals and organisations with interests and responsibilities in medical and health care education’.
Attending Faculty physician responsible for the care of patients while supervising care given to patients by postgraduate trainees and/or medical students (USA).
Best Evidence Medical Education (BEME) collaboration A group of individuals or institutions who are committed to the promotion of Best Evidence Medical Education.
Consultant See main Glossary, p 338.
Faculty development Programme designed to improve the skills of faculty members, usually in areas related to education, such as lecturing skills, curriculum development, or assessment design.
Faculty member A person, generally with a terminal degree, who is often expected to be successful in clinical work, research, teaching, and community service.
Foundation for the Advancement of International Medical Education and Research (FAIMER) A non-profit component of the Educational Commission for Foreign Medical Graduates (ECFMG) devoted to providing “educational opportunities and research and data resources that inform health care policies and create sustainable improvements in health outcomes.” It is best known for its maintenance of The International Medical Education Directory and provision of International Fellowships in Medical Education.
Family medicine Specialty of medicine in the United States related to primary care of adults and children, often including obstetrics. Similar to general practice in the United Kingdom.
Foundation Doctor or Foundation Trainee See main Glossary, p 340.
General practice; see also family medicine Specialty of medicine in the United Kingdom, similar to a family medicine practitioner in the United States, serving as the first line of health care and treatment within the UK system.
General Medical Council (GMC) See main Glossary, p 341.
Higher education Education after secondary school, at a university, college, or professional school, in a discipline such as Medicine or Law.
Imposter syndrome Also known as the imposter phenomenon, in which a student or professional, more often a woman, has an internal experience of being an imposter rather than fully qualified for her or his earned academic or professional station.
Intern See main Glossary, p 339.
Liaison Committee on Medical Education (LCME) The nationally recognised accrediting authority for medical school programmes, leading to the MD degree in the US and Canadian medical schools.
Learner development An academic approach that focuses on building learning skills, attitudes, knowledge, and meta-cognition through targeted programming, directed practice, peer-tutoring, and individual counselling.
Medical Education Unit Office at many medical schools around the world focusing on the support and study of education. Such offices may include curriculum development, faculty development, evaluation, and educational research.
Mission-based budgeting A financial model that aims to identify the flow of funds in a medical school so that each goal or mission of the institution is the recipient of funds in relation to the amount of work, often titrated by quality indicators, required to uphold that goal or mission.
Medical Schools Council (MSC) Organisation that represents the interests and ambitions of UK Medical Schools as they relate to the generation of national health, wealth, and knowledge through biomedical research and the profession of medicine.
One Minute Preceptor A widely accepted teaching model that summarises important tasks or “microskills” for clinical teaching. The model begins with the diagnosis of the learner’s needs and results in focused teaching and feedback. The teaching steps include: ask for a commitment; probe for supporting evidence; teach a general rule; tell the learner what s/he did right and the effect it had; and correct mistakes.
Pastoral counselling Pastoral counselling moves beyond the support or encouragement a religious community can offer, by providing psychologically sound therapy that weaves in the religious and spiritual dimension. From aapc.org
Postgraduate trainee See main Glossary, p 339.
Sami The Sami (also spelled Saami) are the 100,000 Indigenous inhabitants of Norway, Sweden, Finland, and the Russian Kola Peninsula.
Specialist trainee See main Glossary, p 341.
Student Affairs Office Student support office at many US medical schools that may include registrar, financial aid, academic support, academic scheduling, career advising, and general well-being programmes.
World Federation for Medical Education (WFME) A global organisation concerned with education of medical doctors at all levels. It serves as an umbrella organisation for six regional medical education associations. It is active in the promotion of guidelines and standards for worldwide use in the accreditation and continuous improvement of medical schools.
World Health Organisation (WHO) The directing and coordinating authority for health within the United Nations system, which is responsible for leadership on global health, from research to policy, and monitoring and assessing health trends.
Outline
The greatest investment of any educational institution is in its teachers, and the reason for that investment is its learners. Teachers develop; learners develop; the institution grows as well. In this chapter, we will consider the types of programmes needed to create and sustain a learning community of teachers and learners. The first section of the chapter describes a range of programmes useful in assisting faculty members in developing their skills as teachers and the organisational structures needed to support such programmes. The second section addresses: the needs of learners, from students to postgraduate trainees; the design of learning skill development programmes; and typical activities and skills included in such programmes. The section ends with a discussion of the need to extend such programming in order to better prepare the wider range of learners trying for entry into medical school.
Introduction
Educational institutions that invest in the development of their teachers and learners can be called learning organisations according to Senge (1990). Such organisations, capable of continuous adaptation and growth, demonstrate a commitment to five broad principles, which can be used as a lens through which to view the work of medical schools and health care institutions in creating and sustaining faculty and learner development programmes:
The learning organisation is committed to personal mastery. Individuals within such a community, both faculty and learners, never stop learning. It is the journey itself that is important. While individual learning by itself does not necessarily translate into organisational learning, without individual learning, there can be no organisational or community learning.
The members of a learning organisation share a common mental model of desirable actions. In order for the organisation to move in a chosen direction, all members of that organisation must have access to and ability to influence the strategic plan or conceptual model that will guide future actions. Such a model is the product of community members working together: in our case, teachers and learners.
The learning organisation actively works to engage all of its members in developing a sense of the possible, a shared vision. Mutual and regular feedback is a key requisite for elaborating on the vision and refining it to meet the needs of the various community constituencies.
The organisation changes by reflecting on its successes and challenges. Time and resources are committed to building a team-learning environment in which members of the organisation learn from and with one another. Working together, teachers and learners develop a trust and a commitment to continuous improvement based on mutually understood needs.
The learning organisation is committed to systems thinking as opposed to governance from the top down. A learning community is most likely to develop when the organisation understands its existence within the system which encompasses it as well as the microsystems of which it is composed. Medical education institutions include multiple microsystems – central administration, individual academic departments, health care delivery service lines, curricular systems, learners at varying levels, and staff essential to the work product of each constituency. It is incumbent on the learning organisation to develop in response to the varying needs of each group of which it is composed.
Faculty and learner development programmes can serve as the engine that drives the development of a learning organisation. Such programmes instil a commitment to excellence, develop shared models of desirable behaviour, create a common vision, instil a team-learning spirit, and facilitate systems thinking.
Developing teachers
Until the mid 1960s, university faculty members, including those in medical schools, were considered fully prepared for their role as teachers (Sorcinelli, 2006). An advanced degree in their specialty was all that was required since effective teaching was defined as demonstrating expertise in the specified content area through publications and research grants. Faculty development was synonymous with sabbaticals, research opportunities, and travel to professional meetings. Beyond content expertise, good teachers were born, not made. In 1955, George Miller, a faculty member at the University of Buffalo School of Medicine, USA, and Steve Abrahamson, a faculty member in the School of Education, acquired funding to establish a partnership between the two schools called the Project in Medical Education. The goal of the Project was to explore how to apply the growing body of research and theory in education to medical education. A young medical student, Hilliard Jason, who had been extremely vocal about problems in medical school teaching, was invited to join the Project. Jason subsequently became a founder of teaching improvement programmes in medical education (Wilkerson and Anderson, 2004).
In higher education, the growing demand by university students during the 1960s for better teaching led to increased use of teaching evaluations and pressure on university professors to consider the existence of actual skills of teaching – similar to those required of pre-college teachers – that could be learnt and developed. Guided by the work of Berquist and Phillips, Gaff, and Centra, the field of faculty development emerged in higher education in the 1970s (Sorcinelli, 2006). The improvement of teaching skills became a central focus of the field, although Berquist and Phillips also advocated the need for attention to organisational structures that support teaching, and development of the faculty member both as a person and a professional.
Current definitions of faculty development largely focus on the skills of the individual teacher, including teaching skills, scholarship, and well-being issues. However, faculty development also includes goals related to the improvement of individual courses, the broader curriculum, and student learning, and a focus on organisational development to improve the policies and practices of the institution to better support the teaching and learning environment. In this chapter, we focus on aspects of faculty development related to the improvement of teaching and learning.
Teacher training, historically a part of preparing school teachers, extended from the United States (Jason and Westberg, 1982) to the wider world through the World Health Organisation (WHO) and its teacher training programmes (Guilbert, 1981). During this same period in the United Kingdom, general practitioners were taking on specialist training and programmes arose to develop the skills of such GPs as teachers. Yet 30 years later, many medical schools and training programmes still provide limited opportunities for faculty members to develop their skills as teachers. Faculty members continue to report a lack of opportunity to learn how to teach. They feel unsupported in their work as teachers. Almost every recent report on medical education worldwide includes a call for more attention to preparing faculty members for their roles as teachers, including establishing adequate rewards for their teaching contributions (Cohen, 2009; GMC, 2009). Accreditation standards for medical schools in the United States (www.lcme.org/standard.htm) and the United Kingdom (GMC, 2009) require the development of faculty and residents as teachers.
Designing a comprehensive faculty development programme
Three features are central to the development of a comprehensive faculty development programme designed to support the educational mission of a medical education centre: (1) an organisational structure to support the work of teaching and teachers, (2) a variety of faculty development activities and resources targeted at the differing educational roles and individual needs of teachers, and (3) a reward system that values excellence in the various educational roles needed in the institution (Wilkerson and Irby, 1998). These features require an ongoing investment of capital and cannot be sustained without a commitment from the highest level of the organisational unit involved, whether that is a department, a medical school, an academic medical center, a centre of postgraduate medical education, or an entire health care system.
Organisational structure to support teaching and teachers
As educational programmes have increased in complexity, teachers have found themselves confronting teaching situations unlike any that they experienced themselves. Thus, the time-honoured way of learning to teach in medicine – copying one’s own teachers – is no longer adequate. Problem-based learning (PBL), mannequin-based simulations, e-learning platforms, and multimedia smart classrooms were not part of most teachers’ experiences as learners. Even clinical experiences have changed, now employing novel learning experiences within multi-professional teams, service-learning, community immersions, hand-held computing, and outcome-oriented patient care. Several organisational structures have emerged over the past 50 years to support the teaching responsibilities of faculty members and their development as teachers: medical education units and ‘academies’ of educators.
Medical education units
Academic departments are rarely set up in such a way as to provide assistance to faculty members in developing their skills as teachers. General practice, or family medicine, is an exception, both in the United Kingdom and the United States, with the presence of behavioural scientists or educationalists who can help both trainees and faculty grow as educators. More commonly, medical schools have developed medical education units charged with faculty development, sometimes coupled with other educational responsibilities, such as programme evaluation, educational technology, curriculum support, and educational scholarship. In a 2001 WHO survey of medical schools around the world, Boelen and Boyer (2001) found that 58% of the 895 medical schools that responded in a survey had medical education units. Amin et al (2005) profiled 30 Asian medical schools, 72% of which had medical offices. Albanese et al (2001) reported that 50% of North American medical schools had such units although all have an officer at dean level who oversees medical student education and may bear some responsibility for faculty development.
The academy movement
For the past century, the educational mission of medical schools has continued to be subservient to the clinical and research activities of faculty members (Bloom, 1989), which are organised around departmental structures. A mission that extends across departments, such as the education of medical students, may be without the resources, faculty, and political strength needed to accomplish it. A new organisational structure is beginning to emerge directly tied to the support of the educational mission of medical schools and postgraduate training programmes. Known as academies, these structures are designed as a geographical ‘commons’ for skilled teachers (Huber and Hutchings, 2005), through which they can gather to share ideas about teaching and learning as part of their ongoing professional development. Through academies, such educators can be rewarded, encouraged to innovate, provided with faculty development, assisted in developing a scholarly approach to teaching, and nurtured as educational scholars (Irby et al, 2004). In a 2003 survey of medical schools in the United States (Dewey et al, 2005), 21% reported the recent establishment of such an academy as a formal school-wide organisation with a mission to support the work of faculty as teachers with dedicated resources for faculty development, scholarship in education, and innovation. Membership is usually composed of distinguished educators selected via peer review. In the United Kingdom, a national Institute for Teaching and Learning was established in the late 1990s, then renamed the Higher Education Academy, which has similar aims but with a mission to serve faculty development needs across the whole higher education sector. Each subject area or grouping of cognate areas has a national Subject Centre (located in a host university) to act as a resource and foster collaboration and cross-fertilisation in all aspects of UK higher education. The Medicine, Dentistry, and Veterinary Medicine Subject Centre, based in the Faculty of Medical Sciences, Newcastle University, provides support to all UK medical, dental, and veterinary schools (see http://www.medev.ac.uk/). More recently, a national Academy of Medical Educators has been established to focus on the needs of faculty across medical schools and residency training sites (see http://www.medicaleducators.org/).
A range of teaching improvement programmes targeted to needs
Over the past 15 years, evidence on the effectiveness of continuing professional development activities in changing physician behaviour has continued to grow. Mazmanian and Davis (2002) conclude that three key features have been consistently identified as essential: (1) education based on assessment of needs, (2) opportunities for interaction with peers and practice of the skills to be learnt, and (3) longitudinal, sequenced multi-method activities. Although their review is focussed on changes in clinical practice and patient outcomes, the findings mirror those from studies on changing teacher behaviours and learner outcomes (Steinert et al, 2006; Wilkerson and Irby, 1998).
In teaching improvement, needs assessment has often taken the form of surveys of faculty members to determine their interest or self-assessed competency in a variety of teaching skills. While this strategy can be useful, it does not cover the broad range of skills needed by faculty members as educators. Taking institutional need as the defining issue, there are faculty who are: new to the institution who want to understand career expectations and develop basic skills in teaching; experienced teachers who carry the greatest teaching load and may be expected to implement new learning modalities or to improve their performance in clinical or classroom teaching; teachers appointed to serve as educational leaders of courses, clerkships, residency training programmes, and continuing professional development activities; and those teachers who wish to make education the focus of their scholarship. Each of these groups operates within an organisational structure that needs to nurture their accomplishments in order to create, sustain, and constantly improve the educational programmes of the institution.
Needs of new faculty as teachers
Each year medical schools, academic medical centres, and academic community practice groups experience an influx of new teachers, who may be foundation trainees, first-year residents, or specialist trainees. Medical schools may also employ new faculty members, especially those who are expected to provide patient care, or identify new community-based trainers who will teach medical students or postgraduate trainees. Benor and Mahler (1987) stress the need to orient these new teachers to the core values that underlie the teaching programmes of the institution in order to prepare them to participate fully in its educational mission. Before assuming teaching responsibilities, whether formally in the classroom and clinical settings or informally during clinical work, new teachers need to know the norms and expectations for teaching and be able to identify opportunities to teach. For example, new foundation trainees or residents may believe they do not have time to teach, usually meaning that there are no conference-room seminars for which they are responsible. However, residents have innumerable opportunities to teach when supervising medical students or junior trainees on ward rounds, in the operating theatre, and late at night on call.
Many medical schools provide an orientation for new faculty. Orientation sessions typically focus on academic expectations, promotion criteria, and career advancement. Such sessions may also provide a chance for new faculty to connect with more senior faculty for purposes of career mentoring and research collaboration. A typical new faculty orientation lasts a half or full day and includes presentations on various institutional resources and guidance on the academic promotion process. However, there are a number of innovative models, which include the use of online virtual orientation modules (Walling and Chinn, 2002), an informal welcoming reception with key administrators and information booths, and a small group mentoring programme (Pololi et al, 2002). New faculty members who will become a part of the teaching faculty, however, also need an introduction to the prevailing educational mission of the institution, information about expectations and opportunities to teach, and some beginning teaching skills. At UCLA, we have expanded a more traditional orientation day on resources and promotion processes to include a choice of teaching skill workshops, an informal buffet lunch hosted by the faculty development office, and a panel discussion on teaching opportunities and resources.
New groups of postgraduate trainees enter our institutions each year, creating an unending group of new teachers who need to understand our expectations for teaching and how to fulfil them. In the 1960s, special programmes for residents as teachers began to appear but did not become a significant part of faculty development programmes until the 1980s (Bensinger et al, 2005). In a review of resident-as-teachers programme evaluation studies from 1975 to 2008, Post and colleagues (Post et al, 2009) identified 47 articles, of which 24 provided outcome data for the programmes described. Programmes included lectures, practice sessions (such as ‘microteaching’), and retreats, often based on the ‘One Minute Preceptor’ model (Neher et al, 1992), and ranged in length from 1 to 15 hours. Using a variety of outcomes measures, the studies demonstrated changes in teaching behaviour, self-reported confidence, and learner evaluations of residents’ teaching. Based on their review, the authors recommend interventions, such as exploration of the One Minute Preceptor, which should be of 3 hours or longer in duration.
Needs of effective teachers
A growing body of research has demonstrated the effects of excellent clinical teachers on medical students’ knowledge, clinical skills, and specialty choice (Griffith et al, 2000; Wimmers et al, 2006). This work underlines how important it is to provide opportunities for faculty members to develop strong teaching skills, at least in the clinical setting. A 1998 review by Wilkerson and Irby described the changing view of teaching improvement approaches over time, as the predominant educational theories guiding faculty development shifted from behavioural to cognitive, and then to social constructivist, in line with wider changes in the epistemology of medical education described in Chapter 2. Effective interventions across models included workshops of 2 days or more, teaching evaluations coupled with individual consultation, and longitudinal fellowships or courses. In a Best Evidence Medical Education (BEME) review on faculty development initiatives to improve teaching, Steinert et al (2006) identified almost 3000 articles from 1988 to 2002 describing teaching improvement programmes in medical education. The majority of programmes were workshops or seminars focusing on classroom and clinical teaching, which included topics such as lecturing, facilitating group discussion, teaching during patient care, providing effective feedback, and evaluating learner performance. More recently, basic skill workshops have also included teaching with simulations and educational technology.
The BEME review highlights a number of issues that continue to require study and innovation in relation to teaching improvement interventions, first considering the issue of participation. Should basic teaching skill training be a mandatory requirement of medical school teachers as it is for teachers of younger learners? In voluntary programmes, it is often the best teachers who understand the importance of continuous improvement and make the time to participate. Several medical schools have required participation in basic teaching skills training or produced incentives tied to promotion for participation in order to reach more teachers. In the United Kingdom, GP vocational training sites require trainers to participate in some manner of teacher training course.
A second consideration is the question of context. To what degree should basic teaching skills workshops be linked to specific courses or rotations? This linkage strategy produces a targeted audience, the opportunity to identify very specific needs, a context from which to draw examples for experiential components, and more identifiable scheduling possibilities.
A third consideration is how much faculty development is needed by an individual instructor. Reviews have consistently identified the need for numerous interventions over time. One strategy for increasing the impact of single workshops is to link them together to produce more extended engagement. To maximise flexibility and choice, The Center for Faculty Development at St. Michael’s Hospital, University of Toronto, has developed a ‘Stepping Stones’ programme. Participants can earn a Certificate in Teaching by participating in 26 hours of workshops and 17 hours of more theoretically focused medical education journal club sessions over a 2-year period (see: http://www.cfd.med.utoronto.ca/programmes/stepping-stones.html).
Fourth is the issue of delivery modalities. To date, most teaching improvement interventions have been delivered in face-to-face sessions with an emphasis on peer interaction and collaborative learning. The use of online multimedia materials on teaching has the potential to increase participation, especially in a distributed education system. For example, to support clinical teachers across the entire state affiliated with a health professions training programme, the North Carolina Area Health Education programme offers web-based multi-media, interactive modules on clinical teaching skills, the Expert Preceptor Interactive Curriculum (EPIC), which is linked to a centrally monitored online discussion forum at: http://www.ncahec.net/hcprofessionals/preceptor.htm.
To further maximise access and meet individual preferences, the programme also offers each teaching improvement module as a printed manual, a single-page ‘thumbnail sketch’ for quick review, a web-based self-instructional module, or a 1-hour seminar scheduled to meet the preferences of teachers in a specific community. Participation is encouraged by rewarding it with continuing professional development credit. Other modalities that require exploration include peer coaching, mentoring, reflective writing and discussion, communities of practice, and pay-for-performance. Critical to the effectiveness of teaching improvement interventions of any type are the use of multi-faceted learning methods, opportunities for practice with feedback, the involvement of supportive colleagues, and repeated involvement over time (Steinert et al, 2006).
The BEME review also emphasises the need for more high-quality programme evaluation studies to further increase understanding of the features and outcomes of faculty development (Steinert et al, 2006).
Needs of educational leaders and innovators
Educational programmes require faculty members who are prepared to design and implement them based on a sound understanding of what is known about how people learn and the evidence supporting various educational approaches. In a period of ever-changing curricula, these faculty members need to understand issues in organisational change and possess the leadership skills needed to guide that change. These faculty members determine the selection criteria and admissions processes for students, postgraduates, and faculty; they design and set the standards for competency assessment; they create outcome measures to meet accountability and accreditation standards; they recognise and respond to new challenges in medicine by leading curricular changes that address those challenges, e.g. increased demands for clinical productivity, changes in health care delivery systems, changing community demographics. Preparation for educational leadership and innovation requires faculty development interventions that go beyond the acquisition of basic teaching skills.
The medical education literature is rich in descriptions of longitudinal faculty development programmes for a select cohort of faculty members in the form of certificate, fellowship, and degree programmes designed specifically to grow educational leaders and innovators. A survey of medical education deans in North America by Searle et al (2006) identified 42 educational fellowship programmes. A special issue of Academic Medicine (November 2006) included articles on nine of these medical education fellowship programmes. The content of the fellowships emphasised both an understanding of current theories of learning and the implications for curriculum design and evaluation, approaches to curriculum design, and issues in organisational change including leadership. Gruppen et al (2006) summarised the ‘Common Themes and Overarching Issues’ in a final article in the issue:
Each of the nine schools has incorporated best practices in education to prepare faculty to lead, develop, teach, and evaluate educational initiatives. Furthermore, framing these efforts as forms of scholarship consistent with the academic advancement of participating faculty fostered the expansion of expertise on which the programmes could draw … All nine schools completed some form of institutional, departmental, and/or individual faculty needs assessment, resulting in clearly defined programme goals and objectives for their fellowship programmes. These goals and objectives then led to the selection of a programme structure and specific instructional methods, informed by the literature on faculty development, adult learning, leadership, and other sources from the behavioral and social sciences. The programmes were implemented and then evaluated to determine the degree to which the objectives were met. On the basis of this evaluation, each of the programmes was then revised.
Internationally, the Foundation for Advancement of International Medical Education & Research (FAIMER) provides similar longitudinal opportunities for ‘international health professions educators who have the potential to play a key role in improving health professions education at their schools’ (www.faimer.org/education/institute/index.html). FAIMER offers a 2-year faculty development programme that includes sessions on curriculum development, education methods, leadership, and professional networking conducted via two residential sessions and an online discussion forum (Norcini et al 2005). The UK-based Association for the Study of Medical Education (ASME) offers an annual programme on Developing Leaders in Healthcare Education (http://www.asme.org.uk/conferences-a-courses/) as does the US Harvard Macy Institute (www.harvardmacy.org/) on which the former is based.
Needs of educational scholars
Finally, some faculty members choose to focus their academic scholarship on medical education. Through research and writing, they seek to develop new knowledge about learning in medicine, synthesise existing studies to produce ‘best evidence’, apply best evidence to teaching practices, test its efficacy in producing intended learner outcomes, and publish and disseminate innovations with evidence of effectiveness. Skills required include: accessing and appraising the relevant literature in psychology, education, and health professions education; designing educational research and evaluation studies; collecting and analysing data; writing and presenting results; and developing networks of professionals with similar interests.
Some faculty members come more easily to these skills, building on prior work in scientific research or biostatistics. Most require some additional study to translate their medical research experience into the specific skills and understanding needed for more applied social science and/or qualitative research. As in the domain of biomedical research, preparation for a career as a medical education scholar usually requires hours of study and mentored scholarly activity, such as that provided through participation in a medical education research fellowship or degree programme in medical education. Some of the medical education fellowships described above also include an in-depth research component with mentored scholarship. A good example is the Medical Education Scholars programme at the University of Michigan, USA. This year-long fellowship includes a seminar on study design and completion of a mentored educational research study. As of 2003, the 35 graduates of the Scholars programme had published 9 peer-reviewed papers, delivered 21 oral presentations at national meetings, and submitted 16 educational grants (Gruppen et al, 2003).
A search of the internet (July 2009) turned up articles and information on 40 master’s degree programmes in medical education around the world, many including online components, with the largest number of programmes in the United Kingdom. The development of research skills in any domain requires an intensity of involvement that may be difficult for the typical medical school faculty member to sustain. For this reason, faculty development programmes in educational scholarship require a commitment of institutional resources, protected time for faculty participants, and the involvement of doctoral-level trained educational researchers, especially when a formal degree is provided, to ensure an appropriate level of quality (Pugsley et al, 2008).
Interventions designed to meet the needs of individual teachers range from short workshops to intensive, longitudinal courses or even degree programmes. In the BEME review of teaching skill programme outcomes referred to earlier, the authors identified 53 articles from 1980 to 2002 that met their inclusion criteria (Steinert et al, 2006). The majority of these studies evaluated participants’ satisfaction; a smaller number included evidence of change in knowledge or behaviour. Only three studies provided evidence of change in students or residents being taught by participants. Effective programmes were characterised by the following:
More recent studies provide examples of the types of well-designed evaluation studies called for in the BEME review, while including a greater focus on learner outcomes (Gozu et al, 2008; Notzer and Abramowitz, 2008; Branch et al, 2009).
A reward system that values excellence in education
Building organisational structures to support education and providing a range of faculty development programmes related to teacher needs are insufficient to sustain the educational mission of a medical school. The organisational vitality of any school depends on the system of recognition and rewards provided in support of its educational mission (Bland et al, 2002). A vibrant learning organisation values inquiry, innovation, scholarly teaching, and educational scholarship. It promotes and rewards continuous quality improvement and empowers individuals by providing visible credit for their accomplishments as teachers. Essential policies and procedures needed to support the educational mission include a clear statement by leadership that quality teaching is required and funded, a visible programme for reporting and evaluating teaching for promotion, a variety of awards for excellence in multiple aspects of teaching, recognition of the value of scholarship related to teaching, and a budget structure that encourages, rather than discourages, educational innovation.
As an interesting exercise, examine the mission statement of any medical school or academic medical centre. Does the word ‘education’ appear in the statement? The University of Pittsburgh School of Medicine, USA, offers a view of a clear statement of the importance of education in the institution. Its mission is simply stated: ‘A different kind of medical school. A different kind of medicine’. The web page of the School of Medicine opens with a description of that difference. The Dean’s State of the School Address linked from that page reinforces this institutional vision by opening with an update on medical student education and a description of several innovations, including a new requirement for a scholarly project, the initiation of mini-electives for first- and second-year students, and the growth of an Academy of Master Educators.
A clear role for evidence of teaching quantity and quality as part of promotion provides another indicator of an institution’s commitment to its educational mission. The recommendations of a consensus conference hosted by the Association of American Medical Colleges’ (AAMC) Group on Educational Affairs (Simpson et al, 2007) distinguished between effective teaching, scholarly teaching, and educational scholarship. All three are important to the educational mission but the latter two constitute evidence of quality beyond learner evaluations. Scholarly teaching is based on educational theory and best practices and requires an awareness of changing evidence about what works to maximise learning. Classroom and clinical teaching, advising and mentoring, and contributions to learner assessment should all be valued. Evidence supporting the quality of scholarly teaching may include:
Educational scholarship is work done to contribute to the body of theory and practice in medical education that is publicly shared, open for others to build on, and peer-reviewed. Curriculum development and leadership of significant educational components are often included along with more traditional publications and presentations to the larger community of medical educators. Some medical schools have adopted Boyer’s definition of scholarship (Boyer, 1990) and/or Rice’s expanded version (Rice, 2005) to include the scholarship of teaching: discovery of new knowledge about learning, application of existing knowledge to new educational problems, synthesis of existing studies in teaching and learning, and scholarly teaching that demonstrates sound principles of education. Under this expanded definition, the production of instructional materials, textbooks and chapters, and innovative course designs are considered appropriate types of scholarship. The majority of North American medical schools have established separate promotion tracks for clinician educators to which this broader definition of scholarship has been applied. However, there remains a concern about equality in status for such tracks (Fleming et al, 2005).
Educational accomplishments can be documented in a teaching portfolio in which both quantity and evidence of quality are presented in tandem. In a survey of US medical schools in 2002 (Simpson et al, 2004), 64% reported using a teaching portfolio that included at least three of the following components:
In addition to the use of a portfolio, institutional policies that clearly state a requirement for teaching, particularly medical student teaching, and expectations for the quality of that teaching are important in providing a clear message that education is a priority. Until the promotion committee or dean refuses to review a promotion dossier lacking evidence of teaching, or insists on improvements in teaching quality as a standard for promotion, stated policy related to a requirement for teaching may not be interpreted as serious.
Awards and honours for the wide variety of educational activities in which faculty members engage provide another means of rewarding the educational contributions of faculty. While teaching awards from students or residents (e.g. ‘Lecturer of the year’) are highly prized by faculty, it is important for the institution to recognise other types of educational contributions that go beyond outstanding teaching. Peer nominations can result in awards for curricular innovation, educational leadership, mentoring, or clinical performance assessment. Membership in the type of academy described earlier is another form of educational recognition by one’s peers. A broad range of awards with many, rather than a few, being recognised can serve as an incentive for attracting and retaining faculty members in key educational roles within the department or across the institution. Such honours and awards can be enriched when the selection process is transparent and well documented.
A final ingredient in the organisation of a learning-oriented organisation is a clearly identified budget for education, often referred to as mission-based budgeting. The concept is a simple one: to align the institutional budget with its educational mission while stimulating quality improvement (Ridley et al, 2002; Watson and Romell, 1999). Issues to be addressed include decisions on the scope of funds to be included in the mission-based aspect of the institutional budget, alignment of funds and missions, metrics of allocation to account for quantity and quality, and tools for measuring both.
A vibrant medical education organisation requires attention to the organisational features in place to support that community. Faculty development can help create a collegial learning community that shares a vision for personal excellence, continuous learning, and scholarship in teaching; promotes continuous quality improvement through collaborative reflection and action; and makes the contributions of scholarly teachers and educational scholars visible and rewarded. Creating and sustaining organisational vitality requires the empowerment of both personal and corporate leadership to lobby for the very best educational programme delivered by scholarly teachers and informed by the work of educational scholarship to maximise the learning of those entrusted into our care.
Developing learners
One of the significant changes in medical education in the new millennium is a commitment to help learners improve their skills and potential in regards to the learning experience in medical school and residencies. In the past, ill-prepared learners were left to fail. Some schools admitted all applicants with an expectation that a significant number would fail out. The ethos instilled from day one of medical school was embodied in a common saying: ‘Look to your left; look to your right; one of you will not be here at graduation.’ Today, in countries with populations as large as that of the United States and small as that of Mozambique, the learners who are admitted represent a valuable asset of that country. Investing in their success academically and personally makes economic sense, given the cost and time required to train a physician. A failure to complete a medical education degree is expensive for the individual and the country since it reduces the number of physicians prepared to meet the needs of that country’s citizens.
As increasingly heterogeneous groups of learners enter the medical education pipeline, it becomes incumbent on medical schools and residencies to develop a vision of, and programmes for, academic success for everyone. In socioeconomically disadvantaged communities, few high school students may graduate prepared for the demands of medical school. During medical school, students may encounter personal and academic difficulties. Even some residents continue to struggle with the assessments required to maintain progress toward full licensure. The cost to society of any of these learners dropping out of the physician ‘pipeline’ is significantly higher than the cost of helping to develop their academic skills for success.
Establishing a learner development programme
Accreditation standards for medical schools in the United States (www.lcme.org/standard.htm) and the United Kingdom (GMC, 2009), as well as the quality improvement standards of the World Federation for Medical Education (WFME, 2003), include a requirement for academic support or retention programmes, along with personal counselling, for medical students. Medical students and residents themselves recognise the need for learning skills development. One of the authors (Lawrence Doyle) has worked as a learning skills specialist for 30 years with learners from high school through to medical residencies. When he has visited medical schools in other countries, students have approached him to discuss study and test-taking skills relevant to their particular curriculum. At Universidad Eduardo Mondelane in Maputo, Mozambique, for example, first-year medical students arranged a late Friday afternoon session, identifying a student to translate, and then working together to learn from a presenter who did not speak their language. At Esculela de Latino Medicina in Havana, students from many different countries were eager to talk about study skills, particularly those for whom Spanish was a second language. At the National University of Singapore, medical students, on viewing a poster about study skills as the ‘missing element’ in a medical school curriculum, stopped for a quick discussion with the author about the types and levels of skills appropriate for medical students and subsequently recruited their colleagues to continue the discussion later in the day.
In designing programmes to develop medical students and residents as learners, a series of issues need to be addressed:
The first question in planning a learning development programme concerns the target audience. Should the focus be on learners in academic difficulty, all learners, or some balance of the two? This is a good question best answered by the fact that since even elite athletes use a coach, it seems important to extend learning skills activities to all learners, especially for those skills required for lifelong learning as a physician.
A needs assessment will provide guidance in setting programmatic goals and designing services. Existing learners, recent graduates, faculty members, professional educators, staff in a student affairs office, and community practitioners can reflect on the challenges that they have faced as learners in the classroom and clinical setting to provide a broad perspective for planning (Uijtdehaage et al, 2007b). Once a programme is implemented, the needs assessment results can be used as a measure of programme effectiveness and a guide for continuous improvement (Uijtdehaage et al, 2007a).
The next decision in building a learning development programme is whether learning skills should be taught in a separate course, embedded across the curriculum, or only addressed through individual counselling. Although there is little evidence to support one approach over the other, it is clear that learning skills must be explicitly addressed rather than just implicitly modelled if all learners are expected to develop them (Perkins, 2009). If embedded in an existing course or clinical attachment, students or residents will need to receive feedback on their successful demonstration of learning habits, suggesting that faculty development and learner development actually go hand in hand.
It is important for a learner development programme to provide a number of services. Several of these could be linked to other units within the institution: for example, offices of student affairs or medical education. Attachment to offices of medical education may, in fact, strengthen learner development activities by tying them more closely to academic components of the institution. The following services are those most commonly provided.
Individual learning skills counselling
Individual counselling may include discussion of particulars related to learner performance, time management practices, sleep schedules, or moving from a surface learning approach to one more conducive to deeper understanding. It may also include individual assessments related to study skills, reading level, problem-solving skills, or referrals to other professionals for psychiatric problems or learning differences/disabilities. An individualised learning contract is a useful device for structuring activities and identifying the particular goals for each learner.
Workshops
Group sessions on particular learning skills or strategies can help to communicate the importance of personal and academic development to all learners. Topics such as analysing examination performance, scheduling study time, and preparing for licensing exams prove quite popular, particularly when the sessions provide an opportunity to practice newly learnt skills with feedback from peers and faculty. Additional learners, beyond those in academic difficulty, will often attend such workshops to gain insights or ‘secrets’, helping to destigmatise the development programme as being applicable only to those in academic difficulty.
Peer-tutoring
Peer-tutoring provides an opportunity for learners to learn from more advanced learners who have already successfully completed particular courses, mastered clinical skills, and/or demonstrated effective study strategies. The training of peer-tutors is important in that the simple mastery of the material is necessary, but not sufficient for a tutor. In addition, some screening and selection is required, as not all students will be suited to the role of peer-tutor. It is also important that the peer-tutors learn to serve as facilitators of learning rather than merely re-lecturing the targeted content. Helping peer-tutors learn about open-ended questioning, reflective listening, and modelling of learning behaviours can enhance their effectiveness.
One form of peer-tutoring, supplemental instruction (SI), integrates lessons on memorisation, problem solving, time management, and concept mapping into content review sessions for a targeted course (Hurley et al, 2003). A Medical Scholars Programme is another peer-tutoring model based on the work of Triesman (Osborn and Fullilove, 1993; Triesman, 1993). Peer-tutors meet weekly for 2 hours with groups of 20–25 learners to collectively answer questions in anatomy, biochemistry, and physiology framed in such a way as to relate basic science to clinical conditions. Studies have shown that medical students enrolled in such programmes perform better on subsequent basic science tests and licensing examinations than might be predicted by their admissions data.
Personalised assessment
Individual assessments of learning skills can be helpful for learners at all levels, but basic skills inventories such as the following, which are well studied in the literature, are particularly useful in the context of medical education:
One of the authors (Lawrence Doyle) has used these instruments to provide individual learners from pre-medical students, through to residents with a personalised assessment of their readiness for the challenges of continuous and self-directed learning. Such assessments, and discussions of a particular learner’s performance, can illustrate for the individual whether the mix of study and test-taking habits adopted over years of previous success as a learner are helping or hindering performance in the current setting. Repeated studies have shown that surface learning is the least successful strategy for medical students. Most medical students adopt a strategic approach in which they shift their study skills, from memorising to working for a deeper understanding, based on the nature of the examinations they are preparing to take.
Practice tests and formative assessments
Accurate assessment of one’s knowledge and skills is an essential aspect of lifelong learning (Davis et al, 2006). Skills in self-monitoring and self-assessment can be promoted through the use of practice tests and formative assessments coupled with reflection and feedback. For example, weekly formative assessments are part of the medical student curriculum at UCLA with the goal of promoting students’ accurate assessment of their level of understanding on factual recall, application, and interpretation questions related to content of the previous week or assigned readings (Krasne et al, 2006). The results of formative assessments or practice tests of any type can assist faculty, academic support professionals, or peer-tutors, as they guide students in reflecting on current personal results by asking them to identify their depth of understanding, specific knowledge gaps, and projected levels of performance. Faculty feedback on student insight and accuracy is an important aspect of this reflective process (see also Chapter 13).
Well-being counselling and referrals for fitness appraisal
Accreditation standards for medical schools often include the need for personal support systems to assist students in productively managing the physical and emotional demands of medical school. These are not necessarily psychiatric services, although the assessment of learning disabilities may be important to provide. Instead, a well-being programme can teach successful coping mechanisms by linking learners with more advanced learners and faculty members who have successfully navigated similar experiences, by providing a comfortable place for informal learner gatherings, and by offering a friendly listener when learners just need to talk. Formal support groups can be created to address topics such as family issues, professional identity, career choice, death and dying, body image, substance abuse, gender roles, and cultural differences. Learning support professionals can provide referrals to other professionals for in-depth assessment of learning disabilities such as dyslexia or attention-deficit/hyperactivity disorder (ADHD), or for psychological or pastoral counselling for issues such as the ‘imposter phenomenon’ in which students come to view their acceptance to or continuance in medical school as a sham that will soon be dispelled (Clance and Imes, 1978).
Evaluation and curriculum development
Curricular evaluation and development responsibilities are not typically embedded in a student affairs office, but located in other parts of the institution. However, access to such resources can significantly affect success of a student development programme. Assistance in designing, conducting, and analysing needs assessment surveys and programme evaluation studies can be extremely valuable in developing, improving, or sustaining a learning support programme. Summative evaluations of a particular iteration of programming can identify features associated with programmatic success. Well-developed formative assessments can be used for continuous quality improvement.
Establishing a culture of learning
Learning to learn is a critical skill that must be deliberately practised if it is to develop. Thus, programmes for learner development should be integrated with the curriculum planning and evaluation processes for the institution. A culture of learning needs to permeate the curriculum, and the entire institution, if students and postgraduate trainees are to value the development of their skills as learners.
Structured with this goal in mind, the format of classroom sessions and clinical rotations can provide learners with opportunities to engage in guided self-assessment, to set their own learning goals, and to access the resources needed to direct their own learning. For example, in PBL, learners learn to draw on their prior knowledge, ask questions about issues raised in a problem that they do not personally understand, and educate themselves and one another through subsequent self-study. The problems create a level of ‘desirable difficulty’ where challenge motivates without overwhelming (Bjork, 1994). Team-based learning (Searle et al, 2003) reinforces the value of self-quizzing and peer teaching. Being assigned the responsibility to care for a patient in a clinical placement can stimulate the learner to search out and critically appraise the current evidence on treatment options. These skills need to be made a part of the assessment of learner performance as well, if the message about their importance is to be clearly communicated to students or residents.
Faculty development is critical to the success of a learning culture so that the intended curriculum is implemented in a way that reinforces learning skills and engages learners in using the type of study habits described above. John Hattie, New Zealand author of Visible Learning (Hattie, 2009), in a published interview, described the effects of what teachers do on learning outcomes based on his review of meta-analyses relating teaching to achievement (Shaughnessy and Moore, 2008):
What teachers do matters; and what certain teachers do matters in a most positive manner. The most powerful influences on students come from those who know their subject matter and who are trained in the proficiencies of ‘teaching in a most deliberate and visible manner’ with a particular emphasis on teaching learning strategies in the context of the subject being taught. Strategic thinking and the skills needed to deal with the challenge of the unfamiliar are the keys to teaching and learning.
(p 240)
Creating a viable learning community outside class is also important in developing a learning culture. In teaching calculus to college students, Triesman and his colleagues (Triesman, 1993) observed strong social influences on the academic performance of different groups of students, largely along ethnic and racial lines. In seeking an explanation, Triesman considered differences in performance motivation, prior education, family support, and socio-economic status, but none of these variables seemed to matter. He then designed a case study to interview and videotape the students as they studied the material outside class. What he found was that the social interactions and focus of the two groups were extremely different. The college students who did poorly tended to study alone, did not take advantage of other students or faculty as resources, and tended to separate the educational and social parts of their lives. The students who were successful did study alone at times, but a regular part of their study was an interaction with other students in which they talked about education and their future careers, critiqued each others’ problem solving and use of language, practised on old tests, and sought the support of acquaintances or older siblings who had completed the coursework. The underperforming group did not use any of these strategies. However, when the underperforming group of students was taught to work together, and to interact about their education and future careers, their academic performance improved. The learning community programme was so successful that it continues to be replicated, successfully, at colleges, universities, and medical schools around the world (Osborn and Fullilove, 1993).
Barriers to implementation
Few learning skills counsellors are available, particularly at the medical school level where skills counselling might include work on advanced science materials, preparation for licensing examinations, study strategies for mastering an ever-expanding body of scientific knowledge, and skills for succeeding in the unstructured learning environment during clinical rotations. Few courses of study exist for the development of learning skills counsellors who are familiar with the special demands of medical education. Although graduate courses in education and psychology are numerous, most focus on younger learners, rather than adults, or on research rather than application. Some medical schools have drawn on the expertise of professional medical educators with expertise in cognition and learning. Alternatively, faculty members from the basic or clinical sciences with experiences in the various learning environments in medical education can develop the skills and knowledge relevant to providing learner development services through a review of the relevant literature on learning, both in general and in medicine, and discussions with established medical education learning skills professionals at other institutions. The fellowships in medical education discussed earlier in this chapter could be helpful to a basic science or clinical teacher interested in making this transition to learning specialist.
Learning to learn strategies
A review of research on learning conducted by a panel of experts for the US National Academies of Science from a variety of fields, from neuroscience to education, identified three key principles in successful learning, presented in the report How People Learn (Council, 2000). They bear a striking resemblance to the cognitive principles of learning, described in Chapter 2:
The goal of learner development programmes is to help learners of any age understand the process of learning and develop the attitudes, knowledge, and skills needed to maximise that process. Topics generally include strategies for reading, note-taking, memorisation, deep understanding, test-taking, time management, physical readiness, self-quizzing, and behaviour modification. The following suggestions have been particularly valuable over the years for medical students and residents with whom we have worked.
Reading
The simple act of reading daily for periods of an hour or more can increase one’s reading comprehension and enlarge vocabulary. Initially skimming over material prior to a closer reading and, some time later, employing a post-reading process can help learners develop a deeper understanding of the material studied as well as a better overall memory of factual detail through purposeful repetition. Active self-questioning during reading, in which learners, after a page or two, ask themselves what are the key concepts here, how do they relate to things they already know, and how might the concepts apply to a real-life situation, can strengthen both retention and comprehension. Reciprocal reading, developed by Ann Brown and Anne Marie Sullivan Palinscar for use with school-age children, engages two students in questioning, summarising, clarifying, and predicting by alternating ‘teacher’ and ‘learner’ roles using a text that both have read. These active reading strategies are not often used by less well-prepared learners, who tend to simply re-read the text, with the second reading simply being done more quickly. Given the amount of reading expected in medical school, students need to be able to read for understanding the first time round, and to increase their reading speed without the loss of comprehension. Active reading strategies can reduce the time spent on re-reading and move the learner beyond ‘rote’ memorisation to the development of a deeper conceptual framework into which subsequent facts can be integrated.
Note-taking
The major point in any discussion of note-taking strategies with learners is the importance of active engagement throughout a lecture or reading session. With the advent of Podcasts and easy access to digital files of lecture slides, learners no longer have to attempt to write down every word in a lecture. Instead, they can engage in constant decision-making about the relative importance of concepts and details that can then be reflected in their written notes taken as they listen. For example, learners should determine the importance of a concept delivered by the lecturer and vary their note-taking format to reflect relative importance by varying indentation from the left margin or marking with differently coloured pens. These strategies keep learners involved while providing an organisation to their notes that is useful for subsequent review. Since more than half the information in a lecture is forgotten within the next 24 hours, one of the most important study skill activities is simply to review materials the same day they were presented rather than waiting until the weekend. Lecture notes, like other texts, can be approached with the same active reading strategies discussed above. Lectures that are recorded and archived or broadcast as Podcasts have the advantage of linking the words of the lecture to the slide being shown at that point in the lecture. Rather than simply listening to the entire lecture again, the learner can decide what portion of a lecture he or she needs to review and jump immediately to that linked slide and presentation.
Memory
Mnemonics for learning medicine have been passed down from generation to generation of medical students, such as OLDCART or SOCRATES for assessment of pain (i.e. Onset–Location–Duration–Characteristics–Aggravating Factors–Relief–Treatment – or – Signs and symptoms–Onset–Character– Radiation–Alleviating Factors–Timing–Exacerbating Factors–Severity), ROYGBIV (Red–Orange–Yellow–Green–Blue–Indigo–Violet for the colours of the visible portion of the electromagnetic spectrum or of the rainbow), and OILRIG (Oxidation Is a Loss of electrons while Reduction Is a Gain of electrons) from general chemistry. A certain amount of sheer memory continues to be important in medicine. In the early stages of learning, the mnemonic provides scaffolding for disparate ideas that do not yet make ‘logical sense’ or for linking the unfamiliar with something familiar. While such mnemonics lose their power as understanding deepens, they can remain important in areas where use of that understanding is called upon infrequently. A mnemonic later provides a safety net checklist so that essential aspects of the concept or procedure are not inadvertently forgotten due to infrequent use. Useful mnemonics can be visual or verbal, original or inherited, graphic or textual. The only criterion is that they must be compelling enough to be remembered by the user (Whimbey and Lochhead, 1999)!
Test-taking
A critical tool in improving test-taking skill is error analysis from actual or practice examinations. Problem Solving & Comprehension, 6th Edition (Whimbey and Lochhead, 1999) provides an excellent practice test for identifying and analysing non-content-related errors, such as misreading, making unsupported inferences, failing to consider all of the options, not following through on ones’ own logic, or frequently changing answers. An error analysis of actual examination questions allows for identification of content-related errors as well. Content errors might be due to learners mistakenly failing to cover the material at all during study or purposefully ignoring some material judged to be unimportant. A second type of content error occurs when the learner is not able to apply known material to a new situation. This could be a problem with transfer, not seeing the similarity between the test item and the learnt material, or it could be a problem of having memorised the material rather than using active reading methods to reach a deeper understanding. Content mistakes can be reduced by learners applying active reading and note-taking strategies. Anxiety can be a third cause of examination difficulties. Under stress, learners may not read the questions carefully, block on answers that they would otherwise know under non-test conditions, have difficulty in apportioning their time, or engage in second-guessing themselves. Test anxiety may require psychological counselling if it persists after the problem has been identified and the learner has worked on addressing it. Finally, some persistent difficulties may be the result of actual learning disabilities that require formal assessment. If clinically identifiable learning disabilities are found, the learner may require modified testing conditions such as extended time or isolation to avoid distractions.
Time management
The amount of material to be learnt or clinical work to be accomplished in a typical medical school curriculum may require new time management skills for students, especially when entering a new phase of responsibility. Students can be encouraged to create a personal schedule of appointments, classes, and study times and construct an active to-do list. A schedule helps the student break a task down into manageable portions that can be accomplished within a particular day or study session, thereby making the entire task easier to complete. To-do lists can help the student to make appropriate decisions for a given bit of free time. With the extensive scheduling and notes programmes available on smart phones and other handheld devises, these personal planning activities are easier to implement than ever before and have the added benefit of ever-present message alert systems.
Deliberate practice
Drawing on decades of work on expertise in fields as diverse as chess and music, Ericsson and his colleagues (Ericsson, 2004; Ericsson et al, 1993) have identified the characteristics of deliberate practice associated with reproducible skilled performance. Such practice is distinguished from mere experience by four features: (1) a targeted goal, (2) a motivation to improve, (3) frequent feedback, and (4) opportunities for repetition with increasing levels of challenge. Deliberate practice can be helpful as learners seek to develop new learning skills or master new concepts or clinical skills. Learners can be taught how to structure their study periods to include practice tests with items selected to demonstrate accomplishment of a clearly defined, relatively narrow goal. Feedback needs to be available from a coach, although studies continue to refine what type of feedback is most helpful. Mastery requires a study schedule that includes returning to one’s learning goal from time to time with new contexts or examples embedded in subsequent practice tests. The role of the learning skills specialist is to assist the learner in setting a manageable goal, given the time and resources available, securing mechanisms for feedback, and developing a study plan that includes spaced practice and re-testing.
Peak performance skills
Academic performance can be greatly affected by a person’s psychological readiness. This is a regular part of athletic training but less commonly applied to improving academic performance. Strategies from the fields of Sports Psychology or Peak Performance (Jarvis, 2000) can help learners maximise their psychological readiness for academic tasks such as studying, attending lectures, taking examinations, or even managing difficult interactions with colleagues, faculty, or patients.
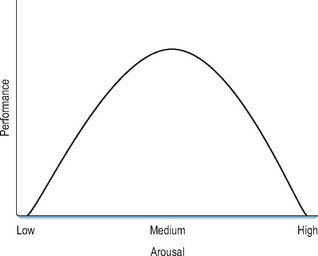
Psychological readiness means that the level of stress associated with performance is experienced as challenging but not overwhelming. The Yerkes–Dodson curve shown in Figure 19.1 (Jarvis, 2000) shows that one’s performance is often related to the level of underlying stress produced by the event or resulting from unrelated life situations. Performance actually rises to a peak with increasing stress before dropping off as the stress reaches overwhelming levels. Learners need to understand the difference between good stress and bad stress, between productive challenges and debilitating anxiety. They need to recognise the onset of negative stressors and use relaxation exercises to lower stress levels. Relaxation exercises provide one means of managing stress so that the learner avoids or delays a negative level of stress.
Controlled breathing is one form of relaxation exercise. Taking slow deep breaths tends to increase the oxygen content of the blood, increase blood flow to the brain, and loosen and expand chest muscles. Breathing practice begins by simply filling and emptying ones lungs to a slow, consistent count of four. Repeating this slow cycle has a calming effect that is brought on more readily with regular practice. Adding a four-count hold between inhaling and exhaling tends to help focus on the breath rather than the coming performance. A second relaxation strategy involves releasing muscle tension by first tensing a group of muscles, holding it tense, and then relaxing it. Progressive relaxation involves repeating the strategy on sequential muscle groups over the entire body. If the count of the cycle is extended until the muscle group tires, this exercise can help learners fall sleep more effectively after a period of intense concentration. With enough practice, the relaxation response can become an almost automatic response to situations that the participant finds stressful.
Psychological readiness may also mean that the person is primed for an upcoming action. The process of visualisation is a powerful tool for priming. It may also have some of the same practice effects as actually performing that same action. Research on a special type of neuron in the brain, the mirror neuron, suggests that when a person observes or visualises an action, the neural pathway that is activated in his or her brain is similar to that used during actual performance of that action (Gallese et al, 2004). For example, an Olympic athlete getting ready to compete in an event would find it quite natural to envision him or herself completing the course, making the ski jump, swimming the required laps. For students or residents preparing to take an examination, such visualisation can involve imagining the types of questions that they will be able to answer after studying specific content or what a positive performance on a patient encounter to be observed by a faculty member will look like. The more vivid and multi-sensorial the image becomes, the more effective it can be in priming the learner for a particular performance.
A third area of psychological readiness requires developing self-confidence. Athletes turn to self-talk to build confidence and increase persistence while preparing for challenging performances. When learners constantly tell themselves that they have difficulty on standardised tests or cannot perform well in mathematics, they may produce a self-fulfilling prophecy (Aronson and Steele, 2005). Without self-confidence, learners may fail to persist in the face of difficulty, lose confidence in what they know during an examination, or even decide not to pursue medicine after experiencing one failure. Self-talk can be supplemented by positive messages from faculty members and counsellors about high expectations for success.
Even concentration can be practised. Focussing visually on a particular object, a candle for instance, and practicing staying focussed on that object for expanded periods of time can help one learn how to narrow focus. In the same concentration exercise, by attempting to widen and narrow the visual field, the learner can experience the ability to control concentration. Similar strategies in terms of focusing on one’s hearing, or other sensory input, then expanding and narrowing awareness of that stimulus, can help the learner to later control the distractions that are so much a part of modern life.
Psychological readiness includes physical readiness as well, e.g. nutrition, sleep, exercise, and caffeine. The timing and content of meals are as important to learners as to athletes. Complex carbohydrates, protein, and limited amounts of fat can all affect a learner’s ability to pay attention during a long day of classroom or clinical work. Eating a suitable breakfast has been associated with improvements in academic performance. Caffeine, which can be helpful to learning in small doses, has been shown, in larger doses, to limit a learner’s ability to assimilate new information or to make new associations with previously learnt information. Ingestion of refined sugars can lead to a drop in blood sugar, which may hinder concentration.
Sleep is a central issue for discussion with learners as well. Humans tend to need 8 hours of sleep. Recent studies suggest that 90-minute REM cycles provide time for consolidating information and that missing a cycle can inhibit recall (Axmacher et al, 2009). Students may believe that the way to master the enormous amount of material in a medical school curriculum is to study long into the night, day after day. Sleep deprivation is a common complaint among post-graduate trainees and at the heart of policies designed to control the pattern and amount of work permitted for residents. In addition to concerns about patient safety, this lack of sleep may actually decrease learning effectiveness. While recommendation from an instructor or learning skills specialist that more sleep might be appropriate is oftentimes met with disbelief, after such a simple modification of behaviour, performance generally improves. Exercise, stretching, and cardiovascular activities can help the learner to stay healthy and provide a counterpoint to the intense concentration involved in studying.
A learner who understands these simple exercises for psychological readiness will learn that responses to stress, time management, concentration, and persistence are under his or her personal control and not dictated by life or academic situations. Combined with healthy lifestyle habits that promote physical readiness for learning, the learner is ready for peak performance. A learning skills counsellor can address these strategies in individual coaching sessions or workshops when particularly challenging academic activities are upcoming or completed.
Action–reflection–action cycle
Learning from immersion in clinical care responsibilities can be maximised, for students and residents, if the learner is taught to use an action–reflection–action approach to generate useful, personal knowledge (Boshuizen, 2004). Students often see clinical work as unplanned and spontaneous. However, as even the most urgent situation can benefit from planned action, the first critical skill is creating a prepared mind. Gut intuition is insufficient unless that intuition is informed by extensive knowledge and experience. However, learners with little actual experience in caring for a patient with a given complaint can prepare for the patient encounter by learning to visualise the rhythm and routine (the algorithm) of the presenting complaint, and subsequently predicting the desirable consequences. Preparation, when time permits, can also include background reading or asking questions of experienced peers or teachers. Such preparation helps the learner to create an interpretive frame within which effective, rapid decision-making can occur. A second critical skill, often missed in the process, is reflective analysis, raising questions such as whether the desired outcome was achieved. And if not, why not? Or if so, why so? Such reflection can be either an individual or a team activity. In order to use this newly generated knowledge successfully in subsequent patient care situations, the learner then must create conditional knowledge in the form of ‘if-then’ linkages between complex knowledge and desirable actions and outcomes, or at a more advanced level, illness scripts. These more generalised knowledge structures avoid over-contextualisation of learning and assist in retrieval for subsequent application in new clinical situations.
Widening participation: preparing a pipeline to medicine
Beyond improving the learning skills and performance of current medical students or residents, an increasingly important reason to build learning development programmes is the emphasis on widening participation in the medical workforce. As Garlick and Brown (2008) note, in discussing the development of the Extended Medical Degree Programme in the United Kingdom:
Today’s prevailing view is that tomorrow’s doctors should reflect the social and ethnic diversity of the countries in which they practise. To this end, initiatives to widen participation have been started in medical schools in several countries.
(p 111)
Such an expanded focus can be seen worldwide, from a programme for Aboriginal Medical and Dental Health at the University of Western Australia to the new Northern Ontario School of Medicine in Canada, where faculty are working to increase the numbers of Aboriginal students enrolled. In the universities of Bergen and Tromsø in Norway, special admissions programmes have worked for over 40 years to increase the numbers of Sami people who matriculate in medical school. A new standard for medical school accreditation in the United States requires that ‘each medical school must develop programmes or partnerships aimed at broadening diversity among qualified applicants for medical school admission’ (www.lcme.org/standard.htm). In the United States, having a diverse student body in medical school has been shown to be associated with a greater commitment on the part of graduating physicians to social justice and a readiness to care for patients unlike themselves (Saha et al, 2008). Studies in the USA have also shown that physicians from underserved populations are more likely to serve those populations, thus improving access to care (Saha and Shipman, 2008).
In reaching out to new student populations, medical schools will need to draw from groups that have not traditionally been competitive for, or even interested in, pursuing a career in medicine. A significant portion of such students come from disadvantaged educational and/or economic backgrounds and have academic records that are weak when compared with their demonstrated record of commitment to, and experience with, medically underserved communities. It is incumbent on medical schools to provide leadership to outreach and pipeline programmes that begin early in students’ educational lives, to strengthen confidence, and build academic skills in order to create a competitive diverse applicant pool for medicine.
Pipeline programmes in the United States, in existence since the mid-1970s, have traditionally focused on high school and college students, often providing summer residential programmes on a university medical school campus so that participants have a chance to experience the medical school environment. Such programmes are typically six to eight weeks in duration and designed to provide participants with exposure to science and mathematics prerequisites for medical school. These programmes usually include some clinical experience or the opportunity to shadow a health care professional. The Robert Wood Johnson Foundation’s Summer Medical and Dental Education Programme (SMDEP, www.smdep.org/) coordinated by the AAMC and the American Dental Education Association is for college students who are 2 years away from applying to medical school. While the majority of SMDEP programmes re-teach basic maths and science competencies, at UCLA the programme includes a large amount of learning skills development and curricular activities focused on practising those skills. Students learn the skills of asking questions about scientific and clinical phenomena, locating sources to answer those questions, and explaining what they have learnt to a peer in PBL tutorials. Working in other small groups led by medical students, who are often themselves from disadvantaged backgrounds, learners search the internet to learn about a common health disparity or the features of a community lacking access to health care. After collecting information to define the problem, learners explore what is currently being done to address the selected issue and recommend changes in health policy, the design of health care systems, community engagement, or even medical education to help resolve the problem. They collaborate as a group in creating a presentation on their recommendations for the faculty and other students enrolled in the programme. Learners also spend time in personal choice reading to work on speed and vocabulary. Participating learners have demonstrated a move from a surface to a deeper approach to learning, improved reading skills, higher scores on practice examinations on science materials, a broader range of problem solving strategies, and an increased commitment to pursuing a career in medicine or dentistry (Doyle, unpublished data).
Conclusion
Faculty members develop. Learners develop. The environment for teaching and learning continuously improves. That is the rhythm of a learning organisation. Resources committed to faculty and learner development should be seen as investments in creating, sustaining, and enhancing the vitality of a medical school or academic health care institution, preparing these institutions to productively respond to the educational implications of the constantly changing demands of scientific discovery and the health care needs of our communities.
Implications for practice
A vibrant learning organisation requires attention being given to the policies and programmes in place in medical schools and other medical education institutions to support the educational mission. Faculty development can help create a collegial learning community that shares a vision for personal excellence, continuous learning, and scholarship in teaching; promotes continuous quality improvement through collaborative reflection and action; and makes the contributions of scholarly teachers and educational scholars visible and rewarded. Learner development can provide the personal and professional skills needed to maximise learning during the long educational process of developing medical expertise. Creating and sustaining organisational vitality requires the empowerment of both personal and corporate leadership to lobby for the very best educational programmes delivered by scholarly teachers and informed by the work of educational scholarship to maximise the learning of those entrusted into our care.
Albanese M.A., Dottl S., Nowacek G.A. Offices of research in medical education: accomplishments and added value contributions. Teach Learn Med. 2001;13:258-267.
Amin Z., Hoon Eng K., Gwee M., et al. Medical education in Southeast Asia: emerging issues, challenges and opportunities. Med Educ. 2005;39:829-832.
Aronson J., Steele C. Stereotypes and the fragility of academic competence, motivation and self concept. In: Elliot A., Dweck C., editors. Handbook of competence and motivation. New York: The Guilford Press; 2005:436-456.
Axmacher N., Draguhn A., Elger C., et al. Memory processes during sleep: beyond the standard consolidation theory. Cell Mol Life Sci. 2009;66:2285-2297.
Benor D.E., Mahler S. Teacher training and faculty development in medical education. Isr J Med Sci. 1987;23:976-982.
Bensinger L., Meah Y., Smith L. Resident as teacher: the Mount Sinai experience and a review of the literature. Mt Sinai J Med. 2005;72(5):307-311.
Bjork R.A. Memory and metamemory considerations in the training of human beings. In: Metcalfe J., Shimamura A.P., editors. Metacognition: knowing about knowing. Cambridge, MA: MIT Press; 1994:185-205.
Bland C.J., Seaquist E., Pacala J.T., et al. One school’s strategy to assess and improve the vitality of its faculty. Acad Med. 2002;77:368-376.
Bloom S. The medical school as a social organization: the sources of resistance to change. Med Educ. 1989;23:228-241.
Boelen C., Boyer M.H. A view of the world’s medical schools: defining new roles. Geneva: World Health Organisation, 2001.
Boshuizen H.P.A. Does practice make perfect? A slow and discontinuous process. In: Boshuizen H.P.A., Bromme R., Gruber H., editors. Professional learning: gaps and transitions on the way from novice to expert. Dordrecht: Kluwer Academic Publishers, 2004.
Boyer E.L. Scholarship reconsidered: priorities of the professoriate. Princeton, NJ: Princeton University Press, 1990.
Branch W.T., Frankel R., Gracey C.F., et al. A good clinician and a caring person: longitudinal faculty development and the enhancement of the human dimensions of care. Acad Med. 2009;84:117-125.
Clance P., Imes S. The imposter phenomenon in high achieving women: dynamics and therapeutic intervention. Psychother Theory Res Pract. 1978;16:231-247.
Cohen J.J. Revisiting the medical school education mission at a time of expansion. New York, NY: Josiah Macy, Jr. Foundation, 2009.
Council N.R. How people learn: brain, mind, experience, and school: expanded edition. Washington, DC: National Academies Press, 2000.
Davis D.A., Mazmanian P.E., Fordis M., et al. Accuracy of physician self-assessment compared with observed measures of competence: a systematic review. JAMA. 2006;296(9):1094-1102.
Dewey C.M., Friedland J.A., Richards B.F., et al. The emergence of academies of educational excellence: a survey of US medical schools. Acad Med. 2005;80(4):358-365.
Ericsson K.A. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10 Suppl):S70-S81.
Ericsson K.A., Krampe RTh, Tesch- Romer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100:363-406.
Fleming V.M., Schindler N., Martin G.J., et al. Separate and equitable promotion tracks for clinician-educators. JAMA. 2005;294:1101-1104.
Gallese V., Keysers C., Rizzolati G. A unifying view of the basis of social cognition. Trends Cogn Sci. 2004;8(9):396-403.
Garlick P.B., Brown G. Widening participation in medicine. Br Med J. 2008;336:1111-1113.
GMC. Tomorrow’s doctors. London: General Medical Council, 2009.
Gozu A., Windish D.M., Knight A.M., et al. Long term follow-up of a 10-month programme in curriculum development for medical educators: a cohort study. Med Educ. 2008;42(7):684-692.
Griffith C.H., Georgesen J.C., Wilson J.E. Six-year documentation of the association between excellent clinical teaching and improved students’ examination performances. Acad Med. 2000;75(10 Suppl):S62-S64.
Gruppen L.D., Frohna A.Z., Anderson R.M., et al. Faculty development for educational leadership and scholarship. Acad Med. 2003;73:137-141.
Gruppen L.D., Simpson D., Searle N.S., et al. Educational fellowship programs: common themes and overarching issues. Acad Med. 2006;81:990-994.
Guilbert J.J. Educational handbook for health personnel. Geneva: World Health Organisation, 1981.
Hattie J.A.C. Visible learning: a synthesis of eight hundred meta-analyses related to achievement. New York: Routledge, 2009.
Huber M., Hutchings P. The advancement of learning: building the teaching commons. San Francisco, CA: Jossey-Bass, 2005.
Hurley K.F., McKay D.W., Scott T.M., et al. The supplemental instruction project: peer-devised and delivered tutorials. Med Teach. 2003;25(4):404-407.
Irby D., Cooke M., Lowenstein D., et al. The academy movement: a structural approach to reinvigorating the educational mission. Acad Med. 2004;79:729-736.
Jarvis M. Sport psychology. London: Taylor & Francis, 2000.
Jason H., Westberg J. Teachers and teaching in US medical schools. Norwalk, CT: Appleton-Century–Crofts, 1982.
Krasne S., Wimmers P.F., Relan A., et al. Differential effects of two types of formative assessment in predicting performance of first-year medical students. Adv Health Sci Educ. 2006;11:155-171.
Mattick K., Dennis I., Bligh J. Approaches to learning and studying in medical students: validation of a revised inventory and its relation to student characteristics and performance. Med Educ. 2004;38:535-543.
Mazmanian P.E., Davis D.A. Continuing medical education and the physician as a learner: guide to the evidence. JAMA. 2002;288(9):1057-1060.
Mitchell R. The development of the cognitive behavior survey to assess medical student learning. Teach Learn Med. 1994;7:233-240.
Mitchell R., Regan-Smith M., Fisher M., et al. A new measure of the cognitive, metacognitive, and experiential aspects of residents’ learning. Acad Med. 2009;84:918-926.
Neher J.O., Gordon K.C., Meyer B., et al. A five-step ‘microskills’ model of clinical teaching. J Am Board Fam Med. 1992;5:419-424.
Norcini J.J., Burdick W., Morahan P.S. The FAIMER Institute: creating international networks of medical educators. Med Teach. 2005;27:214-218.
Notzer N., Abramowitz R. Can brief workshops improve clinical instruction? Med Educ. 2008;42:152-156.
Osborn E., Fullilove M. Lessons learned from FIPSE projects II. San Francisco: University of California, 1993. The Medical Scholars Program. Washington, DC, Office of Post Secondary Education
Perkins D.N. Making learning whole: how seven principles of teaching can transform education. San Francisco, CA: Jossey-Bass, 2009.
Pololi L., Knight S.M., Dennis K., et al. Helping medical school faculty realize their dreams: an innovative, collaborative mentoring program. Acad Med. 2002;77(5):377-384.
Post R.E., Quattlebaum R.G., Benich J.J. Residents-as-teachers curricula: a critical review. Acad Med. 2009;84:374-380.
Pugsley L., Brigley S., Allery L., et al. Counting quality because quality counts: differing standards in master’s in medical education programmes. Med Teach. 2008;30:80-85.
Rice E. Scholarship reconsidered: history and context. In: O’Meara K., Rice R.E., editors. Faculty priorities reconsidered: rewarding multiple forms of scholarship. San Francisco, CA: Jossey-Bass; 2005:17-31.
Ridley G.T., Skochelak S.E., Farrell P.M. Mission aligned management and allocation: a successfully implemented model of mission-based budgeting. Acad Med. 2002;77:124-129.
Saha S., Shipman S.A. Race-neutral versus race-conscious workforce policy to improve access to care. Health Aff (Millwood). 2008;27:234-245.
Saha S., Guiton G., Wimmers P.F., et al. Student body racial and ethnic composition and diversity-related outcomes in US medical schools. JAMA. 2008;300(10):1135-1145.
Searle N.S., Haidet P., Kelly P.A., et al. Team learning in medical education: initial experiences at ten institutions. Acad Med. 2003;78(10 Suppl):S55-S58.
Searle N.S., Hatem C.J., Perkowski L., et al. Why invest in an educational fellowship program? Acad Med. 2006;81:936-940.
Senge P. The fifth discipline: the art and practice of the learning organization. New York: Doubleday, 1990.
Shaughnessy M., Moore T. A reflective conversation with John Hattie. North Am J Psychol. 2008;10:239-248.
Simpson D., Hafler J.P., Brown D., et al. Documentation systems for educators eeking academic promotion in US medical schools. Acad Med. 2004;79:783-790.
Simpson D., Fincher R.M.E., Hafler J.P., et al. Advancing educators and education: defining the components and evidence of educational scholarship. Washington, DC: Association of American Medical Colleges, 2007.
Sorcinelli M.D. Creating the future of faculty development: learning from the past, understanding the present. Bolton, MA: Anker Publishing, 2006.
Steinert Y., Mann K., Centeno A., et al. A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME Guide No. 8. Med Teach. 2006;28(6):497-526.
Triesman U. Lessons learned from FIPSE projects II: University of California, Berkeley, CA, The Professional Development Program. Washington, DC: Office of Postsecondary Education, 1993.
Uijtdehaage S., Vermillion M., et al. ‘Reflective practice’ as a tool for programme evolution. Med Educ. 2007;41:1094-1095.
Uijtdehaage S., Vermillion M., et al. American Educational Research Association (AERA) Annual Meeting. Starting a pipeline program for disadvantaged students: do faculty and students value the same objectives?. 2007.
Walling A., Chinn K.C. A web-based orientation for new faculty members. Acad Med. 2002;77:460.
Watson R.T., Romell L.J. Mission-based budgeting: removing a graveyard. Acad Med. 1999;74:627-640.
WFME. Basic medical education: WFME global standards for quality improvement. Copenhagen, Denmark: World Federation for Medical Education, 2003.
Whimbey A., Lochhead J. Problem solving & comprehension, ed 6. Mahway, NJ: Lawrence Erlbaum Associates, 1999.
Wilkerson L., Irby D.M. Strategies for improving teaching practices: a comprehensive approach to faculty development. Acad Med. 1998;73:387-396.
Wilkerson L., Anderson W.A. Hilliard Jason, MD, EdD: a medical student turned educator. Adv Health Sci Educ Theory Pract. 2004;9(4):325-335.
Wimmers P.F., Schmidt H.G., Splinter T.A. Influence of clerkship experiences on clinical competence. Med Educ. 2006;40:450-458.
L. Wilkerson, D.M. Irby. Strategies for improving teaching practices: a comprehensive approach to faculty development. Acad Med, 73. 1998:387-396.
Provides a framework for planning a faculty development programme.
Professional and Organisational Development Network: a faculty development organisation, largely focussed on classroom teaching in the university. Includes useful links and resources for faculty development programming [Online]. Available from http://www.podnetwork.org/. Accessed December, 2009.
November 2006 issue of Academic Medicine, 81 (11). This issue contains a series of articles on developing and evaluating longitudinal faculty development fellowships
M. Quirk. How to learn and teach in medical schools: a learner centered approach. Springfield, IL: Charles Thomas Publisher. 1996.
Provides a good overview of issues in the design and delivery of medical education.
UT Learning Centre [Online]. Available from http://www.utexas.edu/student/utlc. Accessed December, 2009. Provides an overview of the University of Texas Learning Center, a successful student development programme for university-level students. Includes handouts for student learning skills.
Whimbey A, Lochhead J: Problem solving & comprehension, ed 6, Mahway, NJ, 1999, Lawrence Erlbaum Associates.
Provides strategies useful for a student development programme, including an assessment tool for test-taking habits