CHAPTER 17 The shoulder
Functional anatomy
The upper limb attaches to the trunk via the shoulder (pectoral) girdle. The shoulder complex in total consists of the scapula and clavicle, articulating with the ribcage and sternum to form four joints, all of which require attention in the management of shoulder pain. The clavicle forms a strut for the shoulder, holding the arm away from the side of the body and allowing a greater range of unencumbered movement. At one end the clavicle joins the sternum through the sternoclavicular joint, while at the other it joins the scapula via the acromioclavicular joint.
Definition
The acromioclavicular (A/C) joint is formed between the acromion process of the scapula and the lateral (outer) end of the clavicle. The sternoclavicular (S/C) joint is formed between the top of the sternum and the medial (inner) end of the clavicle.
The scapula rests on the ribcage through muscle tissue alone, an essential point when dealing with stability of the shoulder complex. The glenohumeral joint is the articulation between the head of the humerus and the shallow glenoid fossa of the scapula.
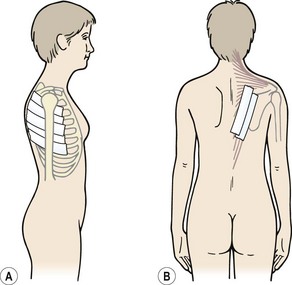
The glenoid fossa is only one third the size of the humeral head, but the fossa is extended by the glenoid labrum attached to its periphery. This fibrocartilage rim is about 4 mm deep with its inner surface lined by, and continuous with, the joint cartilage. The joint itself is surrounded by a loose capsule with a volume twice as large as the humeral head. The anterior capsule is strengthened by the three glenohumeral ligaments. The lower portion of the capsule is lax in the anatomical position, and hangs down in folds. It has two openings, one for the passage of the long head of biceps and the other between the superior and middle glenohumeral ligaments which communicates with the subscapular bursa (between subscapularis and the joint capsule). The capsule is further strengthened by the rotator cuff muscles which act as ‘active ligaments’ and blend with the lateral capsule. The ‘roof’ of the joint is formed by the bony coracoid and acromion processes and the coracoacromial ligament which runs between them, the three structures together forming an arch. Surface marking of the shoulder is shown in Fig. 17.1.
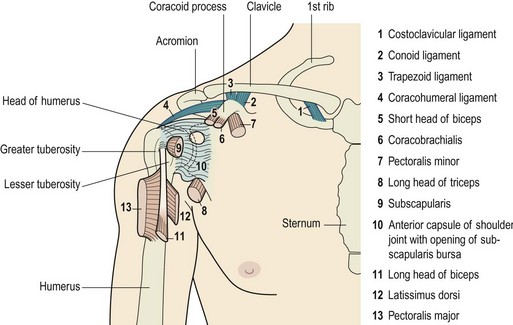
Figure 17.1 Joints of the shoulder complex. 1. Sternoclavicular joint. 2. Acromioclavicular joint. 3. Glenohumeral joint. 4. Scapulothoracic joint.
Rotator cuff action
Most joints have a high degree of passive stability provided by their capsules and ligaments (see also Table 17.3). The shoulder, however, depends more on the active stability provided by its muscles to maintain joint integrity. In the anatomical position, the weight of the arm is largely supported by the coracohumeral ligament and superior capsule. When the arm moves away from the side of the body, tension in the superior capsule is immediately lost. Now joint stability is provided by the rotator cuff muscles alone.
The fibres of the joint capsule are angled forwards and slightly medially when the arm is hanging by the side of the body. As abduction progresses, tension within these fibres causes the shoulder to passively externally rotate. This movement prevents the humeral head from being pulled closer to the glenoid and facilitates a greater range of movement. Importantly, the external rotation also allows the greater tuberosity to clear the acromion process (see below).
Keypoint
The fibres of the joint capsule, angled downwards and slightly medially, are under slight tension at rest. Recoil of these fibres produces a passive lateral rotation force during abduction.
Active abduction of the humerus is accomplished by the supraspinatus and deltoid, acting as the prime movers. With the arm dependent, contraction of the deltoid (particularly the middle fibres) merely approximates the joint (upward translation), because the medial muscle fibres run almost parallel with the humerus. Unopposed, this pull would force the head of the humerus into the coracoacromial arch, resulting in impingement. Contraction of the infraspinatus, subscapularis, and teres minor (Fig. 17.2) causes compression and downward translation to offset the upward translation of deltoid (Culham and Peat, 1993). In an overhead throwing or serving action (Fig. 17.3) the subscapularis moves superiorly because the humerus has externally rotated and the muscle can no longer effectively control the humeral head. The infraspinatus and to a lesser extent the teres minor stabilize the joint anteriorly in this position (Cain, Mutschler and Fu, 1987). For this reason sEMG addresses this muscle in stabilization programmes targeted at throwing sports. By 90° abduction, the pull of the deltoid no longer tends to cause impingement, as shear forces are exceeded by compression, and the humeral head is stabilized into the glenoid (Perry and Glousman, 1995).
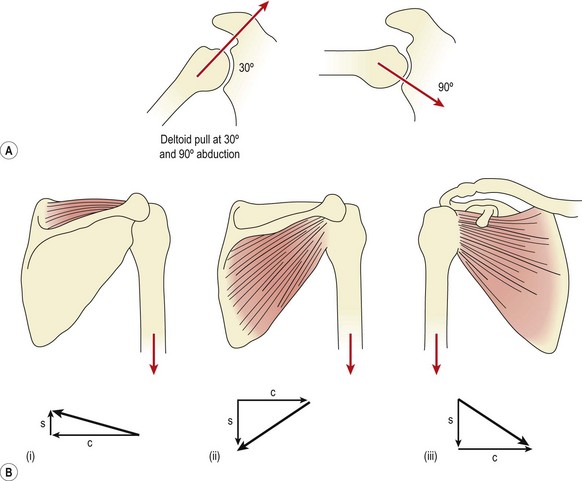
Figure 17.2 (A) Deltoid pull at 30° and 90° abduction. (B) Muscles counteracting pull of deltoid. (i) Supraspinatus, (ii) infraspinatus and teres minor. (C) Subscapularis. Resolution of muscle force: S, shear; C, compression.
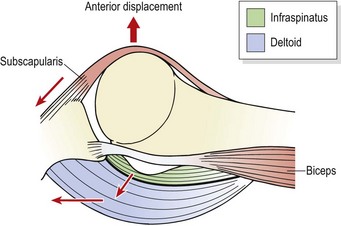
Figure 17.3 Muscular restraints to anterior displacement of the humeral head in an overhead throwing action.
Adapted from Reid (1992), with permission.
The supraspinatus is better placed to produce a rotatory action and therefore initiates abduction for the first 20°. The line of action of supraspinatus is such that less translation is caused, and its contribution to abduction is to reduce the reliance on deltoid and, as a consequence, reduce translation. After 30° of abduction the scapula starts to rotate to alter the glenoid position.
Scapulohumeral rhythm
Motion of the shoulder girdle as a whole changes the position of the glenoid fossa, placing it in the most favourable location for the maximum range of humeral movement. When the glenoid cavity moves, it does so in an arc, the diameter of which is the length of the clavicle (Palastanga, Field and Soames, 1989). The medial border of the scapula moves in a similar but smaller arc and as a consequence the positions of the shoulder girdle structures change in relation to each other.
As the scapula moves medially and laterally towards and away from the vertebral column, the curvature of the ribcage forces the scapula to change from a frontal to a more sagittal position. This, in turn, alters the direction in which the glenoid cavity faces. With elevation, the scapula is accompanied by some rotation, the glenoid cavity gradually pointing further upwards as the scapula gets higher.
With both shoulder abduction and flexion, the clavicle axially rotates. As the scapula twists, the coracoclavicular ligament ‘winds up’ and tightens, causing the clavicle itself to rotate. As the arm is abducted to 90° (phase I and II, see below) the clavicle elevates by 15° but does not rotate. Above 90° (phase III) further elevation of the clavicle occurs (up to 15°) but marked posterior rotation now occurs to 30–50° (Magee, 2002). For this reason a diminished range of movement at either SC or AC joints which reduces clavicular rotation will also impair scapular and therefore glenohumeral motion.
The abduction cycle
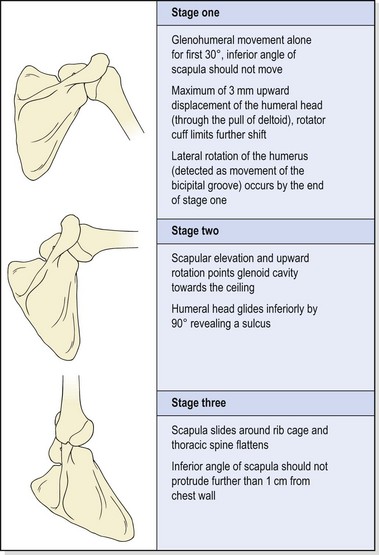
Movement of the arm into abduction may be divided into three overlapping stages (Table 17.1).
Table 17.1 Movement of the arm into abduction
Stage (I)
In stage (I), no movement of the scapula should occur. The scapular stabilizers (serratus anterior especially) should hold the scapula firmly on the ribcage, providing a stable base for the humerus to move upon. As the arm abducts, lateral rotation of the humerus may be detected by palpation of the bicipital groove (intertubercular sulcus). If the humerus is maintained in a neutral position, abduction in the frontal plane is limited to about 90°. Laterally rotating the humerus increases this range to 120° (Lucas, 1973). When the arm is elevated in the sagittal plane, abduction is accompanied by medial rotation due to tightness in the coracohumeral ligament (Gagey, Bonfait and Gillot, 1987). No rotation is required for elevation in the scapular plane (30–45° anterior to the frontal plane). In this position, the joint capsule does not undergo torsion, and the deltoid and supraspinatus are optimally aligned.
At the beginning of abduction in the frontal plane, slight approximation of the humerus should occur (maximum 3 mm) to overcome the weight of the arm as the fibres of the joint capsule are taken off stretch and no longer support the arm through elastic recoil. No noticeable elevation of the shoulder should occur, unless the upper fibres of trapezius dominate the movement. The instantaneous axis of rotation in stage (I) is near the root of scapular spine, and moves superiorly and laterally as abduction progresses.
Stage (II)
By the beginning of stage (II), from 30° of abduction, the scapula should be upwardly rotating to maintain clearance between the acromion and the approaching greater tuberosity of the humerus. Scapular rotation in the beginning of stage (I) occurs as a result of elevation of the clavicle on the SC joint. Between 80 and 140° the instantaneous axis of rotation (IAR) migrates towards the AC joint along the upper central scapular area. Movement then occurs as elevation of the clavicle on the SC joint, and rotation of the scapula on the clavicle at the AC joint. More movement occurs at the glenohumeral joint than at the scapulothoracic joint. Ratios of 2 : 1 are normally quoted, giving 120° of movement at the glenohumeral joint and 60° at the scapulothoracic joint in a total abduction range of 180°. However, some authors (Lucas, 1973) have argued that the ratio is closer to 5 : 4 or 3 : 2 after phase (I) of abduction.
Scapular rotation occurs as a result of force-couples between the various muscles attached to the scapula (Fig. 17.4). Upward (lateral) rotation accompanying shoulder joint abduction or flexion is brought about by contraction of the upper and lower fibres of trapezius and the lower portion of serratus anterior. Serratus anterior is probably the most important of the group. It has two sets of fibres. The fibres of the upper portion run horizontally and slightly upwards, while those of the lower portion are aligned downwards. Both sets pull powerfully on the scapula, anchoring it to the ribcage and causing scapular upward rotation as trapezius lifts the lateral end of the clavicle and acromion process. If serratus anterior and the lower fibres of trapezius are ineffective, the upper trapezius will dominate the movement. In this case, these fibres show increased tone and can be tight. As the abduction moves further into stage (II), the moment arm of lower trapezius is lengthened and this portion of the muscle becomes increasingly active in the movement.
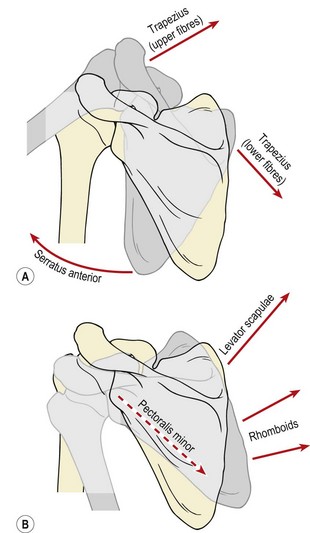
Figure 17.4 Muscle force couples which create scapular rotation. (A) Lateral rotation. (B) Medial rotation.
From Palastanga, Field and Soames (1989), with permission.
Downward (medial) rotation frequently occurs as a result of eccentric action of the above muscles. However, in activities such as hanging and chinning a beam, active scapular rotation is accomplished by levator scapulae and the rhomboids pulling upwards on the medial side of the scapula together with pectoralis minor pulling the coracoid process down. In cases where these muscles are tight or overactive, upward rotation of the scapula will be limited during abduction.
As scapular rotation progresses, lateral rotation of the humerus should be apparent as the cubital fossa and thumb orientate towards the ceiling. Ineffective scapular upward rotators, especially lengthening of the lower fibres of trapezius, will prevent correct orientation of the glenoid and increase the risk of impingement. Tightness in the medial rotators, especially the pectoralis major and subscapularis, combined with lengthening and weakness of the lateral rotators, may lead to delayed lateral rotation at the glenohumeral joint, resulting in impingement of the greater tuberosity against the inferior acromion.
During stage (II), as the humerus reaches 90° abduction, its head slides beneath the acromion, and a noticeable dip is formed in the skin. Failure of the shoulder musculature to pull the humerus into this position may result in the head slipping beneath the acromion with a sudden thud as the arm raises above 90° and similarly in this position during descent.
Stage (III)
During stage (III), as the arm approaches 120° abduction, no further movement is available from the glenohumeral joint. Additional range to reach the arm overhead is achieved by sliding the scapula over the thorax into further upward rotation and abduction. To facilitate this movement, the thoracic spine must reverse its kyphosis and flatten. A kyphotic posture and inflexibility in the thoracic spine will therefore limit the final degrees of abduction. As a simple test for this, the patient is asked to stand with the back flat against a wall and the pelvis posteriorly tilted to avoid any possibility of hyperextension at the lumbar spine. Both arms are then abducted, keeping them in full contact with the wall. If thoracic extension is limited, the patient will be unable to perform pure abduction to full range. Instead, the arm moves through flexion–abduction to bring it in front of the forehead. In conditions where abduction is limited, therefore, greater range may often be gained by mobilizing the thoracic spine as well as working on the glenohumeral joint.
As the arm moves into its final overhead position and the scapula rotates maximally, the inferior angle of the scapula juts out through the outer edge of the thorax. However, no more than 1–2 cm of the inferior angle should be visible at this point. During this final phase the IAR moves to the AC joint. Clavicular elevation is limited by tension in the costoclavicular ligament. As the coracoid process moves away from the clavicle, tension in this ligament causes dorsal rotation of the clavicle about its long axis.
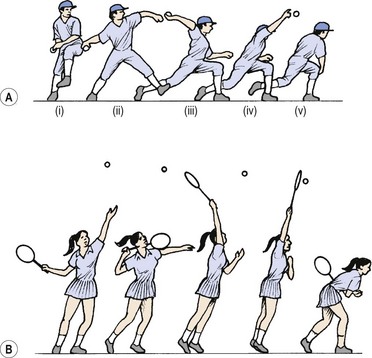
Figure 17.5 (A) Stages of throwing. (i) wind-up—athlete positions him- or herself for the throw; (ii) cocking—lead leg moves forwards, arm moves backwards, stretching body; (iii) acceleration—body drives forwards, leaving arm behind; (iv) deceleration—object released. Elbow continues to extend and shoulder to internally rotate; (v) follow through—trunk and lead leg show eccentric activity to dissipate energy. (B) Similarity to tennis serve.
After Fleisig, Dillman and Andrews (1994), with permission.
The biomechanics of throwing
In sport, throwing is to the upper limb what gait is to the lower limb. It is an activity seen in many sports in some form, and there are similarities between all types of throw and with shots in racquet sports. Throwing can be divided into five stages which form a single continuous motion. In the early stages, up to ball release, the body is accelerating the object. By the later stages, following release, the aim is to decelerate and reduce the effect of stress on the body. The phases are as follows:
Screening examination of the shoulder complex
After a subjective history has been taken, a screening examination is performed to enable the examiner to focus more closely on the injured area. The patient’s posture and actions are noted while undressing, and the area is inspected for swelling, colour and deformity. A combination of active, resisted and passive movements are used to assess the shoulder complex (Cyriax, 1982). The patient is viewed from behind to note any alteration in scapulohumeral rhythm. It is helpful to have the patient facing a full length mirror, so the anterior aspect of the shoulder and the patient’s facial expression may also be assessed. Active abduction and flexion–abduction are performed with overpressure applied at end-range, to assess end-feel. Positional changes of the scapula, either at rest or during movement, warrant closer inspection. Active glenohumeral rotation may be performed by asking the patient to place a hand behind the back (medial rotation) and then behind the head (lateral rotation). Passive lateral rotation is performed with the elbow flexed and upper arm held into the side. This is also the position for resisted lateral and medial rotations. Passive medial rotation is performed with the patient placing a hand into the small of the back. The examiner stabilizes the upper arm, and keeps the patient’s elbow tucked into the side of the body. The examiner then gently pulls the patient’s forearm away from the body, increasing medial rotation. Any limitation of movement is noted, and the percentages of limitation relative to each other reveal if a capsular pattern exists. The capsular pattern for the glenohumeral joint is gross limitation of abduction with some limitation of lateral rotation and little limitation of medial rotation.
Keypoint
The capsular pattern for the glenohumeral (shoulder) joint is gross limitation of abduction with some limitation of lateral rotation and little limitation of medial rotation.
Resisted abduction and adduction are performed in mid-range, the examiner stabilizing the patient’s pelvis to prevent any lateral trunk flexion occurring at the same time as the shoulder moves. Elbow flexion, extension and forearm rotation may be assessed at the same time with the elbow flexed and the upper arm held close to the body. The patient’s forearm rests on the examiner’s when testing the triceps, and resistance is given from above when testing the biceps. Resisted shoulder shrugging tests the trapezius. When a small physiotherapist is examining a large athlete, it is particularly important that resistance is applied from a position which gives maximum mechanical advantage to the therapist.
Referred pain from the neck must always be considered in cases of shoulder pain, and the neck screening examination is performed to establish whether movement is painful or reproduces the patient’s shoulder symptoms. This simple but methodical examination should take no more than 2–3 minutes and tells the examiner whether the shoulder is the cause of pain, if a contractile or non-contractile structure is affected, and reveals if a capsular pattern exists to suggest an intracapsular lesion.
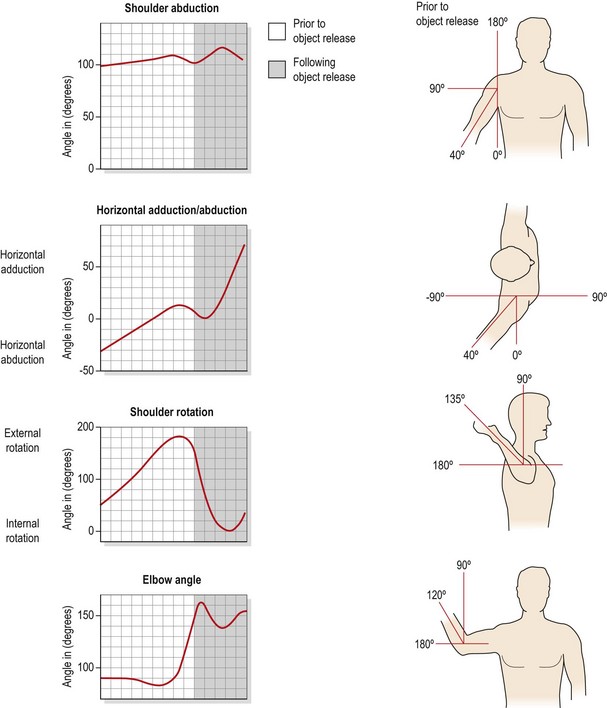
Figure 17.6 Angular displacement of the shoulder during a throwing action.
After Fleisig, Dillman and Andrews (1994), with permission.
Locking test and quadrant test
Should movement apparently be full and painless at the glenohumeral joint, two further procedures are useful to reproduce the patient’s symptoms. These are the locking test and the quadrant position (Maitland, 1991). Both tests refer to the position of the greater tuberosity relevant to acromial arch and glenoid (Corrigan and Maitland, 1994). Each should be assessed for pain and end-feel, and compared with the uninjured side.
Locking test
The locking position combines internal rotation, extension and abduction of the shoulder with the scapula fixed. In this position the subacromial space is compressed and will give pain should an impingement syndrome be present. Cadaveric studies have shown that in the locking position the posterosuperior tip of the glenoid is in contact with the humeral head (Mullen, Slade and Briggs, 1989).
Keypoint
The locking position compresses the subacromial space and gives pain with an impingement syndrome.
To perform the test, the patient is in a supine position, and the practitioner stands by the patient’s side towards the shoulders. The therapist places the palmar aspect of his or her forearm beneath the patient’s shoulder, and grips the trapezius muscle to stop the shoulder shrugging. The therapist holds the patient’s elbow, slightly medially rotates the arm, and lifts it into abduction.
Quadrant test
The quadrant position stresses the anterior and inferior capsule, and combines external rotation, slight flexion and full abduction of the shoulder. The therapist’s forearm grips the patient’s shoulder to prevent shrugging. The action is to hold the elbow and move the patient’s arm into abduction, allowing the humerus to move from medial rotation (palm to chest) to lateral rotation (palm to ceiling). The point at which the humerus begins to change from medial to lateral rotation marks the beginning of the quadrant (Petty and Moore, 2001). From this point horizontal extension is examined by pressing the elbow to the floor, releasing it and then moving into further abduction before pressing again. Both the quality and the range of motion are assessed, as well as the occurrence of muscle spasm. The affected shoulder is compared to the unaffected side.
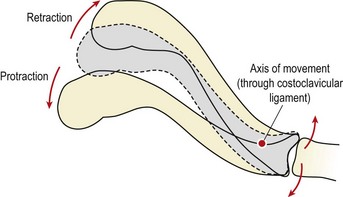
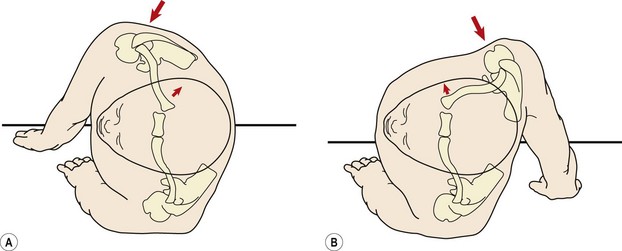
Figure 17.9 Sternoclavicular dislocation. (A) Anteriorly directed force causes posterior dislocation. (B) Posteriorly directed force causes anterior dislocation.
From Garrick and Webb (1990), with permission.
Sternoclavicular joint
The sternoclavicular (SC) joint provides, via the clavicle, the only structural attachment of the scapula to the rest of the body (Norkin and Levangie, 1992). The joint performs functionally as a ball and socket. The medial end of the clavicle articulates with the clavicular notch of the sternum, and the adjacent edge of the first costal cartilage. The congruity of the joint is enhanced by the presence of an interarticular fibrocartilage disc, which separates the joint cavity into two. In addition to improving the congruity of the joint, the disc also provides cushioning between the two bone ends. Furthermore, it holds the medial end of the clavicle against the sternum, preventing it moving upwards and medially when pushing actions are performed.
The joint is strengthened by a capsule attached to the articular margins and four ligaments (anterior SC, posterior SC, interclavicular and costoclavicular). Three degrees of movement are possible at the joint, elevation–depression, protraction–retraction and axial rotation. The axis of rotation for the first two movements (not rotation) is lateral to the joint itself, passing through the costoclavicular ligament. Consequently, when the lateral end of the clavicle moves in one direction, its medial end moves in the opposite direction, an important consideration with clavicular joint dislocation.
A total of about 60° of elevation and depression is available, elevation being limited by tension in the costoclavicular ligament, and depression by the interclavicular ligament and articular disc. When the lateral end of the clavicle is protracted, the medial end moves backwards, the opposite movement occurring with retraction. The total range of motion here is about 35°. This fact may be used in the emergency situation where posterior SC dislocation is causing asphysia (blocked oxygen intake). A folded towel is placed on the ground between the athlete’s shoulders to act as a fulcrum and the arm on the injured side is pushed firmly backwards to draw the medial aspect of the clavicle forwards and away from the trachea.
Keypoint
When the lateral (outer) end of the clavicle moves forwards in a protraction movement, the medial (inner) end moves back. In retraction the movement is reversed.
Axial rotation is purely a passive action accompanying scapular movements. The range of rotation is small (20–40°), but increases slightly as the lateral end of the clavicle is pulled back.
Injury
Injury to the SC joint is unusual, forming about 3% of all shoulder girdle trauma. Anterior dislocations occur more commonly than posterior dislocations in a ratio of 20 : 1 (Zachazewski, Magee and Quillen, 1996). Normally, the clavicle will fracture or the acromioclavicular joint will give way before the SC joint is seriously injured. However, when damage does occur, it is frequently the result of direct lateral compression of the shoulder, such as occurs when falling onto the side of the body. The injury is more common in horse-riding and cycling where sufficient force is produced, but is seen in rugby and wrestling.
The SC joint will dislocate in the opposite direction to the applied force, thus an anterior force (falling onto the back) will dislocate the joint backwards. Several important structures lie in close proximity to the joint including the oesophagus, trachea, lungs, pleurae, brachial plexus and major arteries and veins. Posterior dislocation therefore, if it is severe, may be potentially life-threatening. In contrast, anterior dislocation can occur in the absence of trauma, and frequently results only in slight discomfort.
Keypoint
The SC joint can dislocate in a fall onto the side of the body. The joint will move in the opposite direction to the applied force, an anteriorly directed force causing the joint to move backwards. If severe, this may be potentially life-threatening as the trachea may be damaged.
Initial examination (of posterior dislocation) on the field must obviously be aimed at ruling out life-threatening injury. The presence of stridor, dyspnoea, cyanosis, difficulty with speech, pulsating vessels and neurological signs may all necessitate immediate hospitalization.
If these are not present, joint examination may continue. Pain is generally well localized, and may become progressively more limiting over time. Anterior dislocation leaves a visible step deformity, and with posterior dislocation the usual prominence over the medial clavicle is lost. Local swelling is sometimes present, with crepitus and pain to motion, especially horizontal flexion. The shoulder is frequently held protracted.
Radiographic investigation will rule out clavicular fracture, and may enable differentiation between fracture and epiphyseal injury in the young (below 25 years) athlete. Closed reduction is often possible immediately after injury if pain is not too severe and before muscle spasm sets in. Both anterior and posterior dislocations may be reduced by placing a knee between the scapulae of the seated athlete and gently pulling the shoulders back. The joint often reduces with an audible thud. After reduction the joint is immobilized with a figure-of-eight bandage and ice is used to reduce local swelling.
Posterior dislocations, even if successfully reduced, will still require hospital referral and observation. Posterior dislocations usually stay reduced, but anterior dislocations are apt to recur. Surgical fixation of anterior dislocation is possible, but the number of complications makes the procedure undesirable. Migration of a Steinmann pin or Kirchner wire into the heart or major vessels has been reported (Garrick and Webb, 1990). Rockwood and Odor (1989) reported excellent results following conservative management of atraumatic anterior displacement 8 years after initial treatment. Patients treated surgically (not by these authors) in the same study had complications including scarring, instability, pain and limitation of activity.
Even though the joint is frequently hypermobile, joint mobilizations may be used to relieve pain (Maitland, 1991). Anteroposterior gliding may be performed with the therapist placing his or her thumbs over the sternal end of the clavicle.
Acromioclavicular joint
This joint is formed between the oval facet on the lateral end of the clavicle and the similarly shaped area on the acromion process. The lateral end of the clavicle overrides the acromion, slightly. The joint capsule is fairly loose and strengthened above by fibres from trapezius, and by capsular thickenings which make up the superior and inferior acromioclavicular (AC) ligaments. As with the SC joint there is an intra-articular disc, but this time it does not divide the cavity into two. The joint is further stabilized by the coracoclavicular ligament, divided into its conoid and trapezoid parts. The conoid ligament is fan-shaped and resists forward movement of the scapula, while the stronger trapezoid ligament is flat and restricts backward movements. As with the SC joints, the AC joint moves only in association with the scapula. Three types of movement are again present, protraction–retraction, elevation-depression and axial rotation.
Examination
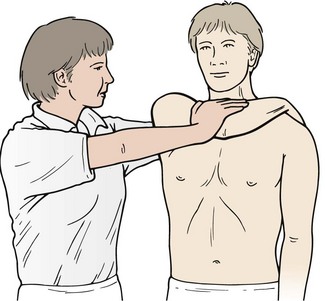
The AC joint is examined using the ‘cross body’ or ‘scarf’ test. Here, the patient’s hand is taken across their chest (horizontal adduction) and placed on top of their other shoulder. Where the joint is especially painful this is carried out as a passive movement with the therapist supporting the weight of the patient’s arm. In cases of high irritability, minimal horizontal adduction is all that is required to provoke symptoms.
Keypoint
Where the AC joint is suspected to be the source of pain, horizontal adduction with overpressure (‘cross body’ or ‘scarf’ test) can be used as a confirmatory test.
The cross body test has been shown to gap the AC joint by an average of 6.4 mm measured using ultrasonography compared to a gap of 7.7 mm with passive end range external rotation. However, greater direct stress is placed on the AC joint using the cross body manoeuvre than with humeral rotation (Park, Park and Bae, 2009). The cross body test has been shown to have a sensitivity of 77% compared to 41% for the active compression test (Chronopoulos et al., 2004). This latter test was designed to assist the diagnosis of labral tears and to differentiate them from AC joint involvement depending on the patient’s description of their pain location as ‘on top’ or ‘inside’ the shoulder (Brian et al.: O’, 1998).
Injury
The most common conditions affecting the AC joint are sprains and degeneration. AC joint sprains vary in intensity between minor grade I injuries to grade III ruptures representing complete disruption of the coracoclavicular ligament and AC joint dislocation (sprung shoulder) (Fig. 17.11). The injury may be further classified using weight-lifting radiographs. Here, the anterior deltoid is contracted by having the patient hold a weight with the elbow flexed and arm next to the body. If the clavicular attachment of the deltoid is intact, the joint may reduce as weight is taken (IIIa), or there may be no change in the joint appearance (IIIb). However, if the lateral end of the clavicle becomes more prominent, the clavicular attachment of the deltoid may have been stripped off (Dias and Gregg, 1991). Radiographs are also used to differentiate the condition from fractures of the distal clavicle where this is suspected.
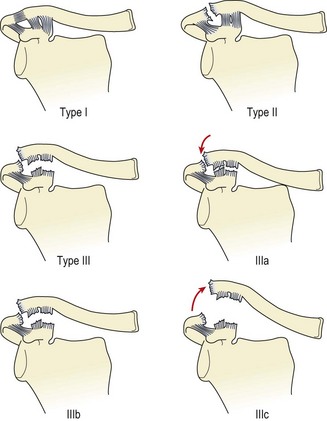
Figure 17.11 Acromioclavicular joint injuries. Type I (sprain), type II (subluxation), type II (dislocation), type IIIa (reduces as weight taken), type IIIb (no change as weight taken), type IIIc (lateral end of clavicle more prominent as weight taken).
Injury is usually the result of a superiorly directed force as occurs with a fall onto the point of the shoulder or being struck from above. The force drives the scapula downwards, an action resisted by the coracoclavicular ligament.
Keypoint
AC joint dislocation normally occurs with a downwardly directed force such as a fall, or blow, onto the point of the shoulder.
Examination reveals local tenderness over the AC joint, sometimes with a noticeable step deformity. The deformity may occur later, if initial muscle spasm reduces acromioclavicular separation.
Initial treatment aims to reduce the symptoms. Ice and a sling support to take the weight of the arm are recommended. The joint is immobilized in the sling for 2–3 weeks, and then gradually mobilized within pain-free limits. With grade I injuries, some relief may be provided by taping.
Acromioclavicular taping
Stress may be taken off the AC joint by a simple taping designed to press the clavicle down and take some of the weight of the arm away from the distal shoulder structures (Austin, Gwynn-Brett and Marshall, 1994; Macdonald, 1994). The athlete is positioned in sitting at the side of the couch with the elbow flexed to 90° and the shoulder abducted to 30°. The shoulder is slightly elevated and the arm rests on the couch. The shoulder and chest on the injured side of the body should be shaved of long hair. Spray adhesive is applied, making sure that the athlete turns the head away from the spray and covers the eyes with the unaffected hand. Also, the nipple area must be protected with a non-adhesive pad.
A felt pad is placed over the acromion to protect it from abrasion. Two anchors of 7.5 cm elastic adhesive tape are applied. The first runs horizontally from the sternum to the paravertebral area on the side of injury. The second is placed around the mid-humerus with light tension, ensuring that the limb is not excessively compressed (Fig. 17.12A). Two stirrups of 7.5 cm elastic adhesive tape are placed (pre-stretched) from the front to the back of the chest anchor, passing over the acromion (Fig. 17.12B). These are then reinforced by two strips of 5 cm zinc oxide taping. Two further strips of elastic adhesive tape are placed (pre-stretched) laterally from the arm anchor across the anterior aspect of the shoulder to join the chest stirrups over the acromion, and laterally from the anchor, passing posteriorly over the shoulder to the acromion (Fig. 17.12C). Again, these stirrups are reinforced by 5 cm zinc oxide taping. If the shoulder stirrups have been applied correctly, their tension will tend to lift the arm into abduction slightly. The chest and arm stirrups are closed by reapplying the chest and arm anchors (7.5 cm elastic adhesive tape) to act as fixing strips. Sensation and pulse should be re-tested after tape application.
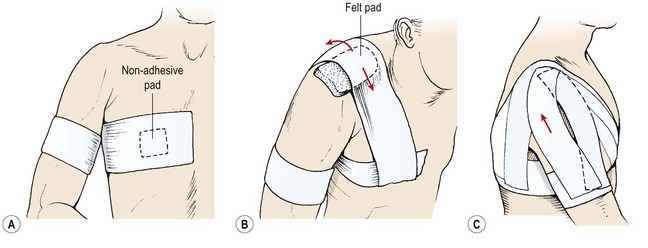
Figure 17.12 Acromioclavicular joint taping. (A) Anchors. (B) Stirrup applied under tension. (C) Arm stirrups.
In the acute phase of injury, the forearm weight may also be taken by a collar and cuff sling. With time, when pain-free arm motion to 90° is available, the humeral portion of the tape may be dispensed with.
Specific exercise therapy
As inflammation subsides, exercise therapy is commenced to restore function. This is used initially to maintain muscle tone in the absence of joint movement. Isometric contractions of the scapular and glenohumeral muscles are used, and the athlete maintains general fitness and lower body strength by exercising with the AC joint taped. When pain subsides and movement commences, gentle scapular actions are used, such as shoulder shrugging and bracing within the limits of pain. These may progress to a scapular stabilization programme. Range of motion exercises for the glenohumeral joint are begun, ensuring that correct scapulohumeral rhythm is maintained.
When full pain-free motion is obtained, the athlete may be seen to have a permanent step deformity, and some joint degeneration may occur in later years. The major problem resulting from this injury is lack of confidence when falling in contact sports. The effects of direct trauma may be limited by placing a felt doughnut pad over the joint. Confidence is built using progressive closed chain exercises and rehearsal of falling actions. These may begin with forward rolls onto the outstretched arm on a mat, initially from a kneeling position, progressing to standing and finally a diving forward roll over a bench. Pressure over the point of the shoulder begins with log rolling on the floor, and builds up to shoulder blows on to a rolled mat or punch bag.
Surgical intervention
There is some controversy concerning the treatment of this condition. Both conservative and surgical approaches restore function to a similar degree (Larsen, Bjerg-Nielsen and Christensen, 1986; Dias et al., 1987; Bannister et al., 1989), and some surgical methods have been shown to give long-term functional detriment. Certainly, removal of the distal end of the clavicle (Gurd, 1941) will disrupt the acromioclavicular ligament, a main stabilizer of the joint (Fukuda et al., 1986). In the literature, the main argument for surgery has been the development of degenerative changes in the joint as a result of non-operative management. However, degeneration does not occur in all patients, and when it does occur, it is not necessarily a limitation (Dias et al., 1987). In addition, surgery is often as effective if done in the acute or chronic condition, so there is normally no advantage to operating immediately. Importantly, surgery carries with it a high risk of complications (Ejeskar, 1974; Lancaster, Horowitz and Alonso, 1987; Taft, Wilson and Oglesby, 1987).
In a literature review of 11 papers detailing the long-term results of both surgical and conservative management of this injury, Dias and Gregg (1991) found poor results to have occurred in 13 out of 247 patients treated conservatively (5.3%), and 22 out of 233 managed surgically (9.4%). These authors argued that as comparable results were obtained regardless of the method used, conservative management was the treatment of choice for most AC injuries. Looking at strength testing following grade III AC injuries treated conservatively (average 4.5 year follow-up), Tibone, Sellers and Tonino (1992) found no subjective complaints in patients, all of whom were able to participate in sport. Full motion occurred in all subjects, and no significant differences were found in muscle strength of injured and non-injured sides in rotation, abduction/adduction or flexion/extension.
AC joint degeneration
Joint degeneration is common in later years following injury, regardless of the grade of damage which occurred, and particularly after repeated trauma. In addition, some sports, such as weight-lifting, have a higher incidence of degenerative changes in the AC joint, even where no incidents of trauma may have occurred. Cahill (1982) reported 46 cases of osteolysis of the distal clavicle, all but one occurring in weight-lifters. He argued that degeneration occurred as a result of subchondral stress fractures resulting from repeated microtrauma. The condition presents as pain, usually dull and aching in nature, brought on by activities such as lifting and throwing. On examination there is point tenderness over the joint, with pain and crepitus to passive horizontal adduction (cross body test).
Where the diagnosis is uncertain, radiographs will frequently reveal degeneration, and injection of local anaesthetic into the joint is helpful to establish if the degeneration is the cause of the patient’s symptoms.
Movements which stress the joint (for example, press-ups, weight training or throwing) should be avoided. Initially, immobilization in a sling may be required in the very acute lesion. Later, joint mobilization provides good results. Anteroposterior gliding may be performed with the patient in a sitting position. The therapist grasps the distal end of the clavicle with his or her thumb and forefingers of one hand, and the acromion process in a similar fashion with the other hand. The hands are worked against each other to glide the joint. Injection of corticosteroid may give many months of relief, a technique made easier if the shoulder is laterally rotated to distract the AC joint.
Fractures of the clavicle
The most common mechanism of injury is a fall onto the outstretched arm, and occasionally direct trauma to the shoulder. Although common, these injuries should not be taken too lightly, as it must be remembered that the subclavian vessels and the medial cord of the brachial plexus lie in close proximity, as does the upper lobe of the lung (Fig. 17.13). Neurovascular and pulmonary examination may therefore be required.
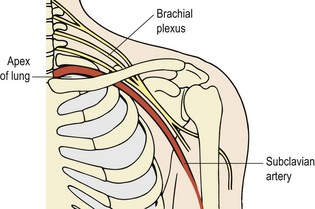
There is usually a cracking sensation at the time of injury, with immediate pain over the fracture sight and rapid swelling. Signs of injury to vital structures are rare, but include dyspnoea and paraesthesia and obviously warrant immediate hospitalization. Laceration of the subclavian artery presents as a readily expanding pulsating haematoma. Deformity following clavicular fracture is common, as is crepitus.
Keypoint
Following suspected clavicular fracture signs of altered sensation (paraesthesia) or breathlessness (dyspnoea) warrant immediate hospital referral.
Fractures of the proximal and middle thirds of the clavicle make up the largest proportion (80%) of such injuries. If not displaced these should be immobilized with the shoulders retracted in a figure-of-eight bandage for 6 weeks. With young athletes the risk of non-union may make it necessary to curtail activity for up to 3 months after injury. Figure-of-eight bandages must not be applied so tightly as to constrict the blood or nerve supply to the arm. When little displacement is present, support in a sling may be all that is required. Some step deformity usually occurs as complete immobilization of athletes (other than in a cast) is difficult. This type of deformity is usually cosmetic rather than functional.
Distal fractures tend to be displaced by retraction immobilization, and are better wired. Internal fixation of the proximal clavicle carries with it similar complications to that of the sternoclavicular (SC) joint. Fractures to the extreme proximal end of the clavicle may be misdiagnosed as SC dislocations, and in the younger individual epiphyseal injury should be considered in this region. It should be noted that the sternoclavicular epiphysis may remain open until the age of 25 (Zachazewski, Magee and Quillen, 1996), so radiological examination must be accurate.
Winged scapula
During normal scapulohumeral rhythm, the scapula slides over the ribcage, and is held in place by the serratus anterior. If weakness or paralysis of the serratus anterior occurs, the scapula will stand prominent from the ribcage when the arm is protracted against resistance. In addition to muscular weakness, there are a number of other causes including damage to the long thoracic nerve, brachial plexus injury, conditions affecting the fifth, sixth and seventh cervical nerve roots, and certain types of muscular dystrophy (Apley and Solomon, 1989).
Where weakness is due to nerve palsy, spontaneous recovery is to be expected. Re-education of scapulohumeral movement is required as habitual alteration of scapulohumeral rhythm is often seen. Strengthening the shoulder musculature in general, and especially serratus anterior, is also useful.
Occasionally, a congenitally undescended scapula (Sprengel’s shoulder) is seen, sometimes associated with marked thoracic kyphosis. Normally, the scapulae descend completely by the third month of fetal life. However, if undescended, the scapula appears slightly smaller, higher, and more prominent. Scapulohumeral rhythm is affected and abduction is limited as a consequence. Minor cases respond to rehabilitation although marked deformity may require surgery.
Apparent winging may occur when the scapulae abduct through lengthening of the scapular retractors and tightening of the protractors. As the scapulae move away from the mid-line, they roll around the ribcage, lifting their medial border. This is not true winging, however, because the condition is present at rest and during muscle contraction. Treatment note 17.1 shows exercise therapy and manual therapy techniques used in the restoration of scapulothoracic stability.
Treatment note 17.1 Restoraton of scapulothoracic stability
Scapular stability is enhanced by restoring the functional capacity of the lower trapezius and serratus anterior, which, as stability muscles, often show reduced activity and lengthening. Surface electromyography (sEMG) may be used with the active electrode placed over the lower trapezius or serratus anterior. The patient is placed in prone lying and the scapula is passively positioned into its neutral position by the therapist. This often requires retraction and depression to neutralize the protraction/elevation often found (Fig. 17.14). The patient is encouraged to hold this position through his or her own muscle activity, gaining feedback from the sEMG readout. Enough muscle activity should be used to keep the anterior aspect of the shoulder off the treatment couch, but not to retract the scapulae. Once this position can be maintained actively, the holding time is built up until the patient can perform 10 repetitions, holding each for 10 seconds.
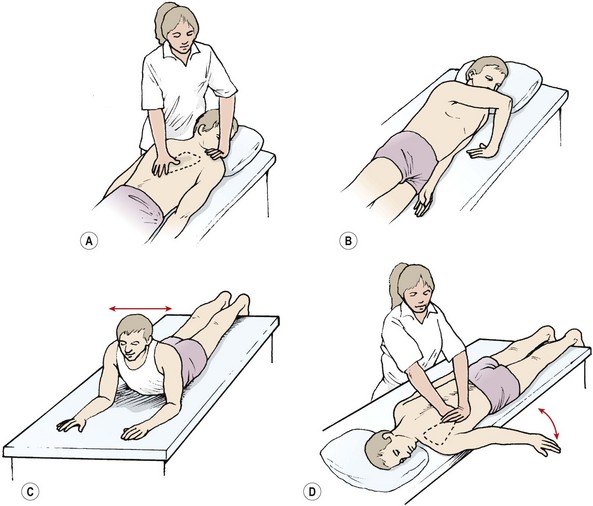
Figure 17.14 Enhancing scapulothoracic stability. (A) Scapular repositioning. (B) Rhythmic stabilization. (C) Trunk rocking. (D) Arm movement progressions.
Keypoint
The main scapular stabilizers are serratus anterior and the lower trapezius. These muscles are worked using low load scapular depression and retraction. The inner range scapular position is held to build postural endurance.
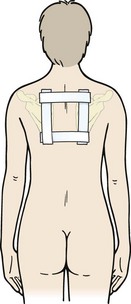
Taping may be used to give feedback about the position of the scapula and lengthened muscle. A positional box tape may be used to facilitate position of the scapula (Fig. 17.15). The tape has two horizontal strips to draw the medial borders of the scapulae together and two vertical strips to facilitate thoracic extension. Non-elastic taping is used to take up skin tension and act as a feedback system for the patient. Facilitatory taping may be used over the serratus anterior (Fig. 17.16A), lower trapezius (Fig. 17.16B) or to increase patient awareness of body segment position and facilitate underlying muscle action.
The scapular force couples may be maximally challenged using a side lying, braced position (Wilk and Arrigo, 1993). The patient begins in side lying with the arm flexed/ abducted to 90° and internally rotated. The hand is now flat on the couch with the fingers pointing towards the patient. Scapular fixation is maintained against the rhythmic stabilization provided by the therapist in all planes.
The next stage is to introduce a limited range of movements of the humerus onto the now stable base of the scapular thoracic joint. Initially, the patient assumes elbow support prone lying to work the shoulder in closed kinetic chain format. He or she moves the body over the arm forward and backwards and side to side to create closed chain flexion/ extension and abduction/adduction. At all times the scapula must remain in contact with the thorax. The patient is now moved to the edge of the couch so the affected arm hangs over the couch side. Maintaining scapula thoracic stability, inner-range movements in all three planes are used in an attempt to automatize stability.
The starting position is now changed to sitting or standing and inner-range movements are used with sEMG monitoring of the lower trapezius. Home exercises may be used by asking the patient to place the thumb of the opposite hand beneath the inferior scapular angle. The patient then gently keeps the inferior ankle pressed against the thumb (retraction and depression) while performing inner-range movements.
These initial actions, where stabilization ability is being re-educated, must keep the arm below 30° abduction to prevent scapular movement. Later, greater glenohumeral range may be used as the patient can control scapulothoracic movement.
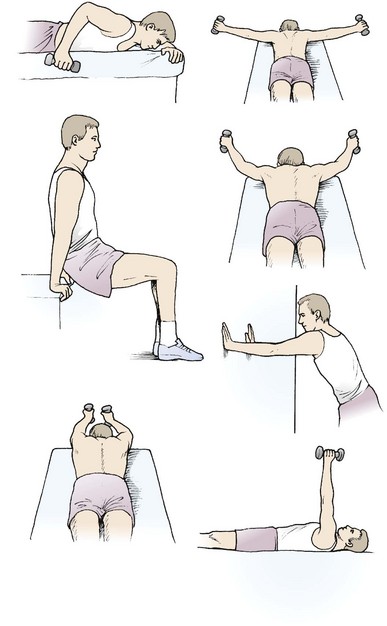
The scapulothoracic muscles may be selectively strengthened using the individual exercises shown in Figure 17.17.
Impingement syndrome
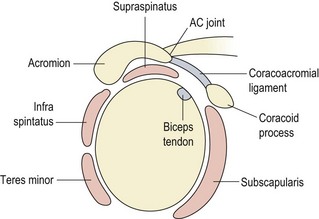
The subacromial space (Fig. 17.18) lies beneath the coracoacromial arch formed by the coracoacromial ligament together with the coracoid and acromion the so-called ‘roof of the joint’. The coracoacromial arch is covered by the deltoid, and inferiorly its fascia is continuous with that of the supraspinatus. The arch prevents upward dislocation of the glenohumeral joint. The supraspinatus passes beneath the arch, being separated from it by the subacromial bursa. The subacromial distance (space between the inferior acromion and the head of the humerus) is normally about 1cm (Petersson and Redlund-Johnell, 1984). If the supraspinatus tendon has ruptured, or the muscle is no longer active, this space will reduce by as much as 50% due to the unopposed pull of the deltoid.
Keypoint
The subacromial space may reduce by as much as 50% if the supraspinatus muscle is dysfunctional.
During elevation and internal rotation, the greater tuberosity, with the supraspinatus riding on top, may press against the anterior edge of the underside of the acromion (or a spur from a degenerating AC joint) causing impingement pain. During flexion, impingement may also involve the long head of biceps (Peat and Culham, 1994). At the point where the greater tuberosity comes close to the acromion (70–120° abduction), a number of structures may be pinched between the involved bones or the tuberosity and the coracoclavicular ligament. Normally, the structures affected are the suprasinatus tendon, the long head of biceps and the subacromial bursa.
Movement dysfunction
The action of abduction involves a complex series of movements. Impingement is associated with a change in the muscle action involved in the abduction sequence. Most commonly there is a reduction in the stabilizing action of the serratus anterior muscle with other muscles (especially the upper trapezius) compensating. The result is an altered scapular position relative to the humerus during abduction. This movement dysfunction has been termed scapula dyskinesia (Paterson, 2008). EMG studies of patients with impingement pain have shown a reduction in serratus anterior muscle action and a change in scapula position (Ludewig and Cook, 2000). The scapula is more anteriorly tipped drawing it closer to the approaching humeral head, and upward rotation during the early stages of abduction is delayed. Decreased force output in the both the serratus anterior and lower trapezius has also been shown with overhead athletes demonstrating shoulder impingement (Cools et al., 2004).
Examination
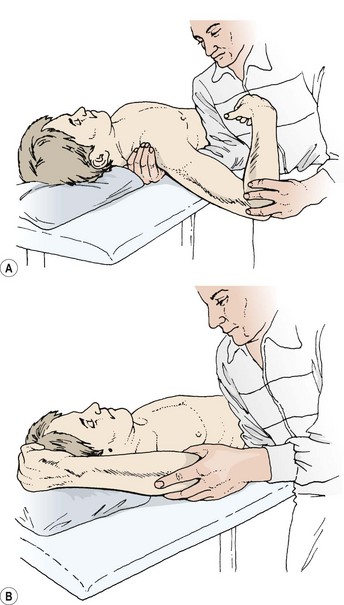
The screening examination is used initially, followed by observation of both static and dynamic position of the scapula and humerus. Two further tests are useful which are specific to impingement. In test one (Fig. 17.19A) the arm is fully abducted and overpressure is put onto the internally rotated (thumb forwards) shoulder. For test two (Fig. 17.19B), the glenohumeral joint is flexed and internally rotated (Hawkins test). Overpressure is then added to internal rotation and abduction or horizontal flexion. Resisting flexion by placing pressure over the elbow may also bring on the athlete’s pain (Hawkins and Hobeika, 1983; Reid, 1992).

Figure 17.19 Impingement tests. (A) Full abduction with overpressure to the internally rotated shoulder. (B) Hawkin’s sign. Flexion and internal rotation. Overpressure to internal rotation and abduction or horizontal flexion.
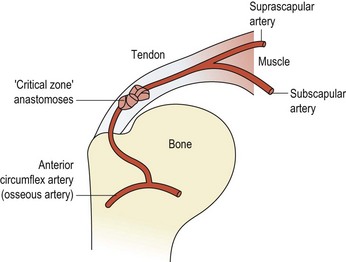
In addition to a purely mechanical impingement, changes in the microvascular supply to the area have been noted. Pressure exerted by the humeral head on the supraspinatus tendon, has the effect of ‘wringing out’ the tendon vessels and creating an avascular zone (Rathbun and Macnab, 1970). This area, known as the critical zone (Fig. 17.20), is an anastomosis between the osseous vessels and the tendinous vessels (Moseley and Goldie, 1963). Furthermore, repeated microtrauma results in local oedema within the tendon and an increase in tissue volume. This in turn makes the structures more susceptible to impingement by reducing the subacromial space and so perpetuates the problem.
A reduction in the subacromial space may be the result of individual variation in the anatomical architecture of this region, with some individuals more prone to impingement than others (Ticker and Bigliani, 1994). Cadaveric studies of 140 specimens have identified three types of acromion associated with full thickness tears of the rotator cuff (Bigliani, Morrison and April, 1986).
The flat (type I) acromion occurred in 17% of subjects, the curved (type II) acromion was seen in 43%, and the hooked (type III) type in 39% (Fig. 17.21). The hooked acromion was present in 70% of rotator cuff tears whereas the flat type was only seen in 3%. By assessing the supraspinatus outlet view x-ray, Morrison and Bigliani (1987) showed 80% of those with positive arthrograms to have a hooked acromion. The same authors showed that 66% of patients who underwent open subacromial decompression had a hooked acromion.
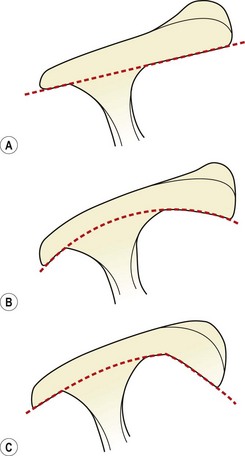
Figure 17.21 Acromion types. (A) Type I, flat. (B) Type II, curved. (C) Type III, hooked.
After Ticker and Bigliani (1994).
Impingement is not simply the result of a lack of subacromial space, however. Weakness in the rotator cuff (or pain inhibition) can cause instability (see below) and allow the humeral head to ride up through deltoid contraction, making examination of rotator cuff strength and order of muscle contraction vital with this condition. The interaction between biomechanics, physiology and pathology creates a painful progressive condition which ultimately may cause mechanical failure, as detailed in Fig. 17.22.
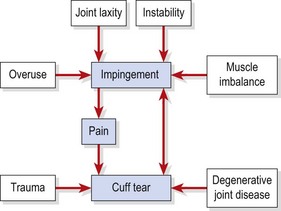
Figure 17.22 Interrelation between pain, impingement and cuff tear.
After Reid (1992) with permission.
Stages of impingement
Three stages of impingement have been described (Neer, 1972).
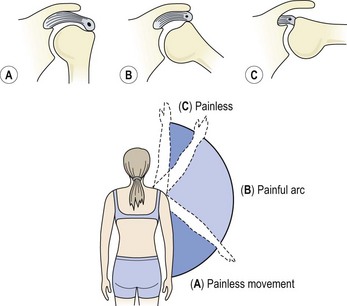
Figure 17.23 The painful arc. (A) No impingement, painless. (B) Tuberosity pinches painful structure. (C) Tuberosity moves beneath acromion, pain disappears.
Keypoint
Stage I lesions are inflammatory, stage II see the development of fibrosis and adhesion. In stage III lesions chronic bony changes, including sclerosis and osteophyte formation, may be present.
Internal rotation of the shoulder is one biomechanical factor which predisposes to impingement (Halbach and Tank, 1990), and should be limited in patients with this condition. While external rotation helps the greater tuberosity clear the acromion, internal rotation has the reverse effect, compressing the two structures. Exercise therapy aims to redevelop scapular stability and to restore the normal internal/external rotation, ratio of the glenohumeral joint to 3 : 2 (Baechle, 1994). As the supraspinatus is affected, external rotation range and strength is normally greatly reduced in these athletes. External rotation exercises, beginning with the arm held to the side and eventually in 90° abduction, are therefore used. Combinations of abduction, extension and external rotation may be performed on a pulley or with elastic tubing, within the pain-free range.
The structures affected by impingement may also be injured in isolation. So, either the supraspinatus or biceps tendons may be subjected to tendinopathy, and the subacromial bursa inflamed without muscular involvement.
Tendon injuries
Pathological changes within tendon
Pathological changes within the Achilles tendon (Chapter 10) and patella tendon (Chapter 9) have been described previously, and changes within the rotator cuff tendons are similar. Tendinopathy, previously considered an inflammatory response (Cyriax, 1982), is now described as degenerative. A new model of tendon pathology (Cook and Purdam, 2009) considers the tendon changes as a continuum of three stages: reactive tendinopathy, tendon dysrepair, and degenerative tendinopathy. During stage I (reactive tendinopathy) there is a non-inflammatory proliferative response as a result of tissue overload. The tendon responds to a sudden load change by increasing its cross-sectional area (thickening) to effectively spread the new load over a greater area. These changes show as a fusiform swelling on MRI or ultrasound scanning. The adaptation occurs due to acute overload and differs from the normal adaptation of tendon to a gradual load increase which is to increase its stiffness (Magnusson et al., 2008). Tendon cells (mainly proteoglycans) change their shape and develop greater numbers of cytoplastic organelles associated with increased protein production. The amount of bound water within the collagen matrix increases, and this change can occur within hours of the load change (Cook and Purdam, 2009).
Keypoint
Reactive tendinopathy is a non-inflammatory response to sudden load increase. The tendon thickens, its protein content rises and the amount of bound water within the tendon is increased.
Stage II (tendon dysrepair) shows a steady increase in the number of chondrocyte cells and greater matrix breakdown. Collagen fibres become separated and disorganized and increased vascularity and neural ingrowth is often evident on colour Doppler ultrasound. Clinically the thickening is well localized to a single tendon area, and changes are still reversible with activity change and exercise therapy.
Degenerative tendinopathy (stage III) occurs in the chronically overloaded tendon. The athlete will have felt a number of recurrences of tendon pain which often partially resolve, only to come back as training is again increased. There is increased tendon size focally, with areas of cell death due to tenocyte exhaustion. The tendon matrix is broken down with areas of acellularity, disorientation and vascular ingrowth. Unfortunately, little reversibility is possible now and tendon rupture may occur with sudden high loading.
Rotator cuff
Tendinopathy of the rotator cuff muscles is common both as a result of overuse and through trauma. Common examples of overuse include excessive repetitions on a single weight-training exercise, while trauma may result from an ill-timed ‘wrenching’ action which combines rotation with abduction. The pathogenesis of tendinopathy has been described as intrinsic and extrinsic (Lewis, 2009). Intrinsic causes originate within the tendon as a result of overload and show tissue cell changes and neovascularization.
Definition
Neovascularization is the pathological formation of a network of new blood vessels within tissue which does not normally contain them. It typically occurs as a result of trauma or disease, and contrasts to angiogenesis which is the normal growth of new vessels by budding from pre-existing vessels.
Supraspinatus
The most commonly affected tendon in the shoulder is that of the supraspinatus. Pain is elicited with resisted external rotation and initiation of abduction. More specifically, pain occurs with the arms abducted to 90°, brought forwards into 30° flexion and internally rotated so that the thumbs point towards the floor (Reid, 1992).
The supraspinatus tendon is made up of six to nine independent fascicles (Fallon et al., 2002) containing proteoglycan lubricant, which facilitates independent sliding of each fascicle. During shoulder abduction the inner (joint side) part of the tendon is subjected to traction while the outer parts are compressed. The attachment of the tendon to bone is fibrocartilage, a tissue less capable of withstanding tension loading. The inner articular fibres have a smaller cross-sectional area compared to those on the superior (bursal) aspect. Stressing the two sets of fibres experimentally has shown the articular fibres to rupture with half the force of the bursal side fibres (Nakajima, Rokuuma and Hamada, 1994). Intrinsic pathology of the rotator cuff tendons leads to decreased function and a lessened ability to control the humeral head position. This reduction in function may allow the humeral head to translate superiorly increasing stress onto the acromion, coracohumeral ligament and bursa. Impingement changes in these tissues are therefore secondary to change within the tendon itself (Lewis, 2009), a reversal of generally accepted opinion.
Keypoint
Impingement of the supraspinatus into the subacromial arch normally occurs secondary to tendon pathology.
Extrinsic causes of rotator cuff tendinopathy have typically been seen as impingement beneath the acromion. However, Gill et al. (2002) investigated 523 patients who had had surgery for rotator cuff pathology and found no significant association between acromial morphology and rotator cuff pathology in patients over 50 years old. In addition results from conservative treatment of subacromial impingement (90 cases) have been found to equal those of surgical decompression at follow-up of 4−8 years (Andersen: Haahr &, 2006) implying that improvement seen post surgery may be the result of relative rest (Lewis, 2009).
Palpation to the muscle insertion is performed with the injured arm medially rotated (hand behind the back) to bring the greater tuberosity forwards and make the tendon more superficial (Fig. 17.24A). This is also the most convenient position for transverse frictions, the area of scarring being found by palpating about one finger’s width below the anterior tip of the acromion. The musculotendinous junction is more conveniently palpated with the injured arm abducted to 90° and supported (Cyriax and Cyriax, 1983). The palpating finger is directed at the space between the posterior aspect of the lateral clavicle and the scapular spine. Again, this is the most convenient starting position for transverse frictional massage (Fig. 17.24B).
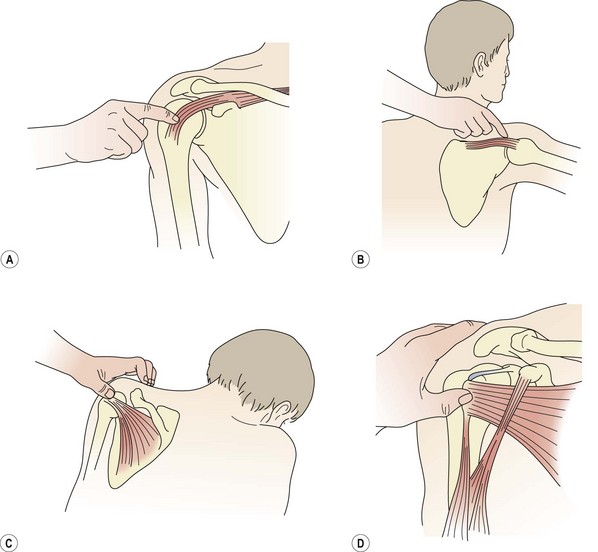
Figure 17.24 Palpation and treatment of rotator cuff tendon injury. (A) Supraspinatus: tendon. (B) Supraspinatus: musculotendinous junction. (C) Infraspinatus. (D) Subscapularis.
After Cyriax and Cyriax (1983), with permission.
Calcification of the supraspinatus (or rarely the other rotator cuff tendons) may develop following chronic tendinopathy within the critical zone (Moseley and Goldie, 1963), an area claimed to be susceptible to injury due to reduced vascularity (Rothman and Parkes, 1965). This area, near the attachment of the supraspinatus (see Fig. 17.20), tends to be wrung out when the arm is held in its resting position of adduction and neutral rotation. Compression of the tendon vessels and microtrauma leads to repetitive hypoxia, and is especially common in activities which involve repeated internal rotation at 90° shoulder abduction. Fibrocytes within the tendon are transformed to chondrocytes, and collagen disintegration, coupled with the accumulation of mucopolysaccharides, begins. Hydroxyapatite mineral deposit deposition is then initiated (Lemak, 1994).
During the acute and subacute phase the deposit is of toothpaste-like consistency (and will escape into the subacromial bursa if punctured during an injection procedure). Conservative management is usually successful if the condition is caught early enough. Active rest and exercise are called for. The repetitive forces causing hypoxia must be removed by correcting impingement. Exercise therapy is then used to enhance the blood supply of the tendon, and healing is good. High repetitions are performed in the pain-free range (Torstensen, Meen and Stiris, 1994) avoiding both the resting position (adduction and neutral rotation) and internal rotation. All other sporting activities which cause pain are curtailed.
In the chronic phase the deposit is gritty and sand-like. This later stage is more painful and may require surgical intervention. Arthroscopy is normally performed to debride the calcific portion of the tendon and remove any necrotic tissue. The tendon should then heal well.
Remaining muscles
Pain on resisted lateral rotation but not abduction implicates the infraspinatus. Local pain may be found by palpation to the posterior aspect of the greater tuberosity with the patient’s shoulder flexed, slightly adducted and laterally rotated. The most convenient position for this is elbow support in a prone-lying position, with the patient leaning forwards and outward over the injured shoulder (Fig. 17.24C).
If resisted medial rotation alone gives pain, the subscapularis is most likely affected, at its insertion into the lesser tuberosity. This structure may be palpated and treated along the inner edge of the intertubercular sulcus. The patient is in a long sitting position, and the therapist grasps the hand on the affected side. A transverse frictional mobilization is carried out by medial and lateral rotation of the patient’s shoulder against the palpating finger of the therapist (Fig. 17.24D).
Pain in combination with resisted adduction implicates the muscles (pectoralis major, latissimus dorsi and teres major) attaching within the intertubercular sulcus. These muscles are usually tight and they show tendinopathy less commonly than muscle tearing.
Treatment note 17.2 Rotator cuff trigger points
Trigger points (TrPs) within the rotator cuff muscles can give pain in shoulder conditions such as impingement where there is a painful arc, and adhesive capsulitis where movement is severely limited. TrPs in these cases are often secondary to other pathologies, but may, in some instances, actually be the primary cause of pain (Simons, Travell and Simons, 1999; Gunn, 1996).
Supraspinatus
The supraspinatus may refer pain into the point of the shoulder and as far down the arm as the lateral epicondyle. TrPs may be found in the muscle bulk, which are usually very painful to palpation as the muscle is more superficial here (Fig. 17.25). As the muscle travels across the head of the humerus it is covered by the deltoid and so less painful to palpation, but at its insertion onto the superior aspect of the greater tuberosity again it may be tender. TrPs may be treated by ischaemic compression and dry needling. When needling over the scapula the possibility of incomplete ossification of the scapula surface must be considered and deep needling (greater than 1.0 cm) should be used with caution.

Infraspinatus
TrPs from the infraspinatus refer to the shoulder and arm in much the same way as the supraspinatus. Differentiation is through palpation and pain to abduction (supraspinatus). In addition, the larger origin of the infraspinatus can refer pain between the scapulae into the rhomboid region. TrPs may be in the belly of the muscle, normally located just below the medial third of the scapular spine, and occasionally right onto the medial border of the scapula (Fig. 17.26). To facilitate palpation ask the patient to place the arm across the chest to grasp the opposite shoulder and place the muscle on slight stretch.

Teres minor
The teres minor has the same action as infraspinatus but a different innervation (teres minor the axillary nerve, infraspinatus the suprascapular nerve). TrPs are often secondary to those of infraspinatus and lie within the muscle belly. They are located at the lateral edge of the scapula between the infraspinatus above and the teres major below.
Subscapularis
TrPs in this muscle have been described as ‘the key to frozen shoulder’ (Simons, Travell and Simons, 1999) and this claim certainly coincides with the pathological changes found within the rotator interval in adhesive capsulitis (see Fig. 17.34). Referred pain is to the posterior aspect of the shoulder and can extend down the posterior aspect of the arm. TrPs are mostly beneath the scapula and only accessible by placing the patient supine with the arm abducted to 45°. The therapist then places traction through the arm to draw the scapula laterally and locates the lateral edge of the scapula beneath the medial to the latissimus dorsi. A pincer grip is used between the thumb and forefinger (Fig. 17.27).

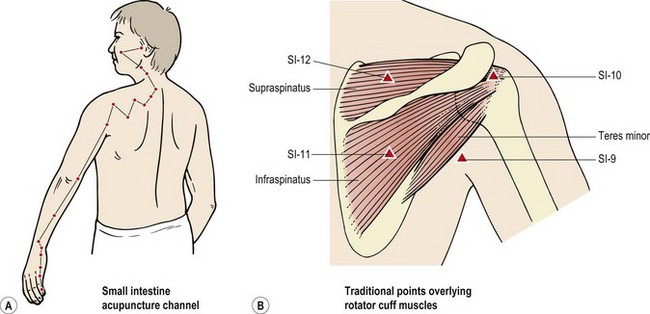
East meets West
Many traditional acupuncture points correspond to TrPs. SI-12 (Small Intestine 12) lies directly within the belly of the supraspinatus, while SI-10 lies on the belly of infraspinatus, and SI-9 within teres minor. The Small Intestine acupuncture channel (meridian) is often used in cases of posterior shoulder pain (Fig. 17.28).
Biceps
The long head of biceps originates at the supraglenoid tubercle and passes intracapsularly into the bicipital groove (intertubercular sulcus). The tendon is round at its origin, flattens as it passes over the shoulder joint and narrows within the intertubercular sulcus (Mariani and Cofield, 1988). As the humerus moves, the tendon slides within its groove by as much as 3–4 cm. The tendon is held in the groove by the transverse ligament which is a thickening of the capsule and bridges the gap between the greater and lesser tuberosities. The coracohumeral ligament travelling from the lateral edge of the coracoid to the lesser and greater tuberosities assists in retaining the long head. Anatomical dissection and MRI studies on this area have revealed that the transverse humeral ligament is not a true separate entity (Gleason et al., 2006) but rather a merger of fibres from the supraspinatus and subscapularis. These fibres fuse into a single unit forming a tunnel over the long head of biceps. In addition the superior glenohumeral ligament folds into a U-shaped sling supporting the long head, and fibres of the supraspinatus tendon join the posterosuperior portion of this sling (Werner et al., 2000). The combination of several structures within this region allows load to be shared between the structural group rather than being taken in isolation by individual units.
Keypoint
In the region of the intertubercular sulcus the long head of biceps has structural associations with the supraspinatus and subscapularis tendons, and with the superior glenohumeral ligament. These associations allow load sharing between the structures.
Cadaveric studies have shown that the biceps tendon will not displace when the transverse ligament is cut, if the coracohumeral ligament remains intact (Slatis and Alato, 1979). The tendency for subluxation or dislocation of the tendon from the bicipital groove is dependent on a number of factors including the depth of the groove, and angle of the medial wall of the groove and the presence of a supratubercular ridge. Normally, the medial wall of the bicipital groove forms an angle of 60–70°, and angles of less than 30° when combined with a shallow groove have been shown to be associated with tendon subluxation (Donoghue: O’, 1973). A supratubercular ridge is present in 55% of the population, and well developed in 18% (Reid, 1992). It is a proximal extension of the medial wall of the bicipital groove, and may force the biceps tendon against the transverse ligament thus increasing tension. When the tendon subluxes, it does so in one of two ways, both normally associated with trauma to the humerus or rotator cuff (Petersson, 1986). The tendon usually moves medially and will lie superficial to the subscapularis if the transverse ligament ruptures. If the subscapularis remains attached to the transverse ligament, the biceps tendon may end up deep to the subscapularis tendon itself (Fig. 17.29).
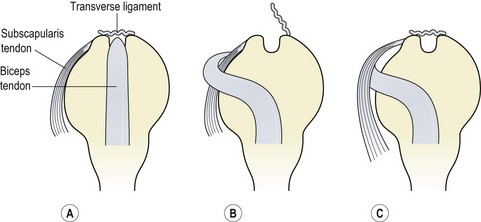
Figure 17.29 Biceps tendon subluxation. (A) Normal alignment. (B) Transverse ligament tears, biceps tendon rides over subscapularis. (C) Transverse ligament intact, biceps tendon slides beneath subscapularis.
After Reid (1992), with permission.
Biceps tendon dislocation typically occurs after a violent overhead action, with the athlete feeling pain on the anterior aspect of the shoulder. The shoulder will feel weak or ‘dead’ and often the athlete describes feeling ‘something going out’ or ‘snapping’. On examination there is tenderness to palpation over the tendon, and medial and lateral rotation may elicit a palpable click. This may be further investigated using Yergason’s sign (Yergason, 1931) or Speed’s test. Yergason’s sign may also be used to detect a labral tear.
Management of biceps tendon dislocation is usually surgical followed by intensive rehabilitation to restore correct scapulothoracic and glenohumeral function.
Keypoint
Both Yergason’s sign and Speed’s test attempt to reproduce biceps tendon dislocation using resisted shoulder and elbow movements.
Tendinopathy of the long head of biceps presents as pain to resisted shoulder and elbow flexion and resisted forearm supination. Yergason’s sign and Speed’s test may again be used. The teno-osseous junction of the muscle at the supraglenoid tubercle and adjacent glenoid labrum is difficult to palpate directly, but the tendon itself within the intertubercular sulcus is easier. A painful arc is only present with these conditions if the inflamed area of tendon is within a pinchable position in mid-range abduction, in which case impingement tests will be positive.
Overuse is the predominant causal factor with alteration in the biomechanics of overhead actions often being present. The synovial sheath of the tendon may become swollen and inflamed, with thickening and haemorrhaging frequently seen. Adhesions are often present. If the locking position and quadrant test reproduce pain, posteroanterior (PA) gliding should be assessed. If limited, PA pressures against the humeral head (see below) should be used.
Rupture of the biceps brachii occurs more commonly at the insertion of the long head into the supraglenoid tubercle, but tears to the short head, distal attachment or belly may occur (Fig. 17.30C). The rupture more frequently follows subacromial impingement and tendon degeneration (Reid, 1992). The mechanism of injury for proximal tendon injuries is normally a forced extension while the muscle is contracting. This can result from an arm tackle or block, where the arm is held abducted and then pushed back behind trunk level. Distal tendon injuries may occur as a result of heavy lifting with the elbow flexed to 90°.
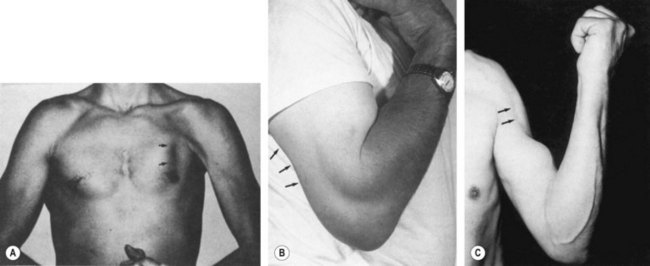
Figure 17.30 Ruptures to muscles in the shoulder region. (A) Pectoralis major. (B) Triceps. (C) Biceps.
After Reid (1992) with permission.
Keypoint
The biceps ruptures more commonly at its long head attaching into the supraglenoid tubercle. The injury normally occurs with forced arm extension as the muscle is contracting.
On examination, pain is elicited to resisted elbow flexion and supination (which may be combined with shoulder flexion), and passive end-range extension. A visible defect may be noted in the muscle, with retraction of the tendon. In the case of the long head, the tendon may no longer be palpable in the intertubercular sulcus, and as the muscle is contracted the belly of the long head is seen to bunch up into a ball-shaped mass. Local swelling and bruising are noted, and lead to an increased arm girth measurement.
Both surgical and conservative management have been recommended in the literature (Friedmann, 1963; Morrey et al., 1985; Bandy, Lovelace-Chandler and Holt, 1991). Surgical management is normally favoured (in the young especially) because conservative treatment has been said to give a loss of supination power (Baker and Bierwagen, 1985; Morrey et al., 1985). However, the reason for this deficit may be the lack of adequate rehabilitation following conservative management (Bandy, Lovelace-Chandler and Holt, 1991).
Conservative management consists of the RICE protocol to minimize inflammation, with gentle mobility exercises to the elbow within the pain-free range. Exercise therapy is used to maintain shoulder function. Multi-angle isometric training begins as soon as possible to reduce muscle atrophy, the deciding factor for starting this being pain. As pain to resisted movement reduces, dynamic exercise is begun against manual, and later isokinetic, resistance. PNF techniques combining shoulder flexion/adduction/medial rotation with elbow flexion/supination are used, as well as static stretching to elbow and shoulder extension. The resistance training programme is progressed with power actions, and functional sporting activities are introduced. The long-term prognosis is good in terms of restoration of function, but a palpable defect will usually remain in the muscle.
Surgery for distal tendon injuries includes re-inserting the tendon into the radial tuberosity, or the use of a fascia lata graft, where surgery has been delayed and the tendon has retracted. The long head may be re-inserted into the supraglenoid tubercle in the case of an avulsion or, in some instances, to the wall of the bicipital groove.
Pectoralis major
Rupture of the pectoralis major is unusual, but when it does occur, the muscle is usually already under tension when further force is imposed on it (Fig. 17.30A). The most common example of this scenario is the bench press exercise in weight-training. The injury normally occurs during the eccentric phase of the exercise as the bar is being lowered. During the last 30° of humeral extension of this action the inferior fibres of the muscle have been shown to lengthen disproportionately (Wolfe, Wickiewicz and Cavanaugh, 1992). In addition, with fatigue, the athlete may move the whole body in an attempt to lift the weight, and so bring accessory muscle groups into action enabling the athlete to exceed his or her safe limit. When lowering this excessive weight, the athlete loses control and the injury occurs.
Keypoint
The pectoralis major is most commonly ruptured while performing a bench press action in weight-training. The injury normally occurs during the last 30° of the eccentric (lowering) phase of the movement.
A tearing sensation is felt, and a large haematoma is apparent over the anterior axilla. Weakness and pain to resisted adduction and medial rotation is noted to manual muscle testing. No defect may be seen at rest, but if the muscle is contracted isometrically by asking the athlete to press the hands together as if clapping, a defect may be apparent. Following injury, the muscle does not retract very far, perhaps due to its varied fibre direction and wide origin. The insertion into the humerus (just lateral to the intertubercular sulcus) of the non-dominant arm is more normally affected (Kretzler and Richardson, 1989).
Non-surgical treatment can be successful for partial tears (Roi, Respizzi and Dworzak, 1990), and in the non-athletic individual (Delport and Piper, 1982). However, surgical management is more generally recommended (Kretzler and Richardson, 1989; Reut, Bach and Johnson, 1991). At operation the deltoid is retracted and the tendon is reattached either via drill holes in the humerus or by suturing the tendon to the remnant of tissue insertion.
The arm is immobilized in a sling and isometric contractions started as soon as the pain stabilizes. Assisted movements are begun 1 week after surgery, and thereafter the rehabilitation programme aims to restore strength, mobility and function. As strength training progresses, eccentric movements must be used to prepare the muscle for its action of decelerating the bar in the bench press exercise. In addition, pectoral muscle stretches and retraction work must be used to avoid a protracted shoulder posture.
Triceps
In addition to the more common elbow site for triceps injury, occasionally the muscle may avulse from its glenoid attachment (Donoghue: O’, 1976), especially in throwing athletes (Fig. 17.30B). Pain occurs to triceps stretching, often palpable at the inferior rim of the glenoid. With rest, a fibrous union will normally fix the fragment back in place, but surgery to remove the avulsed fragment and re-suture the tendon may be required where the injury recurs. When the muscle belly itself is injured, it is usually the medial head which is involved and the treatment of choice is conservative (Kunichi and Torisu, 1984).
It is important to note that the normal tendon is capable of sustaining considerable force before it will rupture, making avulsion fracture the more usual injury. Where tendon rupture occurs, an underlying pathology may be present. High dosage oral steroids may weaken the tendons (Hunter, Shybut and Nuber, 1986), a situation especially important with athletes using heavy resistance exercise or power movements. Conditions such as rheumatoid arthritis, systemic lupus erythematosus and hormone disorders may also predispose to tendon rupture (Reid and Kushner, 1989).
Bursitis
Gray’s Anatomy (Warwick and Williams, 1973) lists some eight bursae around the shoulder joint, but the one most commonly affected in sport is the subacromial (subdeltoid) bursa. This lies between the deltoid and the joint capsule and stretches beneath the acromion process and coracoacromial ligament. The bursa extends over the supraspinatus tendon (Fig. 17.31), and does not usually communicate with the joint capsule except in the case of a supraspinatus tear, where the bursa may be damaged as well. The subacromial bursa provides both proprioceptive and nociceptive information. Mechanoreceptors are found within the bursa adjacent to the corocoacromial ligament suggesting a reflex system to allow the rotator cuff to control the humeral head (Lewis, 2009).
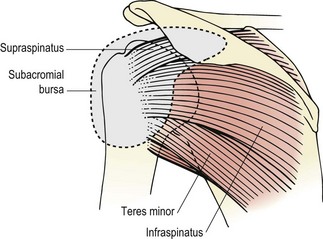
Keypoint
The subacromial bursa has both nociceptive (pain) and proprioceptive (movement sense) nerve endings.
Acute subacromial bursitis is unusual and occurs with sudden onset. The whole bursa is inflamed, and this severely limits abduction, but not in the capsular pattern. Pain is acute and often referred as far down as the wrist in extreme cases. Resisted movements are largely painless, and a painful arc only appears in a subacute case as initially no abduction at all is possible. Treatment in this acute stage is aimed at reducing the intense pain. The arm is supported in a sling to limit all glenohumeral movement, and anti-inflammatory modalities used.
Chronic subacromial bursitis occurs when the bursal sac becomes thickened and adherent, but in one part only. The condition is not a progression of acute bursitis but a separate clinical entity (Cyriax, 1982). The onset is gradual and a painful arc is present, but movements are largely of full range. Injecting the bursa with a local anaesthetic to inflate it is effective, and may act mechanically by simply pushing the walls of the bursal sac apart.
The subacromial bursa is a significant source of pain in many shoulder conditions. Surgical outcomes of bursectomy have been shown to be equal to that of acromioplasty (removal of part of the acromion process). Using arthroscopic debridement of thickened bursal wall (1−2 mm) carried out with an angled motorized shaver without acromioplasty, Budoff et al. (2005) produced excellent or good results in 87% of patients with an average follow-up of 53 months. These authors argued that debridement without acromioplasty minimized surgical trauma.
In all cases of bursitis, shoulder mechanics should be closely examined to detect any abnormality which may give rise to microtrauma. Typically, postural changes around the chest and shoulder can alter the mechanics of glenohumeral movement. This may predispose the athlete to impingement leading eventually to bursitis.
Shoulder instability
Classification
The stability of the glenohumeral joint lies very much on a continuum. At one end there is the stable, fully functional joint and at the other the dislocated joint requiring surgery. In many cases, there is a progression which begins with a reduction of stability through alteration in static, dynamic or proprioceptive factors. Individual differences in bony or soft tissue configuration can give some athletes a greater risk of instability, and training activities can alter the subtle muscle balance that exists around the joint. Trauma will cause both mechanical changes to stabilizing structures and alteration in proprioception. Any or all of these factors may coexist to push the athlete from a position of stability to one of instability of some degree. The progression from minor instability to major instability may then occur with time, unless there is treatment intervention of some type.
Instability may be classified using the TUBS/AMBRI acronyms (Matsen, Harryman and Sidles, 1991). These acronyms represent two ends of the spectrum (Table 17.2), from instability through trauma to instability through congenital factors. The patient with a TUBS lesion will have suffered traumatic instability in one direction only (unidirectional). The glenoid labrum will have been detached from the anterior rim of the glenoid (Bankart lesion) and surgery will probably be required, although rehabilitation should be tried first as this can be successful with minor degrees of injury. The AMBRI patient has an atraumatic aetiology causing multidirectional instability in both shoulders (bilateral). Usually this patient responds well to intensive rehabilitation, but if surgery is required, an inferior capsular shift is normally the treatment of choice.
Table 17.2 Classification of shoulder instability
| TUBS | AMBRI |
|---|---|
| Born loose↔ | Torn loose |
| T — Traumatic aetiology | A — Atraumatic aetiology |
| U — Unidirectional instability | M — Multidirectional instability |
| B — Bankart lesion | B — Bilateral condition |
| S — Surgical repair | R — Rehabilitation normally successful |
| I — Inferior capsular shift if rehabilitation fails |
The TUBS/AMBRI classification does not take into account those patients who present with instability due to altered muscle balance or ‘muscle patterning’ (Gibson, 2005a). An alternative classification is the Stanmore triangle (Lewis, Kitamura and Bayley, 2004). Here, instability is classified as three polar types (Fig. 17.32). Polar type I covers the traditional TUBS lesion where structural change has been induced through trauma. Polar type II is an instability through atraumatic change which is still structural and equates to the AMBRI lesion mostly. Polar type III represents instability through alteration of muscle patterning. The sides of the triangle represent both rehabilitation and surgery, and the essential feature of this classification is that patients can change their position through degeneration or disuse on the one hand and rehabilitation on the other. This classification enables us to predict more accurately those who are likely to respond favourably to rehabilitation. This is important because on the one hand altered muscle patterning has been cited as an important factor in the failure of stabilization surgery (McAuliffe et al., 1988), while on the other hand inappropriate surgical stabilization has been associated with an increased incidence of glenohumeral degeneration (Malone, 2004).
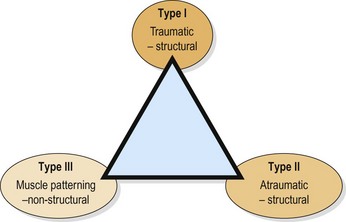
Stability mechanisms
Shoulder stability is supplied by both static and dynamic factors. Static stability is provided by the glenoid labrum, joint capsule and ligaments, while dynamic stability comes from muscle action (Table 17.3). As the arm hangs by the side of the body, the pull of gravity is resisted by the superior capsule and the coracohumeral ligament. If the arm is loaded, when carrying a bag for example, the greater force is resisted by the supraspinatus which shares a common distal attachment with the two previous structures and has a line of action which is virtually identical to them (Norkin and Levangie, 1992).
Table 17.3 Stability of the glenohumeral joint
| Dependent position | Coracohumeral ligament |
| Superior glenohumeral ligament | |
| Supraspinatus muscle | |
| Elevation | |
| Lower range (0–45°) | Anterior capsule |
| Superior glenohumeral ligament | |
| Coracohumeral ligament | |
| Middle glenohumeral ligament | |
| Subscapularis, infraspinatus, and teres minor muscles | |
| Middle range (45–75°) | Middle glenohumeral ligament |
| Subscapularis muscle (decreasing importance) | |
| Infraspinatus and teres minor muscles | |
| Inferior glenohumeral ligament (superior band) | |
| Upper range (.75°) | Inferior glenohumeral ligament (axillary pouch) |
| Throughout elevation | Dynamic activity of rotator cuff |
From Peat and Culham (1994), with permission.
The middle glenohumeral ligament lies directly under the tendon of subscapularis and is attached to it (Fig. 17.33). The ligament varies tremendously between subjects. In some it may be 2 cm wide, while in others it may be completely absent (Peat and Culham, 1994). Both the subscapularis and middle glenohumeral ligament limit external rotation and are important anterior stabilizers in the lower and middle ranges of abduction.
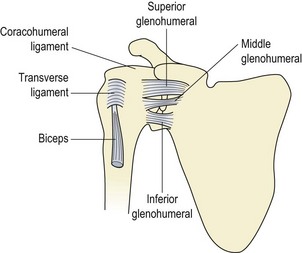
The inferior glenohumeral ligament (the thickest position of the glenohumeral ligament in total) is the most important passive stabilizing structure in overhead actions. The ligament is divided into three bands with the inferior portion forming the axillary pouch. The anterior band wraps around the humeral head at 90° abduction with external rotation and prevents anterior head migration (Brian et al.: O’, 1990). It is therefore the anterior band of the inferior glenohumeral ligament which is most significant in stabilizing the arm in overhead throwing sports. As this ligament tightens, abduction is limited and the humerus must laterally rotate and move towards the scapular plane.
The glenohumeral and coracohumeral ligaments form a ‘Z’ shape on the anterior aspect of the shoulder, with the middle glenohumeral ligament providing the crossbar of the Z. Above and below the crossbar are spaces which create areas of potential weakness. Superiorly (foramen of Weitbrecht) the opening allows the subscapularis bursa to communicate with the joint cavity. Inferiorly, a smaller bursa is sometimes present (Ferrari, 1990). In some subjects, if the Z crossbar (middle glenohumeral ligament) is missing, the anterior defect formed may contribute to anterior instability.
Active stability is provided by the rotator cuff muscles (Fig. 17.34). As previously stated the pull of the deltoid is almost vertical and it tends to cause upward translation of the humeral head. This is counteracted by the rotator cuff muscles, which tend to downwardly translate the head. The combination of the two sets of muscle translation forces stabilizes the head of the humerus in the glenoid. These compressor forces are at their maximum between 60 and 80° and are minimal after 120° (Comtet, Herberg and Naasan, 1989). Where a massive tear of the rotator cuff muscles occurs, stability of the joint can still be maintained by the middle deltoid alone compressing the humeral head into the glenoid (Gagey and Hue, 2000).
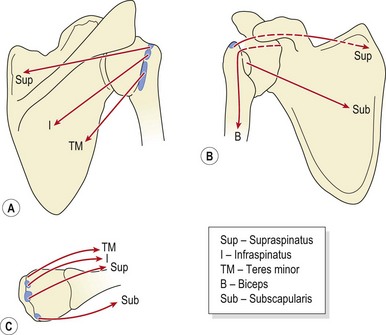
Figure 17.34 Active stabilizers of the glenohumeral joint. (A) Posterior. (B) Anterior. (C) Superior.
Where instability exists through altered rotator cuff or serratus anterior dysfunction, it is likely that compensatory muscle action will be seen. Anterior instability has been associated with change in pectoralis major activity and posterior instability with altered latissimus dorsi and anterior deltoid activity (Malone, 2004). In addition those with atraumatic instability show reduced proprioceptive ability of the upper limb (Barden et al., 2004).
Assessing instability of the shoulder
Passive stability
Passive or static instability of the glenohumeral joint may be assessed clinically by a number of drawer and apprehension tests. Anterior and posterior instability is initially tested with the athlete in a sitting position. The therapist grasps the athlete’s upper arm over the humeral head and applies forward and backward pressure while stabilizing the scapula (Fig. 17.35). The injured and uninjured sides are compared for range and end-feel. Excessive anterior glide leaves a posterior hollow, and the movement can be graded as mild (less than one third of the head coming off the glenoid), moderate (head riding on the edge of the glenoid, but spontaneously reduces when released) or severe (complete dislocation of the head). Posterior subluxation is considered abnormal when more than 50% of the humeral head comes off the glenoid.
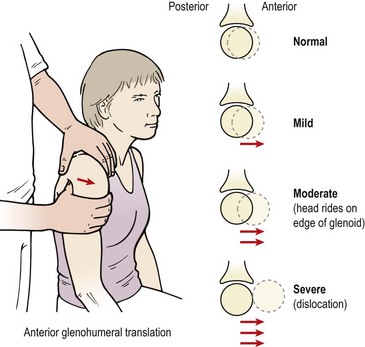
The apprehension test is again performed in a sitting position. The athlete’s arm is taken into 90° abduction and externally rotated. At the same time an anterior pressure is exerted on the proximal humerus (Fig. 17.36A). The test is positive in the presence of spasm or a feeling of impending (or actual) subluxation. A more rigorous procedure is to position the athlete in a supine-lying position, with the injured shoulder over the table edge. The arm is abducted to 90° and externally rotated. From this position the examiner applies an anteriorly directed pressure to increase pain and a posteriorly directed pressure to reduce pain (Fig. 17.36B).
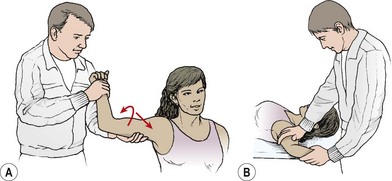
Active stability
Muscle control of the glenohumeral joint may be assessed using the dynamic rotary stability test (DRST) described by Margarey and Jones (2003). The DRST assesses the ability of the rotator cuff to keep the humeral head centred in the glenoid. The patient sits on a couch (Fig. 17.37A) with the therapist standing behind. The patient’s arm is held in a scaption (flexion−abduction) position with the elbow flexed to 90°. The therapist monitors the position of the patient’s humeral head whilst applying firstly resisted lateral rotation (patient twisting arm backwards) and then medial rotation (patient twisting arm forwards). The test is positive where anterior or posterior translation of the humeral head is detected and symptoms are provoked.


The DRST test may be extended to monitor which muscles are stabilizing the joint to differentiate between the local stabilizers (rotator cuff) and the global stabilizers (especially pectoralis major and latissimus dorsi). The patient and therapist take up the same starting position (Fig 17.37) but this time the patient’s forearm is placed on a supporting surface. A small stool may be used, or the therapist’s knee. Gentle longitudinal resistance is given to the patient’s humerus (traction) with the instruction to ‘stop me making your arm longer’ or to ‘suck your arm back into its socket’. The pectoralis and latissimus muscles are monitors for overactivity. The patient is then encouraged to ‘suck the arm back into the socket’ with minimal superficial muscle work as part of a training programme to re-educate the local stabilisor muscles.
Scapular control
Assessment of the patient’s ability to control the scapula throughout the three stages of abduction is vital. Postural assessment of scapular position at rest has been described in Chapter 5. The abduction cycle (see Table 17.1) forms the baseline for comparison during movement. As the arm is abducted, the patient’s posture is noted. Typically instability at the shoulder will be compensated by postural change with the patient weight bearing away from the painful side and shortening the trunk indicating that the latissimus dorsi is overactive. Pectoralis major dominance often presents as a protracted and medially rotated shoulder position at rest.
The scapula should remain fixed to the ribcage through serratus anterior action. Where this muscle is underactive the scapula may appear to wing, and when the arm is placed under load in a closed chain position the rhomboid muscles may compensate by pulling the medial edges of the scapulae together (see eccentric push-up in Fig. 17.38). During open chain actions the scapular position should be monitored as the glenohumeral joint is rotated. Where the latissimus is dominant the patient will often fix the scapular by adducting the arm (elbow tight into side of the body). Where the pectoral muscle dominates protraction and medial rotation often occurs rounding the shoulder into a ‘guarding’ position. The ability to differentiate glenohumeral movement from scapulothoracic movement (segmental control) should be assessed in a number of functional positions such as sitting, standing and reaching. Restoration of scapular stability and control is shown in Treatment note 17.1.
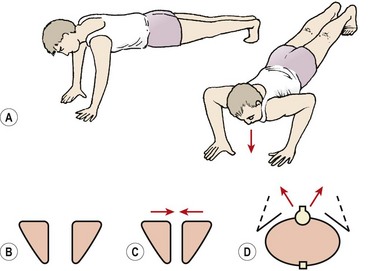
Figure 17.38 Eccentric push-up as a global assessment of scapulothoracic stability. (A) Athlete slowly lowers from a push-up position—note position of scapula. (B) Scapulae sho uld remain apart and fixed to the ribcage as the body is lowered. (C) Scapulae fall together if rhomboids and levator scapulae are dominant. (D) True winging. The medial edges of the scapulae lift.
Enhancing shoulder stability
Glenohumeral stability has been described as a circle concept (Dempster, 1965; Wilk and Arrigo, 1993). Translational movement of the humeral head is related to laxity of both the anterior and posterior structures. For example, anterior translation may be caused by tightness in the anterior structures, but will only be noticeable if the posterior structures are lax. Active stability is achieved through co-contraction of the rotator cuff muscles compressing the humeral head into the glenoid. Rehabilitation must involve work for the entire rotator cuff, rather than simply the supraspinatus, which has a contributory role only (Wilk and Arrigo, 1993).
Keypoint
For the glenohumeral joint to be unstable there must be both anterior and posterior laxity. To regain stability the same process applies, with work on both the anterior and posterior muscles being required.
A differentiation must be made between joint laxity and functional instability. Shoulder laxity is present when the humeral head can be passively translated on the glenoid. Functional instability, on the other hand, exists when unwanted humeral head motion compromises the comfort and function of a movement (Matsen, Harryman and Sidles, 1991). The difference is the patient’s ability to control the translational motion of the humeral head.
Proprioceptive training of the unstable shoulder
The principles behind proprioceptive training of the shoulder are similar to those described in Chapter 13 for the lumbar spine. The aim is to re-educate local and global stabilizers of both the glenohumeral and scapulothoracic joints using multisensory cues. Proprioceptive rehabilitation has been used successfully for shoulder rehabilitation by a number of authors (Smith and Brunolli, 1989; Lephart et al., 1994).
Proprioceptive training of the shoulder involves four elements (Lephart and Henry, 2000), shown in Table 17.4, which aim to re-educate neuromuscular control by stimulating actions at the level of spinal reflexes, brain stem and higher centres (see Chapter 5). Dynamic stabilization addresses both the glenohumeral and scapulothoracic joints. Co-activation of the local stabilizing muscles of the glenohumeral joint may be performed using pushing and pulling forces along the length of the humerus (long axis resistance) encouraging the patient to ‘suck the ball back into the socket’. Scapulothoracic stability is begun by maintaining the position of the scapula as the practitioner places it flat onto the thoracic wall in its optimally aligned position. Joint repositioning may be passive (therapist moves the limb) or active (patient moves the limb) and performed using a dynamometer for visual feedback or therapist dictated motion range. Initially exercises are performed with the eyes open and then closed. Reactive neuromuscular control is performed using unstable surfaces such as a Swiss ball or balance ball. Finally functional motor patterns are used which may involve resistance bands or pulleys in tri-plane motions, or complex whole body actions.
Table 17.4 Proprioceptive training of the shoulder
| Element of retraining | Importance | Exercise type |
|---|---|---|
| Dynamic stabilization | Co-activation of muscle forces to (i) centre humeral head on glenoid and (ii) fix scapula to thoracic wall (local stabilizers) | Joint approximation, building isometric endurance |
| Joint position sensibility | Precision of hand placement | Reproduction of active and passive joint position |
| Reactive neuromuscular control | Maintenance of stability against external loading (global stabilizers) | Unstable base |
| Functional motor patterns | Specific to athlete’s sport | Complex tasks |
From Lephart and Henry (2000) and Gibson and Elphinston (2005).
Closed kinetic chain activities
Essentially, closed kinetic chain activity involves movement of the proximal body segment on a fixed distal segment. This is common in the lower limb, during the stance phase of gait for example. In the upper limb the majority of daily actions occur in open chain format, with the distal segment (arm) moving on a fixed proximal base (thorax). However, the upper limb must be able to work in a closed kinetic chain pattern for ‘fall’ and ‘push’ actions. In many sports, the athlete is likely to fall onto the hand or elbow, and in some sports, such as gymnastics, complex closed kinetic chain actions are involved (handstand/vault). During a closed chain action, such as falling onto the outstretched arm, gravity assists in closing the chain of movement, approximating the joint surfaces. The muscle action is primarily eccentric to control the deceleration of movement and provide a protective role. As concentric action begins to accelerate the body segment, the joint surfaces are still approximated (push-up) whereas during open chain actions, the joint surfaces are under traction (throwing).
Keypoint
In closed kinetic chain exercises the muscle action is mainly eccentric to control excessive movement and protect the joint.
Traditional closed chain exercises include body weight (push-ups, dips) resistance and weights (bench and shoulder presses). Additional movements include the push-up with a press, and the sitting push-up. Hand walking activities are useful and may be performed on a wall, floor, treadmill, stepper, static cycling or on steps, either from a kneeling or prone falling position. Use of a rocker board for double-handed activities and a balance board for single handed activities is also useful for closed kinetic chain rehabilitation and is challenging to proprioception. The same would apply to activities on the Swiss ball and slide trainer (Fig. 17.39).
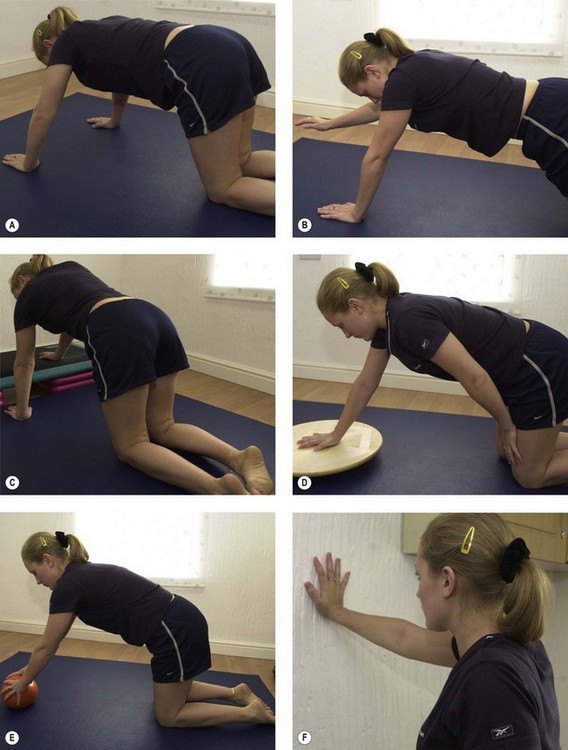
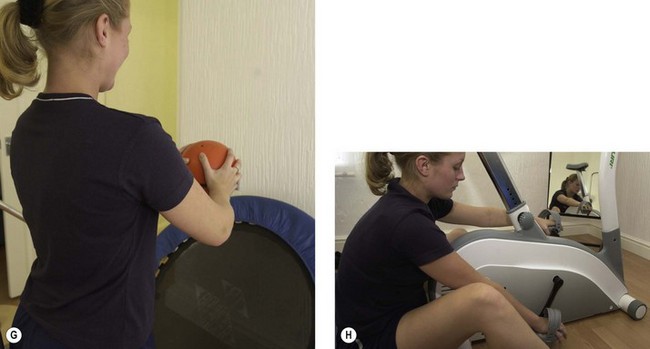
Resistance training
A variety of weight-training exercises may be performed to re-strengthen the shoulder musculature. Fig. 17.40 illustrates four movements which work both the glenohumeral and scapulothoracic muscles in both open and closed chain. The movements minimize the risk of impingement by combining lateral rotation movements with abduction in the scapular plane.
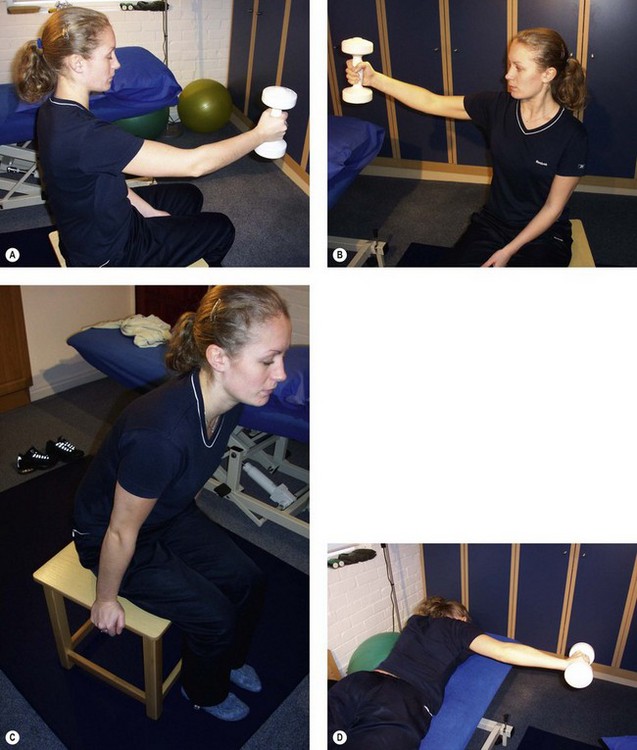
Figure 17.40 Glenohumeral exercises. (A) Elevation and lateral rotation in the sagittal plane. (B) Elevation and lateral rotation in the scapular plane. (C) Sitting press-up. (D) Horizontal abduction in lateral rotation.
In overhead motions, the cocking phase provides an eccentric pre-stretch to the muscles (adductors and internal rotators) closely followed by an explosive acceleration phase. Concentric−eccentric coupling of this type requires plyometric rehabilitation. Plyometrics involve a pre-stretch (eccentric) and short amortization phase where the movement direction is reversed, and finally a rapid facilitated concentric action. Activities include overhead soccer throws, basketball chest passes, single arm tennis ball throws, use of exercise tubing in PNF patterns and use of small medicine balls (Wilk et al., 1993).
Use of surface EMG
In an overhead motion the arm externally rotates, causing the humeral head to move superiorly. In this position the subscapularis is not able to control the humeral head any longer and the tendency to anterior translation is therefore increased. The joint must depend on the inferior glenohumeral ligament for passive stability, the only effective active control coming from the infraspinatus. If the ligamentous control is failing, enhancement of infraspinatus action can effectively control the humeral head (Reid, 1992).
Keypoint
When the arm is overhead and ligamentous stability of the humeral head is inadequate, the infraspinatus muscle can provide active stability.
The sEMG electrode is placed over the bulk of the infraspinatus below the scapular spine avoiding the posterior deltoid. The shoulder is flexed to activate the sEMG signal and the athlete is instructed to maintain the audible or visual signal from the machine by tightening the rotator cuff muscles. Isometric rotator cuff tightening is performed for multiple repetitions (10 sets of 10 repetitions), and then holding time is built (up to a 10-second hold) before active glenohumeral movements are commenced. Short lever shoulder flexion (in neutral rotation) is performed between 70 and 90° as the patient tries to push the sEMG signal up as high as possible. If pain or apprehension occur, the exercise is regressed to isometric holding alone. As sEMG signals can be maintained with active shoulder flexion, further exercises are added in a progression (Table 17.5). When painless and confident full-range motion has been obtained, general shoulder rehabilitation is begun.
Table 17.5 Use of surface EMG in rehabilitation of anterior instability of the shoulder
From Reid (1992), with permission.
Taping and mobilization with movement
When assessing static alignment of the glenohumeral joint, no more than one third of the head of the humerus should lie anterior to the acromion. In cases where the head of the humerus lies further forward (normally with impingement or instability symptoms), mobilization with movement and taping may be of help. Mobilization with movement (MWM) is a technique where a sustained mobilization is applied to a joint, normally at 90° to the plane of movement, to correct joint tracking (Mulligan, 1989).
The mobilization is applied at the same time as the patient performs a painful action with the affected joint. In the case of the shoulder, the painful action is abduction. The therapist stands behind the patient with one hand cupped over the anterior aspect of the shoulder, and the other braced against the scapula. A posterior gliding force is applied over the head of the humerus as the patient performs a previously painful abduction movement. The aim of the MWM is to allow the patient to perform the action painlessly to repetition. Eventually, the posterior glide is released, and the patient should still be able to perform the action with less (or no) pain.
If this technique is successful, a proprioceptive taping, which gives the patient the feeling of posterior glide and scapular depression, is often helpful (McConnell, 1992). The taping consists of the strips of 5 cm zinc oxide taping placed over adhesive net tape (Fig. 17.41). The first strip passes from the anterior aspect of the shoulder around the lateral aspect of the joint and down to the inferior angle of the scapula. The second strip passes from the anterior aspect of the shoulder, over the middle fibres of trapezius and again down to the inferior angle of the scapula. The adhesive net tape is placed on the shoulder in a relaxed state, but the zinc oxide tape pulls the skin to give the patient the sensation of posterior gliding (strip one) and scapula depression (strip two). The gap between the two pieces of tape should correspond to the sulcus which appears at the tip of the acromion at 90° abduction. As with the MWM, the taping should reduce the pain of abduction to re-test.
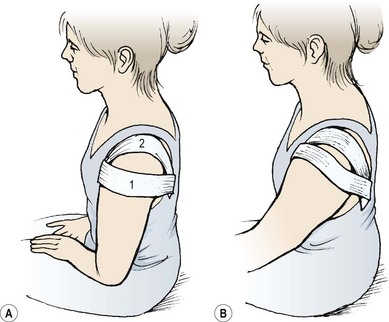
Labral tears
The glenoid labrum (Fig. 17.42) is a 4 mm ring consisting of fibrocartilage which attaches to the rim of the glenoid fossa, and fibrous tissue which attaches to the joint capsule. The inner labral surface is lined with synovium, and the outer surface attaches to the joint capsule and merges with the periosteum of the humerus. The long head of biceps attaches to the supraglenoid tubercle and strengthens the labrum superiorly. This superior aspect of the labrum may not be attached to bone at all on its inner edge but can project into the joint forming a meniscus (Palastanga, Field and Soames, 2006).
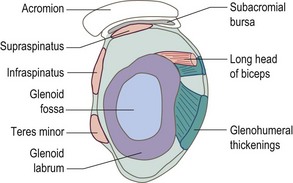
Tears of the labrum may be divided into Bankart tears affecting the anterior inferior portion of the labrum and SLAP lesions affecting the superior portion, the pneumonic SLAP standing for Superior Labral tear travelling Anterior to Posterior. Bankart tears are usually associated with anterior shoulder dislocation and a SLAP lesion with traction of the tendon of the long head of biceps.
SLAP lesions have been classified into several types (Table 17.6). The essential mechanism of injury involves force placed through the long head of biceps, either through trauma or repetitive loading. High eccentric loading occurs during overhead activities involving a combination of abduction and external rotation (cocking phase of throwing). This in combination with shoulder instability has been suggested as the most likely causal factor (Dodson and Altchek, 2009).
| Type I | Fraying or degeneration to edge of superior labrum |
 |
| Type II | Detachment of biceps tendon and superior labrum from glenoid rim (most common type) |
 |
| Type III | Biceps tendon remains intact, superior labrum suffers bucket handle tear and displaces into joint |
 |
| Type IV | Bucket handle tear of superior labrum and part of biceps tendon both of which displace into joint (least common type) |
 |
Several tests exist to identify SLAP lesions clinically with O’Brian’s active compression test perhaps being the most common (Brian et al.: O’, 1998). Here, the shoulder is placed in 90° forward elevation and 20° horizontal abduction. The therapist places a downward force onto the patient’s forearm with the arm firstly pronated (stretching biceps) and then supinated (relaxing biceps). The test is positive where pain is produced with the forearm in the pronated (biceps on stretch) position. This arm action is also a close pack position for the acromioclavicular joint, so the AC joint must be discounted first. Research on the ability of clinical tests to evaluate the presence of a SLAP lesion suggests that a battery of several tests is required. A meta-analysis of 12 studies describing 14 tests concluded that the Yergason’s test was the only test to have a significant ability to influence clinical decision making (Walton and Sadi, 2008). A systematic review of 17 papers concluded that no single test was sensitive or specific enough to determine the presence of a SLAP lesion and suggested that a combination of two or more tests was required (Dessaur and Magarey, 2008).
Keypoint
A single examination test is not sufficient to diagnose a SLAP lesion. A combination of several tests is required.
Treatment of labral tears is conservative initially, with surgery only indicated for those who fail conservative management (Dodson and Altchek, 2009). The aim is to restore normal shoulder motion (both glenohumeral and scapulothoracic) and stability. Where the causal action has involved repeated external rotation and abduction, there is likely to be a soft tissue imbalance with a loss of glenohumeral internal (medial) rotation compared to external (lateral) rotation, a glenohumeral internal rotation deficit (GIRD). In this case stretching into internal rotation is required.
Surgical management is to re-attach the labrum using sutures and bone anchors. Following surgery rehabilitation is vital. For the first 3 weeks post surgery patients are normally protected in a sling for day to day usage. In this period postural awareness, scapulothoracic stability and glenohumeral stability actions are taught. Stability exercise uses shoulder joint control rather than motion range, with bracing actions, closed chain positions and movement awareness drills as for instability. Abduction and external rotation actions are generally avoided with the arm kept predominantly in flexion and below shoulder height. Extension and abduction may be used if pain is tolerated. Motion range progresses after 3 weeks with the aim of full active range by 6−8 weeks post surgery and full sport specific function within 3−4 months.
Glenohumeral dislocation
Dislocation (often a progression from instability) is a commonly seen shoulder injury, with anterior displacement being encountered more often than posterior. Forced movements involving external rotation and abduction are common mechanisms, and a fall onto the outstretched arm is also a frequent aetiology.
Keypoint
The mechanism of injury for anterior dislocation is normally forced abduction and external rotation of the shoulder joint.
At the time of injury the glenoid labrum may become detached (together with the inferior glenohumeral ligament) giving a Bankart lesion, sometimes with a parallel fracture of the glenoid rim. Acute anterior dislocation gives considerable pain. The arm is usually held slightly abducted and externally rotated, and the normal rounded contour of the shoulder is lost. Close inspection shows the acromion process to be more prominent than usual, and a hollow is visible below it. The displaced humeral head can usually be felt on the anterior aspect of the shoulder.
The question of whether to reduce an acute injury is one of debate. On the positive side, early reduction of an uncomplicated injury may be achieved without anaesthetic and with little discomfort. If left, muscle spasm sets in, making reduction under anaesthetic necessary. The main problem is the likelihood of further injury by reduction without x-ray by inexperienced staff. Fracture of the head or neck of the humerus may have occurred at the time of injury and epiphyseal displacement is seen with adolescents. Displaced bone fragments may easily be pulled onto the circumflex or radial nerves causing injury, and vascular damage may also occur.
Where an area of numbness is present over the deltoid, injury to the axillary nerve should be suspected, and swelling in the hand and fingers together with a loss of pulse suggests arterial damage as a result of humeral fracture (Reid, 1992). For these reasons, an acute injury occurring for the first time is better referred to an orthopaedic consultant.
Keypoint
Following shoulder dislocation, the presence of numbness over the shoulder, swelling in the fingers or a loss of pulse suggests complications requiring urgent medical attention.
Recurrent anterior dislocation may be reduced more easily. The forces required to dislocate the shoulder in the first place are considerably less than with the acute injury, and so the chance of associated fracture is minimal. Spontaneous reduction may occur, and frequently the athlete has learnt to reduce the dislocation him- or herself, and the joint is fairly lax. For assisted reduction a number of techniques are available:
With the patient in a supine position on the ground, the therapist sits on the patient’s injured side. The therapist places his or her stockinged foot just below the ipsilateral axilla, while holding the patient’s arm. The therapist then simply leans back to provide traction, and may gently rotate the arm to facilitate reduction.
The simplest self-reduction procedure is for the athlete to bend the ipsilateral leg and grasp the knee with both hands, keeping the arms locked straight. Slowly leaning back produces in-line traction which usually allows the shoulder to reduce. It must be emphasized that these procedures should only be performed in the absence of pain and spasm. The traction is applied gently, brute force or ‘yanking’ the arm by another athlete being obviously contraindicated.
As an alternative the patient may lie prone on a couch or gym bench with the arm hanging over the edge of the couch (hand off the floor). The weight of the arm will usually provide sufficient traction to initiate spontaneous reduction. Holding a weight in the hand (small dumb-bell) will assist the traction force. If the recurrently dislocated shoulder does not reduce readily, referral is still necessary.
Surgical repair (Bankart repair) may be carried out to repair the torn glenoid labrum with sutures and reattach it to the glenoid using anchors. In cases where there is capsular and/or ligamentous laxity the lax tissue may be tightened (capsular shrinkage) using either a radio frequency heating probe or capsular plication (suturing).
Definition
Capsular shrinkage is carried out by heating the capsule arthroscopically and changing the nature of the collagen fibres. Capsular plication involves tightening the loose capsule using sutures (sometimes called ‘nip and tuck’).
Acute posterior dislocation is not as obvious as anterior. Pain is still intense, with the arm held adducted and internally rotated. Any attempt to move the arm is resisted by intense muscle spasm. In thin individuals the coracoid process is more visible than usual, and fullness is often apparent posteriorly. Heavy musculature in an athlete will, however, obscure these signs. Posterior dislocations require referral and reduction under sedation. Gentle in-line traction is applied to the adducted/internally rotated arm with gentle pressure over the humeral head.
Rehabilitation following anterior dislocation
Following reduction, rest and ice are used to limit inflammation. The arm is immobilized, and the initial period of immobilization is an important determinant of recurrence. Normally the recurrence rate for young (20–30 years) athletes may be as high as 85% (Halbach and Tank, 1990). However, this may be reduced considerably, with one study of 50 individuals showing a recurrence rate of 20% after 6 weeks immobilization (Reid, 1992). Exercise therapy is divided into four phases (Table 17.7).
Table 17.7 Guidelines for rehabilitation following anterior glenohumeral dislocation
| Initial post-reduction period |
| 0–3 weeks |
| 3–6 weeks |
| 6–8 weeks |
| Final rehabilitation |
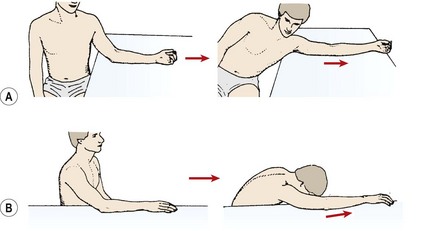
Slow velocity (90°/s) isokinetics may be used, with the velocity gradually increasing to functional sporting levels as the athlete is able to control the movement. Pool exercises are used to incorporate faster actions against the resistance of a paddle, and range of motion exercise using flotation to take the weight of the arm. PNF techniques involving extension/adduction/medial rotation are used initially against manual resistance and subsequently with a weight and pulley system. Later, flexion/abduction/lateral rotation is used with caution. Restoration of kinaesthetic awareness is important after anterior dislocation (Smith and Brunolli, 1989).
Frozen shoulder
Frozen shoulder or ‘adhesive capsulitis’ is an increasingly common pathology found in sport and exercise medicine. As the number of elderly people involved in sport continues to rise, this condition is likely to be seen even more frequently. Exercise therapy is a key component to treatment of this condition meaning that exercise professionals are very likely to see patients who have suffered from this condition.
Between 2% and 3% of the adult population between the ages of 40 and 70 develop the problem and the condition is more common in women. It presents as a gradual loss of shoulder movement, with or without pain. The initial loss of movement may go unnoticed until function is limited. Patients complain that activities of everyday living become increasingly difficult. Combing the hair at the back of the head and fastening a bra strap are frequent sources of complaint. Active sports persons frequently notice the onset of the condition earlier than sedentary individuals. Elderly athletes often complain that their golf swing is affected, or overhead badminton shots are painful for example.
The term ‘frozen shoulder’ (Codman, 1934) is not an accurate diagnosis, but rather a description of the major symptom, which is lack of movement. ‘Adhesive capsulitis’ (Neviaser, 1945) describes the finding of capsular thickening, contraction and adhesions. The condition may appear as a primary (insidious) or secondary (traumatic) adhesive capsulitis. Secondary types can be associated with a number of soft tissue and medical pathologies including rotator cuff injuries, impingement syndrome, traumatic arthritis, osteoarthritis, shoulder joint immobilization, autoimmune disease, diabetes and thyroid dysfunction (Boissonnault and Janos, 1989; Hertling and Kessler, 1990; Ott, Clancy and Wilk, 1994). Up to 30% of individuals develop the condition in the opposite shoulder (Sheridan and Hannafin, 2006).
Keypoint
Frozen shoulder can be primary (idiopathic) or secondary. The condition may be secondary to shoulder injury or a number of medical pathologies, and has a tendency to recur in the opposite shoulder.
Frozen shoulder is normally categorized into three stages representing freezing (stage I), frozen (stage II) and thawing (stage III) (Table 17.8).

During stage (I) pain is the predominant feature, with dull aching at rest. Movement range increases significantly when intra-articular injection or anaesthesia is given, showing that muscle spasm is a key feature. Arthroscopic examination has shown hypervascular synovitis especially lining the anterosuperior capsule in the region of the rotator interval. The capsule itself is normal.
During stage (II) there is diffuse pedunculated synovitis and capsular tightening. No inflammatory infiltrates are present in this stage showing that the synovitis is burning out. The capsule develops fibroplasia with hypercellular collagenous tissue laid down (Sheridan and Hannafin, 2006) explaining the dense rubbery end feel. The capsule may adhere to the humeral head, with the axillary pouch frequently being obliterated. A reduction in joint volume has been noted on arthrogram (Reeves, 1966), and a loss of bone mineral content can be seen on x-ray (Lundberg and Nilsson, 1968). An increase in vascularity and thickening has been noted in the subacromial bursa and rotator cuff (Simmonds, 1949), and a contracture of the coracohumeral ligament (Ozaki et al., 1989). Changes to the subscapular bursa, rotator cuff and biceps tendon (Uitvlugt, Detrisac and Johnson, 1988; Wiley, 1991) indicate that these structures may be key factors in the initiation of the condition. Arthroscopic examination has revealed fibrous contracture of the rotator interval and coracohumeral ligament which primarily limits lateral rotation (Bunker, 1997). Histological evaluation of the fibrous tissue has shown it to be similar to that found in Dupuytren’s contracture (Cleland and Durall, 2002).
Stage (III) is the thawing stage showing an improvement in motion range due to capsular remodeling.
Definition
The rotator interval is the space between the anterior border of the supraspinatus tendon and the superior border of the subscapularis tendon (Fig. 17.44). The space is filled by the coracohumeral ligament which limits inferior translation and lateral rotation.
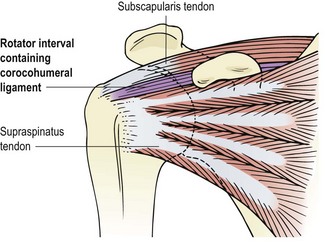
On examination, movement is usually limited in a capsular pattern (subacute) or by muscle guarding (acute), but resisted movements are normally pain free. Accessory movements are limited, particularly inferior and anterior gliding, and the quadrant position is limited and painful when compared to the uninvolved side. Three stages of the condition have been described (Maitland, 1991).
Management
Management of adhesive capsulitis includes physiotherapy, medication and surgery. Physiotherapy tends to use joint mobilization, acupuncture/dry needling and exercises. Surgical intervention is mainly by manipulation under anaesthesia (MUA) and arthroscopic dissection. Medication on the whole includes corticosteroid injection and the use of non-specific anti-inflammatory drugs (NSAIDs) or analgesics. Corticosteroid injection has been shown to be effective in the short term but to have little long term (6–18 months) benefit (Van der Windt and Koes, 2002). Patients treated with MUA have been shown to achieve a 50 point functional improvement score while those treated with physiotherapy gained a 78 point score (Melzer et al., 1995). However, physiotherapy for adhesive capsulitis can be protracted with studies reporting 12–29 treatment sessions on average (Cleland and Durall, 2002). Following an active physiotherapy programme which includes home exercise, 90% of patients have reported a satisfactory result (Griggs, Ahn and Green, 2000) and patients rated their shoulder function improvement as excellent (57%) or good (29%) (Vermeulen et al., 2000). Although spontaneous recovery may occur, as many as 50% of patients can still have symptoms up to 7 years later if not treated (Shaffer, Tibone and Kerlan, 1992).
MUA has been criticized for the intra-articular lessions caused by this procedure. In an arthroscopic study of 30 patients following MUA, Loew, Heichel and Lehner (2005) showed haemarthrosis in all patients, local synovitis in the region of the rotator cuff and capsular rupture. Acute intra-articular lesions were seen in 12 patients, and these consisted of labral detachment, rupture of the glenohumeral ligament, tear of the subscapularis tendon and worsening of supraspinatus fraying. The trauma caused by MUA has made arthroscopic capsular release more popular. In this technique the joint is evaluated arthroscopically making precise surgical release of the fibrosed capsular portion possible. In addition arthrographic distension may be performed under a local anaesthetic to mechanically distend the joint to stretch adhesions within the capsule.
Manual therapy
Pain may be greatly reduced by posteroanterior (PA) oscillations (Maitland, 1991), and scapulothoracic mobilization, and these are the manual treatments of choice for the stage I lesion. For PA mobilization, the patient lies in a supine position with the arm supported in a pain-free position. The elbow is flexed with a folded towel placed under the arm. The patient’s forearm rests on the trunk. This position limits adduction, extension and excessive medial rotation. The therapist kneels on the floor and directs his or her thumbs to the posterior aspect of the humeral head. The oscillations are produced by the therapist’s arms rather than the finger flexors. For scapulothoracic mobilization the patient lies on the side with the injured arm uppermost. The arm should be in a pain-free position supported by towels. The therapist grasps the medial edge of the scapula with his or her fingertips in an attempt to release the scapula from the ribcage first, and secondly to abduct it, easing it away from the spine.
With the stage II condition, the pain is limited first, and then stiffness is addressed. As pain is reduced, the starting position is changed to use the patient’s upper arm as a lever. The therapist grips the patient’s upper arm in his or her cupped hands, high into the axilla. Initially, the arm is by the patient’s side (Fig. 17.45A). From this position the slack is taken up in the joint by lifting it anteriorly, and then the arm is lifted and lowered to perform the PA glide. As pain lessens and movement returns, the same action is performed with the arm held abducted to 45° (Fig. 17.45B), and then in full flexion overhead (Fig. 17.45C).
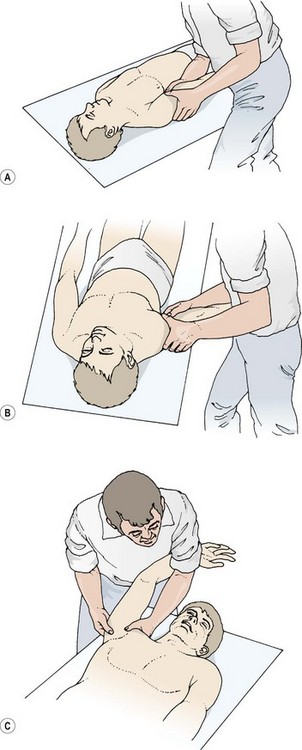
Figure 17.45 Posteroanterior glenohumeral joint movement. (A) Patient’s arm by his or her side. (B) 45° abduction. (C) Maximal flexion–abduction.
Inferior gliding, if limited, may be regained with the patient’s shoulder flexed to 90° and the patient’s hand on the trapezius (central fibres). The therapist stabilizes the patient’s elbow against his or her own shoulder and grips the upper arm in cupped hands. The gliding motion pulls the humeral head inferiorly. As pain reduces, a similar movement may be performed with the patient’s arm abducted and supported. The therapist pushes down on the humeral head with the web of his or her free hand (Fig. 17.46).
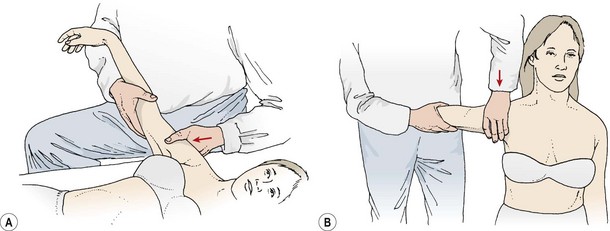
Figure 17.46 Inferior gliding, glenohumeral joint. Patient in (A) supine, or (B) sitting position. The arm is grasped near the elbow to stabilize it in 90° abduction. The web of the other hand contacts the head of the humerus. The head of the humerus is then depressed inferiorly.
The final range of movement may be regained using the quadrant position (see above) as a mobilization to stretch the anterior capsule. This is only used when pain is minimal and stiffness is the predominant symptom (late stage II and stage III lesions). The therapist stands at the head of the couch with his or her knee resting on the couch top (Fig. 17.47A). The arm is then oscillated through approximately 30° to facilitate a grade II mobilization. A grade IV movement may be used by placing the therapist’s nearside arm under the patient’s upper rib angles; a small 5° oscillation is all that is required (Fig. 17.47B).
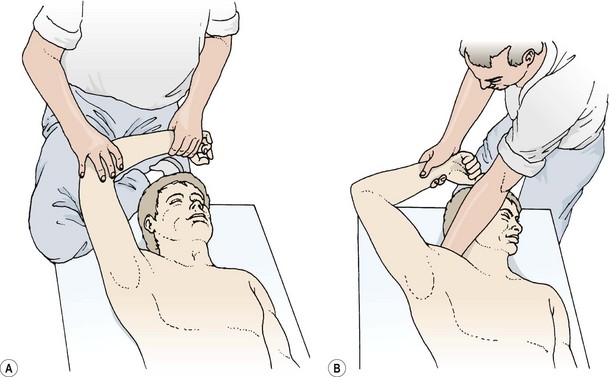
Exercise therapy
In stage (I), the primary aim is to reduce pain and ensure that the joint is not irritated to increase the inflammatory reaction of the involved soft tissues (Table 17.9). Pendular swinging actions may be used to great effect. The patient leans over a table with the unaffected hand supporting them. The affected arm is allowed to relax and ‘go heavy’, allowing arm weight to slightly traction the joint in its flexed–abducted position. The action is to sway the body and impart a gentle circling movement on the straight arm which is transmitted to the glenohumeral joint (Fig. 17.48A). It must be emphasized that shoulder muscle action should not create the movement, but rather bodysway. The action should be performed in both clockwise and anticlockwise directions and repeated every 2 hours throughout the waking day.
Table 17.9 Movement therapy for adhesive capsulitis
| Stage | Pathology and signs | Exercise therapy |
|---|---|---|
| (I) ‘Freezing’ | Scar tissue forming and maturing. External rotation of shoulder markedly reduced, abduction less limited. Spasm end feel |
Active range of motion exercise Joint mobilization for pain relief, not increased range Pendular swinging |
| (II) ‘Frozen’ | Scarring mature. Glenohumeral joint lost mobility. Patient unable to lie on affected side at night. Elastic end-feel |
More aggressive joint mobilizations providing joint is not irritated Stretching Strengthening within pain-free ranges |
| (III) ‘Thawing’ | Arm pain dominates, shoulder pain less intense. Gross reverse scapulohumeral rhythm. Hard leathery end-feel |
Scapular stability Aggressive glenohumeral joint mobilization. End range stretching Movement re-education |

Figure 17.48 Exercise therapy for adhesive capsulitis. (A) Pendulum swinging. (B) Flexion–abduction with traction. (C) Resisted lateral rotation. (D) Initial range of abduction.
In stage (II), pendular swinging may be continued for pain relief, but stretching and strengthening should begin. Stretching focusses on the anterosuperior capsule and/or posterior capsule. Flexion–abduction with traction may be used in kneeling, holding onto an object or simply gripping the floor with the fingertips and moving the bodyweight backwards to sit on the heels (Fig. 17.48B). The aim is to encourage movement rather than force it. Resisted lateral rotation may be used in side lying with the weight of the arm initially and a light dumb-bell as pain allows (Fig. 17.48C). Abduction within the pain-free range should be used in side lying (Fig. 17.48D) rather than standing at this stage. In standing, the increased leverage as the arm reaches the horizontal position encourages shoulder shrugging and reverse scapulohumeral rhythm.
Scapular stability work should begin and as abduction and lateral rotation range increases, all three movements should be combined in sitting (Fig. 17.49). The patient begins the action by drawing the scapula down gently. While maintaining this position, the bent arm is laterally rotated and the elbow lifted from the couch. The distance between the ear and the shoulder should be maintained as shoulder shrugging is avoided.

Figure 17.49 Combining shoulder lateral rotation and abduction with scapular stability. (A) Scapular repositioning. (B) Arm lifting.
Definition
Normally in arm abduction there is more glenohumeral movement than scapulothoracic movement (ratio 2 : 1). With reverse scapulohumeral rhythm, glenohumeral movement is reduced and scapulothoracic movement increased to compensate.
In stage (III) end-range stretching and further strengthening is used. The sit to heels exercise and sitting abduction-lateral rotation may be continued with the aim of increasing range of motion in each. Passive abduction and lateral rotation using a stick or towel in lying (Fig. 17.50A) is useful as the leverage involved assists in obtaining the final few degrees of movement. Both medial and lateral rotation may be gained using a hand behind neck (HBN) and hand behind back (HBB) action (Fig. 17.50B). Several weight-training exercises may be used to regain should strength and improve range of motion, including shoulder press, lateral pull-downs, and pulley abduction movements (Fig. 17.51).
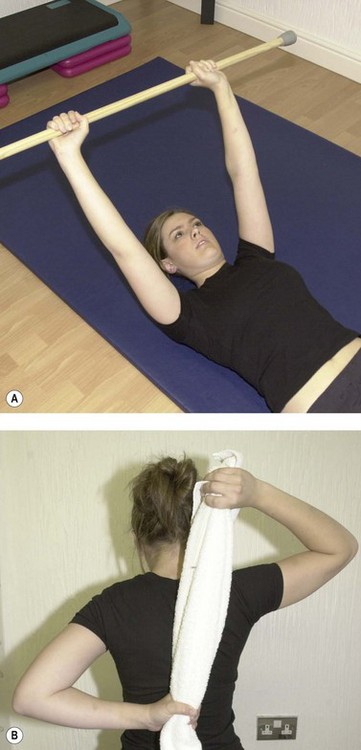
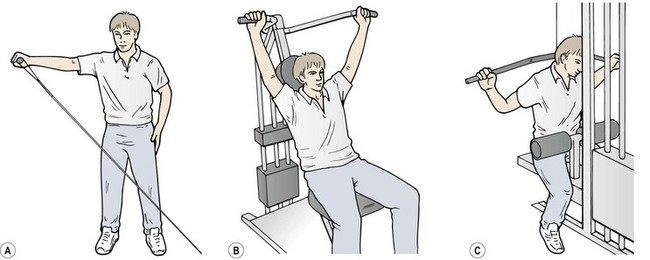
Figure 17.51 Weight training actions for the shoulder. (A) Cable lateral raise. (B) Shoulder press. (C) Lateral pull-down.
From Norris, C.M. (1996). Weight Training. CD-ROM Package. Exercise Association, London. With permission
Snapping scapulae
This unusual condition occurs especially in adolescent females just after skeletal maturity, and in both sexes following surgery. Patients experience a snapping sensation, which is sometimes audible, near the vertebral border of the scapula. Pain is often localized to the rhomboids and levator scapulae over the medial scapular border or the trapezius over the medial aspect of the scapular spine. One possibility is that tendinopathy occurs to the muscles, another that the bursa located beneath the medial border of the scapula becomes inflamed.
The condition occurs through microtrauma from excessive shearing forces beneath the scapula due to abnormal scapulothoracic rhythm. Management relies on the restoration of a more normal scapulothoracic rhythm (Percy, Birbrager and Pitt, 1988).
Nerve entrapment syndromes
Two relatively uncommon nerve entrapments are seen around the shoulder, quadrilateral space syndrome and entrapment of the suprascapular nerve.
The quadrilateral (quadrangular) space lies between the teres minor and the subscapularis above and the teres major below. The long head of triceps forms its medial wall and the surgical neck of the humerus lies laterally (Fig. 17.52A). Entrapment by tethering can occur to both the axillary nerve and circumflex humeral artery (Cahill and Palmer, 1983). The patient, frequently a throwing athlete, is usually young (22–35 years) and complains of shoulder pain of insidious onset. Muscle fatigue and loss of abduction power are apparent and tenderness may be elicited to palpation over the involved quadrilateral space. Arteriograph frequently shows posterior circumflex artery occlusion. Most patients respond to alteration of throwing technique but some may go on to surgical decompression.
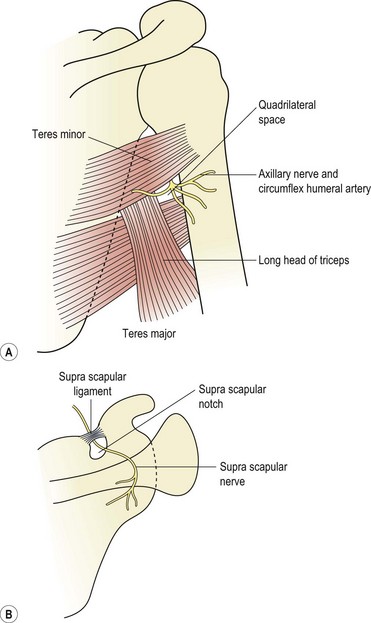
Figure 17.52 Entrapment neuropathy in the shoulder. (A) Quadrilateral space. (B) Suprascapular notch.
The suprascapular nerve (Fig. 17.52B) may be trapped as it passes through the suprascapular notch beneath the suprascapular ligament, or as it winds around the lateral edge of the scapular spine. Direct blows in contact sports are one cause as the nerve is superficial, and occult ganglions pressing on the shoulder have been described (Fritz et al., 1992; Gerscovich and Greenspan, 1993). Entrapment can affect the motor response of both the supraspinatus and infraspinatus, either together or in isolation (Black and Lombardo, 1990). The patient presents with visible muscular atrophy and weakness is often noticed to backhand shots or in serving. Vague pain occurs deep in the posterior aspect of the shoulder. Treatment involves decompression of the nerve at the suprascapular notch and scapular nerve block.
Apley A.G., Solomon L. Concise System of Orthopaedics and Fractures. London: Butterworth; 1989.
Austin K.A., Gwynn-Brett K.A., Marshall S.C. Illustrated Guide to Taping Techniques. St Louis: C.V. Mosby; 1994.
Baechle T.R. Essentials of Strength Training and Conditioning. Champaign, Illinois: Human Kinetics; 1994.
Baker B.E., Bierwagen D. Rupture of the distal tendon of the biceps brachii: operative versus non-operative treatment. Journal of Bone and Joint Surgery. 1985;67A:414-417.
Bandy W.D., Lovelace-Chandler V., Holt A. Rehabilitation of the ruptured biceps brachii muscle of an athlete. Journal of Orthopaedic and Sports Physical Therapy. 1991;13(4):184-190.
Bannister G.C., Wallace W.A., Stableforth P.G., Hutson M.A. The management of acute acromioclavicular dislocation: a randomised prospective controlled trial. Journal of Bone and Joint Surgery. 1989;71B:848-850.
Barden J.M., Balyk R., Raso V.J., et al. Dynamic upper limb proprioception in multidirectional shoulder instability. Clinical Orthopaedics and Related Research. 2004;420:181-189.
Bigliani L.U., Morrison D.S., April E.W. The morphology of the acromion and its relationship to rotator cuff tears. Orthopaedic Transactions. 1986;10:228.
Black K., Lombardo J. Suprascapular nerve injuries with isolated paralysis of the infraspinatus. American Journal of Sports Medicine. 1990;18(3):225-228.
Boissonnault W.G., Janos S.C. Dysfunction, evaluation, and treatment of the shoulder. In: Donatelli R., Wooden M.J., editors. Orthopaedic Physical Therapy. Edinburgh: Churchill Livingstone, 1989.
Budoff J.E., Rodin D., Ochial D., Nirschl R.P. Arthroscopic rotator cuff debridement without decompression for the treatment of tendinosis. Arthroscopy. 2005;21(9):1081-1089.
Bunker T.D. Frozen shoulder: unravelling the enigma. Annals of the Royal College of Surgeons of England. 1997;79:210-213.
Cahill B.R. Osteolysis of distal part of clavicle in male athletes. Journal of Bone and Joint Surgery. 1982;64A:1053-1058.
Cahill B.R., Palmer R.E. Quadrilateral space syndrome. Journal of Hand Surgery. 1983;8:65.
Cain P.R., Mutschler T.A., Fu F.H. Anterior stability of the glenohumeral joint: a dynamic model. American Journal of Sports Medicine. 1987;15:144.
Chronopoulos E., Kin T., Park H., et al. Diagnostic value of physical tests for isolated chronic acromioclavicular lesions. American Journal of Sports Medicine. 2004;32(3):655-661.
Cleland J., Durall J.C. Physical therapy for adhesive capsulitis: systematic review. Physiotherapy. 2002;88(8):450-457.
Codman E.A. The Shoulder. Boston: Thomas Todd; 1934.
Comtet J.J., Herberg G., Naasan I.A. Biomechanical basis of transfers for shoulder paralysis. Hand Clinics. 1989;5:1.
Cook J.L., Purdam C.R. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine. 2009;43:409-416.
Cools A.M., Witvrouw E., Declercq G., et al. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement symptoms. British Journal of Sports Medicine. 2004;38:64-68.
Corrigan B., Maitland G.D. Musculoskeletal and Sports Injuries. Oxford: Butterworth-Heinemann; 1994.
Culham E., Peat M. Functional anatomy of the shoulder complex. Journal of Orthopedic and Sports Physical Therapy. 1993;18(1):342-350.
Cyriax J. 8th edn Textbook of Orthopaedic Medicine vol. 1 London: Baillière Tindall, 1982.
Cyriax J.H., Cyriax P.J. Illustrated Manual of Orthopaedic Medicine. London: Butterworth; 1983.
Delport H.P., Piper M.S. Pectoralis major rupture in athletes. Archives of Orthopaedic and Traumatic Surgery. 1982;100:135-137.
Dempster W.T. Mechanisms of shoulder movement. Archives of Physics in Medicine and Rehabilitation. 1965;46:49-70.
Dessaur W.A., Magarey M.E. Diagnostic accuracy of clinical tests for superior labral anterior posterior lesions: as systematic review. Journal of Orthopaedic and Sports Physical Therapy. 2008;38(6):341-352.
Dias J.J., Gregg P.J. Acromioclavicular joint injuries in sport. Sports Medicine. 1991;11:125-132.
Dias J.J., Steingold R.F., Richardson R.A., Tesfayohannes B., Gregg P.J. The conservative treatment of acromioclavicular dislocation: review after five years. Journal of Bone and Joint Surgery. 1987;69B:719-722.
Dodson C.C., Altchek D.W. SLAP lesions: An update on recognition and treatment. Journal of Orthopaedic and Sports Physical Therapy. 2009;39(2):71-80.
Ejeskar A. Coracoclavicular wiring for acromioclavicular joint dislocation: a ten year follow-up study. Acta Orthopaedica Scandinavica. 1974;45:652-661.
Fallon J., Blevins F.T., Vogel K., Trotter J. Functional morphology of the supraspinatus tendon. Journal of Orthopaedic Research. 2002;20(5):920-926.
Ferrari D.A. Capsular ligaments of the shoulder: anatomical and functional study of the anterior superior capsule. American Journal of Sports Medicine. 1990;18:20.
Fleisig G.S., Dillman C.J., Andrews J.R. Biomechanics of the shoulder during throwing. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. Edinburgh: Churchill Livingstone, 1994.
Friedmann E. Rupture of the distal biceps tendon. Report on 13 cases. Journal of the American Medical Association. 1963;184:60-63.
Fritz R.C., Helms C.A., Steinbach L.S., Genant H.K. Suprascapular nerve entrapment: evaluation with MR imaging. Radiology. 1992;182:437-444.
Fukuda K., Craig E.V., An K., Cofield R.H., Chao E.Y.S. Biomechanical study of the ligamentous system of the acromioclavicular joint. Journal of Bone and Joint Surgery. 1986;68A:434-439.
Gagey O., Hue E. Mechanics of the deltoid muscle. Clinical Orthopedics. 2000;375:250-257.
Gagey O., Bonfait H., Gillot C. Anatomic basis of ligamentous control of elevation of the shoulder. Surgical and Radiological Anatomy. 1987;9:19.
Garrick J.G., Webb D.R. Sports Injuries: Diagnosis and Management. Philadelphia: W.B. Saunders; 1990.
Gerscovich E.O., Greenspan A. Magnetic resonance imaging in the diagnosis of suprascapular nerve syndrome. Canadian Association of Radiologists Journal. 1993;44:307-309.
Gibson J. Shoulder instability—assessment of shoulder instability. Sportex Medicine. 2005:15-17.
Gibson J., Elphinston J. Shoulder instability—treatment and rehabilitation of shoulder instability. Sportex Medicine. 2005:18-21.
Gill T.J., McIrvin E., Kocher M.S., et al. The relative importance of acromial morphology and age with respect to rotator cuff pathology. Journal of Shoulder and Elbow Surgery. 2002;11(4):327-330.
Gleason P.D., Beall D., Sanders T., et al. The transverse humeral ligament: a separate anatomical structure or a continuation of the osseous attachment of the rotator cuff? American Journal of Sports Medicine. 2006;34(1):72-77.
Griggs S.M., Ahn A., Green A. Idiopathic adhesive capsulitis: a prospective functional outcome of non-operative treatment. Journal of Bone and Joint Surgery. 2000;82:1398-1407.
Gunn C.C. Treatment of Chronic Pain, 2nd edn. Edinburgh: Churchill Livingstone; 1996.
Gurd F.B. The treatment of complete dislocation of the outer end of the clavicle: a hitherto undescribed operation. Annals of Surgery. 1941;113:1041.
Haahr J.P., Andersen J.H. Exercises may be as efficient as subacromial decompression in patients with subacromial stage II impingement: 4–8-years’ follow-up in a prospective, randomized study. Scandinavian Journal of Rheumatology. 2006;35(3):224-228.
Halbach J.W., Tank R.T. The shoulder. In Gould J.A., editor: Orthopaedic and Sports Physical Therapy, 2nd edn, St Louis: C.V. Mosby, 1990.
Hawkins R.J., Hobeika P.E. Impingement syndrome in the athletic shoulder. Clinics in Sports Medicine. 1983;2:391.
Hertling D., Kessler R.M. Management of Common Musculoskeletal Disorders. Philadelphia: J.B. Lippincott; 1990.
Hunter M.B., Shybut G.T., Nuber G. The effect of anabolic steroid hormones on the mechanical properties of tendons and ligaments. Transactions of the Orthopaedic Research Society. 1986;11:240.
Kamkar A., Irrang J.J., Whitney S.L. Nonoperative management of secondary shoulder impingement syndrome. Journal of Orthopaedic and Sports Physiotherapy. 1993;17(5):212-224.
Keirns M.A. Conservative management of shoulder impingement. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. New York: Churchill Livingstone, 1994.
Kretzler H.H., Richardson A.B. Rupture of the pectoralis major muscle. American Journal of Sports Medicine. 1989;17:453-458.
Kunichi A., Torisu T. Muscle belly tear of the triceps. American Journal of Sports Medicine. 1984;12(6):485.
Lancaster S., Horowitz M., Alonso J. Complete acromioclavicular separations: a comparison of operative methods. Clinical Orthopaedics and Related Research. 1987;216:80-88.
Larsen E., Bjerg-Nielsen A., Christensen P. Conservative or surgical treatment of acromioclavicular dislocation: a prospective controlled randomised study. Journal of Bone and Joint Surgery. 1986;68A:552-555.
Lemak L.J. Calcifying tendonitis. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. Edinburgh: Churchill Livingstone, 1994.
Lephart S.M., Henry T.J. Restoration of proprioception and neuromuscular control of the unstable shoulder. In: Lephart S.M., Fu F.H., editors. Proprioception and Neuromuscular Control in Joint Stability. Champaign, Illinois: Human Kinetics, 2000.
Lephart S.M., Warner J.P., Borsa P.A., Fu F.H. Proprioception of the shoulder in normal, unstable, and surgical individuals. Journal of Shoulder and Elbow Surgery. 1994;3(4):116-119.
Lewis J.S. Rotator cuff tendinopathy. Br J Sports Med. 2009;43:236-241.
Lewis A., Kitamura T., Bayley J.L. The classification of shoulder instability. Current Orthopaedics. 2004;18:97-108.
Loew M., Heichel T., Lehner B. Intraarticular lesions in primary frozen shoulder after manipulation under general anesthesia. Journal of Shoulder and Elbow Surgery. 2005;14:16-21.
Lovinger A., Mangus B.C., Ingersoll C.D. Shoulder positioning for optimal treatment effects. Athletic Training, Journal of the National Athletic Training Association. 1991;26:81-82.
Lucas D.B. Biomechanics of the shoulder joint. Archives of Surgery. 1973;107:425-432.
Ludewig P.M., Cook T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Physical Therapy. 2000;80(3):276-291.
Lundberg B.J., Nilsson B.E. Osteopenia in the frozen shoulder. Clinical Orthopaedics and Related Research. 1968;60:187.
Macdonald R. Taping Techniques: Principles and Practice. Oxford: Butterworth-Heinemann; 1994.
Magee D.J. Orthopaedic Physical Assessment, 4th edn. Philadelphia: Saunders; 2002.
Magnusson S.P., Narici M.V., Maganaris C.N., Kjaer M. Human tendon behaviour and adaptation in vivo. Journal of Physiology. 2008;586(1):71-81.
Maitland G.D. Peripheral Manipulation, 3rd edn. Oxford: Butterworth-Heinemann; 1991.
Malone Malone, A.A., 2004. Muscle patterning instability—classification and prevalence in a tertiary referral shoulder service. Proceedings of the International Congress of Shoulder Surgery, Washington DC.
Margarey M.E., Jones M.A. Dynamic evaluation and early management of altered motor control around the shoulder complex. Manual Therapy. 2003;8(4):195-206.
Mariani E.M., Cofield R.H. The tendon of the long head of biceps brachii: instability, tendinitis, and rupture. Advances in Orthopaedic Surgery. 1988;11:262.
Matsen F.A., Harryman D.T., Sidles J.A. Mechanics of glenohumeral instability. Clinical Sports Medicine. 1991;10(4):783-788.
McAuliffe T.B., Pangayatselvan T., Baylet I. Failed surgery for recurrent anterior dislocation of the shoulder. Causes and management Journal of Bone and Joint Surgery. 1988;70B(5):798-801.
McConnell J. The Challenge of the Problem Shoulder. London: Course notes; 1992.
McNab I. Rotator cuff tendinitis. Annals of the Royal College of Surgeons of England. 1973;53:271.
Melzer C., Wallny T., Wirth C.J., Hoffman S. Frozen shoulder: treatment and results. Archives of Orthopaedic Trauma Surgery. 1995;114:87-91.
Morrey B.F., Askew L.J., An K.N., Dobyns J.H. Rupture of the distal tendon of the biceps brachii: a biomechanical study. Journal of Bone and Joint Surgery. 1985;67A:418-421.
Morrison D.S., Bigliani L.U. The clinical significance of variations in acromial morphology. Orthopaedic Transactions. 1987;11:234.
Moseley H.F., Goldie I. The arterial pattern of the rotator cuff of the shoulder. Journal of Bone and Joint Surgery. 1963;45B:780.
Mullen F., Slade S., Briggs C. Bony and capsular determinants of glenohumeral locking and quadrant positions. Australian Journal of Physiotherapy. 1989;35:202-208.
Mulligan B.R. Manual Therapy. Wellington, New Zealand: Plane View Services; 1989.
Nakajima T., Rokuuma N., Hamada K. Histological and biomechanical characteristics of the supraspinatus tendon. Journal of Shoulder and Elbow Surgery. 1994;3:79-87.
Neer C. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. Journal of Bone and Joint Surgery. 1972;54A:41-50.
Neviaser J.S. Adhesive capsulitis of the shoulder. Journal of Bone and Joint Surgery. 1945;27:211.
Norkin C.C., Levangie P.K. Joint Structure and Function, 2nd edn. Philadelphia: F.A. Davis; 1992.
Norris C.M. Weight Training. Physiotools, Helsinki: CD-ROM Package; 1996.
O’Brian S.J., Pagnani M.J., Fealy S., et al. The active compression test: a new and effective test for diagnosing labral tears and acromioclavicular joint abnormality. American Journal of Sports Medicine. 1998;26:610-613.
O’Brian S.J., Neves M.C., Arnoczky S.P., et al. The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. American Journal of Sports Medicine. 1990;18:451.
O’Donoghue D.H. Subluxing biceps tendon in the athlete. Journal of Sports Medicine. 1973;1:20.
O’Donoghue D.H. Treatment of Injuries to Athletes. Philadelphia: W.B. Saunders; 1976.
Ott J.W., Clancy W.G., Wilk K.E. Soft tissue injuries of the shoulder. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. Edinburgh: Churchill Livingstone, 1994.
Ozaki J., Nakagawa Y., Sakurai G., Tamia S. Recalcitrant chronic adhesive capsulitis of the shoulder. Journal of Bone and Joint Surgery. 1989;71A:1511.
Palastanga N., Field D., Soames R. Anatomy and Human Movement. Oxford: Heinemann Medical; 1989.
Palastanga N., Field D., Soames R. Anatomy and Human Movement, 2nd edition. Oxford: Butterworth-Heinemann; 1994.
Palastanga N., Field D., Soames R. Anatomy and Human Movement—Structure and Function 5th ed. Edinburgh: Butterworth-Heinemann; 2006.
Park G.Y., Park J.H., Bae J.H. Structural changes in the acromioclavicular joint measured by ultrasonography during provocative tests. Clinical Anatomy. 2009;22(5):580-585.
Paterson C. Scapula dyskinesia and shoulder impingement—what is the evidence? Sportex Medicine. 2008;36(Apr):14-17.
Peat M., Culham E. Functional anatomy of the shoulder complex. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. Edinburgh: Churchill Livingstone, 1994.
Percy E.C., Birbrager D., Pitt M.J. Snapping scapula: a review of the literature and presentation of 14 patients. Canadian Journal of Surgery. 1988;31:248-250.
Perry J., Glousman R.E. Biomechanics of throwing. In Nicholas J.A., Hershman E.B., editors: The Upper Extremity in Sports Medicine, 2nd edn, St Louis: C.V. Mosby, 1995.
Petersson C.J. Spontaneous medial dislocation of the tendon of the long biceps brachii: an anatomic study of prevalence and pathomechanics. Clinical Orthopaedica and Related Research. 1986;211:244.
Petersson C.J., Redlund-Johnell I. The subacromial space in normal shoulder radiographs. Acta Orthopaedica Scandinavica. 1984;55:57.
Petty N.J., Moore A.P. Neuromusculoskeletal Examination and Assessment, 2nd edn. Edinburgh: Churchill Livingstone; 2001.
Rathbun J., Macnab I. The microvascular pattern of the rotator cuff. Journal of Bone and Joint Surgery. 1970;52B:540-553.
Reeves B. Arthrographic changes in frozen shoulder and post traumatic stiff shoulders. Proceedings of the Royal Society of Medicine. 1966;59:827.
Reid D.C. Sports Injury Assessment and Rehabilitation. Edinburgh: Churchill Livingstone; 1992.
Reid D.C., Kushner S. The elbow region. In: Donatelli R., Wooden M.J., editors. Orthopaedic Physical Therapy. Edinburgh: Churchill Livingstone, 1989.
Reut R.C., Bach B.R., Johnson C. Pectoralis major rupture: diagnosing and treating a weight-training injury. Physician and Sports Medicine. 1991;19(3):89-96.
Rockwood C.A., Odor J.M. Spontaneous atraumatic subluxation of the sternoclavicular joint. Journal of Bone and Joint Surgery. 1989;71A:1280-1288.
Roi G.S., Respizzi S., Dworzak F. Partial rupture of the pectoralis major muscle in athletes. International Journal of Sports Medicine. 1990;11(1):85-87.
Rothman R.H., Parkes W.W. The vascular anatomy of the rotator cuff. Clinical Orthopaedics and Related Research. 1965;41:176.
Shaffer B., Tibone J.E., Kerlan R.K. Frozen shoulder: a long term follow up. Journal of Bone and Joint Surgery. 1992;74:738-746.
Sheridan M.A., Hannafin J.A. Upper extremity: emphasis on frozen shoulder Orthopedic Clinics of North. America. 2006:531-539.
Simmonds F.A. Shoulder pain with particular reference to the frozen shoulder. Journal of Bone and Joint Surgery. 1949;31B:426.
Simons D.G., Travell J.G., Simons L.S. 2nd edn Travell and Simons’ Myofascial Pain and Dysfunction vol. 1 Philadelphia: Lippincott, Williams and Wilkins, 1999.
Slatis P., Alato K. Medial dislocation of the tendon of the long head of biceps brachii. Acta Orthopaedica Scandinavica. 1979;50:73.
Smith R.L., Brunolli J. Shoulder kinesthesia after anterior glenohumeral joint dislocation. Physical Therapy. 1989;69:106-112.
Taft T.N., Wilson F.C., Oglesby J.W. Dislocation of the acromioclavicular joint: an end-result study. Journal of Bone and Joint Surgery. 1987;69A:1045-1051.
Thein L.A. Impingement syndrome and its conservative management. Journal of Orthopaedic and Sports Physical Therapy. 1989;11(5):183-191.
Tibone J., Sellers R., Tonino P. Strength testing after third degree acromioclavicular dislocations. American Journal of Sports Medicine. 1992;20:328-331.
Ticker J.B., Bigliani L.U. Impingement pathology of the rotator cuff. In: Andrews J.R., Wilk K.E., editors. The Athlete’s Shoulder. Edinburgh: Churchill Livingstone, 1994.
Torstensen T.A., Meen H.D., Stiris M. The effect of medical exercise therapy on a patient with chronic supraspinatus tendinitis. Diagnostic ultrasound-tissue regeneration: a case study. Journal of Orthopaedic and Sports Physical Therapy. 1994;20:319-327.
Uitvlugt G., Detrisac D.A., Johnson L.L. The pathology of the frozen shoulder: an arthroscopic perspective. Arthroscopy. 1988;4:137.
Van der Windt D., Koes B. Are corticosteroid injections as effective as physiotherapy for the treatment of a painful shoulder? In: MacAuley D., Best T, editors. Evidence Based Sports Medicine. London: BMJ Books, 2002.
Vermeulen H.M., Obermann W.M., Burger B.J., Kok G.J. End range mobilisation techniques in adhesive capsulitis of the shoulder joint. Physical Therapy. 2000;80:1204-1213.
Walton D.M., Sadi J. Identifying SLAP lesions: a meta analysis of clinical tests and exercise in clinical reasoning. Physical Therapy in Sport. 2008;9(4):167-176.
Warwick R., Williams P.L. Gray’s Anatomy, 35th edn. Harlow: Longman; 1973.
Werner A., Mueller T., Boehm D., Gohlke F. The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval. A histoanatomic study. American Journal of Sports Medicine. 2000;28(1):28-31.
Wiley A.M. Arthroscopic appearance of frozen shoulder. Arthroscopy. 1991;7:138.
Wilk K.E., Arrigo C. Current concepts in the rehabilitation of the athletic shoulder. Journal of Orthopaedic and Sports Physical Therapy. 1993;18(1):365-378.
Wilk K.E., Voight M.L., Keirns M.A., Gambetta V., Andrews J.R., Dillman C.J. Stretch shortening drills for the upper extremities: theory and clinical application. Journal of Orthopaedic and Sports Physical Therapy. 1993;17(5):225-239.
Wolfe S.W., Wickiewicz T.L., Cavanaugh J.T. Ruptures of the pectoralis major muscle: an anatomic and clinical analysis. American Journal of Sports Medicine. 1992;20:587-593.
Yergason R.M. Supination sign. Journal of Bone and Joint Surgery. 1931;13A:160.
Zachazewski J.E., Magee D.J., Quillen W.S. Athletic Injuries and Rehabilitation. Philadelphia: W.B.Saunders; 1996.