9 NMT in clinical use
Wherever possible, statements made in this text up to this point have carried citation references. Those statements not referenced represent the personal opinion of the author, based on 45 years of clinical experience as an osteopathic and naturopathic practitioner, in both private and National Health Service settings, in office practice, residential clinic and academic settings, in Britain, Greece and the USA.
It is therefore suggested that any ‘unsubstantiated’ (by citations) statements are seen as demanding personal evaluation, by the reader, before being used clinically.
Contextual thinking and synchronicity
Contextual thinking is a valuable approach when confronted by symptoms that are other than obvious (sprained ankle, whiplash injury, etc.). The tendency in clinical practice to consider symptoms in a linear manner, in which cause and effect are plotted almost mathematically, is often flawed. It is possible to learn to see the patient’s symptoms in terms of the tip of an iceberg. As is obvious, the bulk of the iceberg is invisible, as are the interacting systemic, constitutional, inherited and acquired, biochemical, biomechanical and psychosocial influences operating within individual patients. And just as the iceberg is influenced by the ocean in which it floats, so the patient functions in a physical and psychological environment in which unseen and uncontrollable forces operate. Unless we take these additional factors into account, we are doomed to see symptoms as arising from simplistic backgrounds, which in the case of chronic problems is seldom the case.
Another way of expressing the idea of context, is to speak of synchronicity. There are linear and spatial ways of interpreting what happens in life in general, and to the body in particular. Cause and effect represent the way many people in the West understand the relationships between events (causality). One thing causes, or is caused – or is at least strongly influenced – by another.
A different way of viewing two events is to see them as being part of a complex continuum, each being part of the same (larger) process, but with neither dependent on the other, linked by a synchronistic connective principle. The words synchronicity or ‘simultaneity’ have been used to describe this way of viewing patterns and events. Such spatial thinking may represent the most effective way of evaluating health problems, avoiding simplistic cause and effect approaches (Jung 1973).
Three examples of contextual thinking
1 Hyperventilation and anxiety: which ‘causes’ which?
Hyperventilation is commonly associated with anxiety. Therefore, if we think in simple terms of cause and effect, we might assume that hyperventilation ‘causes’ anxiety. However, anxiety commonly leads to hyperventilation; therefore, again, if thinking simplistically, we might assume that anxiety ‘causes’ hyperventilation. Or, if thinking more contextually, we might observe (more accurately) that anxiety and hyperventilation not only ‘feed’ each other, but can be triggered and/or aggravated by – for example: low blood sugar levels (Brostoff 1992), increased progesterone levels in the post-luteal phase of the menstrual cycle (Cimino 2000), sympathetic arousal (‘stress’) and adrenal stimulation (Nixon & Andrews 1996), metabolic acidosis, for example in pregnancy (Slatkovska et al 2006), climatic conditions, altitude, emotional stimuli, allergic reactions (Brostoff 1992), extreme fatigue, and so on. Therefore, we might conclude that anxiety and hyperventilation are part of a continuum, involving all or any of these (and numerous other) associated aetiological factors, interacting with the unique genetic and acquired biochemical, biomechanical and psychological individuality of the person affected. And we might reflect that treatment that takes account of the broader context is more likely to succeed than a simple, linear, ‘cause and effect’ assessment.
2 Possible ‘usefulness’ of trigger points
Clinical experience suggests that myofascial trigger points may, at times, form part of a functional system for sustaining tension, where this is required by the body – for instance in posturally compromised tissues, as ‘repositioners’ (e.g. for the mandible due to forward head posture), or for sustaining tension across the sacroiliac joint when it is unstable, by strategically increasing hamstring tone (Vleeming et al 1997). In such a situation the body is doing exactly what it was set up to do, as changes occur leading to trigger point development. Simons et al (1999) have shown that, in the absence of adequate levels of adenosine triphosphate (ATP), and in the presence of calcium, the actin and myosin elements of muscles are designed to lock in a shortened position. Trigger points function effectively in the absence of ATP (therefore displaying an economy of resources), and are often strategically located in tissues that are straining to accommodate dysfunctional posture, or habits of use. And trigger points often clear up spontaneously when the immediate causes (and/or other stressors such as dietary imbalance, breathing dysfunction, dehydration, etc.) are corrected (Chaitow & DeLany 2002).
Trigger points also appear to demonstrate a built-in, silent (latent) and non-silent (active) alarm mechanism, when the structures with which they are associated are being abused. Therefore, to release trigger points without regard to correcting the underlying causes (the abuse), to which they are responding, may result in a less than ideal outcome, not least of which could be a rapid, or chronic, return of the trigger point activity. Rather than always being seen as dysfunctional entities, trigger points might be considered as low-energy-consuming contractile devices, established by the absence of available ATP, to maintain a structural or localized tensional element, for immediate or long-term adaptation/compensation purposes, until no longer required. Additionally they may be seen as alarm signals when tissues are being overloaded and abused. In this way of thinking, it is the individual’s posture, patterns of daily use, or lifestyle, that are dysfunctional, not the tissues housing the trigger point, which may be doing exactly what they were designed to do. When this is true – and when we can recognize that it is – it is the context from which trigger points emerge that requires attention, not the trigger points.
Of course there are times – arguably in the majority of cases – when trigger points remain active well past their possible usefulness as stabilizing agents, or when they exist as historical remnants of previous overuse or trauma. In such instances they are nuisances, and may be disturbing normal function, and so require appropriate deactivation. Even when trigger points are potentially useful as stabilizers but are nevertheless causing pain, if more appropriate stabilization can be achieved, via (say) improved core stability, then deactivation – manually or by other means – would be seen to be appropriate.
3 Assessment of sacroiliac dysfunction
Lee (2002) reports that Hungerford & Gilleard (1998) have shown that normal individuals, performing a one-legged, standing, hip flexion (‘stork’) test, vary their motor control strategy each time they perform the test, implying that different muscles can be used to perform the same osteokinematic motion. This will vary the amount of compression each time they lift the leg, and thus vary the range of motion. Lee (2002) has written:
Unless trials are repeated and motions averaged, reliability is impossible – not because the tester can’t feel what’s happening, but because the subject keeps changing from moment to moment … Unless the specific muscle activation pattern is noted during whatever range of motion test (active or passive) is being evaluated for reliability – there is no way of knowing what amount of compression the SIJ is under (at that moment) and therefore what the available range of motion should be.
As if this is not enough to create hesitation as to the validity of such tests, a range of other possible influences has been noted. For example, what if:
• the patient’s head was slightly turned toward the side being tested, causing increased tension in the hip extensors (i.e. hamstrings) (Murphy 2000)?
• the patient’s eyes were turned one way or the other, or were looking slightly up or down, changing markedly the tone in hip flexors, extensors and rotators (Janda 1988, Lewit 1999)?
• the patient’s suboccipital muscles had recently been stretched, altering tone in the extensors of the leg (Pollard & Ward 1997)?
• the patient was anxious, hyperventilating (Garland 1994), suffering an allergic reaction (Randolph 1976), or had fallen arches (Myers 2001)?
There are multiple influences, only some of which can be controlled, during tests of this sort, suggesting that clinical reasoning as to what single tests ‘mean’ is essential. A single test result cannot define dysfunction, offering at best a shadowy indication, and becoming more relevant only when other assessment findings, and the patient’s symptom picture and history are added. Assessment is therefore a spatial exercise, not a linear one, seeking synchronous pieces of evidence that, together, lead to a working hypothesis as to what is happening – and what to do.
Conclusion
Hopefully these three examples, hyperventilation, trigger points and sacroiliac joint assessment, offer sufficient evidence to point towards a need to think contextually, to look for synchronicity, and to be cautious regarding linear thinking, especially when dealing with the complexity of the human body.
Evaluation before treatment
If therapeutic intervention is to be structured and organized, and something other than hit-and-miss, there is an absolute requirement for sound evaluation and assessment as to the causes, extent and possible influences on other areas and tissues, of patterns of pain and restriction, such as myofascial trigger points, locally traumatized areas, shortened and/or weakened muscles, joint restrictions and/or general/systemic factors (such as exist in arthritic conditions).
As discussed above, the contexts in which symptoms exist, and out of which they emerge, are of profound importance in arriving at a stage where a programme of intervention and therapeutic modification can be formulated.
NMT provides one such diagnostic/assessment tool and also offers, by switching from its assessment to its actively therapeutic mode, a means whereby precisely focused and modulated degrees of force can be directed towards influencing restricted tissues, directly or reflexively. Myofascial release techniques, as well as ischaemic compression (osteopathic inhibitory technique), can be applied to precise targets via the contacting thumb or finger in NMT.
Perhaps NMT’s greatest usefulness in assessment relates to the opportunity it offers for the identification of local soft tissue dysfunction in a gentle, non-invasive manner.
In the USA, as well as in the UK, the focus of many therapists using NMT is primarily on myofascial trigger points (and the often widespread musculoskeletal and other dysfunctional patterns that produce them). To use NMT to its full advantage, it is useful to have a clear understanding of the process of facilitation that can occur paraspinally, or locally, in muscle and fascia (trigger points), as described in detail in Chapter 3.
By learning how to use NMT diagnostically and therapeutically, a good deal of information can be obtained regarding the patterns of dysfunction that are operating.
It is important to stress, once more, that NMT may be used in both a diagnostic mode and a therapeutic mode, and that to some extent these overlap, and may be carried out simultaneously. Having identified the structures and tissues that require greater attention, NMT is available as a tool with which to make contact and give direct localized treatment to areas that are contracted or tightened (Fernandez de las Penas et al 2005).
Specific associated and complementary techniques exist to deal with reflex activity, as is noted in trigger points (Fryer & Hodgson 2005). Muscle energy technique methods, as described by Lewit (1999), and elaborations on these derived from a variety of sources, provide a further array of techniques that can be brought into operation, depending on the particular indications. Many of these associated techniques were described in Chapter 8.
What about joints?
Soft tissue manipulation, which includes positional release methods (‘strain/counterstrain’), NMT and MET, is capable of normalizing a great many joint problems, without recourse to active manipulative effort (Schenk 1994, Wilson et al 2003, Speicher et al 2004). MET and NMT are symbiotic, and it is possible to achieve more by combining their repertoire of useful techniques than either can achieve individually. By adding the knowledge of suitable techniques by which to influence reflex activity, demonstrated by the presence of localized areas of soft tissue dysfunction (trigger points, Chapman’s points, localized fibrosis, etc.), as well as by using the tender points described by Jones, in gentle functional techniques, the scope of soft tissue manipulation methods should become apparent.
Employment of these approaches does not necessarily preclude the need for active joint mobilization and/or manipulation, in correcting restriction, but can make for a lesser need to use high-velocity thrusts, or long lever techniques, while making such manipulation simpler and far less likely to traumatize the local tissues, or the patient. By combining MET and NMT, some degree of the potential problem of avoiding tissue damage is likely to be solved. NMT, applied to a region containing fibrotic change, will allow for subsequent use of ‘normal’ MET, or of an isolytic contraction, with less discomfort or likelihood of microtrauma (see Ch. 8).
Are some musculoskeletal problems best left untreated?
The enormous privilege that the patient allows in permitting the practitioner to make physical contact also grants a degree of ‘power’ to the practitioner. Defences are lowered, and the patient is likely to be amenable to discussing areas of their emotions and thoughts, that they might resist in other situations. This presents opportunities for therapeutic intervention on levels other than the physical. The practitioner should be aware of the opportunity to exploit the potent ‘placebo’ effect that such situations allow. Suggestions, and positive guidance, can have powerful influences on the patient, and so care should be exercised, and diligent application of therapeutic techniques undertaken, knowing that the recipient is commonly receptive and highly suggestible (Pollo & Benedetti 2008).
When considering treatment of soft tissue changes that relate to an emotional or psychogenic background, it is important to realize the need for an adequate ability on the part of the practitioner/therapist to handle any emotional repercussions resulting from ‘releasing’ (or attempting to release) the soft tissue manifestations of emotional turmoil, as well as there being a need to have an adequate referral system in place to support the patient in times of crisis (Field et al 2005, Loga 2008).
If the patient is not capable of processing whatever emotional baggage is attached to a particular pattern of soft tissue dysfunction, then it is probably best left intact, until the patient is ready and equipped to process the issues that are submerged in the soma (Mancuso et al 2004).
A scenario is conceivable in which a patient with obvious musculoskeletal dysfunction, but without obvious mento-emotional problems, could be left in a fragile and vulnerable state following apparently appropriate bodywork. The oft-quoted phenomenon of ‘emotional release’, which may occur during or following treatment, is something therapists could usefully reflect upon and possibly re-evaluate. Just how beneficial – or how dangerous – is such a reaction without further support, such as counselling or psychotherapy?
Additionally, there are times when apparently purely physical symptoms, such as active trigger points in a tight hamstring, as in the example given earlier in this chapter, may best be left untreated until underlying, contextual, causes have been evaluated and dealt with.
A focus on trigger points
Travell & Simons (1983) have demonstrated the clear connection between myofascial trigger point activity and a wide range of pain problems and sympathetic nervous system aberrations. Wall & Melzack confirm that there are few chronic pain problems that do not have myofascial trigger point activity as a component, with these acting, in many instances, as prime maintaining factors of the pain (Melzack & Wall 1988, Wall & Melzack 1989, Fernandez de las Penas et al 2007).
Active trigger points (and other non-referring pain points), commonly lie in muscles that have been stressed in a variety of ways, including postural imbalances (Barlow 1959, Goldthwaite 1949, Simons et al 1999), congenital factors such as warping of fascia via cranial distortions (Upledger 1983), short leg problems, small hemipelvis (Travell & Simons 1992), occupational or leisure overuse patterns (Rolf 1977), emotional states affecting soft tissues (Latey 1986), referred/reflex involvement of the viscera producing facilitated segments paraspinally (Beal 1983, Korr 1977), and trauma.
The repercussions of trigger point activity go far beyond simple musculoskeletal pain, however distressing that may be. Take, for example, the involvement of trigger points in cases of hyperventilation, chronic fatigue and apparent pelvic inflammatory disease. Trigger point activity is particularly prevalent in the muscles of the neck/shoulder region, which also act as accessory breathing muscles (scalenes, upper trapezius, etc.). In situations of increased anxiety the incidence of borderline or frank hyperventilation is frequent (Bass & Gardner 1985) and may be associated with chronic fatigue (Nixon & Andrews 1996). Clinically these muscles palpate as tense, and often fibrotic, with active trigger points being common (Garland 1994, Roll & Theorell 1987). Successful breathing retraining and normalization of diminished energy levels, seem to be accelerated and enhanced, following initial normalization of the functional integrity of the involved muscles (Chaitow et al 2002).
Trigger points and pelvic pain
Slocumb (1984) demonstrated that, in a large proportion of chronic pelvic pain problems in women, destined for surgical intervention, the prime cause of pain involves trigger point activity in muscles of the lower abdomen, perineum, inner thigh and even on the walls of the vagina:
The search for common pathological processes, such as endometriosis, active inflammation, or pelvic adhesions is a major objective in assessing the patient with chronic pelvic pain. However, the frustration of finding normal pelvic structures too often results in the conviction that psychogenic causes might account for the pain. What is probably the most alarming aspect of the inadequacy of gynecologic management of chronic pelvic pain is the frequent recourse, by physicians, to operative exploration and removal of pelvic structures for normal physiologic variations … As a result of concentrating patients with pelvic pain in a single clinic I have identified a neurological syndrome that can be shown to account for the majority of those patients with chronic abdominal pain … Several unusual and unexplained phenomena were repeatedly observed. First, the same pain sensation was reproduced by pressure over localized points in several different tissues seemingly anatomically unrelated. These hyperpathic points are consistent with the term trigger points described by Travell and Simons and appear to cause referred pain symptoms as well as sharp pain.
Slocumb describes how the following areas can all produce the identical referred pelvic pain:
1. Pinching the skin over the lower abdominal wall
2. Single-finger pressure in one abdominal wall location
3. Single-finger pressure on tissue overlying the pubic bone
4. Lateral pressure with single finger over one or both levator muscles
5. Single-finger or cotton-tip applicator pressure lateral to the cervix
6. Single-finger or cotton-tip applicator pressure over vaginal cuff scar tissue more than 3 months after hysterectomy
Slocumb demonstrated, in one research study involving 130 patients, that he was able to remove chronic pelvic pain in nearly 90% of cases by deactivating such triggers.
The significance of this and other studies is that trigger points are the cause of serious levels of suffering (see Box 7.1 for evidence relating to trigger point influence on the painful symptoms associated with interstitial cystitis and urgency), and that we need to have an array of tools with which to deal with their activities (Weiss 2001). Further discussion on this topic is to be found in Chapter 7, under the sub-heading ‘NMT and chronic pelvic pain dysfunction’.
Local facilitation
According to Korr (1977), a trigger point is a localized area of somatic dysfunction that behaves in a facilitated manner, i.e. it will amplify and be affected by any form of stress imposed on the individual whether this is physical, chemical or emotional. A trigger point is palpable as an indurated, localized, painful entity with a reference (target) area to which pain or other symptoms are referred (Chaitow 1991a).
Muscles housing trigger points can frequently be identified as being unable to achieve their normal resting length, using standard muscle evaluation procedures (Janda 1983). The trigger point itself commonly lies in fibrotic tissue, which has evolved as a result of exposure of the tissues to diverse forms of stress.
Treatment methods
A wide variety of methods have been advocated for treating trigger points, including inhibitory (ischaemic compression) pressure methods (Lief 1989, Nimmo 1966), acupuncture and/or ultrasound (Kleyhans & Aarons 1974), dry needling (Gerwin & Dommerholt 2002), microcurrent (McMakin 2003), chilling and stretching of the muscle in which the trigger lies (Simons et al 1999), procaine or xylocaine injections (Slocumb 1984), active or passive stretching (Lewit 1992) and even surgical excision (Dittrich 1954).
Clinical experience, confirmed by the diligent research of Travell & Simons (1992), has shown that, while all or any of these methods can successfully inhibit trigger point activity in the short term, more is often needed to eliminate the noxious activity of the structure completely.
Common sense, as well as clinical experience, dictates that the next stage of correction of such problems should involve re-education (postural, breathing, relaxation, etc.) or the elimination of factors that contributed to the problem’s evolution. This might well involve ergonomic evaluation of home and workplace, as well as the re-education and rehabilitation methods mentioned above.
Travell & Simons (1992) have also shown that, whatever initial treatment is offered to inhibit the neurological overactivity of the trigger point, the muscle in which it lies has to be made capable of reaching its normal resting length, following such treatment, if the trigger point is to be prevented from rapid reactivation.
In treating trigger points, the method of chilling the offending muscle (housing the trigger) while holding it at stretch in order to achieve this end was advocated by Travell & Simons (1992), whereas Lewit (1999) has espoused the muscle energy method of a physiologically induced post-isometric relaxation (or reciprocal inhibition) response, before passive stretching. Both methods are commonly successful, although a sufficient degree of failure occurs (trigger points may rapidly reactivate, or fail to ‘switch off’ completely) to require investigation of more successful approaches.
One reason for failure may relate to the possibility that the tissues that are being stretched are not the very fibres surrounding the trigger point.
A popular method for achieving tonus release in a muscle, prior to stretching, involves the use of muscle energy techniques, the introduction of an isometric contraction to the affected muscle prior to stretching. See discussion of MET in Chapter 8 (Chaitow 1991b, 2006).
The original use of isometric contractions before stretching was in proprioceptive neuromuscular facilitation (PNF) techniques, which emerged from physical medicine in the early part of the 20th century. In most forms of MET methodology, a partial (not full-strength) isometric contraction is performed before the stretch, in order to preclude tissue damage or stress to the patient and/or therapist, which PNF quite frequently produces (Greenman 1989, Hartman 1985, Fryer & Fossum 2009).
An integrated combination of methods designed to deactivate trigger points effectively, known as integrated neuromuscular inhibition, will be described later in this chapter.
Lief’s approach: general vs specific
Stanley Lief, the prime developer of NMT, employed few specific manipulative techniques. His main concern was to attempt to normalize mobility and function (circulation, drainage, nerve function, etc.) and, to this end, his neuromuscular treatment was often accompanied by no more than general mobilization of the cervical and lumbar areas, together with a degree of ‘springing’ or stretching of the dorsal region. Peter Lief ND DC, son of the primary developer of NMT Stanley Lief, noted: ‘NMT is a type of specific soft tissue treatment which is followed [or accompanied] by a general mobilising articular manipulation’ (Lief 1963).
Criticism of this approach, by ‘specific’ manipulators, should be softened by the fact that this general, ‘constitutional’ treatment approach (some would call it ‘engine wiping’) achieved phenomenal results in terms of improvements in general well-being, and the alleviation of many specific dysfunctional restrictions.
Brian Youngs ND DO, a colleague of both Stanley and Peter Lief, who is – at the time of writing this in 2009 – still in practice in London in his nineties, has written, regarding Lief’s approach, as follows (Youngs 2008):
Usually accompanying this physical approach (NMT) would be recommendations for dietary changes, exercise, breathing re-education, relaxation and short fasting episodes, as appropriate to the individual’s needs. In this way long-term benefit, deriving from the NMT procedures, would be supported and modified by responses resulting from the accompanying nutritional and lifestyle changes.
This approach represented a package of non-specific interventions, designed to impact on total health – a veritable personalized holistic recipe! The physiological effects of the NMT procedures were, in many ways, akin to those resulting from exercise, setting in train improved physiological function (Youngs 1963).
There was an increase of general mobility; head on neck, on shoulders; increased flexion/extension of spinal movements; increased lung capacity – all of which would continue to improve if accompanying exercise advice was adhered to.
Undoubtedly there exist specific spinal and joint problems that demand individual corrective approaches; however, the improvement of the supporting mechanisms (muscles, fascia, ligaments, tendons) via NMT, on its own, or together with general mobilization techniques, offered by soft tissue manipulation, is able frequently to avoid the need for any more specific technique.
Indeed, it is strongly suggested that the ‘adjustment’ of joints, that ignores the soft tissue component, is far more likely to fail (in the sense of symptoms speedily returning), than the Lief method.
Speransky and Selye: common findings
Early 20th century researcher A.D. Speransky (1887–1961) has offered many pertinent concepts that relate directly to therapeutic approaches including all methods of physical treatment. As a result of decades of research into the functioning of the nervous system in relation to health and disease, he observed that: ‘Hence we obtain the rule that only weak degrees of irritation can have a useful significance; strong ones inevitably do damage’ (Speransky 1943).
These words should be locked in the minds of all therapists, of whatever school. The term ‘irritation’ is used by Speransky, and this is of interest, as a little thought will indicate that whatever is being done to a patient, in terms of therapy, involves to a greater or lesser extent an element of stress (or irritation) – stress, in this sense, being defined as any stimulus, pleasant or unpleasant, that calls upon the body to respond, or adapt, in some manner.
Manipulation, acupuncture, pressure techniques, use of heat and cold, hydrotherapy, electrical and mechanical therapies, surgery, and indeed the whole gamut of medications, whether they be drugs or homeopathic dilutions of herbal substances, all call for a response on the part of the body. All are, therefore, to a degree, ‘stress’ factors. Speransky insists that only mild irritants can have a useful role to play in evoking a positive (i.e. healing) response.
Selye shows stress can be helpful
Hans Selye (1976) has come to precisely the same conclusion in his important research into stress. In experiments carried out in his extensive studies, Selye produced subcutaneous blisters in experimental animals by injecting a given volume of air under the skin. This was followed by the insertion of an irritant of some sort. He first demonstrated that the amount of exudate, and the thickness of the sac wall, varied, as one might anticipate, with the strength and concentration of the irritant substance inserted. He followed this by introducing a form of ‘secondary’ stress, such as intense cold, or heat or forced immobilization.
The response of the animals varied greatly.
• In those that had been injected initially with a weak irritant, the stress that was then added seemed to aid the recovery, as evidenced by resolution of the irritated area and inhibition of tissue fibrosis.
• Those animals, however, that had had strong irritants injected into the subcutaneous sacs, responded to the subsequent stress factor by showing an increase in inflammation, widespread necrosis, and often death.
• Selye concluded with these words: ‘This was the crucial experiment, showing that stress can either cure or aggravate a disease, depending upon whether the inflammatory response to a local irritant is necessary or superfluous.’
We now have Speransky’s and Selye’s combined evidence, suggesting that what we do to a patient therapeutically can be beneficial or harmful, and that this to a great extent will depend upon the degree of the irritation involved in the treatment, whatever form it takes.
Speransky’s work further teaches us that Mann’s words are true (see Chapter 4): any part of the surface of the body can be an initiator of a process involving neurological changes, which can be pathological or therapeutic.
The classification of certain points as being trigger points, others as being acupuncture alarm points, and yet others as being neurolymphatic or neurovascular – or any other – points, is merely a matter of convenience. It helps us to make a degree of sense out of the enormous amount of information available to us. It should be obvious that, to a large extent, these points may be interchangeable, for many are patently found in precisely the same position, on different ‘maps’ of points.
Bearing in mind that the distinction between the variously classified points, as discussed in this book, is manmade, we will continue to classify them in these ways as a matter of convenience. It should also be borne in mind that, whenever acupuncture points are mentioned, the availability of these for manual treatment (pressure, chilling, heating, etc.) remains. There is some evidence that needling can achieve particular effects, not available to pressure techniques, but this is equivocal and, for the purposes of soft tissue manipulation, pressure can usually be shown to be as effective as needling, with the one major drawback, that only a limited number of points can be contacted by hand at any one time, compared with the multiple needling that is possible in acupuncture.
Soft tissue adaptation
Selye has described the progression of changes in tissues that are being locally stressed. There is an initial alarm (acute inflammatory) stage, followed by a stage of adaptation or resistance when stress factors are continuous or repetitive, at which time muscular tissue may become progressively fibrotic. If such changes are taking place in muscle that has a postural rather than a phasic function, the muscle will shorten (Janda 1985, Selye 1984).
Such fibrotic tissue, lying in altered (shortened) muscles, cannot simply ‘release’, in order to allow the muscle to achieve its normal resting length, a prerequisite of normalization of trigger point activity (Simons et al 1999).
Along with various forms of stretching (passive, active, MET, PNF, etc.) inhibitory pressure methods are commonly employed in treatment of trigger points. Such pressure technique methods, together with myofascial release and cross-fibre friction, can focus on normalization of indurated, fibrosed soft tissues, as part of neuromuscular therapy methodology (Chaitow 1991b).
Lewit’s ‘functional pathology’ view
We are in the midst of a change in the concepts of manipulative therapy that have far-reaching implications. One of the major changes is the restoration of the soft tissue component to centrestage, rather than the peripheral role to which it has been assigned in the past.
Lewit (1985) discusses aspects of this. He describes the ‘no man’s land’ that lies between neurology, orthopaedics and rheumatology, that, he says, is the home of the vast majority of patients with pain derived from the locomotor system, and in whom no definite pathomorphological changes are found.
He makes the suggestion that these be termed cases of ‘functional pathology of the locomotor system’. These include most of the patients attending osteopathic, chiropractic and physiotherapy practitioners.
The most frequent symptom of individuals involved in this area of dysfunction is pain, that may be derived from reflex changes involving muscle spasm, myofascial trigger points, hyperalgesic skin zones, periosteal pain points, or a wide variety of other sensitive areas that have no obvious pathological origin. It is a major part of the role of NMT to help in both identifying such areas, and to then offer means for normalizing many of the causative aspects of these myriad and mysterious sources of pain and disability.
NMT and sports injuries: Moule’s methods
One practitioner who has achieved outstanding success in applying NMT to athletic injuries of marked severity is osteopath Terry Moule ND DO, son of Tom Moule ND DO, a one-time associate and assistant to Stanley Lief. In the 1970s Terry Moule restored the former captain of England’s soccer team, Gerry Francis, to playing fitness. Surgery to the lumbar spine was the only prospect left for Francis after months of agony under orthopaedic investigation. In desperation, Moule was consulted and within a few weeks Francis was playing again. He remained fit for many years before becoming a professional soccer team manager.
A similar return to full function was achieved in the case of the then captain of England’s rugby football team, Roger Uttley, whose career appeared to be over following a back injury. Treatment, consisting largely of NMT, resulted in Uttley returning to the England squad in its successful 1980 season.
An even more startling result of the application of NMT to a spinal injury involved then world mile and 1500-metre record-holder, Sebastian Coe (now Lord Coe, leading member of Britain’s Olympic Committee). Coe stated in late 1979: ‘Last winter I had a back problem. I was having trouble getting a diagnosis, let alone treatment.’ Within a few treatments, incorporating NMT, he was running again and setting world record times.
Moule has described NMT as follows (personal communication, 2002):
The principle of NMT is that it is of prime importance to treat connective tissue lesions and abnormalities, prior to any manipulative treatment of the bony structures. If more orthodox and less penetrating soft tissue techniques are used, whilst the bony abnormality may be corrected by the application of a specific adjustment, because the soft tissues remain in a similar state to that existing prior to the manipulation, there is a strong likelihood of a recurrence of the lesion. NMT tends to dispense with specific adjustment, for, subsequent to using these specialised soft tissue measures, a generalised mobilisation adjustment will allow the muscular and connective tissues to encourage the bony structures to return to their normal alignment. This may take a little longer to produce relief from discomfort, but in the long run it means that the correction is more permanent and there is less danger of any damage to the muscular and connective tissues from forceful manipulation.
The great advantage of NMT is that it may be applied to any part of the body. It is particularly effective in dealing with problems related to interference with nerve supply; to any form of muscular or connective tissue lesion; to treatment of the abdominal and pelvic organs etc. It is applied mainly by use of the thumb. It may take some years to develop an adequate ‘feel’ in the hands in general and the thumbs in particular, to effectively diagnose and treat lesions. It is the ability to diagnose through the thumb which is so helpful in the rapid and efficient treatment of all forms of dysfunction. Correctly used it precludes a large number of more conventional techniques and saves a considerable amount of time.
NMT has proved invaluable in the treatment of sports injuries, particularly for the diagnostic reasons outlined above and for the fact that it produces a rapid response as compared to orthodox soft tissue and physiotherapy techniques. With sports injuries one of the major problems is to get the player back in action as soon as possible, particularly where the injury is to a professional sportsman. NMT has been used very effectively on a large number of sportsmen and women following all types of sports.
One of the most common injuries one encounters is hamstring problems. These are particularly prevalent amongst footballers, who in many cases develop the injury through overdevelopment of the quadriceps without adequate attention to the maintenance and mobility (i.e. lengthening and stretching) of the hamstrings at the same time. The normal treatment of hamstring injuries is ultra-sonic and massage. These techniques are not particularly rapid and the resultant loss of overall muscle tone, due to the inability of the leg to be used normally, retards a return to normal function. With NMT a lesion can be accurately and rapidly detected and, by the use of deep thumb manipulation, the soft tissue lesion can be dealt with rapidly and effectively. Where there is muscular fibre damage this can be felt and literally ironed out. The effect of the technique is to stimulate circulation in the area thus encouraging healing. Where there is inflammation and swelling the technique promotes drainage and the restoration of normal tone. With acute lesions the technique is unfortunately painful, but where speed is the prime order in recovery this is a small price to pay.
NMT is also beneficial in the treatment of knee lesions, particularly ligamentous problems and the subsequent inflammation in the joint itself. Correct application of NMT to these lesions will improve drainage from the knee and encourages healing to take place far more rapidly than through orthodox techniques. Where there is knee misalignment or dislocation, reduction of spasm is most important as a prerequisite to satisfactory manipulation of the joint. In many cases injury occurs when the legs become anchored due to studs in the boots. If rotation of the trunk is superimposed onto this static lower limb situation the stress imposed on the knee joint is enormous. The application of NMT prior to attempting correction not only makes the correction less painful but ensures that the result is lasting.
NMT is also beneficial in the treatment of prepatellar bursitis, and any synovial inflammatory problems.
A problem which plagues many sportsmen, particularly footballers, basketball players and volleyball players, is pain in the groin and down the inside of the leg. This is commonly treated as a sacroiliac or a lumbar problem when, in many cases, it is due to a lesion of the symphysis-pubis. There are a number of techniques for dealing with problems of this joint but none so dramatically successful as the application of NMT.
The technique’s effectiveness in producing long-term benefits is perhaps best underlined by the results with sportsmen such as Roger Uttley and Gerry Francis, who had both received short-term benefit from manipulative treatment. The application of NMT, without any change in the manipulative techniques being employed, except to make them less specific, produced long-term improvement which allowed a return to active participation in their respective sports. In both cases the main problem was an imbalance in muscle tone with excessive tension causing persistence of the joint dysfunction. The removal of these soft tissue factors restored balance and encouraged the body to return to normal function, as it always tries to do.
In summary, the benefits of NMT in general are
(1) It is a technique which removes causes rather than dealing with symptoms.
(2) It removes the necessity for the bulk of specific manipulation, instead it encourages the body to normalise itself.
From the specific sports injury point of view the main advantage of NMT is that it provides (a) a more rapid recovery rate and (b) a more permanent one.
The author’s own experience confirms the validity of Terry Moule’s comments.
NMT, apart from all the myriad applications discussed in earlier chapters, is the finest soft tissue system for helping to normalize acute and chronic injuries. The successful use of NMT calls for the applied thought of the practitioner. The body usually responds rapidly to the help this technique offers. Its limitations are almost always related to the limitations of the practitioner. Its success is in direct proportion to the dedication and intelligence with which it is applied.
When is NMT useful?
NMT may be universally applied to any patient of any age suffering from any condition. This is not to say that it will be curative, or even of marked value, in all conditions, however, it will be of some diagnostic and therapeutic value in every condition, and of enormous value in others, because no one is free from some degree of dysfunction, affecting the overall efficiency and economy of the body.
In general terms, NMT may be applied to all cases of musculoskeletal dysfunction and mento-emotional dysfunction with benefit. The basic spinal and basic abdominal techniques are used as diagnostic and therapeutic tools in the majority of cases. The more specific techniques, such as psoas, piriformis, tensor fascia lata and abdominal release techniques, are used as and when indicated. A general, full-body NMT treatment may be applied as part of a programme of postural reintegration, or breathing rehabilitation.
In specific terms, NMT is applied as follows:
• All conditions of the spine and conditions that involve the arms or legs would receive general spinal technique as well as consideration of local areas, in the limbs affected.
• Such treatments would be repeated once or twice weekly until a degree of normality had been achieved.
• Other complementary modalities and techniques would and should be used if called for. NMT combines with anything of a supportive nature that is aimed at the restoration of normal function, such as (in appropriate conditions) ultrasound therapy, diathermy, manipulation, etc.
• At the outset, the aim of general treatment is to remove the more obvious areas of contraction and stasis.
• All active trigger points should be neutralized by pressure techniques (see INIT in this chapter), if possible and if appropriate.
• If found stubborn, trigger points can also be treated by chill-and-stretch, MET or infiltration methods.
• As therapy progresses, individual patterns of dysfunction will become clearer, and NMT may need to be applied to spinal, abdominal, intercostal and pelvic areas that are slow to improve.
• Manipulative techniques, of a non-specific type (i.e. mobilization/articulation) are often useful in the normalization of spinal integrity, once the initial soft tissue rigidity or dysfunction has been improved.
• NMT can be applied with infinite gentleness or with robust enthusiasm, as it is possible to use the same techniques, with a marked difference in the degree of force employed. This enables its application to areas of acute sensitivity as well as in fragile (e.g. osteoporotic) and tender areas. As long as the practitioner is thinking about the task in hand and not applying the techniques in a mechanical, repetitive manner, there is no danger of injury or harm.
• If treatment is aimed at the removal of symptoms stemming from trigger points, it is essential to normalize all the structures related to the local area of dysfunction. Simply to neutralize the trigger that is causing, say, a headache will produce short-term benefits. If the particular trigger lies in the trapezius muscle, then not only must the trigger be normalized, and the trapezius muscle treated, but the entire cervical and spinal musculature and soft tissues should receive attention, as should the patterns of posture and use that provoked the tissues to the state where headaches became a natural consequence.
• A general rule should be that no part of the whole should be considered without the whole also being considered. Thus, even if the spinal areas are receiving the main attention of the therapist on any one visit, the muscles of the lower limb and associated structures should be given some consideration to assess their involvement and possible requirements. The treatment of the back, therefore, calls for the treatment of the front, and this calls for the whole to be considered and treated. The condition in the context of the body, and the body in the context of its (total) environment, are the appropriate areas of investigation and care.
• General abdominal technique is useful in all cases of digestive and intestinal dysfunction of a non-pathological nature. NMT is applicable to all cases of respiratory dysfunction. It is also applicable to all genitourinary conditions of a non-pathological nature. NMT applied to the abdomen will reduce many tension states emerging out of mento-emotional backgrounds.
• General abdominal technique improves circulatory efficiency through the pelvis and abdominal regions, and it enhances respiratory function. The reflex points and zones in the spinal area should always be treated prior to thoracic and abdominal technique, as indicated. In a case of spastic constipation, for example, NMT to the lower spinal areas and the use of neurolymphatic points followed by general abdominal technique would be the pattern recommended. This could be followed by specific abdominal release techniques if areas of marked contractions or ‘adhesion’ were elicited during the general treatment. In the author’s experience, such an approach, combined with general health measures such as nutritional reform, together with appropriate exercise and relaxation programmes, will promote a return to normal. If the body is being given those factors required for normality, its self-healing tendency (homeostasis), which is constantly acting, will respond positively to the removal of obstacles to recovery (structural, mechanical, dietary).
• In dealing with tension and stress of psychic origin, it is as well to recall that the mind will not be calm or relaxed as long as neuromuscular tensions are present. In applying any form of psychotherapy, the use of NMT, applied to the spine and abdomen, will increasingly improve the patient’s ability to relax. NMT is not seen as an end in itself in this regard, but to be a catalyst to the removal or easing of the physical component of a vicious circle. In some cases this physical release of tension, especially when applied to the solar plexus, can produce a sudden emotional release in which the patient may cry and sob. The body becomes a solid mass of tensions and contractions for many individuals, with the tensions of life mirrored by layers of muscular ‘armour’. The posture and tensions thus created all carry specific emotional charges and memories and, as the physical components are eased, so the emotional memories and feelings associated with their origins come to the surface. Just how appropriate it is to initiate such ‘releases’ was discussed earlier in this chapter.
• In restoring total structural and postural integrity to the body, it is necessary to apply NMT to all the supporting structures. This might involve the spinal, thoracic and abdominal soft tissues and the limbs, including the feet. NMT and manipulation, where appropriate, will lay the foundations for a return to normal (or to the patient’s individual optimal norm).
• Specific and general exercise, as well as postural re-education, may then follow. It is possible, via such systems as the Alexander technique, to achieve postural and functional normality. With the careful use of NMT and, if necessary, osseous manipulation, such re-education becomes much easier and less arduous. It must be easier to learn to use a machine correctly if that machine is capable of functioning correctly!
• The same applies to breathing retraining. Unless the thoracic and diaphragmatic structures are to some extent made pliable by therapeutic interventions, such as those detailed in earlier chapters, such retraining will of necessity involve struggling against great odds.
• In attempting to achieve postural and functional normality, a fairly long-term view is required. Some practitioners suggest that a series of eight to ten treatment sessions will produce this result. It is the author’s experience that, while the basic groundwork can be done in eight to ten treatments, some chronic cases require weekly or fortnightly treatment for up to a year if they are to achieve optimal improvement. This should be followed by maintenance visits at intervals of not less than 3 months.
• And just as retraining (posture, breathing) without appropriate bodywork is doomed to partial success at best, so bodywork methods that ignore retraining and re-education will have only short-term benefits, since much of any chronic dysfunctional pattern of use will be firmly locked into habitual neural and behavioural patterns.
• Structural and functional changes are interdependent: they follow each other causally as well as therapeutically.
• NMT is universally applicable. It has no side-effects, and combines with all other methods of positive health care. In itself it is capable of improving general function, releasing tension and removing noxious triggers, which may be responsible for myriad symptoms.
NMT has limits, but within the framework of its own area of application its only limits lie in the ability of the practitioner.
 The INIT hypothesis
The INIT hypothesis
When treating myofascial pain, experience suggests that a light isometric contraction, as used in MET procedures, may not activate the particular fibres surrounding the trigger point being treated. Subsequent stretching of the muscle may then not involve critical tissues surrounding and enveloping the myofascial trigger point.
Failure actively to lengthen the muscle fibres in which the trigger is housed may account for the not infrequent recurrence of trigger point activity, in the same site, following treatment. Repetition of the stress factors that produced the active trigger point, in the first place, could undoubtedly also be a factor in such recurrence – which emphasizes the need for re-education (posture, etc.) as a major part of rehabilitation.
A method that achieved precise targeting of these tissues (in terms of tonus release and subsequent stretching) would therefore be advantageous. Clinical experience indicates that, by combining the methods of direct inhibition (pressure mildly applied, continuously or in a ‘make and break’ pattern), along with the concept of strain/counterstrain and MET, a specific targeting of dysfunctional soft tissues is more likely to be achieved.
INIT methods
Method 1 (Fig. 9.1)
It is reasonable to assume, and palpation confirms, that when a trigger point is being palpated by direct finger or thumb pressure, and when the very tissue in which the trigger point lies is positioned in such a way as to take away the pain (entirely or at least to a great extent), the most (dis)stressed fibres in which the trigger point is housed will be in a position of relative ease. See discussion of strain–counterstrain (SCS) in Chapter 8, and Figs 8.21A, B, C.
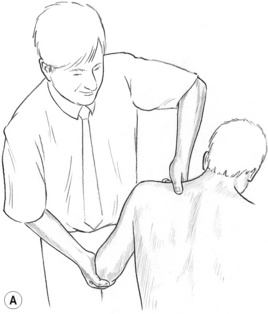
Figure 9.1A First stage of INIT in which a tender/pain/trigger point in supraspinatus is located and compressed ischaemically, either intermittently or persistently.
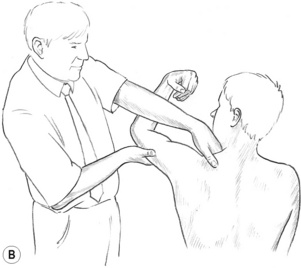
Figure 9.1B The pain is removed from the tender/pain/trigger point by finding a position of ease which is held for at least 20 seconds, after which an isometric contraction is achieved involving the tissues that house the tender/pain/trigger point.
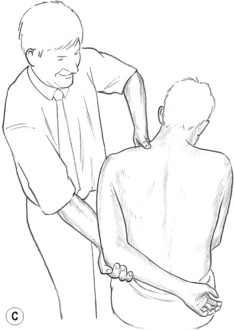
Figure 9.1C After holding the isometric contraction for an appropriate period, the muscle housing the point of local soft tissue dysfunction is stretched. This completes the INIT sequence.
Having been digitally compressed, and then placed into ‘ease’, the trigger point would ideally have already experienced direct inhibitory pressure, and would then have been positioned so that the tissues housing it are relaxed (relatively or completely).
In the INIT sequence, at that time the patient would be asked to induce an isometric contraction into the tissues surrounding the trigger point – and to hold this for 5 to 7 seconds. This contraction would involve the very fibres that had been repositioned to obtain the strain/counterstrain release.
Subsequently there would be a reduction in tone in these tissues, allowing them to be gently stretched (locally), as in any muscle energy procedure (see Chapter 8), with the strong likelihood that the most specifically involved fibres would be stretched.
Subsequently the whole muscle would be stretched, as in any other MET procedure, following a further isometric contraction.
Method 2
There is another possibility – a variation in which, instead of an isometric contraction followed by stretch being commenced following the period of ease (strain/counterstrain position), an isolytic (isotonic eccentric) approach could be used.
The muscle receiving attention is actively contracted by the patient at the same time as a stretch is introduced, resulting in mild trauma to the muscle and the breakdown of fibrous adhesions between it and its interface and within its structures (Mitchell et al 1979).
To introduce this method into trigger point treatment, following the application of inhibitory pressure and SCS release, the patient is asked to contract the muscles around the palpating thumb or finger (lying on the now inhibited pain point) with the request that the contraction should not be a full-strength effort, because the practitioner intends to stretch the tissues gently while the contraction is taking place.
This isotonic eccentric effort – designed to reduce contractions and break down fibrotic tissue – should target precisely the tissues in which the trigger point being treated lies buried. Following the isolytic stretch the tissues could benefit from effleurage and/or hot and cold applications to ease local congestion. An instruction should be given to avoid active use of the area for a day or so.
This method mimics aspects of ‘pin & stretch’/active release treatment, as discussed in Chapter 8.
Summary and comment
The integrated use of inhibitory pressure, strain/counterstrain and a form of muscle energy technique – applied to a trigger point or other area of soft tissue dysfunction involving pain or restriction of range of motion (of soft tissue origin) – is a logical approach, because it has the advantage of allowing precise targeting of the culprit tissues.
Clearly, the use of an isolytic approach as part of this sequence will be more easily achieved in some regions than in others – upper trapezius posing less of a problem in terms of positioning and application, perhaps, than quadratus lumborum.
After either INIT method, it has been found to be useful to instruct the patient to learn a method of gentle activation of the antagonist muscles to the muscle housing the trigger point that has been treated. The patient is asked to reproduce this activity a number of times daily for the days immediately after treatment. This activation of antagonists produces a reciprocal inhibition of the previously hypertonic muscle, and assists in maintaining the deactivation.
Barlow W. Anxiety and muscle tension pain. B J Clin Pract. 13(5), 1959.
Bass C., Gardner W.N. Respiratory and psychiatric abnormalities in chronic symptomatic hyperventilation. Br Med J. 1985;290:1387-1390.
Beal M.C. Palpatory testing for somatic dysfunction in patients with cardiovascular disease. J Am Osteopath Assoc. 1983;82:822-831.
Brostoff J. Complete Guide to Food Allergy. London: Bloomsbury, 1992.
Chaitow L. Neuromuscular technique. Wellingborough, UK: Thorsons, 1983.
Chaitow L. Palpatory literacy. London: Thorsons, 1991.
Chaitow L. Soft tissue manipulation. Vermont: Healing Arts Press, Rochester, 1991.
Chaitow L. INIT in treatment of pain and trigger points. British Journal of Osteopathy XIII. 1994:17-21.
Chaitow L. Muscle energy technique, ed 3. Edinburgh: Churchill Livingstone, 2006.
Chaitow L., DeLany J. Clinical applications of neuromuscular technique. vol 2. Edinburgh: Churchill Livingstone; 2002.
Chaitow L., Bradley D., Gilbert C. Multidisciplinary approaches to breathing pattern disorders. Edinburgh: Churchill Livingstone, 2002.
Cimino R. Does the ovarian cycle influence the pressure-pain threshold of the masticatory muscles in symptom-free women? J Orofac Pain. 2000;14:105-111.
Dittrich R. Somatic pain and autonomic concomitants. Am J Surg. 1954.
Fernández de las Peñas C., Palomeque del Cerro L., Carnero J. Manual treatment of post-whiplash injury. Journal of Bodywork and Movement Therapies. 2005;9(2):109-119.
Fernández-de-las-Peñas C., Simons D., Cuadrado M., et al. The role of myofascial trigger points in musculoskeletal pain syndromes of the head and neck. Curr Pain Headache Rep. 2007;11(5):365-372.
Field T., Hernandez-Reif M., Diego M., et al. Cortisol decreases and serotonin and dopamine increase following massage therapy. Int J Neurosci. 2005;115(10):1397-1413.
Fryer G., Fossum C. Muscle Energy Techniques. In: Fernadez-de-las-Penas C., Arndt-Nielsen L., Gerwin R., Dommerholt J, editors. Tension-type and Cervicogenic Headache. Boston: Jones & Bartlett, 2009.
Fryer G., Hodgson L. The effect of manual pressure release on myofascial trigger points in the upper trapezius muscle. Journal of Bodywork and Movement Therapies. 2005;9(4):248-255.
Garland W. Somatic changes in hyperventilating subject. Paris: Presentation at Respiratory Function Congress, 1994.
Gerwin R., Dommerholt J. Treatment of myofascial pain syndromes. In: Weiner R., editor. Pain management; a practical guide for clinicians. Boca Raton: CRC Press; 2002:235-249.
Goldthwaite J. Essentials of body mechanics. Philadelphia: JB Lippincott, 1949.
Greenman P. Manual medicine. Baltimore: Williams & Wilkins, 1989.
Hartman L. Handbook of osteopathic technique. London: Hutchinson, 1985.
Hungerford B., Gilleard W. SIJ angular rotation during the stork and hip drop tests in normal subjects: pilot study results. Vienna: Third Interdisciplinary World Congress on Low Back and Pelvic Pain, 1998;332-334.
Janda V. Muscle function testing. London: Butterworths, 1983.
Janda V. Glasgow E., editor. Aspects of manipulative therapy. Edinburgh: Churchill Livingstone, 1985.
Janda V. Grant R., editor. Physical therapy in the cervical and thoracic spine. New York: Churchill Livingstone, 1988.
Jones L. Strain/counterstrain. Colorado Springs: Academy of Applied Osteopathy, 1981.
Jung C-G. Synchronicity: an acausal connecting principle. Princeton, New Jersey: Princeton University Press, 1973.
Kleyhans & Aarons. Digest of Chiropractic Economics September. 1974.
Korr I. Spinal cord as organiser of the disease process. 1976 Yearbook of the Academy of Applied Osteopathy. 1977. Colorado Springs
Latey P. Muscular manifesto. London: Published privately, 1986.
Lee D. Palpation issues. Journal of Bodywork and Movement Therapies. 2002;6(1):26-27.
Lewit K. Manipulative therapy in rehabilitation of the motor system. London: Butterworths, 1985.
Lewit K. Manipulation in rehabilitation of the locomotor system, ed 2. London: Butterworths, 1992.
Lewit K. Manipulation in rehabilitation of the locomotor system, ed 3. London: Butterworths, 1999.
Lief S. Cited. In: Chaitow L., editor. Neuro-muscular technique/soft tissue manipulation. Wellingborough, UK: Thorsons, 1989.
Lief P. Neuromuscular technique. British Naturopathic Journal and Osteopathic Review Autumn. 1963:304.
Loga S. Integrative treatment in psychiatry. Psychiatr Danub. 2008;20(3):349-351.
McMakin C. Microcurrent Therapy. In: Chaitow L., editor. Fibromyalgia Syndrome – A Practitioner’s Guide to Treatment. Edinburgh: Churchill Livingstone, 2003.
Mancuso C., Tanzi M., Gabay M. Paradoxical reactions to benzodiazepines: Literature review and treatment options. Pharmacotherapy. 2004;24(9):1177-1185.
Melzack R., Wall P. The challenge of pain. London: Penguin, 1988.
Mitchell F., Moran P., Pruzzo N. Evaluation of osteopathic muscle energy procedure. Valley Park, Illinois: Pruzzo, 1979.
Murphy D., editor. Conservative management of cervical spine syndromes. New York: McGraw Hill, 2000.
Myers T. Anatomy trains. Edinburgh: Churchill Livingstone, 2001.
Nimmo R. Receptor tonus technique. In Lecture notes. London: British College of Naturopathy and Osteopathy; 1966.
Nixon P., Andrews J. A study of anaerobic threshold in chronic fatigue syndrome (CFS). Biol Psychol. 1996;43:264.
Pollard H., Ward G. A study of two stretching techniques for improving hip flexion range of motion. J Manipulative Physiol Ther. 1997;20:443-447.
Pollo A., Benedetti F. Placebo Response: Relevance to the Rheumatic Diseases. Rheumatic Disease Clinics of North America. 2008;34(2):331-349.
Randolph T. Stimulatory withdrawal and the alternations of allergic manifestations. In: Dickey L., editor. Clinical ecology. Springfield, Illinois: Charles C. Thomas; 1976:156-175.
Rolf I. The integration of human structures. USA: Harper & Row, 1977.
Roll M., Thorell T. Acute chest pain without obvious cause before age 40 – personality and recent life events. J Psychosom Res. 1987;31(2):215-221.
Selye H. The stress of life. New York: McGraw-Hill, 1984.
Schenk R., Adelman K. The effects of MET on cervical range of motion. J Manual Manip Ther. 1994;2:149-155.
Simons D., Travell J., Simons L. ed 2. Myofascial pain and dysfunction: the trigger point manual. vol 1. Baltimore: Williams & Wilkins; 1999. Upper half of body
Slatkovska L., Jensen D., Davies A., et al. Phasic menstrual cycle effects on the control of breathing in healthy women. Respiratory Physiology & Neurobiology. 2006;154:379-388.
Slocumb J. Neurological factors in chronic pelvic pain, trigger points and abdominal pelvic pain. Am J Obstet Gynecol. 1984;49:536.
Speicher T., et al. Effect of strain counterstrain on pain and strength in hip musculature. J Manual Manip Ther. 2004;12(4):215-223.
Speransky A. A basis for the theory of medicine. New York: International Publishers, 1943.
Travell J., Simons D. Myofascial pain and dysfunction: the trigger point manual. vol 1. Baltimore: Williams & Wilkins; 1983.
Travell J., Simons D. Myofascial pain and dysfunction: the trigger point manual. vol 2. Baltimore: Williams & Wilkins; 1992. The lower extremities
Upledger J. Craniosacral therapy. USA: Eastland Press, 1983.
Vleeming A., Mooney V., Dorman T., Snijders C., Stoeckart R., editors. Movement, stability and low back pain. Edinburgh: Churchill Livingstone, 1997.
Wall P.D., Melzack R., editors. Textbook of pain, ed 2, Edinburgh: Churchill Livingstone, 1989.
Weiss J. Pelvic floor myofascial trigger points: manual therapy for interstitial cystitis and the urgency–frequency syndrome. J Urol. 2001;166:2226-2231.
Wilson E., Payton O., Donegan-Shoaf L., Dec K. Muscle energy technique in patients with acute low back pain: a pilot clinical trial. Journal of Orthopedic and Sports Physical Therapy. 2003;33:502-512.
Youngs B. The physiological background of neuromuscular technique. British Naturopathic Journal and Osteopathic Review. 1963;5:176-178.
Youngs B. Lief’s Neuromuscular Technique: a recollection. In: Chaitow L., et al, editors. Physical Medicine. Edinburgh: Churchill Livingstone, 2008.