7 Basic abdominal and pelvic NMT application
Objectives
The objectives for the use of NMT – and associated methods – in the treatment of abdominopelvic tissues vary considerably and may include:
1. To attempt to normalize local soft tissue dysfunction and pain (including symptoms produced by myofascial trigger points) resulting from postural or overuse strain (occupational or leisure activities, patterns of use, overload, repetition of movement, lifting, etc.), breathing pattern disorders, obesity, visceroptosis (causing drag of supporting structures, and associated congestion).
2. To enhance relaxation and reduction in symptoms relating to emotional or stress influences, particularly long-held psychological distress.
3. To improve function when the area has been traumatized (accidents, blows, surgery, etc.).
4. To influence internal organ function via reflex stimulation, for example using neurolymphatic (Chapman) reflexes and/or acupuncture points (see Ch. 4).
5. To modify painful and distressing symptoms such as those associated with chronic pelvic pain (CPP), interstitial cystitis and urgency (Weiss 2001). See Box 7.1 for details of research into such influences.
6. To attempt to improve function of the abdomino-pelvic organs by directly influencing circulatory and drainage functions (including lymphatic function) of the region (Wallace et al 1997).
7. To modify the negative local effects of viscerosomatic influences (see Ch. 3).
Between September 1995 and November 2000, 45 women and 7 men, including 10 with interstitial cystitis and 42 with the urgency–frequency syndrome, were treated once or twice weekly for 8–12 weeks, using manual therapy applied to the pelvic floor, aimed at decreasing pelvic floor hypertonus and deactivating trigger points (Weiss 2001).
Of the 42 patients with the urgency–frequency, 35 (83%) had moderate to marked improvement or complete resolution, while seven of the ten with interstitial cystitis had moderate to marked improvement.
In ten cases the subjective results (symptom score sheet) were confirmed by measuring resting pelvic floor tension by electromyography, before and after the treatment course.
Somaticovisceral symptoms
In Chapter 3 there was discussion of the phenomenon in which organ dysfunction reflects reflexogenically to the soma particularly as areas of segmental facilitation (sensitization) in the spinal region. These are, of course, the viscerosomatic reflexes. Later in this chapter possible variations on causes of viscerosomatic reflex pain will be outlined.
Simons et al (1999) reverse the consideration when they report details of somatovisceral responses, particularly arising from abdominal musculature, influencing internal visceral organs and functions.
They note that injection of the trigger affecting an organ may offer symptomatic relief. This is not meant to suggest that local changes (such as trigger points) in the soma, muscles, etc. are necessarily the cause of such dysfunctions and diseases (see list below), but that there exists a strong possibility, in any given case, that the conditions/disease processes may be aggravated and/or maintained by reflexogenic activity associated with myofascial trigger points:
• urinary bladder and sphincter spasm
• pain symptoms mimicking those of appendicitis and cholelithiasis
• symptoms of burning, fullness, bloating, swelling or gas (Gutstein 1944)
• heartburn and other symptoms of hiatal hernia
Junctional tissues
Simons et al (1999) have discussed the sites of trigger points as falling largely into two categories:
These guidelines also apply when treating abdominopelvic, and related areas, where, in addition, the author’s clinical experience suggests that particular attention should be given to specific junctional tissues, such as:
• Lateral aspect of the rectal muscle sheaths
• Attachments of the recti muscles and external oblique muscles to the ribs
• The xiphisternal ligament, as well as the lower attachments of the internal and external oblique muscles
• Intercostal areas from 5th to 12th ribs are equally important
• Scars from previous operations may be the site of formation of connective tissue trigger points (Simons et al 1999). After sufficient healing has taken place, these incision sites can be examined by gently pinching, compressing and rolling the scar tissue between the thumb and finger to examine for evidence of trigger points, as discussed in earlier chapters (Chaitow & DeLany 2000).
Assisting organ dysfunction
Specific general areas are worthy of consideration in treating conditions that affect particular organs or functions, based on the evidence of the different reflex systems described in Chapter 4 (see also notes on percussive methods, such as spondylotherapy, in Chapter 8) (Baldry 1993, Chaitow & DeLany 2000, Fitzgerald et al 2009, Kuchera & Kuchera 1994, Wallace et al 1997):
• Liver dysfunction and portal circulatory dysfunction calls for special attention to the right-side intercostal musculature, from the 5th to the 12th ribs. Especially important are the various muscular insertions into all these ribs.
• Gall bladder dysfunction involves similar areas, with extra attention to the area on the costal margin, roughly midway between the xiphisternal notch and the lateral rib margins.
• Spleen function may be stimulated by attention to the intercostal spaces between the 7th and 12th ribs on the left side.
• Digestive disorders in general may benefit from NMT applied to the central tendon, between the recti, and directly to the rectal sheaths.
• Stomach pain is treated via its reflex area to the left of the xiphisternal notch and to the tendon and rectal sheaths.
• Colonic problems and ovarian dysfunction may benefit from reflex NMT application to both iliac fossae as well as to the midline structures.
• Dysfunction of the kidneys, ureters and bladder requires attention to the inguinal borders of the internal and external oblique insertions, the suprapubic insertions of the recti, the overlying muscles and sheaths of the area, and the internal aspects of the upper thigh.
• In pelvic congestion relating to gynaecological dysfunction, NMT should be applied to the hypogastrium and both iliac fossae. This appears to relieve congestion and stimulates pelvic circulation.
• Ileitis and other functional disturbances of the transverse colon and small intestine may benefit from NMT applied to the umbilical area.
• Prostatic dysfunction may benefit from NMT to the central hypogastric region. Internal drainage massage of the prostate should also be considered.
The above brief indications should be considered in conjunction with other reflex systems and points (see below), as well as attention to the appropriate spinal areas (see notes on facilitation in Ch. 3), which may also benefit from NMT.
More on abdominal reflex areas
Gutstein (1944) noted ‘trigger areas’ in the sternal, parasternal and epigastric regions, and in the upper portions of the recti muscles, all relating to varying degrees of retroperistalsis. He also noted that colonic dysfunction related to triggers in the mid and lower recti muscles. These were all predominantly left-sided.
Other symptoms that improved or disappeared with the obliteration of these triggers include excessive appetite, poor appetite, flatulence, nervous vomiting, nervous diarrhoea, etc.
The triggers were always ‘tender spots’, easily found by palpation, and situated mainly in the upper, mid and lower portions of the recti muscles, over the lower portion of the sternum and the epigastrium, including the xyphoid process and the parasternal region. The parasternal region corresponds to the attachments of the rectus muscles into the 5th, 6th and 7th ribs.
Fielder & Pyott (1955) described a number of reflexes occurring on the large bowel itself. These could be localized by deep palpation and treated by specific release techniques (see Chapter 8, and Figure 8.21). These reflexes palpate as areas of tenderness, and may include a degree of swelling and congestion resulting from adhesions, spasticity, diverticuli, chemical or bacterial irritation, etc.
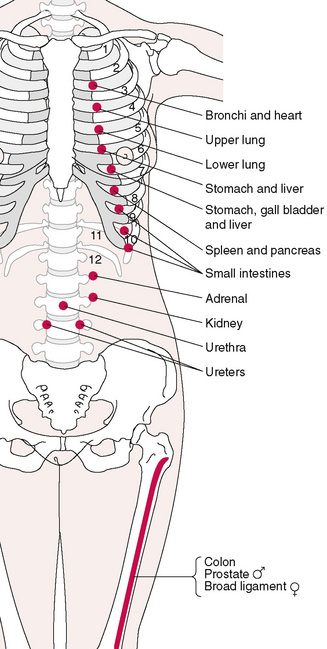
In considering the reflexes available for therapeutic intervention, in the thoracic and abdominal regions, the neurolymphatic points of Chapman are worthy of close attention (see Chapter 4 for more detail). When applying NMT in its evaluative mode, to the anterior thorax and abdomen (as described later in this chapter), an awareness of the reflexes described by Chapman (Owen 1980) is a distinct advantage, especially if there is a need to take account of visceral or thoracic organ dysfunction.
Kuchera (1997) notes:
Palpate for tender anterior Chapman’s [neurolymphatic] points as an indication to specific visceral irritation … Abdominal viscera, because of their innervations, have their first Chapman’s [neurolymphatic] points at the level of the fifth intercostal spaces. If an anterior Chapman’s [neurolymphatic] point is tender, ask the patient questions relating to dysfunction of the organ most likely to produce the tender point.
Anterior neurolymphatic reflexes for the upper lungs are found between the 3rd and 4th ribs, and between the 4th and 5th ribs (lower lung), close to the costal cartilage and the sternum.
See Figure 7.1 for the location of common abdominally related reflexes noted in this region (and also Figs 5.8A,B).
Discussion
To what extent Gutstein’s myodysneuric points are interchangeable with Chapman’s, or Fielder’s, reflexes, or other systems of reflex study (e.g. acupuncture or tsubo points or Travell’s trigger points), and to what extent these involve Mackenzie’s work (Mackenzie 1909) as illustrated in Figure 5.4, is a matter for further research.
What is certain is that, within the soft tissues of this region, there abound palpable, sensitive, discrete areas of dysfunction that, on a local basis, interfere with or modify functional integrity to a greater or lesser degree, and reflexively are capable of massive interference with normal physiological function on a neural, circulatory and lymphatic level, to the extent of producing or mimicking serious pathological conditions. As these areas of dysfunction often yield to the simple, soft tissue manipulative techniques that are incorporated into Lief’s NMT, the value of these techniques becomes apparent.
Many of Jones’ (positional release/strain/counterstrain) tender points (see Figure 4.5A) are located in the abdominal region, specifically relating to those strains that occur in a flexed position (Jones 1981).
Bennett’s neurovascular points (see Chapter 4 and Figure 5.9A) are located mainly on the anterior aspect of the body, and may be located during abdominal NMT work. This may be a link with the work of Mackenzie and others, who have demonstrated a clear relationship between the abdominal wall and the viscera. This and other reflex patterns provide the rationale for NMT application to the abdominal and sternal regions.
These reflex patterns vary in individual cases, but it is clear that the majority of the organs are able to protect themselves by producing contraction, spasm and hyperaesthesia of the overlying, reflexively related, muscle wall – the myotome – which is also often augmented by hyperaesthesia of the overlying skin – the dermatome.
Baldry (1993) details a huge amount of research that validates the link (a somatovisceral reflex) between abdominal trigger points, and symptoms as diverse as anorexia, flatulence, nausea, vomiting, diarrhoea, colic, dysmenorrhoea and dysuria.
Pain of a deep aching nature, or sometimes of a sharp or burning type, is reported as being associated with this range of symptoms, which mimic organ disease or dysfunction (Fitzgerald et al 2009, Melnick 1954, Ranger et al 1971, Travell & Simons 1983).
Baldry (1993) has further summarized the importance of this region as a source of considerable pain and distress involving pelvic, abdominal and gynaecological symptoms. He says:
Pain in the abdomen and pelvis most likely to be helped by acupuncture is that which occurs as a result of activation of trigger points in the muscles, fascia, tendons and ligaments of the anterior and lateral abdominal wall, the lower back, the floor of the pelvis and the upper anterior part of the thigh. Such pain, however, is all too often erroneously assumed to be due to some intra-abdominal lesion, and as a consequence of being inappropriately treated is often allowed to persist for much longer than is necessary.
If we replace the word acupuncture with the term ‘appropriate manual methods’, we can appreciate that a large amount of abdominal and pelvic distress may be remediable via the methods outlined in this book.
What activates these triggers? – similar factors that produce ‘stress’ anywhere else in the musculoskeletal system: postural faults, trauma, environmental stressors such as cold and damp, surgery (another form of trauma) and so on.
Differential diagnosis is obviously important in a region housing so many vital organs, and attention to the overall pattern of symptom presentation is critical.
 Is the pain in the muscle or an organ?
Is the pain in the muscle or an organ?
As there is no underlying osseous structure available to allow compression of the musculature of many of the soft tissues of the abdomen, there is a need for a particular strategy that helps to screen palpated pain occurring at depth from that being produced in surface tissues.
When a local area of pain is noted, using NMT or any other palpation method, it should be firmly compressed by the palpating digit, sufficient to produce pain/referred pain (if a trigger is involved) but not enough to cause distress.
• The supine patient is then asked to raise both (straight) legs from the table (heels must be raised by several inches).
• As this happens there will be a contraction of the abdominal muscles, which produces a compression of the trigger point between the muscle and the finger/thumb, and pain should increase.
• If pain decreases on the raising of the legs, the site of the pain is beneath the muscle and probably involves a visceral problem (Thomson & Francis 1977).
It is, of course, possible for there to be a problem in the viscera as well as in the abdominal wall (see item 3 in the discussion immediately below), in which case this test would be in error in ascribing all symptoms of pain to a muscle wall lesion.
The superficial musculature may be receiving distress sensations from an inflamed or irritated organ. The test described above therefore gives a clue, but not an absolute finding, as to the locality of the problem causing the pain.
Pain variables in abdominal somatic tissues
Kuchera (1997) points to three different manifestations of pain and discomfort arising from irritation or inflammation in the pelvic and abdominal viscera:
1. A ‘vague, gnawing, deep, poorly localized, and mid-abdominal’ pain, derives from afferent impulses from the organs of the region travelling towards the spinal cord.
2. Organs are supplied with their sympathetic input from specific spinal levels. Afferent messages also travel towards the spine, from the organs, along the same pathways, and when the organ is dysfunctional (inflamed, irritated, etc.) paraspinal changes (including tenderness, asymmetry, tissue changes and altered range of movement) will be noted at the level from which sympathetic innervation emerges for particular organs. (See notes on facilitation and viscerosomatic reflexes in Chapter 3, connective tissue massage in Chapter 4, and also zones of dysfunction in Chapter 5.) Beal (1985) has summarized the levels as:
3. Pain may be noted in the soft tissues superficial to the organ. Kuchera (1997) describes these as being due to irritation of contiguous peritoneal tissues and the abdominal wall, and as being ‘responsible for rebound tenderness and abdominal guarding, associated with severe abdominal pain.’ (See also Fig. 5.4 showing abdominal reflexes, as described by Mackenzie in 1909).
Treatment of attachment stress in the mesentery (e.g. visceroptosis effects)
The mesentery (literally ‘the middle intestine’) is the name given to the double layer of peritoneal membrane that supports the small intestine. It is shaped like a fan, with its shorter edge attaching to the back of the abdomen, and the longer edge attaching to the small intestine for a length of around 20 feet (6 metres). The main mesenteric attachment is located in a line running from approximately 1 inch (2.5 cm) above and 1 inch (2.5 cm) to the left of the umbilicus, downward and to the right lower quadrant of the abdomen, just anterior to the sacroiliac joint (see Fig. 7.2).
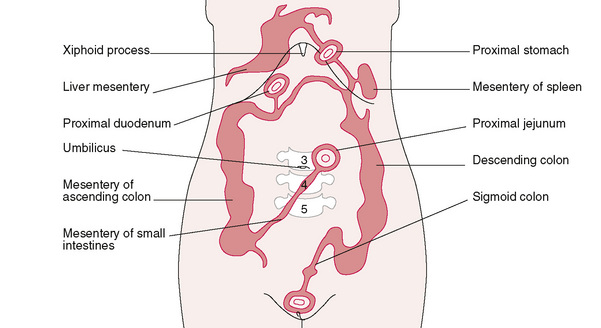
If the organs of the abdomen sag, as occurs in obesity and visceroptosis, enormous degrees of drag occur on the mesenteric attachment tissues, with resulting congestion. Kuchera (1997) reports:
‘[Appropriate] treatment improves organ function, and can decrease many functional visceral symptoms, including bloating, constipation, and pelvic or abdominal pain.
Kuchera acknowledges the clinical research and teachings of the French osteopath Barral, whose work in visceral manipulation has opened this area to improved therapeutic intervention (Barral & Mercier 1988).
The mesenteric structures carry the sympathetic and parasympathetic fibres (as well as arteries) to the viscera, and also afferent fibres, lymphatic and venous vessels, away from the viscera.
Kuchera (1997) suggests that tenderness and tension in the mesentery can be palpated for tension and treated as follows:
By placing the extended fingers flat over the lateral margin of the ascending or descending colon and moving the viscera toward the midline of the body. The [practitioner] monitors continuously for changes in resistance to this movement.
• The mesentery of the sigmoid colon is moved toward the umbilicus (see Fig. 7.3A, B).
• The 6-inch (15 cm) mesentery, along with the 30 feet (9 metres) of small intestines, is palpated by placing the extended fingers carefully into the lower left abdominal quadrant to obtain as much of the small intestines as possible, and moving this towards the upper right quadrant of the abdomen (see Fig. 7.4).
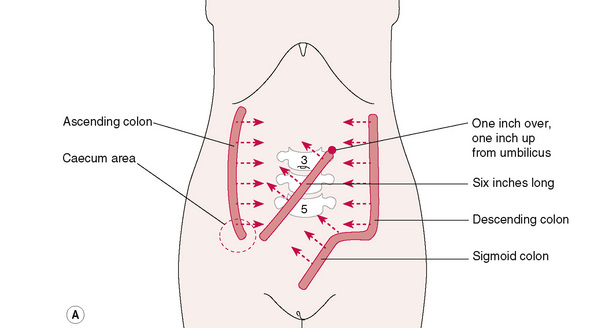
Figure 7.3A Suggested directions of movement in treating intestinal mesentery (after Kuchera).
From Ward (1997), with permission.

Figure 7.3B Lifting the small intestine/sigmoid colon to ease mesenteric drag (after Wallace et al).
From Ward (1997), with permission.
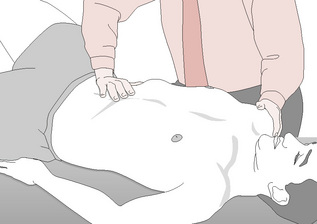
Figure 7.4 Lifting the caecum to ease mesenteric drag (after Wallace et al).
From Ward (1997), with permission.
To treat restrictions noted in such palpation:
• The patient lies supine, with knees flexed and feet flat on the table.
• The fingers are extended and placed flat over the lateral margin of the mesentery (to be treated).
• Medial pressure is then placed over the section of bowel, at right angles to its posterior, mesenteric, abdominal wall attachment.
• The tension is held as the patient takes a half-breath and holds it.
Wallace et al (1997) caution against causing any pain during these procedures, and further suggest that the tissues being held should be gently ‘turned’ clockwise and anticlockwise, to sense their position of greatest tissue freedom. The tissues are then held for not less than 90 seconds, or until a sense of relaxation is noted.
When breathing resumes, after this positional release approach, the tissues should be repalpated.
Abdominal NMT application
If, during palpation or treatment, any large pulsating mass is noted in the midline between the xyphoid and the umbilicus, caution should be exercised.
Kuchera (1997) notes: ‘A normal abdominal aorta in an adult should not be wider than an inch (2.5 cm). Pulsations occurring anteriorly are normal, but lateral pulsations from the aorta suggest a weak vessel wall or aneurysm. Palpate [also] the inguinal area for a good pulse and compare the right and left sides. If a decreased pulse is found on one or both sides, ask the patient about claudication and then palpate and evaluate the pulse at the popliteal, posterior tibial, and dorsal pedis arteries in that leg, and compare to pulses in the opposite leg.’
Box 7.3 Differential abdominal symptoms (Grieve 1994)
Most abdominal disorders can produce pain in the back (e.g. peptic ulcer, colonic cancer, abdominal arterial disease). Therefore, all other symptoms should be evaluated alongside the musculoskeletal assessment.
• A hiatus hernia is usually associated with bilateral thoracic and shoulder pain. Anginal pain classically presents with chest, anterior cervical and (usually left) arm pain.
• Thoracic facet or disc conditions can mimic angina, as can active trigger point activity. Aggravating and ameliorating factors usually offer clues as to whether the condition is cardiac related, or whether it is aggravated or eased by biomechanical influences.
• A dysfunctional gall bladder commonly refers pain to the mid-thoracic area, unilaterally or bilaterally. Aggravating and ameliorating factors can usually offer clues as to whether the condition is related to digestive function or is biomechanically influenced.
• Sacroiliac and right buttock pain may be produced by perforation of the ileum in regional ileitis (Crohn’s disease).
• Pronounced low back pain (possibly referring to the testicles in men) may be associated with an aneurysm that is about to rupture. Grieve (1994) reports that ‘the onset of dissection of the ascending aorta or aortic arch is characterized by a sudden, tearing chest pain’, which may radiate to the neck, thorax, abdomen and legs. The distinction between such symptoms and an acute musculoskeletal problem may be discerned by the ‘suddenness, severity and spread’ of the pain.
• If a patient has a background of coronary, pulmonary or bronchial disease, the vertebral veins may have become varicosed, leading to an ill-defined backache. Grieve (1994) discusses the widespread nature of venous drainage from the vertebral column. These veins, as well as associated arteries and arterioles, are ‘supplied with a dense plexiform arrangement of unmyelinated nerve fibers which constitute an important part of the vertebral column, and which may be irritated in a variety of ways to give rise to pain.’
In treating the abdominal and thoracic regions, the patient should be supine with the head supported by a medium-sized pillow and the knees flexed, either with a bolster under them or drawn right up so that the feet approximate the buttocks. Generous application of lubricant should be made to the area being treated.
Intercostal treatment
Abdominal and anterior intercostal NMT (see Fig. 7.5)
The initial objective of the treatment strokes described below is to evaluate for soft tissue changes (active or latent trigger points, tissue texture changes, asymmetry, tenderness, etc.) with a contact that ‘meets and matches’ tissue tension.
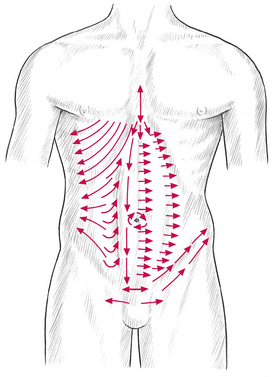
Figure 7.5 Neuromuscular abdominal technique. Suggested lines of application to access primary trigger point and attachment sites, and interfaces between different muscle groups. Note that the lines of application on this chart show one side only, and a full assessment/treatment involves these thumb or finger strokes being applied on each side of the body.
Only when a decision has been made to use subsequent strokes to attempt to alter the status of the tissues should pressure be increased to overcome tension, fibrotic resistance, etc., so stretching, inhibiting, draining – and in other ways modifying – structural features. (See Chapter 3, particularly Box 3.5, for notes on the effects of compressive force.)
• The practitioner should be facing the patient, and be half-turned towards the head, with legs apart for an even distribution of weight, and with knees flexed to facilitate the transfer of pressure through the arms. As many of the manoeuvres in the intercostal area, and on the abdomen itself, involve finger and thumb movements of a lighter nature than those applied through the heavy spinal musculature, the elbows need not be kept as straight as possible for spinal NMT (see Ch. 6).
• However, when deep pressure is called for, and especially when this is applied via the thumb, the same criterion of weight transference, from the shoulder through the thumb, applies, and the straight arm is then an advantage for the economic and efficient use of energy.
• The practitioner should be positioned to be level with the patient’s waist, and a series of strokes would be applied with the tip of the thumb, along the course of the intercostal spaces from the sternum, laterally.
• It is important that the attachments of the internal and external muscles receive attention.
• The margins of the ribs, both inferior and superior aspects, should receive firm gliding pressure from the distal phalanx of the thumb or middle finger.
• If there is too little space to allow such a degree of differentiated pressure, then a simple stroke along the available intercostal space has to suffice.
• If the thumb cannot be insinuated between the ribs, a finger (side of finger) contact can be used (see description of NMT finger technique in Chapter 6), in which this is drawn towards the practitioner, from the side contralateral to that being treated, towards the sternum.
• The intercostals, from the 5th rib to the costal margin below the 12th rib, should receive a series of two or three deep, slow-moving, gliding, sensitive strokes on each side, with special reference to points of particular congestion or sensitivity. These areas may also benefit from sustained or variable pressure techniques, depending on the objective. It is useful to note the possible presence, in the intercostal spaces, close to the sternum of neurolymphatic (Chapman) reflex points.
• These points require only light circular pressure when being treated (see Chapter 5 for more detail). The practitioner should bear in mind other reflex patterns in the region, including those related to acupuncture alarm points and neurovascular points.
• If a localized area of dysfunction is located, which refers pain or other symptoms that are familiar to the patient, an active trigger point will have been located (see Ch. 3).
• Gentle probing on the sternum itself may elicit sensitivity in the rudimentary sternalis muscle, which has been found to house trigger points. If this is found to be sensitive, any of the various trigger point treatments recommended in Chapter 8 may be used.
• It is not necessary for the practitioner to change sides during treatment of the intercostals, unless it is found to be more comfortable to do so.
• Having treated the intercostal musculature and connective tissue, and having charted and/or treated any trigger points located during assessment, the practitioner, using either a deep thumb pressure, or a contact with the pads of the fingertips, applies a series of short strokes in a combination of oblique lateral and inferior directions from the xyphoid process.
Rectal sheath
• Thumbs or fingers may then be used to apply a series of deep slow strokes, along and under the costal margins. Whether diaphragmatic attachments can be located is questionable; however, sustained, firm (but not invasively aggressive) pressure allows for gradual access to an area that may reveal trigger points of exquisite sensitivity, with often surprising areas of referral. Many seem to produce sensations internally, while others create sensations in the lower extremities or in the throat, upper chest and shoulders.
• Deactivation of such triggers needs to be carried out slowly, carefully and with sensitivity.
• A series of short strokes using fairly deep, but not painful, pressure should then be applied by the thumb, from the midline up to the lateral rectal sheath.
• This series of strokes starts just inferior to the xyphoid and concludes at the pubic promontory where trigger points are common.
• The series may be repeated on each side several times, depending on the degree of tension, congestion and sensitivity noted. It is useful during these applications to be aware of the mesenteric attachments as described by Wallace et al (1997) and Kuchera (1997) (see Figs. 7.2 & 7.3).
• A similar pattern of assessment/treatment is followed (using the thumb if working ipsilaterally, and the fingers if working contralaterally) across the lateral border of the rectal sheath, a series of short, deep, slow-moving (usually thumb) strokes being applied from just inferior to the costal margin of the rectal sheath, until the inguinal ligament is reached. Both sides are treated in this way (Fig. 7.5).
• A series of similar strokes is then applied on one side and then the other laterally, from the lateral border of the rectal sheath (see Fig. 7.5).
• These strokes follow the contour of the trunk, so that the upper strokes travel in a slightly inferior curve whilst moving laterally (following the curve of the lower ribs), and the lower strokes have a superior inclination (following the curve of the crest of the pelvis) as the hand moves laterally.
• A total of five or six strokes should be adequate to complete these movements, and this could be repeated, before performing the same strokes on the opposite side.
• Evidence is being sought of local soft tissue changes, as well as any underlying sense of tension or ‘drag’ on supporting tissues.
When treating the side on which the practitioner is standing, it may be more comfortable to apply the therapeutic stroke via the flexed fingertips, which are drawn towards the practitioner, or the usual thumb stroke may be used (see Ch. 6).
In treating the opposite side, thumb pressure can be applied more easily, as in spinal technique, with the fingers acting as a fulcrum and the thumb weaving towards them in a series of 2 to 3 inch (3 to 5 cm) strokes.
The sensing of contracted localized areas of dysfunction is more difficult in abdominal work, and requires great sensitivity of touch, and great concentration on the part of the practitioner.
Symphysis pubis
The sheaths of the rectus abdominis muscles, from the costal margins downwards to the pubic bones, are evaluated by finger or thumb strokes. Attention should be given to the soft tissue component of, as well as the insertions into, the iliac fossa, the pubic bones and the symphysis pubis, including the inguinal ligaments (see Fig. 7.5).
• Strokes should be made, commencing at the anterior superior iliac spine (ASIS), while attempting to assess the attachments of internal and external obliques as well as transversus abdominis, which can be contacted.
• A deep but not painful stroke, employing the pad of a thumb, should be applied to the superior aspect of the pubic crest. This should start at the symphysis pubis and move laterally, first in one direction and, then after repeating it once or twice, in the other.
• A similar series, starting at the centre and moving laterally, should then be applied over the anterior aspect of the pubic bone. Great care should be taken not to use undue pressure as the area is sensitive at the best of times, and may be acutely so if there is dysfunction associated with the insertions into these structures (as well as in relation to sacral torsions, sacroiliac dysfunction or chronic pelvic pain – which is discussed briefly later in this chapter).
• A series of deep slow movements should then be performed, via the thumb, along the superior and inferior aspects of the inguinal ligament, starting at the pubic bone and running up to and beyond the iliac crest.
Positional release implications of abdominal tender points
In this lower abdominal area, close to the ASIS, and towards the umbilicus, many of the tender points (see Chapter 4 on Jones’ points, and Figure 4.5A) associated with flexion strains of the lumbar and lower thoracic spine may be located.
Positional release methods should be employed to relieve the dysfunctional patterns associated with these (see notes on strain/counterstrain in Chapter 8 and also Box 7.4).
Box 7.4 Positional release technique for abdominal muscles
Tender points (which may or may not also be trigger points) located in the abdominal musculature often represent dysfunction of the lumbothoracic region; they result from strain or stress, and occurred in flexion.
Tender points are almost always located in tissues shortened at the time of strain. For a greater understanding of the strain/counterstrain theory, which supports this assertion (see Chaitow 2007, Chaitow & DeLany 2000, Deig 2001, Jones 1981).
Gross positioning to relieve lumbar flexion stresses and strains takes the (usually supine) patient painlessly into flexion (by raising the flexed lower limbs to induce lumbar flexion), with the final position of ease being held for at least 90 seconds.
The ‘position of ease’ is determined by means of palpation of the tender point, with the patient reporting on the change in ‘score’ as the positioning is ‘fine tuned’. A score of 3 or less is the objective, having commenced from a score of 10 before the repositioning starts.
• Jones (1981) reports that L1 has two tender points: one at the tip of the anterior superior iliac spine and the other on the medial surface of the ilium, just medial to ASIS.
• The tender point for 2nd lumbar anterior strain is found lateral to the anterior inferior iliac spine.
• L4 tender point is found at the attachment of the inguinal ligament on the ilium.
• L5 points are on the body of the pubes, just to the side of the symphysis.
• In bilateral strains, both sides should be treated. L3 and L4 usually require greater side-bending in fine-tuning than the other lumbar points.
Lateral rectus sheath
• The thumbs, or fingertips, may then be insinuated beneath the lateral rectus border at its lower margins, and deep pressure applied towards the midline.
• The hand or thumb should then slowly move cephalad, in short stages, whilst maintaining this medial pressure.
• This is thought to lift the connective tissue from its underlying attachments, so helping to normalize localized contractures and fibrous infiltrations.
• Additionally, when working on the right the ascending colon, and on the left the descending colon, will be receiving the ‘lift’ appropriate for release of mesenteric drag symptoms (see Fig. 7.3B).
Umbilicus
A series of strokes should then be applied around the umbilicus.
• Using thumb or flexed fingertips, a number of movements of a stretching nature should be performed, in which the non-treating hand stabilizes the tissue at the start of the stroke, which first runs from approximately 1 inch (2.5 cm) superior and lateral to the umbilicus on the right side, to the same level on the left side.
• The non-treating hand then stabilizes the tissues at this end-point of the stroke and a further stretching and probing stroke is applied inferiorly to a point about 1 inch (2.5 cm) inferior and lateral to the umbilicus, on the left side. This area is then stabilized, and the stroke is applied to a similar point on the right. (See circular arrows around umbilicus on Figure 7.5.)
• The circle is completed by a further stroke upwards, to end at the point at which the cicular exploration of these tissues began.
• This series of movements should have a rhythmical pattern so that, as the treating hand reaches the end of its stroke, the non-treating hand comes to that same point and replaces the contact with a stabilizing pressure, whilst the treating hand begins its next stroke.
• A series of three or four such circuits of the umbilicus should be performed.
• Note that the superior mesenteric attachment, which supports the small intestine, is located approximately 1 inch (2.5 cm) superior and 1 inch (2.5 cm) laterally, to the left of the umbilicus.
• Additional strokes may be applied along the midline and the sheaths of the recti muscles from the costal margins downwards.
A soothing culmination to the foregoing (which should take approximately 10–15 minutes) may be applied by a circular clockwise series of movements in which the palm of one hand and the heel of the other alternately circle the whole abdominal area.
Thus, with the practitioner standing to the right of the patient, the palm and fingers of the left hand stroke deeply but gently down the left abdominal structures and then across the lower abdomen towards the practitioner where, using the heel and palm, the right hand takes over the stroke and proceeds up the right side to the costal margin. At this point it changes direction to run across the upper abdomen, where the left hand takes over to repeat this pattern several times. Alternatively, the positional release methods, as described by Wallace et al (1997) and Kuchera (1997) (see Figs 7.3 & 7.4), may be performed.
Linea alba
Additional strokes should be applied along the midline, on the linea alba itself, while searching for evidence of contractions, adhesions, fibrotic nodules, oedema and sensitivity.
Caution is always required to avoid deep pressure on the linea alba, especially if the patient has weakened this muscular/fascial interface as a result of pregnancy, surgery or trauma (diastasis recti). It should also be recalled that the linea alba is a place of attachment of the external obliques as well as transversus abdominis (Braggins 2000).
Specific release
Specific release techniques may be applied during, or after, this general NMT treatment (see Figure 8.21A,B and accompanying notes in Chapter 8). This might be particularly appropriate in cases where there are abdominal scars, or internal adhesions.
The general NMT abdominal treatment (including specific release methods) can be repeated several times weekly, if indicated, but normally once a week should prove adequate, until improvement in function is achieved.
In chronic conditions of abdominal or pelvic dysfunction (see below), the NMT approach as described, together with specific release movements, and appropriate spinal and whole body treatment, is capable of having a profound effect on function in the area.
With an improvement in circulation and drainage, and a reduction in tensions, contractions and reflex activities, homeostatic mechanisms are automatically enhanced.
NMT and chronic pelvic pain dysfunction
Chronic pelvic pain (CPP) is a widespread and distressing condition that accounts for between 10% and 15% of all gynaecological referrals. Zondervan et al (2001) report that the estimated lifetime occurrence of CPP is 33%, affecting primarily, but not exclusively, females. The main symptoms – apart from chronic pain – are:
• Interstitial (non-bacterial) cystitis (IC) – frequency, urgency discomfort/pain on urination
• Vulvar vestibulitis syndrome – a subset of urinary and genital pain disorders or ‘painful bladder’ syndromes
There are numerous potential causes – however one in particular is relevant to this book.
The European Association of Urology (Fall et al 2008) note that trigger points can be located within the pelvic floor muscle, as well as external pelvic and abdominal muscles (Slocumb 1984, Anderson et al 2005, Srinivasan 2007).
The pelvic floor trigger points can develop for a variety of reasons, one of which involves excessive tone in the muscles of the pelvic floor – something commonly noted in female (mainly) athletes, gymnasts, dancers, or individuals who excessively perform Pilates-style exercises (Chaitow 2007). For example Bo & Borgen (2001) found that 41% of elite female athletes experience stress urinary incontinence, a common feature of CPP.
Pain deriving from pelvic floor trigger points is usually aggravated by specific movements and alleviated by certain positions – for example a patient may sit down cautiously, often on one buttock, and standing up again will commonly be painful. CPP may also be aggravated by sustained or repeated contractions (during urination and/or defecation for example).
Trigger points that reproduce pelvic pain, as well as urgency and other symptoms, can often be identified and treated by deactivating active triggers, both internally, as well as externally in the abdominal, gluteal and piriformis muscles.
Weiss (2001) has noted that in his experience the majority of patients with IC report an early history that resulted in pelvic floor muscle dysfunction, suggestive of increased pelvic floor tension. Weiss reports that he has found that an integral part of the treatment regimen, in such patients, involves normalization of these muscles via manual deactivation of trigger points, while also reducing the pelvic floor hypertonicity by means of stretching and strengthening exercises. See Box 7.1.
Connective tissue manipulation (CTM) as described earlier, has also been used to alleviate the symptoms of CPP, as has deep relaxation and biofeedback (Fitzgerald et al 2009).
Trigger point release, involving NMT methods – as discussed throughout the book, is an effective therapeutic approach, as is stretching of the muscle housing the trigger points.
Note: Internal examination, palpation and treatment of pelvic floor trigger points requires:
Anderson R., Wise D., Sawyer T., Chan C. Integration of myofascial trigger point release and paradoxical relaxation training treatment of chronic pelvic pain in men. J Urol. 2005;174(1):155-160.
Baldry P. Acupuncture, trigger points and musculoskeletal pain. Edinburgh: Churchill Livingstone, 1993.
Barral J.P., Mercier P. Visceral manipulation. Seattle: Eastland Press, 1988.
Beal M. Viscerosomatic reflexes: a review. J Am Osteopath Assoc. 1985;85(12):786-801.
Bo K., Borgen J. Prevalence of stress and urge urinary incontinence in elite athletes and controls. Med Sci Sports Exerc. 2001;33(11):1797-1802.
Braggins S. Back care: a clinical approach. Edinburgh: Churchill Livingstone, 2000.
Chaitow L. Positional release techniques, ed 3. Edinburgh: Churchill Livingstone, 2007.
Chaitow L., DeLany J. Clinical applications of neuromuscular technique. Edinburgh: Churchill Livingstone, 2000.
Chaitow L. Chronic pelvic pain: Pelvic floor problems, sacroiliac dysfunction and the trigger point connection. Journal of Bodywork and Movement Therapies. 2007;11:327-339.
Deig D. Positional release technique. Boston: Butterworth Heinemann, 2001.
Fall M., et al. Guidelines on Chronic Pelvic Pain. European Association of Urology. 2008.
Fielder S., Pyott W. The science and art of manipulative surgery. American Institute of Manipulative Surgery. 1955. Salt Lake City, Utah
Fitzgerald, et al. Randomized feasability trial of myofascial physical therapy for the treatment of urological chronic pelvic pain syndromes. J of Urol. 2009(182):570-580. Aug
Grieve G. The masqueraders. In Boyling J.D., Palastanga N., editors: Grieve’s modern manual therapy, ed 2, Edinburgh: Churchill Livingstone, 1994.
Gutstein R. The role of abdominal fibrositis in functional indigestion. Miss Valley Med J. 1944:66-114.
Jones L. Strain and counterstrain. Colorado Springs: Academy of Applied Osteopathy, 1981.
Kuchera M., Kuchera W. Considerations in systemic dysfunction. Columbus, Ohio: Greyden Press, 1994.
Kuchera W. Lumbar and abdominal region. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Mackenzie J. Symptoms and their interpretation. 1909. London
Melnick J. Treatment of trigger mechanisms in gastrointestinal disease. N Y State J Med. 1954;54:1324-1330.
Owen C. An endocrine interpretation of Chapman’s reflexes. Newark, Ohio: American Academy of Osteopathy, 1980.
Ranger I., et al. Abdominal wall pain due to nerve entrapment. Practitioner. 1971;206:791-792.
Simons D., Travell J., Simons L. Myofascial pain and dysfunction: the trigger point manual. ed 2. Upper half of body. vol 1. Baltimore: Williams & Wilkins; 1999.
Slocumb J. Neurological factors in chronic pelvic pain: trigger points and the abdominal pelvic pain syndrome. Am J Obstet Gynaecol. 1984;149(5):536-543.
Srinivasan A., Kaye J., Moldwin R. Myofascial dysfunction associated with chronic pelvic floor pain: management strategies. Curr Pain Headache Rep. 2007;11(5):359-364.
Theobald G. Relief and prevention of referred pain. J Obstet Gynaecol Br Commonw. 1949;56:447-460.
Thomson H., Francis D. Abdominal wall tenderness: a useful sign in the acute abdomen. The Lancet. 1977;i:1053.
Travell J., Simons D. Myofascial pain and dysfunction – trigger point manual. Baltimore: Williams & Wilkins, 1983.
Wallace E., McPartland J., Jones J., et al. Lymphatic system. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Weiss J. Pelvic floor myofascial trigger points: manual therapy for interstitial cystitis and the urgency–frequency syndrome. J Urol. 2001;166:2226-2231.
Zondervan K., Yudkin P., Vessey M., et al. The community prevalence of chronic pelvic pain in women and associated illness behavior. Br J Gen Pract. 2001;51:541-547.