4 The variety of reflex points
Are all tender points trigger points?
Distinguishing features of myofascial trigger points
Mechanotransduction, fascial pathways, and endocannabinoid influences – some recent advances
Acupuncture points and their morphology
Acupuncture and applied kinesiology
Alarm points, Associated points, Akabane points
Bennett’s neurovascular reflex points
Reflex patterns and areas
In this chapter some of the major systems that have identified and classified reflex areas on the body surface will be discussed, because many of the ‘points’ that these identify are bound to be accessed during the application of NMT in an assessment or a treatment mode.
Osteopathic physician Eileen DiGiovanna (1991) states: ‘Today many physicians believe there is a relationship among trigger points, acupuncture points and Chapman’s reflexes. Precisely what the relationship may be is unknown.’ She quotes from a prestigious osteopathic pioneer, George Northup (1941), who stated as far back as 1941:
One cannot escape the feelings that all of the seemingly diverse observations (regarding reflex patterns) are but views of the same iceberg the tip of which we are beginning to see, without understanding either its magnitude or its depth of importance.
Awareness of the reflex potential of the body surface widens the therapeutic potential of NMT, although deciding which of the many possible applications of reflex activity to utilize in diagnosis or treatment can be a daunting task. The discussion in this text of these reflex systems and classifications should not be taken as indicating recommendation for their use, merely recognition of the fact that they are widely used, and that NMT offers an additional means of access and employment of their potential.
Felix Mann (1983), one of the pioneers of acupuncture in the West, entered the controversy as to the existence, or otherwise, of acupuncture meridians (and indeed acupuncture points). Mann, in an effort to alter the emphasis that traditional acupuncture places on the specific charted positions of points, stated:
McBurney’s point, in appendicitis, has a defined position. In reality it may be 10cms higher, lower, to the left or right. It may be one centimetre in diameter, or occupy the whole of the abdomen, or not occur at all. Acupuncture points are often the same, and hence it is pointless to speak of acupuncture points in the classical traditional way. Carefully performed electrical resistance measurements do not show alterations in the skin resistance to electricity, corresponding with classical acupuncture points. There are so many acupuncture points mentioned in some modern books, that there is no skin left which is not an acupuncture point. In cardiac disease, pain and tenderness may occur in the arm however this does not occur more frequently along the course of the heart meridian, than anywhere else in the arm.
Hence, Mann concludes, meridians do not exist, or – more confusingly perhaps – the whole body is an acupuncture point!
Leaving aside the validity of Mann’s comment, it is true to say that if all the multitude of points described in acupuncture, traditional and modern, together with those points described by Travell and co-workers, Chapman, Jones and Bennett (see later in this chapter), were to be placed together on one map of the body surface, we would soon come to the conclusion that the entire body surface is a ‘potential acupuncture point’.
This realization is supported by Speransky’s findings from the 1930s, as discussed in Chapter 3.
Are all tender points trigger points?
A number of respected researchers and clinicians are frequently in error when they describe localized soft tissue areas that palpate as sensitive, but that do not refer symptoms elsewhere, as trigger points.
Certainly a trigger point will always be palpable, and will always be sensitive to pressure, but then so will most other ‘points’, whether these be Chapman’s reflexes, Gutstein’s myodysneuria points, Jones’s tender points, or acupuncture alarm points. These, however, will not necessarily refer painful symptoms to distant sites in the obvious manner displayed by trigger points.
This is not to say that any ‘tender’ or sensitive point cannot become a trigger point, since, clearly, before it is active, a trigger point has to evolve, and in its earlier stages will be painful, sensitive or tender, but may at the time of palpation not be sufficiently sensitized and hyperreactive to refer pain and other symptoms. If a point ‘belonging’ to any of the various classifications discussed below does refer symptoms in the manner of trigger points, then it can be so classified and treated.
Distinguishing features of myofascial trigger points
(modified from Simons 2002)
• Active myofascial trigger points produce regional pain complaints and not bodywide pain and tenderness.
• Not all tender points are myofascial trigger points, but all myofascial trigger points are tender.
• Referred tenderness, as well as referred pain, is characteristic of a myofascial trigger point.
• All myofascial trigger points are associated with a taut band.
• Not all taut bands are palpable (requires sufficient palpation skill and accessibility).
• All active myofascial trigger points cause a clinical pain (sensory disturbance) that is familiar to the patient.
• Only an active myofascial trigger point, when compressed, reproduces the clinical sensory symptoms that are familiar to the patient.
• However, a latent myofascial trigger point produces no clinical sensory (pain or numbness) complaint that is familiar to the patient.
Some of the major ‘point’ classifications involving reflex activity, and with a diagnostic potential, are considered in this chapter, in alphabetical order (not in order of apparent importance).
Mechanotransduction, fascial pathways, and endocannabinoid influences – some recent advances
Before looking at a selection of point classifications, involving reflex activity, the evidence of recent research relating to the process of mechanotransduction requires a brief introduction, as does introduction of endocannabinoid influences.
We have seen earlier in this chapter that there exist in many individuals discrete localized areas that generate pain, and/or other symptoms (often at a distance), as a result of local or central sensitization.
It is therefore important to be able to demonstrate evidence that these can:
1. be identified via palpation, and
2. be manipulated/treated manually via stretching or compression – for example – or by tool assisted means (e.g. acupuncture).
Assessment/palpation will be investigated in Chapter 5, while therapeutic approaches will be described in Chapters 6, 7, 8, 9, 10 and 11.
But what are the mechanisms associated with influencing symptoms and tissues at a distance?
As we have seen, neurological explanations have been at the forefront of attempts to explain reflex influences. However, there have been other recent developments in our understanding of how manual treatment can influence distant tissues, for example via the biochemical and other processes involved in what is termed mechanotransduction; and also via the release of endocannabinoids.
Mechanotransduction
Burkholder (2006) notes:
There are many ways by which deformation of a myofiber might be converted to a biochemical signal. When a deformation is imposed on a muscle, changes in cellular and molecular conformations link the mechanical forces with biochemical signals, and the close integration of mechanical signals with electrical, metabolic, and hormonal signaling may disguise the aspect of the response that is specific to the mechanical forces. The mechanically induced conformational change may directly activate downstream signaling and may trigger messenger systems to activate signaling indirectly.
A veritable cascade of biochemical changes result from mechanical deformation of tissues, involving calcium, insulin and a variety of complex substances that signal to other tissues ‘downstream’.
It seems probable that such signalling can be modulated, directed, to achieve positive changes, via appropriate manual methods of treatment (Levin 2000).
Fascial communication
Closely linked to these ideas is an increased awareness of fascial connections that link distant, as well as local, areas of the body (Myers 2008, Huijing & Baan 2001).
Langevin et al (2005) have proposed fascia/connective tissue as a communication system:
Connective tissue may function as a previously unrecognized whole body communication system. Since connective tissue is intimately associated with all other tissues (e.g. lung, intestine), connective tissue signaling may coherently influence (and be influenced by) the normal or pathological function of a wide variety of organ systems … connective tissue functions as a body-wide mechanosensitive signaling network [involving] three categories of signals: electrical, cellular and tissue remodeling, each potentially responsive to mechanical forces over different time scales.
Khalsa et al (2005) report that ‘Langevin’s research describes a common feature of manual therapies – the application of mechanical forces to connective tissues. Immediate (viscoelastic and mechanotransduction) and delayed (remodeling) connective tissue effects of these forces may contribute to the mechanism of these therapies.’
Endocannabinoids
In the 1990s a new class of self-generated pain-relieving substances was identified in the body, the endocannabinoids. These substances mimic the pain-relieving and euphoria-generating effects of the use of cannabis, and help to explain its illegal use by many chronically pain-ridden individuals (Degenhardt 2007).
As McPartland & Simons (2007) explain:
The endocannabinoid (eCB) system, like the better-known endorphin system, diminishes nociception and pain, reduces inflammation in myofascial tissues, and plays a role in fascial reorganization. The overall role of the eCB system can be summarized as ‘resilience to allostatic load,’ a phrase synonymous with health. Practitioners wield several tools that upregulate eCB activity, including myofascial manipulation, diet and lifestyle [particularly exercise].
Summary
NMT (and other soft tissue approaches to treatment of somatic dysfunction) clearly ‘deform’ tissues (compression, shear, stretch, etc.), albeit briefly, and over and above the local effects on tissue, the signalling potential that follows remains an intriguing area for further research. At the same time endocannabinoid influences are likely candidates to explain at least some of the local and distant effects of manual treatment such as NMT.
Empirical clinical evidence certainly indicates that distant influences are achieved using NMT, and these current research areas appear to explain some of the mechanisms.
Acupuncture points
Soft tissue changes often produce organized discrete areas that act as generators of secondary problems. A repetitive question arises as to whether traditional acupuncture points are in fact the same as trigger points (Fig. 4.1).
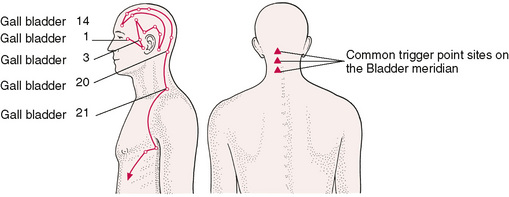
Figure 4.1A, B Location of some important acupuncture points on the head and neck. Research indicates that over 75% of defined acupuncture points are also sites of common trigger points.
The location of acupuncture points, with their fixed anatomical locations, are capable of corroboration by electrical detection, each point being evidenced by a small area of lowered electrical resistance.
When ‘active’, possibly due to reflex factors, these points become even more detectable, as the electrical resistance lowers further. The skin overlying them also alters and becomes hyperalgesic and not difficult to palpate as differing from surrounding skin. Active acupuncture points also become sensitive to pressure and this is of value to the therapist because the finding of sensitive areas during palpation or treatment is of diagnostic importance. Sensitive and painful areas that do not have detectable tissue changes as part of their make-up may well be ‘active’ acupuncture points, or tsubo, which means ‘points on the human body’ in Japanese (Serizawe 1976).
Not only are these points detectable and sensitive, but they are also amenable to treatment by direct pressure techniques. They therefore display, in almost all particulars, the same features as trigger points.
Acupuncture points and their morphology
Pain researchers Wall & Melzack (1989), and others (Travell & Simons 1992, Melzack et al 1977), maintain that there is little, if any, difference between acupuncture points and most trigger points.
Dorsher (2004), carefully compared the location of 255 trigger points, as identified by Travell and Simons, with 747 acupuncture points as identified by the Shanghai College of Traditional Medicine (Chen 1995):
The findings were that 92% of TPs had anatomically corresponding acupuncture points, 83% of these points had similar regional pain indications, and 87% of myofascial TPs had referred pain patterns that are identical or nearly identical to the corresponding acupuncture points’ meridian distributions.
The conclusion was: TPs are essentially a ‘rediscovery’ of the 2000-year-old acupuncture tradition (a subset of acupuncture points). As will be noted below, not all researchers or clinicians agree with these findings (Birch 2008).
The morphology of acupuncture points has been studied, notably by Bosey (1984).
Some of his major conclusions, in summary, are as follows:
• Points are situated in palpable depressions (‘cupules’).
• The skin (epiderm) over the point is a little thinner at the cupule level, under which lies a fibrous cone in which there is frequently found either a neurovascular formation, or simply a cutaneous neurovascular bundle.
• Free nerve endings are noted, and the presence, beneath the point, of Golgi endings and Pacini corpuscles is common.
• Connective tissues lie below at varying depths.
• Fascia and aponeurosis are noted and a passage of vessels and nerves, through the fascia, is very often found under the acupuncture point.
The practice of manipulating the needle in acupuncture imposes a degree of traction on the underlying (muscular) tissue, which imposes stimulation on underlying receptor organs. Fat is also a common factor in the morphology of points, and this, and the connective tissue, is thought to be a key factor in the achievement of the ‘acupuncture sensation’ that accompanies successful treatment. The conclusion reached is that a number of tissues are simultaneously affected needling – a phenomenon confirmed by Langevin (2006), supporting the mechanotransduction mechanisms discussed earlier.
Some points, when dissected, showed that neurovascular structures lie immediately below the point, which could account for the particular effects noted by such points being treated. This is of interest to those using Bennett’s neurovascular points. The implications for those practitioners not employing needles, and who rely on pressure techniques in order to provide stimulus or sedation to such areas, is that, if accurately applied, the effects of pressure should be identical (to needle acupuncture), especially in relation to pain control.
Acupuncture and applied kinesiology
An attempt to correlate the various reflex systems and methods has been made by the American chiropractor George Goodheart. His system of applied kinesiology involves testing muscle groups for weaknesses and then, depending upon the results of such tests, using various massage and pressure techniques applied to specific locations (points) in order to normalize function. These points correspond to Chapman’s reflexes, acupuncture points and other less well known reflex systems. Many of Goodheart’s techniques, theories and methods support and utilize methods that are in line with NMT.
Acupressure and pain thresholds
It has been shown that pain thresholds can be dramatically raised by pressure techniques applied to specific points. Researchers at the Peking Medical College conducted complex experiments which demonstrated that finger pressure acupuncture produced a rise of 133% in pain threshold of rabbits (using radiant heat as the painful stimulus). When cerebrospinal fluid was perfused from one rabbit to another after such experiments, the recipient rabbit was found to have achieved a rise in pain threshold of up to 80%. This suggested the presence of hormone-like substances produced by the brain in response to the original acupressure stimulus. These substances are now known to be enkephalins and endorphins, and these play a role in NMT pain control. The point used in these tests was equivalent to the acupuncture point known as Bladder 60, posterior to the ankle (externally) and just anterior to the Achilles tendon.
Acupuncture points and trigger points: not all agree that they are the same phenomenon
As outlined earlier, because they spatially occupy the same positions in at least 75% of cases (Wall & Melzack 1989, Dorsher 2004, Dorsher & Fleckenstein 2008) there are strong indications that trigger points are in fact no more than active acupuncture points. Wall & Melzack (1989) have concluded that: ‘trigger points and acupuncture points when used for pain control, though discovered independently and labelled differently, represent the same phenomenon’.
Baldry (1993) does not agree, however, claiming differences in their structural make-up. He states:
It would seem likely that they are of two different types, and their close spatial correlation is because there are A-delta afferent-innervated [fast transmitting receptors with a high threshold and sensitive to sharply pointed stimuli or heat produced stimulation] acupuncture points in the skin and subcutaneous tissues immediately above the intramuscularly placed, predominantly C afferent-innervated [slow transmitting, low threshold, widely distributed and sensitive to chemicals – such as those released by damaged cells – mechanical or thermal stimulus] trigger points.
Clearly, stimulation of an area that has, beneath the contacting instrument or digit, both an acupuncture and a trigger point will influence both types of neural transmission and both ‘points’. Which route of reflex stimulation is producing a therapeutic effect, or whether other mechanisms altogether are at work – endorphin or endocannabinoid release, as examples – is therefore open to debate. This debate can be further widened if we include the vast array of other reflex influences identified by other systems and workers, as discussed later in this chapter.
Whereas traditional oriental concepts focus on ‘energy’ imbalances in reaction to acupuncture points, there exist also a number of Western interpretations.
Melzack et al (1977) have assumed that acupuncture points represent areas of abnormal physiological activity, producing a continuous low-level input into the central nervous system (CNS). They suggested that this might eventually lead to a combining with noxious stimuli deriving from other structures, innervated by the same segments, to produce an increased awareness of pain and distress. They found it reasonable to assume that trigger points and acupuncture points represented the same phenomenon, having found that the location of trigger points on Western maps, and acupuncture points used commonly in painful conditions, showed a remarkable 75% correlation in position.
It is interesting that the link between the source of pain or tender points, and the referred area of pain noted in trigger points, in many instances seems to travel along the routes of traditional acupuncture meridians, but certainly not always. Spontaneous pain in such a point, according to acupuncture tradition, indicates the need for urgent attention. It is not the intention of this book to provide instruction in acupuncture methodology, nor necessarily to endorse the views expressed by traditional acupuncture in relation to meridians and their purported connection with organs and systems. However, it would be short-sighted to ignore the accumulated wisdom that has led many thousands of skilled practitioners to ascribe particular roles to these points, for example Alarm, Associated and Akabane points as described in this chapter.
As far as a manual therapy is concerned, there seems to be value in having awareness of the reported roles of particular acupuncture points, and of incorporating this into diagnostic and therapeutic settings.
As we palpate and search through the soft tissues, in basic neuromuscular technique, we are bound to come across areas of sensitivity that relate to these points. They are also often found to overlap with neurolymphatic and neurovascular points, as described elsewhere in this text.
For example, reflex number 19 in Chapman’s reflexes, which relates to the urethra, is identical to the neurovascular point of the bladder, and the acupuncture alarm point of the Bladder meridian. Careful comparison shows many such overlaps.
General guidance as to how to treat acupuncture points, which are sensitive, must relate to whether a stimulating or sedating effect is desired. The body often seems to utilize therapeutic stimulation to its best advantage.
Selye has shown us (see Ch. 1) that homeostatic mechanisms are at work, so that any stimulus, if appropriate and not excessive, can result in a beneficial response. In accord with the methods used in treating neurolymphatic and neurovascular points (described elsewhere in this chapter) it is suggested that, to some extent, the ‘feel’ of the tissues be allowed to guide the practitioner. A change (in the sense of a release of tension, or a softening, or a sensing of a gentle pulsation in the tissues) is often an indication of an adequate degree of therapy. In order to sedate what is an overactive point, up to 5 minutes of sustained or intermittent pressure, or rotary contact, may be required.
For stimulation, the timing could involve between 20 seconds and 2 minutes. By this time, some degree of change should be palpable. As must be clear, if pressure is sustained beyond a certain point quite the opposite effect will be achieved. This is a common natural phenomenon which occurs in response to all factors in life that are initially stimulating. If prolonged, they become enervating or exhausting, and in terms of therapy this is undesirable unless anaesthesia is required.
A short cold (water) application, for example, will stimulate, whereas a long one will sedate, and too much can kill. The words of Speransky and Selye should be recalled and the minimum effort used, consistent with achieving a response.
We have noted previously that many of the different reflex systems have points that seem to be interchangeable, and that many of these are traditional acupuncture points. In terms of local pain, the view of Chifuyu Takeshige (Takeshige 1985), Professor of Physiology at Showa University, is that: ‘The acupuncture point of treatment of muscle pain is the pain-producing muscle itself.’
Respected acupuncture clinicians, such as George Ulett, suggest that ‘acupuncture points are nothing more than time honoured muscle motor points’. Professor C. Chan Gunn, however, finds this too simple an explanation, and states: ‘Calling acupuncture points “motor points” or “myofascial trigger points” is too simple. They are Golgi tendon organs.’ These, and other researchers, are quoted by Stephen Botek, Assistant Professor of Clinical Psychiatry, New York Medical College (Ernst 1983).
Botek (1985) believes that ‘myofascial needling’ is the term of choice to define the type of acupuncture that dispenses with traditional explanations as to the effects of acupuncture. The points utilized in one study were Large Intestine 4 (Hoku) in the web between thumb and the first finger, and Stomach 36 (Tsu san li) below the knee. The study recorded skin temperature of the face, hands and feet. It was found that, compared with a resting period, both manual and electrical stimulation of both points induced a general warming effect. This was immediate in the face (Lewith & Kenyon 1984) and appeared after 10–15 minutes in hands and feet. The temperature increase was notably more marked after manual acupressure than after electrical stimulation. Manual stimulation of these points was shown to be more effective than other forms of stimulation.
Lewith & Kenyon (1984) point to a variety of suggestions having been made as to the mechanisms via which acupuncture, or acupressure, achieves pain-relieving results. These include neurological explanations such as the ‘gate control theory’. This, and variations on this theme, look at the various structures of the CNS and the brain in order to define the precise mechanisms involved in acupuncture’s pain-relieving action.
This, in itself, is seen to be an incomplete explanation, and humoral (endorphin, endocannabinoid release, etc.) and psychological factors, are also shown to be involved in modifying the patient’s perception of pain.
A combination of reflex and direct neurological elements, as well as the involvement of a variety of secretions, such as enkephalins and endorphins, is thought to be the modus operandi of acupressure, and probably of all of the various systems of reflex activity discussed in this section (neurolymphatics, etc.).
Many of the points of referred pain and tenderness used in Western medical diagnosis are also acupuncture points, for example:
• Head’s zones could be shown to include most acupuncture points, especially the Alarm and Associated points (given below).
• The points noted as being ‘tender’ in appendicitis, such as McBurney’s, Clado’s, Cope’s, Kummel’s, Lavitas’s, are on the Stomach, Spleen and Kidney meridians of traditional acupuncture, and these are used by acupuncturists in treating appendicitis.
• Patients with a gastric ulcer produce tenderness at a site known as Boas’ point, and this is sited precisely on Bladder point 21, which is the Associated point of the Stomach meridian.
• Brewer’s point, in Western medicine, is noted in kidney infection, and this is Bladder point 20, the Associated point for the Spleen (in traditional acupuncture this has a controlling role over water, the element of the kidneys).
The degree of overlap between these well-known points can also be noted when comparing other classification systems of points.
Ah Shi points
Acupuncture methodology also includes the treatment of points that are not listed on the meridian maps, and that are known as Ah Shi points. These include all painful points that arise spontaneously, usually in relation to particular joint problems or disease. For the duration of their sensitivity they are regarded as being suitable for needle or pressure treatment. These points may therefore be thought of as identical to the ‘tender’ points described by Lawrence Jones in his strain/counterstrain method, discussed later in this chapter.
Alarm points, Associated points, Akabane points
There are, in traditional acupuncture, a number of key points that are most likely to become painful in relation to particular visceral dysfunction. These have been classified as Alarm points. They are presented below, and the following general information may make their employment easier:
• The Alarm points are found only on the ventral surface of the body, each point being associated with one of the 12 meridians and its functions. Six of the points are on the midline, the others are bilateral. Tenderness elicited by palpation of an Alarm point may indicate dysfunction of the organ related to the point. In traditional acupuncture, if sensitivity is noted on light pressure, there is an associated energy deficiency. If heavy pressure is required, the condition relates to an energy excess.
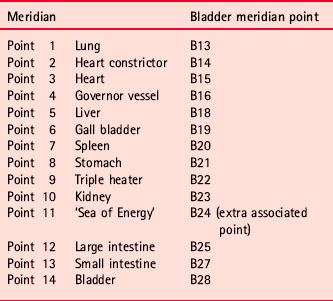
• Associated points lie on the back of the body, and these are all on the Bladder meridian, which runs parallel to the spine, bilaterally. Each Associated point is related to one of the meridians and its function. The same assumed relationship with energy deficit or excess exists, as in Alarm points (sensitivity on light pressure = deficiency, and on heavy pressure = excess). There are also a few extra Associated points, as illustrated (see Fig. 4.3). Spontaneous pain at any of these listed points indicates a disorder in that meridian, and in its associated organ or function.
• Akabane points are found on the fingers and toes, being the terminal points of the meridians. Sensitivity of any of these is said to relate to dysfunction and imbalance of energy in that meridian. Electronic measurement of these points (Melzack et al 1977) is performed in a number of modern electroacupuncture systems such as electroacupuncture according to Voll (EAV). Manual testing is common, and was obviously the method used before electrical methods arrived on the scene. These points are all bilateral.
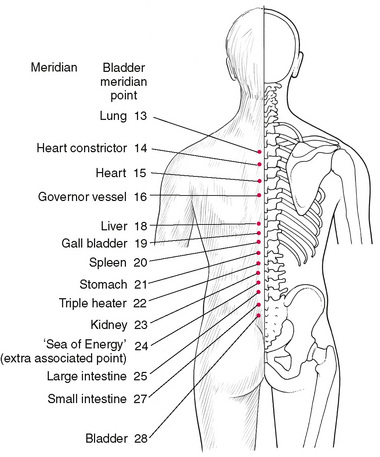
Figure 4.3 Location of Associated points, which lie on the dorsal surface of the body slightly lateral to the median line bilaterally. If spontaneous pain develops in any associated point, the allied meridian is thought to be involved. If light pressure produces tenderness, an ‘energy deficiency’ is considered to exist; if heavy pressure produces tenderness, an ‘energy excess’ is assumed. An understanding of the organs and functions associated with particular meridians is necessary in order to utilize these points therapeutically or diagnostically.
Location of Alarm points
Alarm points (Table 4.1, Fig. 4.2) are on the anterior surface of the body. Spontaneous pain at any point is considered to indicate a disorder of the affiliated meridian. If tenderness is elicited on light pressure, a deficiency of energy in the meridian is assumed, whereas tenderness elicited on heavy pressure indicates an excess of energy in the meridian.
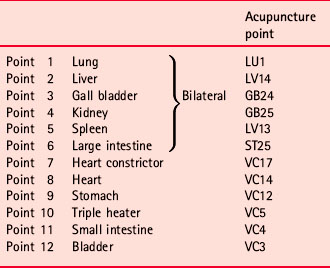
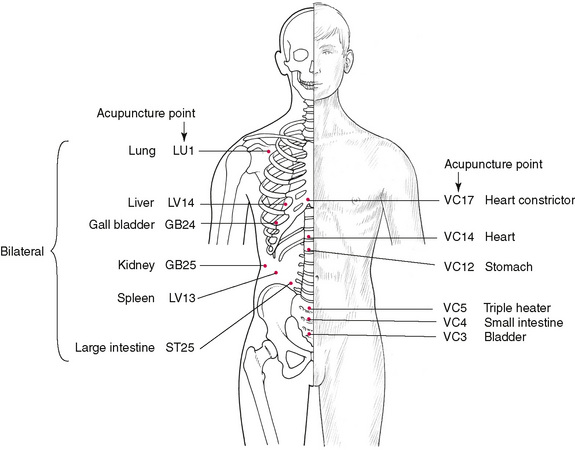
Figure 4.2 Location of Alarm points, which lie on the anterior surface of the body. If spontaneous pain develops in any alarm point, the associated meridian is thought to be involved. If light pressure produces tenderness, an ‘energy deficiency’ is considered to exist; if heavy pressure produces tenderness, an ‘energy excess’ is assumed. An understanding of the organs and functions associated with particular meridians is necessary in order to utilize these points therapeutically or diagnostically.
These are reflex points for meridian function, and awareness of the roles apparently played by the various meridians in body energy economics is necessary to evaluate the significance of reactions that produce tenderness in Alarm points.
Location of Associated points
Associated points are on the dorsum of the body (Fig. 4.3). Spontaneous pain is thought to indicate a disorder in the meridian associated with it. Tenderness elicited on light pressure indicates a deficiency in energy in that meridian, and tenderness elicited on heavy pressure indicates an excess of energy in the associated meridian. These points are all on the Bladder meridian and their associations are given in Table 4.2. The points are slightly lateral to the median line bilaterally and are also reflex points for the meridians with which they are associated.
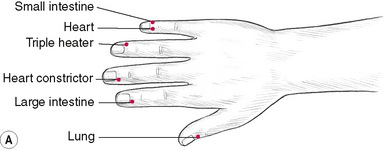
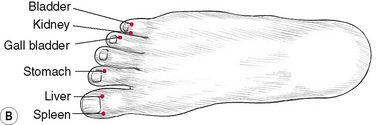
Location of Akabane points
Akabane points (Table 4.3, Fig. 4.4) represent the terminal points of the meridians. Sensitivity of these is thought to relate to imbalance in the energy of the meridian. Comparative sensitivity shows relative imbalance in organ (energy) systems. Manual or electronic testing is possible.
| Points on feet | Points on hands |
|---|---|
| 1. Spleen | 7. Large intestine |
| 2. Liver | 8. Heart constrictor |
| 3. Stomach | 9. Triple heater |
| 4. Gall bladder | 10. Heart |
| 5. Kidney | 11. Small intestine |
| 6. Bladder | 12. Lung |
Bennett’s neurovascular reflex points
A wide degree of clinical experience resulted in an American chiropractor, Terrence Bennett, reaching the conclusion that there was a group of previously unknown reflexes available for diagnostic and therapeutic use, which he termed neurovascular reflexes. He described his work in a series of lecture notes, which were compiled and published by Ralph Martin, after Bennett’s death, as Dynamics of Correction of Abnormal Function (Martin 1977). The major points are listed in Chapter 5, which deals with diagnostic procedures.
Bennett describes the tissues that are palpated as altered in texture, being contracted or indurated, in much the same way as Chapman’s reflexes (described below). His method of treatment calls for a slight degree of pressure, which he describes as ‘only minimal, enough to render the tissues semi-anaemic, which is adequate stimulus’.
 Experience indicates that the light pressure should be accompanied by slight stretching of the skin. In accordance with the views of Karel Lewit (1992), gentle stretching of the skin induces reflex activity when hyperalgesic (sensitized) skin zones are used therapeutically (see Ch. 5). When hyperalgesia occurs, skin becomes less elastic, with greater adherence to the underlying fascia and with lowered resistance to electricity.
Experience indicates that the light pressure should be accompanied by slight stretching of the skin. In accordance with the views of Karel Lewit (1992), gentle stretching of the skin induces reflex activity when hyperalgesic (sensitized) skin zones are used therapeutically (see Ch. 5). When hyperalgesia occurs, skin becomes less elastic, with greater adherence to the underlying fascia and with lowered resistance to electricity.
In Bennett’s system the skin is stretched with the minimum of force, so as to take up the slack, by the fingertips being drawn lightly apart. In most cases, if the area involves any degree of soft tissue dysfunction, a lack of anticipated elasticity will be noted in the skin as this distraction takes place. By maintaining the slight stretch on the tissues (in effect a ‘mini’ myofascial release), a yielding occurs, and it is after this that a pulsation sensation should normally be felt. John Thie (1973) describes this pulsation sensation thus:
A few seconds after contact is made, a slight pulse can be felt, at a steady rate of 70 to 74 beats per minute. This pulse is not related to the heartbeat, but is believed to be the primitive pulsation of the microscopic capillary bed, in the skin.
Bennett insisted that the contact be maintained until a response was noted in the form of the tissue altering, relaxing and, most importantly, until the operator became aware of the presence of pulsation. This could arrive within a few seconds or take some minutes to emerge, depending on the patient and his or her condition. Bennett termed the pulsation felt as the ‘arteriole pulse’ because, he stated:
It is the beginning of the system, at the junction of the artery and the arteriole, that controls the metabolism. The sensation of pulsation is essential … It has to be there, or else we are not accomplishing anything.
Together with this, the change in tissue feel is important:
The tissues under your fingers begin to relax as you work for a few moments; you sense the degree of tension releasing. When it releases that is all you can do.
Some points are purely diagnostic, others are used for treatment, and some are both.
For example, the coronary reflex in the 2nd thoracic interspace on the left, which is a palpable area of tissue change and which is sensitive to the patient, is only diagnostic (not illustrated). Awareness of Bennett’s reflex areas may be found to be a useful addition to the range of available therapeutic and diagnostic knowledge. In using NMT in its diagnostic mode, the tissues being evaluated will yield a multitude of sensitive points. Some of these may correlate with Bennett’s findings, and they may then be used as part of an overall assessment of the nature of the dysfunction affecting the patient. They may, of course, also be used, as Bennett intended, as a system in their own right, for assessing and treating visceral and functional physiological changes and pathology. A number of Bennett’s points have been incorporated into the methods of applied kinesiology, notably the points on the cranium, which are used for treating emotional disturbances.
Among the cautions issued by Bennett are:
• Do not overtreat the points on the cranium (2–3 minutes is a maximum).
• In hyperthyroid patients, do not treat the thyroid and pituitary reflexes at the same visit (one should be treated, and alternated with the other at a subsequent visit).
• If the heart is enlarged then the 3rd rib, at the mid-clavicular line, should not be treated.
• Aortic sinus reflex should be treated before any of the brain reflexes are contacted.
• If the ovary is being treated, the thyroid should receive prior attention.
A list of Bennett’s reflex points can be found in Chapter 5, which considers diagnostic applications of NMT.
Chapman’s reflexes
In the 1930s, Chapman and Owens described a ‘neurolymphatic’ reflex pattern, now widely used in osteopathic and chiropractic methodology. Chaitow (1965) discussed these reflexes as follows:
The reflexes of Chapman that I intend to discuss are not the whole picture – being only a part of the visible portion of the iceberg – but of immense value nonetheless. Drs Chapman and Owens first reported on Chapman’s original findings in the late 1930s. A revised edition of their work has been published by the Academy of Applied Osteopathy. The surface changes of a Chapman’s reflex are palpable. They may best be described as contractions located in specific anatomical areas and always associated with the same viscera. In describing each organ reflex Chapman normally indicated tissue reflex areas, occurring anteriorly and posteriorly. These reflexes found in the deep fascia are described as ‘gangliform’ contractions. These contractions vary in size from a pellet to a large bean and are located anteriorly in the intercostal spaces near the sternum. Similar tissue changes are found in those reflexes occurring on the pelvis. The tissue changes found in reflexes located on the lower extremities are described as ‘stringy masses’ or ‘amorphous shotty plaques’. Those reflexes occurring posteriorly along the spine, midway between the spinal processes and the tips of the transverse processes are of a more oedematous nature.
Characteristics
Patriquin (1997) describes the characteristics of Chapman’s reflexes as:
Sometimes they are described as feeling like small pearls of tapioca, lying, partially fixed, on the deep aponeurosis or fascia.
Clinical value of the reflexes
Because the location of these palpable tissue changes is relatively constant in relation to specific viscera, it is possible to establish the location of pathology without knowing its nature. The value of these reflexes is threefold:
1. As diagnostic aids – Patriquin (1997) points out that some of the reflexes, such as that for appendix (tip of 12th rib on the right; see point 38 on Fig. 5.8B) are invaluable in helping with differential diagnosis when faced with right lower abdominal pain: ‘Today, Chapman’s reflexes are more likely to be used as an integral part of osteopathic physical examination than as a specific therapeutic intervention.’
2. They can be utilized to influence the motion of fluids, mostly lymph.
3. Visceral function can be influenced through the nervous system. ‘[The] reflexes can be clinically manipulated to specifically reduce adverse sympathetic influence on a particular organ or visceral system … patients with frequent bowel movements from the effects of IBS report they have normal or near normal function for days to months after soft tissue treatment over the iliotibial bands and/or the lumbosacral paraspinal tissues and associated Chapman’s reflexes’ (Patriquin 1997). (See point 24, anterior and posterior, in Figs 5.8A and 5.8C.)
Mechanism of the reflexes
Regarding the mechanism whereby these reflexes act, it would appear that, in so far as the intercostal reflexes are concerned, stimulation of the receptor organs that lie between the anterior and posterior layers of anterior intercostal fascia acts through the intercostal nerve, which enervates the external and internal intercostal muscles and thus, through the sympathetic fibres, affects the intercostal arteries, veins, lymph nodes, etc. Stimulation thus causes afferent and efferent vessels draining these tissues to increase or decrease, permitting lymph flow to be increased or decreased, thus affecting the drainage of the entire lymph system in the area. Through the sympathetic fibres associated with these tissues, the lymph nodes of the vital organs are also affected.
Explaining results of neuromuscular technique
These reflexes seem to offer explanations for the sometimes startling results obtained through neuromuscular technique. Stanley Lief placed great emphasis on normalizing the tissues of the intercostal spaces and the paravertebral areas – sites of many major neurolymphatic reflexes. He also stressed the importance of not overtreating, a consideration that cannot be repeated too often.
Research evidence supports Chapman’s reflex usefulness
• Caso (2004) reported a case study involving chronic constipation and low back pain. Use of Chapman’s NL reflexes was seen to be useful diagnostically as well as therapeutically. ‘The rather remarkable outcome from the application of this relatively simple, yet valuable, diagnostic and therapeutic procedure represents a thought-provoking impetus for future study and clinical application.’
• Lines et al (1990) treated 30 asymptomatic individuals, on four separate occasions, employing stimulation of the neurolymphatic reflexes theorized to relate to the diaphragm. Spirometric assessment of respiratory function before and after each treatment was performed. Measurements of forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) over the whole sample showed no significant improvement following the treatment regimen. However eight of the 30 subjects had lower than predicted initial FVC and FEV1 values. When the results for the group of eight subjects were analysed separately, it was found that a significant improvement was attained from the first pretreatment FVC to last posttreatment.
• In a trial conducted to assess the effects of forms of manipulation on blood pressure, one of the methods used was stimulation of a Chapman’s reflex (Mannino 1979). A specific effect attributable to this treatment was noted. The point chosen for treatment was the one related to adrenal function. The trial involved treatment of this point, or a sham point, in which pressure was applied to either the real or a false point, for a total of 2 minutes, in a make-or-break circular motion. The point is located in the intertransverse space, on both sides of the 11th and 12th thoracic vertebrae, midway between the spinous processes and the tips of the transverse processes (see point 37 on Fig. 5.8F). The sham treatment involved the area between the 8th and 9th thoracic vertebrae, which relates to small intestine problems, and would have no effect on the sort of condition being assessed in these trials. The results showed no immediate effect on blood pressure, but did indicate fascinating alteration in aldosterone levels and subsequent blood pressure drop. Abnormalities in aldosterone levels have been shown in populations with essential hypertension. Following treatment of the reflexes there was a demonstrable and consistent fall in aldosterone levels within 36 hours of stimulation of the Chapman reflex for the adrenals, but no change at all in the levels when the sham points were stimulated. A drop of 15 mmHg systolic and 8 mmHg diastolic was noted some 36 hours after treatment of the adrenal points. The delay in response suggested that the treatment had a tendency to interrupt, or damp down, a feedback to the adrenal medulla by the sympathetic nervous system (Patriquin 1997).
Nimmo’s dismissal of the Chapman reflexes
An element of disinformation has emerged regarding Chapman’s neurolymphatic reflexes.
Vannerson & Nimmo (1971) writing in The Receptor – the journal of the organization that used (in the 1960s) to teach Nimmo’s receptor-tonus technique (see Ch. 2) – stated:
Research has not borne out the presumption [by Chapman] of a neurolymphatic reflex. Muscle fibres, which alone have the specific function of constricting vessels, do not exist in the walls of lymph vessels, except for a few fibres in the thoracic duct, and a few large trunks. These are sparsely located, and have little effect in lymph fluid propulsion.
These two authors then deride Chapman’s assertion that the reflexes could exist at specific sites, an idea that they call ‘fantastic’.
Vanneron & Nimmo’s first point is in contradiction to Gray’s Anatomy (Gray 1973), which tells us that lymph moves in a number of ways. Filtration occurs, generated by filtration of fluid from the capillaries. There is also a degree of movement engendered by contraction of surrounding muscles, which compress lymph vessels, the movement of which is determined by the presence of valves. This muscular contraction is dependent upon normal activity, and muscular contraction–relaxation sequences. Lymph is further capable of being moved, in such regions, according to Gray, by massage movements. Pulsating arterial vessels, in close proximity, also assist lymph movement, as does respiratory movement. Also in contradiction of Vanneron & Nimmo, Gray states: ‘The smooth muscle in the walls of the lymphatic trunks is most marked just proximal to the valves; stimulation of sympathetic nerves accompanying the trunks, results in contraction of the vessels; the intrinsic muscle of the vessels thus probably aids the flow of the lymph.’
In 1979, rhythmic pulse waves were recorded from the lymphatic vessels of five healthy, upright, motionless males at a rate of 8–10 per minute, asynchronous with respiration or leg movement (Oszeweski & Engeset 1979). Degenhardt & Kuchera (1996) describe the process as follows: ‘The regulation of the intrinsic contractility of the lymphatic system is based on transmural distension of the vessel walls and neural and humoral mediators.’
The physiology of the lymphatic system is quite complex. Research has only begun to demonstrate the many factors that influence lymphatic flow. The extrinsic compression of the myofascia on the lymphatics has been the focus of many manipulative techniques … Studies now consistently demonstrate contractility in the lymphatic vessels. This intrinsic pumping has been shown to be under autonomic control, modulated locally by soft tissue chemicals and systemically produced hormones. Currently it appears that intrinsic contractions have more influence on lymph flow than extrinsic forces.
This evidence, therefore, suggests that the term ‘neurolymphatic reflex’, as described by Chapman, may indeed be an accurate description of the phenomenon.
Vanneron & Nimmo’s second observation (relating to the specificity of the reflex sites) may be more valid, especially if anatomical individuality is taken into account. Points of the body surface are never likely to be precisely identifiable by description of anatomical position. However, a general identification as to site is possible. McBurney’s point, for example, if present in appendicitis, is usually located within a few degrees of its commonly described location. There are exceptions, of course, and in the inscrutable manner of the Orient, the Chinese have taken this well into account, in describing the locations of acupuncture points. The invention of the ‘human inch’, which takes account of the individual anatomical proportions of each person, allows for such individualization. In terms of the charts and maps to be found in this text, the same factor should be borne in mind. The positions are approximate, because variations exist from person to person.
Dysfunction in soft tissues is, however, palpable, and not dependent upon maps. Thus, the general guidelines provided by charts are useful, but cannot take the place of palpatory skills.
A complete illustrated list of Chapman’s reflexes is found in Chapter 5, which deals with diagnosis and treatment using NMT.
Palpating for, and treating, the neurolymphatic points
Kuchera (1997) suggests: ‘If Chapman’s [neurolymphatic] myofascial tender points are to be tested, palpate them early in the examination because motion of the myofascial tissues in their area decreases their sensitivity. In this case their diagnostic clue, tenderness with palpation, may not be evident.’
If, during NMT assessment mode application to the anterior thorax and abdominal region (see Ch. 7) unusual tenderness is noted in the region of the umbilicus, this may relate to bladder, kidney or adrenal dysfunction (see points 15, 16 and 37 on Figs 5.8A & 5.8B); similarly, tenderness in the area if an anterior point is noted in the left fifth or sixth intercostal interspace (see points 13 and 14 on Fig. 5.8A), the patient may usefully be asked about, for example, stomach or digestive symptoms.
Treatment of the lymphatic aspects of these dysfunctional organs or functions (should their existence be corroborated by other clinical evidence) might usefully include gentle applications of rotary pressure to the posterior points, in the sequence described in Chapter 5.
Arbuckle (1977) writes of Chapman’s reflexes:
The diagnostic value of these reflexes is amazing. For instance, a female having severe pain in the right lower quadrant of the abdomen, presents several possibilities, but the offending organ may well be located by means of the reflexes, the positive one showing whether the disturbance is due to appendix, cecum, tube or ovary. With a degree of understanding of the interrelation of the endocrine glands, and of the importance of the lymphatics and the autonomic distribution, the therapeutic value of these considerations can be shown clinically. There is a definite sequence, which must be followed, in the management of these reflexes, to produce desired results, and, if not so applied, just as surely as the misapplication of any other therapy, further confusion of the body mechanism will result.
Connective tissue massage/manipulation
Another system that uses reflex effects diagnostically as well as therapeutically is connective tissue massage (CTM). CTM involves ‘rolling’ (or stretching using shear forces, or lifting) the tissues in order to achieve reflex and local effects.
Citak-Karakaya (2006) evaluated the use of CTM on 20 female patients with fibromyalgia (FMS). The results showed that:
Statistical analyses revealed that pain intensity, impact of FMS on functional activities, and complaints of non-restorative sleep improved after the treatment program.
Additional studies using CTM have demonstrated benefit in cases of:
• Migraine (Akbayrak et al 2001)
• Tension-type headache (Akbayrak et al 2002, Demiturk et al 2001)
• Fibromyalgia (Citak et al 2001)
• Raynaud’s disease (Demiturk et al 2000)
• Autonomic imbalance (Reed 1988)
• Anxiety (McKechnie A et al 1983).
CTM: Method and mechanism
According to Ebner (1962), the palpable reflex tissue changes that are identified in diagnosis and treatment involving CTM, can take any of the following forms:
The common ‘zones’ of influence involving such changes are illustrated and discussed further in Chapter 5 (see Fig. 5.3). The digital strokes used in CTM pull and stretch the tissues, and it is suggested that the method’s effectiveness is based on a viscerocutaneous reflex.
Bischof & Elmiger (1960) explain:
The specific mechanical stimulation of the pull on connective tissue seems to be the adequate stimulus to elicit the nervous reflex. Connective tissue massage/manipulation acts first on the sympathetic terminal reticulum in the skin. The smallest branches of the autonomic nervous system contact the impulses activated by the pulling strokes to the sympathetic trunk and the spinal cord. The impulses travel from the skin either through a somatosensory spinal nerve via a posterior root ganglion to the grey matter or over the vascular plexus to the same segmental sympathetic ganglion or to the ganglion of the neighbouring segment, through the ramus communicans albus to the posterior root and grey matter of the spinal cord. They terminate either directly or by means of the internuncial neurons at the efferent autonomic root cells.
In the efferent pathway the impulses travel from the autonomic lateral horn, or the intermediolateral column, over the anterior root, ramus communicans albus, to the segmental sympathetic ganglion or to the ganglion of the neighbouring segment and finally to the diseased organ. The origin of the connective tissue reflex zones and the influence of the CTM depend on the relationship between the function of the internal organs, vessels, and nerves as well as the tissues of the locomotor apparatus, which descend from the same metamere.
Some of the reactions to CTM are normal autonomic responses such as pleasant fatigue, bowel movements and diuresis. Oedema is markedly reduced and hormonal distribution is seen to achieve a degree of balance. Aspects of CTM are similar to those of NMT, and the ‘skin rolling’ methods used in some body areas are virtually identical in application. The effects are therefore interesting from a comparative point of view.
Jones’ tender points (Fig. 4.5)
Figure 4.5 Location of Jones’ tender points, which are bilateral in response to specific strain (acute or chronic) but are shown on only one side of the body in these illustrations. The point locations are approximate and will vary within the indicated area, depending upon the specific mechanics and tissues associated with the particular trauma or strain.
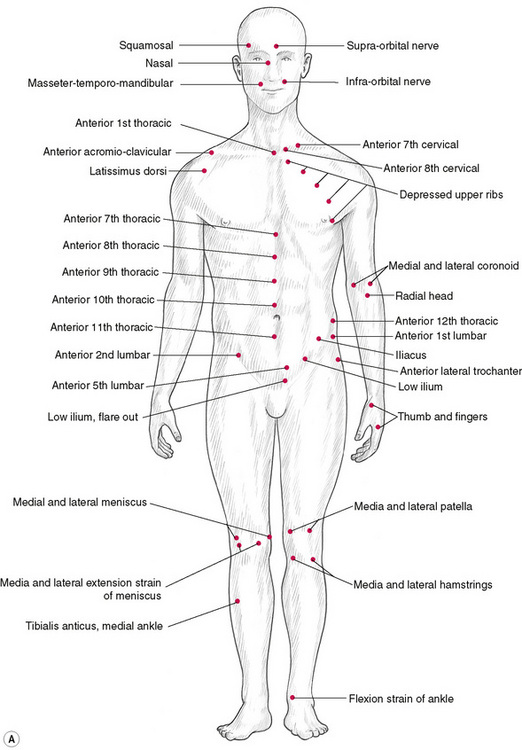
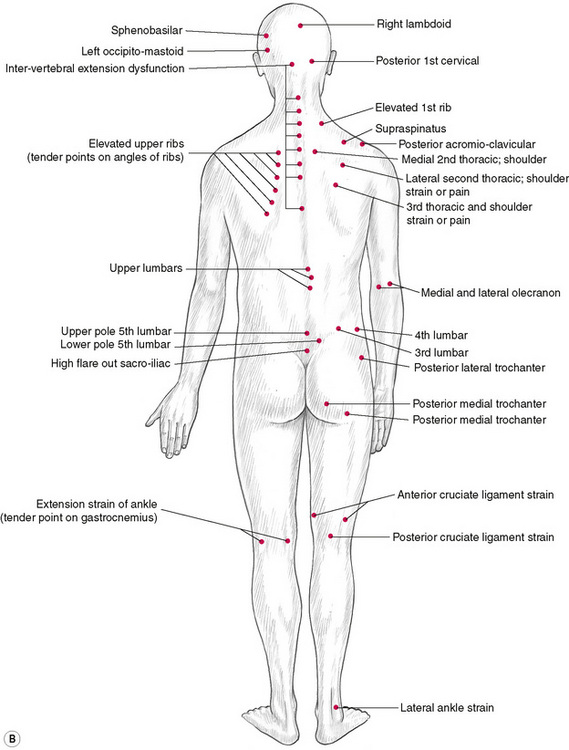
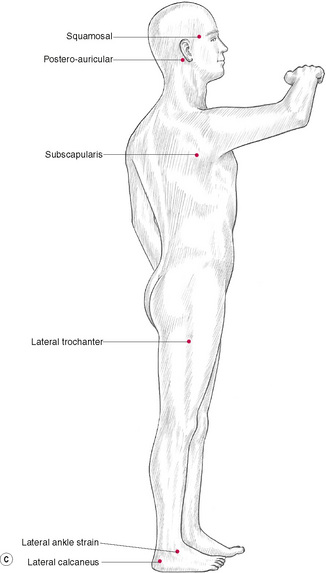
Figure 4.5C Jones’ points on the lateral body surface, commonly relating to strains involving side-bending or rotation.
In his evolution of the ‘strain and counterstrain’ (SCS) functional manipulative approach to the normalization of hypertonicity, Lawrence Jones described a series of ‘points’ that he had identified. These sensitive areas were, Jones discovered, related to specific strains and stresses in the musculoskeletal system, and were used by the therapist as monitors while the areas were being guided into a position of ease, during which process there was both a reduction in sensitivity in the palpated tender point as well as a relaxation (increased ease) of the stressed tissues associated with it. The tender points as described by Jones and the methods of treating them fall within the umbrella term ‘positional release techniques’ (Chaitow 2001, D’Ambrogio & Roth 1997, Deig 2001). The methodology of SCS is summarized in Chapter 8, and is incorporated into the integrated (INIT) sequence for trigger point deactivation, as described in Chapter 9.
In many ways these ‘tender’ points, while sensitive to palpation, are not usually areas in which the patient was previously aware of pain. They are therefore similar to Ah Shi – spontaneously tender – points in traditional Chinese medicine (Chaitow 1991).
Significantly perhaps, as the area being treated is positioned in ‘ease’ so that tenderness vanishes from the tender point, a degree of ischaemic compression/inhibitory pressure/acupressure would be taking place. It is worth considering that the benefits noted, in terms of pain relief and reduction in contraction or spasm, could relate in some part to the resulting inhibitory/endorphin release action as well as to the subsequent improvement in circulation and possible neural influences, through the tissues and neurological modulation produced by the placing of the tissues into a situation of ‘ease’.
Periosteal pain points
(Adapted from Lewit 1992)
These painful areas (Table 4.4) usually relate to acute or chronic contraction of associated muscles and tendons.
Table 4.4 Periosteal pain points (adapted from Lewit 1992)
| Site | Muscular/joint implication |
|---|---|
| Pain on head of metatarsals | Dropped arch, flat foot |
| Spur on calcaneum (pain on pressure) | Tight plantar aponeurosis |
| Pain on tubercle of tibia | Tight long adductor/possible hip dysfunction |
| Pain on head of fibula | Biceps femoris tightness |
| Posterior superior iliac spine tenderness | Various possible implications, involving low back, gluteal and sacroiliac region |
| Lateral aspects of symphysis pubis | Adductors tight. Hip or sacroiliac dysfunction |
| Pain on coccyx | Gluteus maximus tightness, possibly piriformis or levator ani involvement |
| Crest of ilium – pain | Tight quadratus lumborum/gluteus medius and/or lumbodorsal dysfunction |
| Pain on greater trochanter | Tight abductors/hip dysfunction |
| Pain on lumbar spinous processes (especially L5) | Tight paraspinal muscles |
| Pain mid-dorsal spinous processes | Lower cervical dysfunction |
| Pain spinous process of C2 | Levator scapulae tight: C1–2, 2–3, dysfunction |
| Pain on xyphoid process | Rectus abdominus tight. 6–8 rib dysfunction |
| Pain on ribs, on mammary or axillary line | Pectoralis tightness. Visceral dysfunction referred to here |
| Pain at sternocostal junction upper ribs | Scalenus tightness |
| Pain on clavicle, medial aspect | Tight sternocleidomastoid |
| Pain transverse process of atlas | Tight sternocleidomastoid and/or recti capitis lateral. Atlanto-occipital dysfunction |
| Pain on occiput | Upper cervical or atlas dysfunction |
| Pain on styloid process of radius | Elbow dysfunction |
| Pain on epicondyles | Local muscular or elbow dysfunction |
| Pain at deltoid attachment | Scapulohumeral dysfunction |
| Mandibular condyles painful | Temporomandibular joint dysfunction. Tight masticators |
Felix Mann, pioneer acupuncture researcher and author, describes periosteal acupuncture as being more effective than ordinary acupuncture in a number of conditions (Mann 1963). He lists the sites given in Table 4.5 amongst the common sites usefully employed in this approach. Clinical experience indicates that NMT ischaemic compression techniques and muscle energy methods are as likely as traditional needling to produce benefit when treating these points.
Table 4.5 Periosteal acupuncture points and associations
| Site | Associated with |
|---|---|
| 1. Appropriate transverse cervical process | Headache, migraine, interscapular pain and cervical spondylosis |
| 2. Area of sacroiliac joint | Low back pain, sciatica without neurological deficit, testicular pain |
| 3. Coracoid process | Painful shoulder joint |
| 4. Medial condyle tibia | Knee pain, without advanced pathology |
| 5. Neck of femur | Hip pain, without major changes evident on radiography |
| 6. Lateral aspect of posterior spine of lower lumbar vertebrae | If sacroiliac joint (2 above) does not yield benefit, these areas may be used |
Confusion?
The soft tissues are of major importance to the body’s economy, structural integrity and well-being. They are also a major source of pain and dysfunction and, as must now be obvious, of reflex disturbances.
The various theories, methods and descriptive terminologies relating to the many point systems and classifications of ‘points’ are significant inasmuch as NMT offers the opportunity to access and use their potential. If we accept that there are many ways of looking at and interpreting the same phenomenon, then it will be an easy step to acknowledging that an acupuncture point and a trigger point and a Chapman’s reflex point, for example, can all be the self-same point, but with different aspects of its reflex potential being considered in each classification.
NMT can (with other modalities) be used as an effective measure to detect and eliminate noxious trigger points and areas that generate or help to maintain dysfunction, or that influence reflexive activity. Such dysfunction can take the form of muscular weakness, muscular contraction, pain, vasodilatation, vasoconstriction, tissue degeneration, gastrointestinal disturbances, sympathetic nervous system abreactions, respiratory and a myriad other disorders including emotional and ‘psychological’ disorders such as anxiety.
Noxious (pain producing) points that are the end result of various forms of stress imposed on the tissues housing them may reside in either hypertonic or hypotonic muscle, or in ligamentous or fascial tissues, or in apparently normal tissues. When active, such points will always be sensitive to correctly applied pressure and can often be neutralized by manual pressure or a combination of chilling and manual pressure and stretching.
In the treatment sections there will be discussion of methods for locating and treating such points; however, what effects each therapist attempts to achieve by manipulating reflexively active points depends on the individual’s professional training and beliefs.
Akbayrak T., Citak I., Demirturk F., et al. Manual therapy and pain changes in patients with migraine—an open pilot study. Adv Physiother. 2001;3:49-54.
Akbayrak T., Akarcal V.I., Karabudak R., et al. The results of connective tissue manipulation in the treatment of tension type headache. Pain Clin. 2002;13:343-347.
Arbuckle B. The selected writings of Beryl Arbuckle. National Osteopathic Institute and Cerebral Palsy Foundation. 1977.
Baldry P. Acupuncture, trigger points and musculoskeletal pain. Edinburgh: Churchill Livingstone, 1993.
Birch S. On the impossibility of trigger point-acupoint equivalence: a commentary on Peter Dorsher’s analysis. J Altern Complement Med. 2008;14(4):353-359.
Bischof I., Elmiger G. Connective tissue massage. In: Licht E., editor. Massage, manipulation and traction. New Haven: Connecticut, 1960.
Bosey J. Acupunct Electrother Res. 1984;9(2):79-106.
Botek S. Acupunct Electrother Res. 1985;10(3):241.
Burkholder T. Mechanotransduction in skeletal muscle. Front. Biosci. 2006;12:174-191.
Caso M. Evaluation of Chapman’s neurolymphatic reflexes via applied kinesiology: a case report of low back pain and congenital intestinal abnormality. J Manipulative Physiol Ther. 2004;27(1):66-72.
Chaitow L. An introduction to Chapman’s reflexes. British Journal of Naturopathy. 1965. (Spring)
Chaitow L. Acupuncture treatment of pain. Vermont: Healing Arts Press, 1991.
Chaitow. Positional release techniques, ed 2. Edinburgh: Churchill Livingstone, 2001.
Chen E. Cross-sectional anatomy of acupoints. Edinburgh: Churchill Livingstone, 1995.
Citak I., Akbayrak T., Akarcali I., Demirturk F. Connective tissue manipulation in treatment of fibromyalgia syndrome: a pilot study. Turk J Physiother Rehabil. 2001;12:110-114.
Citak-Karakaya I., et al. Short and long-term results of connective tissue manipulation and combined ultrasound therapy in patients with fibromyalgia. J Manipulative Physiol Ther. 2006;29:524-528.
D’Ambrogio K., Roth G. Positional release therapy. Mosby: St Louis, Missouri, 1997.
Degenhardt B., Kuchera M. Update on osteopathic medical concepts and the lymphatic system. J Am Osteopath Assoc. 1996;96(2):97-100.
Degenhardt B., et al. Role of osteopathic manipulative treatment in altering pain biomarkers: a pilot study. Journal American Osteopathic Association. 2007;107:387-394.
Deig D. Positional release technique. Boston: Butterworth-Heinemann, 2001.
DiGiovanna E. An osteopathic approach to diagnosis and treatment. Philadelphia: Lippincott, 1991.
Demirturk F., Akbayrak T., Citak, et al. Acute effects of connective tissue manipulation on skin temperature and blood flow rate in a patient with Raynaud’s disease. Turkish J Physiother Rehabil. 2000;11:159-160.
Demirturk F., Akarcali I., Akbayrak T., et al. Results of two different manual therapy techniques in chronic tension type headache. Pain Clin. 2001;14:121-128.
Dorsher P. (Poster 196) Myofascial pain: rediscovery of a 2000-year-old tradition? Arch Phys Med Rehabil. 2004;85(9):e42.
Dorsher P., Fleckenstein J. Trigger Points and Classical Acupuncture Points. Deutsche Zeitschrift fuer Akupunktur. 2008;51(4):6-11.
Ebner M. Connective tissue massage. Edinburgh: Churchill Livingstone, 1962.
Ernst M. Acupunct Electrother Res. 1983;8(3/4):343.
Gray H. Gray’s anatomy, ed 35. London: Longman, 1973.
Huijing P., Baan G. Myofascial force transmission causes interaction between adjacent muscles and connective tissue: effects of blunt dissection and compartmental fasciotomy on length force characteristics of rat extensor digitorum longus muscle. Arch Physiol Biochem. 2001;109:97-109.
Jones L. Strain and counterstrain. Academy of Applied Osteopathy. 1980. Boulder, Colorado
Khalsa P., et al. The 2005 Conference on the Biology of Manual Therapies. J Manipulative Physiol Ther. 2005;29:341-346.
Kuchera W. Lumbar and abdominal region. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Langevin H.M., Bouffard N.A., Badger G.J., et al. Dynamic fibroblast cytoskeletal response to subcutaneous tissue stretch ex vivo and in vivo. Am J Physiol Cell Physiol. 2005;288(3):C747-C756.
Langevin H. Connective tissue: A body-wide signaling network. Med Hypotheses. 2006;66(6):1074-1077.
Levin S.M. Put the shoulder to the wheel: a new biomechanical model for the shoulder girdle. In: Ribreau C., editor. MechanoTransduction. Paris: Societe Biomechanique; 2000:131-136.
Lewit K. Manipulative therapy in rehabilitation of the locomotor system. London: Butterworths, 1992.
Lewith G., Kenyon J. Soc Sci Med. 1984;19(12):1367-1376.
Lines D., McMillan A., Spehr G. Effects of soft tissue technique and Chapman’s neurolymphatic reflex stimulation on respiratory function. J Aust Chiropr Assoc. 1990;20:17-22.
McKechnie A., et al. Anxiety states: A preliminary report on the value of connective tissue massage. J Psychosom Res. 1983;27(2):125-129.
McPartland J.M., Simons D.G. Myofascial trigger points: translating molecular theory into manual therapy. Journal Manual and Manipulative Therapies. 2007;2007(14):232-239.
Mann F. The treatment of disease by acupuncture. London: William Heinemann Medical, 1963.
Mann F. International Conference of Acupuncture and Chronic Pain. 1983. September 1983
Mannino J. The application of neurological reflexes to the treatment of hypertension. J Am Osteopath Assoc. 1979;79(4):225-230.
Martin R., editor. Dynamics of correction of abnormal function. Sierra Madre: Ralph Martin, 1977.
Melzack R., Stillwell D., Fox E. Trigger points and acupuncture points of pain. Pain. 1977;3:3-23.
Myers T. Anatomy Trains, ed 2. Edinburgh: Churchill Livingstone, 2008.
Northup G. The role of the reflexes in manipulative therapy. J Am Osteopath Assoc. 1941;40:521-524.
Oszeweski W., Engeset A. Intrinsic contractility of leg lymphatics in man. Lymphology. 1979;21:81-84.
Owens C. An endocrine interpretation of Chapman’s reflexes. Newark, Ohio: American Academy of Osteopathy, 1980.
Patriquin D. Chapman’s reflexes. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Reed B., Held J. Effects of sequential connective tissue massage on autonomic nervous system of middle aged and elderly adults. Phys Ther. 1988;68:1231-1234.
Serizawe K. Tsubo: vital points for oriental therapy. San Francisco: Japan Publications, 1976.
Simons D. Understanding effective treatments of myofascial trigger points. Journal of Bodywork and Movement Therapies. 2002;6(2):81-88.
Takeshige C. Acupunct Electrother Res. 1985;10(3):195-203.
Thie J. Touch for health. California: DeVorss, 1973.
Travell J., Simons D. Myofascial pain and dysfunction. vol 2. Baltimore: Williams & Wilkins; 1992.
Vannerson J., Nimmo R. Specificity and the law of facilitation in the nervous system. The Receptor. 2(1), 1971.
Wall P., Melzack R. Textbook of pain. Edinburgh: Churchill Livingstone, 1989.