CHAPTER 28 Range of movement
What is range of movement (ROM)?
The function of a joint is to allow full range, friction free movement between its segments. The full range of movement (FROM) of a joint incorporates both the accessory movement (which cannot be produced in isolation by an individual) and the physiological movement.
Active physiological movement
The physiological movement of a joint is the active voluntary movement that a person can perform themselves. When performing an active physiological movement (AROM) there is combined involvement of the joint, muscle and motor control. Therefore these are all potential sources of dysfunction. The more common presentation is that of a reduced ROM, however instability, loss of proprioception and poor control could lead to an excessive ROM. In a neurologically impaired patient the potential causes of altered AROM include:
Passive physiological movement
A passive physiological movement (PROM) is defined as a movement within the unrestricted ROM for a segment, which is produced entirely by an external force. In the spinal joints this is referred to as a ‘passive physiological intervertebral movement’ (PPIVM). Although not actively involved in producing the movement, muscles and other soft tissue around the joint may still reduce the PROM. Excessive PROM is common in neurologically impaired patients particularly related to hypotonia, e.g. subluxation of the shoulder. Of course motor control does not have any influence in this case.
Why do I need to assess range of movement?
A dysfunction of the neural or musculoskeletal systems may lead to joint hypermobility (excessive movement) or hypomobility (reduced movement) either of which may conclude in soft tissue damage, pain and loss of function. Assessment of ROM allows the therapist to identify a potential limitation to functional ability and when combining the findings of AROM and PROM allows the therapist to begin hypothesizing the structures that may be implicated (differential diagnosis).
How do I assess range of movement?
AROM
AROM should be assessed before the PROM is explored.
Patient
The patient’s position will alter depending upon the joint being tested because where possible, the position must allow for FROM. For example, full ROM of hip flexion (hip extension to hip flexion) is only possible in standing. In circumstances where this is not practical, such as an immobile patient, the movement will need to be assessed in two halves.
Therapist
The therapist will already have observed the patient’s general AROM during the performance of functional activities (S3.18). However, as function involves the combined movement of many joints, a more specific assessment of the individual segments involved may be required. Assessment of all the cardinal planes of movement should be considered although clinical judgement should be used as to whether it is necessary to assess every joint and every direction. For example, at the hip the cardinal planes are flexion, extension, abduction, adduction and medial/lateral rotation.
 Clinical hints and tips
Clinical hints and tips
Based on the subjective assessment and functional objective assessment the therapist needs to use clinical judgement as to whether it is it necessary to assess every joint and every direction.
Limb testing
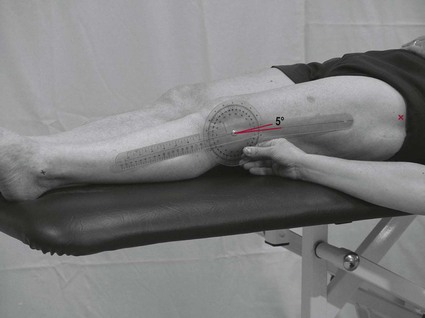
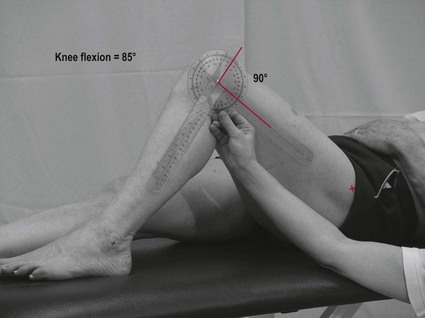
Spinal joint testing
Active physiological movements of the spine involve composite movement of each individual vertebral joint and therefore measurement using a goniometer is not possible. Active spinal movements are therefore measured globally using a tape measure.
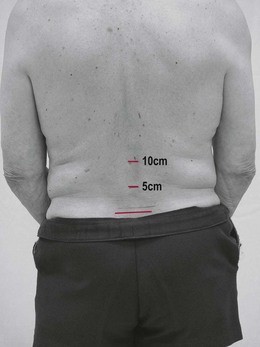

Note: Spinal measurements can also be taken from the tip of the third finger to the floor.
PROM
Patient
The patient’s position will alter depending upon the joint being tested as where possible, the position must allow for FROM.
Therapist
Spinal joint testing
If a restriction of spinal joint movement is suspected, the therapist should explore the region further using passive physiological intervertebral movements (PPIVMs) and passive accessory intervertebral movements (PAIVMs). These assessment techniques are not covered in this text.
Limb testing
Assessment of all the cardinal planes of movement should be considered, although clinical judgement should be used as to whether it is necessary to assess every joint and every direction. Carrying out PROM is identified as a high-risk manual handling task and therefore consideration of the environment/bed height is essential.
End feel
If a reduced PROM is identified using passive physiological movements and the patient’s pain symptoms are not severe, the therapist may continue to investigate the end feel of the joint so that the structures limiting the ROM can be differentiated during analysis.
Note: Hypertonia may restrict the AROM well before the end of PROM. If possible the therapist still needs to investigate the end feel beyond the hypertonic restriction to explore the existence of any soft tissue adaptation.
Recording
The recording of this data could be extensive. It may therefore be wise to note the findings in a list or table form.
Analysis
The therapist’s analysis of ROM will inform other areas of the objective assessment. For example, reduced AROM of the ankle dorsiflexors may explain abnormal gait and poor balance. The aim of this assessment tool is to establish the patient’s ROM and to begin hypothesizing about any possible limiting factors. In the case of a reduced ROM, this can be achieved by comparing the findings from both AROM and PROM assessments. For example, if PROM is greater than AROM then a deficit of muscle contraction should be suspected. This could be caused by muscle weakness, hypotonia, hypertonia or sensory loss. However, if both PROM and AROM are reduced, the limit is more likely to be linked with a soft tissue adaptation. Note: Pain could be a causal factor in both these scenarios and needs further investigation (S3.29).
References and Further Reading
Fox J, Day R. A physiotherapist’s guide to clinical measurement. Edinburgh: Churchill Livingstone/Elsevier; 2009.
Magee DJ. Orthopaedic physical assessment, ed 4. Canada: Elsevier Sciences; 2006.
Petty NJ. Neuromusculoskeletal examination and assessment: a handbook for therapists. Edinburgh: Churchill Livingstone; 2006.