Chapter 20 Osteoporosis
KEY POINTS
INTRODUCTION
Osteoporosis is a condition in which gradually decreasing bone mass and deteriorating bone structure leads to increased bone fragility and increased risk for fractures, particularly of the wrist, hip and spine (WHO 1994). This process progresses without symptoms until fractures occur or kyphosis becomes apparent. Thus osteoporosis is often described as a silent menace.
Once fractures and deformities have occurred, pain may become a prominent problem and a challenge for people with osteoporosis and everyone involved with their care. Such established osteoporosis is a major cause of morbidity, mortality and reduced quality of life (Lips et al 2005).
INCIDENCE
Osteoporosis affects one in three women and one in twelve men over the age of 50 years (Barlow 1994). The incidence of osteoporotic fractures rises with increasing age. In particular, the incidence of hip fractures rises sharply beyond the age of 65 years in both men and women (Cooper & Melton 1992). Of people surviving to 80 years of age, one in three women and one in five men will suffer a hip fracture. Each year in the UK there are about 60,000 hip fractures, 50,000 wrist fractures and 40,000 clinically diagnosed vertebral fractures (Compston et al 1995, Donaldson et al 1990). The annual NHS cost for managing these is estimated to be in excess of £2.1 billion pounds per year (Cooper 1993). As only 25% of people suffering a hip fracture regain their previous level of independence and up to 20% die within six months, the cost to society is much greater (Jensen & Tondevold 1979).
Interventions to reduce fracture risk have been shown to be clinically and cost effective and should be implemented for those at greatest risk. Women are as likely to suffer an osteoporotic fracture in their lifetime as they are coronary heart disease and the cost effectiveness for interventions are similar for both diseases (Johnell et al 2005).
AETIOLOGY
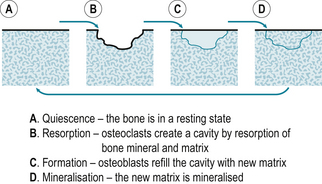
Bone undergoes a repetitive cycle of remodelling. Osteoclasts break down the bone (resorption) and osteoblasts rebuild it (formation) (Fig. 20.1). Throughout childhood bone formation exceeds resorption and bone mass increases. Peak bone mass is achieved by the age of 20 to 30 years and plateaus for approximately 10 years before declining gradually by about 1% per year. During the menopause the rate of bone loss is greater as bone resorption exceeds formation.
Adult bone mass may be lower than average due to impaired acquisition during childhood or a greater than average rate of bone loss later in life. Impaired peak bone mass acquisition accounts for approximately two thirds of the variance in bone mass seen at any age. Genetic factors have the greatest influence on this (Nguyen et al 2003). Suppressed oestrogen, testosterone or growth hormone production and environmental factors such as poor dietary calcium intake and lack of exercise also delay or diminish bone mass acquisition during childhood and adolescence.
Beyond the age of 40 years, hormonal and environmental factors, rather than genetic factors, have the greatest impact on the rate of bone loss (Seeman 2002). A combination of oestrogen deprivation, calcium and vitamin D deficiency and secondary hyperparathyroidism account for the rapid loss seen in postmenopausal women (Cummings et al 1995). Many other epidemiological factors have been identified (Box 20.1). However, the impact of each factor, or combinations of factors, on an individual requires further clarification.

DIAGNOSIS
As osteoporosis causes no symptoms until fractures or kyphosis occur, it may remain undiagnosed for many years. Whilst the strongest predictive factors for sustaining osteoporotic fractures are a previous fracture and a low bone mass measurement (Bouxesin 2003, Cummings et al 1995), diagnosis may predate fractures if individuals and health care professionals routinely consider the risks for osteoporosis, fractures and falls. A variety of tools, such as paper or electronic questionnaires, are available to facilitate the identification of patients at risk (Kanis et al 2002, Kanis & Gluer 2000).
The gold standard method for diagnosis is to measure bone mass, or bone mineral density (BMD), using dual energy x-ray absorptiometry (DEXA). DEXA scans are quick, comfortable and relatively cheap to perform and involve minimal radiation exposure (equivalent to about a days background radiation) (Fig. 20.2). DEXA results correlate strongly with fracture risk (Kanis & Gluer 2000) but other bone qualities such as elasticity and architecture, not measurable with DEXA, also contribute.

Bone density readings of the hip and spine are given as the number of standard deviations below the mean peak bone mass of a 20 to 30 year old woman (T-score), the standard deviations below the age matched mean (Z-score) (Fig. 20.3A,B) and as a reading of g/cm2. A woman has normal bone density if her T-score is no lower than 1 standard deviation below the young adult mean (T-score higher than –1). Osteopaenia (mild thinning of the bones) is present if density lies between 1 to 2.5 standard deviations below the young adult mean. Readings representing osteoporosis are more than 2.5 standard deviations below the young adult mean (T-score below –2.5) and established osteoporosis is present if at least one fragility fracture has occurred at this low level (WHO 1994). If the Z-score is low, bone density is lower than expected for the patient’s age and other risk factors or underlying disease must be considered. The same criteria are used for men but further work is required to determine the relationship between these scores and fracture risk.
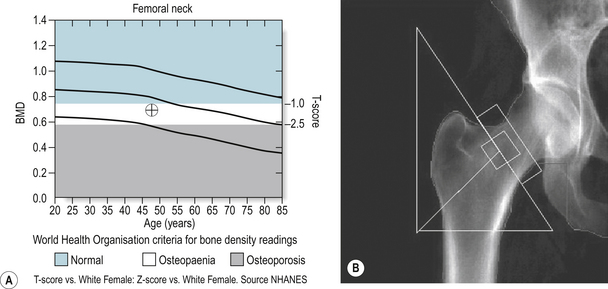
Figure 20.3 DEXA report showing normal hip bone density of a 42-year-old female. The light green shaded area represents normal bone density (T-score above −1), the white osteopaenia (T-score between −1 and −2.5) and the darker green osteoporosis (T-score below −2.5).
Image on loan courtesy of Vertec and Hologic.
Bone biochemistry (consisting of corrected calcium, alkaline phosphatase and inorganic phosphate) is normal in osteoporosis. Serum and urinary bone marker measurements are used to determine osteoblast and osteoclast activity, but may only be available in research departments. Other diagnostic tools used for diagnosis, screening, or research purposes include heel ultrasonography, quantitative computed tomography (QCT) and bone biopsy. Bone biopsy provides a definitive diagnosis of osteoporosis but is rarely required. Axial DEXA is recommended to confirm a diagnosis of osteoporosis following a positive finding on peripheral imaging e.g. heel ultrasonography.
DIFFERENTIAL DIAGNOSIS
Low bone density can be assumed to be due to osteoporosis only if other causes have been excluded (Box 20.2). For this reason screening blood tests for metabolic, endocrine and malignant disease are often performed in patients with low bone density. Typically, these tests include full blood count, erythrocyte sedimentation rate (ESR), urea and electrolytes, liver function, bone biochemistry, thyroid function, testosterone and gonadotrophins (in men) and perhaps parathyroid hormone and vitamin D levels (depending on the history and other findings). Serum immunoglobulins and electrophoresis and urinary Bence-Jones proteins should be measured if myeloma is suspected.
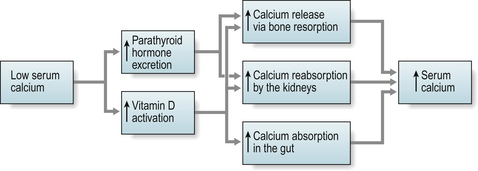
Calcium and vitamin D deficiency can occur in specific populations e.g. those from the Indian sub continent including teenage girls, and is common amongst older people, particularly those in long-term nursing or residential care. This is often due to poor dietary intake, lack of adequate sunlight exposure, reduced intestinal absorption or renal impairment and leads to impaired mineralisation of bone, known as osteomalacia. The bones become soft, prone to fracture and appear less dense on DEXA. Blood tests may show low/normal calcium, high/normal alkaline phosphatase, low phosphate, and a high parathyroid hormone level (secondary hyperparathyroidism) (Fig. 20.4).
An elevated serum corrected calcium level should raise suspicion of underlying malignancy (primary or metastatic), myeloma or primary hyperparathyroidism due to a parathyroid adenoma.
CLINICAL PRESENTATION
Patients may express concern that they have osteoporosis because they have heard or read about it, entered the menopause early (before 42 years), taken steroid therapy or have a family history of osteoporosis or fractures. The incidental finding of radiological osteopaenia, meaning a fainter appearance of the bones on a plain x-ray, also raises suspicion, but does not confirm the presence of osteoporosis. However patients mostly present with a low trauma fracture (e.g. fall from own body height), sudden severe back pain from a vertebral fracture, or the development of kyphosis and loss of height due to asymptomatic vertebral fractures. Only about a third of vertebral fractures come to medical attention (Gallacher et al 2000, Gehlbach et al 2000).
The vast majority of patients who present with their first or subsequent low trauma fractures are not assessed for osteoporosis (RCP 2007). Years later, women who have sustained wrist fractures go on to suffer hip fractures which are associated with high morbidity and mortality rates. Patients with severe osteoporosis may also suffer vertebral, pelvic or rib fractures spontaneously or from minimal trauma such as coughing or rolling over in bed.
CLINICAL EVALUATION
HISTORY
A detailed medical history is essential to assess a patient’s risks for osteoporosis (Box 20.1), falls and fractures and to consider the possibility of underlying metabolic bone disease or malignancy (Box 20.2). Patients at greatest risk for suffering an osteoporotic fracture are those who have already fractured and those with known low bone mass. For instance, the relative risk for sustaining a new vertebral fracture is more than doubled for a patient with a previous vertebral fracture and quadrupled if the patient also has low bone density. A woman who has just sustained a vertebral fracture has a one in five chance of sustaining another within one year (Lindsay et al 2001).
Fracture liaison services have been shown to improve identification of high-risk patients (McClellan et al 2003). Without these services in place, less than 10% of high-risk patients attending fracture clinics are identified, diagnosed or treated for osteoporosis (RCP 2007). As many fractures occur following falls, patients’ risks for falls must also be assessed in detail and referrals made to physiotherapists or specialist falls clinics as appropriate. Reduction of the risk for falls among the older age group requires a comprehensive multidisciplinary falls risk evaluation and multifactorial intervention (NICE 2004).
EXAMINATION
Whilst some fractures may be painfully obvious others may be detected only after careful examination and investigation. Thoracic kyphosis (Fig. 20.5A,B) may develop gradually as one vertebra after another fractures (or is compressed) or more suddenly if one or more severe wedge fractures occur. The development of the Dowager’s hump is a well recognised but late sign of osteoporosis. As this becomes more pronounced, the lower ribs impinge on the iliac crests and the abdomen protrudes. An exaggerated cervical lordosis is apparent when the patient attempts to look straight ahead. Evidence of a previous wrist fracture may also be seen such as the classical dinner fork deformity of a Colle’s fracture. A shortened externally rotated leg is highly suggestive of a fractured neck of femur.
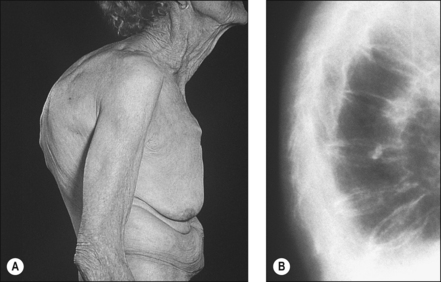
Figure 20.5 (A), (B) Thoracic kyphosis. (Dowager’s hump) (A) Marked thoracic kyphosis due to multiple osteoporotic fractures in an elderly woman with (B) corresponding radiograph.
With permission Hochberg MC (2008). Elsevier.
Examination of the locomotor system includes inspection followed by palpation and then assessment of movement and function. Palpation of the spine for instance may reveal marked tenderness at the site of a fractured vertebra or associated powerful spasm of the paravertebral muscles. Movement of the spine is likely to be globally reduced following an acutely painful vertebral fracture. Pain increases with flexion or with increased intrathoraic pressure such as coughing, patients’ balance, gait and ability to perform simple activities of daily living, including dressing may be significantly impaired.
In addition to examination of the locomotor system it is imperative that patients suspected of suffering with osteoporosis also undergo a full medical examination to elicit signs of any underlying cause for their low bone density (Box 20.2).
RADIOGRAPHY
PLAIN RADIOGRAPHY
The incidental x-ray finding of radiological osteopaenia or vertebral fractures, warrants further assessment for osteoporosis. These incidental vertebral fractures may have been spontaneous and painless or due to trauma many years ago. Previous x-rays may reveal the age of the fracture and progression of the condition. Confusion sometimes arises when reporting which vertebra has fractured. The same fracture may be reported as a T4 vertebral fracture on one x-ray and a T3 compression fracture on another occasion. However, vertebral deformities do not resolve. On a lateral view, they are described as a compression or crush fracture when the vertebra is reduced in height, a wedge fracture when the anterior portion is compressed, or a biconcave fracture if the height of the central portion of the vertebra is reduced superiorly and inferiorly.
BONE DENSITOMETRY
As bone density changes only gradually over years, and DEXAs have a margin of error of a couple of percent, there is nothing to be gained by monitoring patients more frequently than every three to five years. Exceptions include patients with severe established osteoporosis in whom response to treatment is in doubt because of ongoing medical problems, numerous ongoing risk factors, difficulties tolerating medication, further fractures and in whom a deteriorating scan result is likely to influence their management.
SPINAL MORPHOMETRY
Spinal morphometry using bone densitometry can also be used and although less information is provided by these images compared with plain x-ray, the radiation dose is much lower (Fig. 20.6).

TECHNETIUM ISOTOPE SCANS
Isotope bone scans may highlight a recent fracture, such as a pelvic insufficiency fracture, not evident on plain x-ray.
MAGNETIC RESONANCE IMAGING
Magnetic resonance imaging (MRI) scans of the spine or pelvis are indicated when there is clinical suspicion of underlying malignancy or significant neurological compromise. The difficulties of performing an MRI scan on patients with severe back pain and kyphosis must be considered carefully. Extra analgesia and sedation may be required.
QUANTITATIVE COMPUTED TOMOGRAPHY
Quantitative computed tomography (QCT) of the spine have been used mainly in research settings and are reported to give additional information regarding bone quality that is not detected on bone densitometry (Engelke et al 2008).
PROGRESSION AND PROGNOSIS
Osteoporosis cannot be cured but the rate of bone loss may be slowed and the risk for further fractures reduced (but not eliminated). Gradual bone loss is a normal feature of ageing, thus interventions may be deemed to be successful if bone density remains stable. Although most treatments offer only a small increase in bone density of up to about five percent during the first year or two, fracture risk reduction may be up to seventy percent (Black et al 1996, 2007).
Difficulties arise when patients sustain further fractures despite treatment. This may reflect lack of efficacy, or conversely, even more fractures may have occurred had treatment not been given. Poor adherence is common and reasons include the development of side-effects, difficulties following the administration instructions and inappropriate expectations and then disappointment when, for example, the medication fails to relieve back pain.
As osteoporosis does not affect morbidity or mortality until fractures occur, there is a danger of diagnosing people too early and creating a large population of worried well. However, if patients remain undiagnosed and subsequently fracture, the outcome can be devastating. Patients visit their GP approximately 14 times in the first year following a vertebral fracture and quality of life reduces significantly with each subsequent vertebral fracture (Dolan & Jorgensen 1998). Worst still, only 25% of people suffering a hip fracture regain their previous level of independence and up to 20% die within 6 months.
AIMS AND PRINCIPLES OF MANAGEMENT
General population screening for osteoporosis is neither clinically appropriate nor cost effective. Selective screening of patients at high risk for osteoporotic fractures, however, is worthwhile (NICE 2008a, 2008b, NOGG 2008, SIGN 2003). Tools that predict a patient’s absolute risk for fracture over 10 years are particularly useful for directing treatment appropriately (Kanis 2008).
Treatment may be indicated for patients with osteoporosis to reduce their risks for sustaining their first fracture (primary prevention) or subsequent fractures if they have already suffered one (secondary prevention). Treatment is also recommended to prevent the development of osteoporosis (prophylaxis) such as that occurring with longterm corticosteroid use.
NICE Technology Appraisal Guidelines for primary prevention and secondary prevention of osteoporotic fractures in postmenopausal women, recommend treatment only for women of certain age groups, with specific numbers of given risk factors and bone density T-scores (NICE 2008a, 2008b). NICE Clinical Guidance for the management of osteoporosis affecting younger women, men and people on corticosteroids is awaited. Guidance for the prevention and treatment of corticosteroid-induced osteoporosis is available from The Royal College of Physicians (RCP 2000). The National Osteoporosis Guideline Group (NOGG) give guidance on the management of osteoporosis in men and women based on the use of FRAX, an on-line 10-year probability of fracture risk assessment tool that incorporates the main risk factors identified by the World Health Organisation (NOGG 2008).
Whilst recommendations regarding who should receive medication differ, all agree that lifestyle risk factors for osteoporosis, fractures and falls should be addressed and deficiency in calcium and vitamin D avoided.
PATIENT EDUCATION
At risk patients should be educated about osteoporosis prior to diagnosis if prophylaxis or lifestyle changes are required. Once a diagnosis of osteoporosis has been established, the patient requires an explanation of the condition, what they can do to help themselves and how long term treatment slows progression but cannot offer a cure. Clear instructions regarding how to take the medication are essential, including dosage and duration.
Patients should be informed of resources available to them for advice, psychological and social support and further information. A wide variety of information is available from The National Osteoporosis Society (NOS 2003) and Arthritis Research Campaign (http://www.arc.org.uk/). Additional information may also be available at GP surgeries, hospital outpatient clinics or osteoporosis department help lines. Local National Osteoporosis Groups are established in many parts of the UK.
SELF-MANAGEMENT
Lifestyle risk factors for osteoporosis, fractures and falls vary in significance and some are more amenable to modification than others (Box 20.1). Currently patients are advised that they should not smoke at all and should not drink more than 1 or 2 units of alcohol a day. A healthy balanced diet including adequate amounts of calcium is important and excessive caffeine consumption should be reduced.
Approximately ten minutes of sunlight exposure to the face and forearms reduces the risk for vitamin D deficiency. Weight-bearing exercise delivered in a variety of ways, slows or prevents further bone loss, in postmenopausal women (Martyn-St James & Carroll 2008) and physiotherapy improves pain and functional performance (Malmros et al 1998).
THERAPY MANAGEMENT OF OSTEOPOROSIS
Physiotherapists and occupational therapists often have a high profile within the osteoporosis team. Therapists can undertake specialist roles for education and treatment and may adopt a modern matron approach to ensuring all eligible patients are given appropriate treatment, advice and preventative strategies.
ASSESSMENT
Assessment should include metrology, function, pain, general mobility, aerobic testing, and quality of life. The principles of assessment are covered in chapters 3 and 4. In this section specific reference is made to assessments that have been adopted for people with osteoporosis.
METROLOGY
Height is an easy way to assess patients over time, particularly as patients will lose height with each vertebral fracture. Height does vary with other factors, such as diurnal rhythms - patients will often regain height after rehabilitation - therefore some of the height loss may be postural. Tragus or occiput to wall measurement or a flexi curve can be used to assess posture and evaluate the effects of treatment interventions (Laurent et al 1991).
A measurement of posture is important as a kyphotic posture leads to loss of balance, which is exacerbated by muscle weakness, so rehabilitation can be targeted to such problems (Mika et al 2005, Sinaki et al 2005). Trunk lateral flexion can be assessed with a tape measure to evaluate spinal mobility (Moll et al 1972) and highlight balance restrictions or pain limitation. Care should be taken as patients may become unsteady when tested. Upper and lower limb mobility and range of movement should be tested. Due to increasing kyphosis shoulder range of movement and function can be limited (Pearlmutter et al 1995).
FUNCTION
Functional tests are numerous and there are many validated tools (Ch. 4). One of the simplest tests is the timed up and go test (TUG) (Podsiadlo & Richardson 1991). The TUG times a patient standing from a chair with no arms, walking 5 metres and returning to sit down. The average time to complete this test is 15 seconds (Podsiadlo & Richardson 1991). Patients may vary from 12 seconds up to 85 seconds. The TUG can demonstrate clinical improvement following an intervention. Other tests to be considered include functional reach, and timed stairs climb and dressing activities (Helmes et al 1995, Lyles et al 1993).
PAIN
Pain should be monitored. A visual analogue score is quick (Melzack 1983, Scott & Huskisson 1976) where a pain diary can be time consuming. Physiotherapists may use a manual therapy assessment protocol to evaluate symptoms. However, accessory mobilisations of the spine should be excluded due to the potential risk of further fracture and increase in pain levels.
GENERAL MOBILITY
Many patients with osteoporosis are at risk of falls. This could be due to altered proprioceptive and kinaesthetic awareness resulting from kyphosis and altered posture. A record should be maintained of the number of falls, including reason for fall and injuries sustained (NICE 2004).
AEROBIC TESTING
Aerobic testing is not performed routinely by therapists. However, it can form part of a special test in some individuals who would benefit from an intervention improving aerobic capacity.
QUALITY OF LIFE
Quality of life can be assessed using generic measures (Ch. 4) or specific measures, e.g. the European Foundation for Osteoporosis Quality of Life Measure (Qualetto) (Lips et al 1996).
INTERVENTIONS
Osteoporosis is a multi-factorial condition as is the risk of fracture and undertaking an early intervention with the multi-disciplinary team is essential. The high risk areas for fracture are areas of high trabecular bone content, e.g. hip and spine. Treatment and exercises must be targeted to these vulnerable areas. Trunk flexion should be avoided as this can provide a high risk of vertebral fracture due to the biomechanics of the trabecular tissue (Myers & Wilson 1997).
PAIN RELIEF
Following assessment the therapist aims to control pain levels, gain the patient’s trust and confidence and willingness to continue with further treatment. Modalities for pain relief are varied and include management of both acute post-fracture pain and management of chronic pain from altered posture and kyphosis. Treatments should be simple to enable patients to continue at home and self-management should be a priority.
The following interventions may be appropriate for people with osteoporosis pain:
Many patients try alternative treatments such as aromatherapy and reflexology. Further information on pain relief is available within the National Osteoporosis Society booklet (NOS 2003).
POSTURAL CORRECTION
Kyphosis can be due to a combination of muscle weakness and muscle imbalance. Patients with vertebral fracture have a further biomechanical alteration with a reduction in anterior vertebral height in comparison to the posterior height, increasing with multiple fractures (Genant et al 1993, Myers & Wilson 1997). Fractures can exacerbate muscle imbalance and a vicious cycle of muscle pain and weakness can perpetuate increasing kyphosis and further fracture (Huang et al 2006).
By addressing posture correction and giving ergonomic advice, a more muscle-efficient posture can be adopted, pain can be reduced and overall biomechanics improved. This is often demonstrated by an increase in patient activities of daily living and improvement in metrology. Advice should be given regarding sleeping positions with particular attention to the cervical spine and hips, which are common sites of discomfort. The use of lumbar rolls for the spine should be advised for sitting and travelling to improve posture and relieve discomfort. Ergonomic advice regarding sitting positions should be given as basic information, and advice on office seating and armchair design should be highlighted. Patients should be made aware of their local resource centres, e.g. the Disabled Living Foundation.
Osteoporosis does not only affect retired post-menopausal women, therefore occupational therapists may need to perform fit-for-work assessment. Further self-management advice on postural correction is applicable in some cases, e.g. the Alexander technique, Pilates etc.
TAPING
Taping can be used for pain relief and proprioceptive feedback. It is important to assess skin viability as taping may be contraindicated in those with hypersensitivity or susceptibility to skin tears. Glucocorticoid induced osteoporosis needs careful assessment due to possible drag of the tape. The proprioceptive input should be accompanied by suitable home exercise programme for the thoracic spine and shoulder to maximise the benefits of taping.
ORTHOTIC BRACING
The debate for and against bracing continues due to lack of evidence. Orthoses have been shown to reduce deformity and bracing of the trunk may reduce postural sway, pain and possibly reduce risk of falls as well as improving quality of life (Pfiefer et al 2004).
BREATHING EXERCISES
Breathing exercises are important for many patients. Some people experience more pain from vertebral fractures on deep inhalation and coughing. Consequently, they reduce the depth of inhalation and are at further risk of chest infection.
RELAXATION
Relaxation can be very beneficial for patients with osteoporosis and the occupational therapist may lead this aspect of management (Chs 9 & 11). The Laura Mitchell method can be very useful (Bell & Saltikov 2000).
PACING
Pacing may be used as part of a pain management strategy. A gradual increase in exercise repetitions as well as exercise intensity and amount of resistance used can be beneficial. Patients frequently require reassurance that they are increasing their exercise intensity correctly (Harding & Watson 2000).
EXERCISE
There is good evidence for the benefit of exercise as a treatment for osteoporosis and as a prevention strategy (Berard et al 1997, Chow et al 1989, Joakimsen et al 1997, Kemper et al 2000, Wolff et al 1999). Studies in men are also becoming more common (Kelley et al 2000, Maddslozzo & Snow 2000).
Patients worry that if they do too much exercise they will sustain fractures but they need to load trabecular bone areas with gravity and weight to stimulate osteoblast activity. Physiotherapists must therefore reassure patients that movements in the correct patterns, e.g. avoiding flexion, are beneficial not detrimental. Many patients are surprised at how strenuously they can exercise without causing or exacerbating pain. People with osteoporosis can lift surprising amounts of weight (Kerr et al 1996) and weights and spinal loading are recommended for both prevention and treatment (Sinaki et al 2005).
Exercise should be viewed as a lifestyle change and should be undertaken for the rest of their lives and not only for the duration of the intervention. Studies have demonstrated that exercise can improve quality of life following vertebral fracture (Gardner et al 2000, Steinberg et al 2000). It is important to advise the whole family on exercise to prevent osteoporosis.
HYDROTHERAPY
In the hydrotherapy pool the risk of falling and fracturing is much reduced, as long as patients are safely managed in the surrounding pool area. The physiological effects of immersion need to be considered (Hall et al 1990) for example in patients with renal problems.
Immersed patients experience pain relief and buoyancy of the water assists range of movement. Patients progress to resisted movement for muscle strengthening (Levine 1984). The action of a muscle/tendon ‘pull’ on a bone will also stimulate osteoblast activity (Nordin & Frankel 1989). Exercises without resistance including trunk rotation can be very beneficial for pain relief in osteoporosis (Hall et al 1990). Such exercises are easy to perform when standing, improve the patient’s confidence in the water, allow the trunk to be supported by hydrostatic pressure and facilitate spinal column lengthening.
Patients can perform exercises to correct postural alignment, stretch pectoral muscle groups, perform trunk extension with or without equipment and increase the buoyancy, resistance and stamina. Cardiovascular fitness and respiratory exertion can be facilitated more easily in water due to the physiological demands of the immersion (Levine et al 1984). Hydrotherapy alone does not increase bone density and consequently patients also need a land-based exercise programme.
GENERAL MOBILITY AND BALANCE RE-EDUCATION
Balance and mobility need to be addressed to prevent further falls and fracture. Balance exercise is important in preventing fracture (Gardner et al 2000, Steinberg et al 2000) and patients should be advised how to continue their exercise programmes once discharged. Tai Chi is an effective technique for fall prevention. Tai Chi classes, Alexander technique, Pilates and Yoga, may be available locally. Further details can be obtained from the NICE Falls Guideline (NICE 2004).
COMMON PHARMACOLOGICAL APPROACHES
BISPHOSPHONATES
Bisphosphonates reduce the rate of bone resorption and significantly reduce the risk for fracture. Generic alendronate is the first line agent for osteoporosis. Large randomised placebo controlled clinical trials have shown that treatment with alendronate significantly increases bone mineral density and reduces risk for hip fracture by 53% and clinical vertebral fracture by 45% (Black et al 2000). When used for ten years, alendronate remained effective and did not lead to significant deterioration in bone quality, despite the prolonged inhibition of bone resorption (Bone et al 2004). As bisphosphonates bind to bone and continue to exert an antiresorptive effect for years after discontinuation, further studies are required to determine longer-term safety. Some specialists suggest that a break from therapy, after 5 years, may be appropriate for patients at lower risk for fractures (Black et al 2006).
In order to reduce the risk for developing oesophagitis, alendronate should be taken (usually once weekly) with a large glass of water first thing in the morning before having anything to eat or drink. The patient must then keep their oesophagus upright for at least 30 minutes, but preferably 60 minutes, before lying down or having anything else to eat or drink. Some patients misinterpret the instructions and spend the whole hour standing up when sitting upright would suffice.
Other bisphosphonates are available but are not yet generic and therefore much more expensive, e.g. Risedronate (McClung et al 2001), Ibandronate (Delmas et al 2006) and Zoledronate (Black et al 2007). A rare, but potentially severe, side effect of bisphosphonate therapy is osteonecrosis of the jaw in which the bone of the mandible or maxilla becomes exposed and necrotic. Patients are encouraged to maintain good dental hygiene and to inform their dentist that they are taking bisphosphonates. For patients with poor oral hygiene, a dental examination is advisable before commencing therapy. Extractions are not contraindicated but root filling is preferred (Arrain & Masud 2008).
CALCIUM AND VITAMIN D
Calcium and vitamin D supplements are often required in addition to the bisphosphonates to treat, or prevent the development of, osteomalacia. This is particularly important for older people with limited sunlight exposure. Numerous supplements are available, some being more palatable than others. Correction of vitamin D deficiency has also been shown to improve muscle strength and may reduce frequency of falls (Venning 2005).
OTHER THERAPEUTIC AGENTS FOR OSTEOPOROSIS
For some patients, who are unable to take bisphosphonates or fail to respond to them, alternative agents are available, although guidelines may restrict their use. Raloxifene, a selective oestrogen receptor modulator (or SERM) is recommended by NICE as an alternative to bisphosphonate therapy for the secondary prevention of osteoporotic fractures (Ettinger et al 1999).
Strontium ranelate is reported to have both antiresorptive and anabolic (bone building) effects (Meunier et al 2004, Reginster et al 2005). NICE recommend strontium ranelate as a third line agent (after alendronate and risedronate) for primary and secondary prevention but again only if certain clinical and bone density criteria are met (NICE 2008a, 2008b). Teriparatide leads to significant increases in bone mineral density, improved bone architecture and a reduction in risk for vertebral and non-vertebral fractures (Neer et al 2001). The significant cost and potential adverse effects however restrict its use (NICE 2008a, 2008b).
Long-term calcitonin therapy has been shown to increase bone mineral density and reduce the risk for vertebral fractures in postmenopausal women. Calcitonin also has analgesic properties and is given, for up to 2 weeks, to patients with painful vertebral fractures and to facilitate rehabilitation in the acute phase (Knopp et al 2005). Although effective, hormone replacement therapy (HRT) is no longer recommended for the treatment of osteoporosis due to associated increased cardiovascular, cerebrovascular and cancer risks (WHI 2002). However HRT is still indicated for women suffering a premature menopause or severe postmenopausal symptoms.
MANAGEMENT OF FRACTURES
General principles for the management of fractures apply, but are more challenging to implement due to poor bone quality and other comorbidity. Hip fractures require surgical fixation or replacement to enable early mobilisation. A multidisciplinary care package is essential for rehabilitation and to reduce the associated high morbidity and mortality in older people (Morrison et al 1998, Roche et al 2005).
Symptomatic vertebral fractures are usually managed medically, with analgesia and perhaps calcitonin. For patients who fail to respond to conservative measures, the injection of cement into the fractured vertebral body, directly (vertebroplasty) or using a balloon (kyphoplasty), may provide some pain relief and structural support in the short term (Diamond 2006 et al, Grafe et al 2005). Long-term benefits are unclear and these procedures should be performed only in units supported by a spinal surgeon (NICE 2003, 2006).
PREVENTION OF FALLS AND FRACTURES
National guidelines emphasise the need for an integrated approach to the management of osteoporosis and falls in order to reduce the rate of fracture amongst older people (DOH 2001, NICE 2004). Thus, fracture liaison services and falls services must work together to provide education and support for health professionals, patients and their carers.
PAGET’S DISEASE
Paget’s disease is the second most common metabolic bone disease after osteoporosis (ARMA 2007). It affects about 2% of the UK population above the age of 55 years and increases with advancing age (ARMA 2007, Paget 1887). However, only 5% of people with Paget’s disease are symptomatic (ARMA 2007). Despite its prevalence, it is often neglected as some health care practitioners consider it to be a benign condition of older adults for which there is no treatment (ARMA 2007, Cooper et al 1999, Whyte 2006).
In Paget’s disease there is a marked increase in bone turnover in parts of the skeleton, resulting in the development of structurally weak abnormal bone, with an increased risk of pain, fracture, deformity, osteoarthritis of the large joints and deafness (ARMA 2007) (Fig. 20.7). Over the last few years a number of highly effective bisphosphonate treatments have been developed which can effectively suppress the symptoms and may prevent the development of complications (ARMA 2007).
CONCLUSION
Osteoporosis is a common condition and causes significant morbidity and mortality. It is often called the silent epidemic. It increases the risk of fractures and only a quarter of people suffering a hip fracture regain their previous level of independence and up to 20% die within six months. Low bone density measurements strongly predict high fracture risk.
Paget’s disease is the second most common meta-bolic bone disease after osteoporosis.
Management of osteoporosis and Paget’s disease requires a combination of pharmacological and non-pharmacological approaches and, as members of the multidisciplinary team, therapists have a key role in the management of these conditions.
ACKNOWLEDGEMENT
We would like to acknowledge Hilary Jones from the Arthritis Research Campaign National Primary Care Centre for her secretarial support with the therapy manuscript.
Write a treatment plan using the recommended guidance for each of the following cases:
 A post menopausal woman with risk factors for osteoporosis (NICE guidance on primary prevention, Physiotherapy guidelines for osteoporosis)
A post menopausal woman with risk factors for osteoporosis (NICE guidance on primary prevention, Physiotherapy guidelines for osteoporosis)www.sign.ac.uk/guidelines/fulltext/71/index.html/ (accessed March 2009).
www.shef.ac.uk/NOGG/downloads.html/ (accessed March 2009).
www.nice.org.uk/TA160/ (accessed March 2009).
www.nice.org.uk/TA161/ (accessed March 2009).
www.arma.uk.net/pdfs/mbdweb.pdf/ (accessed March 2009).
www.arc.org.uk/ search for: “osteoporosis” (accessed March 2009).
www.csp.org.uk/uploads/documents/OSTEOgl.pdf (accessed March 2009).
http://www.csp.org.uk/uploads/documents/OsteoAudit.pdf accessed March 2009.
References and further reading
ARMA, 2007. Standards of Care for people with metabolic bone diseases. www.arma.uk.net/pdfs/mbdweb.pdf/ date (accessed March 2009).
Arrain Y., Masud T. Recent recommendations on bisphosphonate-associated osteonecrosis of the jaw. Dent. Update. 2008;35(4):238-240.
Barlow D.H. Report of the Advisory Group on Osteoporosis. London: Department of Health, 1994.
Bell J.A., Saltikov J.B. Mitchell’s relaxation technique: is it effective? Physiotherapy. 2000;86(9):473-478.
Berard A., Bravo G., Gauthier P. Meta-analysis of the effectiveness of physical activity for the prevention of bone loss in post-menopausal women. Osteoporos. Int.. 1997;7:331-337.
Black D.M., Cummings S.R., Karpf D.B., et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture intervention trial research group. Lancet. 1996;348:1535-1541.
Black D.M., Delmas P.D., Eastell R., et al. Once yearly zoledronic acid for the treatment of postmenopausal osteoporosis. N. Engl. J. Med.. 2007;356(18):1809-1822.
Black D.M., Schwarz A.V., Ensrud K.E., et al. Effects of continuing or stopping alendronate after 5 years of treatment. The fracture intervention trial long-term extension (FLEX): A randomized trial. J. Am. Med. Assoc.. 2006;296(24):2927-2938.
Black D.M., Thompson D.E., Bauer D.C., et al. Fracture risk reduction with alendronate in women with osteoporosis: The fracture intervention trial. J. Clin. Endocrinol. Metab.. 2000;85(11):4119-4124.
Bone H.G., Hosking D., Devogelaer J.P., et al. Ten years’ experience with alendronate for osteoporosis in post-menopausal women. N. Engl. J. Med. 18;. 2004;350(12):1189-1199.
Bouxesin M.L. Bone quality: where do we go from here? Osteoporos. Int.. 2003;14(Suppl. 5):118-127.
Chow R., Harrison J., Dornan J. Prevention and rehabilitation of osteoporosis program. Exercise and osteoporosis. Int. J. Rehabil. Res.. 1989;1:49-56.
Compston J.E., Cooper C., Kanis J.A. Bone densitometry in Clinical Practice. Br. Med. J.. 1995;310:1507-1510.
Cooper C. Epidemiology and public health impact of osteoporosis. Baillière’s Clin. Rheumatol.. 1993;7:459-477.
Cooper C., Melton L.J. Epidemiology of osteoporosis. Trends Endocrinol. Metab.. 1992;3:224-229.
Cooper C., Schafheutle K., Dennison E., et al. The epidemiology of Paget’s disease in Britain: Is the prevalence decreasing. J. Bone Miner. Res.. 1999;14:192-197.
CSP. Physiotherapy Guidelines for the Management of Osteoporosis. London: Chartered Society of Physiotherapists; 1999. Available at http://www.csp.org/uk/uploads/documents/OSTEOgl.pdf. (accessed March 2009)
CSP. Physiotherapy Guidelines for the Management of Osteoporosis. Osteoporosis Audit Pack. London: Chartered Society of Physiotherapists; 2002. Available at http://www.csp.org.uk/uploads/documents/OsteoAudit.pdf (accessed March 2009).
Cummings S.R., Nevitt M.C., Browner W.S., et al. Risk factors for hip fracture in white women. Study of osteoporotic fractures research group. N. Engl. J. Med.. 1995;332:767-773.
Delmas P.D., Adami S., Strugala C., et al. Intravenous ibandronate injections in postmenopausal women with osteoporosis: one-year results from the dosing intravenous administration study. Arthritis Rheum.. 2006;54(6):1838-1846.
Diamond T.H., Bryant C., Browne L., et al. Clinical outcomes after acute osteoporotic vertebral fractures: a 2-year non-randomised trial comparing percutaneous vertebroplasty with conservative therapy. Med. J. Aust.. 2006;184(3):113-117.
DOH. National Service Framework for Older People. London: Department of Health; 2001. Accessed on 31/01/09 at http://www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/DH_4003066. (accessed March 2009)
Dolan P., Jorgensen D.J. The cost of treating osteoporotic fractures in the United Kingdom female population. Osteoporos. Int.. 1998;8:611-616.
Donaldson L.J., Cook A., Thompson R.G. Incidence of fractures in a geographically defined population. J. Epidemiol. Commun. Health. 1990;44:241-245.
Engelke K., Adams J.E., Armbrecht G., et al. Clinical use of quantitative computed tomography and peripheral quantitative computed tomography in the management of osteoporosis in adults: the 2007 ISCD Official Positions. J. Clin. Densitomet.. 2008;11(1):123-162.
Ettinger B., Black D.M., Mitlak B.H. Reduction of vertebral fracture risk in postemenopausal women with osteoporosis treated with raloxifene: results from a 3 year randomised clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. J. Am. Med. Assoc. 18;. 1999;282(7):637-645.
Gallacher S.J., Gallagher A.P., McQuillan C., et al. The prevalence of vertebral fracture amongst patients presenting with non-vertebral fractures. Osteoporos. Int.. 2000;18:185-192.
Gardner M.M., Robertson M.G., Campbell A.J. Exercise in preventing falls and fall related injuries in older people: a review of randomised controlled trials. Br. J. Sports Med.. 2000;34(1):7-17.
Gehlbach S.H., Bigelow C., Heimisdottir M., et al. Recognition of vertebral fracture in a clinical setting. Osteoporos. Int.. 2000;11:577-582.
Genant H.K., Wu C.Y., van Kuijk C., et al. Vertebral fracture assessment using a semi-quantitative technique. J. Bone Miner. Res.. 1993;8:1137-1148.
Grafe I.A., Da Fonseca K., Hillmeier J., et al. Reduction of pain and fracture incidence after kyphoplasty: 1-year outcomes of a prospective controlled trial of patients with primary osteoporosis. Osteoporos. Int.. 2005;16(12):2005-2012.
Hall J., Bisson D., O’Hare P. The physiology of immersion. Physiotherapy. 1990;76:517-521.
Harding V., Watson P. Increasing activity and improving function in chronic pain management. Physiotherapy. 2000;86(12):619-630.
Helmes E., Hodsman A., Lazowski D., et al. A questionnaire to evaluate disability in osteoporotic patients with vertebral compression fractures. J. Gerontol. Series A Biolog. Med. Sci.. 1995;50(2):M91-M98.
Huang M.H., Barrett-Connor E., Grendale G.A., et al. Hyperkyphotic posture and risk of future osteoporotic fracture- Rancho Bernado Study. J. Bone Miner. Res.. 2006;21(3):419-423.
Jensen J.S., Tondevold E. Mortality after hip fractures. Acta Orthop. Scand.. 1979;50(2):161-167.
Joakimsen R.M., Magnus J.H., Fonnebo V. Physical activity and predisposition for hip fractures: a review. Osteoporos. Int.. 1997;7:503-513.
Johnell O., Kanis J.A., Jonssen B., et al. The burden of hospitalised fractures in Sweden. Osteoporos. Int.. 2005;16:222-228.
Kanis J.A. on behalf of the National Osteoporosis Guideline Group. Case finding for the management of osteoporosis with FRAX – assessment and intervention thresholds for the UK. Osteoporos. Int.. 2008;19:1395-1408.
Kanis J.A., Gluer C.C. For the committee of scientific advisors, International Osteoporosis Foundation. An update of the diagnosis and assessment of osteoporosis with densitometry. Osteoporos. Int.. 2000;11:192-202.
Kanis J.A., Johnell O., Oden A., et al. Ten-year risk of osteoporotic fracture and the effect of risk factors on screening strategies. Bone. 2002;30:251-258.
Kelley G.A., Kelley K.S., Tran Z.V. Exercise and bone mineral density in men: a meta-analysis. J. Appl. Physiol.. 2000;88(5):1730-1736.
Kemper, H.G.C., Bakker, I., van Tulder, M.W., et al., 2000. Exercise for Preventing Low Bone Mass in Young Males and Females (Protocol). The Cochrane Library, issue 4, Oxford 2000.
Kerr D., Morton A., Dick I., et al. Exercise effects on bone mass in postmenopausal women are site specific and load dependent. J. Bone Miner. Res.. 1996;11:218-225.
Knopp J.A., Diner B.M., Blitz M., et al. Calcitonin for treating acute pain of osteoporotic vertebral compression fractures: a systematic review of randomised controlled trials. Osteoporos. Int.. 2005;16(10):1281-1290.
Laurent M.R., Buchanon W.W., Bellamy N. Methods of assessment used in ankylosing spondylitis clinical trials: a review. Br. J. Rheumatol.. 1991;30:326-329.
Levine B. Use of hydrotherapy in reduction of anxiety. Psychol. Rep.. 1984;55:526.
Lindsay R., Silverman S.L., Cooper C., et al. Risk of new vertebral fracture in the year following a fracture. J. Am. Med. Assoc.. 2001;285:320-323.
Lips P., Agnusdei D., Caulin F., et al. The development of a European questionnaire for quality of life in patients with vertebral osteoporosis. Scand. J. Rheumatol.. 1996;103(Suppl.):84-85.
Lips P., Van Schoor N.M. Quality of life in patients with osteoporosis. Osteoporos. Int.. 2005;16(5):447-455.
Lyles K.W., Gold D.T., Shipp K.M., et al. Association of osteoporotic vertebral compression fractures with impaired functional status. Am. J. Med.. 1993;94:595-601.
Maddslozzo G.F., Snow C.M. High intensity resistance training: effects on bone in older men and women. Calcif. Tissue Int.. 2000;66(6):399-404.
Malmros B., Mortensen L., Jensen M.B., et al. Positive effects of physiotherapy on chronic pain and performance in osteoporosis. Osteoporos. Int.. 1998;8(3):215-221.
Martyn-St James, M., Carroll, S., November 3, 2008. A meta-analysis of impact exercise on postmenopausal bone loss: the case for mixed loading exercise programmes. Br. J. Sports Med. [Epub ahead of print].
McClellan A.R., Gallacher S.J., Fraser M., et al. The fracture liaison service: success of a program for the evaluation and management of patients with osteoporotic fracture. Osteoporos. Int.. 2003;14:1028-1034.
McClung M.R., Geusens P., Miller P.D., et al. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N. Engl. J. Med.. 2001;344(5):333-340.
Melzack R. The McGill pain questionnaire in: Pain measurement and assessment. New York: Raven Press; 1983. pp. 41–46
Meunier P.J., Roux C., Seeman E., et al. The effects of strontium ranelate on the risk of vertebral fracture in women with osteoporosis. N. Engl. J. Med.. 2004;350(5):459-468.
Mika A., Unnithan M.P. Differences in thoracic kyphosis and back muscle strength in women with bone loss due to osteoporosis. Spine. 2005;30(2):241-246.
Moll J.M.H., Liyanage S.P., Wright V. An objective clinical method to measure spinal extension. Rheumatol. Phys. Med.. 1972;67:668-673.
Morrison R.S., Chassin M.R., Siu A.L., et al. The medical consultant’s role in caring for patients with hip fracture. Ann. Intern. Med.. 1998;128(12):1010-1020.
Myers E.R., Wilson S.E. Biomechanics of osteoporosis and vertebral fracture. Spine. 1997;22(245):25S-31S.
National Osteoporosis Society. Living with Osteoporosis. Coping after Broken Bones. National Osteoporosis Society; 2003. Bath. www.nos.org.ukaccessedMarch 2009o://ww
Neer R.M., Arnaud C.D., Zanchetta J.R., et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N. Engl. J. Med. 10;. 2001;344(19):1434-1441.
Nguyen T.V., Livshits G., Centre J.R., et al. Genetic Determination of Bone Mineral Density: Evidence for a Major Gene. J. Clin. Endocrinol.Metab.. 2003;88(8):3614-3620.
NICE. Percutaneous Vertebroplasty. Interventional Procedure Guidance 12. London: National Institute for Clinical Excellence; 2003. www.nice.org.uk/guidance/IPG12 (accessed March 2009)
NICE. NICE Clinical Guidance 21 Falls: The Assessment and Prevention of Falls in Older People. London: National Institute for Clinical Excellence; 2004. http://www.nice.org.uk/CG021NICEguideline. (accessed 29.01.09).
NICE. Balloon Kyphoplasty for Vertebral Compression Fractures. Interventional Procedure Guidance 166. London: National Institute for Health and Clinical Excellence; 2006. Available at www.nice.org.uk/download-aspx?0 = 1PG166publicinfo (accessed March 2009)
NICE, 2008a. Alendronate, etidronate, risedronate, raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women. NICE technology appraisal guidance 160. Available at www.nice.org.uk/TA160/ (accessed March 2009).
NICE, 2008b. Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women. NICE technology appraisal guidance 161. Available at www.nice.org.uk/TA161 (accessed March 2009).
NOGG, 2008. National Osteoporosis Guideline Group on behalf of the Bone Research Society, British Geriatrics Society, British Orthopaedic Association, British Society of Rheumatology, National Osteoporosis Society, Osteoporosis 2000, Osteoporosis Dorset, Primary Care Rheumatology Society, and Society for Endocrinology. London Available at www.shef.ac.uk/NOGG/downloads.html/ (accessed March 2009).
Nordin M., Frankel V.H. Basic Biomechanics of the Musculoskeletal System, second ed. Philadelphia: Lea & Febiger; 1989. Ch 1, 3-31
Paget J. On a form of chronic inflammation of bones (osteitis deformans). Med.-Chir. Trans.. 1887;16:37-63.
Pearlmutter L., Bode B., Wilkinson W., et al. Shoulder range of motion in patients with osteoporosis. Arthritis Care Res.. 1995;8(3):194-199.
Pfiefer M., Begerow B., Minne H.W. Effects of a newly developed spinal orthosis on posture, trunk muscle strength and quality of life in women with postmenopausal osteoporosis: a randomized controlled trial. Am. J. Phys. Med. Rehabil.. 2004;83(3):177-186.
Podsiadlo D., Richardson S. The timed up and go: a test of functional mobility for frail elderly persons. J. Am. Geriat. Soc.. 1991;39:142-148.
RCP, 2000. Osteoporosis – clinical guidelines for prevention and treatment. Update on pharmacological interventions and an algorithm for management. Royal College of Physicians & Bone and Tooth Society of Great Britain, London.
RCP, 2007. The Clinical Effectiveness and Evaluation Unit, Royal College of Physicians. The National Clinical Audit of Falls and Bone Health in Older People Report. London. Available at http://www.rcplondon.ac.uk/clinical-standards/ceeu/Documents/fbhop-execsummary.pdf. (accessed March 2009).
Reginster J.Y., Seeman E., De Vernejoul M.C., et al. Strontium ranelate reduces the risk of nonvertebral fractures in postmenopausal women with osteoporosis: Treatment of Peripheral Osteoporosis (TROPOS) study. J. Clin. Endocrinol. Metab.. 2005;90(50):2816-2822.
Roche J.J.W., Wenn R.T., Sahota O., et al. Effects of comorbidities and postoperative complications on mortality after hip fracture in elderly people: prospective observational cohort study. Br. Med. J.. 2005;331(7529):1374-1376.
Scott J., Huskisson E.C. Graphic representation of pain. Pain. 1976;2:175-184.
Seeman E. Pathogenesis of bone fragility in women and men. Lancet. 2002;359:1841-1850.
SIGN. Management of Osteoporosis. Guideline 71. Edinburgh: Scottish Intercollegiate Guidelines Network; 2003. Available from http://www.sign.ac.uk/guidelines/fulltext/71/index.html (accessed 24.01.09)
Sinaki M., Brey R.H., Hughes C.A., et al. Balance Disorders and Muscle Strength. Osteoporos. Int.. 2005;16(8):1004-1010.
Steinberg M., Cartwright C., Peel N., et al. A sustainable programme to prevent falls and near falls in community dwelling older people: results of a randomised controlled trial. J. Epidemiol. Commun. Health. 2000;54(3):227-232.
Venning G. Recent developments in Vitamin D deficiency and muscle weakness in elderly people. Br. Med. J.. 2005;330:524-526.
WHO. Assessment of Fracture Risk and its Application to Screening for Postmenopausal Osteoporosis. Report of a WHO Study Group. Geneva: World Health Organisation. 1994.
Whyte M.P. Pagets Disease of Bone. N. Engl. J. Med.. 2006;355:593-600.
Wolff I., van Croonenborg J.J., Kemper H.C., et al. The effect of exercise training programs on bone mass: a meta analysis of published controlled trials in pre and post menopausal women. Osteoporos. Int.. 1999;9(1):1-12.